correlation between plasma levels of apelin and myocardial hypertrophy in rats and humans: possible...
TRANSCRIPT

1. Introduction
2. Patients and Methods
3. Results
4. Discussion
5. Conclusion
Original Research
Correlation between plasma levelsof apelin and myocardialhypertrophy in rats and humans:possible target for treatment?Ines Falcao-Pires, Nadia Goncalves, Cristina Gavina, Sonia Pinho,Tania Teixeira, Claudia Moura, Mario Jorge Amorim, Paulo Pinho,Jose Carlos Areias & Adelino Leite-Moreira†
University of Porto, Department of Physiology, Cardiovascular R&D Unit, Faculty of Medicine,
4200-319 Porto, Portugal
Objective: To investigate the effects of left ventricular (LV) pressure overload
and diabetes on the apelinergic system. Research design/methods: Pressure
overloadwas established in rats by supra-renal aortic-banding. Six weeks later,
diabetes was induced by streptozotocin (65 mg/kg, intraperitoneal), resulting
in four groups: sham, banded (BA), diabetic (DM) and diabetic-banded (DM-
BA). Twelve weeks later, LV function and structure were evaluated by echo-
cardiography and biopsies and plasma samples collected. Furthermore, plasma
samples and LV-endomyocardial biopsies were procured from aortic stenosis
and mitral stenosis patients during surgery to evaluate myocardial expression
of apelin and APJ-receptor and plasma levels of apelin. Results: Direct correla-
tions between apelin plasma levels and LV-mass index and between apelin and
APJ myocardial expression were observed both in humans and rats. Expression
of apelin andAPJwas not significantly altered by pressure-overload in humans,
being downregulated by pressure overload and even more by diabetes in rats.
Finally, an inverse correlation between apelin rat plasma levels and its
myocardial expressionwas observed.Conclusions:While apelin/APJmyocardial
expression decreases, apelin plasma levels increase in LV hypertrophy.
Considering apelin’s positive inotropic and vasodilator properties, this
elevation in apelin plasma levels may represent a compensatory mechanism
to maintain inotropism and cardiac output during pressure-overload or
diabetic cardiomyopathy.
Keywords: aortic-stenosis, apelin, APJ, banding, diabetes, hypertrophy
Expert Opin. Ther. Targets (2010) 14(3):231-241
1. Introduction
Cardiac hypertrophy is a (de)compensatory response to hemodynamic overload thattakes place during ventricular remodeling. Chronic pressure overload is present inpathological conditions such as arterial hypertension, aortic stenosis or in the remotemyocardium of an infarcted ventricle. In such conditions, left ventricular(LV) hypertrophy may result from the increased myocardial workload, or else,from activation of sympathetic nervous system, renin–angiotensin system or otherneurohumoral systems, which induce direct effects on cardiac myocyte growth [1].
The apelinergic system is an emerging neurohumoral system in cardiovascularpathophysiology. The discovery of apelin, the endogenous ligand of orphan-G-protein-coupled-receptor APJ, in 1998 by Tatemoto and colleagues represented alandmark in the field of cardiovascular research [2]. Since its discovery, a great effort
10.1517/14728220903485685 © 2010 Informa UK Ltd ISSN 1472-8222 231All rights reserved: reproduction in whole or in part not permitted

has been made to better understand the pathophysiologicalrole of this peptide, particularly regarding the metabolicchanges associated with diabetes, insulin-resistance and thecardiovascular system, where the components of the apeliner-gic system are widely expressed. In the heart, APJ receptor isexpressed in cardiomyocytes, vascular smooth muscle cells andendothelium, while apelin is expressed in endocardial endo-thelial cells, suggesting that endothelial apelin may act as aparacrine mediator on APJ receptor to influence cardiaccontractility or vascular tone [3-5]. Recently, apelin wasdescribed as a new adipokine, produced and secreted byhuman and mouse isolated mature adipocytes and upregulatedby insulin and obesity [6].The physiologically active form is thought to be apelin-36,
although shorter C-terminal sequences also elicit biologicalactivity [2]. To date, evidence suggests that apelin-36 mayfunction as a precursor with limited biological activity untilundergoing further proteolysis and post-translational modifi-cation to yield other biologically active peptides, apelin-13and, predominantly, (Pyr1)apelin-13 [5]. These isoforms haverecently been shown to have similar potency in terms ofhuman vascular and cardiac actions [5].In isolated rat hearts, apelin acutely promotes a potent
positive inotropic effect that depends on the activation ofphospholipase C (PLC), PKC, and sarcolemmal Na+–H+
exchange (NHE) and Na+–Ca2+ exchange (NCX) [7]. Thiseffect is present both in normal [8-10] and in failing rathearts secondary to myocardial infarction [9,11] and pulmo-nary hypertension [10]. While in some in vivo animalstudies, a direct inotropic action is more difficult toevaluate, further in vitro experiments confirmed apelin’sdirect positive inotropism [10,11]. Apelin–APJ vasculareffects are controversial but some authors suggest theymay depend on endothelial integrity, that is vasodilationthrough endothelial-dependent nitric oxide and prostanoidsrelease [12-14], or vasoconstriction, by direct binding to APJin vascular smooth muscle cells, when the endothelium isdysfunctional [15].In humans, plasma apelin levels were found to be increased
in patients with early stages of heart failure and decreased inlate stages of the disease [16]. In monocrotaline-induce pul-monary hypertensive rats, plasma apelin was significantlyaugmented, while its cardiac levels were downregulated [17].Despite the large number of reports focusing on the
relationship between apelinergic system andmetabolic disordersinduced by diabetes mellitus or insulin-resistance [6,18-19],none has explored the myocardial changes of this system.Furthermore, alterations in apelin and APJ receptor duringhypertrophy-induced remodeling are poorly understood. Theaim of the present study was to examine the changes in APJ andapelin myocardial expression, as well as plasma apelin in thepresence of pressure overload and diabetes. For this purpose,well-described rodent models of both pathologies were studiedin parallel with human biopsies and plasma samples fromdiabetic and non-diabetic aortic stenosis patients.
2. Patients and Methods
2.1 PatientsThe study population consisted of a pool of 24 patients withsymptomatic isolated aortic stenosis (AS), referred to surgicalvalve replacement and operated on between January andDecember 2008. Exclusion criteria were atrial fibrillation atbaseline, other significant valvular lesions (insufficiency >II/IV or mitral stenosis > than mild), or significant coronaryartery disease (> 50% stenosis in angiography). Diabetesmellitus was diagnosed if the patients were receiving insulinor oral hypoglycemic drugs to control hyperglycemia or ifthe fasting venous plasma glucose levels was ‡ 7.0 mmol/l(AS+DM, n = 13 versus AS, n = 11) [20].
The control group consisted of six patients with isolatedsevere mitral stenosis (MS; mean tansvalvular gradient11 ± 2 mmHg; valvular area index 0.97 ± 0.15 cm2/m2)referred for valve replacement over the same time period.
During surgical valve replacement, endomyocardial sampleswere procured by peroperative biopsy technique. This studywas approved by the local ethics committee. Written,informed consent was obtained from all patients and therewere no complications related to biopsy harvest.
2.1.1 Clinical and echocardiographic dataLV diastolic internal diameter (LVIDd), diastolic septal andposterior wall thicknesses (SWTd, PWTd), relative wall thick-ness (RWT), LVmass (LVM) and LVmass index (LVMI) werederived from 2D-echocardiograms. LV mass and RWT werecalculated in accordance to the recent recommendations forcardiac chamber quantification [21]:
LVM = 0.8 � {1.04 [(LVIDd + PWTd + SWTd)3–LVIDd3]} + 0.6 g
LV end-diastolic volume (LVEDV), aortic valve hemody-namics and severity of the stenosis were assessed by Dopplerechocardiographic examination [22]. The LV outflow tract areawas calculated from the diameter of the outflow tract(area = diameter2 � 0.785), assuming a circular geometry.The velocity of the LV outflow tract was obtained by pulsed-waveDoppler echocardiography from the apical long-axis view,and the maximal instantaneous (aortic valve) gradient wascalculated fromthepeakaorticDoppler velocityby themodifiedBernoulli equation (pressure gradient = 4 � velocity2). Meanaortic pressure gradient and time velocity integral of the aorticandLVoutflow tract flowvelocitieswere calculatedwith on-linesoftware. Three to five cardiac cycles were measured, and thevalues were averaged. Aortic valve area was calculated with thecontinuity equation: AVA= (LVOTarea�LVOTTVI)/aorticTVI, where AVA = aortic valve area, LVOT = LV outflow tract,and TVI = time-velocity integral [23].
2.1.2 Plasma analysisBoth human and rat blood samples were collected in EDTA-containing tubes, span at 5000 r.p.m. for 15 min at 4 �C andplasma separated and frozen at -80 �C until analysis.
Correlation between plasma levels of apelin and myocardial hypertrophy in rats and humans: possible target for treatment?
232 Expert Opin. Ther. Targets (2010) 14(3)

Endogenous plasma apelin was quantified using an Apelin-36enzyme immunoassay kit (Phoenix Pharmaceuticals) accord-ingly to the manufacturer’s instructions. This kit detectsapelin-36 as well as smaller biologically active isoforms(i.e., Apelin-36, 13 and 12). Each sample was analysed induplicate. Absorbance was recorded at 450 nm using anELISA plate reader (Perkin-Elmers) and a standard logarithmiccurve was plotted and used to calculate apelin concentration inthe plasma samples.
2.1.3 mRNA quantificationFor gene expression analyses, RNA was extracted with TriPure(Roche). RT-PCR was performed with total RNA, followedby real time PCR analyses using the SYBR Green method, in aLightCycler 2.0 (Roche).
For the animal studies, results are relative to the meanobtained for the sham group (set as an arbitrary unit) andnormalized for GAPDH. Specific PCR primer pairs for thestudied genes were: rGAPDH – fw 5¢- TGC CAC TCA GAAGAC TGT GG -3¢ and rev 5¢- GGA TGC AGG GAT GATGTT CT -3¢; rAPJ – fw 5¢- ACC ACA AAG GTC AAG TCAGCC A -3¢ and rev 5¢- CCA GTC TGA ATG TGA CTACGC A -3¢; rApelin – fw 5¢ – TGC TCT GGC TCT CCTTGA CT -3¢ and rev 5¢- CTC GAA GTT CTG GGC TTCAC -3¢; type-B natriuretic peptide r(BNP) – fw 5¢- CAG AGCTGG GGA AAG AAG AG -3¢ and rev 5¢- GGA CCA AGGCCC TAC AAA AGA -3¢ andTNF-a – fw 5¢- GCT TGGTGG TTT GCT ACG ACG TGG -3¢ and rev 5¢- ACT TCGGGG TGA TCG GTC CCA A -3¢.
For the human studies, results are relative to the meanobtained for the MS group (set as an arbitrary unit) andnormalized for GAPDH. Specific PCR primer pairs for thestudied genes were: hGAPDH – fw 5¢- GGT GGT CTCCTC TGA CTT CAA CA -3¢ and rev 5¢- GTT GCT GTAGCC AAA TTC GTT GT -3¢; hAPJ – fw 5¢- GGC TGGGAG CAG AGA GAA G -3¢ and rev 5¢- GGC AGA ATCAGG GGA CAG T -3¢; hApelin- fw 5¢- CTG CTC TGGCTC TCC TTG AC -3¢ and rev 5¢- CCC ATT CCT TGACCC TCT G -3¢.
2.2 Animal modelsAll animal experiments were conducted in conformity with theGuide for theCare andUse of LaboratoryAnimals published bythe US National Institutes of Health (NIH Publication N�
85-23, Revised in 1996). The Faculty of Medicine at theUniversity of Porto is a governmental institution grantedapproval by the Portuguese government to perform animalexperiments as described in this study. The experiments wereperformed on adult male Wistar rats weighting 170 – 190 g(Charles River Laboratories; Barcelona, Spain). Animals werehoused in groups of four rats per cage in a controlled environ-ment under a12h:12h light:dark cycle at a room temperature of22�C, with a free supply of food and water.
Left ventricular pressure-overload hypertrophy was inducedby supra-renal aortic banding. After 12 h of fasting, rats were
anesthetized with an intraperitoneal (ip) injection of ketamine(75 mg/kg) and xylazine (5 mg/kg). The suprarenal portion ofthe aorta was exposed and a blunted 21-gauge needle placedparallel to the aorta. A ligature (4-0 silk) was tightly tiedaround both the aorta and the needle. The needle was thenremoved, leaving a fixed internal opening of the aorta equal tothe diameter of the needle (0.8 mm) – (BA group). Sham-operated animals had a loosely tied ligature placed in the samelocation – (Sham group). Six weeks after surgery, rats fastedfor 5 h were randomized and given injections of streptozotocin(STZ, 65 mg/kg, ip) or equal volume of citrate buffer(pH = 4.5). The diabetic state was assessed by measurementof non-fasting serum glucose concentration one week afterSTZ injection. This procedure resulted in four experimentalgroups: Sham (n = 8), Banding (BA, n = 8), Diabetic (DM,n = 10) and Diabetic with banding (DM–BA, n = 10). Twelveweeks after the surgical procedure an echocardiographicevaluation was performed, animals were killed and plasmaand LV samples were collected.
2.2.1 Echocardiography assessmentEchocardiographic evaluation was performed before and12 weeks after the surgery using a 7.5 MHz transducer.Animals were anaesthetized with ketamine (75 mg/kg) andxylazine (5 mg/kg) and allowed to stabilize for 25 min. Fromthe left parasternal short-axis view, two-dimensional guidedM-mode tracings were made just below the mitral valve at thelevel of the papillary muscles for measurements of the inter-ventricular septum thickness (IVS, mm), LV internal diameter(LVD, mm), posterior wall thickness (LVPW, mm), LV mass(LVM, mg), fractional shortening (FS, %), ejection fraction(EF, %), heart rate (HR, beats per minute (b.p.m.) andDoppler assessment of E (m/s) and A (m/s) waves.
Fractional shortening was calculated from measurementsfor the LVD in systole and diastole: FS (%) = [(LVDd–LVDs)/LVDd] � 100. LV ejection fraction was determinedby M-mode echocardiography applying the formula [(LV-end-diastolic3-LV-end-systolic3)/LV-end-diastolic3] � 100(%). IVS, LVD, LVPW and LVM were normalized forbody surface area (BSA) [24].
2.2.2 Morphometric analysis and tissue preparationAfter echocardiographic evaluation was completed, blood wascollected directly from the LV cavity. Afterwards, the heartand lungs were excised and weighed. Heart, lung, RV and LV+septal (LV+S) weights were normalized to BSA. Sampleswere collected and immediately frozen for gene expressionanalysis.
Rat plasma analysis and mRNA quantification wasperformed as described in Sections 2.1.2 and 2.1.3.
2.3 Statistical analysisStatistical analysis was performed using Prim (version 5.0).Group data are presented as means ± SEM. For the animalstudy, groups were compared using two-way ANOVA. When
Falcao-Pires, Goncalves, Gavina, Pinho, Teixeira, Moura, Amorim, Pinho, Areias & Leite-Moreira
Expert Opin. Ther. Targets (2010) 14(3) 233

treatments were significantly different, the Student–Newman–Keuls test was selected to perform pairwise multiplecomparisons. For the human study, one-way ANOVA wasused to calculate the statistical significance between the threegroups. Correlations between two continuous variables wereassessed with linear regression analysis. Statistical significancewas set at p < 0.05.
3. Results
3.1 Patients3.1.1 Clinical and echocardiographic dataTable 1 compares clinical data of AS, AS+DM and MS groupsand Table 2 displays echocardiographic and combined hemo-dynamic–echocardiographic data of aortic stenosis patients.The American College of Cardiology and American HeartAssociation guidelines have defined severe aortic stenosis as anaortic valve area < 1.0 cm2, a mean gradient greater than40 mmHg, or jet velocity higher than 4.0 m/sec [25]. ASpatients fulfilled these criteria and both groups displayedsimilar degree of AS severity when referred to surgical aorticvalve replacement. All patients had preserved systolic LVfunction (EF > 50% and left ventricular end diastolic volumeindex (LVEDVI) far below 97ml/m2), but impaired diastolicfunction, presenting left ventricular end diastolic pressure(LVEDP) > 16 mmHg.
3.1.2 Apelin plasma and myocardial levelsAs shown in Figure 1A, despite a small trend towards anincrease, apelin plasma levels were not significantly different inAS when compared with the MS control group. Similarly, nosignificant changes were observed in AS+DM when comparedwith the other groups (Figure 1A). Interestingly, in AS and AS
+DM patients, apelin levels correlated positively with LVMI(r = 0.63, p = 0.04, Figure 1B), mean transvalvulargradient (r = 0.59, p = 0.02) and correlated negatively withAVAi (r = -0.56, p = 0.04).
With regard to apelin and APJ myocardial expression nodifferences were found between groups (Figure 2). Remark-ably, myocardial expression of apelin was positive and closelycorrelated with that of APJ (r = 0.75, p < 0.001).
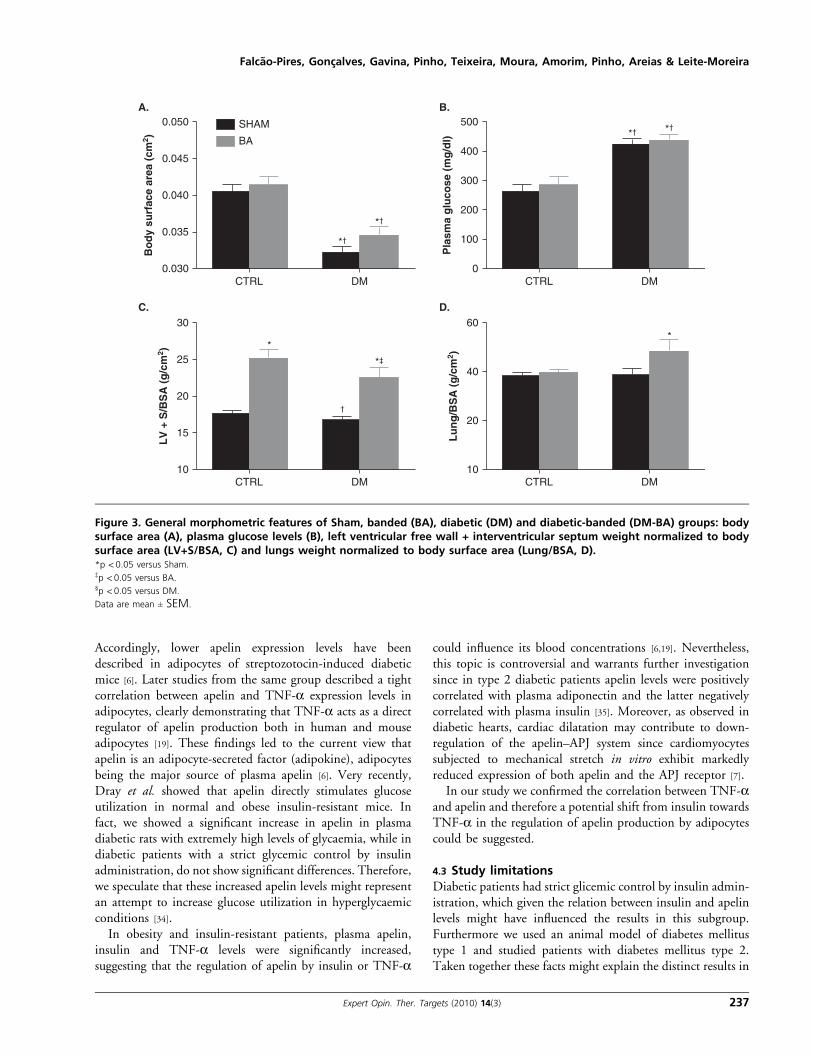
3.2 Animal models3.2.1 General featuresGeneral features of all groups are presented in Figure 3.Weight gain was reduced in diabetic animals compared withtheir non-diabetic counterparts, such that diabetic ratsdisplayed significantly lower body surface area (BSA) andbody weight (BW, SHAM: 401 ± 16 g; BA: 413 ± 18 g;DM: 277 ± 10 g, p < 0.001; DM-BA: 303 ± 15 g, p < 0.001)at the end of the protocol. Plasma glucose was significantlyand similarly elevated in the diabetic groups (Figure 3B).Other signs usually associated with diabetic state such aspolyuria, polydipsia and polyphagia were found in diabeticrats (data not shown).
LV chronic pressure-overload imposed by the aortic band-ing induced hypertrophy as observed from the increased LV+septum weight/BSA. The association of pressure-overloadand diabetes further increased lung weight/BSA suggestingpulmonary congestion and a more advanced stage of cardiacdysfunction in the DM-BA group (Figure 3D). Echocardiog-raphy evaluation confirmed the LV hypertrophy progression(Table 3): at the end of the protocol, both banded groups, BAand DM-BA, presented higher LVMI, IVSI and LVPWI thanthe Sham group. The diabetic condition promoted significantLV dilatation (diastolic LVDI increased) and heart ratedecrease. Ejection fraction and peak atrial contractionvelocity:peak early diastolic velocity ratio (E:A ratio) weresimilar among groups (Table 3).
3.2.2 Apelin plasma levelsChronic pressure overload did not significantly influenceapelin-like immunoreactive plasma levels, even if the BAgroup showed a trend to present higher levels than Sham.On the other hand, these levels were significantly higher inboth groups of diabetic animals (Figure 4A). Notably, apelinplasma levels correlated negatively with its myocardial expres-sion (r = -0.67, p = 0.004) and positively with myocardialexpression of TNF-a and LVMI (r = 0.55, p = 0.03 andr = 0.66, p = 0.03, respectively; Figure 4B).
3.2.3 Gene expression profileAs shown in Figure 5, LV expression of apelin and APJ wassignificantly decreased in both diabetic groups, either with orwithout banding, revealing a marked myocardial downregula-tion of this system in the presence of diabetes. Banded animalsalso displayed decreased apelin and APJ expression, althoughthe latter did not achieve statistical significance. As expected,
Table 1. Clinical characteristics of the AS patients.
Variables MS (n = 6) AS (n = 11) AS+DM (n = 13)
Age 59 ± 3.7 65.4 ± 2.6 69.3 ± 2,9
Female gender 5 8 9
Body massindex (g/cm2)
25.8 ± 3.2 28.4 ± 1.9 28.8 ± 0.9
Medication
Statins 0 7 6
b-blockers 2 7 6
Diuretics 2 8 8
ACE inhibitor 0 4 6
Angiotensin IIreceptor blockers
1 1 2
Insulin 0 0 13*‡
*Versus MS.‡Versus AS.
Values are mean ± SEM p <0.05.
AS: Aortic stenosis patients; AS+DM: Diabetic aortic stenosis patients;
MS: Mitral stenosis patients.
Correlation between plasma levels of apelin and myocardial hypertrophy in rats and humans: possible target for treatment?
234 Expert Opin. Ther. Targets (2010) 14(3)

both overloaded groups (BA and DM-BA) presented highermyocardial expression of BNP (Figure 5C). On the otherhand, diabetes seems to upregulate TNF-a expression(p = 0.07, Figure 5D). Remarkably, and as shown abovein humans, myocardial expression of apelin and APJ wereclosely correlated (r = 0.90, p < 0.001).
4. Discussion
In the present study, we aimed to evaluate plasma andmyocardial apelin concentration in hypertrophic conditionsin the presence or absence of diabetes mellitus, using ananimal model of chronic pressure-overload in parallel withaortic stenosis patients.
We showed an important correlation between apelinplasma levels and LVMI both in human and rat samples.Regarding myocardial expression levels, while in humansapelin and APJ expression was not significantly altered, inrats apelin was downregulated in the presence of chronicpressure-overload-induced hypertrophy and both apelin andAPJ expression was further decreased in untreated type-Idiabetic animals. Notably, we found a strong inverse
correlation between apelin rat plasma levels and its myocardialexpression. Based upon our findings, it appears that there is aprogressive decrease in myocardial apelinergic system expres-sion during cardiac hypertrophy. Moreover, apelin plasmalevels seem to increase together with LV mass in order tocounterbalance apelin/APJ downregulation. Considering thepositive inotropic and vasodilator actions of apelin, thiscompensatory mechanism may represent an attempt to main-tain inotropism and cardiac output during overload- ordiabetic-cardiomyopathy-induced remodeling processes.
4.1 Effect of chronic pressure overload on theapelinergic systemWe demonstrated that apelin myocardial expression wasdecreased in hypertrophied rat hearts, suggesting a progressivedownregulation that follows heart failure development. Ourstudy strengthens and extends previous reports showing that inpatients submitted to mechanical offloading conditions, myo-cardial expression of apelin and APJ were found to beincreased [16]. Additionally, in rodents, a 33% reduction inapelin expression in the LV of double-transgenic rats(harbouring both the human angiotensinogen and human
1.0 180
160
140
120
100
800.0 0.5 1.0 1.5
0.8
0.6
0.4
Pla
sma
apel
in (
ng
/ml)
Plasma apelin (ng/ml)
A. B.
LV
MI (
g/m
2 )
0.2
0.0MS AS AS + DM
Figure 1. A. Apelin plasma levels in patients with mitral stenosis (MS), aortic stenosis (AS) and aortic stenosis plus diabetes mellitus(AS+DM); B. correlation between apelin plasma levels and left ventricle mass index (LVMI, r = 0.63, p = 0.04).Data are mean ± SEM.
Table 2. Echocardiographic and hemodynamic data of aortic stenosis patients.
Variables MS (n = 6) AS (n = 11) AS+DM (n = 13)
Mean transvalvular gradient (mmHg) 11.0 ± 2.0 58.2 ± 3.8 56.2 ± 1.8
Valvular area index (cm2/m2) 0.97 ± 0.15 0.42 ± 0.04 0.53 ± 0.03
LV mass index (g/m2) 130 ± 6 125 ± 12
Ejection fraction (%) 62.5 ± 2.5 65.4 ± 1.2 61.0 ± 2.0
LV peak systolic pressure (mmHg) 216 ± 10 217 ± 7
LV end-diastolic pressure (mmHg) 19.7 ± 3.2 26.7 ± 3.7
LV end-diastolic volume index (ml/m2) 52.1 ± 3.1 53.9 ± 3.7 66.3 ± 4.2
Values are means ± SEM.AS: Aortic stenosis patients; AS+DM: Diabetic aortic stenosis patients; LV: Left ventricle; MS: Mitral stenosis patients.
Falcao-Pires, Goncalves, Gavina, Pinho, Teixeira, Moura, Amorim, Pinho, Areias & Leite-Moreira
Expert Opin. Ther. Targets (2010) 14(3) 235

renin genes) and by 62% in spontaneously hypertensive rats(SHR), both displaying increased LV/body weight indexversus age-matched controls [7]. Also Iwanaga and colleagues,found no changes in apelin and APJ expression duringcompensatory LV hypertrophy stage, while these weremarkedly down-regulated at the heart failure stage (72 and57%, respectively). However, these authors used Dahl-saltsensitive rats, which exhibit other metabolic disturbances andanalyzed them at a time point where hypertrophy was ~ 36%,while we analyzed apelin expression at a more advanced stageof hypertrophy (45% increase of LV/BSA). Furthermore, inangiotensin II-infused rats, cardiac apelin expression wasdecreased after 24 h of treatment and its restoration wasachieved by treatment with angiotensin II receptor blockers(ARB) [26]. These results indicate that the cardiac apelinergicsystem is markedly downregulated in experimental heartfailure and may be regulated by renin–angiotensin system(RAS) [26], which is also known to be significantly activated inhypertrophy [27]. Beneficial effects of RAS inhibition may, atleast in part, be due to the restoration of the cardiac apelinsystem in the treatment of HF. Accordingly, if we considerthat almost 50% of the patients included in this study weremedicated with ARB or ACE-inhibitors, this might to someextent explain why changes in myocardial apelinergic systemwere not so pronounced in humans as they were in rats.In rats, we found an inverse correlation between plasma levels
of apelin and its myocardial expression. Therefore, it seemsreasonable to assume that the systemic plasma increase of apelinmaycompensate for theobservedmyocardial downregulationofthis system. In line with these findings, previous studies havedescribed the importance of the apelin–APJ system in cardiacoverload, reporting that chronic treatmentwith apelin increasedmaximum andminimum rate of rise of left ventricular pressure(dP/dtmax and dP/dtmin) and decreased LVEDP in a HF ratmodel induced by isoproterenol [7,28-29], while in healthy rats, itinduced a significant increase cardiac output without signs of
cellularhypertrophy [8].Moreover,apelin-knockoutmiceexhib-ited normal cardiac development in adulthood, which deteri-orated when chronic pressure overload was imposed or withageing [29]. Interestingly, administration of apelin-13 continu-ously for 2 weeks in elderly mice reversed the decreased con-tractility [29]. Previous studies have reported contradictoryfindings regarding the circulating levels of apelin in patientswith HF (elevated [16], decreased [30-32] or unchanged [33]),suggesting its potential dependence on the underlying cardiacpathology. Currently, it is accepted that plasma levels of apelinare increased in the early stages of heart failure or compensatedhypertrophy,but substantiallydecreased in later stages [13,16,30], afact that has been suggested to indicate a transient compensatoryresponse. These findings together with our results furtherreinforce the idea that there is a strong relationship betweenthe activation of the apelinergic system and cardiac remodeling.Wethussuggest that thecorrelationbetweenapelinplasmalevelsand LVMI helps to maintain inotropism and cardiac outputupon apelinergic systemdownregulation that followsLVhyper-trophy. Therefore, apelin may act as a ‘good peptide’ in heartfailureserving toamelioraterather thanantagonizetheabnormalhemodynamic state of heart failure progression.
4.2 Effect of diabetes mellitus on the apelinergicsystemRegarding diabetes mellitus, although no differences in apelinand APJ myocardial expression were found between AS andAS+DM patients, in rats a significant decrease in diabeticgroups was observed. A direct regulation of apelin expressionby insulin in both human and mouse adipocytes was previ-ously demonstrated [6]. Such seems to be the case in themyocardium as well. In fact, we observed myocardial apelindownregulation in both diabetic groups and it is widelyknown that the streptozotocin-induced diabetic model ischaracterized by a massive destruction of pancreatic b-cellsand, consequently, decreased circulating insulin levels.
MS AS AS + DM MS AS AS + DM
1.5A. B.
1.0
0.5
0.0
1.5
1.0
0.5
0.0
Ap
elin
/ GA
PD
H m
RN
A (
AU
)
Ap
J/G
AP
DH m
RN
A (
AU
)
Figure 2. Expression of apelin (A) and APJ (B) in left ventricle myocardial biopsies collected during valve replacement surgeryof patients with mitral stenosis (MS), aortic stenosis (AS) and aortic stenosis plus diabetes mellitus (AS+DM). Results arenormalized for GAPDH and expressed in arbitrary units (AU).Data are mean ± SEM.
Correlation between plasma levels of apelin and myocardial hypertrophy in rats and humans: possible target for treatment?
236 Expert Opin. Ther. Targets (2010) 14(3)
Accordingly, lower apelin expression levels have beendescribed in adipocytes of streptozotocin-induced diabeticmice [6]. Later studies from the same group described a tightcorrelation between apelin and TNF-a expression levels inadipocytes, clearly demonstrating that TNF-a acts as a directregulator of apelin production both in human and mouseadipocytes [19]. These findings led to the current view thatapelin is an adipocyte-secreted factor (adipokine), adipocytesbeing the major source of plasma apelin [6]. Very recently,Dray et al. showed that apelin directly stimulates glucoseutilization in normal and obese insulin-resistant mice. Infact, we showed a significant increase in apelin in plasmadiabetic rats with extremely high levels of glycaemia, while indiabetic patients with a strict glycemic control by insulinadministration, do not show significant differences. Therefore,we speculate that these increased apelin levels might representan attempt to increase glucose utilization in hyperglycaemicconditions [34].
In obesity and insulin-resistant patients, plasma apelin,insulin and TNF-a levels were significantly increased,suggesting that the regulation of apelin by insulin or TNF-a
could influence its blood concentrations [6,19]. Nevertheless,this topic is controversial and warrants further investigationsince in type 2 diabetic patients apelin levels were positivelycorrelated with plasma adiponectin and the latter negativelycorrelated with plasma insulin [35]. Moreover, as observed indiabetic hearts, cardiac dilatation may contribute to down-regulation of the apelin–APJ system since cardiomyocytessubjected to mechanical stretch in vitro exhibit markedlyreduced expression of both apelin and the APJ receptor [7].
In our study we confirmed the correlation between TNF-aand apelin and therefore a potential shift from insulin towardsTNF-a in the regulation of apelin production by adipocytescould be suggested.
4.3 Study limitationsDiabetic patients had strict glicemic control by insulin admin-istration, which given the relation between insulin and apelinlevels might have influenced the results in this subgroup.Furthermore we used an animal model of diabetes mellitustype 1 and studied patients with diabetes mellitus type 2.Taken together these facts might explain the distinct results in
0.050A. B.
C. D.
SHAM
*†
*†
*†
†
*
*‡
*
*†
BA
500
400
300
200
100
0
0.045
0.040
0.035
Bo
dy
surf
ace
area
(cm
2 )L
V +
S/B
SA
(g
/cm
2 )
Lu
ng
/BS
A (
g/c
m2 )
Pla
sma
glu
cose
(m
g/d
l)
0.030
30
25
20
15
10
60
40
20
10
CTRL CTRL DMDM
CTRL DM CTRL DM
Figure 3. General morphometric features of Sham, banded (BA), diabetic (DM) and diabetic-banded (DM-BA) groups: bodysurface area (A), plasma glucose levels (B), left ventricular free wall + interventricular septum weight normalized to bodysurface area (LV+S/BSA, C) and lungs weight normalized to body surface area (Lung/BSA, D).*p <0.05 versus Sham.‡p <0.05 versus BA.§p <0.05 versus DM.
Data are mean ± SEM.
Falcao-Pires, Goncalves, Gavina, Pinho, Teixeira, Moura, Amorim, Pinho, Areias & Leite-Moreira
Expert Opin. Ther. Targets (2010) 14(3) 237

rats and humans regarding the effects of diabetes on theapelinergic system. The use of mitral stenosis patients as acontrol for our study, which frequently display atrial fribilla-tion, represents a limitation that we were not able to overcomegiven the obvious ethical constrains of procuring myocardialbiopsies from healthy individuals.Finally, subsequent experiments, with chronic administra-
tion of apelin to these groups, would certainly clarify thetherapeutic potential role of apelin in the progression ofLV hypertrophy.
5. Conclusion
The important correlation between plasma apelin and LVMIobserved both in humans and rats, suggests that this peptidemight be used as a biomarker of LV hypertrophy. As previ-ously described, the positive inotropy after exogenous admin-istration of apelin suggests that its endogenous levels are notsufficient to saturate the APJ and maximize the signaltransduction for enhancing contractility in heart failureconditions. Apelin may provide a novel adjunctive inotropic
Table 3. Doppler echocardiographic parameter of sham-operated, banded (BA), diabetic (DM) and diabetic-banded
(DM-BA) animals at the end of the protocol.
Parameter Sham (n = 8) BA (n = 8) DM (n = 8) DM-BA (n = 8)
IVSId (mm/cm2) 35.2 ± 1.9 46.1 ± 1.6* 52.5 ± 2.2* 51.6 ± 1.9*
IVSIs (mm/cm2) 63.6 ± 2.5 68.2 ± 2.0* 82.4 ± 5.8* 88.5 ± 3.4*‡
LVDId (mm/cm2) 175 ± 6 184 ± 6 216 ± 7*‡ 216 ± 7*‡
LVDIs (mm/cm2) 94.8 ± 5.8 98.9 ± 6.5 109 ± 6 109 ± 6
LVPWId (mm/cm2) 34.5 ± 1.7 45.0 ± 1.3* 48.5 ± 3.0* 48.4 ± 1.9*
LVPWIs (mm/cm2) 55.6 ± 2.2 68.2 ± 2.0* 70.6 ± 3.9* 75.9 ± 4.0*
EF (%) 82.2 ± 1.8 81.7 ± 2.0 85.0 ± 1.7 85.2 ± 1.8
FS (%) 46.3 ± 1.8 46.9 ± 2.5 49.1 ± 2.5 50.0 ± 2.1
LVMI (g/cm2) 19.5 ± 1.8 26.4 ± 1.3* 21.9 ± 1.7 25.3 ± 2.2*
HR (b.p.m.) 277 ± 6 287 ± 10 232 ± 7*‡ 242 ± 10*‡
E/A 1.75 ± 0.15 1.66 ± 0.11 1.68 ± 0.11 1.49 ± 0.07
*Versus sham.‡Versus BA.
Values are means ± SEM p <0.05.
A: Mitral flow peak atrial contraction velocity (m/s); E: Mitral flow peak early diastolic velocity (m/s); EF: Ejection fraction (%); FS: Fractional shortening (%); HR: Heart
rate (beats per minute); IVSId: Interventricular septum thickness index in diastole (mm); IVSIs: Interventricular septum thickness index in systole (mm); LVDId: LV
internal diameter index in diastole (mm); LVDIs: LV internal diameter index in systole (mm); LVMI: Left ventricular mass index; LVPWId: Posterior wall thickness index in
diastole (mm); LVPWIs: Posterior wall thickness index in systole (mm).
0.6
A. B.
SHAM
**BA
40
30
20
10
00.0DMCTRL
Pla
sma
apel
in (
ng
/ml)
LVM
I (g
/cm
2 )
0.2 0.4
Plasma apelin (ng/ml)0.6 0.8
0.5
0.4
0.3
0.2
Figure 4. A. Apelin plasma levels of Sham, banded (BA), diabetic (DM and diabetic-banded (DM-BA) animals; B. correlation between apelinplasma levels and left ventricle mass index (LVMI, r = 0.55, p = 0.03).*p < 0.05 versus Sham.
Data are mean ± SEM.
Correlation between plasma levels of apelin and myocardial hypertrophy in rats and humans: possible target for treatment?
238 Expert Opin. Ther. Targets (2010) 14(3)

therapy for heart failure in addition to b1-agonists andphosphodiesterase inhibitors. The ability of apelin to enhancevasodilatation and decrease systemic vascular resistance offersthe potential to decrease afterload, cardiac work and myocar-dial oxygen demands as well as enhance contractility andcardiac output with a single agent.
Although the discussion on the risk/benefit of apelin/APJ incardiovascular diseases is still open, APJ clearly appears to be afuture drug target for the treatment of hear failure,hypertension and even diabetic cardiomyopathy.
Acknowledgments
We thank Soares-Fortunato for critical reading of themanuscript andMOliveira for the excellent technical assistance.
Declaration of interest
This work was supported by the Portuguese Foundation forScience and Technology (grant number PIC/IC/82943/2007)through the Cardiovascular R&D Unit (nr. 51/94).
1.5 SHAM
*
*
*‡
**
* *
BA
1.0
0.5
0.0
5
4
3
2
1
0
CTRL
A. B.
C. D.
Ap
elin
/ GA
PD
H m
RN
A (
AU
)
AP
J/G
AP
DH m
RN
A (
AU
)
BN
P/ G
AP
DH m
RN
A (
AU
)
TN
F-a
/ GA
PD
H m
RN
A (
AU
)
DM CTRL DM
CTRL DM CTRL DM
1.5
1.0
0.5
0.0
2.5
2.0
1.5
1.0
0.5
0.0
Figure 5. Expression of apelin (A), APJ (B), type-B natriuretic peptide (BNP, C) and TNF-a, (D) in left ventricle myocardialsamples collected 12 weeks after surgical banding. Results are normalized for GAPDH and expressed in arbitrary units (AU).*p < 0.05 versus Sham.‡p <0.05 vsersus DM.
Data are mean ± SEM.
Falcao-Pires, Goncalves, Gavina, Pinho, Teixeira, Moura, Amorim, Pinho, Areias & Leite-Moreira
Expert Opin. Ther. Targets (2010) 14(3) 239

Bibliography1. Morgan HE, Baker KM. Cardiac
hypertrophy. Mechanical, neural, and
endocrine dependence. Circulation
1991;83(1):13-25
2. Tatemoto K, Hosoya M, Habata Y, et al.
Isolation and characterization of a novel
endogenous peptide ligand for the human
APJ receptor. Biochem Biophys
Res Commun 1998;251(2):471-6
3. Lee DK, Cheng R, Nguyen T, et al.
Characterization of apelin, the ligand for
the APJ receptor. J Neurochem
2000;74(1):34-41
4. Kawamata Y, Habata Y, Fukusumi S, et al.
Molecular properties of apelin: tissue
distribution and receptor binding.
Biochim Biophys Acta
2001;1538(2-3):162-71
5. Maguire JJ, Kleinz MJ, Pitkin SL,
Davenport AP. [Pyr1]apelin-13 identified
as the predominant apelin isoform in the
human heart: vasoactive mechanisms and
inotropic action in disease. Hypertension
2009;54(3):598-604
6. Boucher J, Masri B, Daviaud D, et al.
Apelin, a newly identified adipokine
up-regulated by insulin and obesity.
Endocrinology 2005;146(4):1764-71
7. Szokodi I, Tavi P, Foldes G, et al. Apelin,
the novel endogenous ligand of the orphan
receptor APJ, regulates cardiac
contractility. Circ Res 2002;91(5):434-40
8. Ashley EA, Powers J, Chen M, et al. The
endogenous peptide apelin potently
improves cardiac contractility and reduces
cardiac loading in vivo. Cardiovasc Res
2005;65(1):73-82
9. Berry MF, Pirolli TJ, Jayasankar V, et al.
Apelin has in vivo inotropic effects on
normal and failing hearts. Circulation
2004;110(11 Suppl 1):II187-93
10. Dai T, Ramirez-Correa G, Gao WD.
Apelin increases contractility in failing
cardiac muscle. Eur J Pharmacol
2006;553(1-3):222-8
11. Farkasfalvi K, Stagg MA, Coppen SR, et al.
Direct effects of apelin on cardiomyocyte
contractility and electrophysiology.
Biochem Biophys Res Commun
2007;357(4):889-95
12. Tatemoto K, Takayama K, Zou MX, et al.
The novel peptide apelin lowers blood
pressure via a nitric oxide-dependent
mechanism. Regul Pept
2001;99(2-3):87-92
13. Cheng X, Cheng XS, Pang CC. Venous
dilator effect of apelin, an endogenous
peptide ligand for the orphan APJ receptor,
in conscious rats. Eur J Pharmacol
2003;470(3):171-5
14. Salcedo A, Garijo J, Monge L, et al. Apelin
effects in human splanchnic arteries. Role
of nitric oxide and prostanoids. Regul Pept
2007;144(1-3):50-5
15. Katugampola SD, Maguire JJ,
Matthewson SR, Davenport AP.
[125I]-(Pyr1)Apelin-13 is a novel
radioligand for localizing the APJ orphan
receptor in human and rat tissues with
evidence for a vasoconstrictor role in man.
Br J Pharmacol 2001;132(6):1255-60
16. Chen MM, Ashley EA, Deng DX, et al.
Novel role for the potent endogenous
inotrope apelin in human cardiac
dysfunction. Circulation
2003;108(12):1432-9
17. Falcao-Pires I, Goncalves N,
Henriques-Coelho T, et al. Apelin
decreases myocardial injury and improves
right ventricular function in
monocrotaline-induced pulmonary
hypertension. Am J Physiol Heart
Circ Physiol 2009;296(6):H2007-14
18. Castan-Laurell I, Boucher J, Dray C, et al.
Apelin, a novel adipokine over-produced
in obesity: friend or foe?
Mol Cell Endocrinol 2005;245(1-2):7-9
19. Daviaud D, Boucher J, Gesta S, et al.
TNFalpha up-regulates apelin expression
in human and mouse adipose tissue.
FASEB J 2006;20(9):1528-30
20. Rodbard HW, Blonde L, Braithwaite SS,
et al. American Association of Clinical
Endocrinologists medical guidelines for
clinical practice for the management of
diabetes mellitus. Endocr Pract
2007;13: (Suppl 1):1-68
21. Lang RM, Bierig M, Devereux RB, et al.
Recommendations for chamber
quantification. Eur J Echocardiogr
2006;7(2):79-108
22. Oh JK, Taliercio CP, Holmes DR Jr, et al.
Prediction of the severity of aortic stenosis
by Doppler aortic valve area
determination: prospective
Doppler-catheterization correlation in
100 patients. J Am Coll Cardiol
1988;11(6):1227-34
23. Zoghbi WA, Farmer KL, Soto JG, et al.
Accurate noninvasive quantification of
stenotic aortic valve area by Doppler
echocardiography. Circulation
1986;73(3):452-9
24. Wolffenbuttel BH, Boulanger CM,
Crijns FR, et al. Breakers of advanced
glycation end products restore large artery
properties in experimental diabetes.
Proc Natl Acad Sci USA
1998;95(8):4630-4
25. Nishimura RA, Carabello BA, Faxon DP,
et al. ACC/AHA 2008 Guideline update
on valvular heart disease: focused update
on infective endocarditis: a report of the
American College of Cardiology/American
Heart Association Task Force on Practice
Guidelines endorsed by the Society of
Cardiovascular Anesthesiologists, Society
for Cardiovascular Angiography and
Interventions, and Society of Thoracic
Surgeons. J Am Coll Cardiol
2008;52(8):676-85
26. Iwanaga Y, Kihara Y, Takenaka H, Kita T.
Down-regulation of cardiac apelin system
in hypertrophied and failing hearts:
possible role of angiotensin II-angiotensin
type 1 receptor system. J Mol Cell Cardiol
2006;41(5):798-806
27. Xiao HD, Fuchs S, Bernstein EA, et al.
Mice expressing ACE only in the heart
show that increased cardiac angiotensin II
is not associated with cardiac hypertrophy.
Am J Physiol 2008;294(2):H659-67
28. Jia YX, Pan CS, Zhang J, et al. Apelin
protects myocardial injury induced by
isoproterenol in rats. Regul Pept
2006;133(1-3):147-54
29. Kuba K, Zhang L, Imai Y, et al. Impaired
heart contractility in Apelin gene-deficient
mice associated with aging and pressure
overload. Circ Res 2007;101(4):e32-42
30. Foldes G, Horkay F, Szokodi I, et al.
Circulating and cardiac levels of apelin, the
novel ligand of the orphan receptor APJ, in
patients with heart failure.
Biochem Biophys Res Commun
2003;308(3):480-5
31. Goetze JP, Rehfeld JF, Carlsen J, et al.
Apelin: a new plasma marker of
cardiopulmonary disease. Regul Pept
2006;133(1-3):134-8
32. Chong KS, Gardner RS, Morton JJ, et al.
Plasma concentrations of the novel peptide
apelin are decreased in patients with
chronic heart failure. Eur J Heart Fail
2006;8(4):355-60
33. Miettinen KH, Magga J, Vuolteenaho O,
et al. Utility of plasma apelin and other
Correlation between plasma levels of apelin and myocardial hypertrophy in rats and humans: possible target for treatment?
240 Expert Opin. Ther. Targets (2010) 14(3)

indices of cardiac dysfunction in the
clinical assessment of patients with dilated
cardiomyopathy. Regul Pept
2007;140(3):178-84
34. Dray C, Knauf C, Daviaud D, et al. Apelin
stimulates glucose utilization in normal
and obese insulin-resistant mice.
Cell Metab 2008;8(5):437-45
35. Erdem G, Dogru T, Tasci I, et al. Low
plasma apelin levels in newly diagnosed
type 2 diabetes mellitus. Exp Clin
Endocrinol Diabetes 2008;116(5):289-92
AffiliationInes Falcao-Pires, Nadia Goncalves,
Cristina Gavina, Sonia Pinho,
Tania Teixeira, Claudia Moura,
Mario Jorge Amorim, Paulo Pinho,
Jose Carlos Areias & Adelino Leite-Moreira†
†Author for correspondence
Alameda Professor Hernani Monteiro,
University of Porto,
Department of Physiology,
Cardiovascular R&D Unit,
Faculty of Medicine,
4200-319 Porto, Portugal
Tel: +351 225 513 644; Fax: +351 225 513 646;
E-mail: [email protected]
Falcao-Pires, Goncalves, Gavina, Pinho, Teixeira, Moura, Amorim, Pinho, Areias & Leite-Moreira
Expert Opin. Ther. Targets (2010) 14(3) 241