computed tomographic validation of the porcine model for thoracic scoliosis
TRANSCRIPT

SPINE Volume 35, Number 1, pp 18–25©2009, Lippincott Williams & Wilkins
Computed Tomographic Validation of the PorcineModel for Thoracic Scoliosis
Ashish Patel, MD,* Frank Schwab, MD,* Virginie Lafage, PhD,* Archit Patel, MD,†Moutasem M. Obeidat, MD,‡ and Jean-Pierre Farcy, MD*
Study Design. Computed Tomographic Analysis of thePorcine Scoliosis Model.
Objective. To describe the spinal and rib cage modifi-cations using computed tomography (CT).
Summary of Background Data. Optimal developmentof nonfusion techniques for treatment of adolescent idio-pathic scoliosis (AIS) requires a reliable large animalmodel that achieves spinal and rib cage modificationssimilar to AIS. Previous work has described the global3-dimensional nature of the progressive deformity.
Methods. This IACUC-approved study includes 11 ex-tracted scoliotic spines from a previous investigation.Scoliosis was induced through unilateral posterior liga-ment tethering of the spine via pedicle screw fixation, andipsilateral rib cage tethering. CT analysis was used toquantify rib cage asymmetry, axial rotation, and wedgingof the apical functional unit (2 vertebrae and interveningdisc) for each specimen.
Results. The mean coronal Cobb angle was 55.7° (n �11). Vertebral and intervertebral heights of the apicalfunctional unit demonstrated convex heights (untethered)were always larger than concave (tethered) heights (P �0.05). Axial rotation was maximal (mean, 20°) at 1 to 2levels distal to the coronal apex. Maximal rib cage asym-metry was demonstrated at the transverse apex with sig-nificant coupling of the rotational and rib cage modifica-tions (r � 0.82). A large initial Cobb index (tether tension)was significantly correlated with vertebral and interverte-bral wedging and coronal curve progression.
Conclusion. The present study has used CT analysis toanalyze spinal and rib cage modifications in the PorcineScoliosis Model. Placement of a unilateral ligamentous spi-nal tether combined with concave rib cage ligament tether-ing during the rapid growth stage of the Yorkshire pig resultsin significant apical vertebral and intervertebral wedging androtational and rib cage modifications. The porcine model is areliable and duplicable model for scoliosis, which bears signif-icant similarities to AIS.
Key words: growth modulation, nonfusion, AIS. Spine
2010;35:18–25
Adolescent idiopathic scoliosis (AIS) is a complex 3-di-mensional deformity affecting 2% to 3% of the generalpopulation.1–3 Although the etiology currently remainsunclear, typical regional and global spinal modificationshave been described, which are unique to this disorderincluding one or more spinal curve(s) in the coronalplane, possible flattening of the sagittal curves, vertebralrotation in the transverse plane and thoracic cage dys-plasia resulting in a rib prominence, or “rib-hump.”Within the curve, at the segmental spinal level, there issignificant vertebral and intervertebral wedging; the ver-tebrae are trapezoidal in nature, predominately in thefrontal plane at the apex of the deformity.
Spinal fusion remains the mainstay for progressiveand severe scoliotic deformities, although there is recentinterest in nonfusion technologies.4–9 Theoretically, ap-plication of nonfusion devices would favorably redirectremaining skeletal growth to leave the spine in balancedalignment while sparing mobile elements (discs, facets)to conserve spinal motion. The authors believe that de-velopment and optimization of nonfusion devices re-quires a large animal model; with local, regional, andglobal modifications typical to those observed in AIS.
Investigations involving unilateral mechanical tether-ing systems in immature animals have demonstrated tobe extremely effective at creating spinal deformities.Most recently, Braun et al10,11 described creation of ascoliotic deformity in goats. Significant progressive de-formities were achieved, although the investigationlacked detailed assessment of the vertebral and interver-tebral modifications. Additionally, several inherentshortcomings exist in the goat model; flattened thoraciccage, seasonal breeding, malignant curves, and limitedgrowth potential that led our team to investigate furtheralternative animal models.
Schwab et al12 have recently reported work on a por-cine scoliosis model (PSM). With placement of a flexibletether fixated to the spine with pedicle screws and ipsilat-eral rib cage tethering; progressive, 3-dimensional deformi-ties have been obtained. Radiographic analysis demon-strated moderate to severe right-sided convex coronalcurves, sagittal flattening (lordosis), and vertebral axial ro-tation, with posterior elements displaced into the curveconcavity. Curves induced were predictable in there pro-gression generating consistent 3-dimensional radiographicfeatures pathognomonic of idiopathic scoliosis. With alarge round thorax (similar to young adolescents), compa-rable vertebral morphology,13 year round availability, easeof handling, and rapid growth potential, the porcine model
From the *Department of Orthopaedics, NYU Hospital for Joint Dis-eases, New York, NY; †Maimonides Medical Center, Brooklyn, NY;and ‡Department of Orthopedic Surgery, Jordan University of Scienceand Technology (JUST), Irbid, Jordan.Acknowledgment date: March 16, 2009. First revision date: April 15,2009. Second revision date: May 4, 2009. Acceptance date: May 7,2009.The manuscript submitted does not contain information about medicaldevice(s)/drug(s).Corporate/Industry funds were received in support of this work. Oneor more of the author(s) has/have received or will receive benefits forpersonal or professional use from a commercial party related directlyor indirectly to the subject of this manuscript: e.g., honoraria, gifts,consultancies.Supported by Medtronic Sofamor Danek.Address correspondence and reprint requests to Ashish Patel, MD,NYU Hospital for Joint Diseases, 380 2nd Ave., Suite 1001, NewYork, NY 10010; E-mail: [email protected]
18
represents a viable candidate for the study and reliablemodeling of spinal deformity.
The purpose of the current investigation was to de-scribe the local and global modifications of the PSM withthe use of computed tomography.
Materials and Methods
Scoliotic Spinal SpecimensA total of 11 animals meeting specific end point criteria from aprevious investigation12 were enrolled in this study. Spineswere extracted from scoliotic animals, which had reachedgreater than 50° coronal Cobb angulation as part of the PSMinvestigation. The technique of scoliosis induction was de-scribed in detail in a previous report.12 Briefly, Yorkshire pigswere obtained at 11 weeks of age; after 1 week acclimatizationperiod, the surgical induction of scoliosis via a left-sided spinaltether fixated with pedicle screws, and ipsilateral rib cage teth-ering was preformed. A mean 24.5° initial coronal curve wasestablished with a mean of 8 vertebrae between proximal anddistal fixation points. Animals were observed for a mean of 11weeks (range, 6–14 weeks), with biweekly posterior, anterior,and sagittal radiographs until severe deformity developed(�50°), following which euthanasia was preformed.
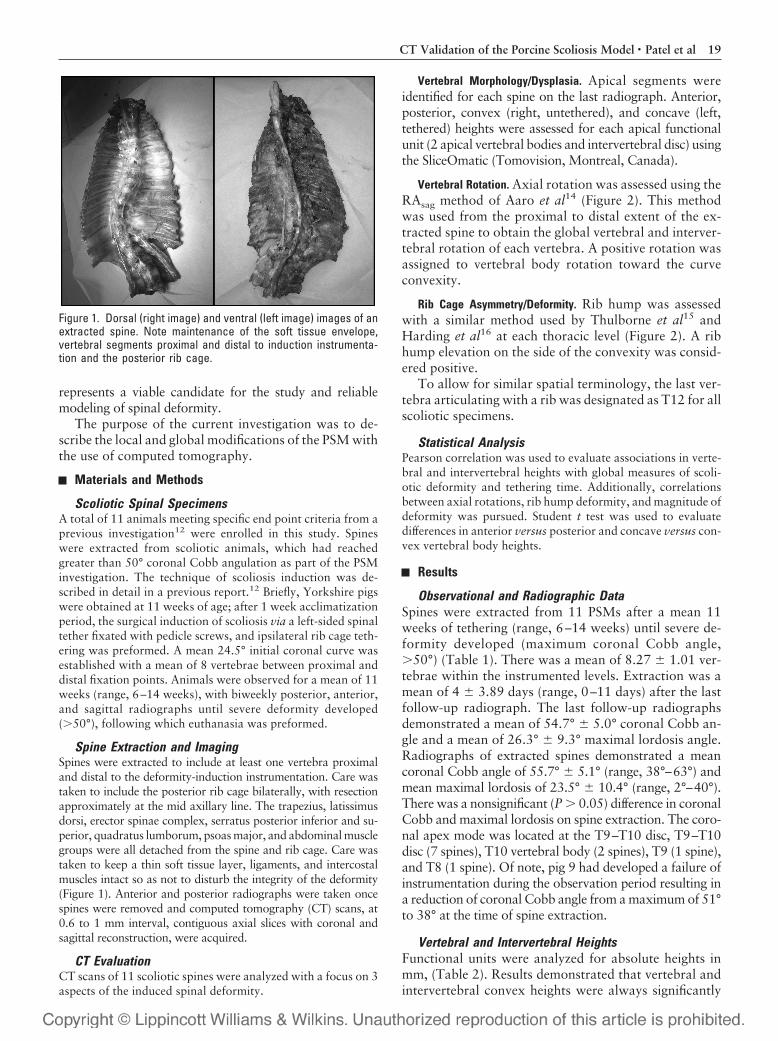
Spine Extraction and ImagingSpines were extracted to include at least one vertebra proximaland distal to the deformity-induction instrumentation. Care wastaken to include the posterior rib cage bilaterally, with resectionapproximately at the mid axillary line. The trapezius, latissimusdorsi, erector spinae complex, serratus posterior inferior and su-perior, quadratus lumborum, psoas major, and abdominal musclegroups were all detached from the spine and rib cage. Care wastaken to keep a thin soft tissue layer, ligaments, and intercostalmuscles intact so as not to disturb the integrity of the deformity(Figure 1). Anterior and posterior radiographs were taken oncespines were removed and computed tomography (CT) scans, at0.6 to 1 mm interval, contiguous axial slices with coronal andsagittal reconstruction, were acquired.
CT EvaluationCT scans of 11 scoliotic spines were analyzed with a focus on 3aspects of the induced spinal deformity.
Vertebral Morphology/Dysplasia. Apical segments wereidentified for each spine on the last radiograph. Anterior,posterior, convex (right, untethered), and concave (left,tethered) heights were assessed for each apical functionalunit (2 apical vertebral bodies and intervertebral disc) usingthe SliceOmatic (Tomovision, Montreal, Canada).
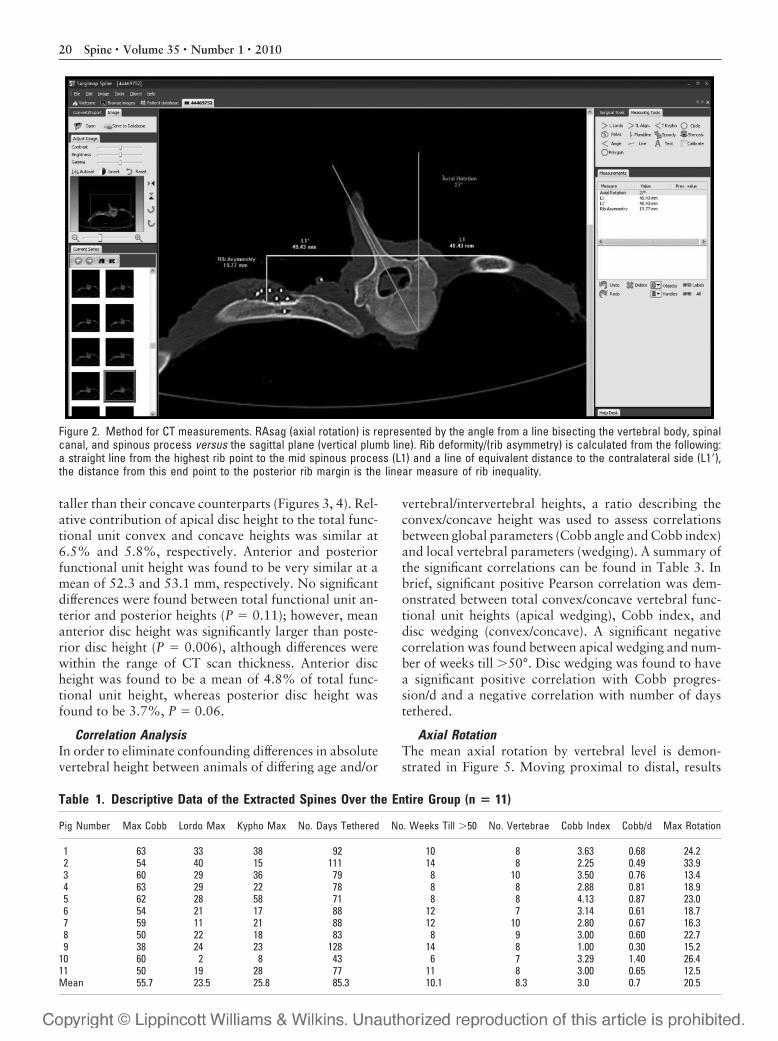
Vertebral Rotation. Axial rotation was assessed using theRAsag method of Aaro et al14 (Figure 2). This methodwas used from the proximal to distal extent of the ex-tracted spine to obtain the global vertebral and interver-tebral rotation of each vertebra. A positive rotation wasassigned to vertebral body rotation toward the curveconvexity.
Rib Cage Asymmetry/Deformity. Rib hump was assessedwith a similar method used by Thulborne et al15 andHarding et al16 at each thoracic level (Figure 2). A ribhump elevation on the side of the convexity was consid-ered positive.
To allow for similar spatial terminology, the last ver-tebra articulating with a rib was designated as T12 for allscoliotic specimens.
Statistical AnalysisPearson correlation was used to evaluate associations in verte-bral and intervertebral heights with global measures of scoli-otic deformity and tethering time. Additionally, correlationsbetween axial rotations, rib hump deformity, and magnitude ofdeformity was pursued. Student t test was used to evaluatedifferences in anterior versus posterior and concave versus con-vex vertebral body heights.
Results
Observational and Radiographic DataSpines were extracted from 11 PSMs after a mean 11weeks of tethering (range, 6–14 weeks) until severe de-formity developed (maximum coronal Cobb angle,�50°) (Table 1). There was a mean of 8.27 � 1.01 ver-tebrae within the instrumented levels. Extraction was amean of 4 � 3.89 days (range, 0–11 days) after the lastfollow-up radiograph. The last follow-up radiographsdemonstrated a mean of 54.7° � 5.0° coronal Cobb an-gle and a mean of 26.3° � 9.3° maximal lordosis angle.Radiographs of extracted spines demonstrated a meancoronal Cobb angle of 55.7° � 5.1° (range, 38°–63°) andmean maximal lordosis of 23.5° � 10.4° (range, 2°–40°).There was a nonsignificant (P � 0.05) difference in coronalCobb and maximal lordosis on spine extraction. The coro-nal apex mode was located at the T9–T10 disc, T9–T10disc (7 spines), T10 vertebral body (2 spines), T9 (1 spine),and T8 (1 spine). Of note, pig 9 had developed a failure ofinstrumentation during the observation period resulting ina reduction of coronal Cobb angle from a maximum of 51°to 38° at the time of spine extraction.
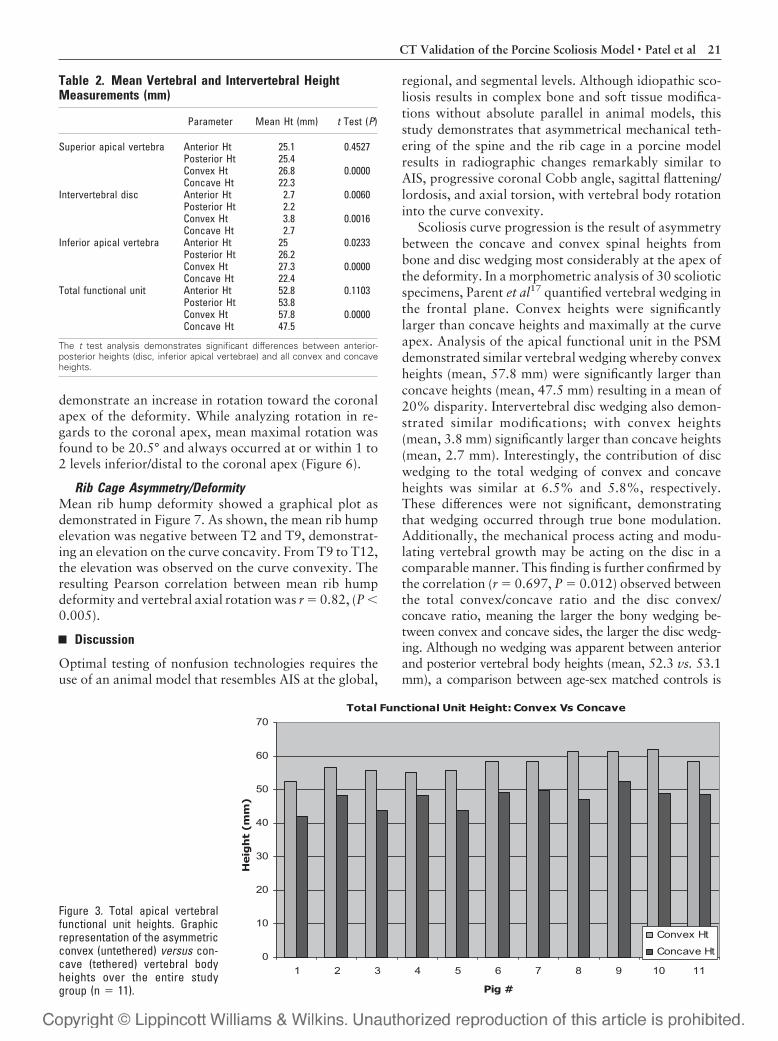
Vertebral and Intervertebral HeightsFunctional units were analyzed for absolute heights inmm, (Table 2). Results demonstrated that vertebral andintervertebral convex heights were always significantly
Figure 1. Dorsal (right image) and ventral (left image) images of anextracted spine. Note maintenance of the soft tissue envelope,vertebral segments proximal and distal to induction instrumenta-tion and the posterior rib cage.
19CT Validation of the Porcine Scoliosis Model • Patel et al
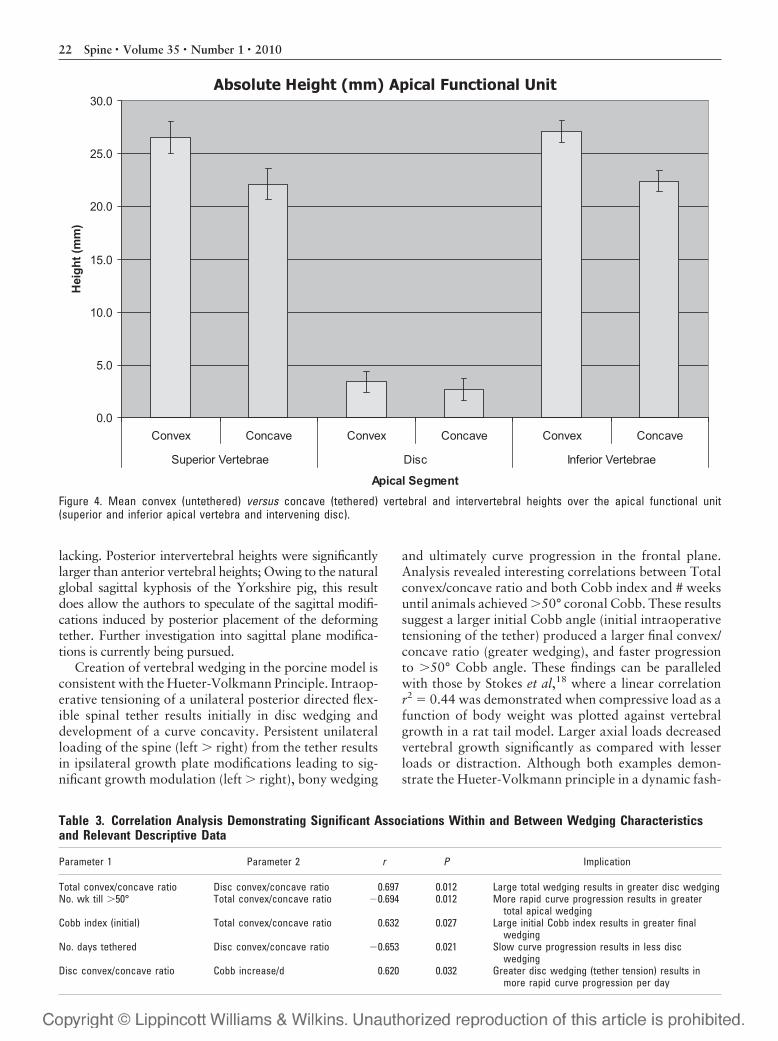
taller than their concave counterparts (Figures 3, 4). Rel-ative contribution of apical disc height to the total func-tional unit convex and concave heights was similar at6.5% and 5.8%, respectively. Anterior and posteriorfunctional unit height was found to be very similar at amean of 52.3 and 53.1 mm, respectively. No significantdifferences were found between total functional unit an-terior and posterior heights (P � 0.11); however, meananterior disc height was significantly larger than poste-rior disc height (P � 0.006), although differences werewithin the range of CT scan thickness. Anterior discheight was found to be a mean of 4.8% of total func-tional unit height, whereas posterior disc height wasfound to be 3.7%, P � 0.06.
Correlation AnalysisIn order to eliminate confounding differences in absolutevertebral height between animals of differing age and/or
vertebral/intervertebral heights, a ratio describing theconvex/concave height was used to assess correlationsbetween global parameters (Cobb angle and Cobb index)and local vertebral parameters (wedging). A summary ofthe significant correlations can be found in Table 3. Inbrief, significant positive Pearson correlation was dem-onstrated between total convex/concave vertebral func-tional unit heights (apical wedging), Cobb index, anddisc wedging (convex/concave). A significant negativecorrelation was found between apical wedging and num-ber of weeks till �50°. Disc wedging was found to havea significant positive correlation with Cobb progres-sion/d and a negative correlation with number of daystethered.
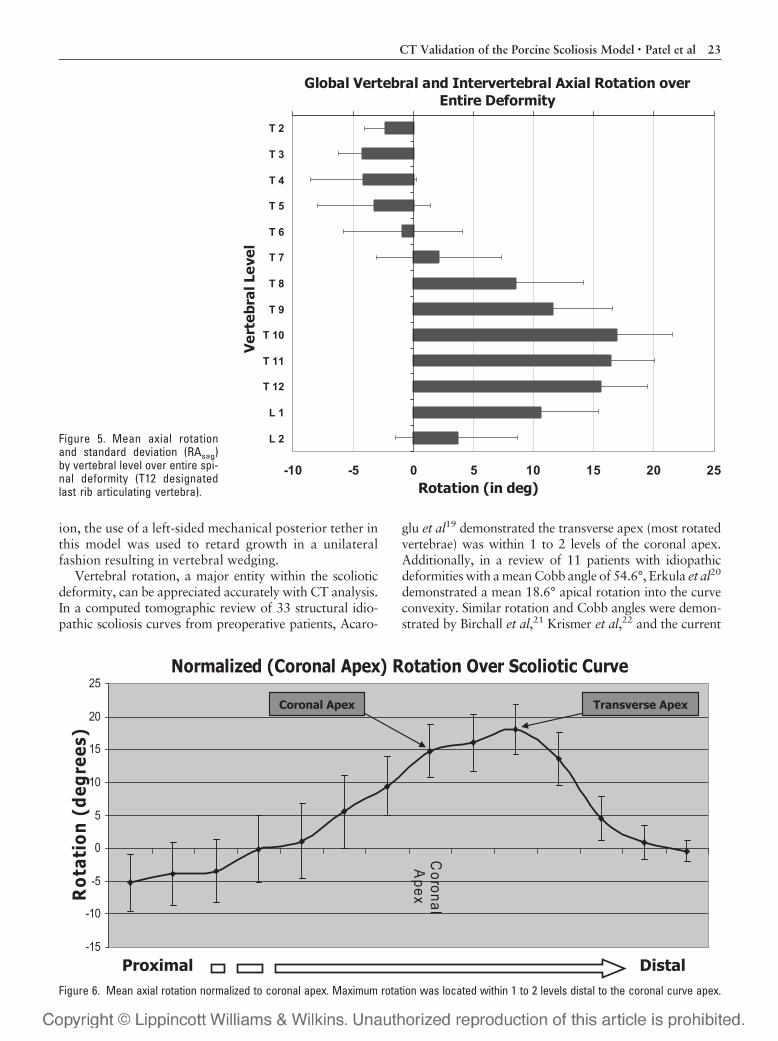
Axial RotationThe mean axial rotation by vertebral level is demon-strated in Figure 5. Moving proximal to distal, results
Figure 2. Method for CT measurements. RAsag (axial rotation) is represented by the angle from a line bisecting the vertebral body, spinalcanal, and spinous process versus the sagittal plane (vertical plumb line). Rib deformity/(rib asymmetry) is calculated from the following:a straight line from the highest rib point to the mid spinous process (L1) and a line of equivalent distance to the contralateral side (L1�),the distance from this end point to the posterior rib margin is the linear measure of rib inequality.
Table 1. Descriptive Data of the Extracted Spines Over the Entire Group (n � 11)
Pig Number Max Cobb Lordo Max Kypho Max No. Days Tethered No. Weeks Till �50 No. Vertebrae Cobb Index Cobb/d Max Rotation
1 63 33 38 92 10 8 3.63 0.68 24.22 54 40 15 111 14 8 2.25 0.49 33.93 60 29 36 79 8 10 3.50 0.76 13.44 63 29 22 78 8 8 2.88 0.81 18.95 62 28 58 71 8 8 4.13 0.87 23.06 54 21 17 88 12 7 3.14 0.61 18.77 59 11 21 88 12 10 2.80 0.67 16.38 50 22 18 83 8 9 3.00 0.60 22.79 38 24 23 128 14 8 1.00 0.30 15.2
10 60 2 8 43 6 7 3.29 1.40 26.411 50 19 28 77 11 8 3.00 0.65 12.5Mean 55.7 23.5 25.8 85.3 10.1 8.3 3.0 0.7 20.5
20 Spine • Volume 35 • Number 1 • 2010
demonstrate an increase in rotation toward the coronalapex of the deformity. While analyzing rotation in re-gards to the coronal apex, mean maximal rotation wasfound to be 20.5° and always occurred at or within 1 to2 levels inferior/distal to the coronal apex (Figure 6).
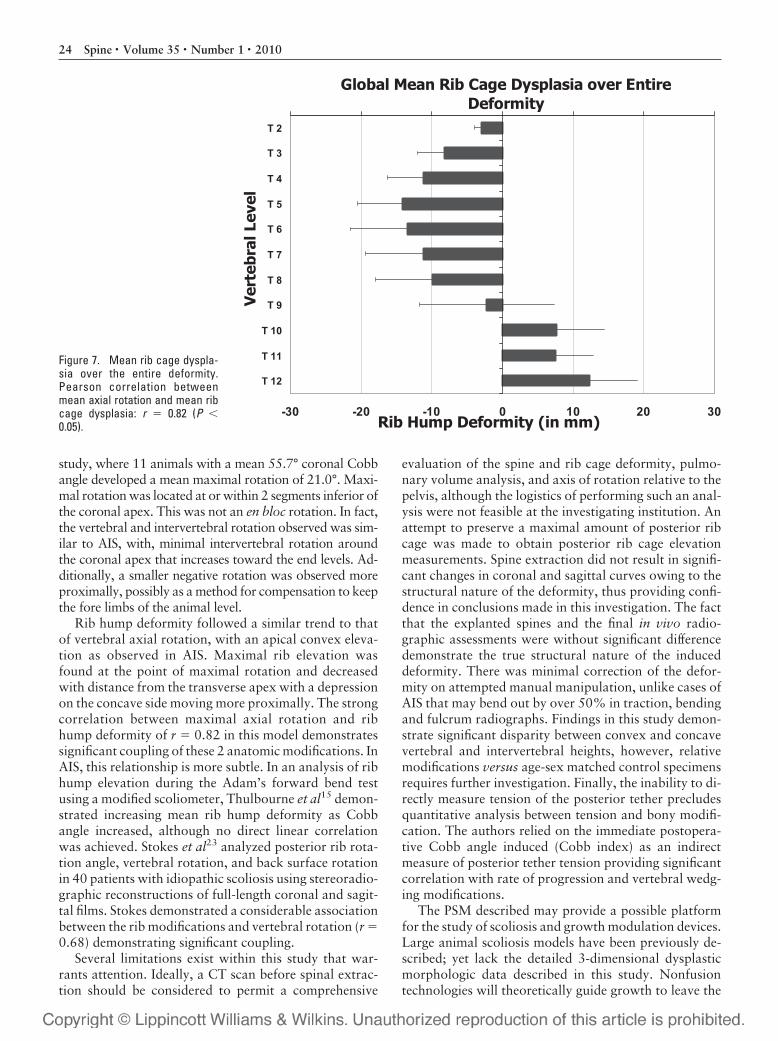
Rib Cage Asymmetry/DeformityMean rib hump deformity showed a graphical plot asdemonstrated in Figure 7. As shown, the mean rib humpelevation was negative between T2 and T9, demonstrat-ing an elevation on the curve concavity. From T9 to T12,the elevation was observed on the curve convexity. Theresulting Pearson correlation between mean rib humpdeformity and vertebral axial rotation was r � 0.82, (P �0.005).
Discussion
Optimal testing of nonfusion technologies requires theuse of an animal model that resembles AIS at the global,
regional, and segmental levels. Although idiopathic sco-liosis results in complex bone and soft tissue modifica-tions without absolute parallel in animal models, thisstudy demonstrates that asymmetrical mechanical teth-ering of the spine and the rib cage in a porcine modelresults in radiographic changes remarkably similar toAIS, progressive coronal Cobb angle, sagittal flattening/lordosis, and axial torsion, with vertebral body rotationinto the curve convexity.
Scoliosis curve progression is the result of asymmetrybetween the concave and convex spinal heights frombone and disc wedging most considerably at the apex ofthe deformity. In a morphometric analysis of 30 scolioticspecimens, Parent et al17 quantified vertebral wedging inthe frontal plane. Convex heights were significantlylarger than concave heights and maximally at the curveapex. Analysis of the apical functional unit in the PSMdemonstrated similar vertebral wedging whereby convexheights (mean, 57.8 mm) were significantly larger thanconcave heights (mean, 47.5 mm) resulting in a mean of20% disparity. Intervertebral disc wedging also demon-strated similar modifications; with convex heights(mean, 3.8 mm) significantly larger than concave heights(mean, 2.7 mm). Interestingly, the contribution of discwedging to the total wedging of convex and concaveheights was similar at 6.5% and 5.8%, respectively.These differences were not significant, demonstratingthat wedging occurred through true bone modulation.Additionally, the mechanical process acting and modu-lating vertebral growth may be acting on the disc in acomparable manner. This finding is further confirmed bythe correlation (r � 0.697, P � 0.012) observed betweenthe total convex/concave ratio and the disc convex/concave ratio, meaning the larger the bony wedging be-tween convex and concave sides, the larger the disc wedg-ing. Although no wedging was apparent between anteriorand posterior vertebral body heights (mean, 52.3 vs. 53.1mm), a comparison between age-sex matched controls is
Table 2. Mean Vertebral and Intervertebral HeightMeasurements (mm)
Parameter Mean Ht (mm) t Test (P)
Superior apical vertebra Anterior Ht 25.1 0.4527Posterior Ht 25.4Convex Ht 26.8 0.0000Concave Ht 22.3
Intervertebral disc Anterior Ht 2.7 0.0060Posterior Ht 2.2Convex Ht 3.8 0.0016Concave Ht 2.7
Inferior apical vertebra Anterior Ht 25 0.0233Posterior Ht 26.2Convex Ht 27.3 0.0000Concave Ht 22.4
Total functional unit Anterior Ht 52.8 0.1103Posterior Ht 53.8Convex Ht 57.8 0.0000Concave Ht 47.5
The t test analysis demonstrates significant differences between anterior-posterior heights (disc, inferior apical vertebrae) and all convex and concaveheights.
Total Functional Unit Height: Convex Vs Concave
0
10
20
30
40
50
60
70
1 2 3 4 5 6 7 8 9 10 11
Pig #
He
igh
t (m
m)
Convex Ht
Concave Ht
Figure 3. Total apical vertebralfunctional unit heights. Graphicrepresentation of the asymmetricconvex (untethered) versus con-cave (tethered) vertebral bodyheights over the entire studygroup (n � 11).
21CT Validation of the Porcine Scoliosis Model • Patel et al
lacking. Posterior intervertebral heights were significantlylarger than anterior vertebral heights; Owing to the naturalglobal sagittal kyphosis of the Yorkshire pig, this resultdoes allow the authors to speculate of the sagittal modifi-cations induced by posterior placement of the deformingtether. Further investigation into sagittal plane modifica-tions is currently being pursued.
Creation of vertebral wedging in the porcine model isconsistent with the Hueter-Volkmann Principle. Intraop-erative tensioning of a unilateral posterior directed flex-ible spinal tether results initially in disc wedging anddevelopment of a curve concavity. Persistent unilateralloading of the spine (left � right) from the tether resultsin ipsilateral growth plate modifications leading to sig-nificant growth modulation (left � right), bony wedging
and ultimately curve progression in the frontal plane.Analysis revealed interesting correlations between Totalconvex/concave ratio and both Cobb index and # weeksuntil animals achieved �50° coronal Cobb. These resultssuggest a larger initial Cobb angle (initial intraoperativetensioning of the tether) produced a larger final convex/concave ratio (greater wedging), and faster progressionto �50° Cobb angle. These findings can be paralleledwith those by Stokes et al,18 where a linear correlationr2 � 0.44 was demonstrated when compressive load as afunction of body weight was plotted against vertebralgrowth in a rat tail model. Larger axial loads decreasedvertebral growth significantly as compared with lesserloads or distraction. Although both examples demon-strate the Hueter-Volkmann principle in a dynamic fash-
Absolute Height (mm) Apical Functional Unit
0.0
5.0
10.0
15.0
20.0
25.0
30.0
Convex Concave Convex Concave Convex Concave
Superior Vertebrae Disc Inferior Vertebrae
Apical Segment
Hei
ght (
mm
)
Figure 4. Mean convex (untethered) versus concave (tethered) vertebral and intervertebral heights over the apical functional unit(superior and inferior apical vertebra and intervening disc).
Table 3. Correlation Analysis Demonstrating Significant Associations Within and Between Wedging Characteristicsand Relevant Descriptive Data
Parameter 1 Parameter 2 r P Implication
Total convex/concave ratio Disc convex/concave ratio 0.697 0.012 Large total wedging results in greater disc wedgingNo. wk till �50° Total convex/concave ratio �0.694 0.012 More rapid curve progression results in greater
total apical wedgingCobb index (initial) Total convex/concave ratio 0.632 0.027 Large initial Cobb index results in greater final
wedgingNo. days tethered Disc convex/concave ratio �0.653 0.021 Slow curve progression results in less disc
wedgingDisc convex/concave ratio Cobb increase/d 0.620 0.032 Greater disc wedging (tether tension) results in
more rapid curve progression per day
22 Spine • Volume 35 • Number 1 • 2010
ion, the use of a left-sided mechanical posterior tether inthis model was used to retard growth in a unilateralfashion resulting in vertebral wedging.
Vertebral rotation, a major entity within the scolioticdeformity, can be appreciated accurately with CT analysis.In a computed tomographic review of 33 structural idio-pathic scoliosis curves from preoperative patients, Acaro-
glu et al19 demonstrated the transverse apex (most rotatedvertebrae) was within 1 to 2 levels of the coronal apex.Additionally, in a review of 11 patients with idiopathicdeformities with a mean Cobb angle of 54.6°, Erkula et al20
demonstrated a mean 18.6° apical rotation into the curveconvexity. Similar rotation and Cobb angles were demon-strated by Birchall et al,21 Krismer et al,22 and the current
Global Vertebral and Intervertebral Axial Rotation over Entire Deformity
-10 -5 0 5 10 15 20 25
T 2
T 3
T 4
T 5
T 6
T 7
T 8
T 9
T 10
T 11
T 12
L 1
L 2
Ver
tebr
al L
evel
Rotation (in deg)
Figure 5. Mean axial rotationand standard deviation (RAsag)by vertebral level over entire spi-nal deformity (T12 designatedlast rib articulating vertebra).
Normalized (Coronal Apex) Rotation Over Scoliotic Curve
-15
-10
-5
0
5
10
15
20
25
CoronalA
pexRot
atio
n (d
egre
es)
Proximal Distal
Coronal Apex Transverse Apex
Figure 6. Mean axial rotation normalized to coronal apex. Maximum rotation was located within 1 to 2 levels distal to the coronal curve apex.
23CT Validation of the Porcine Scoliosis Model • Patel et al
study, where 11 animals with a mean 55.7° coronal Cobbangle developed a mean maximal rotation of 21.0°. Maxi-mal rotation was located at or within 2 segments inferior ofthe coronal apex. This was not an en bloc rotation. In fact,the vertebral and intervertebral rotation observed was sim-ilar to AIS, with, minimal intervertebral rotation aroundthe coronal apex that increases toward the end levels. Ad-ditionally, a smaller negative rotation was observed moreproximally, possibly as a method for compensation to keepthe fore limbs of the animal level.
Rib hump deformity followed a similar trend to thatof vertebral axial rotation, with an apical convex eleva-tion as observed in AIS. Maximal rib elevation wasfound at the point of maximal rotation and decreasedwith distance from the transverse apex with a depressionon the concave side moving more proximally. The strongcorrelation between maximal axial rotation and ribhump deformity of r � 0.82 in this model demonstratessignificant coupling of these 2 anatomic modifications. InAIS, this relationship is more subtle. In an analysis of ribhump elevation during the Adam’s forward bend testusing a modified scoliometer, Thulbourne et al15 demon-strated increasing mean rib hump deformity as Cobbangle increased, although no direct linear correlationwas achieved. Stokes et al23 analyzed posterior rib rota-tion angle, vertebral rotation, and back surface rotationin 40 patients with idiopathic scoliosis using stereoradio-graphic reconstructions of full-length coronal and sagit-tal films. Stokes demonstrated a considerable associationbetween the rib modifications and vertebral rotation (r �0.68) demonstrating significant coupling.
Several limitations exist within this study that war-rants attention. Ideally, a CT scan before spinal extrac-tion should be considered to permit a comprehensive
evaluation of the spine and rib cage deformity, pulmo-nary volume analysis, and axis of rotation relative to thepelvis, although the logistics of performing such an anal-ysis were not feasible at the investigating institution. Anattempt to preserve a maximal amount of posterior ribcage was made to obtain posterior rib cage elevationmeasurements. Spine extraction did not result in signifi-cant changes in coronal and sagittal curves owing to thestructural nature of the deformity, thus providing confi-dence in conclusions made in this investigation. The factthat the explanted spines and the final in vivo radio-graphic assessments were without significant differencedemonstrate the true structural nature of the induceddeformity. There was minimal correction of the defor-mity on attempted manual manipulation, unlike cases ofAIS that may bend out by over 50% in traction, bendingand fulcrum radiographs. Findings in this study demon-strate significant disparity between convex and concavevertebral and intervertebral heights, however, relativemodifications versus age-sex matched control specimensrequires further investigation. Finally, the inability to di-rectly measure tension of the posterior tether precludesquantitative analysis between tension and bony modifi-cation. The authors relied on the immediate postopera-tive Cobb angle induced (Cobb index) as an indirectmeasure of posterior tether tension providing significantcorrelation with rate of progression and vertebral wedg-ing modifications.
The PSM described may provide a possible platformfor the study of scoliosis and growth modulation devices.Large animal scoliosis models have been previously de-scribed; yet lack the detailed 3-dimensional dysplasticmorphologic data described in this study. Nonfusiontechnologies will theoretically guide growth to leave the
Global Mean Rib Cage Dysplasia over Entire Deformity
-30 -20 -10 0 10 20 30
T 2
T 3
T 4
T 5
T 6
T 7
T 8
T 9
T 10
T 11
T 12
Ver
tebr
al L
evel
Rib Hump Deformity (in mm)
Figure 7. Mean rib cage dyspla-sia over the entire deformity.Pearson correlation betweenmean axial rotation and mean ribcage dysplasia: r � 0.82 (P �0.05).
24 Spine • Volume 35 • Number 1 • 2010

patient with a balanced spine. Ideal modifications duringprogressive correction would include normalization ofconcave, convex vertebral heights in the frontal plane,reduction of lateral spinal displacement, derotation ofidiopathic modifications in the axial plane, and re-establishment of harmonious curves in the sagittal plane.Additionally, if feasible, correction of the rib hump de-formity to leave an even surface contour. These modifi-cations would address the relevant functional and cos-metic concerns in the setting of a progressivelydeforming vertebral column and rib cage deformitywhile potentially sparing mobile segments. Whether thisis possible in a single, safe, cost-effective intervention willbe the focus of our efforts moving forward.
Conclusion
A Porcine Model for progressive thoracic scoliosis hasbeen described, with application of a unilateral posteriortether and ipsilateral rib cage tethering during the rapidgrowth stage of a Yorkshire pig, a 3-dimensional spinaldeformity can be achieved. The present study has usedCT analysis to further detail spinal and rib cage modifi-cations of the extracted spines. The porcine model is areliable and duplicable model for scoliosis, which bearssignificant similarities to AIS.
Key Points
● Application of a unilateral posterior ligamentoustether and ipsilateral rib cage tethering in an im-mature Yorkshire pig results in spinal and ribcage modifications similar to adolescent idio-pathic scoliosis.
● Scoliotic curve progression in the porcine scolio-sis model results from true vertebral and inter-vertebral growth modulation.
● With a large growth potential, ease of handlingand comparative spinal anatomy to an adoles-cent human, the porcine scoliosis model mayprovide a possible platform for the study of sco-liosis and growth modulation devices.
AcknowledgmentsThe authors thank Anthony Siconolfi and Amanda Vegafor their contributions.
References
1. Dubousset J. [Idiopathic scoliosis. Definition–pathology–classification–etiology]. Bull Acad Natl Med 1999;183:699–704.
2. Dubousset J. Scoliosis and its pathophysiology: do we understand it? Spine2001;26:1001.
3. Graf H, Hecquet J, Dubousset J. [3-dimensional approach to spinal defor-mities. Application to the study of the prognosis of pediatric scoliosis]. RevChir Orthop Reparatrice Appar Mot 1983;69:407–16.
4. Betz RR, Kim J, D’Andrea LP, et al. An innovative technique of vertebralbody stapling for the treatment of patients with adolescent idiopathic scoli-osis: a feasibility, safety, and utility study. Spine 2003;28:S255–65.
5. Braun JT, Akyuz E, Ogilvie JW, et al. The efficacy and integrity of shape memoryalloy staples and bone anchors with ligament tethers in the fusionless treatmentof experimental scoliosis. J Bone Joint Surg Am 2005;87:2038–51.
6. Lowe TG, Wilson L, Chien JT, et al. A posterior tether for fusionlessmodulation of sagittal plane growth in a sheep model. Spine 2005;30:S69 –74.
7. Newton PO, Farnsworth CL, Faro FD, et al. Spinal growth modulation withan anterolateral flexible tether in an immature bovine model: disc health andmotion preservation. Spine 2008;33:724–33.
8. Newton PO, Faro FD, Farnsworth CL, et al. Multilevel spinal growth mod-ulation with an anterolateral flexible tether in an immature bovine model.Spine 2005;30:2608–13.
9. Wall EJ, Bylski-Austrow DI, Kolata RJ, et al. Endoscopic mechanical spinalhemiepiphysiodesis modifies spine growth. Spine 2005;30:1148–53.
10. Braun JT, Ogilvie JW, Akyuz E, et al. Creation of an experimental idiopath-ic-type scoliosis in an immature goat model using a flexible posterior asym-metric tether. Spine 2006;31:1410–4.
11. Braun JT, Ogilvie JW, Akyuz E, et al. Experimental scoliosis in an immaturegoat model: a method that creates idiopathic-type deformity with minimalviolation of the spinal elements along the curve. Spine 2003;28:2198–203.
12. Schwab F, Patel A, Lafage V, et al. A porcine model for progressive thoracicscoliosis. Spine 2009;34:E397–404.
13. McLain RF, Yerby SA, Moseley TA. Comparative morphometry of L4 ver-tebrae: comparison of large animal models for the human lumbar spine.Spine 2002;27:E200–6.
14. Aaro S, Dahlborn M, Svensson L. Estimation of vertebral rotation in struc-tural scoliosis by computer tomography. Acta Radiol Diagn (Stockh) 1978;19:990–2.
15. Thulbourne T, Gillespie R. The rib hump in idiopathic scoliosis. Measurement,analysis and response to treatment. J Bone Joint Surg Br 1976;58:64–71.
16. Harding IJ, Chopin D, Charosky S, et al. Long-term results of schollnercostoplasty in patients with idiopathic scoliosis. Spine 2005;30:1627–31.
17. Parent S, Labelle H, Skalli W, et al. Morphometric analysis of anatomicscoliotic specimens. Spine 2002;27:2305–11.
18. Stokes IA, Spence H, Aronsson DD, et al. Mechanical modulation of verte-bral body growth. Implications for scoliosis progression. Spine 1996;21:1162–7.
19. Acaroglu E, Yazici M, Deviren V, et al. Does transverse apex coincide withcoronal apex levels (regional or global) in adolescent idiopathic scoliosis?Spine 2001;26:1143–6.
20. Erkula G, Sponseller PD, Kiter AE. Rib deformity in scoliosis. Eur Spine J2003;12:281–7.
21. Birchall D, Hughes DG, Hindle J, et al. Measurement of vertebral rotation inadolescent idiopathic scoliosis using three-dimensional magnetic resonanceimaging. Spine 1997;22:2403–7.
22. Krismer M, Sterzinger W, Haid C, et al. Axial rotation measurement ofscoliotic vertebrae by means of computed tomography scans. Spine 1996;21:576–81.
23. Stokes IA. Axial rotation component of thoracic scoliosis. J Orthop Res1989;7:702–8.
25CT Validation of the Porcine Scoliosis Model • Patel et al