complications and co-morbidities in radiographs of patients in traditional bone setters’ homes in...
TRANSCRIPT
Cs
KD
a
ARA
KTCCOR
1
saomtmbfltfsi
0d
European Journal of Radiology 81 (2012) 2323–2328
Contents lists available at ScienceDirect
European Journal of Radiology
journa l homepage: www.e lsev ier .com/ locate /e j rad
omplications and co-morbidities in radiographs of patients in traditional boneetters’ homes in Ogwa, Edo State, Nigeria: a community-based study
enneth C. Eze ∗
epartment of Radiology, Faculty of Medicine, College of Health Sciences, Nnamdi Azikiwe University, Nnewi Campus, Anambra State, Nigeria
r t i c l e i n f o
rticle history:eceived 12 March 2011ccepted 7 June 2011
eywords:raditional bone settersomplicationso-morbiditiesgwaadiographs
a b s t r a c t
Background: Musculoskeletal injuries are common in developing countries, but access to high qualityorthopedic care is not. Traditional bone setters (TBS) serve to fill the gap, but the nature and qualityof their treatment are largely understudied. Traditional bone setting in Idunmunkpaghan clan of Ogwacommunity, Edo State, Nigeria, was founded by Odion Ekhimere between about 1680 and 1705. The TBSpractice in this community is studied to find out the complications and co-morbidities associated with it.Methods: A prospective community-based study of the patients admitted in the traditional bone setters’homes was done at Ogwa over a -2-year period by studying the admission and discharge radiographs ofpatients treated in the community and by interviewing the TBS and patients.Result: Ninety patients with radiographs of the lesion sites were followed up from admission to dischargeat the TBS homes, comprising 53 males (53.89%) and 37 females (41.11%) with a male to female ratio of1.4:1. Sixty five patients (72.2%) had fracture or dislocation. Forty four of the 65 patients (67.7%) withfracture/dislocation had complications including mal-union 31(70.4%), secondary osteoarthritis 8 (18.2%),non-reduction of dislocation 7 (11.9%), non-union 8 (18.2%), and others 12 (27.2%). Co-morbidities wereidentified in 15 patients (16.7%) and included severe osteoarthritis 7 (46.7%), diabetic foot ulcer 4 (26.7%),
severe hypertension with cardiomegaly 4 (26.7%), metastatic carcinoma of the prostate 3 (20.0%), septicarthritis 2 (13.3%), pulmonary tuberculosis 1 (6.7%) and others 3 (20.0%).Conclusion: The practice of traditional bone setting is well established in Idunmunkpaghan clan in Ukpogoquarter of Ogwa. Education and training of the TBS is the key to reduction of complications and co-morbidities seen in their practices as they have high patronage and the patients have high regards forthem and will continue to patronize them.. Introduction
Traditional bone setters (TBS) are common in many rural andub-urban areas in developing countries and serve as readily avail-ble, accessible, highly acceptable orthopedic practitioners andffer affordable treatment options for fractures in the areas whereodern orthopedic practice is absent. The TBS admit patients in
heir homes and have high patronage in these rural areas. Theethod they use in fixing fractures involves setting the bones
y closed manipulation of the fragments, stabilizing the fractureragments at the fracture site with sticks of about 1.5–2 feet inength and tying the sticks with ropes around the fracture siteo hold it in place [1–5] (Fig. 1). The TBS are a source of hope
or the patients, are from the same social group and share theame cultural belief with the patients. These contribute to mak-ng them highly acceptable [6,7]. Some TBS have embraced the use∗ Corresponding author. Tel.: +234 8037275383.E-mail address: [email protected]
720-048X/$ – see front matter © 2011 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.ejrad.2011.06.030
© 2011 Elsevier Ireland Ltd. All rights reserved.
of X-rays for diagnosing fractures, assessing their treatment andchecking for adequate alignment and union. The recent availabil-ity of X-ray facilities in some rural and sub-urban hospitals hasalso helped the TBS in accessing this technology [8,9]. In addition,because the TBS are not very efficient in the control of infectionsdue to open soft tissue injuries, some of them have recognizedthis and developed the practice of referral of these patients to thehospital in the acute stages where X-ray examinations are alsocarried out [6,7,9]. The bone condition is later taken to the TBSeither after discharge of the patient against medical advice, self-referral by patients or referral by a few orthodox doctors (withoutorthopedic experience or skill) who have come to recognize theproficiency of TBS in treating uncomplicated fractures in areaswhere modern orthopedic practice is absent. This is a study of com-plications and co-morbidities associated with the practices of theTBS, to document them for educational purposes toward improved
their awareness, and understanding of the existing socioeconomicconditions that encourage it and ultimately to bring the issue tothe attention of relevant authorities and political elite in order toinstitute measures to educate, recognise and control them with
2324 K.C. Eze / European Journal of Radi
FO
ns
2
mL
saf
cOEohDw2buEkvp
ftpthttatpTfait
ig. 1. Photograph of a limb with fractures that was already set (reduced) by TBS ingwa. Note the sticks and the bandages used to tie the sticks around the leg.
ecessary laws and prevent or reduce future occurrence of theimilar complications and co-morbidities.
. Material, subjects, and methods
A prospective community-based study was conducted at Idun-unkpaghan clan in Ukpogo quarters of Ogwa town, Esan West
ocal government Area, Edo State, Nigeria.Over a period of two years (21 April 2008 to 20 April 2010), a
tudy of the practices of TBS was done at Ogwa. The town is uniquend popular for traditional bone setting practice ever since it wasounded in the town by one Odion Ekhimere about 1680 and 1705.
An ethnographical sketch shows that Ogwa is an agrarian ruralommunity. The native inhabitants are Esan, a sub-tribe of Bini.gwa is lying between 06.25′ N and 0.06.15 latitudes and 0.06.06′
and 0.06.12 longitudes [10]. It is located about 60 km northeastf Benin City, 40 km southeast of Ekpoma, the local governmenteadquarters of Esan West LGA and 45 km northwest of Agbor inelta State. The population of Ogwa according to the 1991 censusas 5971. Since the annual population growth rate of Edo State is
.74% per annum as shown by the 2006 census, Ogwa’s populationy 2010 is estimated to be about 9458 [11]. Ogwa town is madep of five different villages called quarters namely Eguare, Ukpogo,ha, Izogen and Upper Izogen. Only a clan in the Ukpogo quarternown as Idunmunkpaghan practises traditional bone setting, andirtually all of the blood-born adult males of Idunmunkpaghan clanractise the art as ancestral heritage.
Informed consent explained in native language was obtainedrom the patients, their relations (in the case of a minor), the tradi-ional bone setters and the chief of the community for the study. Theatients were followed up from admission to discharge and some-imes up to eight repeated visits as clinic attendance at the TBSomes. Only patients with admission and discharge radiographso prove the complications and co-morbidities were included inhis study. On the whole 90 patients with radiographs of the lesionnd fracture sites were studied. The radiographs were viewed bywo radiologists and the conclusion arrived at by consensus. Theatients seen at TBS’ homes and some TBS were also interviewed.here were several logistic problems in obtaining the radiographs
or this study. The patients who visited orthodox health centreslways had their radiographs as this was ordered by the attend-ng physicians or requested by the patients knowing full well thathey intend to visit the TBS after the acute phase of their injuries.ology 81 (2012) 2323–2328
However, the repeat radiographs were always ordered by the TBS.Chief Isaac Igbode who is the coordinator of the practice alreadyexplained that radiographs are usually ordered for fresh patientsbut in practice this was not always so. This constituted a sourceof bias and limitation for the study as those without admissionand discharge radiographs were excluded from the study. In prac-tice many patients had many repeated radiographs within the 2years of the study period allowing for adequate assessment of theprogress of the healing process. A number of patients ordered theserepeat radiographs by themselves in many occasions, so that manypatients had what appeared like a library of radiographs for theirinjuries. On further interview of some of the patients and scrutinyof some of the medical documents they used to attend orthodoxhospitals before coming to the TBS for what they considered as“bone conditions”, it was observed that the patients with hyper-tension, diabetes mellitus and cardiomegaly, septic arthritis witheffusion were previously attending different specialist clinics forthese conditions and had several reports of hospital investigationsconfirming their conditions. They defaulted when they felt that thepain associated with these conditions was of bone origin and shouldbe best treated at the TBS’ homes. Blood pressure measurementswere recorded in the request cards for X-rays and other laboratoryinvestigations by the physicians at the hospitals where the patientswere previously admitted before opting for treatment at the TBS’homes and their chest radiographs showed marked cardiomegalywithout any evidence of chest injury. Many of the radiographs seenat the TBS’ homes were poorly kept and some matted together dueto contact with liquid material.
The patient with tuberculosis had sputum examination for acidand alcohol fast bacilli which proved positive in addition to posi-tive chest radiographic signs of tuberculosis. However, the patientconsidered the chest pain to be originating from the ribs andtherefore sought treatment at the TBS’ home. Two of the patientswith metastatic carcinoma of the prostate had several hospitalinvestigations confirming carcinoma of prostate but did not havesevere urinary symptoms. They therefore considered their condi-tion a primary bone condition since they had severe waist andchest pain. The third patient with metastatic carcinoma of theprostate had orchidectomy 4 years previously. The patients withsecondary osteoarthritis had their admission, discharge and followup radiographs over two years which clearly showed absence ofosteoarthritis in the initial radiographs and its progressive devel-opment in serial repeat radiographs.
Patients without complain of fracture or dislocation wereexcluded from this study since complications were not possiblein these patients. Also, patients without admission and dischargeradiographs were excluded from the study since an objectiveassessment of the bone injury and treatment outcome or compli-cation could not be made. The data is presented and analyzed usingMicrosoft Excel in simple statistical terms.
3. Results
A total of 90 patients with radiographs of the fracture or lesionsites were seen at the TBS homes in Ogwa comprising 53 (58.89%)males and 37 (41.11%) females with a male to female ratio of 1.4:1.The number of TBS who participated in the treatment of patientsin this study was 17, all of whom are males resident in the Idun-munkpaghan clan. Most of the patients had visited the TBS after aroad traffic accident (RTA) 64 (71.1%). The causes were not known in14 (15.6%), 7 (7.8%) were due to a fall, and 3 (3.3%) assault, 1 (1.1%)sports, while 1 (1.1%) was due to fire arm injury. In 28 patients
(31.1%) there was only one fracture site, 26 (28.9%) had multiplefractures while in 15 (16.7%) no injury at all was noted or no frac-ture was seen. Of the 64 patients with RTA, there were 33 malesand 31 females.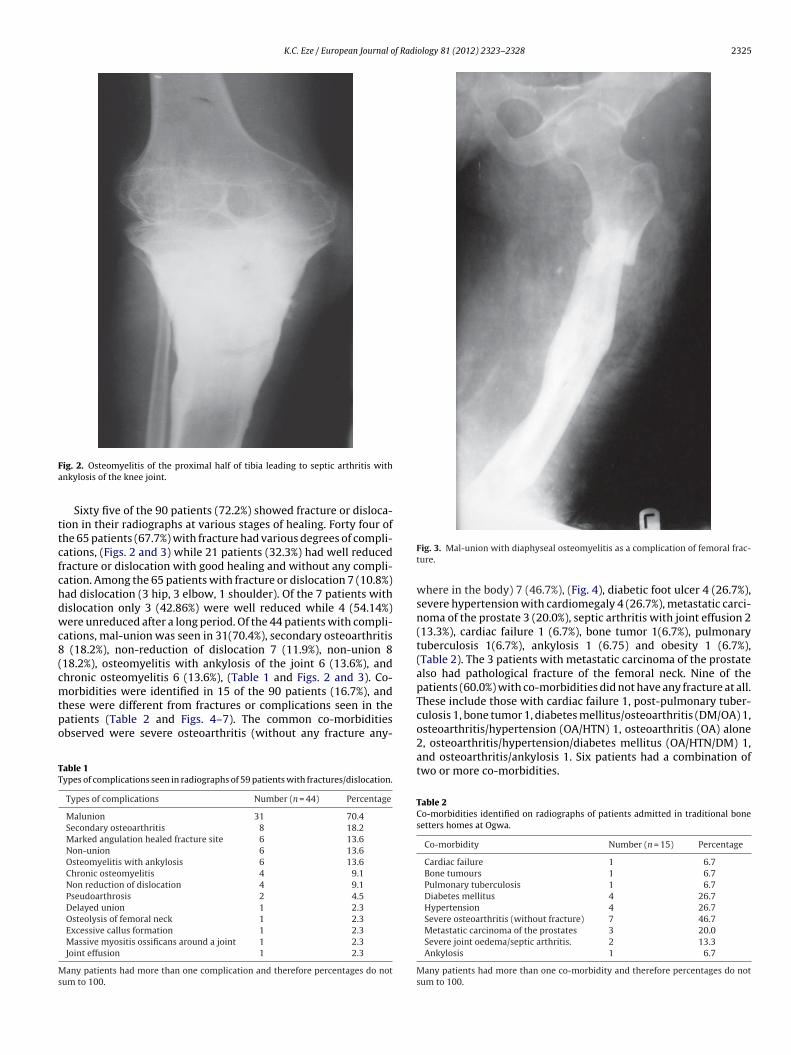
K.C. Eze / European Journal of Radiology 81 (2012) 2323–2328 2325
Fa
ttcfchdwc8(cmtpo
TT
Ms
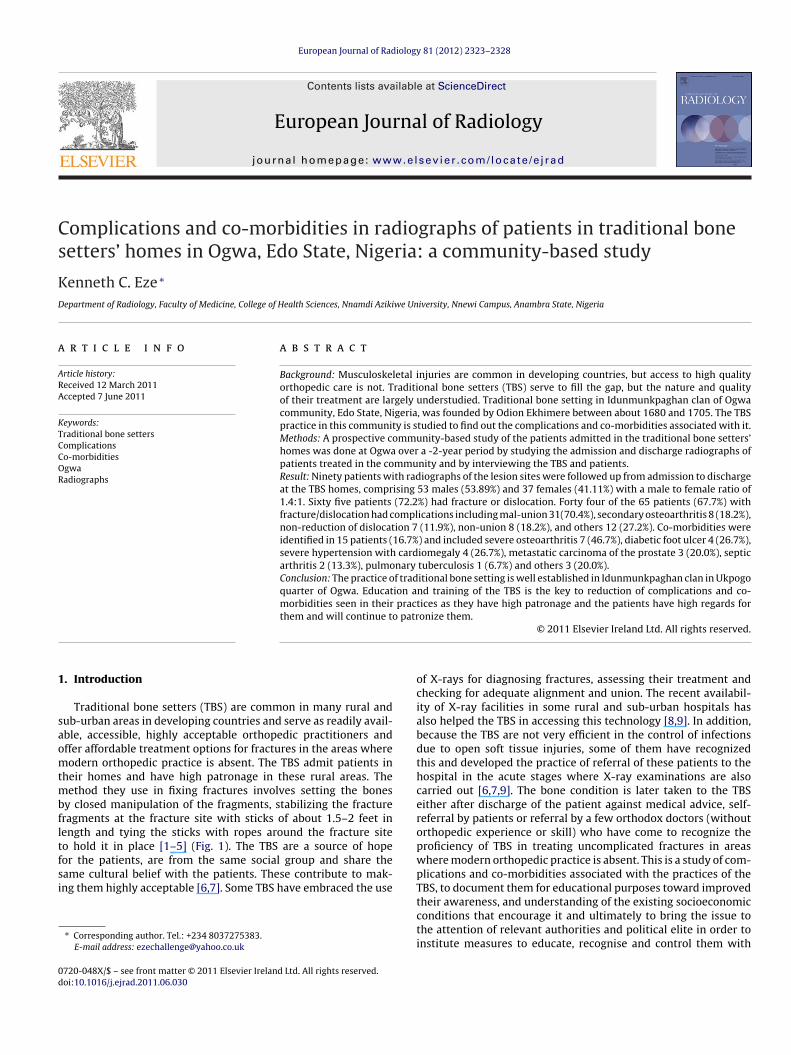
ig. 2. Osteomyelitis of the proximal half of tibia leading to septic arthritis withnkylosis of the knee joint.
Sixty five of the 90 patients (72.2%) showed fracture or disloca-ion in their radiographs at various stages of healing. Forty four ofhe 65 patients (67.7%) with fracture had various degrees of compli-ations, (Figs. 2 and 3) while 21 patients (32.3%) had well reducedracture or dislocation with good healing and without any compli-ation. Among the 65 patients with fracture or dislocation 7 (10.8%)ad dislocation (3 hip, 3 elbow, 1 shoulder). Of the 7 patients withislocation only 3 (42.86%) were well reduced while 4 (54.14%)ere unreduced after a long period. Of the 44 patients with compli-
ations, mal-union was seen in 31(70.4%), secondary osteoarthritis(18.2%), non-reduction of dislocation 7 (11.9%), non-union 8
18.2%), osteomyelitis with ankylosis of the joint 6 (13.6%), andhronic osteomyelitis 6 (13.6%), (Table 1 and Figs. 2 and 3). Co-orbidities were identified in 15 of the 90 patients (16.7%), and
hese were different from fractures or complications seen in theatients (Table 2 and Figs. 4–7). The common co-morbiditiesbserved were severe osteoarthritis (without any fracture any-
able 1ypes of complications seen in radiographs of 59 patients with fractures/dislocation.
Types of complications Number (n = 44) Percentage
Malunion 31 70.4Secondary osteoarthritis 8 18.2Marked angulation healed fracture site 6 13.6Non-union 6 13.6Osteomyelitis with ankylosis 6 13.6Chronic osteomyelitis 4 9.1Non reduction of dislocation 4 9.1Pseudoarthrosis 2 4.5Delayed union 1 2.3Osteolysis of femoral neck 1 2.3Excessive callus formation 1 2.3Massive myositis ossificans around a joint 1 2.3Joint effusion 1 2.3
any patients had more than one complication and therefore percentages do notum to 100.
Fig. 3. Mal-union with diaphyseal osteomyelitis as a complication of femoral frac-ture.
where in the body) 7 (46.7%), (Fig. 4), diabetic foot ulcer 4 (26.7%),severe hypertension with cardiomegaly 4 (26.7%), metastatic carci-noma of the prostate 3 (20.0%), septic arthritis with joint effusion 2(13.3%), cardiac failure 1 (6.7%), bone tumor 1(6.7%), pulmonarytuberculosis 1(6.7%), ankylosis 1 (6.75) and obesity 1 (6.7%),(Table 2). The 3 patients with metastatic carcinoma of the prostatealso had pathological fracture of the femoral neck. Nine of thepatients (60.0%) with co-morbidities did not have any fracture at all.These include those with cardiac failure 1, post-pulmonary tuber-culosis 1, bone tumor 1, diabetes mellitus/osteoarthritis (DM/OA) 1,
osteoarthritis/hypertension (OA/HTN) 1, osteoarthritis (OA) alone2, osteoarthritis/hypertension/diabetes mellitus (OA/HTN/DM) 1,and osteoarthritis/ankylosis 1. Six patients had a combination oftwo or more co-morbidities.Table 2Co-morbidities identified on radiographs of patients admitted in traditional bonesetters homes at Ogwa.
Co-morbidity Number (n = 15) Percentage
Cardiac failure 1 6.7Bone tumours 1 6.7Pulmonary tuberculosis 1 6.7Diabetes mellitus 4 26.7Hypertension 4 26.7Severe osteoarthritis (without fracture) 7 46.7Metastatic carcinoma of the prostates 3 20.0Severe joint oedema/septic arthritis. 2 13.3Ankylosis 1 6.7
Many patients had more than one co-morbidity and therefore percentages do notsum to 100.
2326 K.C. Eze / European Journal of Radiology 81 (2012) 2323–2328
Fb
4
rcpatvet
dom
Ft
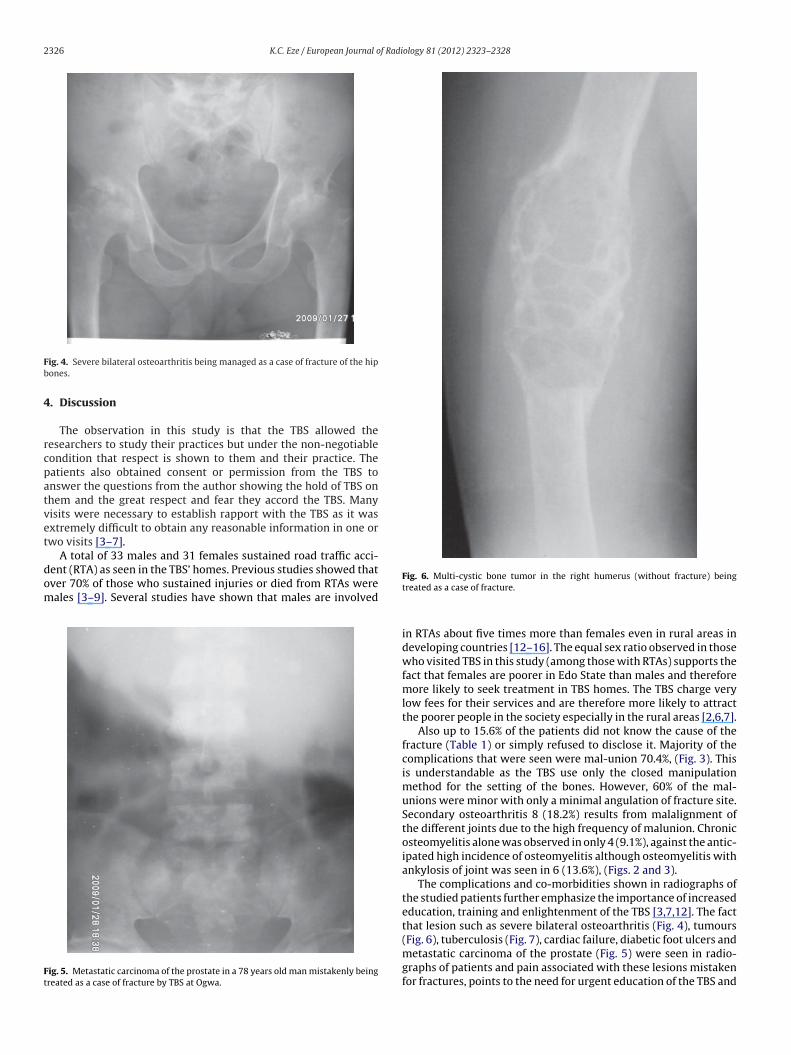
ig. 4. Severe bilateral osteoarthritis being managed as a case of fracture of the hipones.
. Discussion
The observation in this study is that the TBS allowed theesearchers to study their practices but under the non-negotiableondition that respect is shown to them and their practice. Theatients also obtained consent or permission from the TBS tonswer the questions from the author showing the hold of TBS onhem and the great respect and fear they accord the TBS. Manyisits were necessary to establish rapport with the TBS as it wasxtremely difficult to obtain any reasonable information in one orwo visits [3–7].
A total of 33 males and 31 females sustained road traffic acci-ent (RTA) as seen in the TBS’ homes. Previous studies showed thatver 70% of those who sustained injuries or died from RTAs wereales [3–9]. Several studies have shown that males are involved
ig. 5. Metastatic carcinoma of the prostate in a 78 years old man mistakenly beingreated as a case of fracture by TBS at Ogwa.
Fig. 6. Multi-cystic bone tumor in the right humerus (without fracture) beingtreated as a case of fracture.
in RTAs about five times more than females even in rural areas indeveloping countries [12–16]. The equal sex ratio observed in thosewho visited TBS in this study (among those with RTAs) supports thefact that females are poorer in Edo State than males and thereforemore likely to seek treatment in TBS homes. The TBS charge verylow fees for their services and are therefore more likely to attractthe poorer people in the society especially in the rural areas [2,6,7].
Also up to 15.6% of the patients did not know the cause of thefracture (Table 1) or simply refused to disclose it. Majority of thecomplications that were seen were mal-union 70.4%, (Fig. 3). Thisis understandable as the TBS use only the closed manipulationmethod for the setting of the bones. However, 60% of the mal-unions were minor with only a minimal angulation of fracture site.Secondary osteoarthritis 8 (18.2%) results from malalignment ofthe different joints due to the high frequency of malunion. Chronicosteomyelitis alone was observed in only 4 (9.1%), against the antic-ipated high incidence of osteomyelitis although osteomyelitis withankylosis of joint was seen in 6 (13.6%), (Figs. 2 and 3).
The complications and co-morbidities shown in radiographs ofthe studied patients further emphasize the importance of increasededucation, training and enlightenment of the TBS [3,7,12]. The factthat lesion such as severe bilateral osteoarthritis (Fig. 4), tumours
(Fig. 6), tuberculosis (Fig. 7), cardiac failure, diabetic foot ulcers andmetastatic carcinoma of the prostate (Fig. 5) were seen in radio-graphs of patients and pain associated with these lesions mistakenfor fractures, points to the need for urgent education of the TBS and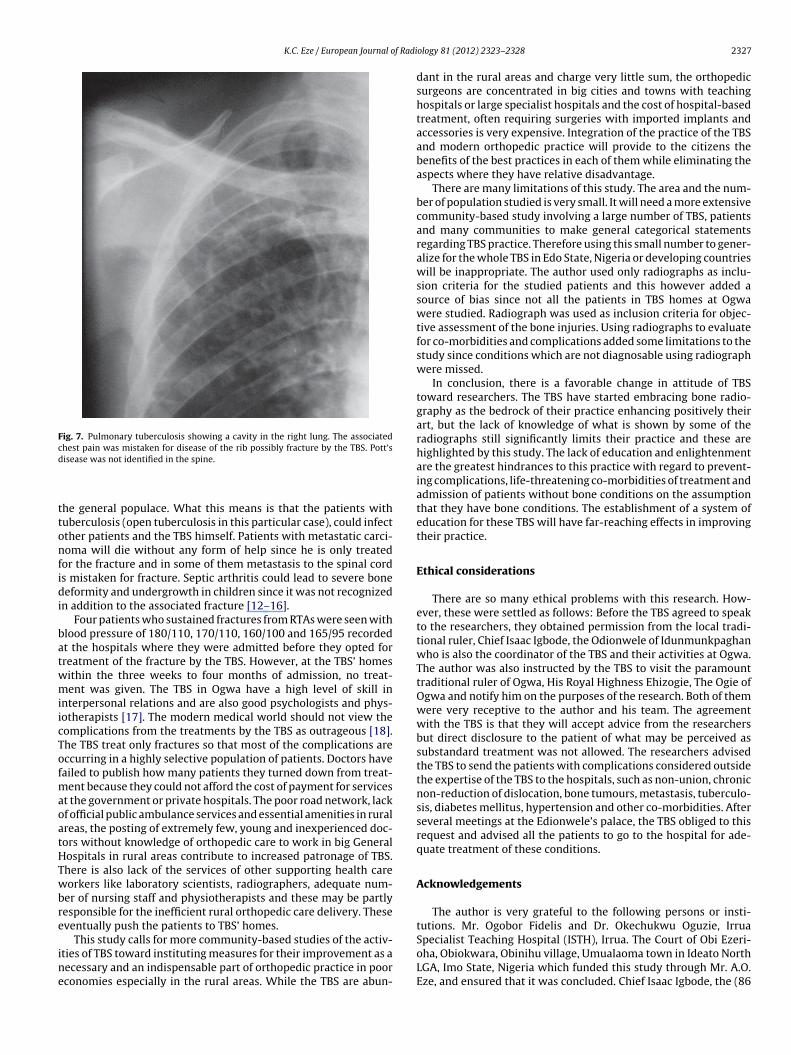
K.C. Eze / European Journal of Radi
Fig. 7. Pulmonary tuberculosis showing a cavity in the right lung. The associatedchest pain was mistaken for disease of the rib possibly fracture by the TBS. Pott’sd
ttonfidi
batwmiicTofmaoatHTwbre
ine
Specialist Teaching Hospital (ISTH), Irrua. The Court of Obi Ezeri-
isease was not identified in the spine.
he general populace. What this means is that the patients withuberculosis (open tuberculosis in this particular case), could infectther patients and the TBS himself. Patients with metastatic carci-oma will die without any form of help since he is only treated
or the fracture and in some of them metastasis to the spinal cords mistaken for fracture. Septic arthritis could lead to severe boneeformity and undergrowth in children since it was not recognized
n addition to the associated fracture [12–16].Four patients who sustained fractures from RTAs were seen with
lood pressure of 180/110, 170/110, 160/100 and 165/95 recordedt the hospitals where they were admitted before they opted forreatment of the fracture by the TBS. However, at the TBS’ homesithin the three weeks to four months of admission, no treat-ent was given. The TBS in Ogwa have a high level of skill in
nterpersonal relations and are also good psychologists and phys-otherapists [17]. The modern medical world should not view theomplications from the treatments by the TBS as outrageous [18].he TBS treat only fractures so that most of the complications areccurring in a highly selective population of patients. Doctors haveailed to publish how many patients they turned down from treat-
ent because they could not afford the cost of payment for servicest the government or private hospitals. The poor road network, lackf official public ambulance services and essential amenities in ruralreas, the posting of extremely few, young and inexperienced doc-ors without knowledge of orthopedic care to work in big Generalospitals in rural areas contribute to increased patronage of TBS.here is also lack of the services of other supporting health careorkers like laboratory scientists, radiographers, adequate num-
er of nursing staff and physiotherapists and these may be partlyesponsible for the inefficient rural orthopedic care delivery. Theseventually push the patients to TBS’ homes.
This study calls for more community-based studies of the activ-
ties of TBS toward instituting measures for their improvement as aecessary and an indispensable part of orthopedic practice in poorconomies especially in the rural areas. While the TBS are abun-ology 81 (2012) 2323–2328 2327
dant in the rural areas and charge very little sum, the orthopedicsurgeons are concentrated in big cities and towns with teachinghospitals or large specialist hospitals and the cost of hospital-basedtreatment, often requiring surgeries with imported implants andaccessories is very expensive. Integration of the practice of the TBSand modern orthopedic practice will provide to the citizens thebenefits of the best practices in each of them while eliminating theaspects where they have relative disadvantage.
There are many limitations of this study. The area and the num-ber of population studied is very small. It will need a more extensivecommunity-based study involving a large number of TBS, patientsand many communities to make general categorical statementsregarding TBS practice. Therefore using this small number to gener-alize for the whole TBS in Edo State, Nigeria or developing countrieswill be inappropriate. The author used only radiographs as inclu-sion criteria for the studied patients and this however added asource of bias since not all the patients in TBS homes at Ogwawere studied. Radiograph was used as inclusion criteria for objec-tive assessment of the bone injuries. Using radiographs to evaluatefor co-morbidities and complications added some limitations to thestudy since conditions which are not diagnosable using radiographwere missed.
In conclusion, there is a favorable change in attitude of TBStoward researchers. The TBS have started embracing bone radio-graphy as the bedrock of their practice enhancing positively theirart, but the lack of knowledge of what is shown by some of theradiographs still significantly limits their practice and these arehighlighted by this study. The lack of education and enlightenmentare the greatest hindrances to this practice with regard to prevent-ing complications, life-threatening co-morbidities of treatment andadmission of patients without bone conditions on the assumptionthat they have bone conditions. The establishment of a system ofeducation for these TBS will have far-reaching effects in improvingtheir practice.
Ethical considerations
There are so many ethical problems with this research. How-ever, these were settled as follows: Before the TBS agreed to speakto the researchers, they obtained permission from the local tradi-tional ruler, Chief Isaac Igbode, the Odionwele of Idunmunkpaghanwho is also the coordinator of the TBS and their activities at Ogwa.The author was also instructed by the TBS to visit the paramounttraditional ruler of Ogwa, His Royal Highness Ehizogie, The Ogie ofOgwa and notify him on the purposes of the research. Both of themwere very receptive to the author and his team. The agreementwith the TBS is that they will accept advice from the researchersbut direct disclosure to the patient of what may be perceived assubstandard treatment was not allowed. The researchers advisedthe TBS to send the patients with complications considered outsidethe expertise of the TBS to the hospitals, such as non-union, chronicnon-reduction of dislocation, bone tumours, metastasis, tuberculo-sis, diabetes mellitus, hypertension and other co-morbidities. Afterseveral meetings at the Edionwele’s palace, the TBS obliged to thisrequest and advised all the patients to go to the hospital for ade-quate treatment of these conditions.
Acknowledgements
The author is very grateful to the following persons or insti-tutions. Mr. Ogobor Fidelis and Dr. Okechukwu Oguzie, Irrua
oha, Obiokwara, Obinihu village, Umualaoma town in Ideato NorthLGA, Imo State, Nigeria which funded this study through Mr. A.O.Eze, and ensured that it was concluded. Chief Isaac Igbode, the (86

2 f Radi
ytam
eimttAOoEfiiTa
R
[
[
[
[
[
[
[
[of traditional Chinese and western medicine. In: Robert HB, Burton J, Ch’enW, editors. Traditional medicine and health care coverage. A reader for health
328 K.C. Eze / European Journal o
ears in 2010) Edionwele of Idunmunkpaghan clan in Ukpogo quar-ers, Ogwa who is the present co-ordinator of the activities of TBSt Ogwa. Mr. Imafidon Fada, a TBS and a direct descendant of thean that brought the art of bone setting to Ogwa.Mr Gallowey Omoghabhie, a TBS at Ogwa who has some level of
ducation and therefore was invaluable in obtaining the relevantnformation. Chief Ikpalaba Ukhurebhor who helped to convince
any TBS to give audience to the researchers and therefore enabledhe author to interview the relevant patients and TBS and to viewheir radiographs. Staff of the Department of Geography, Ambroselli University, Ekpoma, for their help in reading the co-ordinates ofgwa in the map. Mr. Benjamin O. Oware, head of research sectionf the National Population Commission, Ikpoba Slope, Benin City,do State, Nigeria. He provided the statistics of National Censusgures and poverty assessment for Ogwa and Edo State. The author
s also very grateful to numerous patients and their relatives andBS seen at Idunmunkpaghan between April 2008 and April 2010s their excellent co-operation made this study possible.
eferences
[1] Carmody DL, Carmody JT. Ways to the centre: an introduction to the worldreligions. 3rd ed. Belmont, CA, USA: Wadsworth Publishing Company; 1989,41–43, 45, 48, 70–120.
[2] Solagberu BA. Long bone fracture treated by traditional bone setters: a studyof patients’ behaviour. Trop Doct 2005;32:106–8.
[3] Puckree T, Mkhize M, Mgobhozi Z, Lin J. African traditional healers: what healthcare professionals need to know. Int J Rehabil Res 2002;25:247–51.
[4] Aries MJ, Joosten H, Wegdam HH, Vander Geest S. Fracture treatment by bonesetters in central Ghana: patients explain their choices and experiences. TropMed Int Health 2007;12:564–74.
[
ology 81 (2012) 2323–2328
[5] Oyebola DD. The Yoruba traditional bone setters and the practice of orthopedicsin a primitive setting in Nigeria. J Trauma 1980;20:312–22.
[6] Thanni LO. Factors influencing patronage of traditional bone setters. West AfrJ Med 2000;19:220–4.
[7] Onuminya JE. The role of traditional bone setters in primary fracture care inNigeria. S Afr Med J 2004;94:652–8.
[8] Lagundoye SB, Olowa P. A basic X-ray service for a rural communityin Southwestern Nigeria 1976–1980. A preliminary report. Diagn Imaging1982;51(3–4):193–7.
[9] Makanjuola D. Trauma in the rural areas of Western Nigeria and the need forbasic radiological services. Diagn Imaging 1982;51(3–4):139–45.
10] Heritage A, editor. World atlas. Millennium ed. London: Dorling KindersleyBook; 1999. p. 132.
11] National Population Commission 2006. The 2006 census priority tables, Abuja,Nigeria, 5th June 2009, SDM/1/S-Z/XVII/II.
12] Onuminya JE, Obekpa PO, Ihezue HC, Ukegbu ND, Onabowale BO. Majoramputations in Nigeria. A plea to educate traditional bone setters. Trop Doct2000;30:133–5.
13] Omololu B, Ogunlade SO, Alonge TO. The complications seen from the treatmentof traditional bone setters. West Afr J Med 2002;21:335–7.
14] Ofiaeli RO. Complications of methods of fracture treatment used by traditionalbone setters. A report of three cases necessitating amputation at Ihiala, Nigeria.Trop Doct 1991;21:182–3.
15] Alonge TO, Dongo AE, Nottridge TE, Omololu AB, Ogunlade SO. Traditionalbone setters in South Western Nigeria – friends or foes? West Afr J Med2004;23:81–4.
16] Garba ES, Deshi PJ. Traditional bone setters. A risk factor in limb amputations.East Afr Med J 1998;75:553–5.
17] Tienyu S. Treatment of fractures and soft tissue injury by integrated method
administrators and practitioners. Geneva: WHO; 1983. p. 221–69.18] Fido M, Fido K. The world’s worst medical mistakes. Canterbury, UK: Seve-
nAorks; 1996. pp. 14–218.