research on severe maternal morbidities and near-misses in brazil: what we have learned
TRANSCRIPT

Research on Severe Maternal Morbidities and
Near-Misses in Brazil: What We Have Learned
Jose Guilherme Cecatti,a Joao Paulo Souza,b Mary Angela Parpinelli,c
Maria Helena de Sousa,d Eliana Amarale
a Full Professor of Obstetrics, Department of Obstetrics and Gynecology, School of Medical Sciences,Universidade Estadual de Campinas (UNICAMP), Campinas SP, Brazil. E-mail: [email protected]
b Coordinator, Intensive Care Unit, Maternity Hospital, Department of Obstetrics and Gynaecology,School of Medical Sciences, UNICAMP, Campinas SP, Brazil
c Assistant Professor of Obstetrics, Department of Obstetrics and Gynaecology, School of MedicalSciences, UNICAMP, Campinas SP, Brazil
d Statistician, Department of Obstetrics and Gynaecology, School of Medical Sciences, UNICAMP,Campinas SP, Brazil
e Associate Professor of Obstetrics, and Director, Obstetrics Unit, Department of Obstetrics andGynaecology, School of Medical Sciences, UNICAMP, Campinas SP, Brazil
Abstract: The occurrence of complications during pregnancy depends less on the degree ofhuman development than differences in the way complications in pregnancy are detected andmanaged. It is the quick diagnosis and correct management that really contribute to the enormousdifferences in maternal mortality ratios between countries and regions. Understanding of thedeterminants of maternal mortality may be improved by studying cases of severe maternalmorbidity. In this paper, various approaches to the concept of severe maternal morbidity andnear-misses are discussed, and the relationship between these and maternal deaths. Although noconsensus has been reached on a strict definition of near-miss or severe maternal morbidity,we show that the definitions used may be tailored to support diverse objectives, includingmonitoring progress, epidemiological surveillance and auditing of health care. We conclude thatthe versatility of the concept, the greater frequency of cases available for study and the possibilityof interviewing the survivors of severe complications all support the value of studying severematernal morbidity to help guide local efforts to reduce maternal mortality. Although this mayalmost be a reality in developed countries, it continues to represent an important and difficultchallenge to overcome in places where its benefits would be most evident. A2007 ReproductiveHealth Matters. All rights reserved.
Keywords: near-miss, severe maternal mortality and morbidity, health surveillance systems, Brazil
ALTHOUGH reducing the number of mater-nal deaths is one of the Millennium Deve-lopment Goals, these deaths constitute
merely the tip of the iceberg of severe mor-bidity related to pregnancy, childbirth and thepuerperium. The extent of all this morbidity isstill unknown, but must be confronted before anyreal improvement in maternal health can in facttake place. The incidence of acute complications
during pregnancy may possibly be similar in bothdeveloped and developing countries; neverthe-less, the differences in how these complicationsare detected and managed may be responsible forthe enormous gap in maternal mortality ratios andin the incidence of long-term sequelae.1
Since the 1990s, a special group of womenwho have survived acute and severe compli-cations of pregnancy and who escaped death by
A 2007 Reproductive Health Matters.All rights reserved.
Reproductive Health Matters 2007;15(30):125–1330968-8080/06 $ – see front matterPII: S0968-8080 (07 )30333-9www.rhm-elsevier.com www.rhmjournal.org.uk
125

JG Cecatti et al / Reproductive Health Matters 2007;15(30):125–133
luck or by receiving timely, appropriate care,have attracted the attention of investigators andpolicy-makers. Their experience is known as a‘‘near-miss’’.2 These women share important char-acteristics with those who die during pregnancy,childbirth or the puerperium, and constitute aproxy model for maternal death. Moreover, study-ing what happened to them is made easier bytheir greater numbers and the possibility ofbeing able to listen to them directly.3–5
Although the concept of near-miss is alreadywell-established, a consensual definition has yetto be adopted, including how the women com-prising this group may be recognised.6–8 Consid-ering the potential of near-misses to contributeto the development of strategies for reducingmaternal mortality, we decided to study differ-ent aspects of them using different approaches.
This paper summarises a series of studies onmaternal morbidity carried out by our researchgroup at the Department of Obstetrics and Gyne-cology, School of Medical Sciences, UniversidadeEstadual de Campinas (UNICAMP) in Campinas,Brazil, and discusses their findings and signifi-cance. Over the last 20 years, our group hasbeen working in the field of maternal mortalityand more recently maternal near-misses almostentirely with local resources. There is an unfor-tunate negative belief as regards most researchthat, after a study has been performed, practi-cally nothing will actually change in the set-ting where it was carried out. This is exactlywhat we do not want to happen with our data.We took up the challenge of writing a more con-ceptual paper outlining our experience, in orderto share with other research groups from thedeveloping world what can be done locally withlimited resources. The paper covers the definitionof a near-miss, the scoring system we developedfor severe maternal morbidity, population-basedstudies and surveys that we undertook, informa-tion systems we set up in health and monitor-ing, and what we have learned from listeningto women’s experiences. The papers reporting thisresearch have been or are in process of being pub-lished elsewhere and are referenced in this paper.
DefinitionsFollowing a long history of concern about andresearch on the subject of maternal mortality inBrazil, we recently began to intensify our interest
126
in near-misses by carrying out a systematic lit-erature review of the published data on theincidence of near-misses and the different oper-ational definitions of them adopted in the stud-ies.9 We found that the majority (57%) of studieson the subject had adopted definitions relatedto the complexity of management of the cases(i.e. admission to intensive care units, need forhysterectomy or transfusions of blood deriva-tives), while 24% defined them according to thepresence of certain clinical conditions (i.e. severepre-eclampsia or uterine rupture), 15% accordingto the presence of organ failure (i.e. respiratory orrenal failure, coma or shock) and 3% were basedon a mixture of criteria (i.e. severe maternal mor-bidity score). In the studies reviewed, the near-miss ratio reported varied from 0.3/1,000 to 101.7/1,000 deliveries and the case-fatality ratio variedfrom 2:1 to 223:1. The review also found a ten-dency towards a greater in-hospital incidence ofcases of near-miss in the studies in developingcountries than in developed countries.9
Evaluating the definitions and the scoringsystem for severe maternal morbidityOur institution is a tertiary referral centre inthe city of Campinas, Sao Paulo state, one ofthe most developed regions of Brazil. Approx-imately 3,000 deliveries are carried out annuallythere. Although a good part of the cases attendedhere are considered high risk, the occurrenceof maternal death in this centre is infrequent. Ifwe were to use only cases of maternal death forauditing the quality of obstetric care, it wouldprobably be a fairly ineffective approach becauseof the low rate of maternal death. Likewise, ser-vices that deal with few obstetric cases or lesscomplex cases find it difficult to use only cases ofmaternal death to evaluate the quality of obstetriccare offered and the difficulties faced by womenin obtaining maternity care. A long period of timewould be required to accumulate a reasonablenumber of cases and by then it would be too latefor a good number of women. Hence, we felt it wasvaluable to study cases of severe maternal morbid-ity and near-misses, to see what they would teachus about dealing with obstetric complications.
To evaluate the applicability of the differentconcepts of severe maternal morbidity and obstet-ric near-miss in hospitals, we surveyed cases ofsevere maternal morbidity in our hospital over a
JG Cecatti et al / Reproductive Health Matters 2007;15(30):125–133
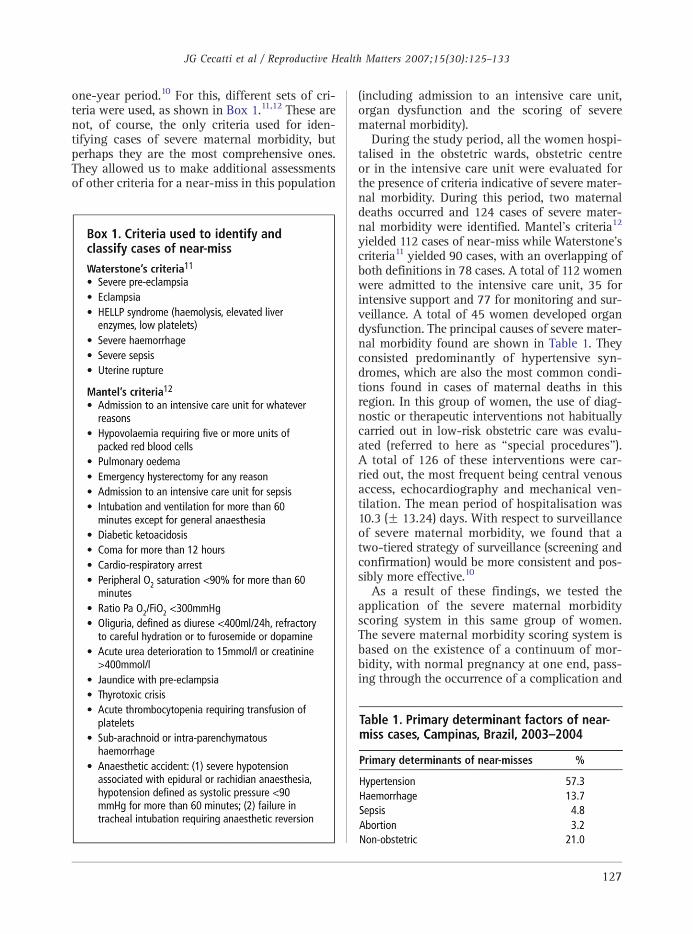
one-year period.10 For this, different sets of cri-teria were used, as shown in Box 1.11,12 These arenot, of course, the only criteria used for iden-tifying cases of severe maternal morbidity, butperhaps they are the most comprehensive ones.They allowed us to make additional assessmentsof other criteria for a near-miss in this population
(including admission to an intensive care unit,organ dysfunction and the scoring of severematernal morbidity).
During the study period, all the women hospi-talised in the obstetric wards, obstetric centreor in the intensive care unit were evaluated forthe presence of criteria indicative of severe mater-nal morbidity. During this period, two maternaldeaths occurred and 124 cases of severe mater-nal morbidity were identified. Mantel’s criteria12
yielded 112 cases of near-miss while Waterstone’scriteria11 yielded 90 cases, with an overlapping ofboth definitions in 78 cases. A total of 112 womenwere admitted to the intensive care unit, 35 forintensive support and 77 for monitoring and sur-veillance. A total of 45 women developed organdysfunction. The principal causes of severe mater-nal morbidity found are shown in Table 1. Theyconsisted predominantly of hypertensive syn-dromes, which are also the most common condi-tions found in cases of maternal deaths in thisregion. In this group of women, the use of diag-nostic or therapeutic interventions not habituallycarried out in low-risk obstetric care was evalu-ated (referred to here as ‘‘special procedures’’).A total of 126 of these interventions were car-ried out, the most frequent being central venousaccess, echocardiography and mechanical ven-tilation. The mean period of hospitalisation was10.3 (F 13.24) days. With respect to surveillanceof severe maternal morbidity, we found that atwo-tiered strategy of surveillance (screening andconfirmation) would be more consistent and pos-sibly more effective.10
As a result of these findings, we tested theapplication of the severe maternal morbidityscoring system in this same group of women.The severe maternal morbidity scoring system isbased on the existence of a continuum of mor-bidity, with normal pregnancy at one end, pass-ing through the occurrence of a complication and
127

* There might be some concern about the use of multiple
hospital-based studies as a proxy for a population-based
study because, according to Fortney and Smith,18 they
include only women who sought treatment. However, in
the specific situation of Campinas, the ‘‘untreated’’ segment
of the target population was considered to be irrelevant.
JG Cecatti et al / Reproductive Health Matters 2007;15(30):125–133
different degrees of severity with maternal deathat the other end.13 Initially, we sought to iden-tify the greatest possible number of cases ofsevere maternal morbidity by using a wide rangeof criteria. Next, a specific scoring system wasapplied in each case, depending on the presenceor absence of factors of severity (organ failure,admission to intensive care, transfusion of morethan three blood derivatives, prolonged intuba-tion and major surgical interventions other thancaesarean section). This system permits identifi-cation of the most severe cases, and once the scoreis applied to the survivors of severematernalmor-bidity, it is possible to identify cases of near-miss.
According to the scoring system as applied toour sample, 20 cases were classified as near-missand 104 cases as other severe maternal morbidity.Considering duration of hospitalisation and theuse of special procedures, we observed that thegroup of near-miss women required more com-plex care over a longer period of time comparedto women in the group of other severe mor-bidities (pb0.05). The mean number of specialprocedures carried out in the group of womenwith near-misses was 3.75 (F2.34) per case,whereas in the group of other severe morbid-ities, the number was 0.38 (F0.83). The meanduration of hospitalisation in near-miss caseswas 24.2 days (F28.1), whereas in the groupof other severe morbidities, this period was7.6 days (F4.3). Among the cases of near-miss,there was a predominance of cases of haemor-rhage, while in cases of other severe morbidities,hypertensive complications predominated. Thisinstitutional data does not necessarily reflectthe national figures on maternal morbidity andmortality. We could hypothesise that hyper-tensive complications are more prevalent andheterogeneous in terms of severity and that theyare more effectively managed in a tertiary facil-ity. The implications for practice of haemorrhagebeing the main determinant cause of a near-miss,taking into account that it is generally identifiedas having the most complex complications,are that it demands the prompt availability ofsurgical, anaesthetic and haemotherapeutic pro-cedures. This study provided additional valida-tion of the severe maternal morbidity scoringsystem, and we concluded that the same scoringsystem could be used to objectively describe andidentify the most extreme cases of severe maternalmorbidity (near-misses).14,15
128
The use of different sets of criteria for iden-tifying cases of severe maternal morbidity and/or near-misses worldwide is a problem that stillneeds to be resolved, especially for purposes ofcomparing data. It was not our intention to setunique criteria, but rather to show our experi-ence in testing different criteria in the field. Acommon definition and standard procedures forthe identification of severe maternal morbidityand near-miss cases should probably be addressedin the near future. The World Health Organizationand other international health agencies could playa major role in this challenge.
Population-based study of severematernal morbidityAfter investigating the concept of severe mater-nal morbidity and near-miss in a hospital envi-ronment, we carried out a population-based studyof the occurrence of severe maternal morbidityand maternal and perinatal mortality in the cityof Campinas. Hospital coverage for obstetric casesin the region is almost 100%, with only 0.4% ofhome deliveries being reported in 1996.16 The fewcases of deliveries taking place outside the hospi-tal are due to the current trend of home deliveryamong women with a high socio-economic statusand to deliveries occurring on the way to hospital.In both cases, maternal and perinatal complica-tion rates are not very likely to be significant.*
The cases of interest were identified by pro-spective surveillance carried out in all the mater-nity hospitals (public and private) in the cityover a three-month period. The objective was toidentify all the cases of maternal and perinataldeath and severe maternal morbidity. The casesof maternal morbidity were identified in accor-dance with a set of criteria similar to that used inthe hospital-based study. All the cases identifiedwere submitted to clinical audit by the municipaland regional Maternal Mortality Committees.17
A total of 158 adverse perinatal events wereidentified. In this period, 4,491 liveborn infantswere delivered and there were 32 fetal deaths,or 34.9 fetal deaths per 1,000 deliveries. Four

JG Cecatti et al / Reproductive Health Matters 2007;15(30):125–133
maternal deaths (maternal mortality ratio 89 per100,000 live births) and 95 cases of severe mater-nal morbidity (21.2 per 1,000 live births) occurred.The case-fatality ratio was 24:1. Hypertensivecomplications were responsible for 57.8% ofcases of severe maternal morbidity, followed infrequency by cases of post-partum haemorrhage.The audit process revealed that provision ofappropriate care was delayed in 54 cases (34%).Of these 54 cases, in 32 (59%), the delay occurredin initiating adequate treatment despite the factthat the woman had already reached a health careservice; in 23 cases (43%), the delay occurred inseeking care; and in only 7 cases (13%) was thedelay caused by difficulty in obtaining access tohealth services.17 The majority of delays, then,were due to a physician’s decisions as regardsboth time and appropriateness of care. Duringthe audit process specifically for the cases ofsevere maternal morbidity, it was found that thedelays were mainly due to lack of timely use ofmagnesium sulphate for pre-eclampsia, manage-ment of pre-eclampsia and hypertension, adher-ence to antenatal care guidelines, managementof obstetric haemorrhage or use of prophylaxisfor post-partum haemorrhage. We recommendedthat these topics become a priority part of thecontent of refresher courses for professionals andalso that the institutions involved should checkwhether any constraints existed that were causingdelays in or failure to implement best practice.17
It is important to note that in this proxypopulation-based prospective study, the causes ofsevere maternal morbidity were very similar tothose obtained in the previously described insti-tutional study.10 This is relevant as it indicatesthat it is possible to identify interventions thatcould be carried out during antenatal care19,20
or delivery20 to try to reduce the risk of maternaldeath from specific, identified problems.
The main conclusions of this study werethat, despite the large number of cases, investi-gation of the cases of severe maternal morbiditywas feasible. Moreover, the process of audit-ing these cases led to increased experience in awide spectrum of causes of maternal morbidity,which also motivated the members of the Mater-nal Mortality Committees to tackle determinantsof maternal death. Hypertensive complications andpost-partum haemorrhage were highlighted as pri-ority topics for training. Concrete recommenda-tions for changing the practice of physicians in
order to address these issues were to use auditand feedback on proper evidence based interven-tions, the opinions of local leaders on when andhow to implement such evidence based interven-tions and the use of reminders of best practices.21
Information systems in health andmonitoring of severe maternal morbidityIn several countries, much of the informationon health is routinely collected by governmentaland/or non-governmental organisations. Theuse of information on health stored in publicinformation systems may be useful for the con-tinuous and prospective monitoring of severematernal morbidity. If these systems operatedautomatically and concurrently with the careprovided (using, for example, the hospital costmanagement systems) a mechanism of local orin-hospital alert could be established so that adifferentiated support system would trigger ther-apeutic or preventive interventions, in each caseautomatically indicated by the system.22
In the case of maternal morbidity, the deve-lopment of such a system and mechanisms ofalert constitute an innovation designed to stopthe progression of a woman through the contin-uum of severe morbidity and to prevent a maternaldeath. However, very few countries systemati-cally use this approach.23,24 In Brazil, one of theprincipal public sources of information on healthis the Ministry of Health. In this context, we car-ried out a study25 with the aim of identifying themedical records of those women with conditionssuggestive of severe maternal morbidity, usingthe Brazilian Hospital Information System (HIS).The criteria shown in Box 1 have been adapted topermit recognition of the records stored in theHospital Information System. In addition to iden-tifying the records, we also attempted to describethe diagnoses and the procedures used, withthe aim of identifying factors associated withmaternal death. The records of women hospital-ised during pregnancy, delivery or in the puer-perium in the 27 Brazilian state capitals in2002 were analysed. The records of the womenwho had at least one of the criteria that we hadadopted as defining severe maternal morbiditywere selected. The records of 32,379 women withat least one factor suggestive of severe mater-nal morbidity were identified, as well as 154maternal deaths (case-fatality ratio 210:1). The
129

JG Cecatti et al / Reproductive Health Matters 2007;15(30):125–133
consolidated ratio of severe maternal morbid-ity observed was 44.3/1,000 liveborn infants.Despite several limitations, principally the needfor a structured information system, the per-spective of routinely using the information col-lected was found to be promising25 for settingup an automatic mechanism of alert. However,implementation of this mechanism first requiresthe development of agile local information sys-tems to make it viable.
Estimating maternal morbidity bypopulation surveysPopulation surveys and demographic and healthsurveys may constitute good sources of informa-tion on maternal morbidity, particularly in placeswhere integrated systems of epidemiological infor-mation have not yet been implemented.18,26 Weanalysed the information obtained from demo-graphic and health surveys carried out in LatinAmerica and the Caribbean on maternal mor-bidity. The databases of seven population sur-veys carried out in the 1990s in Bolivia, Brazil,Colombia, Dominican Republic, Guatemala, Nica-ragua and Peru contained indirect informationon maternal morbidity identified through com-plications reported as associated with childbirth.The rate of complications reported by the womensurveyed was very high, 20–40% of all deliveriesin the majority of the countries. We concludedthat the majority of these demographic andhealth surveys involving questions on maternalmorbidity resulted in over-estimation of the occur-rence of morbidity, possibly because they werenot adequately validated.27
Using this same approach, we recently eval-uated the situation in Brazil by geographicalregion from data in a 1996 demographic andhealth survey. This showed a varied panoramaof reported complications, ranging from around15% in the state of Sao Paulo to as high as 23%in the northern part of the country. These vari-ations were in line with the degree of economicand human development of the different regionsof the country, with complications being sig-nificantly greater in the east central, northeast,north and west central parts of the country, theleast developed areas of Brazil.28 This findinghas stimulated our decision to continue inves-tigating the regional distribution of occurrencesof severe maternal morbidity, probably through
130
a process of geographical referencing, takinginto consideration the geographic location ofthe occurrences and the local demographic char-acteristics, as well as the characteristics of thequantity and quality of maternal health servicesavailable. This currently represents a challengeto both scientists and health planners, if mea-sures specifically aimed at combating local andregional difficulties are to be recommended andimplemented with the clear objective of avoid-ing delays and improving maternal health.
To further evaluate the question of the validityof questionnaires on morbidity, we carried outa systematic review on the subject. This was ourfirst attempt to summarise the findings of vari-ous studies on the validation of questionnaireson severe maternal morbidity in developingcountries. We found that information on theoccurrence of eclampsia and other hypertensivecomplications in the same seven surveys fromLatin American and the Caribbean mentionedearlier was considered satisfactorily accurate infour out of seven studies, dystocia and infec-tion in only two, and the questions dealing withhaemorrhagic complications were consideredsatisfactory in only one. Another finding of thisreview was that, when the true prevalence ofthe condition investigated is low (b5%), studiesfrequently over-estimate prevalence.29
We therefore suggest that questionnaires onsevere maternal morbidity included in demo-graphic and health surveys should be previouslyvalidated and, if necessary, correction factors deve-loped to adjust for the estimates obtained.29 In viewof these findings, we developed a questionnaire forthe evaluation of the occurrence of severe mater-nal morbidity in Portuguese. This questionnaire iscurrently being validated and the correction fac-tors obtainedmay be used to interpret future popu-lation surveys that adopt this instrument.
Listening to women’s experienceOne of the principal advantages of case studiesof near-misses is the possibility of hearing theexperience of the women directly. Women whohave survived potentially fatal complicationsin pregnancy or the puerperium are believed tobe able to adequately report the obstacles anddelays they had to face to assure their survival.30
Considering these points, we designed a qualita-tive research study to acquire knowledge on the

JG Cecatti et al / Reproductive Health Matters 2007;15(30):125–133
experience of women who have survived acuteand severe complications during pregnancy andthe puerperium. Our preliminary findings showthat there were difficulties and obstacles thatthe women had to overcome to receive adequatecare when the complication developed, includ-ing problems related to the quality of primarylevel care, lack of local resources, poverty andcorrespondent social disadvantages, and delaysin the referral process. This study is still in pro-cess, but its findings will provide importantinsights into the causes of maternal morbidityin our region. Transferring knowledge comingfrom research into practice is a difficult task, espe-cially in developing country settings. However, thelessons already learnt from women indicate theneed for improvement of local primary level carein identifying and referring complications duringpregnancy so that they can be adequately andcomprehensively managed in time.
DiscussionNo consensus has yet been reached on howbest to recognise cases of severe maternal mor-bidity and obstetric near-miss. Although lack ofstandardisation in the definition and evaluationmethods represents an aspect that still requiresimprovement, since this deficiency hampers com-parison between services and over time, thediversity of applications of the concept repre-sents its versatility. As described in the previoussections, the definition of morbidity or near-missmay be tailored to each purpose or to each popu-lation of interest, and this facilitates its use atthe different levels for action and planning.
For a long time, reducing the number of com-plications occurring during pregnancy was theprincipal objective of many programmes aimedat reducing maternal mortality.31 Nevertheless,the majority of acute, severe obstetric compli-cations are considered difficult to predict andseldom possible to prevent, which may explain,in part, the failure of a good number of theseprogrammes.32 On the other hand, appropriatetreatment for the majority of these complicationsis known and timely treatment may avoid theoccurrence of a great number of maternal deaths.1
In this context, the study of severe maternal mor-bidity and cases of near-miss may contributetowards improving strategies for combating acutecomplications of pregnancy, thus contributing
towards reducing the number of deaths. How-ever, probably the main reason why more progressin reducing maternal mortality has not been madeis not the lack of knowledge of what the compli-cations are or what to do about them, but ratherthe organisation, delivery and utilisation of ser-vices. This appears to include significant regionaldifferences, as found in Brazil. For this reason,research on these factors should be repeated, when-ever possible, in different contexts to determine thelocal characteristics upon which the adoption ofappropriate interventions depends. In fact, up tothe present moment, no large population-basedstudies that deal directly with severe maternalmorbidity (near-miss) have been carried out. Inour view, this justifies performing a large, pro-spective, international, multicentre study, prefer-ably in developing countries in which maternalmortality is high, to learn more about the con-dition and the factors associated with it.
A system of epidemiological surveillance basedon the early identification of cases of severe mater-nal morbidity would permit a more adequate levelof monitoring and care, stopping the progres-sion of women through the continuum of mor-bidity and preventing the occurrence of avoidabledeaths.4 On the other hand, carrying out auditsof the care provided in cases of severe maternalmorbidity may permit a local diagnosis of thecauses of delay either in seeking, gaining accessto or receiving adequate care. This type of auditis being used more and more frequently as acomplement to the reviews of maternal deathand may help support the planning of actionsadapted for each situation identified.33
ConclusionsThe study of severe maternal morbidity may con-tribute significantly to the formulation of strat-egies to reduce maternal mortality. The versatilityof the concept, together with the greater fre-quency of cases and the possibility of directlyinterviewing the survivors of severe compli-cations, allows local actions to be implementedwithin a global perspective to improve maternalhealth. Recommendations for changing practicewould be the implementation of multi-facetedstrategies based on audit and feedback.
AcknowledgementsWe would like to acknowledge all the people inour institution who have participated in all stages
131
JG Cecatti et al / Reproductive Health Matters 2007;15(30):125–133
of our research on maternal mortality and mor-bidity, including sponsors, researchers, inter-viewers, statisticians, physicians, social workers,research assistants and the women who agreed
132
References1. Paxton A, Maine D, Freedman L,
et al. The evidence for emergencyobstetric care. InternationalJournal of Gynecology andObstetrics 2005;88(2):181–93.
2. Stones W, Lim W, Al-Azzawi F,et al. An investigation ofmaternal morbidity withidentification of life-threatening‘‘near miss’’ episodes. HealthTrends 1991;23(1):13–15.
3. Berg CJ, Bruce FC, CallaghanWM. From mortality tomorbidity: the challenge of thetwenty-first century. Journal ofAmerican Medical Women’sAssociation 2002;57(3):173–74.
4. Pattinson RC, Hall M. Nearmisses: a useful adjunct tomaternal death enquiries. BritishMedical Bulletin 2003;67:231–43.
5. Filippi V, Brugha R, Browne E,et al. Obstetric audit inresource-poor settings: lessonsfrom a multi-country projectauditing ‘‘near miss’’ obstetricalemergencies. Health Policy andPlanning 2004;19(1):57–66.
6. Filippi V, Alihonou E,Mukantaganda S, et al. Nearmisses: maternal morbidityand mortality. Lancet 1998;351(9096):145–46.
7. Nashef SA. What is a near miss?Lancet 2003;361(9352):180–81.
8. Say L, Pattinson RC, GulmezogluAM. WHO systematic review ofmaternalmorbidityandmortality:the prevalence of severe acutematernal morbidity (near miss).Reproductive Health 2004;1(1):3.
9. Souza JP, Cecatti JG, ParpinelliMA, et al. [Systematic review ofnear miss maternal morbidity].[In Portuguese] Cadernos deSaude Publica 2006;22(2):255–64.
10. Souza JP, Cecatti JG, ParpinelliMA, et al. Appropriate criteria
for identificatiomaternal morbicare facilities: astudy. BMC PreChildbirth 2007
11. Waterstone M, BC. Incidence ansevere obstetriccase-control stu2001;322(7294)
12. Mantel GD, BucH, et al. Severemorbidity: a pildefinition for aBritish Journaland Gynaecolog985–90.
13. Geller SE, Rosenet al. A scoringnear-miss mateduring pregnanClinical Epidem57(7):716–20.
14. Souza JP, Cecatnear-miss matescoring systemclinical setting iof Clinical Epid58(9):962.
15. Souza JP, CecattMA. [Factors assthe severity of mmorbidity for theof near miss]. [InRevista Brasileire Obstetrıcia 200
16. Brazil. [NationaHealth Survey 1Portuguese] ORCMeasure DHS S2006. At: bwwwcom/pubs/pub_ID=119&ctry_idavailableN. Acc13 August 2007
17. Amaral E, Souzet al. A populatsurveillance stumaternal morbi
to share their experiences. Special recognitiongoes to Anibal Faundes, who motivated our inter-est in this subject and its potential for improvingwomen’s health in our country.
n of near-missdity in tertiarycross sectional
gnancy &. (In press)ewley S, Wolfe
d predictors ofmorbidity:dy. BMJ:1089–94.hmann E, Reesacute maternalot study of anear-miss.of Obstetricsy 1998;105(9):
berg D, Cox S,system identifiedrnal morbiditycy. Journal ofiology 2004;
ti JG. Thernal morbiditywas tested in an Brazil. Journalemiology 2005;
i JG, Parpinelliociated withaternalcharacterizationPortuguese]
a de Ginecologia5;27(4):197–203.l Demographic996]. [InMacro:
TAT compiler,.measuredhs.details.cfm?=49&SrchTp=essed.a JP, Surita FG,ion-baseddy on severedity (near-miss)
in Campinas, Brazil: TheVigimoma Project. XVIII FIGOWorld Congress of Gynecologyand Obstetrics, Kuala Lumpur,2006. Abstract 2:96.
18. Fortney JA, Smith JB. Measuringmaternal morbidity. In: Berer M,Ravindran TKS, editors. SafeMotherhood Initiatives: CriticalIssues. London7 ReproductiveHealth Matters, 2000. p.43–50.
19. Carroli G, Rooney C, Villar J.How effective is antenatal care inpreventing maternal mortalityand serious morbidity? Anoverview of the evidence.Paediatric and PerinatalEpidemiology 2001;15(Suppl.1):1–42.
20. Campbell OM, Graham WJ,Lancet Maternal SurvivalSeries steering group. Strategiesfor reducing maternalmortality: getting on withwhat works. Lancet 2006;368(9546):1284–99.
21. Chaillet N, Dube E, Dugas M,et al. Evidence-based strategiesfor implementing guidelines inobstetrics: a systematic review.Obstetrics & Gynecology 2006;108(5):1234–45.
22. Sousa MH, Cecatti JG, HardyEE, et al. [Health informationsystems and surveillance ofsevere maternal morbidity andmaternal mortality]. [InPortuguese]. Revista Brasileirade Saude Materno Infantil2006;6(2):161–68.
23. Canada, Minister of PublicWorks and Government Services.Health Canada: special report onmaternal mortality and severemorbidity in Canada - enhancedsurveillance: the path toprevention. Ottawa, 2004.
24. US Agency for InternationalDevelopment. Developing and

133
implementing a hospital-basedsurveillance system for maternaland newborn health. At: bwww.mnh.jhpiego.org/global/dvlsrvsys.aspN. Accessed15 May 2005.
25. Sousa MH, Cecatti JG, Hardy EE.Use of the health informationsystems on severe maternalmorbidity (near miss) andmaternal mortality. At: bhttp://libdigi.unicamp.br/document/?code=vtls000386164N.Accessed 13 August 2007.
26. Stewart MK, Stanton CK, FestinM, et al. Issues in measuringmaternal morbidity: lessonsfrom the Philippines SafeMotherhood Survey Project.Studies in Family Planning1996;27(1):29–35.
27. Souza JP, Parpinelli MA, AmaralE, et al. Obstetric care andsevere pregnancy complicationsin Latin America and Caribbean:an analysis of informationfrom demographic and healthsurveys. Pan American Journalof Public Health 2007;21(6):396–401.
28. Souza JP, Sousa MH, ParpinelliMA, et al. Self-reported maternalmorbidity and associated factorsamong Brazilian women.(Submitted 2007)
29. Souza JP, Parpinelli MA, AmaralE, et al. Population surveysusing validated questionnairesprovided useful information onthe prevalence of maternalmorbidities. Journal of ClinicalEpidemiology 2007. (In press)
30. Weeks A, Lavender T, NazziwaE, et al. Personal accountsof ‘‘near-miss’’ maternalmortalities in Kampala, Uganda.BJOG 2005;112(9):1302–07.
31. Australia. Queensland Councilon Obstetric and PaediatricMorbidity and Mortality. MaterPerinatal Epidemiology Unit,Mater Hospitals Maternaland Perinatal Audit. Guidelinesfor Queensland hospitals.Brisbane, 2001.
32. Rosenfield A, Maine D, FreedmanL.MeetingMDG-5: an impossibledream? Lancet 2006;368(9542):1133–35.
33. Penney G, Brace V. Near missaudit in obstetrics. CurrentOpinion in Obstetrics &Gynecology 2007;19(2):145–50.
ResumeL’apparition de complications pendant la grossessedepend moins du degre de developpement humainque des differences dans la detection et la gestionde ces cas. Ce sont le diagnostic rapide et la gestionadaptee qui contribuent reellement aux enormesdifferences entre le taux dematernite maternelle depays et regions. L’etude des cas de grave morbiditematernelle peut aider a comprendre les facteursde la mortalite maternelle. Cet article etudieplusieurs definitions du concept de grave morbiditematernelle et d’T echappee belle r, et la relationentre ces cas et les deces maternels. Meme s’iln’y a pas de consensus sur une definition strictedes T echappees belles r ou de la morbiditematernelle grave, nousmontrons que les definitionsutilisees peuvent etre concues de maniere asoutenir differents objectifs, notamment le suivides progres, la surveillance epidemiologique etle controle des soins de sante. Nous en concluonsque la versatilite du concept, la frequence accruede cas disponibles pour l’etude et la possibilited’interroger les patientes ayant survecu sont autantd’arguments en faveur de l’etude de la morbiditematernelle grave pour guider les activites localesde reduction de la mortalite maternelle. Si c’estpresque une realite dans les pays developpes,cela demeure un defi difficile a relever la ou sesavantages seraient les plus evidents.
ResumenLapresencia de complicaciones durante el embarazodependemenos del grado de desarrollo humano quede las diferencias en la forma en que se detectan ymanejan. Un diagnostico rapido ymanejo correctocontribuyen a las enormes diferencias en razonesde mortalidad materna entre paıses y regiones. Elestudio de casos de morbilidad materna graveayuda a entender mejor los determinantes de lamortalidadmaterna. Este artıculo trata de diversosenfoques respecto al concepto de la morbilidadmaterna severa y casos que casi conducen a lamuerte, ası como la relacion entre estos y muertesmaternas. Aunque no se ha establecido unadefinicion estricta dedichos casos o de lamorbilidadmaterna severa, se muestra que las definicionesutilizadas pueden adaptarse para apoyar diversosobjetivos: el monitoreo de los avances, la vigilanciaepidemiologica y la auditorıa de los servicios desalud. Concluimos que la versatilidad del concepto,el aumento en casos disponibles para el estudio yla posibilidad de entrevistar a las sobrevivientes,apoyan el valor de estudiar la morbilidad gravepara guiar los esfuerzos locales por disminuirla mortalidad materna. Aunque esto es casi unarealidad en los paıses desarrollados, continuasiendo un gran reto difıcil de vencer en lugaresdonde sus beneficios serıan mas evidentes.
JG Cecatti et al / Reproductive Health Matters 2007;15(30):125–133