community organizing participatory action research family case study
TRANSCRIPT

College ofNursing Education
3rd Floor, DPT Building Matina Campus, Davao City
A Family Case StudyPresentedTo the
College of Nursing
In Partial Fulfillment of the Requirements in Community Organizing Participatory Action
Research Family Case Study
Submitted to:Ms. Arlene D. Layupan, RNMr. Henrries Dan Tulas, RNMr. Ronald Allan Ramo, RN
Submitted by:Elorza, Shekinah L.
1
September 2013
T A B L E O F C O N T E N T S
I.TITLE
PAGE..........................................................
..............................................1
II.TABLE OF
CONTENTS......................................................
...............................2-3
III.ACKNOWLEDGEMENT...........................................
........................................4
IV.INTRODUCTION...............................................
...............................................5-6
V.OBJECTIVES of the
CASE..........................................................
....................7
VI. IDENTIFICATION OF THE
CASE..........................................................
.........8
2
VII.FAMILY
BACKGROUND....................................................
............................9-10
VIII.SOCIO- ECONOMIC
BACKGROUND....................................................
.......10-11
IX.FAMILY MEDICAL and HEALTH
HISTORY...................................................11-
13
X.GENOGRAM....................................................
..............................................14-15
XI.FAMILY
APGAR.........................................................
.................................16-18
XIII.FAMILYCOPING
INDEX.........................................................
...................19-27
XIV.NURSINGTHEORY.............................................
.......................................27-29
XV. MANAGEMENT
A.MEDICAL
MANAGEMENT....................................................
................................................29-38
B.NURSING MANAGEMENT
3
B.1 Problem List (Maslow’s
Hierarchy)....................................................
.39-41
B.2 Problem Identification (Health Threat/ Deficit/
Foreseeable Crisis)...42-44
B.3Family Nursing Care
Plan..........................................................
..........45-55
B.4Health Teachings (Three Levels of
Prevention)..................................56-59
XVI.
SUMMARY.......................................................
.............................................59-60
XVII.IMPLICATION..............................................
.................................................60-62
XVIII.HEALTH
UPDATES.......................................................
......................................................62-65
XIX.REFERENCES................................................
......................................66
4

ACKNOWLEDGEMENT
I, Shekinah L. Elorza, BSN IV student would like to
express my heartfelt gratitude as a fourth year nursing
researcher to the following people who extend much effort for
their professional assistance and direction.
5
To Mr. Ronald Allan Ramo, RN, MAN, Miss Analyn Salamero,
RN, MN, Miss Arlene Layupan, RN, MAN and Mr. Henrries Dan
Tulas, RN, MAN for their valuable guidance and help during the
entire community exposure.
To Dean Ofelia C. Lariego, RN, MAN for allowing us to
have our exposure and giving us the chance to improve our
knowledge and skills in Community Organizing Participatory
Action Research.
I would like to extend my sincere appreciation to my dear
parents, my beloved whole family for their unstoppable
financial support and for unending prayers to keep us safe
during the community exposure.
To the Brgy. Captain Robert E. Olanolan, for permitting
us to conduct the community exposure in the site selected.
To all residents who participated in all our activities
and willingly cooperated for community’s changes from their
identified problem.
And finally, the researcher would like to thank our
Almighty God for His guidance, wisdom, protection during our
activities and difficulties in going to the community with His
never ending support.
6
INTRODUCTION
Diabetes is a chronic disease, which occurs when the
pancreas does not produce enough insulin, or when the body
cannot effectively use the insulin it produces. This leads to
an increased concentration of glucose in the blood
(hyperglycaemia). Type 1 diabetes (previously known as
insulin-dependent or childhood-onset diabetes) is
characterized by a lack of insulin production. Type 2 diabetes
(formerly called non-insulin-dependent or adult-onset
diabetes) is caused by the body’s ineffective use of insulin.
It often results from excess body weight and physical
inactivity. Gestational diabetes is hyperglycaemia that is
first recognized during pregnancy.
Among U.S. residents ages 65 years and older, 10.9 million,
or 26.9 percent, had diabetes in 2010. About 215,000 people
younger than 20 years had diabetes—type 1 or type 2—in the
United States in 2010. About 1.9 million people ages 20 years
or older were newly diagnosed with diabetes in 2010 in the
United States. In 2005–2008, based on fasting glucose or
hemoglobin A1C (A1C) levels, 35 percent of U.S. adults ages 20
years or older had prediabetes—50 percent of adults ages 65
years or older. Applying this percentage to the entire U.S.
population in 2010 yields an estimated 79 million American
adults ages 20 years or older with prediabetes (Centers for
Disease Control and Prevention, 2012).
7
As of 2010, 25.8 million people—8.3% of the population—
have diabetes; 1.9 million new cases of diabetes were
diagnosed in people aged 20 years or older in 2010. Among
Americans aged 20 years or younger, about one-quarter of 1%
(215,000 people) have diabetes. Among Americans aged 20 years
or older, 11.3% (25.6 million people) have diabetes. The
prevalence of diabetes is greater among older people. Among
Americans aged 65 years or older, 26.9% (10.9 million people)
have diabetes (Centers for Disease Control and Prevention,
2012).
The estimated economic cost of diabetes in 2007 was $174
billion. Of this amount, $116 billion was due to direct
medical costs and $58 billion due to indirect costs such as
lost workdays, restricted activity, and disability due to
diabetes. People with diagnosed diabetes incur average
expenditures of $11,744 per year, of which $6,649 is
attributed to diabetes. People with diagnosed diabetes, on
average, have medical expenditures that are approximately 2.3
times higher than what expenditures would be in the absence of
diabetes. Approximately $1 of $5 health care dollars in the
United States is spent caring for someone with diagnosed
diabetes, while approximately $1 of $10 health care dollars is
attributed to diabetes (Centers for Disease Control and
Prevention, 2012).
I chose Ms. X’s case because her case is one of the most
common disease worldwide afflicting humans, which is Type II
Diabetes Mellitus. It is known as sixth leading cause of death
in the Philippines, according to the World Health Rankings. It
may lead to cardiovascular diseases such as stroke, heart
disease, hypertension, blindness and eye problems, kidney
8
disease, nervous system disease, dental disease, amputations
which are the leading causes of death among Filipinos. It is
actually the leading cause of kidney failure, nontraumatic
lower-limb amputations, and new cases of blindness among
adults in the United States and the major cause of heart
disease and stroke.
Age, family history, physical inactivity, unhealthy diet,
lifestyle nowadays is one of the major predisposing factors of
the condition. These lifestyle factors include high sugar
intake, excessive carbohydrate/calorie intake, and lack of
physical exercise.
9
OBJECTIVES OF THE CASE
General Objectives:
After 12 days of span of nursing care, nursing students and
the assigned family would be able to:
Determine the level of cognition in the determination and
prioritization of problems that exist in the community.
Dvelop the skill of intervention prompt to the social
health care problem in accordance with its
appropriateness and effectiveness.
Provide services and facilitate for the better and
appropriate solutions present in a particular community.
Specific Objectives:
After 12 days of span of nursing care, nursing students and
the assigned family would be able to:
1. Apply knowledge and skills on how to give health
education to the community in relation to their
identified problem;
2. Discuss briefly and explain the etiology of prioritized
problem, its causes and effects and ways on how to
eradicate or just prevent it;
3. Determine the family’s APGAR score and family coping
index in assessing the functioning and potential areas of
family strength and resources;
4. Established a nursing care plan which would be beneficial
to the family, as well as to the community;
10
5. Formulate a clear and specified plan of action to give
solutions to the existing health problems identified
within the community;
6. Relate existing health problems with different nursing
theories;
7. Provide health updates with the identified health problem
within the family; and
8. Give summary, evaluation to the family with implication
to the study.
IDENTIFICATION OF THE CASE
Code Name: Mrs. X
Nationality: Filipino
Religion: Roman Catholic
Address: Pursok 6-A, Barangay 76-A, Bucana, Davao City
Age: 53 years old
Birthday: July 02, 1960
Civil Status: Married
Menarche: 11 years old
Parity: 4
11
Gravida: 4
Abortion: 0
Menstrual Cycle: Menopause but her menstrual cycle before is
regular
Diagnosis: Diabetes Mellitus (37 years old), on 1997at Davao
Doctor’s Hospital
Date study Begun: August 30, 2013
Date study Ended: September 13, 2013
FAMILY BACKGROUND
The X family which is a nuclear type of family is the
chosen family to be the subject for my case study. They are
currently residing at Purok 6-A, Barangay 76-A Bucana, Davao
City. Mrs. X who is 53 years old, an elementary graduate and a
mother of the family was diagnosed with Diabetes Mellitus,
Hypertensive, and Gout Arthritis. She doesn’t work at all and
doesn’t have any alternative ways of earning money for she
just used to stay at their home because of her diseases. She
experienced easy fatigue due to DM and joints pain due to Gout
12
Arthritis. But her husband and two sons had their own work
that supported and offered her money for their needs. She also
used to be involved in making the decision in relation to
health or medical care and other family concerns. Her husband
Mr. X is 58 years old, an undergraduate, completing only the
second year high school level is a self-employed driver that
slightly supported by the Pepsi Company. He was also diagnosed
as Hypertensive last May 2013 near at Mission Hospital near
the Magsaysay Street. He used to be dominant in terms of
decision making on financial budget. They have 4 children who
grew older and were independent in earning money and living
except for her two daughters as they were just at their
respective home. But only 2 of their children are still living
near with them to help and overlook their mother’s condition.
Their eldest child is a female, 34 years old, a college
graduate, married with 3 children and just staying at their
home nearby to their parent’s house as a housewife to overlook
her children and to monitor her mother’s health condition.
Their 2nd child is 32 years old, only a high school graduate,
single and working also as a driver by his father’s help at
Pepsi Company. Their 3rd child is 31 years old, married and
was already out of the country who has also Hypertension.
Finally, their youngest child is 30 years old, with a live in
partner and college graduate who worked as a salesman in
Emperador company. Their fourth child has a live-in partner
who was already separated from them and lived at Agdao area.
Their family has owned their house that is made of light
wood and a concrete floor with 3 rooms. The space in between
their house is enough with well ventilation. But the structure
of their house with their neighbors is quite narrowed with
13
their floor is in low ground. According to her, every time
there is a rain, they experience flood as they are prone to it
and their ceiling needs a repair for drops of rain entered to
their house. They have enough furniture and sufficient
appliances like refrigerator, electric fan, television, DVD,
personal computer, telephone, cellphone as their means of food
storage, diversional devices, and communication. They also
have sufficient lighting facility with electricity and there
is no presence of any accident hazards with the absence of
stairs and easy-reached sharps objects locations. Their water
supply is a public source. They used a pail system in toilet
facility and they have an open drainage system. They are
throwing their garbage properly. They used firewood and
charcoal in cooking in their dirty kitchen which is located in
the middle of their sink and comfort room. But most of the
time, they used gas stove when cooking. They have also
available transportation facilities such as elf, motorcycle
(private), and van as supported by their father’s employment.
They ate a complete meal in a day and were provided by
sufficient foods, clothing, and shelter. They usually have
close family ties and support each other’s needs.
The family was used to spend their leisure time sometimes
like outdoors activity during Sunday even without the presence
of their mother due to the disease. They also used to gather
together and spend some joyful moments most of the times. They
used to cooked foods for meals then eat together and tackled
some interesting topics to be discussed. They are so much open
to each other that they shared each other’s experiences.
SOCIO-ECONOMIC BACKGROUND
14
Mrs. X is 53 years old, and was married to Mr. X who is
a self-employed driver but slightly supported by the Pepsi
Company where he worked before. She is a plain housewife and a
loving mother to her four (4) children. She stays in her
place, at home as a plain housewife in their family and was
not involve in any organizations or businesses in the
community. The eldest child works as a housekeeper or
housewife to her respective family. The second child works as
a driver at Pepsi Company by the help of his father. The third
child is a housewife with her new and respective family who
already went outside the country. The fourth child was a
salesman and still a new employee which income is not yet
sufficient enough to be contributed to the whole family. With
regards with their family’s economic status, her husband
earned P10,000-20,000 per month from 8 hours of work per day.
Her second child also earned a monthly income for about P5,
000-10,000 from 8 hours of work per day. The money they got
from their work as their source of income was greatly and
fairly contributed to the whole family to sustain their basic
needs especially for their medical care.
Mrs. X is just used to accept what her husband and her
children gave her and how much money they would contribute to
the family for the electric current, water bills, and her
medical treatments and prescribed medications. She tends to
wait about their family’s financial transactions or reports.
FAMILY MEDICAL and HEALTH HISTORY
15
The X family is residing at Purok 6-A, Barangay 76-A,
Bucana, Davao City is composed of 6 members; Mr. and Mrs. X
with their four children. Her husband was used to gamble
sometimes during the day-off from his work that serves as an
outlet and hobby for stress-free. Her eldest child has no
known disease or illness as well as her last child. Her 2nd
child (son) oftentimes felt pain in his legs. It wasn’t
diagnosed yet. The 3rd child who has also Hypertension got
married and went outside the country. The 4th child was
already living separately from the family and lives with his
partner. In their family, they experience common colds and
cough especially during rainy season. They even experienced
headache, fever, stomach ache as their common illnesses and
Hypertension, Diabetes Mellitus, Arthritis, and UTI as their
common and potential diseases.
The 53 years old female client was diagnosed with Type II
Diabetic Mellitus last 1997 at Davao Doctor’s Hospital on her
last 37 years old which now runs for about 16 years. Since
before until now, she used to have her regular visit and close
monitoring with their family doctor at Matina Aplaya Clinic,
Davao City. They don’t have any first aid kit but she has with
her the other paraphernalia in Diabetes Mellitus for medical
care support.
According to Mrs. X when she was scheduled to her medical
care and regular monitoring at Matina Aplaya Clinic, Davao
City with their family doctor, her eldest child will accompany
her to go and visit there her since her husband and second
child were not around all the time. They couldn’t assist her
anytime and anywhere she goes due to their works/jobs. Her
eldest daughter’s family with her grandchildren and her
16
siblings who lived nearby them with her nephews will overlook
and assist her she wants to do and where she wants to go apart
from their home. She can’t freely goes somewhere especially on
attending any community activities and health care services
because of her painful experience of gout arthritis and
fatigue feeling due to diabetes. Last September 03, 2013, she
was also diagnosed having a Gout Athritis upon having her
regular visit in the clinic with her eldest daughter.
Her latest results in current diagnostic procedure in
urine physical examination this September are the following:
light yellow urine color, slight cloudy character, 5.0
reaction, 1.010 specific gravity with 6-8 pus cells and 1-2
RBC in microscopic examination. With regards to her chemical
reaction results with the use of Benedict’s solution and
Asetic Acid, her test for albumin in urine result is +1 and
the test for sugar in her urine results about +4. Her latest
Blood Chemistry results were also determined: Glucose FBS=
13.69, Uric Acid= 0.619, Creatinine= 57.43. Her total
cholesterol was also examined which results about 6.4,
Triglycerides= 4.16, HDL-Cholesterol= 0.92, LDL-Cholesterol=
3.59.
Because of those diagnostic results even with her
previous results, Mrs. X was expected to be diagnosed with
Hypertension and it was so right after the Diabetes Mellitus
diagnosis. Mr. X was also diagnosed as Hypertensive last May
2013 near at Mission Hospital near the Magsaysay Street. They
were both diagnosed with Hypertension. They usually go to
their family doctor directly at Matina Aplaya Clinic to have a
regular medical monitoring.
17
During my assessment with her and validation with her
diagnosis, I collected her urine specimen last September 12,
2013 since Bag technique procedure was conducted for that
day’s activity to determine who the residents had already
Diabetes Mellitus are and potentially high at risk of it. The
results confirmed that her sugar in urine is quietly high,
still +4 result (brick red) and her albumin in urine is +1,
with cloudiness. Because of that, health teachings and health
education were carried out and implemented to the client for
diet and lifestyle modifications. She even stated that she was
in that changes since before like eating less of ice cream, no
softdrinks at all, and others that are high in sugar. So, she
used to eat low sugar and less carbohydrates content and low
salt and low fat diet for she’s aware of it. She also
emphasized that she took her prescribed medications but as of
now, she tried her new food supplement if there would be
reaction occurs from taking it that would prevent her disease
to further complications. So, until now, she’s still complying
her medications prescribed by her doctor in addition with
Usana food supplement. She has a good compliance of the
therapeutic regimen. Their family has strong bond of
attachment with close family ties as their good relationship
with all the members of the family was still maintained.
18
G E N O G R A M
1st Generation Mother’s side Father’s side
2nd Generation
3rd Generation
HPNHPN DM
HPN DM DM HPNDM DMDMDMDM
DM DMSTP DMHPNGADMDM RO DM
DM DMHPN
DM
LEGENDS: Deceased Male Married
Deceased Female Male
Identified Client Female
Identified Client’s Wife DM – Diabetes
HPN – Hypertension STP – Sore Throat Pain
GA – Gout Arthritis RO – Rectum Operation
19

LEGENDS: Deceased Male Married
Deceased Female Male
Identified Client Female
Identified Client’s Wife DM – Diabetes
HPN – Hypertension STP – Sore Throat Pain
GA – Gout Arthritis RO – Rectum Operation
20
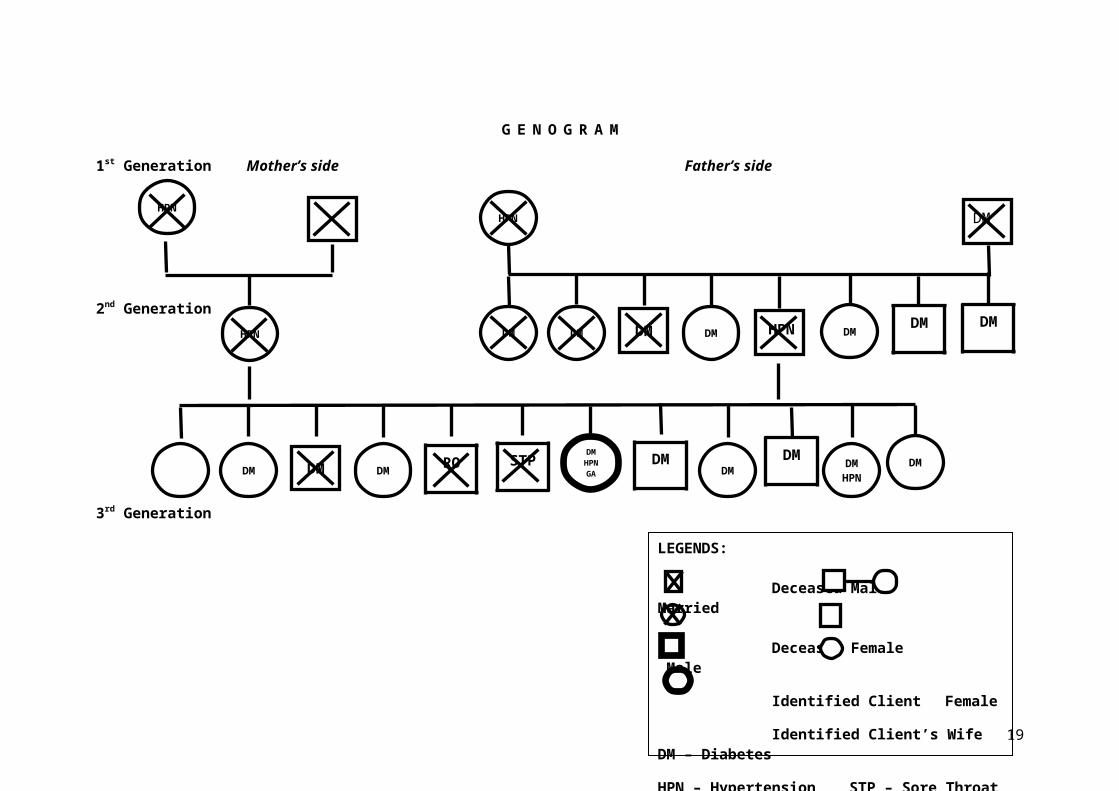
Interpretation
The presentation above shows about the structure of Mrs.
X’s family or the genogram from first generation to third
generation. Mrs. X’s grandparents in both sides were died. For
the first generation, Mrs. X’s grandparents in her father’s
side had eight children in which his father was included. Mrs.
X’s grandfather has a history of Diabetes Mellitus that seven
of the siblings of Mrs. X’s father had acquired it. For the
second generation, only his siblings, four females and three
males who had acquired Diabetes Mellitus as it is also said to
be a heredofamilial disease. Three of them had died (2
females and 1 male) because of Diabetes Mellitus. Mrs. X’s
father was already deceased not because of acquiring DM but
because of Hypertension. Mrs. X’s father had only acquired
Hypertension form his mother. In the other corner, Mrs. X’s
grandparents in her mother’s side had no history of Diabetes
Mellitus but only Hypertension. Because it is also a sort of
hereditary disease, Mrs. X’s mother had acquired it in the
second generation and was also deceased because of it. For the
third generation, Mrs. X had a total number of twelve siblings
including her. Her eldest sibling has no history of any
diseases whereas nine of them had acquired Diabetes Mellitus
disease. Her third sibling died because of DM. Her fifth
sibling died because of the complication of the rectum
operation. Her sixth sibling was also died because of having
pain in the sore throat as it wasn’t clearly diagnosed. Mrs. X
and her remaining siblings from Mrs. X to her youngest sibling
had acquired Diabetes Mellitus and sort of Hypertension. Both
parents of Mrs. X didn’t acquired DM disease from the first
21
generation. It was just come to the point that DM was mostly
inherited to the third generation (Mrs. X and her siblings)
from the first generation which skips the second generation to
acquire it.
22
FAMILY APGAR
Adaptation 1 Discusses the manner
of adapting and
dealing the family’s
problem as
sometimes, they used
to gather together
and have an open
forum. Mrs. X has
accepted her health
condition the moment
he discovered her
serious disease and
she’s even satisfied
with their life’s
status. She was even
thankful despite of
everything.Partnership 2 They tend to discuss
their problems
corporately and used
their available
resources. Mrs. X
stated that both her
husband shared their
ideas in decision
making for the
solutions of the
problems with the
presence of their
23
children (except for
the fourth child).
The father and their
2nd child were tasked
to do the job well
for more income for
the provision of
their basic needs.
Mrs. X was also
commissioned to
comply her medical
treatments for her
own good as the
whole family agreed
on it. They tell
each other’s
concerns when it
comes to family
issues.Growth 2 Mrs. X had
verbalized that her
children were well
taken care of until
they grew older.
They were able to
learn many things
especially the
parenthood matters
as they were already
independent and
supported each
24
other. They used to
respond and give
feedback their
mother’s needs due
to the disturbance
of her health
condition. Affection 2 The family has
always a time to
bond with each other
by doing any leisure
and recreational
activities such as
cooking foods for
their meals and
gather and eating
together in one
area. They used to
do it during lunch
time, dinner, and
breakfast sometimes.
They shared each
other’s foods as
some of her siblings
were assigned to
take grocery and
assigned to cook.
They watched
television, ate
together, shared and
opened-up something
25
with Mrs. X’s
siblings. They were
all considerate,
sensitive, helpful,
supportive, and
caring who showed
love and respect
despite of
everything. They
used to understand
and help each
other’s needs.Resolve 2 Every time the
family has conflict
or misunderstanding
occurrences, they
used to set a time
and gather together
to open-up the
concerned issue or
problem in the
family to formulate
better solutions and
actions that are
approved by all.
They don’t used to
have conflict all
the time but
occurred seldom.
They can manage and
understand it well.
26
Total 9 The family’s APGAR
Score is 9 which
indicate that the
structure of their
family is highly
functional. It shows
that the family was
able to communicate
and interact well
with the family
members and other
siblings as they
provided each
other’s needs with
showed total family
strong bond of pure
love and care. They
support each other
well using any
available personal
resources.
27
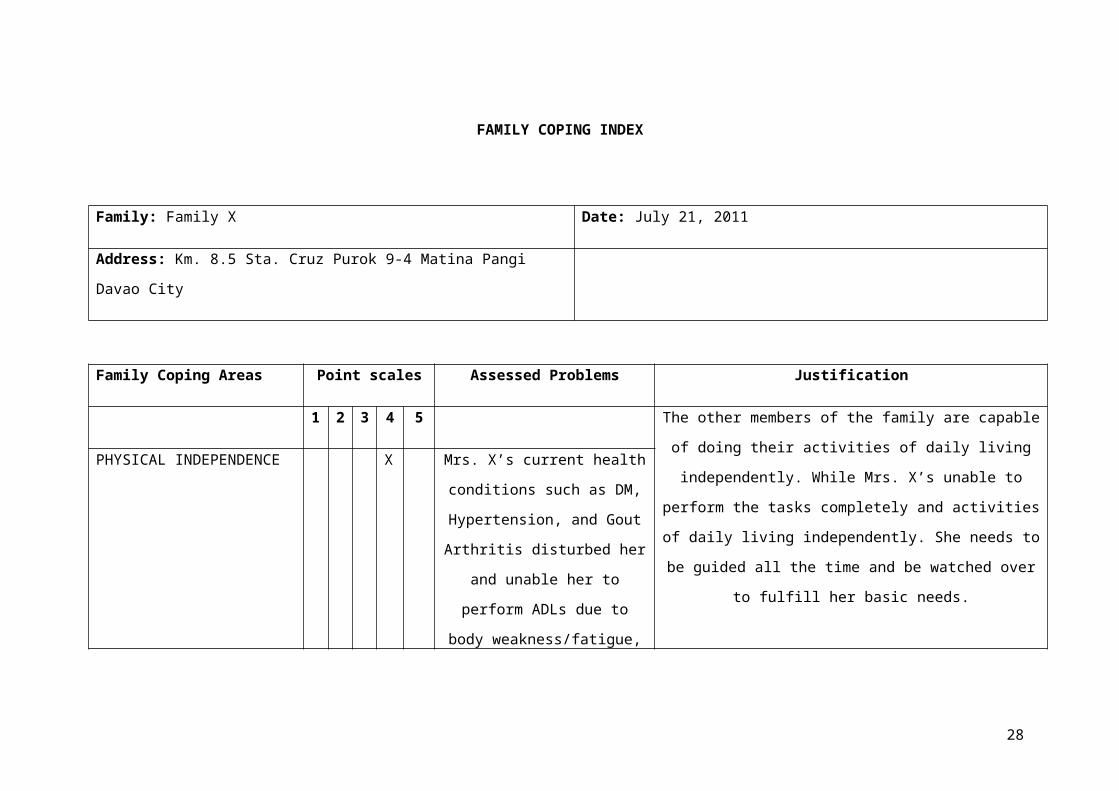
FAMILY COPING INDEX
Family: Family X Date: July 21, 2011
Address: Km. 8.5 Sta. Cruz Purok 9-4 Matina Pangi
Davao City
Family Coping Areas Point scales Assessed Problems Justification
1 2 3 4 5 The other members of the family are capable
of doing their activities of daily living
independently. While Mrs. X’s unable to
perform the tasks completely and activities
of daily living independently. She needs to
be guided all the time and be watched over
to fulfill her basic needs.
PHYSICAL INDEPENDENCE X Mrs. X’s current health
conditions such as DM,
Hypertension, and Gout
Arthritis disturbed her
and unable her to
perform ADLs due to
body weakness/fatigue,
28
blurred vision,
polydipsia, polyuria,
polyphagia and other
signs and symptoms of
DM who also experienced
joints pain because of
Gout Arthritis. She
needs assistance and
help most of the time.
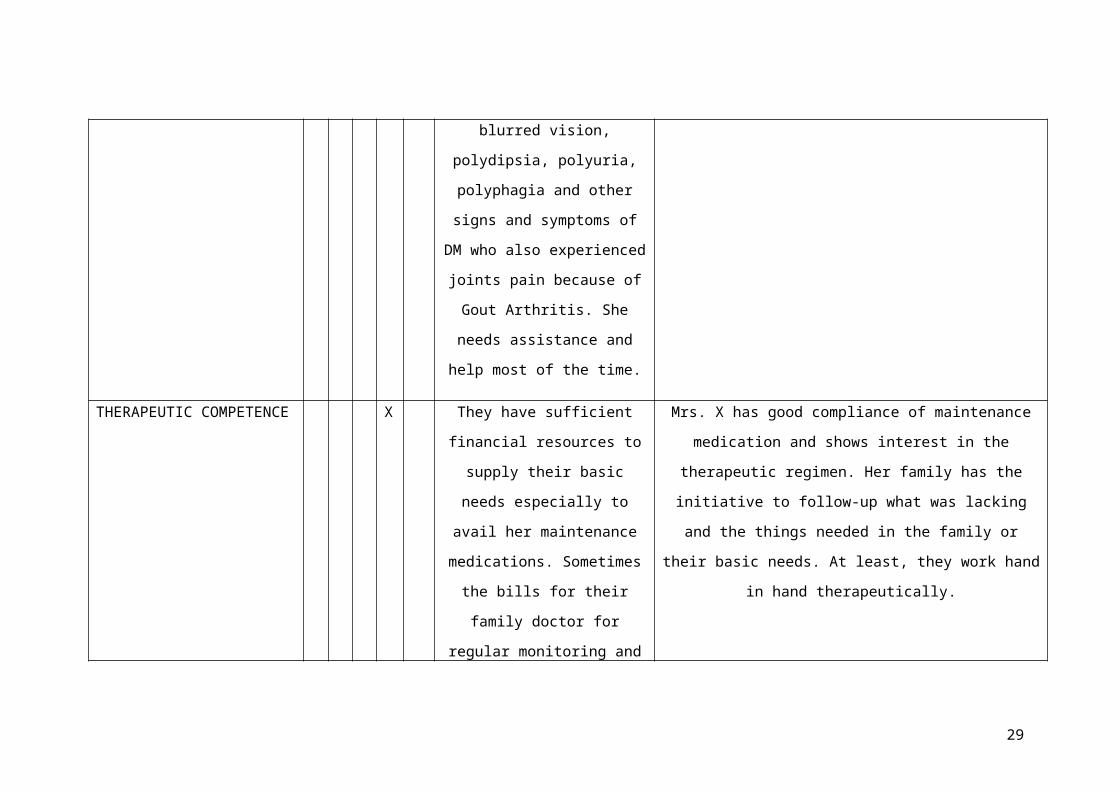
THERAPEUTIC COMPETENCE X They have sufficient
financial resources to
supply their basic
needs especially to
avail her maintenance
medications. Sometimes
the bills for their
family doctor for
regular monitoring and
Mrs. X has good compliance of maintenance
medication and shows interest in the
therapeutic regimen. Her family has the
initiative to follow-up what was lacking
and the things needed in the family or
their basic needs. At least, they work hand
in hand therapeutically.
29
for her prescribed
medications cost
expensive that caused
other family member’s
worried. But her second
child (son) would save
them for any lack of
financial resources in
order to supply them
with their basic needs
and to fulfill her
medical treatments as
stated.
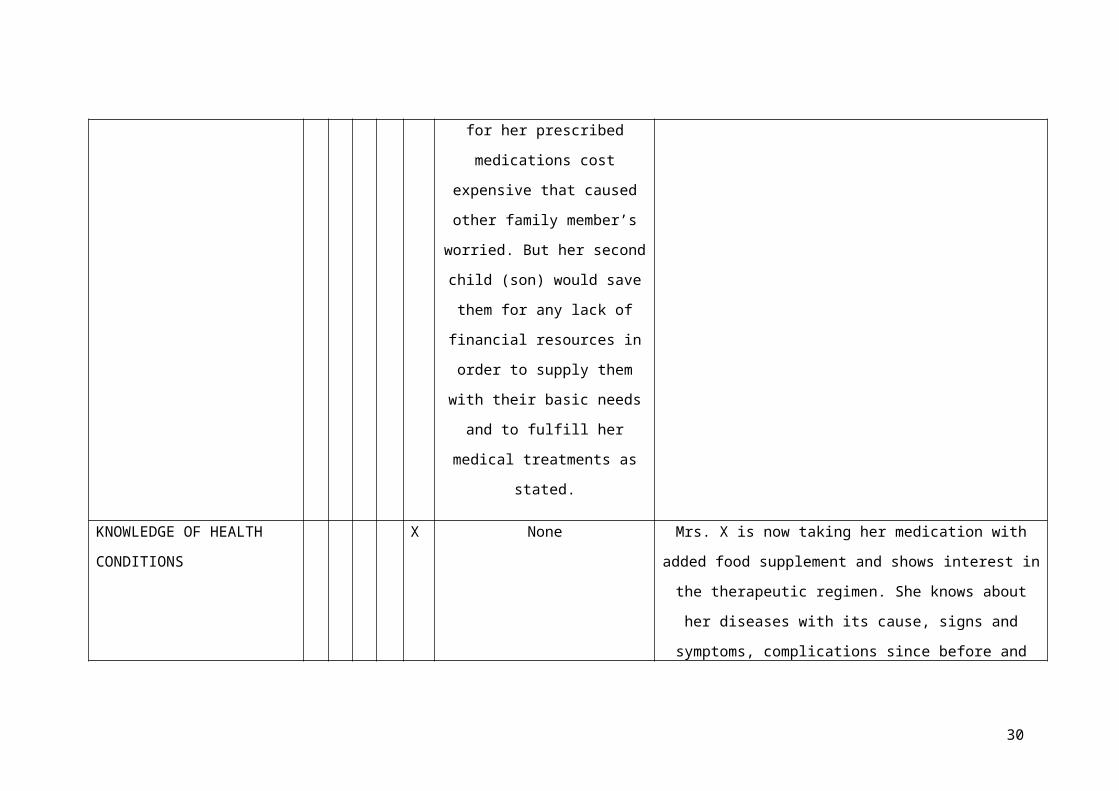
KNOWLEDGE OF HEALTH
CONDITIONS
X None Mrs. X is now taking her medication with
added food supplement and shows interest in
the therapeutic regimen. She knows about
her diseases with its cause, signs and
symptoms, complications since before and
30
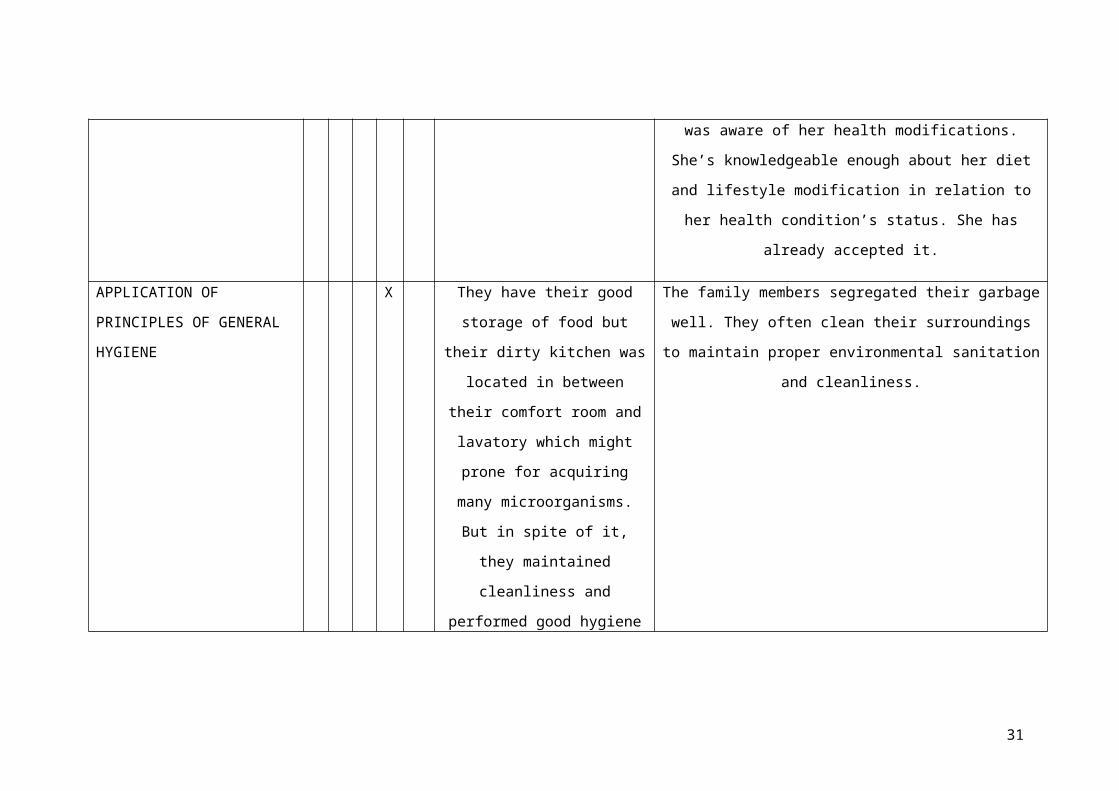
was aware of her health modifications.
She’s knowledgeable enough about her diet
and lifestyle modification in relation to
her health condition’s status. She has
already accepted it.
APPLICATION OF
PRINCIPLES OF GENERAL
HYGIENE
X They have their good
storage of food but
their dirty kitchen was
located in between
their comfort room and
lavatory which might
prone for acquiring
many microorganisms.
But in spite of it,
they maintained
cleanliness and
performed good hygiene
The family members segregated their garbage
well. They often clean their surroundings
to maintain proper environmental sanitation
and cleanliness.
31
especially Mrs. X.
HEALTH ATTITUDES X They don’t have any
first aid kit but only
the provided
paraphernalia of Mrs. X
for her Diabetes
Mellitus. Sometimes she
feels hopeless for
there are still no
changes. She already
accepted what diseases
she has and obtains her
prescribed medicines
with regular check-up
or medical monitoring.
She was able to accept
it but she’s still
hopeful as she’s
Mrs. X was still consistent in taking her
prescribed medications and modified diet
(low sugar/carbohydrate, low fat, low salt
diet) and lifestyle. She once verbalized
“Nagtumar man ko sa akong mga tambal pero
ako pang gisulayan ning food supplement sa
USANA kung naa bay reaksyon.” She’s still
trying and determine for her disease
prevention to gain good quality of life.
They do not use any herbal medicines that
are approved or not approved by the DOH.
They often go directly with their family
doctor.
32
looking forward for her
better treatment and
positive outlook for
cure that’s why she
tried to take USANA
food supplement.
EMOTIONAL COMPETENCE X None Mrs. X verbalized “Pag naay mga problema o
dili pagkasinabtanay, magtapok2x mi tanman
ug tarong namong saboton. Naa mi panahon sa
pagistoryahanay bahin niana aron masulbad.
Nagtabang ug nagsuporta jud sila. Nagpakita
man ug gugma ug pag-atiman sa ako.” Their
affection within the family members was
showed up with all the support, assistance,
guidance, and strong family ties.
33
FAMILY LIVING 5 None Their family living is good and enough to
supply and provide their basic necessities.
They have good management of their money or
financial resources as they tend to
contribute it to their whole family with
generosity basic one’s needs. They’re
generous, joyful, and truly good enough.
PHYSICAL ENVIRONMENT X The toilet facility
is near the kitchen
and lavatory which
is prone to health
hazards; the roof or
ceiling has little
holes that every
time the rain comes,
raindrops would pass
through it. The
foundation of the
Their toilet facility is near the kitchen
and lavatory which is prone to health
hazards like it is prone for contamination
by acquiring undesirable microorganisms.
Their rooftop with little holes that
supports the foundation of their house is
prone for raindrops that could enter into
their interior structure of their house.
Not having well spacious of location of the
residence would lead to any danger of the
family especially if there would any fire
34
house is strong but
the ground is too
low which is prone
to floods. Their
house is narrowed to
other neighbor’s
house. Presence of
undeveloped canals
makes them also
worried that could
lead any danger
during rainy
seasons.
disaster occurrences. The location of their
house is near the undeveloped canals which
prone to Dengue fever, Leptospirosis
disease from having flood during rainy
season. It would also lead to other common
and emergent diseases.
USES OF COMMUNITY
RESOURCES
X They can’t access more
of the health care
services offered from
their health center for
Mrs. X can’t walk alone
Mrs. X verbalized “Modritso lang mi adto sa
doctor
para ifollow-up ug imonitor akong sakit. Dili
kayo ko makaadto sa health center ug
35
but needs assistance
and company from going
a little bit distance
from their house. Her
husband and second
child were busy and
always at work. Her
eldest daughter was
also busy taking care
of her children and
Mrs. X. But somehow,
they were able to avail
any information and
health care services by
home visitation and
through any available
other family members
like Mrs. X’s siblings
makaapil sa mga aktibidadies sa komunidad kay
magluya ko ug ngulngol akong tiil. Akong
anank lang nga baye ug akong mga igsoon ang
makaadto diadto usahay ug magsulti sa ako
unsay gipanghisgutan ug pagkuha sa mga
benepisyo bahin sa kalawasan o problema sa
komunidad.”
36
as their messenger of
information. They
usually go directly to
their family doctor for
their scheduled close
health monitoring.
Scaling: 1- No Competence, 3- Moderate Competence, 5- Complete Competence
37
FAMILY COPING INDEX
The score for Physical Independence category is 4 because
Mrs. X is unable to perform completely the household chores
even though the other family members are capable of doing
their entire daily living activities; therefore there is
assessed problem for Physical Independence.
The Therapeutic Competence category scored 4 because Mrs.
X has good compliance of maintenance with medications and
shows interest in therapeutic regimen. Mrs. X can able to
manage her maintenance medications despite of her previous
medical treatments and medications expenditures that are
expensive.
Knowledge of Health Education category is scored 5
because Mrs. X is taking her medication consistently. She
knows about when to take and when she will visit and go to the
doctor with company and assistance. She’s knowledgeable enough
to change her diet (low sugar/carbohydrate, low salt, low fat
diet) and lifestyle with limit physical exercise and household
activities. She verbalized “Nagalikay na ko ug kaon anang mga
tam-is, limit lang ug mga parat o tambok nga mga pagkaon
parehas anang karne.”
For the Application of Principles of General Hygiene
category, I scored 4 because they segregate garbage
thoroughly, clean their surroundings but they don’t have safe
toilet facility and dirty kitchen structure which was located
in between their comfort room and lavatory that might prone
for contamination by acquiring many undesirable
microorganisms. They have their good storage of food. But in
38
spite of it, they maintained cleanliness and performed good
hygiene especially Mrs. X.
In Health Attitudes category, I scored 5 because Mrs. X
is compliant and consistent with her treatment regimen and
medical interventions or treatments.
For Emotional Competence category, I scored 5 because
Mrs. X’s family members were supportive to each other and
showed love and care with strong bond of family ties or family
member’s attachment.
For Family Living category, I scored 5 because their
family living is good and enough to supply and provide their
basic necessities. They have good management of their money or
financial resources as tend to contribute it to their whole
family with generosity basic one’s needs. They’re generous,
joyful, and truly good enough.
In Physical Environment category, I scored 2 because
their toilet facility is near the kitchen in which their dirty
kitchen was located in between the comfort room and lavatory;
the rooftop has little holes that makes them uncomfortable
during rainy season with the ground prone for flood which was
located near the canal area. The space between houses is also
narrow.
For the use of Community Resources category, I scored 3
because they were not so accessible with the health care
services given from the health care center and the community
activities.
NURSING THEORY
39
Florence Nightingale’s (Environmental Theory)
Florence nightingale’s theory talks about how important
environment is to our health. Like the ventilation and warmth,
light, cleanliness, health of houses, noise, bed and beddings,
personal cleanliness, variety, chattering hopes and advices,
taking foods, petty management and observation of the sick.
Florence Nightingale’s can be applied to our case study
because although the cleanliness is fair in their house and
environment, the toilet facility is near the kitchen in which
their dirty kitchen was located in between the comfort room
and lavatory. Hence, it is prone for contamination by
acquiring undesirable microorganisms. The rooftop has little
holes that make them uncomfortable during rainy season then
their ground is also prone for flood which was located near
the canal area. The space between houses is also narrow.
Thereby, the location of their house is prone to any accidents
or disasters like fire. Though there was a settled agreement
on proper garbage/waste disposal, their community has lack
management on cleaning of canal areas. It may cause the
breeding places for mosquitoes that are dengue carriers and
leptospirosis from having a flood. They are also a little bit
near from the sea. These physical factors affect them to their
vital functions in the community with their activities of
daily living resulting to discomfortability and unhealthy
condition of an individual.
40
Sister Callista Roy (Adaptation Model)
Sister Callista Roy developed the Adaptation model of
nursing. Roy’s models see the person as a biopsychosocial
being who has constant interaction with the changing
environment. According to her, the environment affects the
development and behavior of the person. She also stated that
health is a state and a process of being and becoming an
integrated and whole person.
In our client’s case, Roy’s theory can be applied to them
since they have been diagnosed and were already aware of their
medical diagnoses especially Hypertension, Diabetes Mellitus,
Gout Arthritis to Mrs. X and Hypertension to the other family
members. Mrs. X has fully recognized her serious disease and
already accepted it with appropriate interventions and
modifications. She even knows the risks factors as her
children are potentially risked at it and complications of her
diseases that’s why there are already restrictions. She was
able to adapt it and adjust her diet and lifestyle with
physical activities. As knowing all of their health
condition’s status, they were able to cope up it by
acceptance, determination, and pursuance in life by having
better prevention. She still has her faith and positive coping
mechanism as acceptance, being thankful for all things and
satisfaction for everything were in her, no matter what
happens.
Virginia Henderson (14 basic Human Needs)
41
Henderson conceptualized the 14 Fundamental Needs of
Humans, which are: breathing normally, eating and drinking adequately,
eliminating body wastes, moving and maintaining desirable position, sleeping and
resting, selecting suitable clothes, maintaining normal body temperature by
adjusting clothing and modifying the environment, keeping the body clean and well
groomed to promote integument, avoiding dangers in the environment and avoid
injuring others, communicating with others in expressing emotions, needs, fears, or
opinions and worshipping according to faith. She believes that Health is
a quality of life and a basic for a person to function fully.
It is important for a healthy individual to control the
environment but as illness occurs, this ability is diminished
or affected in caring for the sick.
Virginia Henderson’s theory in relation to the family
that we chose to study is essential information because this
family has alterations and adjustments in their personal
living especially to Mrs. X. There was already an adjustment
and interruption with her eating, drinking, sleeping patterns
with modified environment because of her long-term diseases
which are DM, Hypertension, and Gout Arthritis. She
frequently experienced polydipsia for about how many minutes
even just talking for less minutes. She used to experienced
polyuria or frequent urination every day and every night. She
even seeks for any foods as she easily got hungry and easily
got tired or has body weakness. She also verbalized even her
eldest daughter and nearby siblings that she doesn’t have
enough rest and sleeping pattern all the time because of her
condition and joints pain occurrences. She even experienced
blurred vision that even upon talking and interviewing her in
near distance, she couldn’t see clearly as she has the
42
difficulty on recognizing well the person she’s talking to.
She can’t go and walk alone to where she wants to go even
though it’s a little bit far from their house. That’s why she
needs guidance and assistance for accompaniment most of the
time when she wants to stay for a while with her neighbors
(siblings’ houses) and go somewhere. Base on Henderson’s
theory, this family has an undisputedly concern in dealing
Mrs. X health’s condition for they can’t leave her alone. It
would interrupt and distract other’s business as big burden to
them when they supposedly do their activities of daily living
or household chores in their respective family. But it doesn’t
imply to the family that it was a big burden to them. They
were able to support and assist her from time to time. But in
overall impression, it really has an alteration in Mrs. X’s 14
Fundamental Human Needs.
MEDICAL MANAGEMENT FOR DIABETES MELLITUS
Overview of Diabetes Mellitus
Diabetes Mellitus (commonly referred to as diabetes)
is a disease of the pancreas, an organ behind your stomach
that produces the hormone insulin. Insulin helps the body use
food for energy. When a person has diabetes, the pancreas
either cannot produce enough insulin, uses the insulin
incorrectly, or both. Insulin works together with glucose
(sugar) in the bloodstream to help it enter the body's cells
to be burned for energy. If the insulin isn't functioning
properly, glucose cannot enter the cells. This causes glucose
43
levels in the blood to rise, creating a condition of high
blood sugar or diabetes, and leaving the cells without fuel.
There are two common forms of diabetes: type 1 and type 2.
Type 1: Type 1 diabetes occurs because the insulin-producing
cells of the pancreas (beta cells) are damaged. In type 1
diabetes, the pancreas makes little or no insulin, so sugar
cannot get into the body's cells for use as energy. People
with type 1 diabetes must use insulin injections to control
their blood glucose. Type 1 is the most common form of
diabetes in people under age 20-30, but it can occur at any
age. Ten percent of people with diabetes are diagnosed with
type 1. Type 2: In type 2 diabetes, the pancreas makes
insulin, but it either doesn't produce enough insulin or the
insulin does not work properly. Type 2 diabetes may sometimes
be controlled with a combination of diet, weight management
and exercise. However, treatment also may include oral
glucose-lowering medications or insulin injections.
Generally, type 2 diabetes is more common in people over
age 40 who are overweight. However, the prevalence of obesity
among people in North America has increased the number of
people under age 40 who are diagnosed with type 2 diabetes.
Nine out of 10 people with diabetes have type 2.
Ideal Medical Management for Diabetes Mellitus
Diabetes is a chronic illness that requires continuing
medical care and patient self-management education to prevent
acute complications and to reduce the risk of long-term
complications. Diabetes care is complex and requires that many
issues, beyond glycemic control, be addressed. A large body of
44
evidence exists that supports a range of interventions to
improve diabetes outcomes. There is no cure for diabetes, but
it can be treated and controlled.
The goals in caring for patients with diabetes mellitus
are to eliminate symptoms and to prevent, or at least slow,
the development of complications. Microvascular (ie, eye and
kidney disease) risk reduction is accomplished through control
of glycemia and blood pressure; macrovascular (ie, coronary,
cerebrovascular, peripheral vascular) risk reduction, through
control of lipids and hypertension, smoking cessation, and
aspirin therapy; and metabolic and neurologic risk reduction,
through control of glycemia.
Diabetes care is best provided by a multidisciplinary team
of health professionals with expertise in diabetes, working in
collaboration with the patient and family. Management includes
the following: appropriate goal setting, dietary and exercise
modifications, medications, appropriate self-monitoring of
blood glucose (SMBG), regular monitoring for complications,
laboratory assessment.
Ideally, blood glucose should be maintained at near-normal
levels (preprandial levels of 90-130 mg/dL and hemoglobin A1C
[HbA1c] levels < 7%). However, focus on glucose alone does not
provide adequate treatment for patients with diabetes
mellitus. Treatment involves multiple goals (ie, glycemia,
lipids, blood pressure).
Aggressive glucose lowering may not be the best strategy in
all patients. Individual risk stratification is highly
recommended. In patients with advanced type 2 diabetes who are
45
at high risk for cardiovascular disease, lowering HbA1c to 6%
or lower may increase the risk of cardiovascular events.
Laboratory and Diagnostic tests for Diabetes Mellitus
The diagnosis of Diabetes Mellitus (DM) comes from
careful evaluation of the patient's history, the physiologic
symptoms and the clinical laboratory results. The clinical
laboratory performs the required tests on an appropriate
patient's sample and the results would then be used to confirm
the diagnosis of DM. The following are laboratory results that
could confirm DM in a patient:
- Glucosuria is the presence of glucose (sugar) in urine.
The urine specimen would be positive for sugar. The renal
threshold for glucose is 160 mg/dL. When this
concentration is exceeded in the blood, then it would
then appear in the urine making the urine specimen
positive for sugar. This is an indication that the
concentration of glucose in blood could be more than 160
mg/dL.
- Ketonuria in which presence of ketone bodies (acetone,
hydroxybutyric acid, etc) in urine. This indicates that
the body could not utilize the carbohydrates as a source
of energy because of the insufficiency of insulin; so it
makes use of lipids (fats) instead. The utilization of
fats as a source of energy will lead to an increase
concentration of the by-product of lipid which are the
ketone bodies. These will then lead to the increased
excretion of ketones in the urine called ketonuria.
46
- Hyperglycemia that leads to the increased levels of
sugar, predominantly glucose, in the blood stream. This
could be detected by allowing the patient to fast for 8
to 12 hours before collection of blood specimen. A
patient with a sample value above the normal which is 60-
110 mg/dL (Orthotoluidine method), would be considered as
hyperglycemic and a candidate for DM.
- Oral Glucose Tolerance Test (OGTT) could also be
performed on a patient suspected of DM.
- Glycated Hemoglobin (A1C) test is a blood test which
indicates the average blood sugar level for the past two
to three months. It measures the percentage of blood
sugar attached to hemoglobin, the oxygen-carrying protein
in red blood cells. The higher your blood sugar levels,
the more hemoglobin you'll have with sugar attached. An
A1C level of 6.5 percent or higher on two separate tests
indicates that you have diabetes. It is a test for the
patient's adherence to his medications for DM. If the
patient did not adhere to his medications, then the value
of this type of hemoglobin is usually elevated.
- Random blood sugar test where in a blood sample will be
taken at a random time. Regardless of when you last ate,
a random blood sugar level of 200 milligrams per
deciliter (mg/dL) — 11.1 millimoles per liter (mmol/L) —
or higher suggests diabetes.
- Fasting blood sugar test in which a blood sample will be
taken after an overnight fast. A fasting blood sugar
level between 100 and 125 mg/dL (5.6 and 6.9 mmol/L) is
considered prediabetes. If it's 126 mg/dL (7 mmol/L) or
47
higher on two separate tests, you'll be diagnosed with
diabetes.
Actual Medical Management
Mrs. X is 53 years old female client who was
diagnosed with Type II Diabetic Mellitus last 1997 at Davao
Doctor’s Hospital on her last 37 years old. From 1997 until
now, it runs for about 16 years. Because of that, from time to
time, she used to have her regular visit and close monitoring
with their family doctor at Matina Aplaya Clinic, Davao City.
From that moment, she’s also developing Hypertension. Last
September 03, 2013, she was also diagnosed as having a Gout
Arthritis upon having her regular visit in the clinic
accompanied by her eldest daughter. Her husband was diagnosed
with Hypertension as well as their second daughter. They had
taken their prescribed medication. Lucky to say, her children
didn’t acquire Diabetes Mellitus. With their preventive
measures especially to Mrs. X, she modified her diet and
lifestyle and limit intake of certain prohibited foods like
increase sugar (ice cream and softdrinks) and meats. She was
prescribed with her medications for DM which are Deptan (once
a day), Metformin (three times a day), and antihypertensive
drug which are Propanolol (three times a day) and Mediclamide
(three times a day). She complied her medications prescribed
by their physician with regular also physical activities as
promoted.
48

DRUG STUDY
Anti-diabetic drug:
49
Generic name: Metformin and Sitagliptin
Brand name: Janumet
Classification: Anti-diabetic
Dosage: 50mg 1 tab OD
Action: Decreases hepatic glucose production. Decreases
intestinal glucose absorption. Increases sensitivity to
insulin.
Indications: Management of type 2 diabetes mellitus; may be used
with diet, insulin, or sulfonylurea hypoglycemia.
Contraindications: Hypersensitivity, metabolic acidosis, dehydration,
sepsis, renal dysfunction, hepatic impairment.
Side effects: Diarrhea, nausea, unpleasant metallic taste.
Nursing considerations:
• Assess for patient's history of diabetes.
• Monitor for patient's blood glucose before and after giving
medications.
• Assess for hypersensitivity to Metformin.
• Assess for patient's renal function.
• Monitor for signs and symptoms of hypoglycemic reactions
(e.g. cold andclammy skin).
• Discontinue if renal impairment occurs.
• Instruct patient to do proper foot care.
• Instruct patient for unpleasant metallic taste of the drug.
Antihypertensive drug:
Generic Name: Propranolol hydrochloride
Brand Name: Apo-Propranolol (CAN), Inderal, Inderal LA, InnoPran
XL, Nu-Propranolol (CAN), Propranolol Intensolol
50
Classification: Beta-adrenergic blocker (nonselective),
Antianginal, Antiarrhythmic, Antihypertensive
Pregnancy Category C
Dosage & Route
Available forms: ER capsules—60, 80, 120, 160 mg; tablets—10, 20,
40, 60, 80, 90 mg; SR capsules—60, 80, 120, 160 mg; injection—
1 mg/mL; oral solution—4, 8 mg/mL; concentrated oral solution—
80 mg/mL
ADULTS
Oral
Hypertension: 40 mg regular propranolol bid or 80 mg SR
daily initially; usual maintenance dose, 120–240 mg/day
given bid or tid or 120–160 mg SR daily (maximum dose,
640 mg/day).
Angina: 80–320 mg/day divided bid, tid, or qid or 80 mg
SR daily initially; gradually increase dosage at 3- to 7-
day intervals; usual maintenance dose, 160 mg/day
(maximum dose, 320 mg/day).
IHSS: 20–40 mg tid or qid or 80–160 mg SR daily.
Arrhythmias: 10–30 mg tid or qid.
MI: 180–240 mg/day given tid or qid (maximum dose, 240
mg/day).
Pheochromocytoma: Preoperatively, 60 mg/day for 3 days in
divided doses; inoperable tumor, 30 mg/day in divided
doses.
51
Migraine: 80 mg/day daily (SR) or in divided doses; usual
maintenance dose, 160–240 mg/day.
Essential tremor: 40 mg bid; usual maintenance dose, 120
mg/day (maximum dose, 320 mg/day)
Parenteral
WARNING: IV dose is markedly less than oral because of first-
pass effect with oral propranolol.
Life-threatening arrhythmias: 1–3 mg IV with careful
monitoring, not to exceed 1 mg/min; may give second dose
in 2 min, but then do not repeat for 4 hr.
PEDIATRIC PATIENTS
Safety and efficacy not established.
Therapeutic actions
Propranolol competitively blocks β1- and β2-receptors
resulting to decreased heart rate myocardial
contractility, BP and myocardial oxygen demand. It only
possesses membrane-stabilising properties.
Indications
Hypertension alone or with other drugs, especially
diuretics
Angina pectoris caused by coronary atherosclerosis
Idiopathic hypertrophic subaortic stenosis to manage
associated stress-induced angina, palpitations, and
syncope
52
Cardiac arrhythmias, especially supraventricular
tachycardia, and ventricular tachycardias induced by
digitalis or catecholamines
Prevention of reinfarction in clinically stable patients
5–21 days after MI
Pheochromocytoma, an adjunctive therapy after treatment
with an alpha-adrenergic blocker to manage tachycardia
before or during surgery or if the pheochromocytoma is
inoperable
Prophylaxis for migraine headache
Treatment of essential tremor, familial or hereditary
Unlabeled uses: Recurrent GI bleeding in cirrhotic
patients, schizophrenia, tardive dyskinesia, acute panic
symptoms, anxiety, CHF
Adverse effects
Cold extremities, insomnia, fatigue, dizziness, vivid
dreams, lassitude, nausea, constipation or diarrhoea,
vomiting, anorexia, stomach discomfort, impotence.
Weakness, paraesthesia, wheezing, pharyngitis,
bronchospasm. CNS disturbances at higher doses and mood
alterations. Thrombocytopenic purpura, agranulocytosis,
nonthrombocytopenic purpura, thrombocytopenia.
Depression, confusion, cognitive dysfunction, emotional
lability, fatigue, hallucinations.
Potentially Fatal: Heart failure, heart block and
bronchospasm.
53
Contraindications
Sinus bradycardia, cardiogenic shock, pulmonary oedema,
severe hyperactive airway disease, compensated cardiac
failure, Raynaud’s disease, hypoglycaemia, severe
haemorrhage, metabolic acidosis, severe peripheral
arterial disease, 2nd or 3rd degree heart block.
Pregnancy (2nd and 3rd trimesters).
Nursing considerations
Assessment
History: Allergy to beta-blocking agents, sinus
bradycardia, second- or third-degree heart block,
cardiogenic shock, CHF, bronchial asthma, bronchospasm,
COPD, hypoglycemia and diabetes, thyrotoxicosis, hepatic
impairment, pregnancy, lactation
Physical: Weight, skin color, lesions, edema, T;
reflexes, affect, vision, hearing, orientation; BP, P,
ECG, peripheral perfusion; R, auscultation; bowel sounds,
normal output, liver evaluation; bladder palpation; LFTs,
thyroid function tests; blood and urine glucose
Interventions
WARNING: Do not discontinue drug abruptly after long-term
therapy (hypersensitivity to catecholamines may have
developed, causing exacerbation of angina, MI, and ventricular
arrhythmias). Taper drug gradually over 2 wk with monitoring.
WARNING: Ensure that alpha-adrenergic blocker has been given
before giving propranolol when treating patients with
pheochromocytoma; endogenous catecholamines secreted by the
tumor can cause severe hypertension if vascular beta receptors
are blocked without concomitant alpha blockade.
54
Consult with physician about withdrawing drug if patient
is to undergo surgery (withdrawal is controversial).
Provide continuous cardiac and regular BP monitoring with
IV form. Change to oral form as soon as possible.
Give oral drug with food to facilitate absorption.
Teaching points
Take this drug with meals. Do not discontinue the
medication abruptly; abrupt discontinuation can cause a
worsening of your disorder.
If you have diabetes, the normal signs of hypoglycemia
(tachycardia) may be blocked by this drug; monitor your
blood or urine glucose carefully; eat regular meals, and
take your diabetic medication regularly.
You may experience these side effects: Dizziness,
drowsiness, light-headedness, blurred vision (avoid
driving or performing hazardous tasks); nausea, loss of
appetite (eat frequent small meals); nightmares,
depression (request change of your medication); sexual
impotence.
Report difficulty breathing, night cough, swelling of
extremities, slow pulse, confusion, depression, rash,
fever, sore throat.
55

B.1 MASLOW’S HIERARCHY OF NEEDS
56
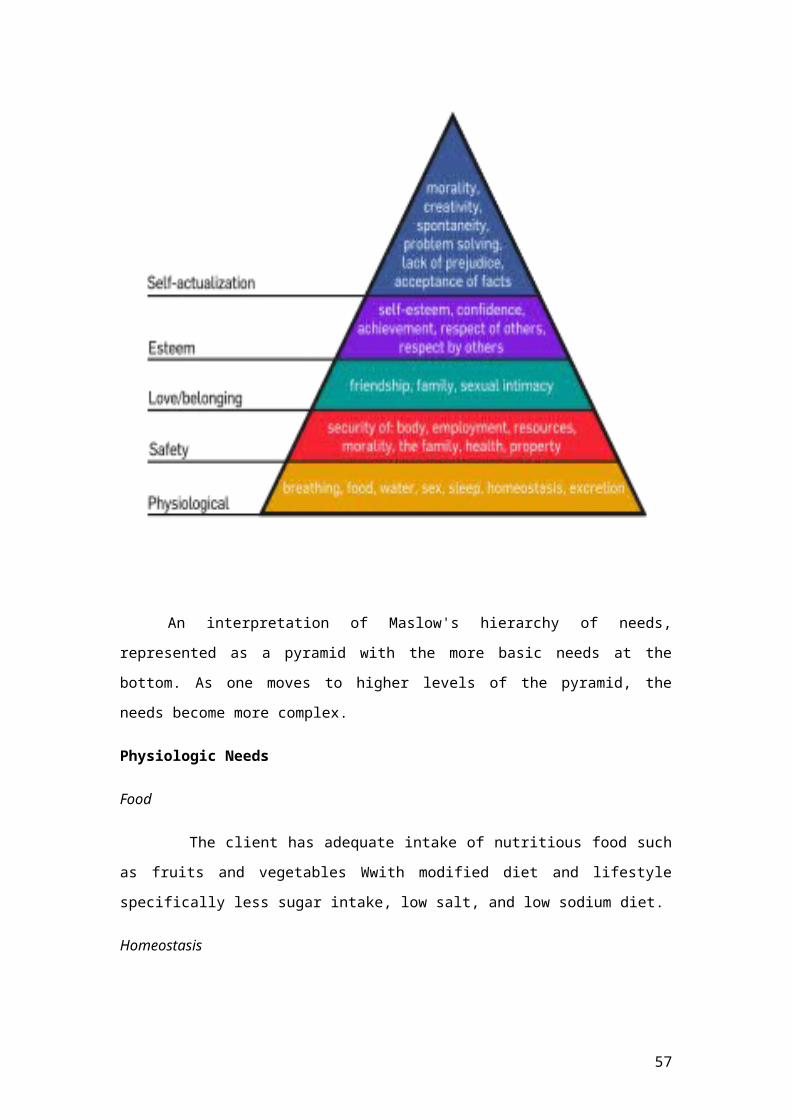
An interpretation of Maslow's hierarchy of needs,
represented as a pyramid with the more basic needs at the
bottom. As one moves to higher levels of the pyramid, the
needs become more complex.
Physiologic Needs
Food
The client has adequate intake of nutritious food such
as fruits and vegetables Wwith modified diet and lifestyle
specifically less sugar intake, low salt, and low sodium diet.
Homeostasis
57
The client usually suffers from fatigue or body
weakness as she lacks her sleep. She even experienced joints
pain most of the time that cause her interuuption from sleep
and unable to attain good sleeping pattern. As she experienced
fatigue and any discomforst, she’s unable to continue all the
household chores in the remaining hours of the day.
Shelter
Mrs. X’s house is made up of wood and some cement. As
we went and visited their house, we observed that the
structure of their house was already old yet it’s still clean,
well arranged with proper ventilation and sufficient
appliances. The only thing that concerns them most about their
house’s structure is the rooftop in which raindrops would
enter in their house during rainy season because of the
presence of the little holes.
Safety and Security
Prone to Flood
The setting of the house is safe but somehow, they are
prone to flood. Their house is built near the opened canals.
When the rain pours heavily water in the surroundings, there
will be an overflow of stagnant water especially from canal
areas. The ground of their house is also prone for the
overflowing rainwater. Thus, making the family vulnerable for
occurring any potential diseases from natural calamity like
usual floods.
Prone to Fire
Their house also is too narrow with other houses from
their neighbor. It may prone to any human unsafe occurrences
58
like fire disasters. Thereby, it would lead them to any health
and life hazards.
Health and Well-being Security
Mrs. X is 53 years old. Last 1996, she was diagnosed with
Diabetes Mellitus by a doctor and was prescribed with specific
medications for DM which are Deptan (once a day), Metformin
(three times a day), Carbas (twice a day) and antihypertensive
drug which are Propanolol, (three times a day) and Mediclamide
(three times a day). She was been supported by her family with
her basic necessities especially the need of drug
administration compliance and for the finances from the
doctor’s drug prescriptions.
Financial Security
The client is a simple housewife. She stays at home for
she can’t able to work for a long period of time but she can
do household chores but limited with physical activity. She
can’t work alone and do any activities for a long period of
time due to her condition. Her husband and her second child
had only their work who can earn money for about 10, 000-20,
000.
Property
The family does own their land or territory where their
house was built up and located. They lived there in Bucana
place for a long period of time, for about 30 years since
marriage.
Love and Belongingness
Family
59
Closely knit relationship with all the family members but
with readily acceptance and solution of any conflicts between
members of the family, including Mrs. X’s siblings who lived
nearby their house.
Self-esteem
Self-esteem is Moderate
When I conducted my interview to her, she is willing and
opene to be interviewed with her warm welcome. She is quite
conscious about the condition of their house and her
condition. But during the interview, she portrays confidence
and moderate self-esteem as still within her despite of
everything with her serious health condition.
Self-actualization
This is still an on-going process to reach the final
stage.
B.2 PROBLEM IDENTIFICATION
(Health Threat, Health Deficit, Foreseeable Crisis)
60
Health Threats
The roof and foundation of the house is strong enough to
support the house or can’t be immediately destroyed when
there will be calamities like flashfloods and
earthquakes. The little holes in the rooftop that
raindrops would enter into their house during rainy
season still their concern regarding their house’s
structure.
The location of the house is prone to flood since it is
just near the open canal that wasn’t well-managed which
sometimes smell so foul by the stagnant water. Mrs. X’s
flooring of the house is low in the ground that is prone
for overflowing of rainwater from flood.
They have proper storage of food like refrigerator or
food cabinets but their kitchen, comfort room, and
lavatory are near to each other. Thus, their food is
prone to contact with flies or other pests which might
cause other potential disease.
Their toilet facility is near their kitchen and lavatory
in which the kitchen was located in the middle of it.
There is possibility that flies from the toilet will come
in contact with their food when they are just preparing
or cooking for their meal. So, contamination might
probably occur.
Narrowed space between houses also served as the possible
health threat to the family especially it deals about
life involvement if there would be fire occurred in any
instances.
Health Deficits
61
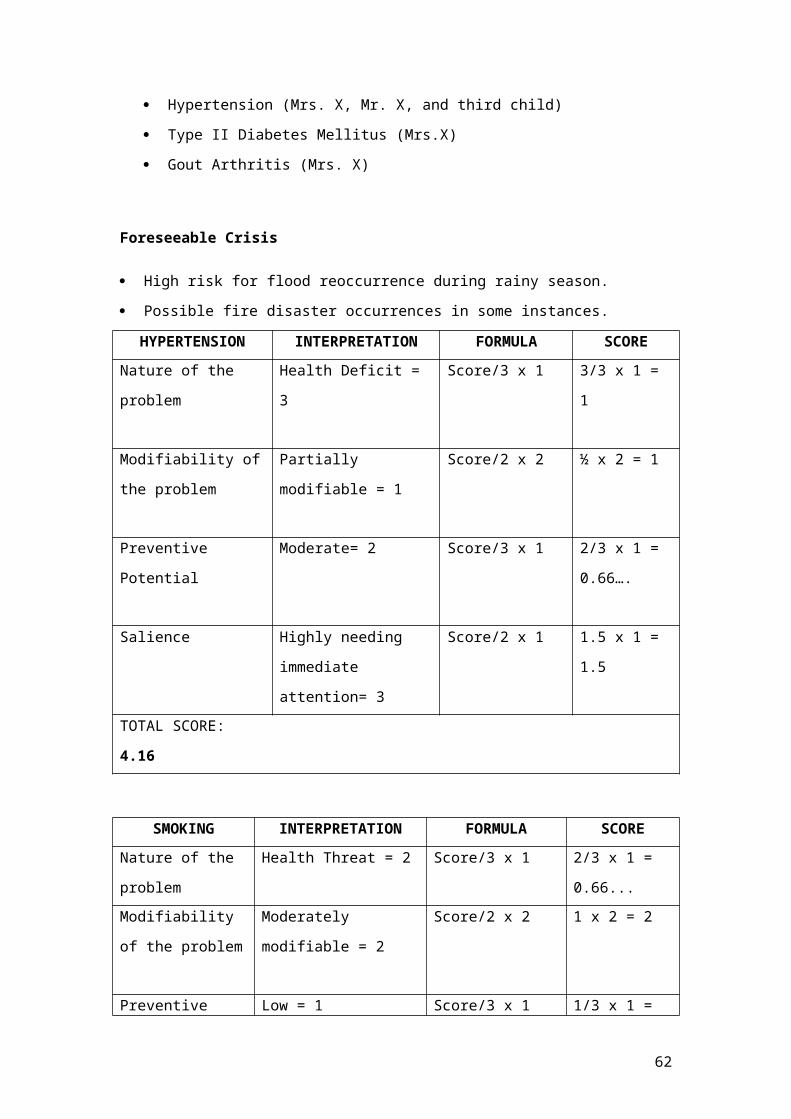
Hypertension (Mrs. X, Mr. X, and third child)
Type II Diabetes Mellitus (Mrs.X)
Gout Arthritis (Mrs. X)
Foreseeable Crisis
High risk for flood reoccurrence during rainy season.
Possible fire disaster occurrences in some instances.
HYPERTENSION INTERPRETATION FORMULA SCORENature of the
problem
Health Deficit =
3
Score/3 x 1 3/3 x 1 =
1
Modifiability of
the problem
Partially
modifiable = 1
Score/2 x 2 ½ x 2 = 1
Preventive
Potential
Moderate= 2 Score/3 x 1 2/3 x 1 =
0.66….
Salience Highly needing
immediate
attention= 3
Score/2 x 1 1.5 x 1 =
1.5
TOTAL SCORE:
4.16
SMOKING INTERPRETATION FORMULA SCORENature of the
problem
Health Threat = 2 Score/3 x 1 2/3 x 1 =
0.66...Modifiability
of the problem
Moderately
modifiable = 2
Score/2 x 2 1 x 2 = 2
Preventive Low = 1 Score/3 x 1 1/3 x 1 =
62
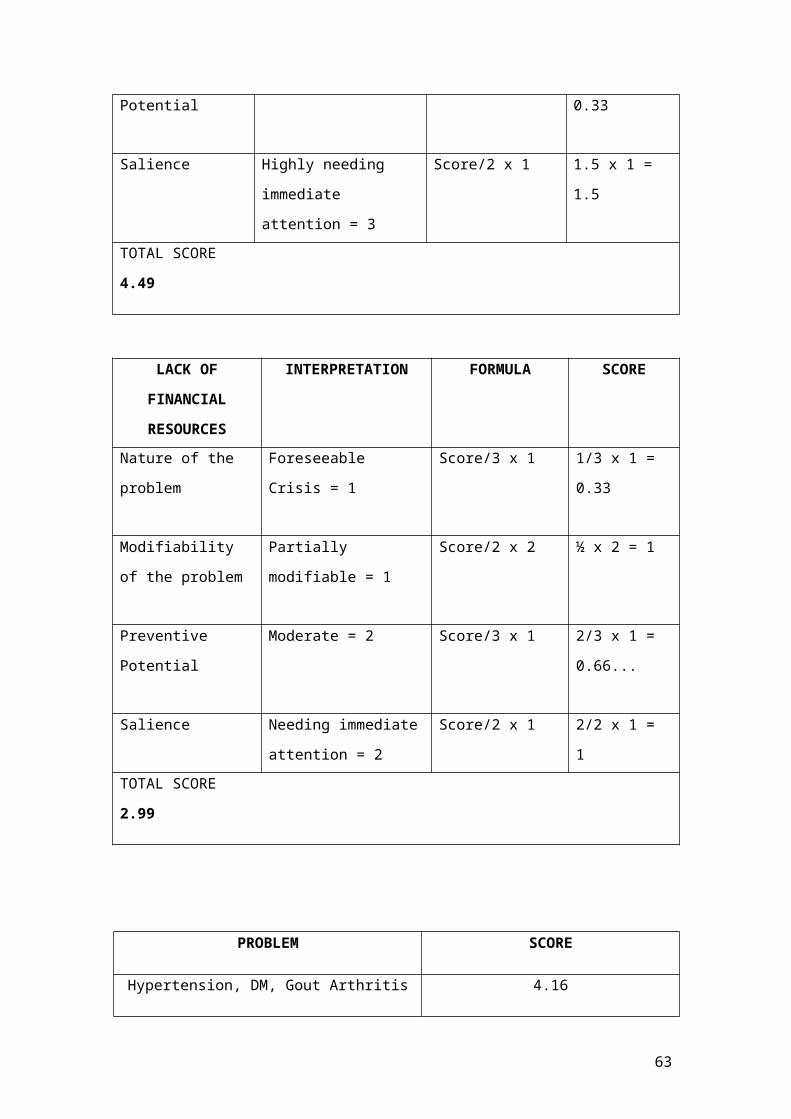
Potential 0.33
Salience Highly needing
immediate
attention = 3
Score/2 x 1 1.5 x 1 =
1.5
TOTAL SCORE
4.49
LACK OF
FINANCIAL
RESOURCES
INTERPRETATION FORMULA SCORE
Nature of the
problem
Foreseeable
Crisis = 1
Score/3 x 1 1/3 x 1 =
0.33
Modifiability
of the problem
Partially
modifiable = 1
Score/2 x 2 ½ x 2 = 1
Preventive
Potential
Moderate = 2 Score/3 x 1 2/3 x 1 =
0.66...
Salience Needing immediate
attention = 2
Score/2 x 1 2/2 x 1 =
1TOTAL SCORE
2.99
PROBLEM SCORE
Hypertension, DM, Gout Arthritis 4.16
63
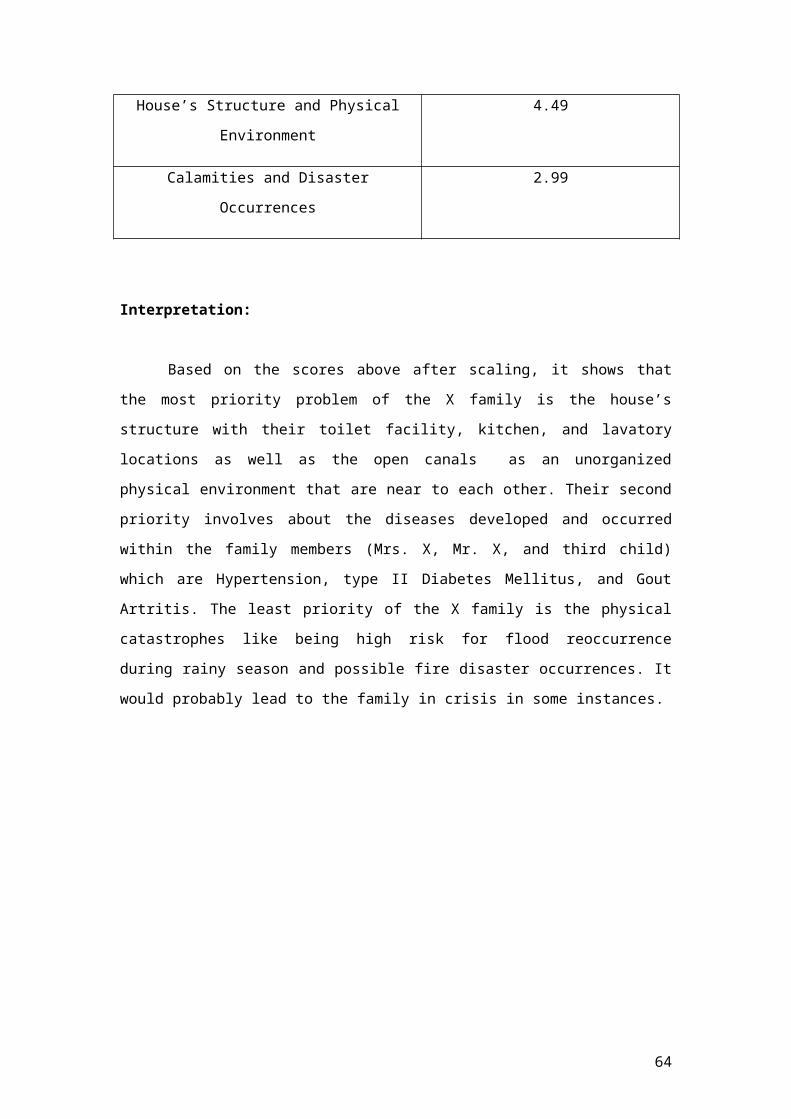
House’s Structure and Physical
Environment
4.49
Calamities and Disaster
Occurrences
2.99
Interpretation:
Based on the scores above after scaling, it shows that
the most priority problem of the X family is the house’s
structure with their toilet facility, kitchen, and lavatory
locations as well as the open canals as an unorganized
physical environment that are near to each other. Their second
priority involves about the diseases developed and occurred
within the family members (Mrs. X, Mr. X, and third child)
which are Hypertension, type II Diabetes Mellitus, and Gout
Artritis. The least priority of the X family is the physical
catastrophes like being high risk for flood reoccurrence
during rainy season and possible fire disaster occurrences. It
would probably lead to the family in crisis in some instances.
64
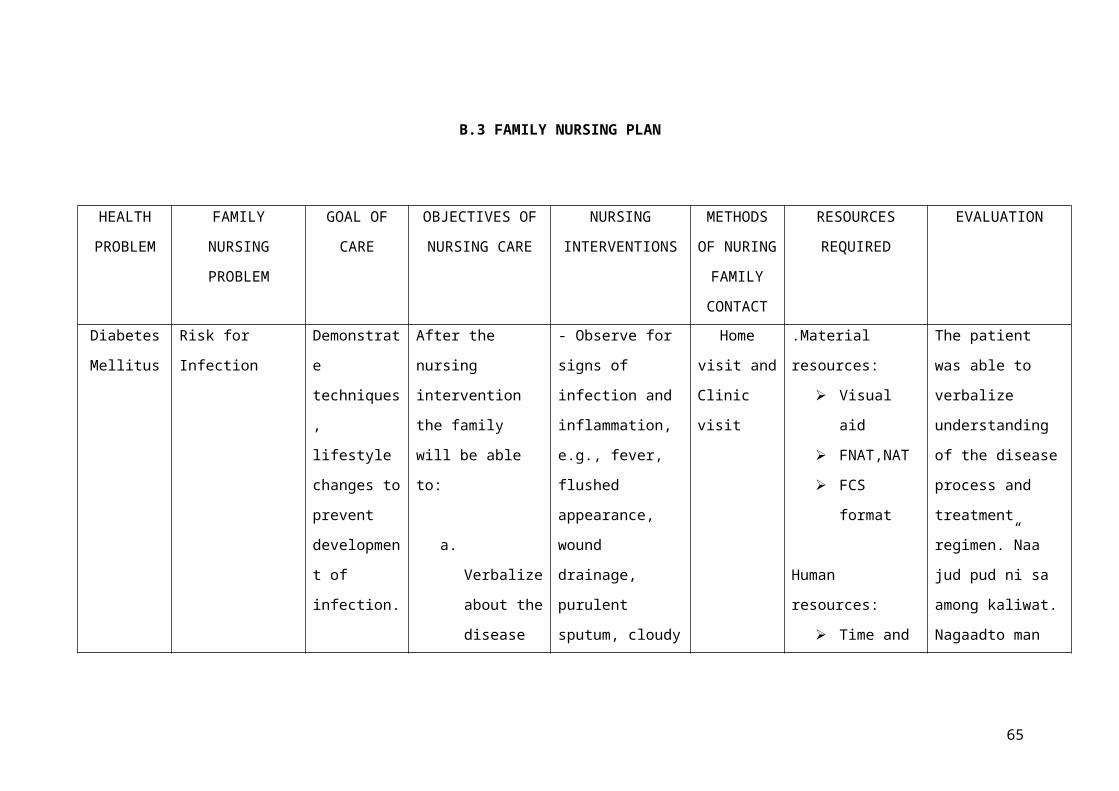
B.3 FAMILY NURSING PLAN
HEALTH
PROBLEM
FAMILY
NURSING
PROBLEM
GOAL OF
CARE
OBJECTIVES OF
NURSING CARE
NURSING
INTERVENTIONS
METHODS
OF NURING
FAMILY
CONTACT
RESOURCES
REQUIRED
EVALUATION
Diabetes
Mellitus
Risk for
Infection
Demonstrat
e
techniques
,
lifestyle
changes to
prevent
developmen
t of
infection.
After the
nursing
intervention
the family
will be able
to:
a.
Verbalize
about the
disease
- Observe for
signs of
infection and
inflammation,
e.g., fever,
flushed
appearance,
wound
drainage,
purulent
sputum, cloudy
Home
visit and
Clinic
visit
.Material
resources:
Visual
aid
FNAT,NAT
FCS
format
Human
resources:
Time and
The patient
was able to
verbalize
understanding
of the disease
process and
treatment
regimen.”Naa
jud pud ni sa
among kaliwat.
Nagaadto man
65
pocess
and
proper
complianc
e of the
treatment
regimen.
b. Identify
individua
l risk
factors
and
potential
intervent
ions to
reduce
infection
.
urine.
R: Patient may
be admitted
with
infection,
which could
have
precipitated
the
ketoacidotic
state, or may
develop a
nosocomial
infection.
- Increase
prevention
efforts by
effort of
the
student
nurse and
family/cl
ient.
Financial
resources:
Transportation
expenses of
the student
nurse to
conduct home
visit.
ko sa among
doctor ug
ginatumar nako
ang mga tambal
nga giresita
sa akong
doctor.
Nagalimit na
pud ko ug kaon
ug mga pagkaon
nga tam-is
kayo ug taas
ang asukal.
Nagalakaw-
lakaw lang pud
ko sulod sa
balay ug sa
silingan.”
66
c. Maintain
a safe
aseptic
environme
nt.
performing
good hand
washing, each
contact on all
items related
to the
patient,
including his
or her own
patients.
R: To
prevention of
nosocomial
infections.
- Provide
conscientious
skin care;
67
gently massage
bony areas.
Keep the skin
dry, linens
dry and
wrinkle-free.
R: Peripheral
circulation
may be
impaired,
placing
patient at
increased risk
for skin
irritation/bre
akdown and
infection.
68
- Encourage
adequate
dietary and
fluid intake
(approximately
3000 mL/day if
not
contraindicate
d by cardiac
or renal
dysfunction),
including 8 oz
of cranberry
juice per day
as
appropriate.
R: Decreases
susceptibility
69
to infection.
Increased
urinary flow
prevents
stasis and
aids in
maintaining
urine
pH/acidity,
reducing
bacteria
growth and
flushing
organisms out
of system.
Note: Use of
cranberry
juice can help
70
prevent
bacteria from
adhering to
the bladder
wall, reducing
the risk of
recurrent UTI.
HEALTH
PROBLEM
FAMILY
NURSING
PROBLEM
GOAL OF
CARE
OBJECTIVES OF
NURSING CARE
NURSING
INTERVENTIONS
METHODS OF
NURSING
FAMILY
RESOURCES
REQUIRED
EVALUATION
71
CONTACTPhysical
disarrangem
ent of
inner and
outer
housing
with
unmanaged
open
canals.
Inabilit
y to
recogniz
e the
presence
of
health
hazards
due to
less
action
facilita
ted and
inadequa
te
knowledg
e.
The
patient
will
verbalize
understand
ing of
developing
health
hazards
leading to
health
threat.
After nursing
intervention
the family will
be able to:
a. Define the
factors of
health
hazards
from
unorganize
d
physical/e
nvironment
al
arrangemen
t.
- Define and
state the common
factors that
could contribute
to health
hazards and
life-threatening
conditions.
R: Provides
basis for
understanding
the basic
factors leading
to unhealthy
condition.
- Assist the
patient in
Home visit
and
Clinic
visit
Material
resources:
Visual
aid
FNAT,NAT
FCS
format
Human
resources:
Time and
effort of
the
student
nurse and
family/cl
ient.
The
patient
was able
to
verbalize
“Maayo pud
kay
nagahinlo
name ug
tarong sa
among
palibot.
Nagasilhig
pud ko sa
gawas
ilabi na
sa mga
72
b. Explain
the
importance
of having
good
hygiene
and proper
environmen
tal
sanitation
inside and
outside
the house.
c. Showed
willingnes
s in
facilitati
ng and
identifying
desirable and
attainable plan
and solutions
for well
management of
open canals.
R: Formulated
plans and
actions helped
them to start
managing and
restoring the
open canals.
- Reinforce the
importance
proper
segregation of
Financial
resources:
Transportation
expenses of the
student nurse
to conduct home
visit.
basura nga
anaa dapit
sa mga
kanal duol
sa amo.”
73
restoring
the open
canals.
d. Showed
participat
ion in
different
resources
and
offered
community
services.
garbage.
R: Lack of
knowledge about
proper
segregation of
garbage and
proper
environmental
sanitation would
threaten one’s
life.
- Encourage the
family members
to clean up the
potential
breeding of
mosquitoes which
74
are the open
canals from time
to time.
R: To reduced
the number of
breeding
mosquitoes which
are dengue
carriers that
could harm the
residents lived
nearby the open
canals.
75
76
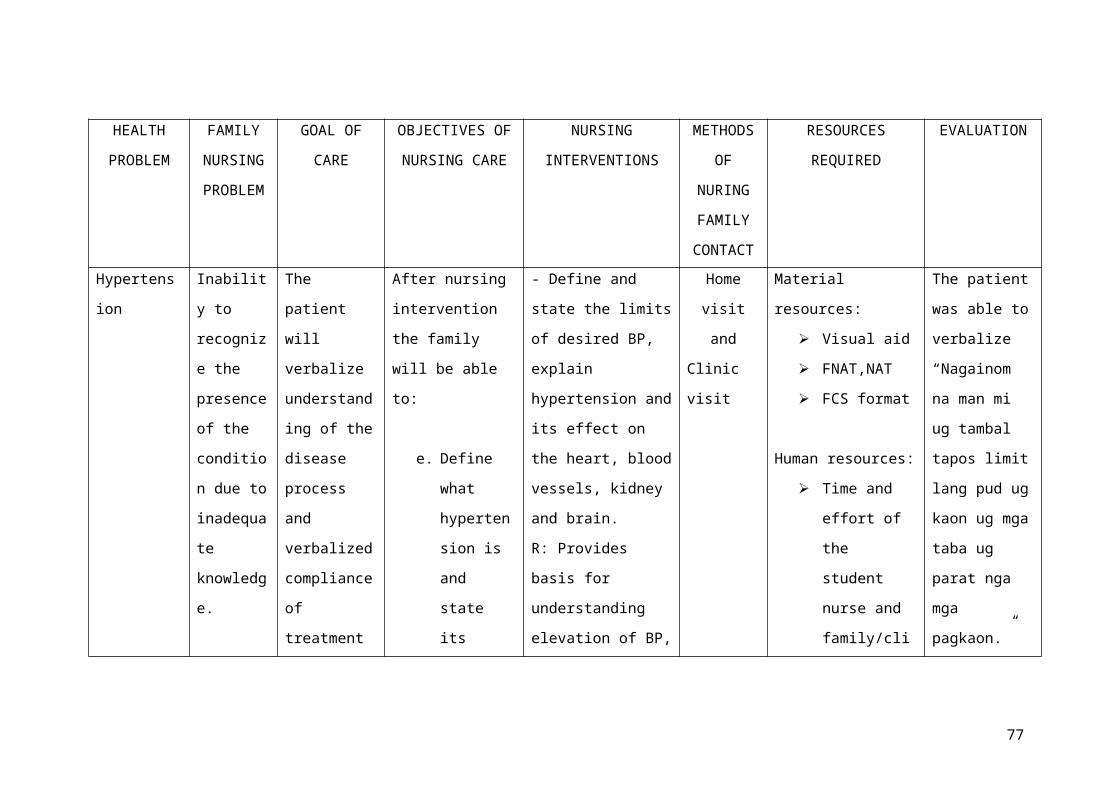
HEALTH
PROBLEM
FAMILY
NURSING
PROBLEM
GOAL OF
CARE
OBJECTIVES OF
NURSING CARE
NURSING
INTERVENTIONS
METHODS
OF
NURING
FAMILY
CONTACT
RESOURCES
REQUIRED
EVALUATION
Hypertens
ion
Inabilit
y to
recogniz
e the
presence
of the
conditio
n due to
inadequa
te
knowledg
e.
The
patient
will
verbalize
understand
ing of the
disease
process
and
verbalized
compliance
of
treatment
After nursing
intervention
the family
will be able
to:
e. Define
what
hyperten
sion is
and
state
its
- Define and
state the limits
of desired BP,
explain
hypertension and
its effect on
the heart, blood
vessels, kidney
and brain.
R: Provides
basis for
understanding
elevation of BP,
Home
visit
and
Clinic
visit
Material
resources:
Visual aid
FNAT,NAT
FCS format
Human resources:
Time and
effort of
the
student
nurse and
family/cli
The patient
was able to
verbalize
“Nagainom
na man mi
ug tambal
tapos limit
lang pud ug
kaon ug mga
taba ug
parat nga
mga
pagkaon.”
77
regimen effects
on the
heart,
blood
vessels,
kidney
and
brain.
f. Explain
the
importan
ce of
having
healthy
lifestyl
e.
g. Showed
willingn
and clarifies
misconception.
- Assist the
patient in
identifying
modifiable risk
factors like
diet high in
sodium,
saturated fats
and cholesterol.
R: These risk
factors have
been shown to
contribute
hypertension.
ent.
Financial
resources:
Transportation
expenses of the
student nurse to
conduct home
visit.
78
ess to
particip
ate
differen
t
resource
s in
controll
ing
hyperten
sion.
- Reinforce the
importance of
adhering to
treatment
regimen and
keeping follow
up appointments.
R: Lack of
cooperation is
common reason
for failure of
antihypertensive
therapy.
- Encourage
patient to
decrease or
eliminate
79
caffeine like
coffee, cola,
and chocolates.
R: Caffeine is a
cardiac
stimulant and
may adversely
affect the
cardiac
function.
80
B.4 HEALTH TEACHINGS
(3 Levels of Prevention)
Primary Prevention
A term sometimes used, related to primary prevention, is
"primordial prevention," which refers to creating an environment
where certain challenges to health are eliminated. Primary
prevention relates to general knowledge that is applicable to the
client and the rest of the family members upon assessment and
identification of risk factors causing disequilibrium. Groups at
risk for diabetes include those with high levels of sugar and a
family history of it associated with hypertension.
Diet
Encourage the family members to eat a well-balanced diet,
minimizing the intake of high sugar, fatty, oily and salty
foods. Emphasize that Diabetes Mellitus and Hypertension are a
heredofamilial diseases that affect the other vital organs,
resulting to dysfunction and further complications.
Exercise
Educate the family members the importance of increasing
physical activity (30-45 minutes most days of the week) like
brisk walking which promotes proper blood circulation. Regular
exercise has been shown to be a powerful tool in promoting
proper blood circulation and the prevention of hypertension.
Unhealthy Habits
81
Educate the family members on the disadvantages of high intake
of sweets, sodium, and high fatty foods with its effects to
the body.
Sleep/Rest Pattern
Emphasize to the family members that each of them must have an
adequate rest or sleep everyday which is very important to
prevent fatigue, exhaustion and stress that can be a
predisposing factor to some diseases like diabetes and
hypertension. It would help them to conserve more of their
energy and ability to do household chores or outdoor
activities enthusiastically.
Proper Hygiene and Sanitation
1. Teach the family members the importance of proper hand
washing and its benefit to our health.
2. Emphasize the importance of exposing the pillows and foams
to the sunlight for technique of sterilization.
3. Teach the family members the importance of proper waste
disposal or having a proper environmental sanitation.
4. Teach the family members about oral care and proper
grooming.
5. Tell client to cover the water containers as well as to
cover their garbage containers.
6. Teach the family to facilitate for proper management of open
canal areas.
Secondary Prevention
82
Secondary prevention refers to the prevention of clinical
illness through the early and asymptomatic detection and
remediation of certain diseases and conditions that, if left
undetected, would likely become clinically apparent and harmful.
This is often referred to as "screening." Secondary prevention
relates to symptomatology following a reaction to stressors,
appropriate ranking of intervention priorities, and treatment to
reduce their noxious effects.
So, the following are the recommended health education or
health teaching in this category of prevention.
Encourage the family members to have their blood pressure
check at least once a week since the mother and father as
well as the third child is known hypertensive. Encourage the
family to limit high intake of sweet and salty foods as they
are likely to have this diseases because these are also
heredofamilial diseases. Early detection is very necessary.
Teach the female family members how and when to do fasting
blood glucose test for the sugar level in the blood within
the body.
Teach the family to do or perform blood pressure taking at
least once awake for the close monitoring and update of
their follow-up regular check-up.
Tertiary Prevention
Prevention of disease progression and additional disease
complications after overt clinical diseases are manifested. This
is generally the province of physicians and other health
83
professionals, who manage acute and chronic conditions. Tertiary
prevention concentrates on the readjustment toward optimal
patient stability. The paramount goal is to increase the
resistance to identified stressors or decrease stressors to help
prevent reoccurrence of illness. This process moves the client
back in a circular manner toward primary prevention. For the
purpose of this study, concepts of Neuman’s (1998) model provided
information to patients diagnosed with DM and Hypertension in
order to assist them toward restoring their health and optimal
stability. This is the goal of tertiary prevention. The focus of
this prevention is on the mother of the family which was
diagnosed of Type II Diabetes Mellitus last 1996.
Tell the client to increase physical activity (30-45 minutes
most days of the week) like brisk walking or just doing the
household chores for proper blood circulation.
Emphasize to the client the importance of reducing lessen
the high sugar intake as well as the sodium intake or to
have a low salt diet, in any case, salt should not exceed
more than three grams or about half a teaspoon per day.
The sugar can be lessen by restricting high intake of sweet
foods and the pressure can be lowered and blood clotting
diminished by increasing the consumption of fruits, reducing
protein intake, and sticking to a vegetarian diet. A natural
diet consisting of fresh fruits and vegetables instead of a
traditional diet helps to get rid of the toxins from the
body.
Persons suffering from DM and Hypertension as well as Gout
Arthritis must get at least eight hours of good sleep,
84
because proper rest is a vital aspect of the treatment. Most
important of all, the patient must avoid overstrain,
worries, tension, anger, and haste. He or she must develop a
calm and cheerful attitude and develop a contented frame of
mind.
Emphasize to the client to have a regular medical checkups,
to take her medicines faithfully, to follow her doctor's
recommendations about diet and exercise and to talk to the
health care team in their health center if she has any
health concerns and questions or problems about health
services that were carried out.
Encourage the client to get her whole family involved in her
care plan as well as to remind the other family members how
important it is to be sensitive to client’s present
situation.
SUMMARY/ EVALUATION
Nursing Education enhances the skills and personality of
every individual. Knowing Community Organizing and Participatory
Action Research (COPAR) is very significant for us. The kind of
community organizing that does not merely deals on the shallow
aspect of community health but immerses student to delve deeper
to fully understand the essence of community organizing with the
establishment of self-reliance to residents in the covered
85
community. Before going into the community we need to collaborate
first with the head of the barangay so that every activity that
will be implemented will be legal. Through courtesy call we will
be able to gain trust and cooperation from the community, it is
also form of respect that would facilitate good working
relationship between the community and the community organizers
or students.
As we went into the community we have interviewed the
families as our assigned clients and conducted activities in
order to determine the common problems existing in their
community and formulate community diagnosis from the gathered
data. We facilitated them and they are responsible enough to find
solutions to their problems. They have shared some of their
important-feature of their lives and fully trusted us with that.
They must have cooperation and unity to achieve a desire goal
especially in taking care of their health as the important gift
that God had given us. When communicating with the head of the
family we need to use words that they understand, so usually the
mother tongue, and give time for them to answer the questions and
also listen attentively to show politeness and obtain more
rapport. These would also allow us to get accurate data or
information. Utilization of nursing process in different level of
clientele-individual, families, population groups and community
concerned with the promotion of health, prevention of diseases
and disability and rehabilitation.
In our ocular survey to the community of Purok 6-A, Barangay
76-A, Bucana, Davao City, we observed that they are prone to
certain disease occurrences because of the improper environmental
86
sanitation especially the stagnant water of the open canal that
wasn’t well-managed. The chance of helping these people and do
good works is in our hand. So as we implement our activities to
the community of the said place, some people living there were
participative in responding our invitation but few are active in
implementing the planned action regarding the cleaning operation
or general clean-up conducted by the nursing students on
September 19, 2013. Some of our activities include their assembly
or a call for gathering the residents, bag technique, values
education to children, action planning of proper environmental
sanitation. We conducted problem identification in which the
people were able to identify and suggest solutions from it.
Aside from that, we conducted a series of health teaching that
includes common illnesses occurring in a within the family with
their acquired diseases like Diabetes Mellitus and Hypertension.
We also gave another health education and health teaching in the
community by having the dengue awareness program in relation to
proper environmental sanitation. At the end of every duty we had
in the community Purok 6-A, Barangay 76-A, Bucana area, we felt
fulfilled because every activity was successfully implemented
with the cooperation of the other households or residents.
Camaraderie and cooperation of the group contributed to the
success of the case study. We distributed the task of each of the
members equally in which they provide accurate and well-
validated information and data that are necessary for the success
of the case. At the end of this duty, new insights will be added
and it will improve our knowledge when it comes to community
87
health nursing and community organizing with participatory action
research.
IMPLICATION OF THE STUDY
NURSING EDUCATION
The nursing family case study enlightens us to the real
scenario in the community. It also gave us the opportunity to
know that Community Organizing and Participatory Action Research
(COPAR) is important so that nursing students would be able to
experience how it works. The availability of health services is
necessary in the community. It gave us the view that every
community must have enough and available public health nurses to
accommodate each family.
The maintenance of the ability of both public health
agencies and private provides to manage day to day operations and
the capacity to respond immediately to the community should
always be accessible.
Through nursing individual family case study and community
diagnosing, we were able to assess the health needs of the
family, plan, implement, and evaluate the impact of health
services in the community. It gave us the basic knowledge and
skills in Community Organizing and Participatory Action Research
(COPAR) from Community Health Nursing (CHN) that one could
formulate policies and develops on nursing aspect of specific
88
program such as health education or health teaching about pre-
existing illnesses and potential diseases.
NURSING PROFESSION
In the nursing profession, competence, credibility,
commitment and knowledge are needed in the profession. The
dedication of a nurse to serve in the community is remarkable and
outstanding. However, nurses must continuously enhance their
knowledge and skills to explore the capability to be used in the
community.
The nurse and the community must collaborate in order to
achieve the nursing intervention when dealing with diseases like
Diabetes Mellitus, Hypertension, and any other common diseases.
This nursing case study will give the public health nurse the
awareness of how the community does the home management in their
disease.
For a nurse should enhanced the knowledge like political
science or environmental science and any other things related to
dealing with people, it helps the nurses to understand the health
care delivery system for them to better respond to clients and
use academic principles like sociology and psychology to know
better on how to understand the community.
NURSING RESEARCH
This research found out that the assigned household in the
community resolve to deal with DM, Hypertension, and Gout
89
Arthritis on their own seeking medical assistance and help to
their family physician. The researches therefore recommend that
future studies in those existing cases of diseases especially in
the community should focus on determining tangible ways to
educate the people about the disease and the value of medical
treatment in general.
HEALTH UPDATES
What to Eat After a Diabetes Diagnosis
By The Daily Meal | Shine Food – Mon, Sep 16, 2013 11:38 PM PHT
The Centers for Disease Control aren't painting a pretty
picture these days.
The latest statistics show that diabetes affects 25.8
million people in the United States alone, or about 8 percent of
the population. That's quite an alarming figure, especially when
it seems like healthy eating is a huge focus for many people
these days. But others may not realize just how serious a problem
diabetes can be. Diabetes results in a number of other serious
health conditions, including kidney failure, non-traumatic lower-
limb amputations, and even blindness among adults - in fact, it
is the number one cause of these conditions in the United States.
It is also a contributing factor to heart disease and stroke.
90
Diabetes is a disease of the pancreas, the organ responsible
for insulin production. Without its proper functioning, glucose,
the body's source of fuel, can't enter cells, and essentially
results in a condition that can be characterized as starvation
from the inside out. Instead, sugar begins to accumulate in the
bloodstream, and side effects such as constant itching and
thirst, frequent urination, fatigue, and even blurry vision begin
to manifest.
There are two types of diabetes. Type 1 diabetes is an
autoimmune disorder, meaning the body destroys the cells in the
pancreas that produce insulin. People with type 1 diabetes make
no insulin and need to take insulin injections about four times a
day. They are usually diagnosed in childhood and continue to live
with the disorder for the rest of their lives.
With type 2 diabetes, the onset occurs more often in middle
age, and differs from type 1 diabetes in that insulin is still
produced, but cells have become resistant to it and no longer
respond properly. Furthermore, insulin resistance is also
accompanied by insulin deficiency - people with type 2 diabetes
make less insulin than healthy individuals.
A genetic component figures more prominently into type 2
diabetes than type 1 diabetes, but the key takeaway is that type
2 diabetes can sometimes be prevented. We spoke with Donna
Gebert, MPH, a certified diabetes educator affiliated with Novo
Nordisk, a company that specializes in diabetes care, and whose
history includes the first use of insulin as a diabetes
treatment. Gebert helps physicians take care of their patients by
91
offering nutrition and health advice related to diabetes, and has
worked as a dietitian in outpatient care for more than 15 years.
She says it is now possible to diagnose "pre-diabetes" using
some special blood tests that nip the problem in the bud just
before anything goes seriously wrong. A pre-diabetes diagnosis is
returned when tests reveal current and historic fasting blood
sugar levels to be just below the threshold for a full-blown
diabetes diagnosis.
In her experience, people who are overweight and have a pre-
diabetes diagnosis can often prevent the onset of type 2 diabetes
and see a significant reduction in their fasting blood sugar
levels just by losing approximately 5 percent of their body
weight over a period of three months. This is a result achieved
by a change in lifestyle - namely, a switch to a high-fiber diet
with emphasis on eating more vegetables, and exercise.
Not exactly stuff that anyone hasn't heard before. But, it's
what really works. She estimates about 80 to 85 percent of the
patients who have a pre-diabetes diagnosis and fail to do this go
on to develop type 2 diabetes.
That's staggering. But as always, the devil is in the
details. What, exactly, is one to do after the diagnosis? Gebert
offers some sound advice, as well as tips on specific
substitutions for favorite foods. These guidelines are also
useful for those who have already been diagnosed with diabetes
and need to manage their condition.
Rice
92
Some patients have hard time giving up pasta, some have
trouble with grits, and others, rice. Brown rice is the way to go
since it contains more fiber than processed rice and slows the
release of sugar into the bloodstream. Gebert says just to be
careful of portion sizes. One cup of cooked rice contains 45
grams of carbs, or about three servings. Women should only have
three to four servings of carbs in one meal, while men should
only have about four to five servings - so that one cup of cooked
rice might be it for the whole meal. No more carbs after that.
Milk, the Dark Horse in the Room
This one sometimes surprises patients. Milk contains
lactose, a sugar that is found in dairy products. When broken
down by the body, however, it all turns to glucose, which can
mean a spike in blood sugar levels. Gebert says that milk is OK
to drink, but make sure to limit it to just two 8-ounce servings
per day. Since most cups these days are much larger than 8-
ounces, she says that it's a good idea to purchase a measuring
cup.
REACTION
I like this research journal which deals about the
prevention or the promotion of healthy diet and lifestyle to
diabetic persons after the diabetic diagnosis. As provided and
supported by the research data above, the latest statistics show
that diabetes affects 25.8 million people in the United States
93
alone, or about 8 percent of the population. That's quite an
alarming figure, especially when it seems like healthy eating is
a huge focus for many people these days. Somehow, this disease
condition is a lifelong process in which persons that had already
this kind of disease and it’s developing would feel and take it
as a big burden to their side. It leads to further complications
and the major contributing factor to heart disease and stroke.
Thereby, it leads to further organ damage and vital organs’
dysfunction. So, unhealthy diet and lifestyle must be modified
into healthy adjustments. That’s why, brown rice was recommended
for it is the way to go since it contains more fiber than
processed rice and slows the release of sugar into the
bloodstream. Milk was also advisable but it needs to be limited,
making sure to limit it to just two 8-ounce servings per day in
order to lessen the glucose intake since it is still has sugar
content. So, taking carefully of the food to be eaten with
portion of sizes is deemed necessary and carefully monitored!
Hence, health promotion and disease prevention is always better
than cure.
94
REFERENCES
Khardori, R., et. al. (2010). Type 2 Diabetes Mellitus Treatment
& Management. Retrieved on September 10, 2013 from
http://emedicine.medscape.com/article/117853-treatment
American Diabetes Association. (2011). Standards of Medical Care
for Patients With Diabetes Mellitus. Retrieved on September 10,
2013 from
http://care.diabetesjournals.org/content/25/suppl_1/s33.full
95
American Diabetes Association. (2013). Diseases and Conditions.
Retrieved on September 10, 2013 from
http://my.clevelandclinic.org/disorders/Diabetes_Mellitus/hic_Dia
betes_Mellitus_An_Overview.aspx
Gaces, V. (2008). Common Laboratory Tests Performed to Confirm
Diagnosis of Diabetes Mellitus. Retrieved on September 11, 2013
from http://voices.yahoo.com/common-laboratory-tests-performed-
confirm-diagnosis-2383835.html
Mayo Clinic staff. (2012). Diabetes. Retrieved on September 11,
2013 from
http://www.mayoclinic.com/health/diabetes/DS01121/DSECTION=tests-
and-diagnosis
The Daily Meal. (2013). What to Eat After a Diabetes Diagnosis.
Retrieved on September 11, 2013 from
http://ph.she.yahoo.com/blogs/shine-food/eat-diabetes-diagnosis-
153800282.html
96