clinico-pathologic features of primary melanoma and sentinel lymph node predictive for non-sentinel...
TRANSCRIPT
lable at ScienceDirect
Surgical Oncology xxx (2010) 1e6
Contents lists avai
Surgical Oncology
journal homepage: www.elsevier .com/locate/suronc
Review
Clinico-pathologic features of primary melanoma and sentinel lymph nodepredictive for non-sentinel lymph node involvement and overall survivalin melanoma patients: A single centre observational cohort study
P. Quaglino a,*,1, S. Ribero c,1, S. Osella-Abate a, L. Macrì b, M. Grassi c, V. Caliendo c, S. Asioli b, A. Sapino b,G. Macripò c, P. Savoia a, M.G. Bernengo a
aDepartment of Biomedical Sciences and Human Oncology, Section of Dermatology, 1st Dermatologic Division, University of Turin, Italyb Section of Surgical Pathology University of Turin, Italyc Section of Dermatologic Surgery, Oncology and Haematology Department, San Giovanni Hospital Turin, Italy
a r t i c l e i n f o
Article history:Accepted 3 November 2010
Keywords:MelanomaOverall survivalNon-sentinel lymph nodes
* Corresponding author.E-mail address: [email protected] (P. Quagli
1 Both authors contributed equally.
0960-7404/$ e see front matter � 2010 Elsevier Ltd.doi:10.1016/j.suronc.2010.11.001
Please cite this article in press as: Quaglino PSurgical Oncology (2010), doi:10.1016/j.suro
a b s t r a c t
Objective: Completion Lymph Node Dissection (CLND) is the current standard of practice for patients witha positive Sentinel Lymph Node Biopsy (SLNB). Significant morbidity is associated to CLND, so we tried toevaluate which prognostic variables could predict NSLN invasion in SLN-positive patients and theirimpact on the overall survival (OS).Methods: A retrospective chart review of 603 patients that had undergone SLNB for melanoma between2000 and 2009 at our department was done. 100 SLN were positive at the histopathological analysis ofSLN. Demographic variables, primary melanoma, SLN pathologic features and results of CLND wereanalysed. Multivariate logistic regression and OS analyses were carried out to test the prognostic rele-vance of clinico-pathologic variables on CLND results and disease course.Results: Breslow thickness, ulceration and micro/macrometastatic pattern of SLN invasion carrieda significantly independent higher likelihood of NSLN involvement; Starz classification did not maintaina statistical significance in multivariate analysis. Only one patient (4.3%) without adverse prognosticfactors showed NSLN involvement, which was found in 33.3% of patients with one and 55.9% with two ormore adverse parameters (p ¼ 0.0001). OS analyses confirmed the prognostic significance of thesefactors.Conclusion: Waiting for the results of Multicenter Selective Lymphadenectomy Trial II, our study suggestsa clinically useful and easily applicable means of identifying patients with an unfavourable diseasecourse. The presence of one or more adverse factors identifies patients in whom CLND is mandatory toinclude thereafter in a more strict follow-up program. Moreover, the finding of no adverse prognosticindicators associated to the presence of significant co-morbidities and/or elderly age, could be useful inidentifying patients not to treat by CLND.
� 2010 Elsevier Ltd. All rights reserved.
Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Materials and methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Patients, lymphatic mapping, sentinel lymph node biopsy and completion lymphadenectomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Statistical analyses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Clinico-pathologic variables associated to NSLN involvement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Overall survival . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
no).
All rights reserved.
, et al., Clinico-pathologic features of primary melanoma and sentinel lymph node predictive for...,nc.2010.11.001

P. Quaglino et al. / Surgical Oncology xxx (2010) 1e62
Conflict of interest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Authorship statement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Uncited reference . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
Introduction
Since the introduction of sentinel lymph node biopsy (SLNB)from Morton et al. [1] in early 1990s for patients with melanoma,this approach has been established as a diagnostic procedure inmelanoma. SLNB represents the to-date most accurate stagingprocedure for the early identification of regional node metastases.Micrometastases in sentinel lymph node are prognostically signif-icant in melanoma [2] and were therefore included in the revisedAmerican Joint Committee on Cancer (AJCC) Classification [3]. Thefinding of a positive SLN identify patients who might benefit fromcompletion lymph node dissection (CLND) [4]. However, CLNDcarries significant morbidity [5,6] and there is no consensus on thebenefit of a completion dissection in melanoma patients. In factreports in the literature showed that only from 14 to 28% [7e11] ofpositive patients will harbour further disease in the affected basin.Theoretically, only patients with involvement of additional, non-sentinel lymph nodes (NSLN) in the CLND specimen should benefitfrom a CLND. This suggests that a large percentage of patients mayundergo an unnecessary, morbid procedure for no apparent gain[12e16]. Recent efforts have been made to identify those patientsleast likely to have a metastatic disease in the NSLN, who maypotentially avoid a further surgical operation [17e21].
The objective of this study was to identify which clinico-path-ologic features of primary melanoma and SLN are predictive forNSLN involvement and to further ascertain their prognostic role byassessing their relationship with the clinical course in terms of OS.
Materials and methods
Patients, lymphatic mapping, sentinel lymph node biopsy andcompletion lymphadenectomy
SLNB was performed in 603 primary melanoma patients in ourDepartment from January 2000 until March 2009, the follow-upwas extended until December 2009. An SLN involvement wasfound in 100/603 patients (16.6%). Patients were enrolled on thebasis of guideline criteria [3,22e24]. SLN was performed in thepresence of melanoma >1 mm, or even lower if ulcerated or ClarkIVeV or presence of mitoses more than or equal to 1/mm2. SLNBwas not performed in patients aged more than 75 years. Staging forvisceral occult metastases before SLNB was performed according tonational Italian guidelines [22]. Patients with primary melanomaless than or equal to 2 mm without ulceration underwent chestX rays and abdomen ultrasound, whereas patients with deeperBreslow thickness performed brain, lung and abdomen computedtomography (CT). At the time of SLNB, there was no clinical orradiological evidence of melanoma metastases.
The SLNs were detected by lymphoscintigraphy and patent bluedye. All radio-labeled lymph nodes were considered to be SLN andexcised. A median number of 2 sentinel nodes (range: 1e4) wereremoved. SLNs were fixed in formaldehyde and bisected along thelong axis of the ilar region [25]. Depending of its size, the bisectednodes were embedded in one or more paraffin blocks. Paraplastsections at five intervals of 50 mmwere prepared from each paraffinblock. From each paraplast section, four slides were made and
Please cite this article in press as: Quaglino P, et al., Clinico-pathologic feaSurgical Oncology (2010), doi:10.1016/j.suronc.2010.11.001
stained with conventional histopathology (hematoxylin-eosin) andimmuno-hystochemistry (S-100 and HMB-45).
The pattern of SLN involvement was defined as macro- ormicroscopic on the basis of the presence or absence, respectively, ofgross extracapsular extension [3].
The penetration depth was measured with an ocular microm-eter as maximum distance of tumour cells from the interior marginof the lymph node capsule, as described by Starz et al. [17]. Presenceof tumour cells up to 0.3 mm was classified as Starz-I, invasionbetween 0.3 mm and 1.0 mm was Starz-II, and a deeper invasionmeant Starz-III. The NSLN were analysed only with H&E.
Patient’s characteristics included: 1) demographic data (sex,age); 2) histologic features of the primary melanoma (Breslowthickness, Clark level, histologic subtype, ulceration); 3) data fromthe SLN included: number of SLN removed, number of positiveSLNs, localisation of SLN (head/neck, axilla, inguinal), pattern ofinvasion (micro-/macro-metastases), depth invasion of metastaticcells in the SLN (Starz Classification 2004) [17]. The mitotic rate wasrecorded for all patients but it was not taken into consideration forthis study purposes in as much as according to the updated AJCCclassification [3] was not shown to carry a prognostic relevance inthe disease outcome of stage III patients.
Statistical analyses
Statistical analyses were performed using the SPSS 17 StatisticalSoftware. Both parametric and non-parametric tests were used;only “p” values of parametric tests were reported, as the results ofthe two tests were similar. Univariate and multivariate logisticregression were used to test for the significance of the predictorvariables’ association with NSLN metastases. Overall survival (OS)was calculated from the surgical excision of SLN to the date of deathor last check-up for all patients. Survival estimates were derived bythe KaplaneMeier method [26] and the statistical comparison wasdone by the log-rank test [27]. Univariate analyses were carried outto evaluate the prognostic role of different variables.
Results
Clinico-pathologic variables associated to NSLN involvement
Patients characteristics with regard to clinical data, primarymelanoma, SLN and CLND are given in Table 1 according to thepresence of NSLN involvement which was detected in 31 out of 100of patients (Table 1).
Univariate logistic regression showed that the parametersassociated with a higher likelihood of NSLN involvement wereBreslow thickness, ulceration, micro-/macro-metastatic patternand Starz classification. In particular, the odds ratio (OR) was 1.52for Breslow thickness, 4.59 for ulceration, 6.42 for themicro/macro-metastatic pattern and 2.32 for the Starz classification [17](Table 2). The highest percentages of NSLN involvement werefound in patients with Breslow thickness >4 mm (52%), ulceration(53.6%), macro-metastatic pattern (70%) and grade III Starz classi-fication (40%). On the other hand, NSLN involvement after a positiveSLN was found in 11.5% of patients with thin primary (between 1and 2 mm) and 5.5% Starz I.
tures of primary melanoma and sentinel lymph node predictive for...,
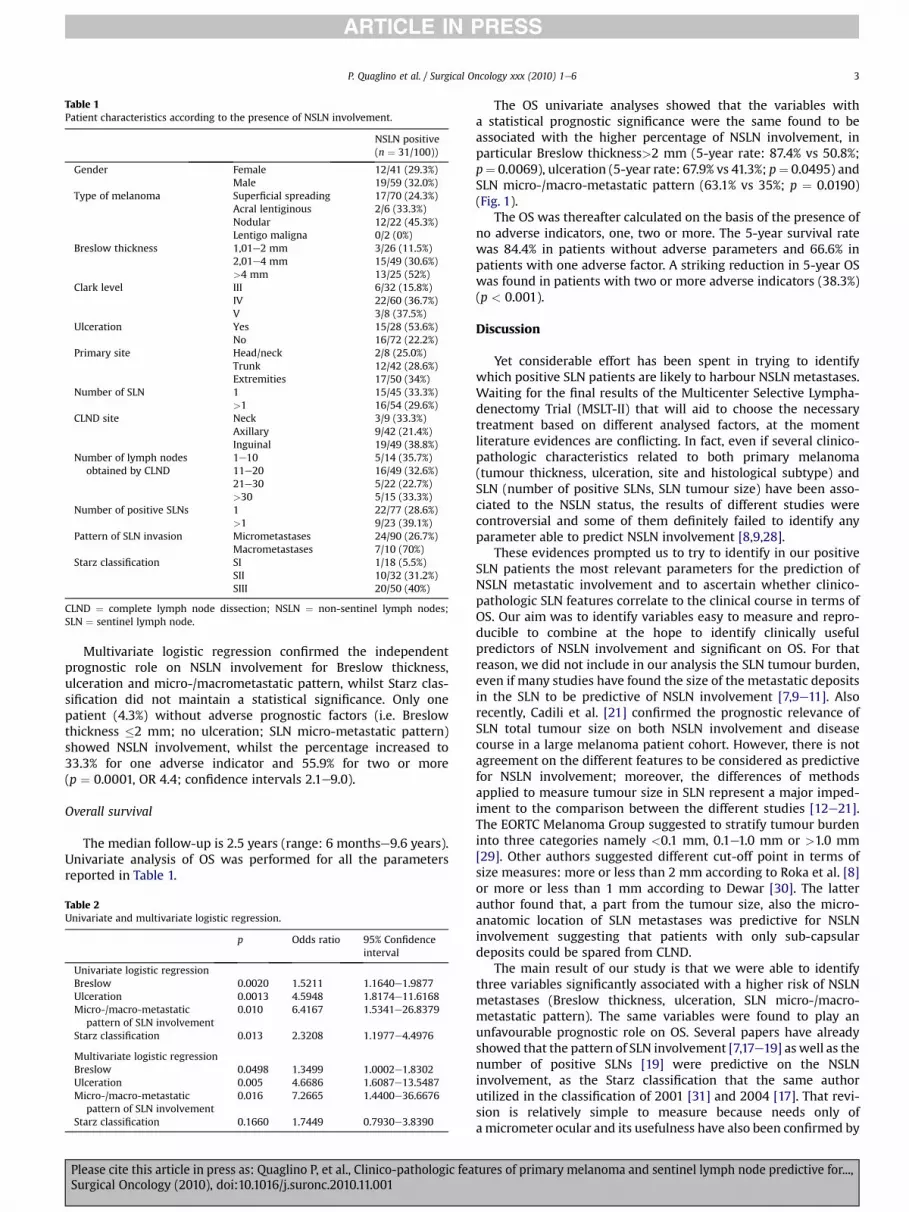
Table 1Patient characteristics according to the presence of NSLN involvement.
NSLN positive(n ¼ 31/100))
Gender Female 12/41 (29.3%)Male 19/59 (32.0%)
Type of melanoma Superficial spreading 17/70 (24.3%)Acral lentiginous 2/6 (33.3%)Nodular 12/22 (45.3%)Lentigo maligna 0/2 (0%)
Breslow thickness 1,01e2 mm 3/26 (11.5%)2,01e4 mm 15/49 (30.6%)>4 mm 13/25 (52%)
Clark level III 6/32 (15.8%)IV 22/60 (36.7%)V 3/8 (37.5%)
Ulceration Yes 15/28 (53.6%)No 16/72 (22.2%)
Primary site Head/neck 2/8 (25.0%)Trunk 12/42 (28.6%)Extremities 17/50 (34%)
Number of SLN 1 15/45 (33.3%)>1 16/54 (29.6%)
CLND site Neck 3/9 (33.3%)Axillary 9/42 (21.4%)Inguinal 19/49 (38.8%)
Number of lymph nodesobtained by CLND
1e10 5/14 (35.7%)11e20 16/49 (32.6%)21e30 5/22 (22.7%)>30 5/15 (33.3%)
Number of positive SLNs 1 22/77 (28.6%)>1 9/23 (39.1%)
Pattern of SLN invasion Micrometastases 24/90 (26.7%)Macrometastases 7/10 (70%)
Starz classification SI 1/18 (5.5%)SII 10/32 (31.2%)SIII 20/50 (40%)
CLND ¼ complete lymph node dissection; NSLN ¼ non-sentinel lymph nodes;SLN ¼ sentinel lymph node.
P. Quaglino et al. / Surgical Oncology xxx (2010) 1e6 3
Multivariate logistic regression confirmed the independentprognostic role on NSLN involvement for Breslow thickness,ulceration and micro-/macrometastatic pattern, whilst Starz clas-sification did not maintain a statistical significance. Only onepatient (4.3%) without adverse prognostic factors (i.e. Breslowthickness �2 mm; no ulceration; SLN micro-metastatic pattern)showed NSLN involvement, whilst the percentage increased to33.3% for one adverse indicator and 55.9% for two or more(p ¼ 0.0001, OR 4.4; confidence intervals 2.1e9.0).
Overall survival
The median follow-up is 2.5 years (range: 6 monthse9.6 years).Univariate analysis of OS was performed for all the parametersreported in Table 1.
Table 2Univariate and multivariate logistic regression.
p Odds ratio 95% Confidenceinterval
Univariate logistic regressionBreslow 0.0020 1.5211 1.1640e1.9877Ulceration 0.0013 4.5948 1.8174e11.6168Micro-/macro-metastatic
pattern of SLN involvement0.010 6.4167 1.5341e26.8379
Starz classification 0.013 2.3208 1.1977e4.4976
Multivariate logistic regressionBreslow 0.0498 1.3499 1.0002e1.8302Ulceration 0.005 4.6686 1.6087e13.5487Micro-/macro-metastatic
pattern of SLN involvement0.016 7.2665 1.4400e36.6676
Starz classification 0.1660 1.7449 0.7930e3.8390
Please cite this article in press as: Quaglino P, et al., Clinico-pathologic feaSurgical Oncology (2010), doi:10.1016/j.suronc.2010.11.001
The OS univariate analyses showed that the variables witha statistical prognostic significance were the same found to beassociated with the higher percentage of NSLN involvement, inparticular Breslow thickness>2 mm (5-year rate: 87.4% vs 50.8%;p¼ 0.0069), ulceration (5-year rate: 67.9% vs 41.3%; p¼ 0.0495) andSLN micro-/macro-metastatic pattern (63.1% vs 35%; p ¼ 0.0190)(Fig. 1).
The OS was thereafter calculated on the basis of the presence ofno adverse indicators, one, two or more. The 5-year survival ratewas 84.4% in patients without adverse parameters and 66.6% inpatients with one adverse factor. A striking reduction in 5-year OSwas found in patients with two or more adverse indicators (38.3%)(p < 0.001).
Discussion
Yet considerable effort has been spent in trying to identifywhich positive SLN patients are likely to harbour NSLN metastases.Waiting for the final results of the Multicenter Selective Lympha-denectomy Trial (MSLT-II) that will aid to choose the necessarytreatment based on different analysed factors, at the momentliterature evidences are conflicting. In fact, even if several clinico-pathologic characteristics related to both primary melanoma(tumour thickness, ulceration, site and histological subtype) andSLN (number of positive SLNs, SLN tumour size) have been asso-ciated to the NSLN status, the results of different studies werecontroversial and some of them definitely failed to identify anyparameter able to predict NSLN involvement [8,9,28].
These evidences prompted us to try to identify in our positiveSLN patients the most relevant parameters for the prediction ofNSLN metastatic involvement and to ascertain whether clinico-pathologic SLN features correlate to the clinical course in terms ofOS. Our aim was to identify variables easy to measure and repro-ducible to combine at the hope to identify clinically usefulpredictors of NSLN involvement and significant on OS. For thatreason, we did not include in our analysis the SLN tumour burden,even if many studies have found the size of the metastatic depositsin the SLN to be predictive of NSLN involvement [7,9e11]. Alsorecently, Cadili et al. [21] confirmed the prognostic relevance ofSLN total tumour size on both NSLN involvement and diseasecourse in a large melanoma patient cohort. However, there is notagreement on the different features to be considered as predictivefor NSLN involvement; moreover, the differences of methodsapplied to measure tumour size in SLN represent a major imped-iment to the comparison between the different studies [12e21].The EORTC Melanoma Group suggested to stratify tumour burdeninto three categories namely <0.1 mm, 0.1e1.0 mm or >1.0 mm[29]. Other authors suggested different cut-off point in terms ofsize measures: more or less than 2 mm according to Roka et al. [8]or more or less than 1 mm according to Dewar [30]. The latterauthor found that, a part from the tumour size, also the micro-anatomic location of SLN metastases was predictive for NSLNinvolvement suggesting that patients with only sub-capsulardeposits could be spared from CLND.
The main result of our study is that we were able to identifythree variables significantly associated with a higher risk of NSLNmetastases (Breslow thickness, ulceration, SLN micro-/macro-metastatic pattern). The same variables were found to play anunfavourable prognostic role on OS. Several papers have alreadyshowed that the pattern of SLN involvement [7,17e19] aswell as thenumber of positive SLNs [19] were predictive on the NSLNinvolvement, as the Starz classification that the same authorutilized in the classification of 2001 [31] and 2004 [17]. That revi-sion is relatively simple to measure because needs only ofa micrometer ocular and its usefulness have also been confirmed by
tures of primary melanoma and sentinel lymph node predictive for...,

Figure 1. Overall Survival (OS) according to prognostic indicators: a) Breslow thickness > 2 mm (p ¼ 0.0069); b) ulceration (p ¼ 0.0495) c) SLN micro-/macro-metastatic pattern(p ¼ 0.0190); d) number of adverse prognostic indicators (0,1,2 or more; p < 0.001).
P. Quaglino et al. / Surgical Oncology xxx (2010) 1e64
recent works [32]. In our experience, the number of positive SLNswas not associated to an increasing NSLN involvement, whilst theprognostic relevance of Starz classification was ascertained inunivariate but not confirmed in multivariate logistic regressionanalysis. The predictive value of Breslow thickness on NSLNinvolvement has been found in some previous papers, but notconfirmed by others [10,13e15,20,31,33]; the same happens forulceration, thus confirming a great deal of variability which limitsthe drawing of definite conclusions. Some studies suggested also toconsider the association of two or more variables. In fact Frankelet al. [19] utilized the relation between percentage of the surfacearea of the metastases on SLN and Breslow thickness while Reeveset al. [20] utilized S/U score (size of metastases on SLN/ulceration).
As a second step in our study, we showed that the likelihood ofNSLN involvement increased in our patients along with the numberof adverse indicators (Breslow thickness > 2 mm; ulceration;macro-metastatic pattern of SLN invasion) from 4.3% in patientswithout adverse features up to 55.9% when two or three adversefactors were present. Therefore, our results do suggest that inselected cases with significant co-morbidities and/or elderly age,the finding of no adverse prognostic indicators could be useful inidentifying patients not to treat by regional node dissection. Inthese patients, a strict follow-up program with radiological work-ups such as nodal ultrasound and/or positron emission tomographyplus computed tomography (PET/CT) could be applied. Ultraso-nography associated with Doppler evaluation is of choice in themonitoring of the regional basin, in as much as its sensibility in thedetection of occult nodal metastases is approaching 90%;
Please cite this article in press as: Quaglino P, et al., Clinico-pathologic feaSurgical Oncology (2010), doi:10.1016/j.suronc.2010.11.001
ultrasound utility is now being evaluated by the MSLT-II trial. Onthe other hand, PET/TC has a diagnostic accuracy superior to that ofTC alone in the early detection of visceral metastases whilst itssensitivity in the evaluation of nodemetastases appears to be lowerdue to the fact that tumour deposits can be far below its detectionthreshold [34e36].
Another controversial point is the impact of SLN features on OS.In comparison with the high literature coverage of NSLN involve-ment predictive factors, few data are reported on this latter topic.Previous studies indicated that the dimensions of nodal tumourdeposits could be significant predictors [37,38]. Roka et al. [8]reported an SLN tumour size >2 mm, presence of NSLN involve-ment and Breslow thickness to be associated with different recur-rence-free and disease-specific survival and confirmed theprognostic relevance of the S/U score proposed by Reeves et al. [20]In another paper, the presence ofmicro-metastatic tumour depositsin SLNwas associated to a significantly better prognosiswith respectto macrometastases [9]. A recent German study [39] found thegreatest dimension of the largest tumour cell deposit, the tumourpenetrative depth and capsular involvement as independentparameters for relapse-free and overall survival. The invasion depth(Starz classification) [17] was also found by previous studies to bestpredict overall survival [16,18,40]. In our experience, however, Starzclassification failed to disclose a significant association witha different clinical course, aswell as the numberof positive SLNs. It isinteresting to note that our study found that the same variablesassociated with a higher likelihood of NSLN involvement carriedalso a prognostic impact on OS. However, it could be hypothesized
tures of primary melanoma and sentinel lymph node predictive for...,

P. Quaglino et al. / Surgical Oncology xxx (2010) 1e6 5
that these variables may not have a prognostic impact on their ownbut only depending on their associationwith NSLN involvement. Tothis aim, we separated our patients according to NSLN involvementinto two groups (presence or absence of melanoma cells) and weanalysed in both groups the OS of patients according to the Breslowthickness, ulceration and micro-/macro-metastatic pattern (datanot shown). The number of adverse prognostic indicators main-tained a statistically significant association with the disease coursenot only in patients without NSLN involvement (p ¼ 0.001) but alsoinpatients harbouringNSLNmetastases (p¼0.05) evenwith a lesserdegree of evidence. These results suggest therefore that the evalu-ation of the factors emerged from our study maintain a potentialprognostic significance to be considered together with the well-known significance of NSLN score.
In conclusion, this study suggests a clinically useful and an easilyapplicable means of identifying melanoma patients with a poten-tially more unfavourable disease course on the basis of theconcomitant evaluation of Breslow thickness, ulceration and SLNmicro/macro-metastatic pattern. The presence of at least one ofthese adverse factors identify patients inwhomCLND ismandatory;these patients should be included thereafter in amore strict follow-up program with more frequent clinical visits and radiologicalprocedures given the unfavourable prognosis. On the other hand,the finding of no adverse indicators identify patients who could bespared from CLND in the presence of significant co-morbidities orelderly age. The relatively low number of patients included in thissingle centre study and the absence of a control group for validation,limit the achievement of more insights into this controversial topicfor which the conclusions of the MSLT-II trial are awaited.
Conflict of interestNone declared.
Authorship statement
Guarantor of the integrity of the study: MG Bernengo, P Savoia,P Quaglino
Study concepts: S Ribero, S Osella-AbateStudy design: S Ribero, P QuaglinoDefinition of intellectual content: S Osella-Abate, P Quaglino,
P SavoiaLiterature research: S RiberoClinical studies: G Macripò, M Grassi, V Caliendo, P QuaglinoExperimental studies: eData acquisition: S Ribero, L Macrì, S Asioli, A Sapino, G MacripòData analysis: S Ribero, P Quaglino, S Osella-AbateStatistical analysis: S Ribero, S Osella-Abate, P QuaglinoManuscript preparation: P Quaglino, S Osella-Abate, S RiberoManuscript editing: S Osella-Abate, S RiberoManuscript review: P Quaglino, P Savoia, G Macripò,
MG Bernengo
References
[1] Morton DL, Wen DR, Wong JH, Economous JS, Cagle LA, Storm FK, et al. Tech-nical details of intraoperative lymphatic mapping for early stage melanoma.Arch Surg 1992;127(4):392e9.
[2] Gershenwald JE, Thompson W, Mansfield PF, Lee JE, Colome MI, Tseng CH, et al.Multi-institutional melanoma lymphatic mapping experience: the prognosticvalue of sentinel lymph node status in 612 stage I or II melanoma patients.J Clin Oncol 1999;17(3):976e83.
[3] Balch CM, Gershenwald JE, Soong SJ, Thompson JF, Atkins MB, Byrd DR, et al.Final version of 2009 AJCC melanoma staging and classification. J Clin Oncol2009;27(36):6199e206.
[4] Morton DL, Thompson JF, Cochran AJ, Mozzillo N, Elashoff R, Essner R, et al.Sentinel-node biopsy or nodal observation in melanoma. N Engl J Med2006;355(13):1307e17.
Please cite this article in press as: Quaglino P, et al., Clinico-pathologic feaSurgical Oncology (2010), doi:10.1016/j.suronc.2010.11.001
[5] Van Akkooi AC, Bouwhuis MG, Van Geel AN, Hoedemaker R, Verhoef C,Grunhagen DJ, et al. Morbidity and prognosis after therapeutic lymph nodedissections for malignant melanoma. Eur J Surg Oncol 2007;33:102e8.
[6] Baas PC, Schraffordt Koops H, Hoekstra HJ, van Bruggen JJ, van der Weele LT,Oldhoff J. Groin dissection in the treatment of lowe- extremity melanoma.Short-term and longeterm morbidity. Arch Surg 1992;127:281e6.
[7] Satzger I, Volker B, Meier A, Kapp A, Gutzmer R. Criteria in sentinel lymphnodes of melanoma patients that predict involvement of nonsentinel lymphnodes. Ann Surg Oncol 2008;15(6):1723e32.
[8] Roka F, Mastan P, Binder M, Okamoto I, Mittlboeck M, Horvat R, et al. Predictionof non-sentinel node status and outcome in sentinel node-positive melanomapatients. Eur J Surg Oncol 2008;34:82e8.
[9] GuggenheimM, Dummer R, Jung FJ, Mihic-Probst D, Steinert H, Rousson V, et al.The influence of sentinel lymph node tumour burden on additional lymph nodeinvolvement and disease-free survival in cutaneous melanoma-a retrospectiveanalysis of 392 cases. Br J Cancer 2008;98(12):1922e8.
[10] Cochran AJ, Wen DR, Huang RR, Wang HJ, Elashoff R, Morton DL. Prediction ofmetastatic melanoma in nonsentinel nodes and clinical outcome based on theprimary melanoma and the sentinel node. Mod Pathol 2004;17(7):747e55.
[11] Gershenwald JE, Andtbacka RH, Prieto VG, Johnson MM, Diwan AH, Lee JE,et al. Microscopic tumour burden in sentinel lymph nodes predicts synchro-nous nonsentinel lymph node involvement in patients with melanoma. J ClinOncol 2008;26(26):4296e303.
[12] Scolyer RA, Li LX, McCarthy SW, Shaw HM, Stretch JR, Sharma R, et al.Immunohistochemical stains fail to increase the detection rate of micro-metastatic melanoma in completion regional lymph node dissection speci-mens. Melanoma Res 2004;14:263e8.
[13] Wagner JD, Gordon MS, Chuang TY, Coleman 3rd JJ, Hayes JT, Jung SH, et al.Predicting sentinel and residual lymph node basin disease after sentinellymph node biopsy for melanoma. Cancer 2000;89:453e62.
[14] Salti GI, Das Gupta TK. Predicting residual lymph node basin disease inmelanoma patients with sentinel lymph node metastases. Am J Surg 2003;186:98e101.
[15] Sabel MS, Griffith K, Sondak VK, Lowe L, Schwartz JL, Cimmino VM, et al.Predictors of nonsentinel lymph node positivity in patients with a positivesentinel node for melanoma. J Am Coll Surg 2005;201:37e47.
[16] Van der Ploeg IM, Kroon BB, Antonini N, Valdés Olmos RA, Nieweg OE. Iscompletion lymph node dissection needed in case of minimal melanomametastasis in the sentinel node? Ann Surg 2009;249:1003e7.
[17] Starz H, Siedlecki K, Balda BR. Sentinel lymphonodectomy and s-classification:a successful strategy for better prediction and improvement of outcome ofmelanoma. Ann Surg Oncol 2004;11(3 Suppl):162Se8S.
[18] Van der Ploeg IM, Kroon BB, Antonini N, Valdés Olmos RA, Nieweg OE.Comparison of three micromorphometric pathology classifications of mela-noma metastasis in the sentinel node. Ann Surg 2009;250:301e4.
[19] Frankel TL, Griffith KA, Lowe L, Wong SL, Bichakjian CK, Chang AE, et al. Domicromorphometric features of metastatic deposits within sentinel nodespredict nonsentinel lymph node involvement in melanoma? Ann Surg Oncol2008;15(9):2403e11.
[20] Reeves ME, Delgado R, Busam KJ, Brady MS, Coit DG. Prediction of nonsentinellymph node status in melanoma. Ann Surg Oncol 2003;10:27e31.
[21] Cadili A, Smylie M, Danyluk J, Dabbs K. Prediction of nonsentinel lymph nodemetastasis in malignant melanoma. J Surg Res 2009;154:324e9.
[22] Quaglino P, Borgognoni L, Bottoni U, Calvieri S, Carli P, Catricalà C, et al. Italianguidelines for staging and follow-up of stage I-II cutaneous melanomapatients. G Ital Dermatol Venereol 2007;142:41e7.
[23] Cochran AJ, Balda BR, Starz H, Bachter D, Krag DN, Cruse CW, et al. TheAugsburg consensus. Techniques of lymphatic mapping, sentinel lymphade-nectomy, and completion lymphadenectomy in cutaneous malignancies.Cancer 2000;89:236e41.
[24] Sober AJ, Chuang TY, Duvic M, Farmer ER, Grinchnik JM, Halpern AC, et al.Guidelines of care for primary cutaneous melanoma. J Am Acad Dermatol2001;45(4):579e86.
[25] Cook MG, Di Palma S. Pathology of sentinel lymph nodes for melanoma. J ClinPathol 2008;6:897e902.
[26] Kaplan EL, Meier P. Non-parametric estimation from incomplete observations.J Am Stat Assoc 1958;53:475e80.
[27] Mantel N. Evaluation of survival data and two new rank order statistics arisingin its consideration. Cancer Chemother Rep 1966;50:163e70.
[28] McMasters KM, Wong SL, Edwards MJ, Chao C, Ross MI, Noyes RD, et al.Frequency of nonsentinel lymph node metastasis in melanoma. Ann SurgOncol 2002;9(2):137e41.
[29] van Akkooi AC, Spatz A, Eggermont AM, Mihm M, Cook MG. Expert opinion inmelanoma: the sentinel node; EORTC melanoma group recommendations onpractical methodology of the measurement of the microanatomic location ofmetastases and metastatic tumour burden. Eur J Cancer 2009 Nov;45(16):2736e42.
[30] Dewar DJ, Newell B, Green MA, Topping AP, Powell BW, Cook MG. Themicroanatomic location of metastatic melanoma in sentinel lymph nodespredicts nonsentinel lymph node involvement. J Clin Oncol 2004 Aug 15;22(16):3345e9.
[31] Starz H, Balda BR, Krämer KU, Büchels H, Wang H. A micromorphometry-based concept for routine classification of sentinel lymph node metastasesand its clinical relevance for patients with melanoma. Cancer 2001;91(11):2110e21.
tures of primary melanoma and sentinel lymph node predictive for...,

P. Quaglino et al. / Surgical Oncology xxx (2010) 1e66
[32] Younan R, Bougrine A, Watters K, Mahboubi A, Bouchereau-Eyegue M,Loufi A, et al. Validation study of the S classification for melanoma patientswith positive sentinel nodes: the Montreal experience. Ann Surg Oncol2010;17(5):1414e21.
[33] Lee JH, Essner R, Torisu-Itakura H, Wanek L, Wang H, Morton DL. Factorspredictive of tumor-positive nonsentinel lymph nodes after tumor-positivesentinel lymph node dissection for melanoma. J Clin Oncol 2004;22(18):3677e84.
[34] Amersi F, Morton DL. The role of sentinel lymph node biopsy in themanagement of melanoma. Adv Surg 2007;41:241e56.
[35] Forschner A, Eigentler TK, Pflugfelder A, Leiter U, Weide B, Held L, et al.Melanoma staging: facts and controversies. Clin Dermatol 2010 MayeJun;28(3):275e80.
[36] Jiménez-Requena F, Delgado-Bolton RC, Fernández-Pérez C, Gambhir SS,Schwimmer J, Pérez-Vázquez JM, et al. Meta-analysis of the performance of
Please cite this article in press as: Quaglino P, et al., Clinico-pathologic feaSurgical Oncology (2010), doi:10.1016/j.suronc.2010.11.001
(18)F-FDG PET in cutaneous melanoma. Eur J Nucl Med Mol Imaging 2010Feb;37(2):284e300.
[37] Ranieri JM, Wagner JD, Azuaje R, Davidson D, Wenck S, Fyffe J, et al. Prognosticimportance of lymph node tumor burden in melanoma patients staged bysentinel node biopsy. Ann Surg Oncol 2002;9(10):975e81.
[38] Carlson GW, Murray DR, Lyles RH, Staley CA, Hestley A, Cohen C. The amountof metastatic melanoma in a sentinel lymph node: does it have prognosticsignificance? Ann Surg Oncol 2003;10(5):575e81.
[39] Meier A, Satzger I, Völker B, Kapp A, Gutzmer R. Comparison of classificationsystems in melanoma sentinel lymph nodesean analysis of 697 patients froma single center. Cancer 2010;116(13):3178e88.
[40] Rossi CR, De Salvo GL, Bonandini E, Mocellin S, Foletto M, Pasquali S, et al.Factors predictive of nonsentinel lymph node involvement and clinicaloutcome in melanoma patients with metastatic sentinel lymph node. AnnSurg Oncol 2008 Apr;15(4):1202e10.
tures of primary melanoma and sentinel lymph node predictive for...,