clinical performance of zirconia–ceramic cantilever ... - j-stage
TRANSCRIPT
journal of prosthodontic research 63 (2019) 334–339
Original article
Clinical performance of zirconia–ceramic cantilever fixed partialdentures—Longitudinal nine-year results from a prospective,randomized, controlled pilot study
Wolfgang Bömicke*, Peter Rammelsberg, Andreas Zenthöfer1, Brigitte Ohlmann1
Department of Prosthetic Dentistry, University Hospital Heidelberg, University of Heidelberg, Heidelberg, Germany
A R T I C L E I N F O
Article history:Received 4 October 2018Received in revised form 8 January 2019Accepted 21 January 2019Available online 22 February 2019
Keywords:Rehabilitation of partial edentulismRestoration survivalClinical trialPrognosis of all-ceramic prosthesesMetal–ceramic restoration of tooth loss
A B S T R A C T
Purpose: The aim of this study was to prospectively compare the clinical performance of veneeredzirconia cantilever fixed partial dentures (Z-CFPDs) and metal–ceramic CFPDs (MC-CFPDs) over 9 years offollow-up in terms of survival.Methods: Twenty-one participants were assigned by simple randomization to receive either 1 Z-CFPD (n = 11)or 1 MC-CFPD (n = 10). CFPDs were retained by 2 full crowns and replaced a missing premolar or a central orlateral incisor. Modified USPHS (United States Public Health Service) criteria were used to classify materialchipping, retention, marginal integrity, secondary caries, and color of the restorations. The satisfaction ofthe study participants with the esthetics of their restorations was surveyed; pocket probing depths (PPD),plaque index (PI), and gingival index (GI) were also measured. Study groups were compared by use of Utests (continuous variables), or by use of Fisher exact probability tests (categorical variables) with α = 0.05.Results: Sixteen participants (n = 8 with a Z-CFPD and n = 8 with an MC-CFPD) attended the 9-year follow-up examination (response rate: 76.2%). Over the 9-year study period, survival of 50% for Z-CFPDs and 75%for MC-CFPDs was recorded (p = 0.608). No framework fractures occurred, and no statistically significantdifferences were observed between the groups regarding changes in PPD, PI, GI, or participant satisfaction(p > 0.05). USPHS criteria revealed statistically significantly poorer marginal quality for Z-CFPDs than forMC-CFPDs (p = 0.009).Conclusion: Within the limitations of this study, Z and MC-CFPDs demonstrated no statistically significantdifference in terms of survival.
© 2019 Japan Prosthodontic Society. Published by Elsevier Ltd. All rights reserved.
Journal of Prosthodontic Research
1. Introduction
Although use of end abutment fixed partial dentures (FPDs) is awidely accepted and widely used therapeutic option for thetreatment of partial edentulism [1], there is no agreement in theinternational literature on replacement of teeth with conventionalcrown-retained cantilever FPDs (CFPDs). For example, the obser-vation that the risk of loss is greater for CFPDs than forconventional FPDs [2–4] has not been consistently confirmed[5–7]. Several risk factors are, however, known to affect theprobability of survival and incidence of complications of CFPDs [8].Treatment with CFPDs could, therefore, be considered a compro-mise compared with treatment with end abutment FPDs orimplant supported single crowns. However, if implant treatment isnot possible, CFPDs may be a viable alternative to removable
* Corresponding author at: MZK 8.2 Poliklinik für Zahnärztliche Prothetik, ImNeuenheimer Feld 400, 69120 Heidelberg, Germany.
E-mail address: [email protected] (W. Bömicke).1 The authors contributed equally to this work.
https://doi.org/10.1016/j.jpor.2019.01.0071883-1958/© 2019 Japan Prosthodontic Society. Published by Elsevier Ltd. All rights re
partial dentures, especially in terms of patient satisfaction [9,10].Finally, it may be useful to prefer a CFPD to an FPD if two adjacentteeth adjacent to a tooth gap already have major substance defectsand the second abutment to be included in an FPD is sound.
In view of the increasing demand for fully tooth-colored andmetal-free prostheses [11,12], a ceramic alternative to the classicmetal–ceramic CFPD is also desirable [13]. Despite increasedresearch activities in the field of ceramic dental prostheses [12,14–16], few clinical data on ceramic CFPDs are available. Whereaspromising long-term results have been recorded for single-retainer ceramic CFPDs used to replace a missing anterior tooth[17], equivalent long-term data for ceramic CFPDs in the posteriorregion are missing [18,19]. In particular, ceramic and metal–ceramic CFPDs have not been directly compared over an extendedobservation period. Such a comparison seems advisable, however,because the tensile stresses that occur in restorations due toloading of the pontics pose a specific challenge for ceramic CFPDs.In this context, fracture loads of ceramic CFPDs recorded in vitroindicate that although these CFPDs are made from high-strengthzirconium dioxide, their safety factor is small compared with the
served.
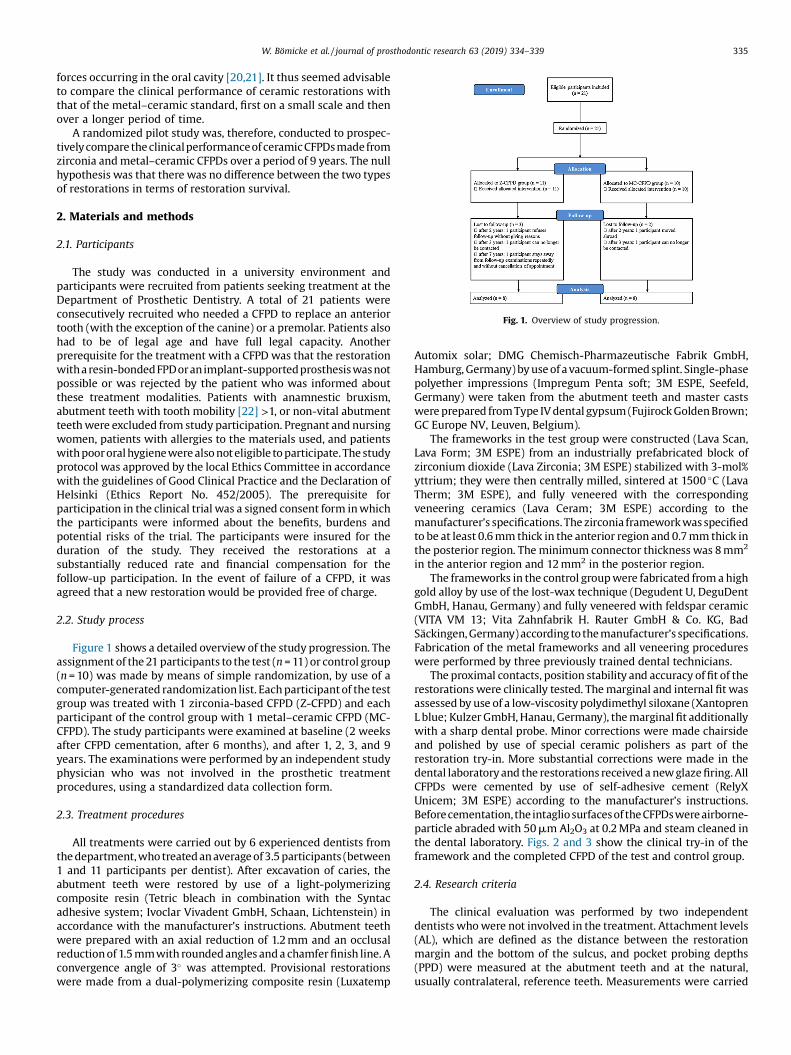
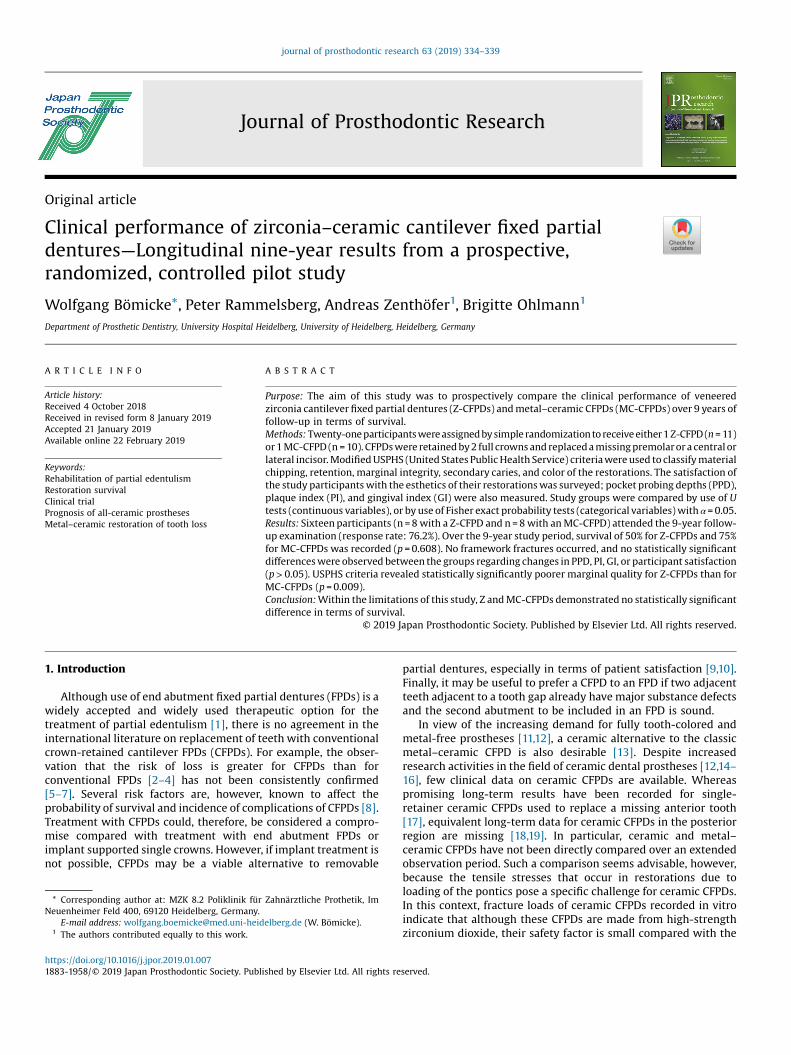
Fig. 1. Overview of study progression.
W. Bömicke et al. / journal of prosthodontic research 63 (2019) 334–339 335
forces occurring in the oral cavity [20,21]. It thus seemed advisableto compare the clinical performance of ceramic restorations withthat of the metal–ceramic standard, first on a small scale and thenover a longer period of time.
A randomized pilot study was, therefore, conducted to prospec-tivelycompare the clinicalperformanceof ceramic CFPDs made fromzirconia and metal–ceramic CFPDs over a period of 9 years. The nullhypothesis was that there was no difference between the two typesof restorations in terms of restoration survival.
2. Materials and methods
2.1. Participants
The study was conducted in a university environment andparticipants were recruited from patients seeking treatment at theDepartment of Prosthetic Dentistry. A total of 21 patients wereconsecutively recruited who needed a CFPD to replace an anteriortooth (with the exception of the canine) or a premolar. Patients alsohad to be of legal age and have full legal capacity. Anotherprerequisite for the treatment with a CFPD was that the restorationwitha resin-bondedFPDoranimplant-supportedprosthesiswasnotpossible or was rejected by the patient who was informed aboutthese treatment modalities. Patients with anamnestic bruxism,abutment teeth with tooth mobility [22] >1, or non-vital abutmentteeth were excluded from study participation. Pregnant and nursingwomen, patients with allergies to the materials used, and patientswith poororal hygiene were also not eligible to participate. The studyprotocol was approved by the local Ethics Committee in accordancewith the guidelines of Good Clinical Practice and the Declaration ofHelsinki (Ethics Report No. 452/2005). The prerequisite forparticipation in the clinical trial was a signed consent form in whichthe participants were informed about the benefits, burdens andpotential risks of the trial. The participants were insured for theduration of the study. They received the restorations at asubstantially reduced rate and financial compensation for thefollow-up participation. In the event of failure of a CFPD, it wasagreed that a new restoration would be provided free of charge.
2.2. Study process
Figure 1 shows a detailed overview of the study progression. Theassignment of the 21 participants to the test (n = 11) or control group(n = 10) was made by means of simple randomization, by use of acomputer-generated randomization list. Each participant of the testgroup was treated with 1 zirconia-based CFPD (Z-CFPD) and eachparticipant of the control group with 1 metal–ceramic CFPD (MC-CFPD). The study participants were examined at baseline (2 weeksafter CFPD cementation, after 6 months), and after 1, 2, 3, and 9years. The examinations were performed by an independent studyphysician who was not involved in the prosthetic treatmentprocedures, using a standardized data collection form.
2.3. Treatment procedures
All treatments were carried out by 6 experienced dentists fromthe department, who treated an average of 3.5 participants (between1 and 11 participants per dentist). After excavation of caries, theabutment teeth were restored by use of a light-polymerizingcomposite resin (Tetric bleach in combination with the Syntacadhesive system; Ivoclar Vivadent GmbH, Schaan, Lichtenstein) inaccordance with the manufacturer’s instructions. Abutment teethwere prepared with an axial reduction of 1.2 mm and an occlusalreduction of 1.5 mmwith rounded angles and a chamfer finish line. Aconvergence angle of 3� was attempted. Provisional restorationswere made from a dual-polymerizing composite resin (Luxatemp
Automix solar; DMG Chemisch-Pharmazeutische Fabrik GmbH,Hamburg, Germany) by use of a vacuum-formed splint. Single-phasepolyether impressions (Impregum Penta soft; 3M ESPE, Seefeld,Germany) were taken from the abutment teeth and master castswere prepared from Type IV dental gypsum (Fujirock Golden Brown;GC Europe NV, Leuven, Belgium).
The frameworks in the test group were constructed (Lava Scan,Lava Form; 3M ESPE) from an industrially prefabricated block ofzirconium dioxide (Lava Zirconia; 3M ESPE) stabilized with 3-mol%yttrium; they were then centrally milled, sintered at 1500 �C (LavaTherm; 3M ESPE), and fully veneered with the correspondingveneering ceramics (Lava Ceram; 3M ESPE) according to themanufacturer’s specifications. The zirconia framework was specifiedto be at least 0.6 mm thick in the anterior region and 0.7 mm thick inthe posterior region. The minimum connector thickness was 8 mm2
in the anterior region and 12 mm2 in the posterior region.The frameworks in the control group were fabricated from a high
gold alloy by use of the lost-wax technique (Degudent U, DeguDentGmbH, Hanau, Germany) and fully veneered with feldspar ceramic(VITA VM 13; Vita Zahnfabrik H. Rauter GmbH & Co. KG, BadSäckingen, Germany) according to the manufacturer’s specifications.Fabrication of the metal frameworks and all veneering procedureswere performed by three previously trained dental technicians.
The proximal contacts, position stability and accuracy of fit of therestorations were clinically tested. The marginal and internal fit wasassessed by use of a low-viscosity polydimethyl siloxane (XantoprenL blue; Kulzer GmbH, Hanau, Germany), the marginal fit additionallywith a sharp dental probe. Minor corrections were made chairsideand polished by use of special ceramic polishers as part of therestoration try-in. More substantial corrections were made in thedental laboratory and the restorations received a new glaze firing. AllCFPDs were cemented by use of self-adhesive cement (RelyXUnicem; 3M ESPE) according to the manufacturer’s instructions.Beforecementation,the intagliosurfacesof the CFPDswere airborne-particle abraded with 50mm Al2O3 at 0.2 MPa and steam cleaned inthe dental laboratory. Figs. 2 and 3 show the clinical try-in of theframework and the completed CFPD of the test and control group.
2.4. Research criteria
The clinical evaluation was performed by two independentdentists who were not involved in the treatment. Attachment levels(AL), which are defined as the distance between the restorationmargin and the bottom of the sulcus, and pocket probing depths(PPD) were measured at the abutment teeth and at the natural,usually contralateral, reference teeth. Measurements were carried
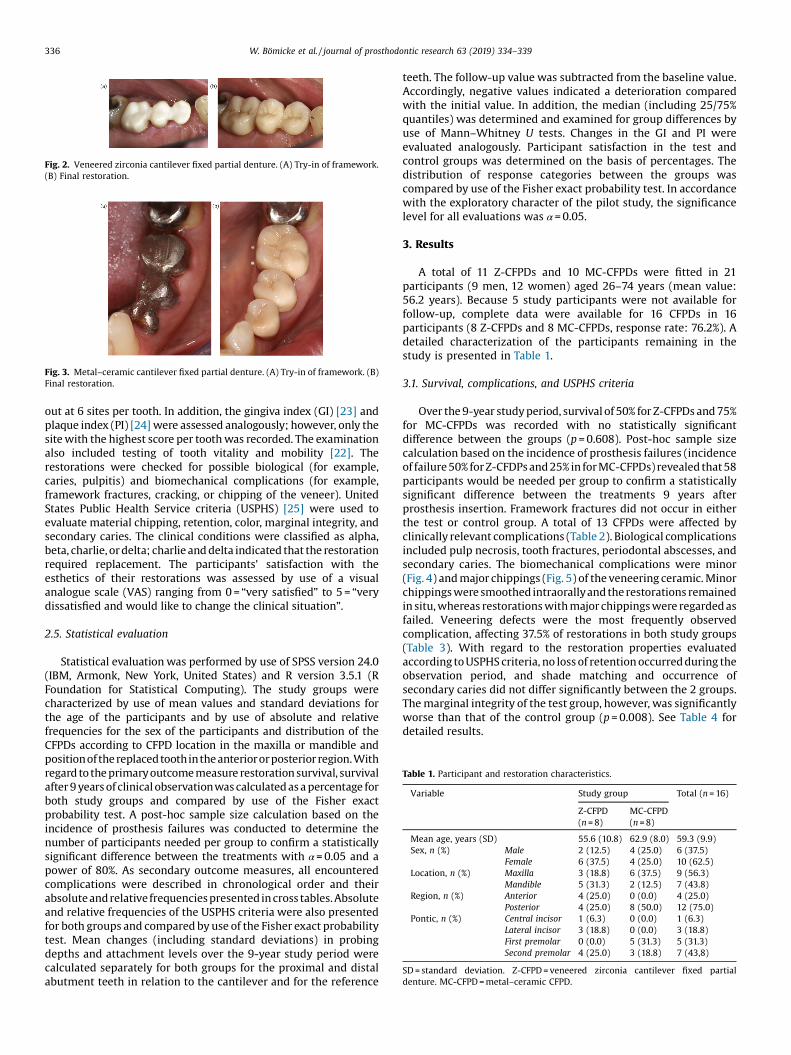
Fig. 2. Veneered zirconia cantilever fixed partial denture. (A) Try-in of framework.(B) Final restoration.
Fig. 3. Metal–ceramic cantilever fixed partial denture. (A) Try-in of framework. (B)Final restoration.
Table 1. Participant and restoration characteristics.
Variable Study group Total (n = 16)
Z-CFPD(n = 8)
MC-CFPD(n = 8)
Mean age, years (SD) 55.6 (10.8) 62.9 (8.0) 59.3 (9.9)Sex, n (%) Male 2 (12.5) 4 (25.0) 6 (37.5)
Female 6 (37.5) 4 (25.0) 10 (62.5)Location, n (%) Maxilla 3 (18.8) 6 (37.5) 9 (56.3)
Mandible 5 (31.3) 2 (12.5) 7 (43.8)Region, n (%) Anterior 4 (25.0) 0 (0.0) 4 (25.0)
Posterior 4 (25.0) 8 (50.0) 12 (75.0)Pontic, n (%) Central incisor 1 (6.3) 0 (0.0) 1 (6.3)
Lateral incisor 3 (18.8) 0 (0.0) 3 (18.8)First premolar 0 (0.0) 5 (31.3) 5 (31.3)Second premolar 4 (25.0) 3 (18.8) 7 (43,8)
SD = standard deviation. Z-CFPD = veneered zirconia cantilever fixed partialdenture. MC-CFPD = metal–ceramic CFPD.
336 W. Bömicke et al. / journal of prosthodontic research 63 (2019) 334–339
out at 6 sites per tooth. In addition, the gingiva index (GI) [23] andplaque index (PI) [24] were assessed analogously; however, only thesite with the highest score per tooth was recorded. The examinationalso included testing of tooth vitality and mobility [22]. Therestorations were checked for possible biological (for example,caries, pulpitis) and biomechanical complications (for example,framework fractures, cracking, or chipping of the veneer). UnitedStates Public Health Service criteria (USPHS) [25] were used toevaluate material chipping, retention, color, marginal integrity, andsecondary caries. The clinical conditions were classified as alpha,beta, charlie, or delta; charlie and delta indicated that the restorationrequired replacement. The participants’ satisfaction with theesthetics of their restorations was assessed by use of a visualanalogue scale (VAS) ranging from 0 = “very satisfied” to 5 = “verydissatisfied and would like to change the clinical situation”.
2.5. Statistical evaluation
Statistical evaluation was performed by use of SPSS version 24.0(IBM, Armonk, New York, United States) and R version 3.5.1 (RFoundation for Statistical Computing). The study groups werecharacterized by use of mean values and standard deviations forthe age of the participants and by use of absolute and relativefrequencies for the sex of the participants and distribution of theCFPDs according to CFPD location in the maxilla or mandible andpositionof the replacedtoothinthe anteriororposterior region.Withregard to the primary outcome measure restoration survival, survivalafter 9 years of clinical observationwas calculated as a percentage forboth study groups and compared by use of the Fisher exactprobability test. A post-hoc sample size calculation based on theincidence of prosthesis failures was conducted to determine thenumber of participants needed per group to confirm a statisticallysignificant difference between the treatments with α = 0.05 and apower of 80%. As secondary outcome measures, all encounteredcomplications were described in chronological order and theirabsolute and relativefrequencies presented in cross tables. Absoluteand relative frequencies of the USPHS criteria were also presentedfor both groups and compared by use of the Fisher exact probabilitytest. Mean changes (including standard deviations) in probingdepths and attachment levels over the 9-year study period werecalculated separately for both groups for the proximal and distalabutment teeth in relation to the cantilever and for the reference
teeth. The follow-up value was subtracted from the baseline value.Accordingly, negative values indicated a deterioration comparedwith the initial value. In addition, the median (including 25/75%quantiles) was determined and examined for group differences byuse of Mann–Whitney U tests. Changes in the GI and PI wereevaluated analogously. Participant satisfaction in the test andcontrol groups was determined on the basis of percentages. Thedistribution of response categories between the groups wascompared by use of the Fisher exact probability test. In accordancewith the exploratory character of the pilot study, the significancelevel for all evaluations was α = 0.05.
3. Results
A total of 11 Z-CFPDs and 10 MC-CFPDs were fitted in 21participants (9 men, 12 women) aged 26–74 years (mean value:56.2 years). Because 5 study participants were not available forfollow-up, complete data were available for 16 CFPDs in 16participants (8 Z-CFPDs and 8 MC-CFPDs, response rate: 76.2%). Adetailed characterization of the participants remaining in thestudy is presented in Table 1.
3.1. Survival, complications, and USPHS criteria
Over the 9-year study period, survival of 50% for Z-CFPDs and 75%for MC-CFPDs was recorded with no statistically significantdifference between the groups (p = 0.608). Post-hoc sample sizecalculation based on the incidence of prosthesis failures (incidenceof failure 50% for Z-CFDPs and 25% in for MC-CFPDs) revealed that 58participants would be needed per group to confirm a statisticallysignificant difference between the treatments 9 years afterprosthesis insertion. Framework fractures did not occur in eitherthe test or control group. A total of 13 CFPDs were affected byclinically relevant complications (Table 2). Biological complicationsincluded pulp necrosis, tooth fractures, periodontal abscesses, andsecondary caries. The biomechanical complications were minor(Fig. 4) and major chippings (Fig. 5) of the veneering ceramic. Minorchippings were smoothed intraorallyand the restorations remainedin situ, whereas restorations with major chippings were regarded asfailed. Veneering defects were the most frequently observedcomplication, affecting 37.5% of restorations in both study groups(Table 3). With regard to the restoration properties evaluatedaccording to USPHS criteria, no loss of retention occurred during theobservation period, and shade matching and occurrence ofsecondary caries did not differ significantly between the 2 groups.The marginal integrity of the test group, however, was significantlyworse than that of the control group (p = 0.008). See Table 4 fordetailed results.

Table 2. Complications of 16 CFPDs within 9-year observation period.
Sequential number Study group Complication Failure Location Region Duration to occurrence of complication (years)
1 Z-CFPDa Pulp necrosis No Mandible Posterior 0.742 Z-CFPDb Minor chipping No Mandible Posterior 1.173 Z-CFPD Pulp necrosis No Maxilla Anterior 2.964 MC-CFPD Minor chipping No Mandible Anterior 2.975 MC-CFPD Pulp necrosis No Maxilla Posterior 2.976 MC-CFPD Secondary caries Yes Maxilla Posterior 6.617 Z-CFPDa Abutment tooth fracture Yes Mandible Posterior 6.838 MC-CFPD Secondary caries Yes Mandible Posterior 6.879 Z-CFPD Secondary caries + marginal insufficiency Yes Mandible Posterior 8.0310 Z-CFPDb Major chipping Yes Mandible Posterior 8.8911 MC-CFPD Minor chipping No Maxilla Posterior 8.9712 Z-CFPD Minor chipping No Mandible Posterior 9.3113 MC-CFPD Minor chipping No Maxilla Posterior 9.3314 Z-CFPD Periodontal abscess Yes Maxilla Anterior 9.3315 Z-CFPD Minor chipping No Mandible Anterior 9.64
CFPD = cantilever fixed partial denture. Z-CFPD = veneered zirconia CFPD. MC-CFPD = metal–ceramic CFPD.a Multiple complications of the same restoration. b Multiple complications of the same restoration.
W. Bömicke et al. / journal of prosthodontic research 63 (2019) 334–339 337
3.2. PPD, AL, PI, and GI
The values for PPD, AL, PI, and GI increased slightly over time inthe test group; however, these values did not statistically signifi-cantly differ from those in the metal–ceramic group (Tables 5 and 6).Because both the abutment and reference teeth were equallyaffected, deterioration of the values indicated a general deteriorationof the periodontal health or oral hygiene of the participant and notdeterioration specific to the abutment teeth or study group.
3.3. Restoration esthetics
Nine-year data on restoration esthetics were collected from 13participants. Satisfaction with esthetics did not differ significantlybetweenparticipants (p = 0..266). Most study participants were verysatisfied: in the test group, 4 participants were very satisfied (VASgrade 0) and 3 were satisfied (VAS grade 1); in the metal–ceramicgroup, 5 participants were very satisfied and 1 was satisfied.
4. Discussion
Clinical data on CFPDs made from In-Ceram alumina showedthat framework fractures are one of the complications leading tothe loss of ceramic CFPDs [13]. No difference between cantileverand end abutment FPDs was observed in the present study,however; it can therefore be assumed that in this case the fractureprobability of the restorations depended much more on thematerial used than on FPD design.
After the introduction of yttria-stabilized tetragonal zirconiapolycrystal, which has the ability to counteract crack propagationby means of phase transformation, the question arose whetherCFPDs made from this material can withstand chewing forces in
Fig. 4. Minor chipping of metal–ceramic cantilever fixed partial denture (CFPD). (A)Clinical view after 9 years in position. (B) Clinical view of same CFPD at baseline.
the posterior region in the long term. A previous in vitro studysuggested that the fracture loads observed for zirconia CFPDs wereinsufficient to permit the clinical use of these restorations in theposterior region without restrictions [20]. In the study cited,however, an extremely unfavorable load case was simulated; forcewas applied exclusively to the cantilever pontic, which is unlikelyto occur in the oral cavity. In addition, initial clinical studies on theperformance of posterior CFPDs have shown that zirconiumdioxide framework fractures are unlikely over an averageobservation period of 3 or 4 years [18,19]. This is confirmed bythe results of the pilot study presented here for a longer period oftime. As in previous studies, no framework fracture of a ceramicCFPD was observed over an observation period of 9 years.
In addition to the occurrence of biological complications,chipping of the veneering ceramic was decisive for the failure ofthe restorations in this study. First-generation fully veneeredzirconia frameworks appear to be more susceptible to chipping in
Fig. 5. Major chipping at pontic of zirconia cantilever fixed partial denture withproximal contact completely dissolved. (A) Occlusal view. (B) Lateral view.
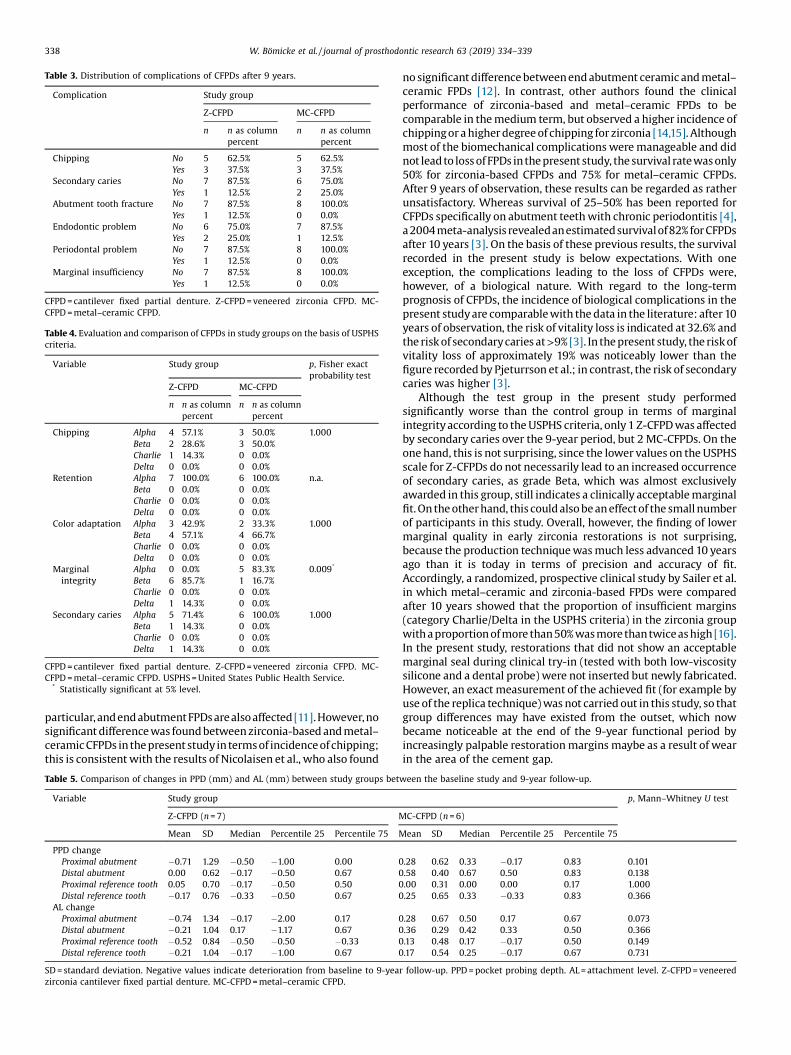
Table 3. Distribution of complications of CFPDs after 9 years.
Complication Study group
Z-CFPD MC-CFPD
n n as columnpercent
n n as columnpercent
Chipping No 5 62.5% 5 62.5%Yes 3 37.5% 3 37.5%
Secondary caries No 7 87.5% 6 75.0%Yes 1 12.5% 2 25.0%
Abutment tooth fracture No 7 87.5% 8 100.0%Yes 1 12.5% 0 0.0%
Endodontic problem No 6 75.0% 7 87.5%Yes 2 25.0% 1 12.5%
Periodontal problem No 7 87.5% 8 100.0%Yes 1 12.5% 0 0.0%
Marginal insufficiency No 7 87.5% 8 100.0%Yes 1 12.5% 0 0.0%
CFPD = cantilever fixed partial denture. Z-CFPD = veneered zirconia CFPD. MC-CFPD = metal–ceramic CFPD.
Table 4. Evaluation and comparison of CFPDs in study groups on the basis of USPHScriteria.
Variable Study group p, Fisher exactprobability test
Z-CFPD MC-CFPD
n n as columnpercent
n n as columnpercent
Chipping Alpha 4 57.1% 3 50.0% 1.000Beta 2 28.6% 3 50.0%Charlie 1 14.3% 0 0.0%Delta 0 0.0% 0 0.0%
Retention Alpha 7 100.0% 6 100.0% n.a.Beta 0 0.0% 0 0.0%Charlie 0 0.0% 0 0.0%Delta 0 0.0% 0 0.0%
Color adaptation Alpha 3 42.9% 2 33.3% 1.000Beta 4 57.1% 4 66.7%Charlie 0 0.0% 0 0.0%Delta 0 0.0% 0 0.0%
Marginalintegrity
Alpha 0 0.0% 5 83.3% 0.009*
Beta 6 85.7% 1 16.7%Charlie 0 0.0% 0 0.0%Delta 1 14.3% 0 0.0%
Secondary caries Alpha 5 71.4% 6 100.0% 1.000Beta 1 14.3% 0 0.0%Charlie 0 0.0% 0 0.0%Delta 1 14.3% 0 0.0%
CFPD = cantilever fixed partial denture. Z-CFPD = veneered zirconia CFPD. MC-CFPD = metal–ceramic CFPD. USPHS = United States Public Health Service.
* Statistically significant at 5% level.
338 W. Bömicke et al. / journal of prosthodontic research 63 (2019) 334–339
particular, and end abutment FPDs arealsoaffected[11]. However,nosignificant difference was found between zirconia-based and metal–ceramic CFPDs in the present study in terms of incidence of chipping;this is consistent with the results of Nicolaisen et al., who also found
Table 5. Comparison of changes in PPD (mm) and AL (mm) between study groups bet
Variable Study group
Z-CFPD (n = 7) M
Mean SD Median Percentile 25 Percentile 75 M
PPD changeProximal abutment �0.71 1.29 �0.50 �1.00 0.00 0Distal abutment 0.00 0.62 �0.17 �0.50 0.67 0Proximal reference tooth 0.05 0.70 �0.17 �0.50 0.50 0Distal reference tooth �0.17 0.76 �0.33 �0.50 0.67 0
AL changeProximal abutment �0.74 1.34 �0.17 �2.00 0.17 0Distal abutment �0.21 1.04 0.17 �1.17 0.67 0Proximal reference tooth �0.52 0.84 �0.50 �0.50 �0.33 0Distal reference tooth �0.21 1.04 �0.17 �1.00 0.67 0
SD = standard deviation. Negative values indicate deterioration from baseline to 9-yeazirconia cantilever fixed partial denture. MC-CFPD = metal–ceramic CFPD.
no significant difference between end abutment ceramic and metal–ceramic FPDs [12]. In contrast, other authors found the clinicalperformance of zirconia-based and metal–ceramic FPDs to becomparable in the medium term, but observed a higher incidence ofchipping or a higher degree of chipping for zirconia [14,15]. Althoughmost of the biomechanical complications were manageable and didnot lead to loss of FPDs in the present study, the survival ratewas only50% for zirconia-based CFPDs and 75% for metal–ceramic CFPDs.After 9 years of observation, these results can be regarded as ratherunsatisfactory. Whereas survival of 25–50% has been reported forCFPDs specifically on abutment teeth with chronic periodontitis [4],a2004 meta-analysis revealedanestimatedsurvivalof82% for CFPDsafter 10 years [3]. On the basis of these previous results, the survivalrecorded in the present study is below expectations. With oneexception, the complications leading to the loss of CFPDs were,however, of a biological nature. With regard to the long-termprognosis of CFPDs, the incidence of biological complications in thepresent study are comparable with the data in the literature: after 10years of observation, the risk of vitality loss is indicated at 32.6% andthe risk of secondarycaries at >9% [3]. In the present study, the risk ofvitality loss of approximately 19% was noticeably lower than thefigure recorded by Pjeturrson et al.; in contrast, the risk of secondarycaries was higher [3].
Although the test group in the present study performedsignificantly worse than the control group in terms of marginalintegrity according to the USPHS criteria, only 1 Z-CFPD was affectedby secondary caries over the 9-year period, but 2 MC-CFPDs. On theone hand, this is not surprising, since the lower values on the USPHSscale for Z-CFPDs do not necessarily lead to an increased occurrenceof secondary caries, as grade Beta, which was almost exclusivelyawarded in this group, still indicates a clinically acceptable marginalfit. On the other hand, this could also be an effect of the small numberof participants in this study. Overall, however, the finding of lowermarginal quality in early zirconia restorations is not surprising,because the production technique was much less advanced 10 yearsago than it is today in terms of precision and accuracy of fit.Accordingly, a randomized, prospective clinical study by Sailer et al.in which metal–ceramic and zirconia-based FPDs were comparedafter 10 years showed that the proportion of insufficient margins(category Charlie/Delta in the USPHS criteria) in the zirconia groupwith a proportion of more than 50% was more than twiceas high [16].In the present study, restorations that did not show an acceptablemarginal seal during clinical try-in (tested with both low-viscositysilicone and a dental probe) were not inserted but newly fabricated.However, an exact measurement of the achieved fit (for example byuse of the replica technique) was not carried out in this study, so thatgroup differences may have existed from the outset, which nowbecame noticeable at the end of the 9-year functional period byincreasingly palpable restoration margins maybe as a result of wearin the area of the cement gap.
ween the baseline study and 9-year follow-up.
p, Mann–Whitney U test
C-CFPD (n = 6)
ean SD Median Percentile 25 Percentile 75
.28 0.62 0.33 �0.17 0.83 0.101
.58 0.40 0.67 0.50 0.83 0.138
.00 0.31 0.00 0.00 0.17 1.000
.25 0.65 0.33 �0.33 0.83 0.366
.28 0.67 0.50 0.17 0.67 0.073
.36 0.29 0.42 0.33 0.50 0.366
.13 0.48 0.17 �0.17 0.50 0.149
.17 0.54 0.25 �0.17 0.67 0.731
r follow-up. PPD = pocket probing depth. AL = attachment level. Z-CFPD = veneered

Table 6. Comparison of changes in PI (scale 0–3) and GI (scale 0–3) between study groups between baseline and follow-up after 9 years.
Variable Study group p, Mann–Whitney U test
Z-CFPD (n = 7) MC-CFPD (n = 6)
Mean SD Median Percentile 25 Percentile 75 Mean SD Median Percentile 25 Percentile 75
PI changeAbutment teeth �0.50 0.76 �1.00 �1.00 0.00 0.17 0.98 0.50 �1.00 1.00 0.295Reference teeth �0.43 0.93 �1.00 �1.00 0.00 �0.42 0.66 �0.50 �1.00 0.00 0.836
GI changeAbutment teeth �0.79 1.07 �1.00 �2.00 0.00 �0.17 0.52 0.00 �0.50 0.00 0.234Reference teeth �0.57 1.02 �0.50 �1.50 0.00 �0.17 0.82 0.00 �0.50 0.00 0.445
SD = standard deviation. Negative values indicate deterioration from baseline to 9-year follow-up. PI = plaque index. GI = gingival index. Z-CFPD = veneered zirconia cantileverfixed partial denture. MC-CFPD = metal–ceramic CFPD.
W. Bömicke et al. / journal of prosthodontic research 63 (2019) 334–339 339
The results of this study should be interpreted with caution. It isa pilot study with few participants. The small number of patients inboth groups and additionally the distribution in posterior andanterior CFPDs and the number of treating dentists may haveinfluenced the presented results. The number of participants wasparticularly low for specific criteria (USPHS, periodontal param-eters, GI, and PI) because CFPDs or abutment teeth were sometimeslost between follow-up examinations or were removed elsewherein the event of complications, although the study participants hadbeen instructed to contact the study physicians in such cases. Post-hoc sample size calculation revealed that 58 participants per groupwould have been necessary to be able to detect a statisticalsignificant difference between the groups with regard to theprimary outcome measure restoration survival. Finally, the studydoes not include results for 1 of the most common indications ofcantilever FPDs, which is replacement of the first molar to avoidremovable partial dentures. With regard to the question ofclarifying the risk of biomechanical complications for Z-CFPDscompared with a control group, however, the recorded data maysupport the design of a randomized clinical trial with a largernumber of participants.
5. Conclusion
Based on a very limited number of participants, veneeredzirconia and metal–ceramic CFPDs demonstrated no statisticallysignificant difference in terms of restoration survival after 9 yearsin clinical function. Further long-term observations with a largernumber of participants would be desirable to better assess thelong-term success of zirconia-based CFPDs.
Acknowledgments
We thank the participants in this study, for their patience andcooperation during the follow-up examinations. We are grateful to3M ESPE, Germany, for supplying the study materials andsupporting the study financially. 3M ESPE had no involvementin the conduct of the research and/or data collection and/or dataanalysis/interpretation and/or preparation of the article and/or thedecision to submit the article for publication. We thank HazelDavies for the English-language revision of the manuscript. Thiswas paid for with department funds.
References
[1] Karl M. Outcome of bonded vs all-ceramic and metal-ceramic fixed pros-theses for single tooth replacement. Eur J Oral Implantol 2016;9(Suppl.1):S25–44.
[2] Karlsson S. Failures and length of service in fixed prosthodontics after long-term function: a longitudinal clinical study. Swed Dent J 1989;13:185–92.
[3] Pjetursson BE, Tan K, Lang NP, Brägger U, Egger M, Zwahlen M. A systematicreview of the survival and complication rates of fixed partial dentures (FPDs)
after an observation period of at least 5 years. Clin Oral Implants Res2004;15:667–76.
[4] Brägger U, Hirt-Steiner S, Schnell N, Schmidlin K, Salvi GE, Pjetursson B, et al.Complication and failure rates of fixed dental prostheses in patients treated forperiodontal disease. Clin Oral Implants Res 2011;22:70–7.
[5] Sasse M, Kern M, Marré B, Walter MH. Clinical performance of cantileveredfixed dental prostheses abutments in the shortened dental arch. J Dent2014;42:373–6.
[6] Rehmann P, Podhorsky A, Wöstmann B. Treatment outcomes of cantileverfixed partial dentures on vital abutment teeth: a retrospective analysis. Int JProsthodont 2015;28:577–82.
[7] Mourshed B, Samran A, Alfagih A, Samran A, Abdulrab S, Kern M. Anteriorcantilever resin-bonded fixed dental prostheses: a review of the literature. JProsthodont 2018;27:266–75.
[8] Naumann M, von Stein-Lausnitz M, Rosentritt M, Walter C, Meyer-Lückel H,Sterzenbach G. Impact of simulated reduced alveolar bone support, increasedtooth mobility, and distal post-supported, root-treated abutment tooth onload capability of all-ceramic zirconia-supported cantilever FDP. Clin OralInvestig 2018;22:2799–807.
[9] Jepson N, Allen F, Moynihan P, Kelly P, Thomason M. Patient satisfactionfollowing restoration of shortened mandibular dental arches in a randomizedcontrolled trial. Int J Prosthodont 2003;16:409–14.
[10] Sharma A, Rahul GR, Poduval ST, Shetty K. Assessment of various factors forfeasibility of fixed cantilever bridge: a review study. ISRN Dent2012;2012:259891.
[11] Rinke S, Gersdorff N, Lange K, Roediger M. Prospective evaluation of zirconiaposterior fixed partial dentures: 7-year clinical results. Int J Prosthodont2013;26:164–71.
[12] Nicolaisen MH, Bahrami G, Schropp L, Isidor F. Comparison of metal-ceramicand all-ceramic three-unit posterior fixed dental prostheses: a 3-yearrandomized clinical trial. Int J Prosthodont 2016;29:259–64.
[13] Olsson KG, Fürst B, Andersson B, Carlsson GE. A long-term retrospective andclinical follow-up study of In-Ceram Alumina FPDs. Int J Prosthodont2003;16:150–6.
[14] Sailer I, Gottnerb J, Kanelb S, Hämmerle CH. Randomized controlled clinicaltrial of zirconia-ceramic and metal-ceramic posterior fixed dental prostheses:a 3-year follow-up. Int J Prosthodont 2009;22:553–60.
[15] Pelaez J, Cogolludo PG, Serrano B, Serrano JF, Suarez MJ. A four-yearprospective clinical evaluation of zirconia and metal-ceramic posterior fixeddental prostheses. Int J Prosthodont 2012;25:451–8.
[16] Sailer I, Balmer M, Hüsler J, Hämmerle CHF, Kanel S, Thoma DS. 10-yearrandomized trial (RCT) of zirconia-ceramic and metal-ceramic fixed dentalprostheses. J Dent 2018;76:32–9.
[17] Kern M, Passia N, Sasse M, Yazigi C. Ten-year outcome of zirconia ceramiccantilever resin-bonded fixed dental prostheses and the influence of thereasons for missing incisors. J Dent 2017;65:51–5.
[18] Wolfart S, Harder S, Eschbach S, Lehmann F, Kern M. Four-year clinical resultsof fixed dental prostheses with zirconia substructures (Cercon): end abut-ments vs. cantilever design. Eur J Oral Sci 2009;117:741–9.
[19] Zenthöfer A, Ohlmann B, Rammelsberg P, Bömicke W. Performance of zirconiaceramic cantilever fixed dental prostheses: 3-year results from a prospective,randomized, controlled pilot study. J Prosthet Dent 2015;114:34–9.
[20] Ohlmann B, Marienburg K, Gabbert O, Hassel A, Gilde H, Rammelsberg P.Fracture-load values of all-ceramic cantilevered FPDs with different frame-work designs. Int J Prosthodont 2009;22:49–52.
[21] Ohlmann B, Dittmar A, Rues S, Rammelsberg P. Comparison of fracture-loadvalues of cantilevered FDPs. Acta Odontol Scand 2013;71:584–9.
[22] Lindhe J, Nyman S. The effect of plaque control and surgical pocket eliminationon the establishment and maintenance of periodontal health. A longitudinalstudy of periodontal therapy in cases of advanced disease. J Clin Periodontol1975;2:67–79.
[23] Loe H, Silness J. Periodontal disease in pregnancy. I. Prevalence and severity.Acta Odontol Scand 1963;21:533–51.
[24] Silness J, Loe H. Periodontal disease in pregnancy. II. Correlation between oralhygiene and periodontal condition. Acta Odontol Scand 1964;22:121–35.
[25] Ryge G. Clinical criteria. Int Dent J 1980;30:347–58.