clinical application of a humanoid robot in pediatric cancer interventions
TRANSCRIPT

1 23
International Journal of SocialRobotics ISSN 1875-4791 Int J of Soc RoboticsDOI 10.1007/s12369-015-0294-y
Clinical Application of a Humanoid Robotin Pediatric Cancer Interventions
Minoo Alemi, Ashkan Ghanbarzadeh,Ali Meghdari & Leila Jafari Moghadam

1 23
Your article is protected by copyright and all
rights are held exclusively by Springer Science
+Business Media Dordrecht. This e-offprint
is for personal use only and shall not be self-
archived in electronic repositories. If you wish
to self-archive your article, please use the
accepted manuscript version for posting on
your own website. You may further deposit
the accepted manuscript version in any
repository, provided it is only made publicly
available 12 months after official publication
or later and provided acknowledgement is
given to the original source of publication
and a link is inserted to the published article
on Springer's website. The link must be
accompanied by the following text: "The final
publication is available at link.springer.com”.

Int J of Soc RoboticsDOI 10.1007/s12369-015-0294-y
Clinical Application of a Humanoid Robot in Pediatric CancerInterventions
Minoo Alemi1,2 · Ashkan Ghanbarzadeh1 · Ali Meghdari1 ·Leila Jafari Moghadam3
Accepted: 28 February 2015© Springer Science+Business Media Dordrecht 2015
Abstract This paper propounds a novel approach byexploring the effect of utilizing a social humanoid robot as atherapy-assistive tool in dealing with pediatric distress. Thestudy aims to create a friendship bond between a humanoidrobot and young oncology patients to alleviate their painand distress. Eleven children, ages 7–12, diagnosed withcancer were randomly assigned into two groups: a socialrobot-assisted therapy (SRAT) group with 6 kids and a psy-chotherapy group with five kids at two specialized hospitalsin Tehran. A NAO robot was programmed and employedas a robotic assistant to a psychologist in the SRAT groupto perform various scenarios in eight intervention sessions.These sessions were aimed at instructing the children abouttheir affliction and its symptoms, sympathizing with them,and providing a space for them to express their fears andworries. The same treatment was conducted by the psychol-ogist alone on the control group. The children’s anxiety,anger, and depression were measured with three standardquestionnaires obtained from the literature before and afterthe treatment (March et al., in J Am Acad Child AdolescPsychiatry 36:554–565, 1997; Nelson and Finch, in Chil-dren’s inventory of anger, 2000; Kovacs, in PsychopharmacolBull 21:995–1124, 1985). The results of descriptive statistics
B Ali [email protected]://meghdari.sharif.edu
Minoo [email protected]://sharif.ir/∼alemi/
1 Social Robotics Laboratory, Center of Excellence in Design,Robotics, and Automation Sharif University of Technology,Tehran, Iran
2 Islamic Azad University, Tehran West Branch, Tehran, Iran
3 Mahak Hospital and Rehabilitation Complex, Tehran, Iran
and MANOVA indicated that the children’s stress, depres-sion, and anger were considerably alleviated during SRATtreatment and significant differences were observed betweenthe two groups. Considering the positive reactions from thechildren to the robot assistant’s presence at the interven-tion sessions, and observing the numerical results, one cananticipate that utilizing a humanoid robot with different com-munication abilities can be beneficial, both in elevation ofefficacy in interventions, and fomenting kids to be more inter-active and cooperative in their treatment sessions. In addition,employing the humanoid robot was significantly useful inteaching children about their affliction and instructing themin techniques such as: relaxation or desensitization in orderto help them confront and manage their distress themselvesand take control of their situation.
Keywords Social robot-assisted therapy (SRAT) · Cancer ·Anxiety · Anger · Depression
1 Introduction
Treatment of cancer, besides its hardships and setbacks, hasconsiderable mental and physical side effects that may be assignificant as the disease itself. Psychological distress, anxi-ety, reduction of appetite, and weight loss are among the mostprevalent symptoms in cancer patients at all stages of treat-ment. Distress symptoms have been found to be prevalent inchildren suffering from cancer, in a spectrum from mild tocritical, thereby producing a major obstruction in the pathof acceptance of treatment and the patient’s adaptation to it.One can measure the children’s distress symptoms such as:anxiety, anger, and depression with standard questionnairesbefore and after treatment [1–3]. To deal with this psy-chological suffering, researchers have proposed and tested
123
Author's personal copy

Int J of Soc Robotics
several methods such as: relaxation, hypnosis, desensitiza-tion, and distraction [4–13]. In the physical respect, chronicpain, post-operational pain and anticipatory nausea are com-monly observed in most patients suffering from cancer [4].Reduction in the intensity of these symptoms, and the sub-sequent enhancement in patients’ mental health can, in turn,ease the medical treatment.
In recent years, numerous studies have been conductedin this area, with the aim of alleviating the aforemen-tioned symptoms through non-pharmacological interven-tions. Early organized attempts to define and diagnosecancer-related distress were made by “The National Com-prehensive Cancer Network” (NCCN) in 1999. According toNCCN guidelines, distress -in the scope of cancer- is referredto as a multifaceted emotional experience that could interferewith patient’s capabilities in coping with cancer, its physicalsymptoms, and treatment [4,5].
As for diagnosis of distress, early monitoring and identifi-cation were found to be effectual. The distress thermometer(DT) is an initial instrument for screening distress, proposedby NCCN. This measurement tool has a rating scale of 0–10 which can be effectively utilized in classifying distresslevels from mild (DT of 0–4) to moderate or severe (DTmore than 4). Mild distress, which encompasses symptomssuch as fear, doubt, and preoccupation about the future, treat-ment and death, is observed in most patients. At a moderateor severe level, which is recognized by excessive worries,hopelessness, and spiritual crises, referral to a mental healthprofessional is mandatory.
Distress treatment in cancer patient consists of psy-chological and psycho-pharmacological methodologies. Inpsychological intervention, which is the focus of this review,cognitive-behavioral therapy (CBT) and group therapy havebeen successful in decreasing distress and enhancing thequality of life in cancer patients. CBT concentrates on thecorrection of automatic thoughts that result in depressionand other forms of distress. This method has been provedto be fulfilling in appeasing the physical and psychologicalsymptoms of distress, including depression, anxiety, cancerfatigue and pain [4,14–18].
Various forms of group therapy have been studied inthe context of cancer, all of which have shown improve-ment in adjustment skills, pain management, and traumaticstress among adult cancer patients. Three major methodsin these studies are supportive-expressive (SE), cognitive-existential (CE), and meaning-centered (MC) group therapy.The first type has proven to be undeniably effective in elevat-ing the quality of life, enhancing psychological symptoms,and assuaging pain among patients diagnosed with metastaticbreast cancer [19]. CE and MC approaches in group therapyhave exhibited significant impact on reducing cancer dis-tress in women with early-stage cancer, and patients withend-stage cancer, respectively [20–23].
Researchers suggest that mind-body interventions, includ-ing hypnosis, distraction, and imagery, may be effective,alone or as adjuncts to pharmacological interventions, inmanaging procedure-related pain, anxiety, and distress inpediatric oncology [4–13]. In addition to psychological inter-ventions, behavioral techniques have displayed effectiveresults in the management of cancer distress. These tech-niques include relaxation, distraction, desensitization, andhypnosis and all have been modified with regard to age-considerations, so that they could be used in child patients [4].Utilization of the mentioned methods has been shown to beeffective in the management of anticipatory nausea and vom-iting, and ameliorating anxiety [24–26]. Behavioral methodshave been recognized as the primary means of pacifyingside effects in pediatric afflictions that require periodic treat-ment procedures by the World Health Consensus Conference.Wide adoption of these methods is due to the comparativesimplicity of their application and directness of the beneficialinfluence they provide for patients, in their most vulnerablemoments [24].
Hypnosis and relaxation both involve guided imagerymethods in which the patient learns to concentrate her atten-tion on thoughts far from the source of distress. In general,the patient is relaxed via a meditation journey to enjoyableplaces, while the psychologist/psychiatric verbally guidesher through the feeling of calm and well-being. Since, bothrelaxation and hypnosis constitute deep-breathing and theuse of imagining pacifying pictures, it is hard to differenti-ate between these two in clinical practice [24]. Hypnosis andrelaxation were also successful in lessening procedural painin cancer care, both for adults and children [8–12]. Distrac-tion diverts the patient’s attention from the invasive proce-dures, resulting in reduction of pain and anxiety. This tech-nique can be carried out by engaging the participant in highlyinteresting tasks such as guided imagery, storytelling, play-ing video games, or playing with a party blower [13,24–28].
In the category of behavioral techniques, other methodsare observed. These encompass modeling, emotive imaging,and cognitive restructuring. Modeling is basically instructingpatients in the required coping skills via demonstrating theactual procedure or a videotape containing successful similarexperiences. Emotive imaging is most commonly executedwith children. This method assimilates personal storytellingand makes use of a child’s active imagination. In fact, in aseries of stories, the favorite hero/heroine of the child comesto aid her during the feared procedures, and she and the heromanage the situation together. In cognitive restructuring, thepatient is persuaded to reframe his beliefs and thoughts inviewing stressful or fearful events, in a way that make themless threatening [24].
Whereas all types of behavioral interventions have por-trayed positive impacts in the scope of distress, studies showthat they are not equally efficacious in practice. In Liossi and
123
Author's personal copy

Int J of Soc Robotics
Hatira’s study, CBT and hypnosis approaches both displayedpromising outcomes in the relief of pain; still, hypnosisappeared to have better results in controlling anxiety anddistress [29]. Some studies combine two or more behav-ioral techniques to see whether the effectiveness of distressreduction could be increased. As a recent example, Shockeyand others’ study merged relaxation techniques with biofeed-back, and resulted in beneficial coping and pain managementstrategies in children [30,31].
Alongside the advances in psychological methods, theprogress in social robotics (SR) has prompted tremendouspotentials in patient–robot interactions. Clinical and educa-tional applications of robots are of distinct importance incases involving children, since robots have attractive featuresthat can increase the efficacy of communication [32–34].One of the recent research concentrations has been in theutilization of humanoid robots in both diagnosis and treat-ment of autism spectrum disorders (ASD). These studies haveproved that the use of interactive robotics not only raisesautistic children’s interest in treatment sessions, but also pro-vides more responsive feedback from them, when comparedto cases in which only a human administers the treatmentprocess [35,36]. Researchers utilizing robots as autism ther-apy devices have reported an increase in levels of attention,engagement, and social behaviors like unrehearsed imitationand joint attention in the presence of social robots as a partof the treatment. This improvement in catching the atten-tion of autistic children and teenagers can be ascribed to thenovel sensory impetuses robots provide, such as the displayof emotions [35–41]. In addition, it has also been reportedthat companion robot could fulfill a number of specific func-tions to support diabetic children in their daily lives [42].
In the study at hand, in an original and novel proce-dure, we tried to combine psychological methods with socialapplications of a humanoid robot to observe its influenceon distress management of pediatric cancer patients. Severalfactors have been considered in this study such as encompass-ing the short-term changes in the children’s level of anxiety,depression and anger. The robot acted as an assistant to thepsychologist (or psychiatrist) in order to work on the abovementioned factors with children through several pre-plannedscenarios, each of which focused on one concept. These sce-narios were performed in an interactive manner between thetrainer, the psychologist, the robot, and the kids. The con-cepts of these plays were selected from the common issuesof children in oncology sections of hospitals. In the case oftypical psychological intervention, the treatment was carriedout directly, while in the human-robot interactive approach,our effort was to make use of the NAO’s baby face and voicetone to convey the instructive messages in an indirect andmore enjoyable manner. Moreover, the humanoid robot usedin this study was able to exhibit sympathetic emotions withspeech tone and body motions and could play a part that was
close to the child being treated. Therefore, it could providethe incentive for the child to express his or her feelings, andthereby engender enhancements in targeted factors increas-ing the efficacy of the treatment as a whole. Consequently,possibly it reduces the rate of death among kids with cancer.
2 Research Questions
In this study, the answers to the following questions are to beinvestigated:
(a) What are the anxiety, anger, and depression levels of thechildren with cancer before and after social robot-assistedtherapy (SRAT) and psychotherapy?
(b) Is there any significant difference between SRAT andpsychotherapy groups regarding their anxiety, anger, anddepression levels after their therapies?
3 Method
3.1 Participants
Participants were gathered for an 8-sessioned period (24April to 12 May, 2014), from a non-governmental hospital,MAHAK, specializing in pediatric cancer, and the oncol-ogy sector of another medical center, the Children’s MedicalCenter (ChMC). Due to the unavailability of patients forcontinuous 1-month duration, and the difference in theirtreatment protocols, only 11 children who were in the samestage of cancer met the criteria for taking part in this study;therefore, the patients were homogeneous. Due to the unpre-dictability of the patients’ health status, the project wasdesigned in a short-term outline. During the trial, all childrenwere receiving active treatment and were able to attend thescheduled sessions. Participants were chosen in an age rangeof 7–12 years old, with an average age of 9.5 (SD = 1.63).Table 1 shows the SRAT group participants’ specifications,and the sessions each of them managed to attend.
The control group was also selected randomly from avail-able patients in both medical centers. The psychotherapygroup participants’ specifications and their attendance areshown in Table 2. (Average age = 9.8, SD = 1.36). Obvi-ously, the members of each group did not have any contactwith each other throughout the project. Finally, 10 partic-ipants were included in the data analysis since one of thepatients in the SRAT group did not take part in the post-test.
3.2 Instrument
The core device of this study was the NAO (renamed Nima, aPersian name, in order to appear more acceptable and friendlyto Iranian kids), a programmable humanoid robot developed
123
Author's personal copy

Int J of Soc Robotics
Table 1 SRAT group participants’ specifications and their attendance
Attendance distribution in 8 sessions
Medical Center
Duration of treatment (months)
Age (y)
GenderParticipant’s No.
1234567 & 8
CHMC1810Girl1CHMC2410Girl2CHMC307Girl3MAHAK3611Boy4MAHAK2410Girl5MAHAK129Girl6
Present: Absent:
Table 2 Psychotherapy group participants’ specifications and their attendance
Attendance distribution in 8 sessions
Medical Center
Duration of treatment (months)
Age (y)
GenderParticipant’s No.
1234567 & 8
CHMC1812Girl1CHMC2210Girl2CHMC367Girl3MAHAK3011Girl4MAHAK209Girl5
Present: Absent:
by Aldebaran Robotics Company. Its physical specificationsare presented in Table 3.
Nima is capable of displaying human-like body gestures,speaking, playing sound effects and music, and dancing.All of the mentioned capabilities can be designed and pro-grammed in order to display the desired and pertinent actions.Though, this robot can be coded to react actively to externalstimuli such as sound or movement, and therefore becomeindependent from a programmer’s intervention, because ofthe limitations in the study, and it’s instructive and interac-tive purposes, all scenarios were designed in a preplannedmanner. The conversations between two trainers (one psy-chologist and the study investigator) and robot, and also therobot’s dialogs to the children were all composed and loadedon the device before each session. All Nima’s dialogs wererecorded in the Persian language in order to be fully under-standable to Iranian children. The software used to designand plan Nima’s speeches and animations was Choregraphe1.14.5 developed by the original company. Choregraphe isa multi-platform desktop application that allows the user toconnect to the real robot, and conveniently create animationsfor its joints and body parts, as well as synchronizing themoves with dialogs.
After designing and loading the scenarios, a humanoperator took charge of sending commands from a laptop(Windows 7, SP1, 2.5 GHz processor), via a modem to NAO
at suitable times, and in accordance with the outline and thefeedback from patients. Another laptop (Windows XP, SP2,1.0 GHz processor) was utilized to display presentation slidesfor each session.
3.3 Questionnaires
Three factors were assessed by three standard psychologicalquestionnaires (See Appendix), scaled for children [1–3]. Alltests were administrated twice, prior to the first and after theeighth sessions.
Anxiety This factor was assessed with the Multidimen-sional Anxiety Children Scale (MASC). This test was devel-oped by March and others for an age span of 8–18 [1], andits validity for Iranian children was confirmed in a report byMashhadi and others for a sample of 507 students from the3rd, 4th, and 5th grade [44]. MASC has 39 items, format-ted in Likert self-report on a 4-point rating response choice[ranging from Never (1) to Always (4)]. It measures anxietylevel in four different categories: physical symptoms (itemno.: 1, 5, 8, 12, 15, 18, 20, 24, 27, 31, 35, 38), social anxiety(item no.: 3, 10, 14, 16, 22, 29, 33, 37, 39), harm avoidance(item no.: 4, 11, 17, 19, 23, 26, 30, 34), and separation anxiety(item no.: 2, 6, 9, 13, 21, 25, 28, 32, 36) [1,44].
Depression Depression was measured by Kovaks’ (1985)Children’s Depression Inventory (CDI), developed for indi-
123
Author's personal copy

Int J of Soc Robotics
Table 3 Some physical andtechnical specifications of theNAO Robot
Nao Next Gen (2011)
Height 58 cm (23 in)
Weight 4.3 kg (9.5 lb)
Autonomy 60 min (active use),90 min (normal use)
Degrees of freedom 21
CPU Intel Atom @ 1.6 GHz
Built-in OS Linux
Compatible OS Windows, Mac OS,Linux
Programming languages C++, Python, Java, MAT-LAB, Urbi, C, .Net
Vision Two HD 1280 × 960cameras
Connectivity Ethernet, Wi-Fi
viduals from 7 to 17 years old. CDI is a self-report test andcontains 27 items. Each item asks the participant to decideamong three different choices, with regard to what he felt,thought or how he behaved in the past two weeks. Items arerated from 1 to 3. Higher scores show more depressive symp-toms [3,43]. Confirmatory retests for CDI in Iran were alsoreported in [44].
Anger Children’s Inventory of Anger (CIA, Nelson andFinch, 2000) was employed to measure this factor in par-ticipants. CIA consists of 39 items, and was developed foryoungsters between 6 to 16 years old. Similar to MASC, eachitem response is given in a 4-point format. CIA yields foursubscales scores in different areas which might arouse angerreactions in children: Physical Aggression (10, 11, 12, 22,23, 24, 35, 36, 37), Frustration (1, 2, 3, 12, 14, 15, 25, 26, 27,28, 38), Peer Relationships (7, 8, 9, 19, 20, 21, 32, 33, 34),and Authority Relations (4, 5, 6, 16, 17, 18, 29, 30, 31, 39)[2,45].
It is important to note that all these tests were adminis-trated on paper, and the kids were given a sufficient amountof time to answer the questions. A psychologist and trainedperson were present at the time children were filling the ques-tionnaires to clarify if the kids had any questions. In general,the questions were clearly read by a psychologist and partic-ipants marked the answer closest to their feelings for eachquestion. Most questions were easy for kids to understand,yet, some questions were first elucidated with some exam-ples and if kids needed further explanations, the psychologistwould explain it to them. Each questionnaire took about 15–20 min for participants to complete (all questions were to beanswered), and the kids had a short break between two teststo refresh their minds. Psychologists strived to have the leasteffect on children’s answer, and the participants were seatedin different places, so that they could not see each other’sanswers.
3.4 Intervention (Data Collection)
With respect to the study’s objectives, eight scenarios werecomposed, each focusing on a concept of major importancefor the children who were receiving treatment. The generalplot was primarily based on the conjecture that knowingabout the procedure and the necessity of their treatment couldmeaningfully influence the child’s level of acceptance, coop-eration, and adjustment. Hence, each session was designed torevolve around a definite subject chosen from the children’smain concerns. Moreover, the sessions were designed for agroup of children, and not for individual patients. This studyis also classified as a Wizard-of-Oz experiment since thepatients interact with a robot which is operated by a humanbeing.
The NAO robot was programmed to play a different rolein each session, and convey all the general and necessaryinformation that could serve the purpose of reducing distress.Alongside with making children aware of their condition,Nima displayed a sense of sympathy with the situation thatpatients were in.
In this study, Nima was introduced as a baby robot thathad an illness similar to the patients and was mandated by adoctor to attend hospital twice every week to obtain his doseof chemotherapy. After the first session (introduction), Nimastarted to take various parts such as a doctor, a nurse, or acook, with the aim of not only elevating his own knowledgeof cancer and its treatment (the purpose that was told to thechildren), but also to transmit this awareness to the kids witha tone apropos to their age.
The abridged outline and main ideas of each scenario areas follows:
(1) I ntroduction Nima introduces himself and talks aboutthe place he comes from and his family. Then he involves
123
Author's personal copy

Int J of Soc Robotics
Fig. 1 The psychologist with the patients and the NAO robot acting ill
the kids in a discussion about why he wants to come tothe hospital for several weeks and spend time with them.After speaking about his illness, he confesses that he isscared of the hospital (letting the patients know that it isnormal to be afraid and they are not alone) and the onlything that motivates him to overcome his fear is to seethe children and become a close friend to them. Then thetrainers promise the robot and children to find a way tomanage their fear and stress (see Fig. 1a).
(2) Nima as a doctor Since Nima is a robot; he tells thekids that by connecting to the internet he can learn aboutmany subjects in a short time. At the beginning of thissession, he connects to the network and then he turnsinto Dr. Nima. Children are given all the information theyrequire about the medical devices, treatment procedures,possible surgeries, and the reasons why they should gothrough all these. There will be a discussion about whysometime doctors are not responsive to the kids due tothe doctor’s fatigue.
(3) Nima as chemo-hero This session is adopted from abook named “Chemotherapy Hero” by “P. Lajevardi”(in Persian) [46]. This book contains the story of Mr.Chemotherapy’s battle with cancerous cells. Nima whohas collected data by talking to one of these heroes,grows into Nima-Hero, and narrates all the adventuresthe heroes go through to lead the “ill cells” out of thebody. There is a brief disquisition on body cells, andchildren will become acquainted with “healthy” and “ill”cells. The reason why kids become nauseous, or losetheir hair is related to Chemo-Heroes’ getting lost in thestomach or mistakenly harming healthy cells. The majordisparity between this scenario and the book’s storylineis that unlike the book, cancerous cells are not depicted as“bad” or “harmful” cells, but rather “ill”, “unsociable”,and “impatient”, so that children don’t make the incor-
rect assumption that they have done something wrong orbad and now these bad cells are in their bodies to punishthem. Also, the “ill” cells are not killed in this scenario;still, they are sucked into Mr. Chemotherapy’s stomachand then thrown outside the body. At the end, kids areawarded with a “Braveness Accolade” to celebrate theirresilience.
(4) Nima as a nurse This session is centered on the fear andpain management of injection, and other invasive pro-cedures. Nurse Nima first explains about the necessityof vessel injections and how drugs are delivered to cellsthrough veins. Afterwards, Nima asks each child to cre-ate a good message for their cells, send it to them, andalways repeat it before getting an injection. This part wasdesigned for kids to have positive images about their cellsand body parts’ getting better. Then Nima teaches thekids a relaxation method designed to decrease their painand stress. This method is called “robot-spaghetti” and isanalogous to other relaxation techniques. First, the kidsare encouraged by Nima to act and move like a robot,i.e. stiffen their body, and then in a playful way, they aretold to loosen themselves as spaghetti. This relaxationmethod is practiced several times with the help of a psy-chologist, in order for children to master it. At the endof the session there are discussions on sanitary points,and washing hands, brushing teeth, and drying skin afterbath are practiced in a way that is most preferred for thesechildren.
(5) Nima as a cook This time, Nima appears as an adeptcook who is willing to aid children to eat well andwholesomely. In the beginning Nima explains the specificmethods and foods that are able to reduce the feeling ofnausea. Then, he talks about how kids can improve theirappetite by walking for a short time or engaging in intel-lectual games. Moreover, a number of nutritious foods are
123
Author's personal copy

Int J of Soc Robotics
introduced. At the end of the session Nima teaches thekids how to use their imagination power to make eatingtheir meals more joyous.
(6) Nima as an ill kid In this session, as a part of the sce-nario, Nima is to lose his memories due to a technicalincident. At first, Nima covers himself under a blanket todemonstrate his sickness (see Fig. 1b). Then kids findNima as a sad and cranky child. Inasmuch as he haslost his memory, he doesn’t know why he has to cometo the hospital and why he needs to take his medicine.Also, he is very scared of the injection, he doesn’t eat hismeals, and he cries most of the time. Now it is time togive the children a chance to be the “wise” and “power-ful” ones. This time, the kids are asked to help Nima toovercome his stress, lack of appetite, and fear. They cansympathize with Nima’s condition, which is also theirown condition sometimes. Additionally, this session isabout the empowerment of the kids, to see themselvesas strong and knowledgeable. The level of kids’ under-standing from previous sessions is also tested throughoutthe session. It’s worth mentioning that this session wasliked the best since the kids sympathized with Nima andtried to help him to get over his disease.
(7) Hopes and dreams After learning about various aspectsof their disease, it is time for children to possess a clearervision about their future. As many children lose their hopefor the future in the situation of confronting assiduousillnesses, this session is dedicated to their lost dreamsand hopes. In the beginning, Nima tells the children thathe is not certain what he will become when he growsup, and asks them to help him choose a way that is bestfor him. He starts to talk about different vocations suchas engineering, medicine, and art. Also, he introducessignificant achievements in the scientific arena which canhelp needy people. Then, the kids share their opinions ontheir desired future jobs. At the end, Nima says that he cantake the children’s wishes to the moon, where a “meetingof space robots is going to be held”, and make them true!Yet, they can only come true, if the kids believe in themand try to achieve them.
(8) Saying goodbye In this last session, the photos that weretaken from previous sessions are displayed and kids areasked to guess to which session each image belongs. Inthis manner, kids can review what they have gatheredthroughout this trial. Then, the children are involved inan instructive game. Nima plays a short dialog from onearbitrary session, and the kids, as a team, guess fromwhich session this dialog has been selected and played. Toencourage them to be responsive, small incentives such aschocolates or applause by Nima were used. The sessioncloses with Nima’s dancing and singing which is the lastscene the children will have from him, before he leaves.
Table 4 Clinical goals of each intervention session
Session Clinical Objective
Introduction Children getting prepared to communicatewith the NAO robot, sharing fears andworries in a hospital milieu
Nima as a doctor Getting more acquainted with the hospitaland its different sections, treatment anddiagnostic procedures, kid’s confrontingtheir fears and stress by making themaware of the reason behind eachprocedure, kid’s expressing theirfeelings and sharing their emotionsabout various kinds of treatment
Nima as chemo-hero Establishing a positive image aboutchemotherapy and its adverse sideeffects, appreciation of kid’s forbearanceand bravery against the disease
Nima as a nurse Instruction in important points abouthygiene and respecting children’sindependence in their everyday tasks,teaching kids how to relax themselveswith the “robot-spaghetti” techniquewhile listening to soothing music
Nima as a cook Introducing beneficial and necessaryfoods while constructing an image abouttheir advantages for health and strength,instructing methods to reduce nausea,discussing various solutions to increaseappetite
Nima as an ill kid Kid’s developing a sense of sympathywith a sick and confused robot whilecomparing him with themselves, seeingthemselves in the “sad”, “cranky”, andoccasionally “angry” ego of Nima, andalso in the state of power and wisdom
Hopes and dreams Giving children hope for their future life,and helping them visualize themselvesin inspiring, wonderful, andadvantageous jobs when they grow up
Saying goodbye Reviewing the instructed concepts duringprevious sessions, preparing the kids tosay farewell to Nima
The clinical objective of each session is presented briefly inTable 4.
3.5 The Performance of Sessions
All sessions were performed in the play room of the medicalcenters. These rooms were equipped with basic accommoda-tions, such as chairs, tables, monitors, and some toys. Eachsession began with the robot saying hello and revealing hisemotions for his “new friends”. After warming up to theambience, Nima pretended that he was connecting to thenetwork by playing a special sound, and acquiring informa-tion associated with his role. Then, some costumes (such
123
Author's personal copy

Int J of Soc Robotics
as a hat for a nurse, or cloak for a hero) were put on therobot and the session continued with different discussions onsignificant subjects. Each discussion was initiated by Nimawith a digest disquisition in the form of instructive data or asimulated experience in 3–5 min timeframes. All the robot’sactions were guided by a trained operator, whose control ofthe robot was not observed by the children, via an ordinarycomputer. Afterward, the robot remained silent, pretendinghe was carefully listening to the kids’ opinions and sharingexperiences, for example about spending time in the CT scan-ning machine. Then, the psychologist and/or a trained person(experienced in communication with children) intervened toencourage the participants to get involved in discussions andexchange their feelings. The trainers also elucidated any pos-sibly vague concept for the kids.
Nima’s program was designed to constitute some encour-aging comments such as “bravo!” or “how interesting!” asinducements for the kids to be active and expressive. Thesecomments were performed by the operator’s order at the righttime, via a computer-modem-robot connection. Sessions usu-ally closed with a cheerful song accompanied with Nima’sdancing, to enhance the children’s mood and instigate themto participate in the next sessions.
Generally, all sessions consisted of a number of specialactions designed for Nima to make the concepts more endur-ing in the children’s memories and thus, render them moreeffective. Furthermore, some tasks were assigned to the chil-dren in the middle of the session to engage them as muchas possible (see Fig. 1). A summary of these actions aredescribed as following:
• Introduction When Nima was showing his fear of thehospital, both his voice and hand were designed to shake.Kids were fomented to express their own fears so that“Nima doesn’t feel that he is the only one scared.”
• Nima as a doctor In the part that Nima talked about CTscanning or the MRI machine, he started to act as if he waslying on the machine bed (actually, a table in the room).Then, as planned, he began to play peaceful music to calmhimself, while he theatrically waited for the scans to betaken. Also, he narrated a short funny story to teach thechildren some possible ways to have fun when they are inboring situations like waiting in such medical machines.
• Nima as chemo-hero Nima exhibited some karate figuresto show his swiftness and bravery in chasing “sick” and“impatient” cells. At the end, it was asked from Nimawhat heroes do when they win over the sickness, andhe replied they would dance, and subsequently began todance cheerfully.To teach the kids about how “tumors” might form in thebody, a medium-sized piece of play dough was given toeach of them. Then they were asked to turn that pieceinto several small segments, as they desired. These tiny
pieces could be the portrayal of “sick” cells. In the storyof Mr. Chemotherapy, the “sick” cells, gather in a group(the tumor) to avoid loneliness. So, the kids were told tocollect the pieces and attach them together to see howmasses may form inside their own bodies.
• Nima as a nurse Nima performed the aforementionedrelaxation method one time, and when he was in his“stiffen robot” mode (in opposition to spaghetti) mode,he instigated the kids to mimic his funny hand and headmovements. Also, a towel was brought to the room andthe most suitable way to dry sensitive skin (putting thetowel on skin and picking it up repetitively) was taughtto them.
• Nima as a cook According to what children reported, themost interesting part of this session was the pictures dis-played on the screen. A picture of each beneficial foodNima described was shown to the participants, so thatthey could bear that in mind. Also, an adequate amount oftime was dedicated to the kids’ opining on their favoritefoods and imagining them. Finally, the correct way ofwashing hands was shown and practiced for 20 s, byNima, trainers, and of course the kids.
• Nima as an ill kid Sad music was played by Nima at thebeginning of the session. Also, Nima had a sad and peev-ish tone in all of his dialogs. An artificial IV serum wasattached to Nima’s body as a demonstration of his analo-gous situation to the kids. At last, when Nima recoveredhis memory (a part of the scenario), he played a cheerfulsong to show his appreciation (see Figs. 1 and 2). Thisscenario was also planned to convey the message thatawareness could bring more comfort and happiness.
• Hopes and dreams Since the first section of this sessionwas about some interesting jobs kids could have in thefuture, Nima was designed to act out each vocation ashe discussed them. For example, he pretended that hewas riding a plane (with its take-off sound) when he wasshowing his enthusiasm for becoming a pilot in the future.He also acted as an opera singer and a policeman, forchildren to guess what he was trying to be (see Fig. 2).
As observed, all of these special performances elevated theparticipants’ cooperation in doing the assigned activities andmade the sessions more enjoyable and friendly. Moreover,they gave the robot a human character with whom the kidsfelt much more close and easy to communicate. The mainpurpose was to make the best use of the robot in an interven-tion practice.
4 Results
In order to answer the first research question on groups’ anx-iety, anger, and depression levels, first the mean and standarddeviation of each group were computed (see Table 5).
123
Author's personal copy

Int J of Soc Robotics
Fig. 2 The NAO robot entertaining and performing for the patientswith the help of education specialists and psychologist
As shown in Table 5 (and clearly in Fig. 3), the total meanfor (all the psychological scores based on the scales summedup and divided by the number of the patients to get the averagescore) the anxiety scores for the experimental-group’s pre-test is 2.23 and their post-test is 1.89. However, the anxietyscore of control group’s pre-test is 2.36 and their post-test is2.38. This shows the anxiety level in the experimental groupwas lowered while that of control group even increased a bit.With regard to depression level, the experimental group’s pre-test is 1.35 and their post-test is 1.00, however, that of thecontrol group’s pre-test is 1.31 and post-test is 1.30 indicatingdepression level decreases just in the experimental group,but control group didn’t improve. Regarding anger level, theexperimental-group’s pre-test is 2.73 and their post-test is2.31 whereas that of the control group’s pre-test is 2.60 andpost-test is 2.82. The results revealed that the anger levelincreased in the control group while it was alleviated in theexperimental group as they calmed down. This shows thatthe kids are almost fed up with hospital personnel interactionregarding their treatment; their psychologist either was notpatient enough or not attractive enough to influence and helpthe kids to lower their anger; however, the psychologist wasthe same for both groups. Kids with cancer appear to needmore attention, sympathy, and novelty in terms of treatmentduring their therapy.
In order to answer the second research question, “Is thereany significant difference between SRAT and psychotherapy
Table 5 Descriptive statistics of experimental and control groups(pre/post-tests)
GROUP Min Max Meana SD
Experimental Total anxiety(pre-test)
1.90 2.49 2.23 0.227
Total anxiety(post-test)
1.69 2.18 1.89 0.203
Total depression(pre-test)
1.26 1.48 1.35 0.093
Total depression(post-test)
1.07 1.26 1.00 0.078
Total anger(pre-test)
2.10 3.41 2.73 0.546
Total anger(post-test)
1.97 2.82 2.31 0.313
Control Total anxiety(pre-test)
2.05 3.10 2.36 0.440
Total anxiety(post-test)
2.00 3.05 2.38 0.425
Total depression(pre-test)
1.11 1.59 1.31 0.195
Total depression(post-test)
1.04 1.52 1.30 0.180
Total anger(pre-test)
1.95 3.18 2.60 0.504
Total anger(post-test)
2.67 3.00 2.82 0.161
SD Standard deviationa The numerical average of participants’ scores, out of 4 for anxiety andanger scores, and out of 3 for depression scores
Fig. 3 Descriptive statistics of the overall post-test mean of anxiety,depression, and anger of both groups
groups regarding anxiety, depression, and anger levels aftertherapy”,a multivariate ANOVA (MANOVA) was run on thegained scores (post-test minus pre-test) of the subjects inorder to probe which group(s) showed significant decreases
123
Author's personal copy

Int J of Soc Robotics
Table 6 Descriptive statisticsfor experimental and controlgroups (mean difference ofgained scores)
Dependent variable GROUP Mean difference Std. error 95 % Confidence interval
Lower bound Upper bound
Gained scores Experimental −0.34 0.05 −0.47 −0.20
Anxiety Control 0.01 0.05 −0.11 0.15
Gained scores Experimental −0.16 0.03 −0.24 −0.07
Depression Control −0.01 0.03 −0.09 0.07
Gained scores Experimental −0.40 0.13 −0.71 −0.08
Anger Control 0.21 0.13 −0.09 0.52
Table 7 Multivariate tests
Effect F Sig. Partial eta squared
Intercept Wilks’ lambda 5.25 0.041 0.724
GROUP Wilks’ lambda 7.89 0.017 0.798
in their anxiety, depression and anger after receiving theirtherapy.
It should be mentioned that the assumptions of homogene-ity of variance (anxiety = 0.50, depression = 0.73, anger =0.26) and covariance (sig = 0.64) were met since the proba-bilities associated with Levene’s values were all higher than0.05.
As shown in Table 6, the experimental group showed moreloss of anxiety (Exp Mean = −0.34vs. Control Mean =0.018), depression (Exp Mean = −0.16vs. Control Mean =0.012) and anger (Exp Mean = −0.40vs. Control Mean =0.216).
The results of the MANOVA (F (3, 6) = 7.89, P < 0.05,Partial η2 = 0.79 representing a large effect size) shown inTable 7 indicated that there were significant differencesbetween the loss of anxiety, depression and anger of theexperimental and control groups. Based on these results itcan be concluded how much robot therapy has a positiveeffect on the children.
Table 8 displays the comparisons made between the twogroups on each test. Based on these results and the descriptivestatistics displayed in Table 6 it can be concluded that;
A: The experimental groups (M = −0.34) showed sig-nificantly more loss of anxiety than the control group(M = 0.018)(F (1, 8) = 19.14, P < 0.05, Partial η2 =0.70 representing a large effect size).
B: The experimental groups (M = −0.16) showed sig-nificantly more loss of depression than the control group(M = 0.012) (F (1, 8)=8.66, P < 0.05, Partial η2 =0.52representing a large effect size).C: The experimental groups (M = −0.40) showed sig-nificantly more loss of anger than the control group(M = 0.216) (F (1, 8)=10.28, P < 0.05, Partial η2=0.56 representing a large effect size).
The results revealed that the control group did not improve inany of the anxiety, depression, or anger levels while the exper-imental group clearly showed us that the use of a social robotas a psychologist assistant helped to lower the children’s psy-chological problems. It is worth noting that the robot affectedthe SRAT group’s anger the most and it shows that Nima couldhelp the kids to calm down by educating them about their ill-ness and how they can overcome it. Moreover, Nima provideda happy atmosphere for the kids by entertaining them withdancing, making jokes and laughing.
The kids in the SRAT group felt they received emotionalsupport from Nima and they even shared their desires for thefuture with him since he embodied their emotional and socialdevelopment. However, the same result was not observed inthe other group since children usually feel more supportedby their peers than by adults. Our finding is in line withLolanda Leite’s research which was “Long-term interactionswith empathic robots: evaluating perceived support in chil-dren”. Their result also suggested that children felt supportedby the robot as their peer and the robot reinforced the kids’self-esteem [47,48].
Moreover, the hospital staff and the parents claimed thatthey were extremely happy with the results of the SRATgroup and could not believe the level of improvement dur-ing the therapy. However, the integration of a robot in such
Table 8 Table tests ofbetween-subjects effects
Source Dependent variable F Sig. Partial eta squared
GROUP Gained anxiety 19.14 0.002 0.70
Gained depression 8.66 0.019 0.52
Gained anger 10.28 0.012 0.56
123
Author's personal copy

Int J of Soc Robotics
a context was a big challenge due to unpredictable status ofthe young patients.
5 Conclusion
Cancer treatment consists of many invasive and painfulprocedures that are the main sources of distress and dis-contentment for patients. It is important to note that theseprocedures could be psychologically more influential onpediatric patients [9]. Chemotherapy injections, blood draw-ing, and bone-marrow aspirations are some of the mainstressors patients confront repeatedly. In addition, the sideeffects that treatment brings, such as hair loss, lack ofappetite, fatigue, and inability to do many activities exac-erbate this situation. So, it is apparent that seeking a methodwhich could alleviate distress and its debilitating impacts isa necessity.
All the techniques developed for the management of dis-tress, encompassing cognitive distraction, relaxation, andhypnosis have been proved to be advantageous in decreasingthe level of distress symptoms. This study suggests a methodthat can be used independently or with other methods, i.e.as a new technique aimed at the reduction of distress, or asan assistant in techniques such as relaxation, or desensiti-zation to help kids to cooperate more. From a closer view,a humanoid robot can be used as an addition in any othermethod (whether it be behavioral techniques or interven-tion) as a device to increase the efficiency of communication,involve kids’ imaginations in learning, and induce them tobe more responsive, as well as cooperative.
In order to make this novel method more acceptable tohospital authorities or doctors, it is important to make itclear that the robot would be an assistant in the interventionsession, and highlight the irreplaceable role of the psychol-ogist. Another important point is to make sure that all thepersonnel present at the session are trained and examinedin communication with children dealing with cancer, bothin physical (hygiene, paying attention the each kid’s bodycondition, etc.) and mental respects. These points should beobserved in designing the robot’s programs and keeping itshardware tidy, as well. It is evident that families should becomfortable about their kids’ health and safety in the SRATsessions, thereby; it would be advantageous to let the parentstake part in the first sessions (or some trial sessions only forparents) and get feedback from them. One or several intro-ductory meetings could be arranged to familiarize parentswith this new technique. Furthermore, the children’s reac-tions could be monitored by asking their families about theirreaction to the robot at home, after initial sessions.
To conclude, considering the positive reactions from thechildren to a robot assistant present at intervention session,and observing the statistical results, utilizing a humanoid
robot with different communication abilities can be ben-eficial, both in elevation of efficacy in interventions, andfomenting kids to be more interactive. Also, a humanoidrobot was shown to be significantly useful in teaching chil-dren about their afflictions, and also instructing them in themethods (relaxation or any other techniques) to confront theirdistress themselves, and take control of their situation. More-over, the core ethical principles regarding socially assistiverobotics technologies have been taken into account in thisstudy and hopefully we aim at conducting a long-term studyin the near future to work on kids’ appetite to help reducethe rate of death among kids with cancer. However, we facedmany challenges in this study. The promising results of thisstudy could render using social robots in psychological inter-ventions for pediatric cancer, and its implications shall bebeneficial to psychologists, oncologists, and robot special-ists.
5.1 Study Limitations
This study like other researches had some limitations one ofwhich was the small sample size. This was due to a num-ber of reasons. Firstly, having the participants take part in allsessions was not convenient, considering their difficult situ-ation and possible interference with their treatment protocol.Additionally, with respect to the novelty of the project, andthe scant number of systematic psychological interventionsmade in Iranian hospitals, particularly for the patients diag-nosed with cancer or other refractory illnesses, persuadingthe children’s parents to take part in this study was relativelydifficult. Generally, it was hard for parents to bring their kidsto sessions on a regular basis.
Another impeding factor in gathering a middle-sizedgroup was patients’ and their parents’ lack of willingnessto come to the medical centers in their spare time, inas-much as they didn’t like the environment of hospitals, whichbrought back unpleasant memories. This was mostly reportedby some of the older children, around 11–12 years old. Theselimitations continued to exist to a degree, after the start ofsessions, hence, the initial group size was reduced from 10to 6 after 2–3 sessions.
Though not documented or scientifically measured, it wasobserved that parents who were more wary of cancer’s impacton their children’s psychological status, showed more will-ingness to bring their kids to the sessions. This brings theconjecture that parents’ awareness level or educational statuscould have a meaningful influence on their children’s initialdistress level, before the beginning of the study. This supposi-tion could be the reason why no severe depression, anxiety, oranger was observed in the participants’ pre-test results. Manypatients at the hospital had higher distress levels (accordingto psychologists’ reports), yet their parents were not willingto take part in the study. The closeness of this conjecture to
123
Author's personal copy

Int J of Soc Robotics
reality must be precisely investigated, before any conclusionis made.
The researcher who was present at all sessions, as a medi-ator between the kids and the robot, was a certified personin communication with children suffering from cancer. Hehad two years of experience in this field, and was trained bythe psychologists of MAHAK. This not only facilitated thecooperation of the medical centers in this project, but also itwas a strong reason for many parents to trust the project teamwith their kids. Thereby, this might be counted as a limitationin the study, since most of the participants knew the researchteam, before the study began.
Acknowledgments We would like to thank the National Elites Foun-dation of Iran (http://www.bmn.ir) for their moral and financial supportthroughout this project. Furthermore, the cooperation of MAHAK andMARKAZ-e-TEBI-KOODAKAN Hospitals in Tehran during the courseof this research is highly appreciated. We also thank all individuals whohelped us throughout this research specially: Dr. Leyli Koochakzadeh,Dr. Farzad, Anooshe Ghanbarzadeh, Marjan Vosoughi, Kompani, ShadiAnsari, Saeedeh Zorofchi, Elaheh Rahimian, Fatemeh Mirdoraghi.
Appendix
Psychological Questionnaires (Anxiety, Depression, andAnger) used in this study (translated from Persian to Eng-lish).
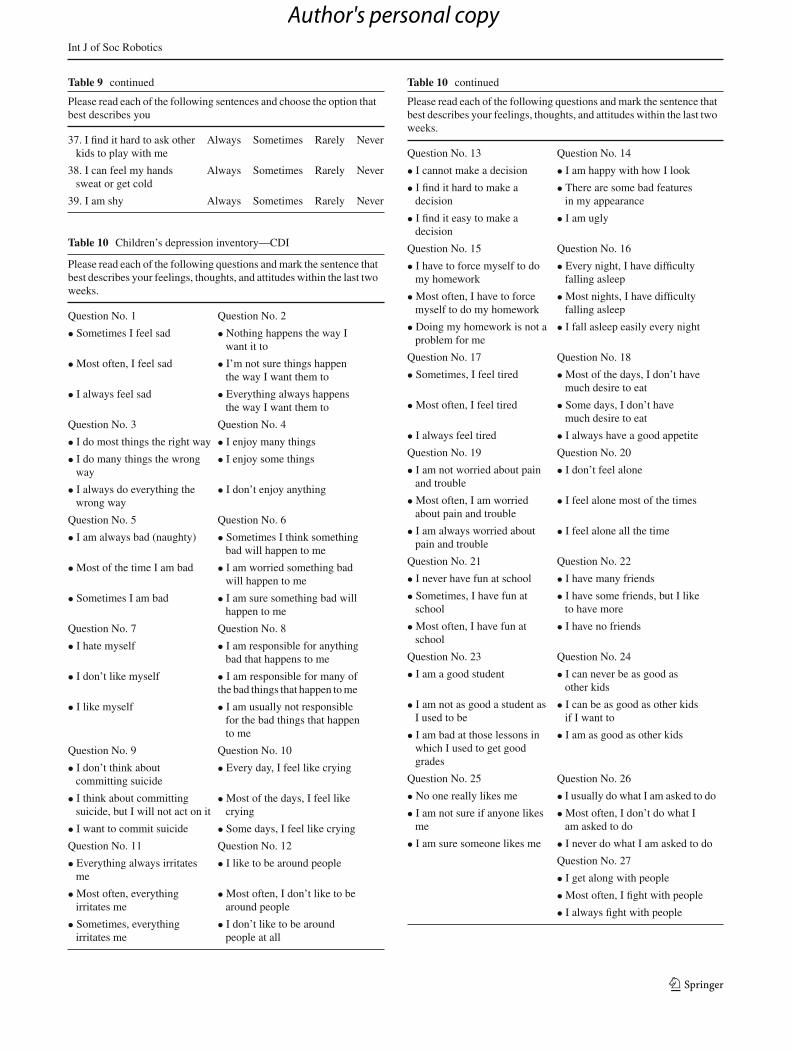
See Tables 9, 10 and 11.
Table 9 Multiple anxiety scale for children—MASC
Please read each of the following sentences and choose the option thatbest describes you
1. I feel worried or upset Always Sometimes Rarely Never
2. I usually ask others forpermission
Always Sometimes Rarely Never
3. I’m worried that I willbe laughed at
Always Sometimes Rarely Never
4. When my parents areaway from me, I feelscared
Always Sometimes Rarely Never
5. I have difficulty inbreathing
Always Sometimes Rarely Never
6. I am always carefulwith dangerous things
Always Sometimes Rarely Never
7. I feel scared when Iimagine going on acamping trip
Always Sometimes Rarely Never
8. I feel scared andanxious
Always Sometimes Rarely Never
9. I try hard to obey myparents and my teachers
Always Sometimes Rarely Never
10. I feel scared that otherkids want to make fun ofme
Always Sometimes Rarely Never
Table 9 continued
Please read each of the following sentences and choose the option thatbest describes you
11. I try to stay close to myparents
Always Sometimes Rarely Never
12. I feel weak and dizzy Always Sometimes Rarely Never
13. First, I carefully checkeverything
Always Sometimes Rarely Never
14. I am worried that myname will be called in theclass
Always Sometimes Rarely Never
15. I am very active Always Sometimes Rarely Never
16. I am scared that othersfind me stupid
Always Sometimes Rarely Never
17. I keep a light on at night Always Sometimes Rarely Never
18. I feel pain in my chest Always Sometimes Rarely Never
19. I avoid going outwithout my familymembers
Always Sometimes Rarely Never
20. I feel strange, weird,and unreal
Always Sometimes Rarely Never
21. I try to do what otherslike me to do
Always Sometimes Rarely Never
22. I am worried about theway people think aboutme
Always Sometimes Rarely Never
23. I avoid watching horrormovies or TV programs
Always Sometimes Rarely Never
24. My heart beats fast Always Sometimes Rarely Never
25. I avoid things that makeme sad
Always Sometimes Rarely Never
26. I sleep with one of myfamily members
Always Sometimes Rarely Never
27. I feel restless andanxious
Always Sometimes Rarely Never
28. I try to do everythingperfectly
Always Sometimes Rarely Never
29. I am worried that I willdo stupid or embarrassingthings
Always Sometimes Rarely Never
30. I am scared of gettinginto a car or a bus
Always Sometimes Rarely Never
31. I feel nausea Always Sometimes Rarely Never
32. When I feel sad orscared, I inform someoneimmediately
Always Sometimes Rarely Never
33. I feel overwhelmedwhen I have to do thingsin front of people
Always Sometimes Rarely Never
34. I’m afraid of badweather, the dark, heights,animals, and insects
Always Sometimes Rarely Never
35. My hands shake Always Sometimes Rarely Never
36. I carefully checkeverything to make sureit’s totally safe
Always Sometimes Rarely Never
123
Author's personal copy
Int J of Soc Robotics
Table 9 continued
Please read each of the following sentences and choose the option thatbest describes you
37. I find it hard to ask otherkids to play with me
Always Sometimes Rarely Never
38. I can feel my handssweat or get cold
Always Sometimes Rarely Never
39. I am shy Always Sometimes Rarely Never
Table 10 Children’s depression inventory—CDI
Please read each of the following questions and mark the sentence thatbest describes your feelings, thoughts, and attitudes within the last twoweeks.
Question No. 1 Question No. 2
• Sometimes I feel sad • Nothing happens the way Iwant it to
• Most often, I feel sad • I’m not sure things happenthe way I want them to
• I always feel sad • Everything always happensthe way I want them to
Question No. 3 Question No. 4
• I do most things the right way • I enjoy many things
• I do many things the wrongway
• I enjoy some things
• I always do everything thewrong way
• I don’t enjoy anything
Question No. 5 Question No. 6
• I am always bad (naughty) • Sometimes I think somethingbad will happen to me
• Most of the time I am bad • I am worried something badwill happen to me
• Sometimes I am bad • I am sure something bad willhappen to me
Question No. 7 Question No. 8
• I hate myself • I am responsible for anythingbad that happens to me
• I don’t like myself • I am responsible for many ofthe bad things that happen to me
• I like myself • I am usually not responsiblefor the bad things that happento me
Question No. 9 Question No. 10
• I don’t think aboutcommitting suicide
• Every day, I feel like crying
• I think about committingsuicide, but I will not act on it
• Most of the days, I feel likecrying
• I want to commit suicide • Some days, I feel like crying
Question No. 11 Question No. 12
• Everything always irritatesme
• I like to be around people
• Most often, everythingirritates me
• Most often, I don’t like to bearound people
• Sometimes, everythingirritates me
• I don’t like to be aroundpeople at all
Table 10 continued
Please read each of the following questions and mark the sentence thatbest describes your feelings, thoughts, and attitudes within the last twoweeks.
Question No. 13 Question No. 14
• I cannot make a decision • I am happy with how I look
• I find it hard to make adecision
• There are some bad featuresin my appearance
• I find it easy to make adecision
• I am ugly
Question No. 15 Question No. 16
• I have to force myself to domy homework
• Every night, I have difficultyfalling asleep
• Most often, I have to forcemyself to do my homework
• Most nights, I have difficultyfalling asleep
• Doing my homework is not aproblem for me
• I fall asleep easily every night
Question No. 17 Question No. 18
• Sometimes, I feel tired • Most of the days, I don’t havemuch desire to eat
• Most often, I feel tired • Some days, I don’t havemuch desire to eat
• I always feel tired • I always have a good appetite
Question No. 19 Question No. 20
• I am not worried about painand trouble
• I don’t feel alone
• Most often, I am worriedabout pain and trouble
• I feel alone most of the times
• I am always worried aboutpain and trouble
• I feel alone all the time
Question No. 21 Question No. 22
• I never have fun at school • I have many friends
• Sometimes, I have fun atschool
• I have some friends, but I liketo have more
• Most often, I have fun atschool
• I have no friends
Question No. 23 Question No. 24
• I am a good student • I can never be as good asother kids
• I am not as good a student asI used to be
• I can be as good as other kidsif I want to
• I am bad at those lessons inwhich I used to get goodgrades
• I am as good as other kids
Question No. 25 Question No. 26
• No one really likes me • I usually do what I am asked to do
• I am not sure if anyone likesme
• Most often, I don’t do what Iam asked to do
• I am sure someone likes me • I never do what I am asked to do
Question No. 27
• I get along with people
• Most often, I fight with people
• I always fight with people
123
Author's personal copy

Int J of Soc Robotics
Table 11 Children’s inventory of anger—CIA
Children's Inventory of Anger
1 I don't
care
2 That
bothers me.
3 I'm really
mad (angry)
4 I can't stand that
1 Your mother calls you to dinner in the middle of your favorite TV show.
2 Your bike has a flat �re.3 Your brother or sister or friend ignores you.4 You clean up your room and want to go out to
play. Your mom says you have to clean some more.
5 You have to do a job that your brother or sister was supposed to do.
6 You want to go somewhere with a friend. Your dad says “No” for no reason.
7 The teacher’s pet gets to do all the fun jobs in class.
8 In a game, someone on the other side tries to cheat.
9 Someone bumps your desk on purpose and you mess up your work.
10 You are playing a game and someone on the other side tries to punch you.
11 Someone spits at you.12 You get a piece of pie at lunch and someone
knocks it out of your hand.13 Somebody calls you a “chicken”.14 You want to show someone a new trick on your
bike and you can't do it.15 You put all your change in the soda machine. It
takes your money but you don’t get a drink.16 A teacher gives you a lot of homework on the
weekend.17 Someone says that you are not old enough to do
something.18 Someone turns the TV to another channel when
you are watching a show.19 You want something from your brother or sister
and they refuse to give it to you.20 Your friends are playing a game and they won’t
let you play.21 Somebody says “I told you so” a�er something
goes wrong.22 Your mom or dad slaps you.23 Someone puts gum on your seat on the bus and
you sit on it. 24 You bump into a stranger on the bus. He says he
will beat you up if you get near him again.
123
Author's personal copy

Int J of Soc Robotics
Table 11 continued
25 Someone cuts in front of you in line.26 You brought your favorite candy bar in your
lunch. When you go to eat It, it’s melted.27 Your mom won’t buy your favorite cereal.28 On your bike, you come to a steep hill. You have
to get off the bike and walk it all the way up the hill.
29 Your mom says she does not want you to play with one of your friends.
30 Your dad yells at you in front of other people.31 You don’t have any homework but your mom
makes you study anyway.32 You do something special for a friend and he or
she won't do anything for you.33 Your friends pick you last to be on a team.34 Your friend gets what he or she wants for New
Year, but you don't. 35 Two bigger kids came and take your basketball
and play, “Keep Away” with it.36 Somebody punches you.37 Someone tries to trip you on purpose.
38 You have to do your homework and your brother or sister gets to watch TV.
39 You have to go to bed at 9:30 and your friends get to stay up un�l 10:30 or 11:00.
References
1. March JS, Parker JDA, Sullivan K, Stallings P (1997) The multi-dimensional anxiety scale for children (MASC): factor structure,reliability, and validity. J Am Acad Child Adolesc Psychiatry36:554–565
2. Nelson WM, Finch AJ (2000) Children’s inventory of anger. West-ern Psychological Services, Los Angeles
3. Kovacs M (1985) The children’s depression inventory (CDI). Psy-chopharmacol Bull 21:995–1124
4. Holland JC, Alici Y (2010) Management of distress in cancerpatients. J Support Oncol 8:4–12
5. The National Comprehensive Cancer Network (2009) Dis-tress management clinical practice guidelines in oncology, ver-sion 1. www.nccn.org/professionals/physician_gls/f_guidelines.asp#supportive
6. Kuppenheimer WG, Brown RT (2002) Painful procedures in pedi-atric cancer: a comparison of interventions. Clin Psychol Rev22(5):753–786
7. Beale IL (2006) Scholarly literature review: efficacy of psycholog-ical interventions for pediatric chronic illnesses. J Pediatr Psychol31(5):437–451
8. Richardson J, Smith JE, Pilkington K (2006) Hypnosis forprocedure-related pain and distress in pediatric cancer patients:a systematic review of effectiveness and methodology related tohypnosis interventions. J Pain Symptom Manag 31(1):70–84
9. Butler LD, Symons BK, Henderson SL, Shortliffe LD, SpiegelD (2005) Hypnosis reduces distress and duration of an invasivemedical procedure for children. Pediatrics 115:77–85
10. Syrjal KL, Donaldson GW, Davis MW, Kippes ME, Carr JE(1995) Relaxation and imagery and cognitive-behavioral trainingreduce pain during cancer treatment: a controlled clinical trial. Pain63(2):189–198
11. Spiegel D, Moore R (1997) Imagery and hypnosis in the treatmentof cancer patients. Oncology (Williston Park) 11(8):1179–1189
12. Smith JE, Mccall G, Richardson A, Pilkington K, Kirsch I (2006)Hypnosis for procedure-related pain and distress in pediatric cancerpatients: a systematic review of effectiveness and methodologyrelated to hypnosis interventions. J PainSymptom Manag 31(1):70–84
13. Kleibe C, Harper DC (1999) Effects of distraction on children’spain and distress during medical procedures: a meta-analysis. NursRes 48(1):44–49
14. Dalton JA, Keefe FJ, Carlson J, Youngblood R (2004) Tailoringcognitive-behavioral treatment for cancer pain. Pain Manag Nurs5(1):3–18
15. Gielissen MF, Verhagen S, Witjes F, Bleijenberg G (2006) Effectsof cognitive behavior therapy in severely fatigued disease-free can-cer patients compared with patients waiting for cognitive behaviortherapy: a randomized controlled trial. J Clin Oncol 24(30):4882–4887
16. Strong V, Waters R, Hibberd C, Murray G, Wall L, Walker L,McHugh G, Walker A, Sharpe M (2008) Management of depressionfor people with cancer (SMaRT oncology 1): a randomised trial.Lancet 372:40–48
17. Hopko DR, Bell JL, Armento M, Robertson S, Mullane C, WolfN, Lejuez CW (2008) Cognitive-behavior therapy for depressed
123
Author's personal copy

Int J of Soc Robotics
cancer patients in a medical care setting. J Behav Ther 39(2):126–136
18. Jacobsen PB, Jim HS (2008) Psychosocial interventions for anxietyand depression in adult cancer patients: achievements and chal-lenges. CA Cancer J Clin 58:214–230
19. Classen C, Butler LD, Koopman C, Miller E, DiMiceli S, Giese-Davis J, Fobair P, Carlson RW, Kraemer HC, Spiegel D (2001)Supportive-expressive group therapy and distress in patients withmetastatic breast cancer: a randomized clinical intervention trial.Arch Gen Psychiatry 58(5):494–501
20. Kissane DW, Bloch S, Smith GC, Miach P, Clarke DM, Ikin J, LoveA, Ranieri N, McKenzie D (2003) Cognitive-existential group psy-chotherapy for women with primary breast cancer: a randomisedcontrolled trial. Psycho-oncology 12(6):532–546
21. Kissane DW, Love A, Hatton A, Bloch S, Smith G, Clarke DM,Miach P, Ikin J, Ranieri N, Snyder RD (2004) Effect of cognitive-existential group therapy on survival in early-stage breast cancer.J Clin Oncol 22(21):4255–4260
22. Goodwin PJ, Leszcz M, Ennis M, Koopmans J, Vincent L, GutherH, Drysdale E, Hundleby M, Chochinov HM, Navarro M, SpecaM (2001) The effect of group psychosocial support on survival inmetastatic breast cancer. N Engl J Med 345(24):1719–1726
23. Boesen EH, Johansen C (2008) Impact of psychotherapy on cancersurvival: time to move on? Curr Opin Oncol 20(4):372–377
24. Redd WH, Montgomery GH, DuHamel KN (2001) Behavioralintervention for cancer treatment side effects. J Natl Cancer Inst93(11):810–823
25. Figueroa-Moseley C, Jean-Pierre P, Roscoe JA, Ryan JL, KohliS, Palesh OG, Ryan EP, Carroll J, Morrow GR (2007) Behavioralinterventions in treating anticipatory nausea and vomiting. J NatlCompr Cancer Netw 5(1):44–50
26. Lotfi-Jam K, Carey M, Jefford M, Schofield P, Charleson C,Aranda S (2008) Nonpharmacologic strategies for managing com-mon chemotherapy adverse effects: a systematic review. J ClinOncol 26(34):5618–5629
27. Gershon J, Zimand E, Lemos R, Rothbaum BO, Hodges L (2003)Use of virtual reality as a distracter for painful procedures in apatient with pediatric cancer: a case study. Cyber Psychol Behav6(6):657–661
28. Windich-Biermeier A, Sjoberg I, Dale JC, Eshelman D, GuzzettaCE (2007) Effects of distraction on pain, fear, and distress duringvenous port access and venipuncture in children and adolescentswith cancer. J Pediatr Oncol Nurs 24(1):8–19
29. Liossi C, Hatira P (1999) Clinical hypnosis versus cognitivebehavioral training for pain management with pediatric cancerpatients undergoing bone marrow aspirations. Int J Clin Exp Hypn47(2):104–116
30. Shockey DP, Menzies V, Glick DF, Taylor AG, Boitnott A, RovnyakV (2013) Preprocedural distress in children with cancer: an inter-vention using biofeedback and relaxation. J Pediatr Oncol Nurs30(3):129–138
31. Landier W, Tse AM (2010) Use of complementary and alternativemedical interventions for the management of procedure-relatedpain, anxiety, and distress in pediatric oncology: an integrativereview. J Pediatr Nurs 25(6):566–579
32. Meghdari A, Alemi M, Ghazisaedy M, Taheri AR, Karimian A,Zandvakili M (2013) Applying robots as teaching assistant inEFL classes at Iranian middle-schools, CD. In: Proc. of the int.conf. on education and modern educational technologies, Venice,Italy
33. Alemi M, Meghdari A, Ghazisaedy M (2014) Employing humanoidrobots for teaching english language in Iranian junior high-schools.Int J Humanoid Rob 11(3):1–25
34. Baroni I, Nalin M, Zelati MC, Oleari E, Sanna A (2014) Designingmotivational robot: how robots might motivate children to eat fruitsand vegetables. In: The 23rd IEEE international symposium on
robot and human interactive communication (RoMAN 2014), pp796–801
35. Taheri AR, Alemi M, Meghdari A, Pouretemad HR, HolderreadSL (2014) Clinical application of a humanoid robot in playingimitation games for autistic children in Iran. In: Proc. of the 14thint. educational technology conference (IETC), Chicago, USA
36. Robins B, Dautenhahn K, Dubowski J (2006) Does appearancematter in the interaction of children with autism with a humanoidrobot? Interact Stud 7(3):509–542
37. Scassellati B, Admoni H, Matari M (2012) Robots for use in autismresearch. Annu Rev Biomed Eng 14:275–294
38. Belpaeme T et al. (2013) Child-robot interaction: perspectives andchallenges. In: Social robotics, LNCS 8239. Springer InternationalPublishing, pp. 452–459
39. Meghdari A, Alemi M, Taheri AR (2013) The effects of usinghumanoid robots for treatment of individuals with autism in Iran,6th Neuropsychology Symp., Tehran, Iran
40. Alemi M, Daftarifard P, Pashmforoosh R (2011) The impact of lan-guage anxiety and language proficiency on WTC in EFL context.Cross Cult Commun J 7(3):150–166
41. ALIZ-E project. http://fostsvn.uopnet.plymouth.ac.uk/index.php42. Baroni I, Nalin M, Baxter P, Pozzi C, Oleari E, Sanna A et al. (2014)
What a robotic companion could do for a diabetic child. In: 23rdIEEE int. conf. on robot and human interactive communication(RoMAN 2014)
43. Chorpita BF, Moffitt CE, Gray J (2005) Psychometric properties ofthe revised child anxiety and depression scale in a clinical sample.Behav ResTher 43:309–322
44. Mashhadi A, Mirdoraghi F, Bahrami B, Soltani Shal R (2012)Effect of demographic variables on children anxiety. Iran J Psy-chiatry 7:3
45. Zibaei A, Gholami H, Zare M, Mahdian H, Yavari M, HaresabadiM (2013) The effect of offline education on anger management inguidance school girls in Mashhad. J North Khorasan Univ Med Sci5(2):385
46. Lajevardi P. http://www.mahak-charity.org/main/fa/about-mahak2/593 (in Persian)
47. Leite I, Castellano G, Pereira A, Martinho C, Paiva A (2012)Long-term interactions with empathic robots: evaluating perceivedsupport in children. In: Proc. of int. conf. on social robotics.Chengdu, China, pp. 298–307
48. Alemi M, Meghdari A, Ghazisaedy M (2015) The impact of socialrobotics on L2 learners’ anxiety and attitude in english vocabularyacquisition. Int J Soc Robot. doi:10.1007/s12369-015-0286-y
Minoo Alemi received her Ph.D. in Applied Linguistics from AllamehTabataba’i University (Iran) in 2011. In 2012, with the support ofNational Elites Foundation of Iran, she joined the Social Robotics Labo-ratory of the Center of Excellence in Design, Robotics, and Automation(CEDRA) of the Sharif University of Technology as a Post-DoctoralResearch Associate. During her tenure at CEDRA, she creativelyapplied game-based education with robotics and engineering studentsin social robotics projects such as: Robot Assisted Language Learning(RALL) and Humanoid Robot Assistants in Autism and Cancer Thera-pies. Since January 2015, she joined the Department of Humanities atthe Islamic Azad University-Tehran West Branch as an Assistant Pro-fessor. Thus far she has been the author of over 70 papers and books.
Ashkan Ghanbarzadeh received his B.Sc. in Mechanical Engineeringfrom Sharif University of Technology (Iran) in June 2014. His areas ofinterest are Robotics and Clinical Applications of Social Robots. He iscurrently a M.Sc. student of mechanical engineering at the NortheasternUniversity in Boston, USA.
123
Author's personal copy

Int J of Soc Robotics
Ali Meghdari received his Ph.D. in Mechanical Engineering andRobotics from the University of New Mexico in 1987, and then as aPost-Doctoral research fellow, he spent a year at the robotics groupof the Los Alamos National Laboratory. Dr. Meghdari’s research hasbeen in various areas of robotics systems. He has been the recipientof a number of scholarships and awards, the latest being the 2012Allameh Tabataba’i Distinguished Professorship Award for Excellencein Teaching and Research by the National Elites Foundation of Iran. Heis a Fellow of the American Society of Mechanical Engineers (ASME)since 2001. With over 230 publications, he is on the editorial board
of various engineering journals and an affiliate member of the IranianAcademy of Sciences (IAS). He is currently Professor and Director ofthe Center of Excellence in Design, Robotics and Automation (CEDRA)at Sharif University of Technology.
Leila Jafari Moghadam received her M.A in Clinical Psychology fromIslamic Azad University, and is currently practicing as a psychologistat the Mahak Hospital and Rehabilitation Complex in Tehran, Iran.
123
Author's personal copy