cl073 - la rate oscillante chez l’enfant : étude multicentrique
TRANSCRIPT

www.elsevier.com/locate/jpedsurg
Journal of Pediatric Surgery (2010) 45, 1519–1524
Wandering spleen in children: multicenterretrospective studyCaroline Fiquet-Francois a,⁎, Mohamed Belouadah a, Hugues Ludot b, Benoit Defauwc,Jiad Noel Mcheik d, Jean Paul Bonnet e,f, Charly Udozen Kanmegneg,Dominique Weil h, Lionel Coupry h, Benjamin Fremont i, Francois Becmeur j,Isabelle Lacreuse j, Philippe Montupet k, Éliane Rahal k, Nathalie Botto l,Alaa Cheikhelard l, Sabine Sarnacki l, Thierry Petitm, Marie Laurence Poli Merol a
aPediatric Surgery Department, American Memorial Hospital, Centre Hospitalier Universitaire, 51092 Reims FrancebDepartment of Pediatric Anesthesia, American Memorial Hospital, Centre Hospitalier Universitaire, 51092 Reims, FrancecPediatric Surgery Department, Centre Hospitalier, 26000 Valence, FrancedPediatric Surgery Department, Hôpital J.Bernard, CHU, 86021 Poitiers, FranceePediatric Surgery Department, Hôpital Debrousse, 69322 Lyon cedx 05 Lyon, FrancefPediatric Surgery Department, Centre Hospitalier, 95160 Montmorency, FrancegDepartment of Radiology, Centre Hospitalier Simone Veil, 95160 Montmorency, FrancehPediatric Surgery Department, Centre Hospitalier Universitaire, 49033 Angers, FranceiPediatric Surgery Department, Hôpital Pontchailou, 35033 Rennes, FrancejPediatric Surgery Department, Hôpital Universitaire de Hautepierre, 67098 Starsbourg, FrancekPediatric Surgery Department, 94275 Le Kremlin-Bicêtre Paris, Bicetre, FrancelPediatric Surgery Department, Hôpital Necker Enfants-Malades, Université Paris Descartes, 75015 Paris, FrancemPediatric Surgery Department, Centre Hospitalier Universitaire, Avenue de la côte de Nacre, 14033 Caen, France
Received 23 August 2009; revised 7 March 2010; accepted 7 March 2010
0d
Key words:Wandering spleen;Splenopexy;Gastropexy;Splenectomy;Laparoscopy;Children
Abstract Wandering spleen in children is a rare condition. The diagnosis is difficult, and any delay cancause splenic ischemia. An epidemiologic, semiological, and surgical diagnosis questionnaire onincidence of wandering spleen in children was sent to several French surgical teams. We report theresults of this multicenter retrospective study.Fourteen cases (6 girls, 8 boys) were reported between 1984 and 2009; the age range varies between1-day-old and 15 years; 86% were seen in the emergency department. Ninety-three percent had diffuseabdominal pain. For 57% of the cases, it was their first symptomatic episode of this type. Nodiagnosis was established based on the clinical results alone. All patients had presurgical imagingdiagnosis. Open surgery was performed on 64% cases. Forty-three had splenectomy for splenicischemia. Thirty-six percent had splenopexy, 14% had laparoscopic gastropexy, and 7% had spleenrepositioning and regeneration. Complications were noted in 60% of the cases resulting inpostsplenopexy splenic ischemia.
⁎ Corresponding author. Pediatric Surgery, Service de Chirurgie Pédiatrique, American Memorial Hospital, 51092 Reims, France.E-mail address: [email protected] (C. Fiquet-Francois).
022-3468/$ – see front matter © 2010 Elsevier Inc. All rights reserved.oi:10.1016/j.jpedsurg.2010.03.003

1520 C. Fiquet-Francois et al.
Early diagnosis and surgery are the best guarantee for spleen preservation. Even if the choice of onetechnique, splenopexy or gastropexy, can be argued, gastropexy has the advantage of avoiding splenicmanipulation and restoring proper physiologic anatomy. When there is no history of abdominalsurgery, laparoscopy surgery seems the best procedure.© 2010 Elsevier Inc. All rights reserved.
Wandering spleen is a rare condition characterized by theabsence or underdevelopment of one or all of the ligamentsthat hold the spleen in its normal position in the left upperquadrant of the abdomen. In the literature, we find isolatedcase reports but rarely studies on larger populations [1-6].
A thorough clinical examination will not yield a precisediagnosis because the symptoms are not specific enough.Abdominal sonogram is the imaging examination of choicefor establishing a precise diagnosis.
Surgery is the appropriate therapeutic management, butmany different approaches are available: laparoscopic surgery,laparotomy, splenopexy, gastropexy, and splenectomy…
The aim of this study was to focus on this rare conditionon several levels as follows: epidemiologic and semiolog-ical diagnoses and also the various surgical proceduresavailable. We report the results from a national multicenterpediatrics study, and we confront them to the availableliterature on this topic.
1. Material and method
A questionnaire was sent by e-mail to French pediatricsurgical teams.
The retrospective study based on the patients' medicalcharts focused on the following items:
age, sex, and medical history;- the circumstances around the discovery of the pathologiccondition and clinical information;
- additional diagnostic imaging;- surgical care: surgical indications, choice of the surgicalapproaches, and technical details;
Fig. 1 Number of cases per city.
- postoperative care and potential complications; and- follow-up and monitoring of the patients.
2. Results
Fourteen centers answered the questionnaire and reportedbetween 1 and 3 cases. Four centers never encountered thispathologic condition (Fig 1).
A total of 14 cases of congenital wandering spleen werereported between 1984 and 2009.
2.1. Epidemiology
Regarding the congenital wandering spleens, 6 girls and8 boys presented this condition. The mean age at the time ofdiagnosis for the congenital condition is 7 years (minimum, 1day; maximum, 15 years). It is essential to underline that theyounger case of the series is neonatal. The diagnosis was notestablished during the prenatal period, and this little boypresented a torsion requiring emergency surgery at day 1 afterhis birth.
All are unique cases in their families; none of theirsiblings are affected by this condition.
Regarding the medical and surgical history, 4 patients hadsignificant medical history as follows: 2 diaphragmatic hernias(1 discovered during the clinical checkup), 1 omphalocele, 1interauricular communication, and 1 gastroesophageal refluxdisease treated by laparoscopic Nissen fundoplication.
2.2. Semiology
We will only focus on the congenital conditions for theremaining of the results. Of the patients, 93% (13/14)presented objective abdominal pain. For the 1-day-oldpatient, these data could not be validated. This symptomwas the main reason for consulting (Table 1).
Three patients had already been hospitalized in the surgicalunit for the same symptoms: 1 was hospitalized twice for 3similar episodes in the past 6 months because of diffuseabdominal pain evolving crescendo, lethargy, abdominaldistension, and vomiting. Because the symptoms had dis-appeared after nasogastric tube decompression and bed rest, nofurther investigations were performed. The differential diagno-sis included small bowel intussusceptions, incomplete volvu-lus, and abdominal distension. Another patientwas hospitalizedand ended up having an appendectomy.

Table 1 Initial clinical presentation
Clinical presentation No. of cases
First symptomatic episode 7/13Emergency context 11/13Pain 13/14Pain location Diffuse 4/14, periumbilical 2/14,
left side 2/14, pelvis 1/14,left hypochondrium 1/14,data not available 4/14
Intense pain 7/13Vomiting 7/13Acute intestinal obstruction 3/14Hemorrhagic shock 1/14Hyperthermia, 39°C 1/14Hypotonic/breathingdifficulties
1/14
Fig. 3 Magnetic resonance imaging abdominal frontal view.Gadolinium injection: long pedicle, vascularized spleen.
1521Wandering spleen
None of the diagnoses of wandering spleen were based onclinical evidence only.
2.3. Additional imaging examinations
Of 14 patients, 13 had clinical imaging checkups; adiagnosis was established based on these results in 13 of 13cases. Four patients of 14 had a unique radiographic imaging.
An abdominal Doppler sonogram is the most commonadditional imaging examination prescribed (9 cases). Com-puted tomographic (CT) scan was the second mostprescribed imaging examination (8 cases). Splenic scintig-raphy was only proposed in one case.
These examinations showed the following.
- The absence of spleen in its normal position.- The presence of a «mass» (spleen) in the left iliacfossa in most cases or, in one case, at the level of the
Fig. 2 Magnetic resonance imaging abdominal frontal view. Spleenin a low position below the stomach, long pedicle, good vascularization.
right hypochondrium. The spleen was often describedas voluminous.
- In case of ischemia, inadequate vascular supply ortight circumvolutions.
Plain abdomen radiography led to simple and quickdiagnoses of 2 cases of gastric volvulus and 1 diaphragmatichernia.
Magnetic resonance imaging was only proposed in onecase outside an emergency context. This examination founda hypertrophic spleen with a long splenic pedicle (Figs. 2and 3).
2.4. Therapeutic care
Open surgery was performed on 9 patients (64%). Opensurgery was chosen for different reasons as follows:
- insufficient experience with laparoscopic surgery and rarepathology (1 case),
- history of abdominal surgery (3 cases),- cecocolic distension (1 case),- splenic hypertrophy (1 case),- combined surgery of a gastric volvulus and diaphragmatichernia, and
- patient's age, that is, 1-day-old patient with clinicalbreathing difficulties.
1522 C. Fiquet-Francois et al.
Laparoscopic-assisted surgery was suggested in 5 cases(36%). A 10-mm 0° laparoscope was inserted through theumbilical port. The number of trocars varied between 3 and5. For types of surgical techniques, 6 patients had anischemic spleen (43%), leading to 6 splenectomy procedures.
Splenopexies were performed on 5 patients as follows:
- 3 cases were by Vicryl mesh: 2 cases fixed to theabdominal wall and 1 case sutured to the diaphragm;
- 1 case was by peritoneal capsule sutured and wrappedwith the omentum; and
- in 1 case, the approach was not described.
The gastropexy performed in 2 patients consisted ofmoving the spleen freely from its abnormal location (left iliacfossa) to its normal one (subdiaphragmatic). We performed aparietal peritoneal posterolateral incision, opposite the largegastric curve, up to the diaphragm (7 cm). We created anextraperitoneal pocket and proceeded with the gastropexy;we fixed the anterior stomach lining with sutures (Mersuture3/0; Johnson and Johnson, Somerville, NJ) on the freeanterior peritoneum.
In one case (neonatal patient), the spleen was repositionedin its proper location with a simple regeneration of theperitoneal wall without splenopexy.
For all 14 patients, no complications were reportedduring surgery.
The mean postoperative follow-up is 1.5 years (medianat 1 year) with a minimum at 2 months and maximum at5 years.
No postoperative clinical symptoms were reported.The follow-up was always a clinical one; imaging
examinations were used for monitoring patients who didnot have a splenectomy.
For postoperative additional imaging examinations, of the8 patients with initial spleen preservation, 6 had an
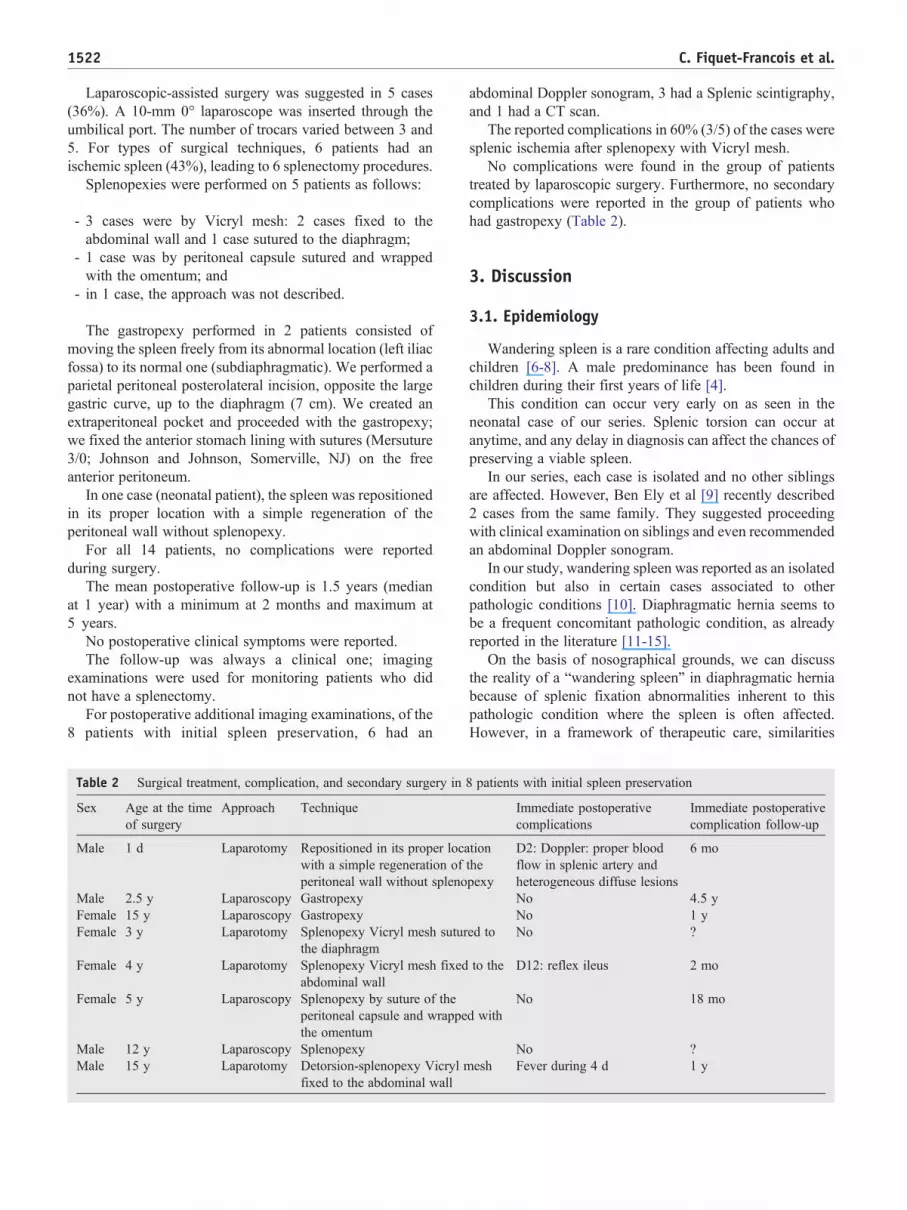
Table 2 Surgical treatment, complication, and secondary surgery in
Sex Age at the timeof surgery
Approach Technique
Male 1 d Laparotomy Repositioned in its proper locawith a simple regeneration ofperitoneal wall without spleno
Male 2.5 y Laparoscopy GastropexyFemale 15 y Laparoscopy GastropexyFemale 3 y Laparotomy Splenopexy Vicryl mesh sutur
the diaphragmFemale 4 y Laparotomy Splenopexy Vicryl mesh fixed
abdominal wallFemale 5 y Laparoscopy Splenopexy by suture of the
peritoneal capsule and wrappethe omentum
Male 12 y Laparoscopy SplenopexyMale 15 y Laparotomy Detorsion-splenopexy Vicryl m
fixed to the abdominal wall
abdominal Doppler sonogram, 3 had a Splenic scintigraphy,and 1 had a CT scan.
The reported complications in 60% (3/5) of the cases weresplenic ischemia after splenopexy with Vicryl mesh.
No complications were found in the group of patientstreated by laparoscopic surgery. Furthermore, no secondarycomplications were reported in the group of patients whohad gastropexy (Table 2).
3. Discussion
3.1. Epidemiology
Wandering spleen is a rare condition affecting adults andchildren [6-8]. A male predominance has been found inchildren during their first years of life [4].
This condition can occur very early on as seen in theneonatal case of our series. Splenic torsion can occur atanytime, and any delay in diagnosis can affect the chances ofpreserving a viable spleen.
In our series, each case is isolated and no other siblingsare affected. However, Ben Ely et al [9] recently described2 cases from the same family. They suggested proceedingwith clinical examination on siblings and even recommendedan abdominal Doppler sonogram.
In our study, wandering spleen was reported as an isolatedcondition but also in certain cases associated to otherpathologic conditions [10]. Diaphragmatic hernia seems tobe a frequent concomitant pathologic condition, as alreadyreported in the literature [11-15].
On the basis of nosographical grounds, we can discussthe reality of a “wandering spleen” in diaphragmatic herniabecause of splenic fixation abnormalities inherent to thispathologic condition where the spleen is often affected.However, in a framework of therapeutic care, similarities
8 patients with initial spleen preservation
Immediate postoperativecomplications
Immediate postoperativecomplication follow-up
tionthepexy
D2: Doppler: proper bloodflow in splenic artery andheterogeneous diffuse lesions
6 mo
No 4.5 yNo 1 y
ed to No ?
to the D12: reflex ileus 2 mo
d withNo 18 mo
No ?esh Fever during 4 d 1 y
1523Wandering spleen
with wandering spleen must be looked for. We believe thatfor patients who had surgery for diaphragmatic hernia withassociated abdominal pain, splenic torsion has to be evokedand an abdominal sonogram must be done to identify theexact location of the spleen and the length of its pedicle.Furthermore, if splenic torsion is suspected on a so-calledwandering spleen with a long pedicle, we will suggest thesame therapeutic care than for isolated congenital wander-ing spleen. In our opinion, we have to consider all patientswith diaphragmatic hernia as potential candidates forwandering spleen, but a therapeutic option will only besuggested in case of painful complications.
3.2. Clinical
In our series, we have noticed 2 distinct clinical pictures.
(1) The acute clinical picture.
On one hand, a splenic torsion is the main complication ofthis congenital abnormality because it can quickly lead toirreversible splenic ischemia. In our series, 6 patients (43%)had splenectomy for ischemia, but the torsion can complicateup to 65% of pediatrics cases [16].
On the other hand is a gastric volvulus (±associated tosplenic torsion) [1,17-20]. Gastric volvulus associated towandering spleen is a rare condition, and its quick clinicalimprovement with a simple medical treatment often delaysthe diagnosis and proper surgical care [1].
The combination of wandering spleen and gastricvolvulus in children should be explored and requires aquick and adapted therapeutic care.
(2) The more insidious chronic clinical picture.
Forty-three percent of patients treated for wanderingspleen already presented similar symptoms. This prevalencerate is close to the one published by Brown (39%) [4].
This fact underlines the difficulty of establishing a properdiagnosis when faced with an atypical clinical picture. In ourstudy, a patient was hospitalized 3 times for the samesymptoms, another one even had an appendectomy [6].
3.3. Additional imaging examinations
Abdominal Doppler sonogram was not always performedin our series, it is unfortunate as it can validate the diagnosiswithout the use of radiation. Abdominal Doppler sonogramis the imaging examination of choice for the diagnosis ofwandering spleens [4,5,21].
A CT scan was sometimes performed after a sonogram. Itobviously was not relevant for our study because thediagnosis was already established with the Doppler sono-gram. The CT scan should remain a last-resort examinationin children because of radiation exposure [22-24].
In the series, older children with chronic pain had anabdominal magnetic resonance imaging (not requiringanesthesia), which answered our questions and allowed usto establish a proper diagnosis. This imaging examinationseems to be a good alternative to CT scan [25]. However,because it is not available in all clinical settings, it can limitits indications. It can also be recommended for uncompli-cated chronic types.
Dynamic sonogram (on the side, standing up) was usedonce in our series and is a simple examination that can helpdefine the splenic ptosis and be relevant for chronic and hard-to-identify cases. It is also a good follow-up and monitoringimaging examination.
Plain abdomen radiography is still useful as a first-lineimaging examination. It allows for a quick diagnosis ofgastric volvulus as seen in 2 cases in our study. Aftervalidation of the gastric volvulus and gastric decompressionby the nasogastric tube, the Doppler sonogram can beperformed to confirm the diagnosis of wandering spleen.
3.4. Surgery
Even if in our series we were only faced with preoperativediagnoses in the literature, we found that this diagnosis canoccur during surgery in up to 49% of cases [4]. In thiscontext, laparoscopic surgery is the procedure of choice. Itallows for an etiologic diagnosis, a good evaluation of thesurgical situation, and offers several therapeutic possibilities:splenectomy, splenopexy [26-29], or gastropexy [1]. Itsindication is valid for adults and children alike. For ourreported cases, laparotomy was chosen for patients with ahistory of abdominal surgery.
Regarding the surgical approach, nowadays, it iscommonly accepted to try and preserve the spleen, whenviable, during the procedure, to avoid postsplenectomyinfectious complications.
In our series, 6 patients had splenectomy after surgicalevaluation; this validates any delay in diagnosis can lead tosevere consequences.
To preserve the spleen, when possible, it is necessary toperform a pexy. For our reported cases, splenopexy was theapproach most performed.
In spite of finding a well-vascularized spleen duringsurgery, 60% of cases can lead to secondary splenicischemia. All of them happened in the group that hadsplenopexy procedure; even if it is a small series, we canwonder if there is a correlation between the approach and thesecondary ischemia. We cannot conclude if one splenopexyapproach is more detrimental than the other.
Only 2 gastropexy procedures were performed; theresults seem encouraging, but faced with such a smallnumber of cases, no conclusion can be established(literature). Gastropexy seems to avoid the risk of gastricvolvulus by restoring the most of physiologic anatomypossible while preserving the spleen by lack of manipula-tion [1,17,25].

1524 C. Fiquet-Francois et al.
4. Conclusion
The diagnosis of wandering spleen is extremely difficultto establish because it is such a rare condition and isclinically nonspecific.
An early diagnosis and surgical care are the best guaranteefor preserving the spleen. Additional imaging examinations,especially abdominal sonogram as the imaging examination ofchoice, can help establish a diagnosis when faced with anabnormal location of the spleen. Splenopexy and gastropexyare 2 fixation approaches aiming to maintain the viable spleenin place. Even if the choice of one approach vs another can beargued, gastropexy seems to have the advantage of avoidingsplenic manipulation and restore normal anatomy.
The choice for classic open surgery or laparoscopicsurgery can vary according to the different surgical teams.
When there is no history of abdominal surgery,laparoscopic surgery seems to be the treatment of choice.
References
[1] François-Fiquet C, Belouadah M, Chauvet P, et al. Laparoscopicgastropexy for the treatment of gastric volvulus associated withwandering spleen. J Laparoendosc Adv Surg Tech 2009;19:137-9.
[2] IqbalM, TareenMA, Sohail U. Torsion of awandering spleen presentingas a case of acute abdomen. J Coll Physicians Surg Pak 2009;19:123-4.
[3] Wallace S, Herer E, Kiraly J, et al. A wandering spleen: unusual causeof a pelvic mass. Obstet Gynecol 2008;112:478-80.
[4] Brown CV, Virgilio GR, Vazquez WD. Wandering spleen and itscomplications in children: a case series and review of the literature. JPediatr Surg 2003;38:1676-9.
[5] Di Crosta I, Inserra A, Gil CP, et al. Abdominal pain and wanderingspleen in young children: the importance of an early diagnosis. JPediatr Surg 2009;44:1446-9.
[6] Allen KB, Andrews G. Pediatric wandering spleen—the case forsplenopexy: review of 35 reported cases in the literature. J Pediatr Surg1989;24:432-5.
[7] Desai DC, Hebra A, Davidoff AM, et al. Wandering spleen: achallenging diagnosis. South Med J 1997;90:439-43.
[8] Steinberg R, Karmazyn B, Dlugy E, et al. Clinical presentation ofwandering spleen. J Pediatr Surg 2002;37:E30.
[9] Ben Ely A, Seguier E, Lotan G, et al. Familial wandering spleen: a firstinstance. J Pediatr Surg 2008;43:E23-5.
[10] Yilmaz O, Genc A, Ozcan T, et al. Unusual association of omphaloceleand wandering spleen. Eur Surg Res 2008;41:331-3.
[11] Kulkarni ML, Sneharoopa B, Vani HN, et al. Eventration of thediaphragm and associations. Indian J Pediatr 2007;74:202-5.
[12] Ratan SK, Grover SB, Kulsreshtha R, et al. Left diaphragmaticeventration with a suprapubic spleen: report of a case. Surg Today2001;31:184-6.
[13] Bonnet J, Louis D. Intrathoracic volvulus of the spleen revealing leftposterolateral diaphragmatic hernia. Arch Pediatr 1996:701-4.
[14] Hosgor M, Karaca I, Karkiner A, et al. Associated malformations indelayed presentation of congenital diaphragmatic hernia. J PediatrSurg 2004;39:1073-6.
[15] Pelizzo G, Lembo MA, Franchella A, et al. Gastric volvulus associatedwith congenital diaphragmatic hernia, wandering spleen, and intra-thoracic left kidney: CT findings. Abdom Imaging 2001;26:306-8.
[16] Romero JR, Barksdale EM. Wandering spleen: a rare cause ofabdominal pain. Pediatr Emerg Care 2003;19:412-4.
[17] Spector JM, Chappell J. Gastric volvulus associated with wanderingspleen in a child. J Pediatr Surg 2000;35:641-2.
[18] Liu HT, Lau KK. Wandering spleen: an unusual association withgastric volvulus. AJR Am J Roentgenol 2007;188:W328-30.
[19] Lin CH, Wu SF, Lin WC, et al. Wandering spleen with torsion andgastric volvulus. J Formos Med Assoc 2005;104:755-8.
[20] Qazi A, Awadalla S. Wandering spleen: a rare cause of mesenteroaxialgastric volvulus. Pediatr Surg Int 2004;20:878-80.
[21] Karmazyn B, Steinberg R, Gayer G, et al. Wandering spleen—thechallenge of ultrasound diagnosis: report of 7 cases. J Clin Ultrasound2005;33:433-8.
[22] Ben Ely A, Zissin R, Copel L, et al. The wandering spleen: CT findingsand possible pitfalls in diagnosis. Clin Radiol 2006;61:954-8.
[23] Thambidorai CR, Imtiaz A, Nafiqudin M, et al. Torsion of a wanderingspleen with whorled appearance of the splenic hilum in CT scan. Med JMalaysia 2005;60:653-4.
[24] Marinaccio F, Caldarulo E, Nobili M, et al. Uncommon etiology ofacute abdomen in pediatric age: the torsion of spleen. G Chir 2005;26:34-6.
[25] Arda K, Kizilkanat K, Celik M, et al. Intermittent torsion of awandering spleen in a child: the role of MRI in diagnosis. Jbr-Btr2004;87:70-2.
[26] Hirose R, Kitano S, Bando T, et al. Laparoscopic splenopexy forpediatric wandering spleen. J Pediatr Surg 1998;33:1571-3.
[27] Lacreuse I, Moog R, Kauffmann I, et al. Laparoscopic splenopexy for awandering spleen in a child. J Laparoendosc Adv Surg Tech A2007;17:255-7.
[28] Cavazos S, Ratzer ER, Fenoglio ME. Laparoscopic management of thewandering spleen. J Laparoendosc Adv Surg Tech A 2004;14:227-9.
[29] Kleiner O, Newman N, Cohen Z. Pediatric wandering spleensuccessfully treated by laparoscopic splenopexy. J LaparoendoscAdv Surg Tech A 2006;16:328-30.