cervicogenic headaches - dpt portfolios -
TRANSCRIPT
Cervicogenic HeadachesBy: Anjali PaintalUNC DPT Student Class of 2020
Primary and Secondary Headaches● Primary headaches consist of
migraines, tension type headaches, and medication overdose headaches
● Secondary headaches are symptoms of another condition and include headaches caused by tumors, hemorrhage, trauma, TMJ, and cervicogenic headaches.
Description of Cervicogenic Headache ● Cervicogenic headaches are head and/or face pain that originates
from the cervical spine. These headaches occur due to a disruption or injury within the upper cervical spine that affects the area of convergence between the trigeminal, spinal accessory, and cervical afferents.
● It is crucial for physical therapists to rule out other potential causes for headaches before treating a suspected cervicogenic headache.
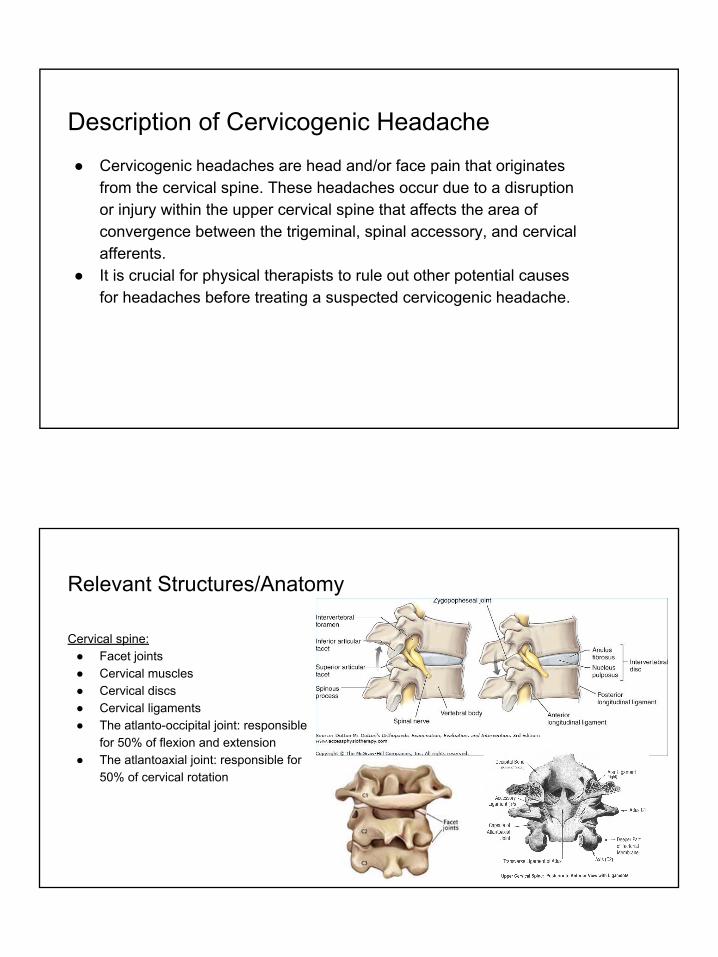
Relevant Structures/Anatomy
Cervical spine:● Facet joints ● Cervical muscles● Cervical discs ● Cervical ligaments● The atlanto-occipital joint: responsible
for 50% of flexion and extension ● The atlantoaxial joint: responsible for
50% of cervical rotation
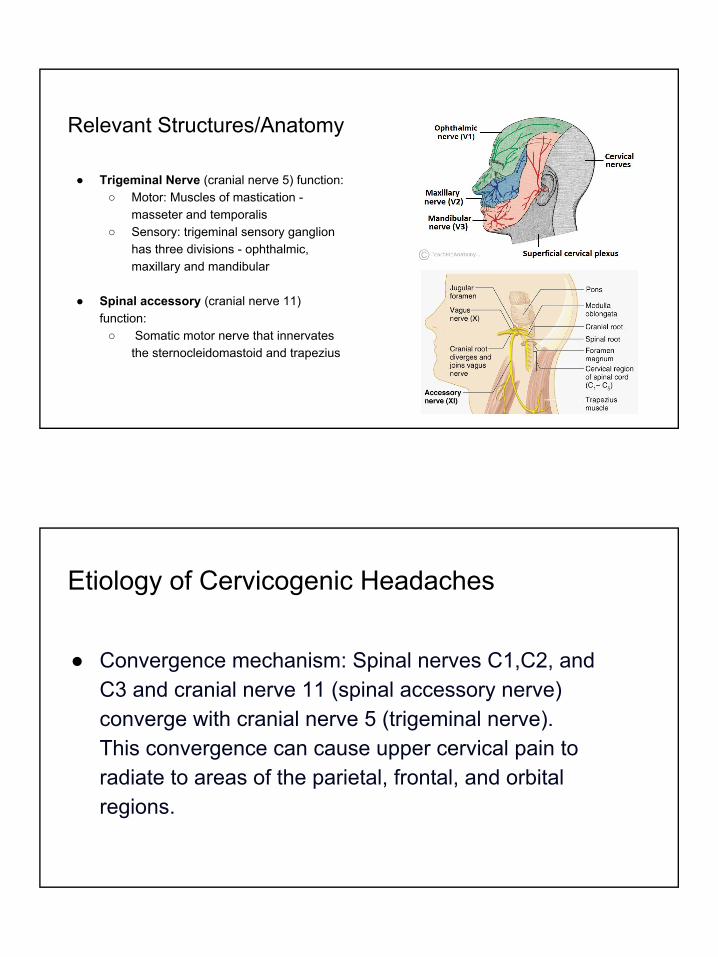
Relevant Structures/Anatomy
● Trigeminal Nerve (cranial nerve 5) function: ○ Motor: Muscles of mastication -
masseter and temporalis ○ Sensory: trigeminal sensory ganglion
has three divisions - ophthalmic, maxillary and mandibular
● Spinal accessory (cranial nerve 11) function:
○ Somatic motor nerve that innervates the sternocleidomastoid and trapezius
Etiology of Cervicogenic Headaches
● Convergence mechanism: Spinal nerves C1,C2, and C3 and cranial nerve 11 (spinal accessory nerve) converge with cranial nerve 5 (trigeminal nerve). This convergence can cause upper cervical pain to radiate to areas of the parietal, frontal, and orbital regions.
Common Causes/ Triggers
● Poor posture● Sleeping habits● Carrying heavy items on one shoulder ● Poorly designed workstations● Sitting in chairs or car seats for prolonged period of time ● Trauma to cervical spine ● Whiplash
Epidemiology ● According to data from 2011 about 47% of global
population suffers from a headache and 15-20% of those headaches are cervicogenic.
● Cervicogenic headaches affect approx 2.2% of global population
● In pain management clinics, prevalence over cervicogenic headaches is as high as 20% of patients with chronic headache
● Some studies say women are as likely as men to experience cervicogenic headaches.
● Other studies say women are 4x more likely than men to experience cervicogenic headaches
● Usually affects people from 30-44 years old...can you guess why?
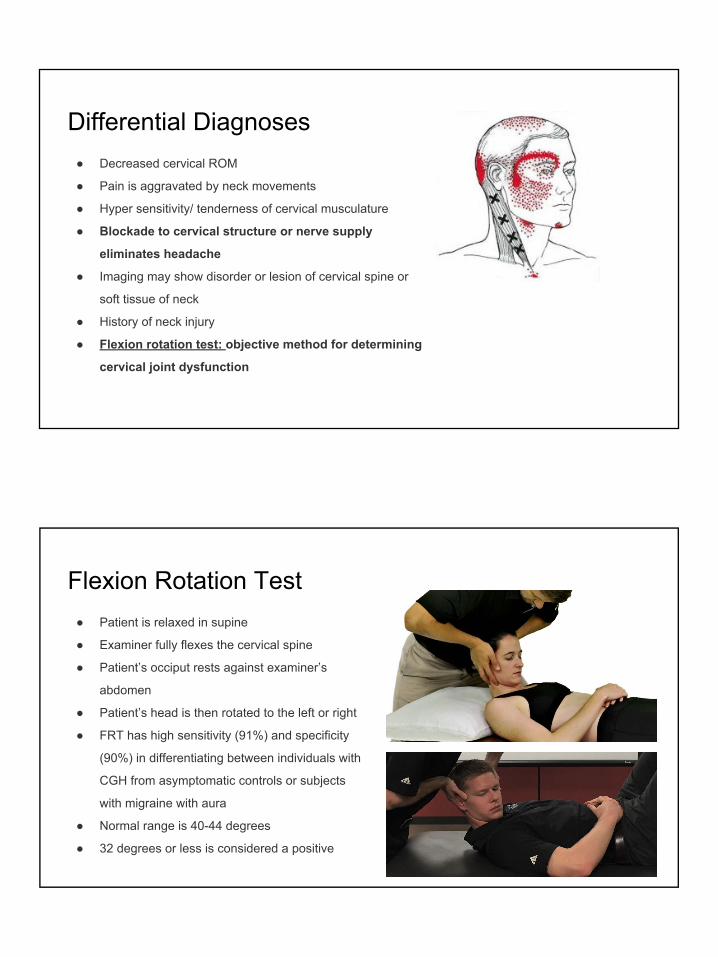
Differential Diagnoses ● Decreased cervical ROM
● Pain is aggravated by neck movements
● Hyper sensitivity/ tenderness of cervical musculature
● Blockade to cervical structure or nerve supply
eliminates headache
● Imaging may show disorder or lesion of cervical spine or
soft tissue of neck
● History of neck injury
● Flexion rotation test: objective method for determining
cervical joint dysfunction
Flexion Rotation Test ● Patient is relaxed in supine
● Examiner fully flexes the cervical spine
● Patient’s occiput rests against examiner’s
abdomen
● Patient’s head is then rotated to the left or right
● FRT has high sensitivity (91%) and specificity
(90%) in differentiating between individuals with
CGH from asymptomatic controls or subjects
with migraine with aura
● Normal range is 40-44 degrees
● 32 degrees or less is considered a positive
PT Treatment ● Cervical manipulations and
mobilizations ● Cervical SNAGS ● Thoracic manipulations and
mobilizations● Muscle stretching● Strengthening exercises
○ esp endurance exercises for deep cervical flexors and scapular stabilizers
● Postural reeducation
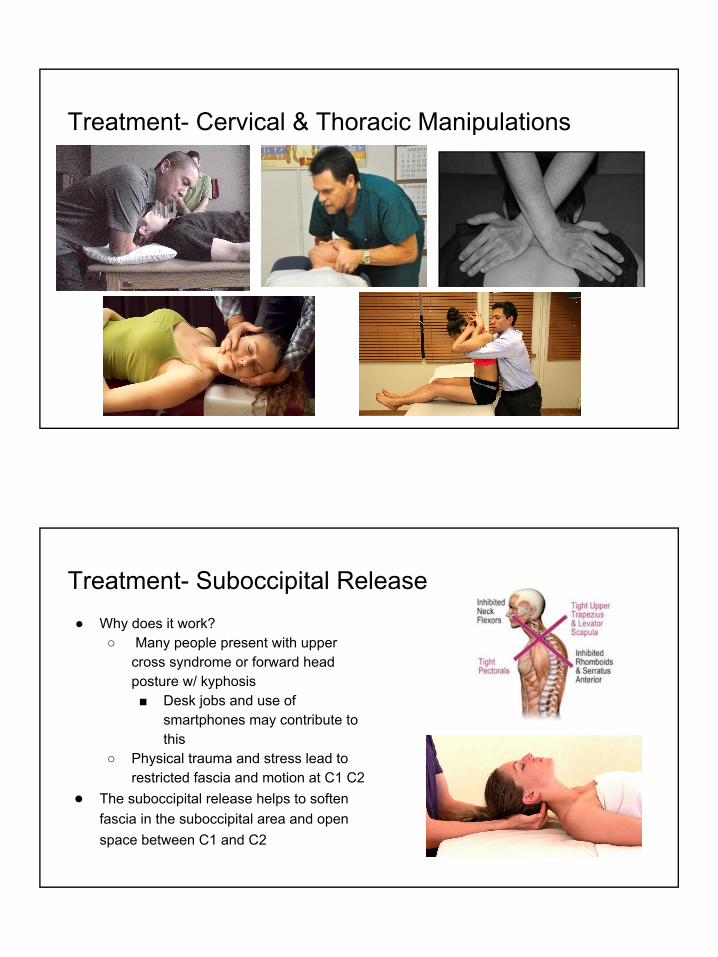
Treatment- Cervical & Thoracic Manipulations
Treatment- Suboccipital Release ● Why does it work?
○ Many people present with upper cross syndrome or forward head posture w/ kyphosis ■ Desk jobs and use of
smartphones may contribute to this
○ Physical trauma and stress lead to restricted fascia and motion at C1 C2
● The suboccipital release helps to soften fascia in the suboccipital area and open space between C1 and C2
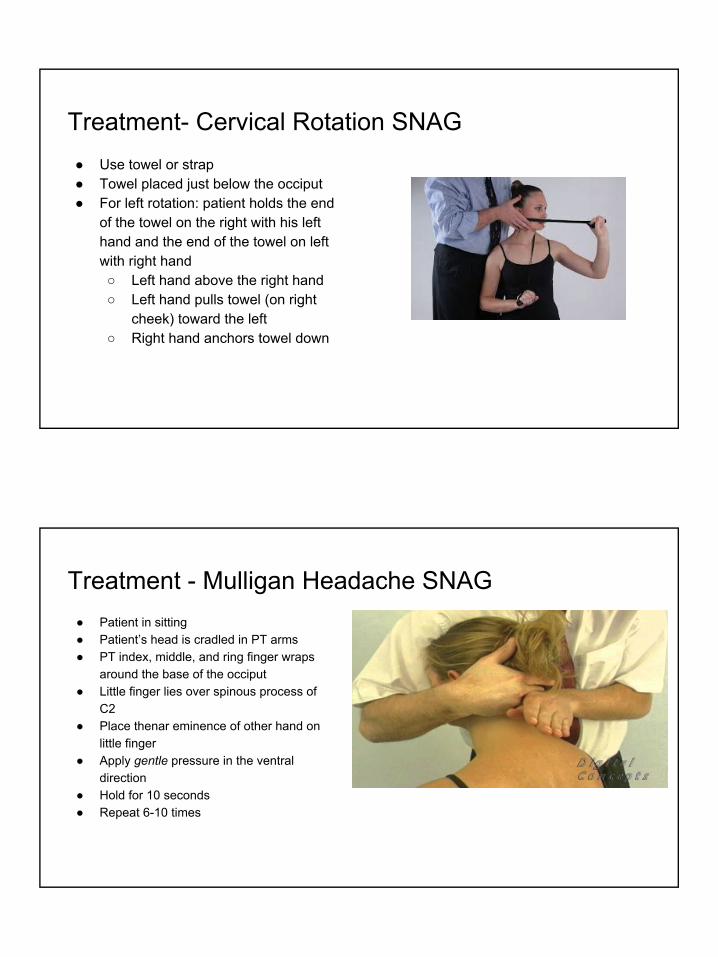
Treatment- Cervical Rotation SNAG● Use towel or strap● Towel placed just below the occiput ● For left rotation: patient holds the end
of the towel on the right with his left hand and the end of the towel on left with right hand ○ Left hand above the right hand ○ Left hand pulls towel (on right
cheek) toward the left ○ Right hand anchors towel down
Treatment - Mulligan Headache SNAG ● Patient in sitting● Patient’s head is cradled in PT arms ● PT index, middle, and ring finger wraps
around the base of the occiput● Little finger lies over spinous process of
C2● Place thenar eminence of other hand on
little finger ● Apply gentle pressure in the ventral
direction ● Hold for 10 seconds● Repeat 6-10 times
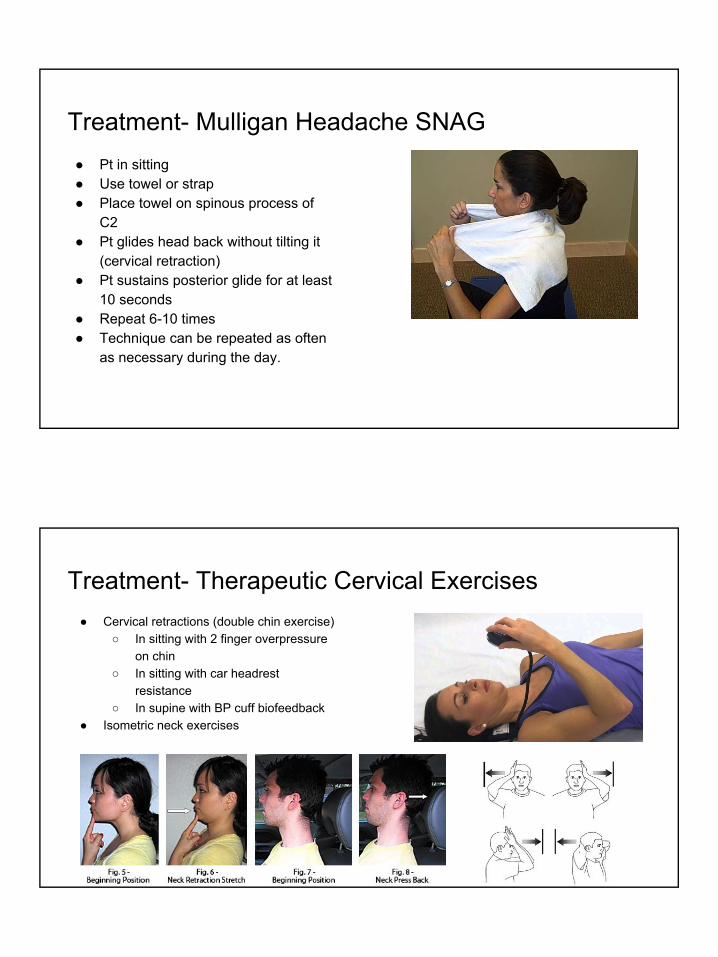
Treatment- Mulligan Headache SNAG● Pt in sitting● Use towel or strap● Place towel on spinous process of
C2 ● Pt glides head back without tilting it
(cervical retraction)● Pt sustains posterior glide for at least
10 seconds ● Repeat 6-10 times● Technique can be repeated as often
as necessary during the day.
Treatment- Therapeutic Cervical Exercises ● Cervical retractions (double chin exercise)
○ In sitting with 2 finger overpressure on chin
○ In sitting with car headrest resistance
○ In supine with BP cuff biofeedback ● Isometric neck exercises
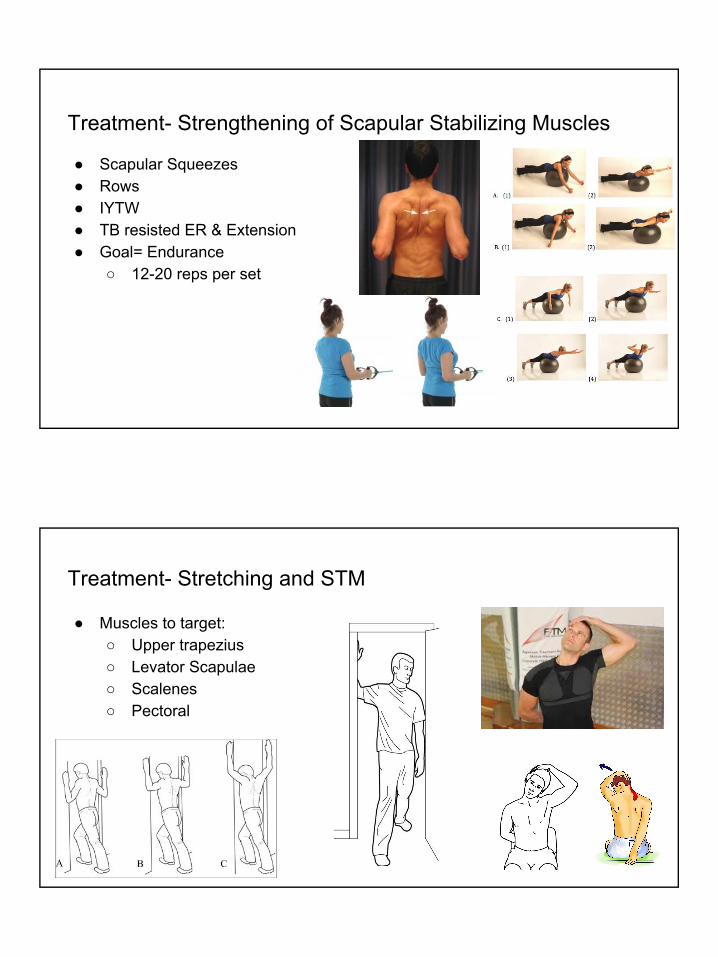
Treatment- Strengthening of Scapular Stabilizing Muscles ● Scapular Squeezes● Rows● IYTW ● TB resisted ER & Extension● Goal= Endurance
○ 12-20 reps per set
Treatment- Stretching and STM
● Muscles to target:○ Upper trapezius ○ Levator Scapulae○ Scalenes ○ Pectoral

ResourcesSanders RD. The Trigeminal (V) and Facial (VII) Cranial Nerves: Head and Face Sensation and Movement. Gillig PM, ed. Psychiatry (Edgmont). 2010;7(1):13-16.
Page P. CERVICOGENIC HEADACHES: AN EVIDENCE-LED APPROACH TO CLINICAL MANAGEMENT. International Journal of Sports Physical Therapy. 2011;6(3):254-266.
Hall T, Briffa K, Hopper D. Clinical Evaluation of Cervicogenic Headache: A Clinical Perspective. The Journal of Manual & Manipulative Therapy. 2008;16(2):73-80.Page P. CERVICOGENIC HEADACHES: AN EVIDENCE-LED APPROACH TO CLINICAL MANAGEMENT. International Journal of Sports Physical Therapy. 2011;6(3):254-266.
Howard PD, Behrns W, Martino MD, DiMambro A, McIntyre K, Shurer C. Manual examination in the diagnosis of cervicogenic headache: a systematic literature review. The Journal of Manual & Manipulative Therapy. 2015;23(4):210-218. doi:10.1179/2042618614Y.0000000097.
Dunning JR, Butts R, Mourad F, et al. Upper cervical and upper thoracic manipulation versus mobilization and exercise in patients with cervicogenic headache: a multi-center randomized clinical trial. BMC Musculoskeletal Disorders. 2016;17:64. doi:10.1186/s12891-016-0912-3.
Lewis, Fran & Olivier, Benita. (2010). The Effectiveness of Physiotherapy in Cervicogenic Headache and Concurring Temporomandibular Dysfunction: A Case Report. South African Journal of Physiotherapy. 66. 26-31. 10.4102/sajp.v66i1.60.
Biondi, D. M. (2005, June). Physical treatments for headache: A structured review. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/15953306
Cervicogenic Headache. (n.d.). Retrieved from https://www.physio-pedia.com/Cervicogenic_Headache#cite_note-Fritz-17