categorization and cognitive deficits in compulsive hoarding
TRANSCRIPT

1
Categorization and Cognitive Deficits in Compulsive Hoarding
Jessica R. Grisham1*, Melissa M. Norberg2, Alishia D. Williams1, Sarah P. Certoma1, & Raja
Kadib1
1 School of Psychology, University of New South Wales, Sydney NSW 2052, Australia
2 National Cannabis Prevention and Information Centre, University of New South Wales,
Sydney NSW 2052, Australia
*Corresponding author:
Phone: (+61 2) 9385 3031
Fax: (+61 2) 9385 3641
Email: [email protected]
Word Count – 7,603
2
Abstract
According to the cognitive-behavioural model of compulsive hoarding, information
processing deficits in the areas of attention, memory, decision-making, and categorization
contribute to hoarding behaviour. The purpose of the current study was to examine whether
individuals with compulsive hoarding exhibited impairment on executive functioning and
categorization tasks. Three groups of participants were recruited (N = 60): individuals with
compulsive hoarding syndrome, individuals with an Axis I mood or anxiety disorder, and
nonclinical control participants. All participants completed self-report measures of cognitive
difficulties, neuropsychological tests of executive functioning and decision-making, and four
categorization tasks. Results suggested that hoarding participants reported more cognitive
failures and more problems with attention and decision-making than nonclinical control
participants. In addition, hoarding participants performed worse than both control groups on
the Stockings of Cambridge (SOC), a neuropsychological test of planning ability, and were
slower and more anxious during a categorization task. These findings suggest that specific
deficits in executive functioning may be associated with the difficulties hoarding patients
have organizing their possessions.
Keywords: categorization; compulsive hoarding; executive functioning; planning; saving
3
Categorization and Cognitive Deficits in Compulsive Hoarding
Compulsive hoarding patients exhibit problems grouping their possessions into
categories, which contributes to the disorganization and clutter that are hallmark features of
this disorder (Frost & Hartl, 1996). They treat each object as unique, which leads them to feel
more anxious, sort more slowly, and create numerous categories when a few may suffice.
Wincze, Steketee, and Frost (2007) investigated differences in the way hoarding patients
categorize by contrasting hoarding participants, obsessive-compulsive non-hoarding
participants and non-psychiatric controls on categorization tasks. Participants sorted both
common household items and index cards on which the experimenter had written the name of
an object commonly found in the participant’s home. Although the groups did not differ
when sorting common household items, hoarding participants created more categories than
non-psychiatric controls when sorting personal index cards. They also took more time to sort
personal index cards than both control groups. Lastly, hoarding participants and obsessive-
compulsive non-hoarding participants reported higher anxiety prior to sorting than did non-
psychiatric controls. The results of this study suggested that categorization problems may
occur only when individuals with hoarding sort their own possessions.
On the other hand, Luchian, McNally, and Hooley (2007) demonstrated that
nonclinical hoarding participants engage in under-inclusive behaviour when categorising
non-personal objects. Using similar non-personal objects to Wincze and colleagues’
household items, Luchian and colleagues found that individuals who self-identified as
“packrats” created more categories, took almost twice as long to sort objects, and found
sorting common household items to be more difficult and stressful than did nonhoarding
participants. Inconsistencies between this study and Wincze et al. (2007) may be due to
4
sample (nonclinical versus clinical hoarding participants) and methodological differences
between the two studies. One difficulty in comparing the two studies is the manner in which
Wincze and colleagues (2007) represented personal objects in their study. Rather than using
participants’ actual belongings, they used words written on index cards to represent personal
objects. Therefore, their findings may represent a difficulty with sorting paper items (Frost &
Hartl, 1996), and not necessarily difficulties with sorting personal items. Together, findings
from Wincze et al. (2007) and Luchian et al. (2007) suggest that individuals who hoard may
have problems with sorting personal items, nonpersonal items, common household items,
and/or paper items. Thus, the exact circumstances under which hoarding patients have
categorization difficulties remains unknown due to the lack of systematic comparisons
between personal and non-personal objects.
The categorization problems demonstrated by hoarding patients may be linked to
information-processing difficulties proposed to underline hoarding behaviour (Frost & Hartl,
1996; Frost & Steketee, 1998). Hoarding patients report increased symptoms of attention
deficit hyperactivity disorder (ADHD; Hartl, Duffany, Allen, Steketee, & Frost, 2005) and
have been found to perform worse on certain neuropsychological tasks, including measures
of attention and nonverbal intelligence (Grisham, Brown, Savage, Steketee, & Barlow, 2007),
memory (Hartl et al., 2004) and decision-making (Lawrence et al., 2006). According to the
cognitive-behavioural model, the combination of these information-processing deficits
contributes to organizational problems (Grisham et al., 2007). For example, efficient
categorization involves planning, developing strategies for how to best group objects,
sustained attention, sufficient impulse control, and decision-making abilities. With respect to
planning, the individual must identify and organize the steps needed to carry out the goal of
creating distinct categories. He or she needs to consider alternatives, weigh these alternatives,
5
and make choices. Furthermore, the individual must be able to stick to the task at hand. All of
these skills are needed in order to make a decision about where an object belongs. Along
these lines, Wincze and colleagues (2007) found that self-reported indecisiveness related
positively with the number of categories created and pre-task anxiety levels.
The purpose of the current study was to clarify the nature of the executive functioning
and categorization difficulties associated with compulsive hoarding. To investigate these
issues, three groups of participants were recruited: individuals whose most prominent
psychiatric symptom was compulsive hoarding, as defined by Steketee and Frost (2003),
individuals with a primary Axis I mood or anxiety disorder who did not meet criteria for
compulsive hoarding, and nonclinical control participants. All participants completed four
categorisation tasks (personal versus non-personal; actual versus index card), as well as self-
report measures of cognitive difficulties and neuropsychological tests of executive
functioning.
We hypothesised that, relative to clinical and nonclinical controls, those in the
hoarding group would report more cognitive failures and more difficulty with sustained
attention and decision-making. In addition, we hypothesised that hoarding patients would
perform worse on tests of executive functioning. With respect to the categorization task, we
predicted that the hoarding group would create more categories, take more time to create
categories, and experience more discomfort before and after the task. We also predicted that
these differences would be more pronounced for personal objects compared to non-personal
objects.
Method
Participants
6
Three groups of participants (total N = 60) were recruited from the community via
advertisements in local newspapers: individuals with compulsive hoarding problems (n = 23),
participants with a current mood or anxiety disorder who did not compulsively hoard (n =
17), and nonclinical control participants with no current Axis I disorder (n = 20). Individuals
who were currently psychotic or suicidal or had a neurological disorder (e.g., dementia) were
excluded from the study. Hoarding participants were required to meet compulsive hoarding
criteria as defined by Frost and Hartl (1996): (1) the acquisition of, and failure to discard a
large number of possessions that appear to be useless or of limited value; (2) living spaces
sufficiently cluttered so as to preclude activities for which those spaces were designed; and
(3) significant distress or impairment in functioning caused by the hoarding. Four individuals
who reported subclinical hoarding symptoms were excluded from the hoarding group due to
their failure to meet these criteria, leaving 19 participants in the hoarding group (N =56). All
participants were offered a small financial reward in exchange for their time.
Persons recruited to participate in the comparison groups were matched to the
hoarding group with respect to age, F (2, 53) =2.04, p =.14, and gender, χ2 (2, N=56) = 3.94,
p =.14, due to the potential effect of these characteristics on neuropsychological performance.
The mean age of the sample was 48.0 years (SD = 11.0) and 39 of the participants (70%)
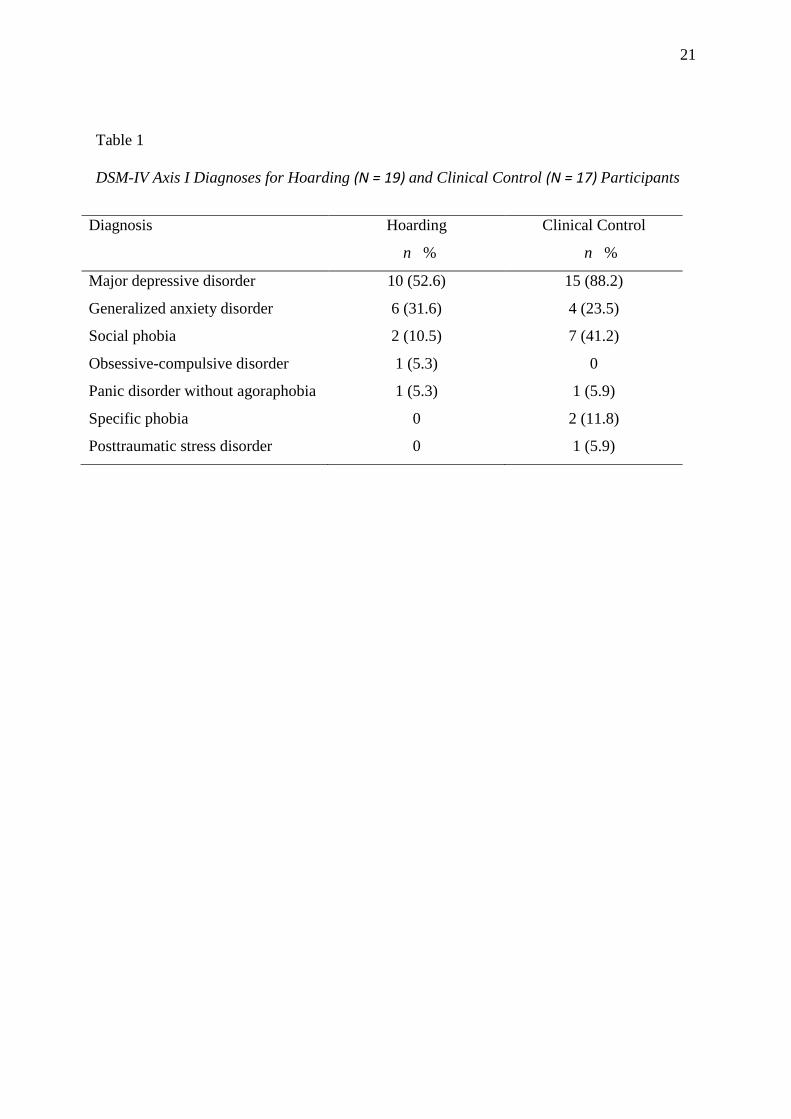
were female. See Table 1 for the Axis I diagnoses of the hoarding and clinical control groups.
Measures
Diagnostic Assessment
Anxiety Disorders Interview Schedule for DSM-IV (ADIS-IV; Brown, Di Nardo, &
Barlow, 1994) is a semi-structured interview to diagnose anxiety, mood, somatoform, and
7
substance use disorders and to screen for the presence of other conditions, such as psychosis.
The ADIS has demonstrated good to excellent reliability for the majority of anxiety and
mood disorders (Brown, Di Nardo, Lehman, & Campbell, 2001). A dimensional Hoarding
Rating Scale was also administered to enable interviewers to diagnose compulsive hoarding.
Five hoarding symptoms (clutter, acquisition, difficulty discarding, distress, and impairment)
were rated from 0 (no difficulty) to 8 (extreme difficulty) (Tolin, Frost, & Steketee, in press).
Self-Report Questionnaires
ADHD Symptom Checklist (ADHD-CL; Barkley & Murphy, 1998). The adult version
of the ADHD-CL is an 18 item self-report measure. Participants are required to rate from 0
(never or rarely) to 3 (very often) the intensity of a number of ADHD symptoms. This
measure has demonstrated good reliability and internal consistency (Barkley & Murphy,
1998). An overall mean of 20.0 (SD = 11.71) has been previously reported in a sample of
compulsive hoarding patients (Grisham et al., 2007).
Clutter Image Rating (CIR; Frost, Steketee, Tolin, & Renaud, 2008). The CIR is a
visual rating scale for clutter in three living spaces – the living room, kitchen and bedroom.
For each living space, participants are shown photographs of the same room with different
levels of clutter. Participants are required to choose which of the nine photographs looks most
like the different areas in their home (1 = least cluttered, 9 = most cluttered). A mean
composite score is calculated for each participant (range 1-9). The scale has good internal
consistency (α = .84) and good convergent and discriminant validity (Frost et al., 2008). Frost
and colleagues (2008) reported an overall mean of 4.01 (SD = 1.80) among individuals with
significant hoarding difficulties.
Cognitive Failures Questionnaire (CFQ; Broadbent, Cooper, Fitzgerald, & Parkes,
1982). This 25-item questionnaire requires participants to rate on a scale from 0 (never) to 4
8
(very often) the frequency with which they make a number of common cognitive mistakes.
The CFQ has demonstrated good convergent and discriminant validity, test-retest reliability
and internal reliability (Broadbent et al., 1982). An overall mean of 40.62 (SD = 17.00) has
been reported for a sample of patients with neurological disorders (e.g., Alzheimer’s,
dementia), while an overall mean of 56.80 (SD = 18.00) has been reported for a sample of
depressed individuals (Wagle, Berrios, & Ho, 1999).
Depression Anxiety Stress Scales (DASS; Lovibond & Lovibond, 1995). The DASS is
a 21-item self-report measure which requires participants to rate on a scale from 0 (does not
apply to me at all) to 4 (applies to me very much) the extent to which each item applies to
them. The items on the DASS tap into depression, anxiety and stress, with subscale scores
ranging from 0 to 42. Depression scores 13 and lower, anxiety scores 9 and lower, and stress
scores 18 and lower indicate symptoms in the mild to normal range (Lovibond & Lovibond,
1995). This measure demonstrates good reliability (Brown, Chorpita, Korotitsch, & Barlow,
1997) and internal consistency (Henry & Crawford, 2005).
Frost Indecisiveness Scale (FIS; Frost & Shows, 1993). The FIS is a 15-item self-
report measure that assesses difficulty making decisions. Participants rate on a scale from 1
(strongly disagree) to 5 (strongly agree) the extent to which each of the statements is true for
them. The FIS has demonstrated good reliability and validity (Frost & Shows, 1993; Rassin,
Muris, Franken, Smit, & Wong, 2007). In a study by Steketee, Frost, and Kyrios (2003),
mean total scores on the FIS were 50.1 (SD = 12.5) for individuals with primary compulsive
hoarding, and 40.6 (SD = 10.0) for individuals with OCD without hoarding.
Obsessive-Compulsive Inventory-Revised (OCI-R; Foa et al., 2002). The OCI-R is an
18-item measure of OCD symptoms containing 7 subscales: doubting, checking, hoarding,
neutralizing, obsessing, ordering, and washing. Participants are required to rate the frequency
9
of each symptom on a scale from 0 (never) to 4 (almost always). The scales show good
reliability, internal consistency and convergent validity (Foa et al., 2002). An and colleagues
(2008) reported a mean hoarding subscale score of 6.6 (SD= 3.2) for individuals with primary
compulsive hoarding, and 1.4 (SD = 2.1) for individuals with OCD without hoarding.
Saving Inventory–Revised (SIR; Frost, Steketee, & Grisham, 2004). The SI-R is a 23
item self-report measure that assesses difficulty discarding, clutter and compulsive
acquisition. It has shown good internal consistency and reliability (Frost et al., 2004).
Previous studies have reported an overall mean of 60 for individuals with hoarding (Frost et
al., 2008; Hartl et al., 2005).
Subjective Units of Distress Scale (SUDS). SUDS ratings are used as an idiographic
anxiety barometer to determine how anxious a person feels from 0 (no anxiety) to 100 (most
anxiety). SUDS rating scales have shown good reliability and validity (Thyer, Papsdorf,
Davis, & Vallecorsa, 1984).
Neuropsychological Tests
Wechsler Abbreviated Scale of Intelligence (WASI; Psychological Corporation,
1999). WASI subtests were used to estimate participants’ verbal and nonverbal intelligence.
WASI Vocabulary and Matrix Reasoning are similar to the Vocabulary and Matrix Reasoning
subtests of the WAIS-III (Wechsler, 1997). Both WASI subtests have demonstrated good
reliability (Psychological Corporation, 1999).
Cambridge Neuropsychological Test Automated Battery (CANTAB; Cambridge
Cognition, 1995) is a battery of neuropsychological tests. It consists of 19 tests administered
through a computer. The subtests have been validated and norms are available for each
subtest. The following subtests were used in the current study:
10
Affective Go/No-go (AGN). The AGN was selected to assess whether hoarding is
associated with decreased response inhibition and ability to shift attention. In this task a
series of positive, negative and neutral words are presented and subjects are required to press
a key when the word matches the target valence. This task measures participants’ ability to
shift between different concepts (i.e. their ability to shift attention from one valence to
another). The measures of performance on this task are latency to respond and number of
omission errors for each target valence.
Cambridge Gambling Task (CGT). Decision-making has been suggested to be
impaired in compulsive hoarding. Hoarding participants may be risk averse, as demonstrated
by their avoidance of discarding because of hypothetical future need. The CGT was included
to measure decision making and risk-taking. On each trial of the CGT, participants are
presented with a number of red and blue cards and must make a decision about which colour
card has a yellow token hidden behind it. They are also asked to select the number of points
they wish to bet on each trial. The bets represent a fixed percentage of the current total points
score (5, 25, 50, 75, and 95%). After selecting a bet, one of the cards is removed to reveal the
actual location of the yellow token, and the chosen bet is added to or subtracted from the total
score depending on whether the prediction was correct. Performance on this task was
measured in terms of two dependent variables. The first was quality of decision making
(proportion correct), which was the proportion of trials on which participants chose the more
likely outcome. The second was risk adjustment (percentage bet), which was the percentage
of accumulated points bet on each trial in relation to the different ratios of coloured boxes.
Intra-Extra Dimensional Set Shift (IED). Mental flexibility and attention are
important aspects of executive functioning that could influence an individual’s ability to sort
and discard objects. This task measures participants’ ability to see concepts, flexibly shift
11
between them and maintain attention. Participants must learn to sort coloured shapes
according to a rule before contingencies are reversed and they must shift to the new rule.
There are nine stages in total on the IED. The number of stages completed and the number of
errors made across trials are indicators of performance on this task.
Stockings of Cambridge (SOC). Finally, individuals must be able to plan effectively in
order to make choices about possessions, categorize them, and effectively arrange for their
appropriate placement or disposal. The SOC is a computerized adaptation of the Tower of
London test and measures planning and problem solving. Participants must move coloured
balls in the lower half of the screen to match the pattern in the upper half. The number of
steps required to complete each trial (i.e. the task’s difficulty) increases as the task
progresses. Performance on this task is indicated by thinking time before attempting the
problem (latency to first response), thinking time between executing each step in the solution,
and number of problems solved within the minimum number of moves.
Procedure
Individuals who responded to the advertisements and did not meet any of the
exclusion criteria were mailed out the self-report questionnaires (ADHD-CL, CFQ, FIS, OCI,
and SI-R) and were scheduled for an appointment within one week of mailing out the
questionnaires. Participants were instructed to bring in 20 items that were representative of
the types of items they would have in their home. On the day of the study, a clinically-trained
experimenter answered any questions about the study and obtained signed consent forms and
completed questionnaires. During the testing session, the experimenter administered the
ADIS-IV (Brown et al., 1994) plus the Hoarding Rating Scale to diagnose primary hoarding
symptoms and comorbid Axis I conditions. Participants also completed the DASS and the
CIR.
12
All participants completed a battery of neuropsychological tests (CANTAB and
WASI subtests), as well as four categorisation tasks. These categorisation tasks included
sorting 20 personal objects, 20 non-personal objects, 20 personal index cards (i.e., cards
labelled with the objects participants brought in), and 20 non-personal index cards (i.e., cards
labelled with the names of the non-personal objects). A counterbalanced design was
employed to control for order effects. Replicating Wincze et al.’s (2007) study, the 20 non-
personal items reflected five types of items commonly found in hoarding participants’ homes:
reading material (newspaper, magazine, book, journal article), clothing (baseball cap, tie, tee-
shirt, sock), used containers (empty coffee can, empty paper-towel roll, lolly wrapper, worn
paper bag), stationary (pencil, paper clip, elastic band, transparent tape), and bathroom items
(soap bar, tooth paste, deodorant, shaving cream). Prior to the sorting tasks, the investigator
explained the use of the SUDS and instructed participants to rate their anxiety prior to and
following each categorisation task. The following instructions were then read, based on those
used by Wincze et al. (2007):
I am going to ask you to sort [20 common household items/the 20 items
you brought in today/20 index cards on which I’ve written the name of
common household items/20 index cards on which I’ve written the name
of the items that you brought in today]. I would like you to separate these
items into different piles in a way that makes sense to you. A pile can
have as few or many items that you want to place in it. There are no right
or wrong ways to complete this task. I would like to see how long it takes
you to do this, naturally, so I’ll be using my stopwatch, but you should
take as much time as you’d like. Any questions? Tell me when you are
finished.

13
When participants indicated that they were finished sorting, the investigator logged
the time taken to complete the task, the number of piles created, the items in each pile, and
SUDS ratings. The entire battery took approximately 2-3 hours to complete, plus
approximately 1 hour to complete the self-report questionnaires. Upon completion of the
study, participants were debriefed and received financial reimbursement for their time.
Results
Descriptive Information
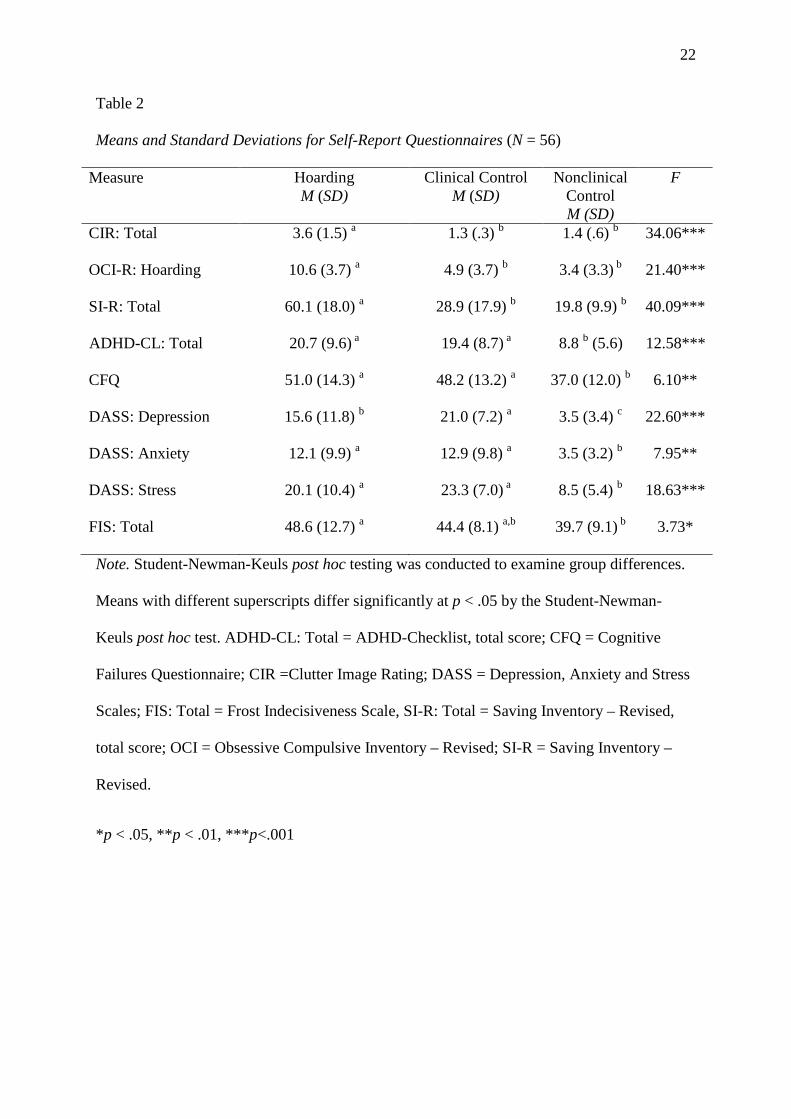
To validate participants’ assignment to groups, the groups were compared to each
other on measures of compulsive hoarding, depression, anxiety, and stress (see Table 2). All
analyses were conducted using analysis of variance (ANOVA) and Student-Newman-Keuls
(SNK) post hoc testing. As expected, ANOVA revealed a significant main effect of groups on
the SI-R, F(2,53)= 40.09, p < .001. Post hoc tests demonstrated that the compulsive hoarding
group reported significantly more hoarding symptoms than the two comparison groups.
Consistent with previous studies, the hoarding group scored a 60.1 on this measure (Frost et
al., 2004). There were also significant main effects of group on the OCI-R Hoarding subscale
(F(2,52)= 21.40, p < .001) and the CI-R (F(2,53)= 34.06, p < .001). Again, post hoc tests
revealed that the hoarding group reported more symptoms than the two comparison groups on
both of these measures. ANOVA also revealed a significant main effect of groups for the
DASS depression subscale, F(2, 53)= 22.60, p < .001, DASS anxiety subscale, F(2, 53)=
7.95, p < .01, and DASS stress subscale, F(2, 53)= 18.63, p < .001. Post hoc tests indicated
that both clinical groups reported significantly more anxiety, depression, and stress than
individuals in the community comparison group. Individuals in the hoarding and clinical
comparison groups did not differ with respect to self-reported level of anxiety or stress,
although the clinical comparison group reported significantly more symptoms of depression.

14
Self Report Measures of Cognitive Functioning
Groups were also contrasted on self-report measures of ADHD symptoms, indecision,
and cognitive failures (Table 2). ANOVA revealed a significant main effect of groups on the
CFQ, F(2, 53)= 6.10, p < .01, the ADHD-CL Total, F(2, 52)= 12.58, p < .01, and the FIS,
F(2, 53)= 3.73, p < .05. Post hoc tests revealed that the hoarding and clinical comparison
groups did not differ with respect to ADHD symptoms or cognitive failures although both
groups had significantly higher scores than the community comparison group. Similarly, with
respect to the FIS, post hoc tests demonstrated that the hoarding group reported significantly
more indecisiveness than the community comparison group, but not the clinical control
group.
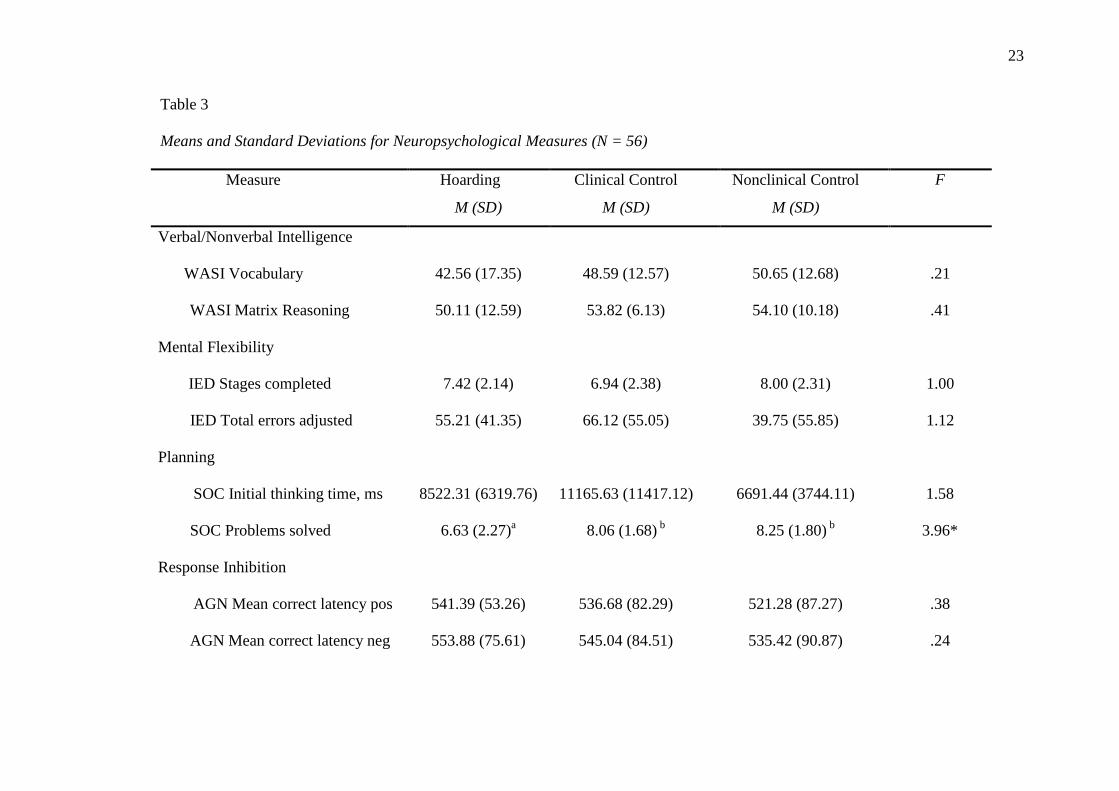
Neuropsychological Tests
Means and standard deviations on each of the neuropsychological measures are
displayed in Table 3. There were no differences between the three groups with respect to
verbal or nonverbal intelligence (Vocabulary and Matrix Reasoning subtests from the WASI).
On a test of planning ability (SOC), ANOVA revealed a significant main effect of groups
with respect to the number of problems solved, F(2, 49)= 5.14, p = .01. Post hoc tests
demonstrated that the hoarding group solved fewer problems than either of the comparison
groups. Contrary to prediction, there were no significant between-group differences with
respect to decision-making (CGT) or ability to shift attention (AGN and IED).
Categorisation Task
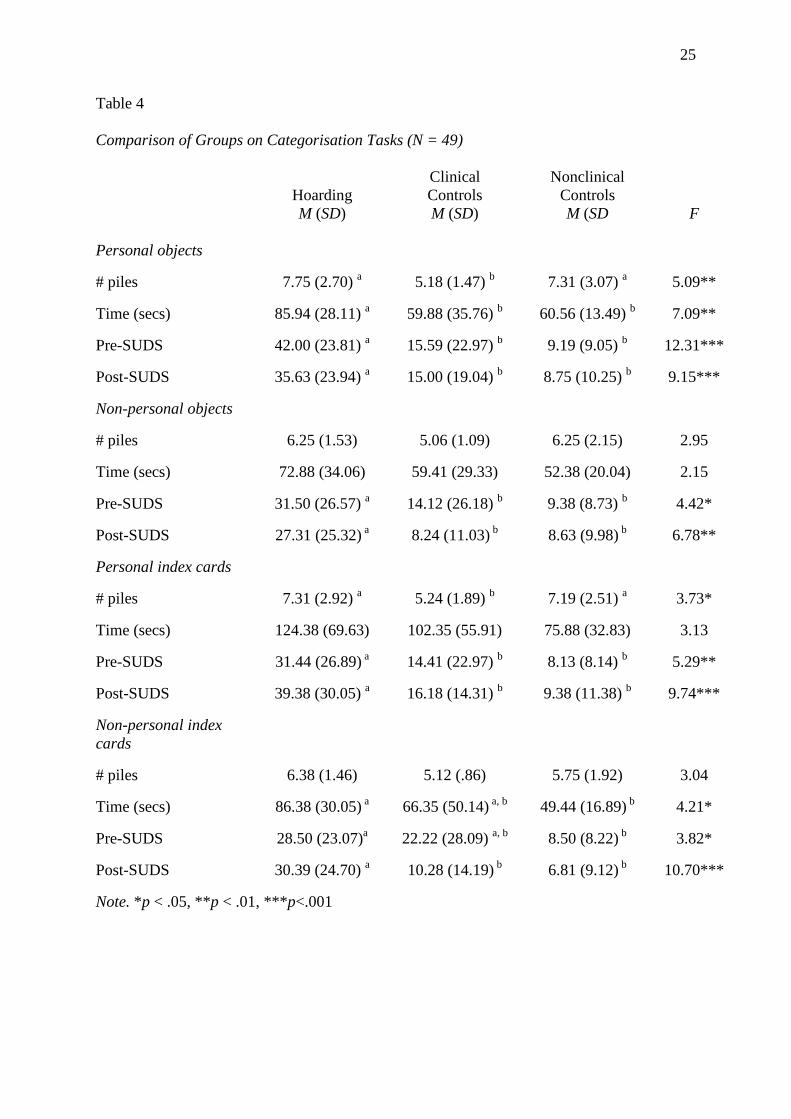
Results from the categorisation tasks are summarised in Table 4. Given the potential
effects on variables of interest, participants who brought in less than 20 personal objects were
excluded from the analyses for personal objects and personal index cards. Thus, after
15
excluding 3 participants in the hoarding group and 4 in the nonclinical control group for this
reason, n = 16 in the hoarding and nonclinical control group and n = 17 in the clinical control
group (N = 50).
There were several between-groups differences on the categorization tasks. With
respect to the number of piles created, there was a significant main effect of groups for
personal objects, F(2, 46)= 5.09, p = .01, and personal index cards, F(2, 46)= 3.73, p < .05.
Post hoc tests revealed that hoarding participants created significantly more categories than
clinical control participants, but not nonclinical control participants, for both types of
personal possessions. Regarding the time taken to sort items, there was a significant main
effect of groups for personal objects, F(2, 46)= 7.09, p < .01, and non-personal index cards,
F(2, 46)= 4.21, p < .05 and a trend for personal index cards, F(2, 46)= 3.13, p = .05. Post hoc
tests demonstrated that hoarding participants took significantly longer to sort personal objects
relative to both comparison groups. They also took significantly more time than nonclinical
control participants to sort non-personal and personal index cards, although they did not
differ significantly from clinical comparison participants on these indices.
The results for anxiety pre sorting task revealed a significant overall effect of groups
for every type of possessions: personal objects, F(2, 46)= 7.09, p < .01, non-personal objects,
F(2, 46)= 7.09, p < .01, personal index cards, F(2, 46)= 7.09, p < .01, and non-personal index
cards, F(2, 46)= 7.09, p < .01. For anxiety post-sorting task, there was also a significant
overall effect of groups for every type of possessions: personal objects, F(2, 46)= 7.09, p <
.01, non-personal objects, F(2, 46)= 7.09, p < .01, personal index cards, F(2, 46)= 7.09, p <
.01, and non-personal index cards, F(2, 46)= 7.09, p < .01. Follow-up tests indicated that the
hoarding group rated their anxiety (SUDS) as significantly higher than both comparison
groups, both before and after the task, regardless of the type of item. The only exception was
16
pre-task anxiety for the non-personal index cards; on this measure hoarding participants
reported significantly more anxiety than nonclinical control participants, but not clinical
control participants.
Discussion
The results of the current study provide further insight into the nature of cognitive
difficulties associated with compulsive hoarding. On self-report measures hoarding
participants reported more difficulties than nonclinical control participants with respect to
decision-making, cognitive failures and ADHD symptoms, although they were not
significantly more impaired on these measures than clinical control participants. This finding
suggests that self-reported cognitive difficulties are not unique to hoarding patients. In
contrast, Grisham et al. (2007) found that hoarding participants reported more ADHD
symptoms than a mixed anxiety control group. Although the hoarding participants in the two
studies reported virtually identical levels of ADHD symptoms, the clinical control group in
the current study reported more ADHD symptoms than the clinical control group in Grisham
et al. (2007). This increased level of ADHD among current clinical controls may be
attributable to the increased depression symptomatology in this group relative to the previous
study, as there is a high rate of comorbidity between ADHD and depression (Jensen et al.,
2001; Jensen, Shervette, Xenakis, & Richters, 1993). Alternatively, higher ADHD symptoms
in the current clinical comparison group may be due to sampling fluctuations between the two
studies.
Contrary to hypotheses, hoarding participants were not impaired on most
neuropsychological tasks. It is noteworthy that while hoarding participants reported
indecisiveness on a self-report questionnaire, their performance on a decision-making task
was unimpaired. This suggests a slight discrepancy between perceived and actual decision-
17
making deficits in compulsive hoarding, which is consistent with memory difficulties (Hartl
et al., 2004). It is also possible that individuals with hoarding problems have decision-making
deficits that are specific to items of personal relevance, which would not be detected by the
Gambling Task. Hoarding participants may only experience decision-making difficulties
when a choice involves options that are emotionally salient or when decisions are tied to
rigid, inflexible beliefs. It is also possible that the CGT was sufficiently structured to help
individuals with compulsive hoarding compensate for decision making difficulty. Including a
decision-making task that is more naturalistic and ecologically valid would help elucidate
whether this is a problem in compulsive hoarding.
A test of planning ability was the only neuropsychological task for which the
hoarding group performed worse than both comparison groups. In this task, participants were
required to complete a number of subgoals and move individual circles while keeping in
mind the main goal of matching the pattern. To score well, the participant had to mentally
plan a series of moves before beginning the sequence. Individuals who hoard may have
demonstrated poor planning on this task due to a failure of inhibitory mechanisms (e.g., they
may have begun trying to solve the problems without sufficient forethought). This finding is
intriguing in light of a recent study reporting that hoarding-related anxiety was negatively
correlated with dorsal prefrontal-striatal and parietal regions, which is consistent with
difficulties in planning (An et al., 2008).
Results of the categorization tasks provided mixed support for the hypothesis that
hoarding participants have categorization difficulties. Visual inspection of Table 4 reveals
that hoarding participants had more difficulty with sorting personal items than non-personal
items. Although the differences were small, hoarding participants created slightly more
categories and remained more anxious after sorting personal items than non-personal items.
18
They also took much longer to sort personal index cards relative to the other tasks. When
examining hoarding participants’ sorting behaviour in comparison to clinical and nonclinical
controls, hoarding participants were generally more anxious when asked to sort, regardless of
the type of item, both before and after the task, yet hoarding patients only created more
categories than clinical controls for personal possessions (both objects and index cards).
There were no categorization tasks, however, for which hoarding participants created
significantly more categories than both control groups.
With respect to time taken to sort items, hoarding participants took significantly
longer than both comparison groups to sort personal objects, taking almost twice as long as
nonclinical control participants. This result is consistent with findings from Wincze et al.
(2007) who suggested that hoarding participants are slow to organize their own possessions
because of the unique qualities they attribute to them. Interestingly, hoarding participants
took longer to sort their own personal items when they were represented on an index card and
experienced an increase in anxiety from pre- to post-sorting, although their anxiety decreased
after sorting the actual objects. Hoarding participants may have expected sorting index cards
to be easier than the actual objects given the contrived nature of the task; however, the
vagueness of the items (e.g., no visual detail regarding object characteristics) may have
contributed to the task being harder than expected (i.e., increased sorting time, increased
post-anxiety rating). Future research may benefit from asking participants about their
perceived reasons for number of categories created, sorting time, and anxiety levels
experienced during these experimental tasks.
Future research may further investigate the role of executive control processes (e.g,
working memory capacity, cognitive flexibility, planning ability) in compulsive hoarding. It
is important to consider, however, that sorting duration may be due to a variety of factors,
19
such as object characteristics, beliefs about and emotional attachment to an object, and
anxiety (Steketee & Frost, 2003; Wincze et al., 2007). Future studies may examine all of
these factors with a larger sample. It will be particularly important to examine the interplay
between executive functioning and the cognitive appraisals and beliefs associated with
hoarding behaviour.
There are several important clinical implications for the current study. Planning skills
are relevant to sorting and organizing possessions, which sometimes involves planning a
temporary placement of an object while clearing out the space where the object will
ultimately be placed. Hoarding patients may find it challenging to plan several steps ahead in
order to dispose of or organize their possessions. It is possible that directly targeting these
difficulties with planning and categorizing may help alleviate some of the core symptoms of
hoarding. Therapy goals may include practicing planning ahead a series of smaller steps
while pursuing the larger organizational goal. In addition, specific categorization training has
been found to be helpful with individuals with traumatic brain injury (Constantinidou et al.,
2005). Although hoarding patients show much milder deficits, it may be possible to
incorporate some type of categorization training into hoarding treatments.
While this study had several strengths, including the use of structured psychiatric
interviews and gold-standard neuropsychological measures, a clinical comparison group, and
improvements in methodology regarding the categorisation task, there were nonetheless
several limitations. First, the hoarding group presented with a large amount of comorbid
diagnoses, which is common for this population (Grisham & Barlow, 2005). This potential
confound is partially addressed by the inclusion of a clinical control group, which reported
equivalent (or greater) levels of general emotional distress compared to the hoarding group.
The clinical group, however, was diagnostically diverse and reported a higher level of
20
depressive symptoms than the hoarding group. Further, while the comparison groups were
matched to the hoarding group for age and gender, we did not assess education level and thus
the groups may have differed with respect to education. In addition, the study would have
been strengthened by determining medication use for all participants. Finally, while we
included several key neuropsychological tests of executive functioning, future studies may
benefit from the inclusion of a more comprehensive battery of tests, including measures of
naturalistic task performance specific to hoarding.
In conclusion, a limited understanding of cognitive factors associated with
compulsive hoarding may contribute to the modest treatment outcomes for this disorder
(Steketee & Frost, 2003). The results of the current study increase our understanding of the
neuropsychological factors that are related to hoarding behaviour. This type of research is an
essential initial step toward significant improvements in treatment for compulsive hoarding.
21
Table 1
DSM-IV Axis I Diagnoses for Hoarding (N = 19) and Clinical Control (N = 17) Participants
Diagnosis
Hoarding
n %
Clinical Control
n %
Major depressive disorder 10 (52.6) 15 (88.2)
Generalized anxiety disorder 6 (31.6) 4 (23.5)
Social phobia 2 (10.5) 7 (41.2)
Obsessive-compulsive disorder 1 (5.3) 0
Panic disorder without agoraphobia 1 (5.3) 1 (5.9)
Specific phobia 0 2 (11.8)
Posttraumatic stress disorder 0 1 (5.9)
22
Table 2
Means and Standard Deviations for Self-Report Questionnaires (N = 56)
Measure Hoarding M (SD)
Clinical Control M (SD)
Nonclinical Control M (SD)
F
CIR: Total 3.6 (1.5) a 1.3 (.3) b 1.4 (.6) b 34.06***
OCI-R: Hoarding 10.6 (3.7) a 4.9 (3.7) b 3.4 (3.3) b 21.40***
SI-R: Total 60.1 (18.0) a 28.9 (17.9) b 19.8 (9.9) b 40.09***
ADHD-CL: Total 20.7 (9.6) a 19.4 (8.7) a 8.8 b (5.6) 12.58***
CFQ 51.0 (14.3) a 48.2 (13.2) a 37.0 (12.0) b 6.10**
DASS: Depression 15.6 (11.8) b 21.0 (7.2) a 3.5 (3.4) c 22.60***
DASS: Anxiety 12.1 (9.9) a 12.9 (9.8) a 3.5 (3.2) b 7.95**
DASS: Stress 20.1 (10.4) a 23.3 (7.0) a 8.5 (5.4) b 18.63***
FIS: Total 48.6 (12.7) a 44.4 (8.1) a,b 39.7 (9.1) b 3.73*
Note. Student-Newman-Keuls post hoc testing was conducted to examine group differences.
Means with different superscripts differ significantly at p < .05 by the Student-Newman-
Keuls post hoc test. ADHD-CL: Total = ADHD-Checklist, total score; CFQ = Cognitive
Failures Questionnaire; CIR =Clutter Image Rating; DASS = Depression, Anxiety and Stress
Scales; FIS: Total = Frost Indecisiveness Scale, SI-R: Total = Saving Inventory – Revised,
total score; OCI = Obsessive Compulsive Inventory – Revised; SI-R = Saving Inventory –
Revised.
*p < .05, **p < .01, ***p<.001
23
Table 3
Means and Standard Deviations for Neuropsychological Measures (N = 56)
Measure Hoarding
M (SD)
Clinical Control
M (SD)
Nonclinical Control
M (SD)
F
Verbal/Nonverbal Intelligence
WASI Vocabulary
WASI Matrix Reasoning
Mental Flexibility
42.56 (17.35)
50.11 (12.59)
48.59 (12.57)
53.82 (6.13)
50.65 (12.68)
54.10 (10.18)
.21
.41
IED Stages completed
IED Total errors adjusted
7.42 (2.14)
55.21 (41.35)
6.94 (2.38)
66.12 (55.05)
8.00 (2.31)
39.75 (55.85)
1.00
1.12
Planning
SOC Initial thinking time, ms
SOC Problems solved
8522.31 (6319.76)
6.63 (2.27)a
11165.63 (11417.12)
8.06 (1.68) b
6691.44 (3744.11)
8.25 (1.80) b
1.58
3.96*
Response Inhibition
AGN Mean correct latency pos
AGN Mean correct latency neg
541.39 (53.26)
553.88 (75.61)
536.68 (82.29)
545.04 (84.51)
521.28 (87.27)
535.42 (90.87)
.38
.24

24
AGN Total omissions positive
AGN Total omissions negative
2.74 (2.58)
2.95 (3.61)
3.35 (5.12)
1.94 (2.34)
2.80 (4.18)
1.70 (2.03)
.12
1.10
Decision Making
CGT Quality decision making
CGT Risk adjustment
.83 (.20)
.13 (.79)
.84 (.22)
.37 (1.28)
.74 (.23)
.83 (1.30)
1.12
1.91
Note. Student-Newman-Keuls post hoc testing was conducted to examine group differences. Means with different superscripts differ
significantly at p < .05 by the Student-Newman-Keuls post hoc test.
*p < .05
25
Table 4
Comparison of Groups on Categorisation Tasks (N = 49)
Hoarding M (SD)
Clinical Controls M (SD)
Nonclinical Controls M (SD
F
Personal objects
# piles 7.75 (2.70) a 5.18 (1.47) b 7.31 (3.07) a 5.09**
Time (secs) 85.94 (28.11) a 59.88 (35.76) b 60.56 (13.49) b 7.09**
Pre-SUDS 42.00 (23.81) a 15.59 (22.97) b 9.19 (9.05) b 12.31***
Post-SUDS 35.63 (23.94) a 15.00 (19.04) b 8.75 (10.25) b 9.15***
Non-personal objects
# piles 6.25 (1.53) 5.06 (1.09) 6.25 (2.15) 2.95
Time (secs) 72.88 (34.06) 59.41 (29.33) 52.38 (20.04) 2.15
Pre-SUDS 31.50 (26.57) a 14.12 (26.18) b 9.38 (8.73) b 4.42*
Post-SUDS 27.31 (25.32) a 8.24 (11.03) b 8.63 (9.98) b 6.78**
Personal index cards
# piles 7.31 (2.92) a 5.24 (1.89) b 7.19 (2.51) a 3.73*
Time (secs) 124.38 (69.63) 102.35 (55.91) 75.88 (32.83) 3.13
Pre-SUDS 31.44 (26.89) a 14.41 (22.97) b 8.13 (8.14) b 5.29**
Post-SUDS 39.38 (30.05) a 16.18 (14.31) b 9.38 (11.38) b 9.74***
Non-personal index cards
# piles 6.38 (1.46) 5.12 (.86) 5.75 (1.92) 3.04
Time (secs) 86.38 (30.05) a 66.35 (50.14) a, b 49.44 (16.89) b 4.21*
Pre-SUDS 28.50 (23.07)a 22.22 (28.09) a, b 8.50 (8.22) b 3.82*
Post-SUDS 30.39 (24.70) a 10.28 (14.19) b 6.81 (9.12) b 10.70***
Note. *p < .05, **p < .01, ***p<.001
26
References
An, S. K., Mataix-Cols, D., Lawrence, N. S., Wooderson, S., Giampietro, V., Speckens, A., et
al. (2008). To discard or not to discard: the neural basis of hoarding symptoms in
obsessive-compulsive disorder. Molecular Psychiatry, 14, 318-331.
Barkley, R. A., & Murphy, K. R. (1998). Attention-deficit hyperactivity disorder: A clinical
workbook (2nd ed.). New York: Guilford Press.
Broadbent, D. E., Cooper, P. F., Fitzgerald, P., & Parkes, L. R. (1982). The cognitive failures
questionnaire (CFQ) and its correlates. British Journal of Clinical Psychology, 21, 1-
16.
Brown, T. A., Chorpita, B. F., Korotitsch, W., & Barlow, D. H. (1997). Psychometric
properties of the Depression Anxiety Stress Scales (DASS) in clinical samples.
Behaviour Research and Therapy, 35, 79-89.
Brown, T. A., Di Nardo, P. A., & Barlow, D. H. (1994). Anxiety Disorders Interview
Schedule for DSM-IV (ADIS-IV). New York, NY: Oxford University Press.
Brown, T. A., Di Nardo, P. A., Lehman, C. L., & Campbell, L. A. (2001). Reliability of
DSM-IV anxiety and mood disorders: Implications for the classification of emotional
disorders. Journal of Abnormal Psychology, 110, 49-58.
Cambridge Cognition (1995). Cambridge Neuropsychological Test Automated Battery
(CANTAB) manual. Cambridge: Author.
Constantinidou, F., Thomas, R. D., Scharp, V. L., Laske, K. M., Hammerly, M. D., &
Guitonde, S. (2005). Effects of categorization training in patients with TBI during
postacute rehabilitation. Journal of Head Trauma Rehabilitation, 20, 143-157.
27
Foa, E. B., Huppert, J. D., Leiberg, S., Langner, R., Kichic, R., Hajcak, G., et al. (2002). The
Obsessive-Compulsive Inventory: development and validation of a short version.
Psychological Assessment, 14, 485-496.
Frost, R. O., & Hartl, T. (1996). A cognitive-behavioral model of compulsive hoarding.
Behaviour Research and Therapy, 34, 341-350.
Frost, R. O., & Shows, D. L. (1993). The nature and measurement of compulsive
indecisiveness. Behaviour Research and Therapy, 31, 683-692.
Frost, R. O., & Steketee, G. (1998). Hoarding: Clinical aspects and treatment strategies. In M.
A. Jenike, L. Baer & W. E. Minichiello (Eds.), Obsessive-compulsive disorder:
Practical management (3rd ed., pp. 533-554). St Louis: Mosby Yearbook Medical.
Frost, R. O., Steketee, G., & Grisham, J. R. (2004). Measurement of compulsive hoarding:
Saving Inventory Revised. Behaviour Research and Therapy, 42, 1163-1182.
Frost, R. O., Steketee, G., Tolin, D. F., & Renaud, S. (2008). Development and validation of
the Clutter Image Rating. Journal of Psychopathology and Behavior Assessment, 30,
193-203.
Grisham, J. R., & Barlow, D. H. (2005). Compulsive hoarding: Current research and theory.
Journal of Psychopathology and Behavior Assessment, 27, 45-52.
Grisham, J. R., Brown, T. A., Savage, C. R., Steketee, G., & Barlow, D. H. (2007).
Neuropsychological impairment associated with compulsive hoarding. Behaviour
Research and Therapy, 45, 1471-1483.
Hartl, T. L., Duffany, S. R., Allen, G. J., Steketee, G., & Frost, R. O. (2005). Relationships
among compulsive hoarding, trauma, and attention-deficit/hyperactivity disorder.
Behaviour Research and Therapy, 43, 269-276.

28
Hartl, T. L., Frost, R. O., Allen, G. J., Deckersbach, T., Steketee, G., Duffany, S. R., et al.
(2004). Actual and perceived memory deficits in individuals with compulsive
hoarding. Depression and Anxiety, 20, 59-69.
Henry, J. D., & Crawford, J. R. (2005). The short-form version of the Depression Anxiety
Stress Scales (DASS-21): construct validity and normative data in a large non-clinical
sample. British Journal of Clinical Psychology 44, 227-239.
Jensen, P. S., Hinshaw, S. P., Kraemer, H. C., Lenora, N., Newcorn, J. H., Abikoff, H. B., et
al. (2001). ADHD comorbidity findings from the MTA study: Comparing comorbid
subgroups. Journal of the American Academy of Child & Adolescent Psychiatry,
40(2), 147-158.
Jensen, P. S., Shervette, R. E., Xenakis, S. N., & Richters, J. (1993). Anxiety and depressive
disorders in attention deficit disorder with hyperactivity: New findings. The American
Journal of Psychiatry, 150(8), 1203-1209.
Lawrence, N. S., Wooderson, S., Mataix-Cols, D., David, R., Speckens, A., & Phillips, M. L.
(2006). Decision making and set shifting impairments are associated with distinct
symptom dimensions in obsessive-compulsive disorder. Neuropsychology, 20, 409-
419.
Lovibond, S. H., & Lovibond, P. F. (1995). Manual for the Depression Anxiety and Stress
Scales (2nd ed.). Sydney: Psychological Foundation.
Luchian, S. A., McNally, R. J., & Hooley, J. M. (2007). Cognitive aspects of nonclinical
obsessive-compulsive hoarding Behaviour Research and Therapy, 45, 1657-1662.
Psychological Corporation (1999). Wechsler Abbreviated Scale of Intelligence Manual. San
Antonio, TX: Author.
29
Rassin, E., Muris, P., Franken, I., Smit, M., & Wong, M. (2007). Measuring general
indecisevenss. Journal of Psychopathology and Behavior Assessment, 19, 61-68.
Steketee, G., & Frost, R. O. (2003). Compulsive hoarding: Current status of the research.
Clinical Psychology Review, 23, 905-927.
Steketee, G., Frost, R. O., & Kyrios, M. (2003). Cognitive aspects of compulsive hoarding.
Cognitive Therapy and Research, 27, 463-479.
Thyer, B. A., Papsdorf, J. D., Davis, R., & Vallecorsa, S. (1984). Autonomic correlates of the
subjective anxiety scale. Journal of Behavior Therapy and Experimental Psychiatry,
15, 3-7.
Tolin, D., Frost, R., & Steketee, G. (in press). A brief interview for assessing compulsive
hoarding: The Hoarding Rating Scale-Interview. Psychiatry Research.
Wagle, A. C., Berrios, G. E., & Ho, L. (1999). The cognitive failures questionnaire in
psychiatry. Comprehensive Psychiatry, 40, 478-484.
Wechsler, D. (1997). WAIS-III administration and scoring manual. San Antonio, TX:
Psychological Corporation.
Wincze, J. P., Steketee, G., & Frost, R. O. (2007). Categorization in compulsive hoarding.
Behaviour Research and Therapy, 45, 63-72.