can morbidly obese patients safely lose weight preoperatively
TRANSCRIPT

Can Morbidly Obese Patients Safely Lose Weight Preoperatively?
Louis F. Martin, MD, FACS, Tjiauw-Ling Tan, MD, Pamela A. Holmes, RN, Dolores A. Becker, RD, John Horn, BS, Edward 0. Bixler, PhD, Hershey, Pemsylvmia
BACKGROUND: Preoperative weight loss is often suggested as a means of reducing operative risk in obese patients re@ring Iaparotomy but there are no large studies docwnenting that &is is fea- sible or helpful. Although several commercial products are available that provide high levels of protein witb low levels of carbohydrates in con- venient liquid preparations, recommendation regarding the extent to which weight loss can be pursued preoperatively are not available.
PURPOSE: To determine whether it is practical and safe to have obese patients lose weight pre- operatively.
PAT~BNTS AND METHODS: We asked 100 severely obese patients requesting gastric bypass surgery to diet before their operations. Seventy patients agreed to diet by consuming a 420 Kcal, 70 g protein liquid diet daily for at least 1 month.
RESULTS: Forty-seven patients lost at least 7.5 kg (mean f SD 17.1 f 0.7). The patients who successfully lost weight preoperatively (dieters group) were significantly heavier than patienta (nondieters group) who did not lose weight (251% * 45% of ideal body weight [IBW] ver- sus 229% * 33% IB’FIP; respectively; P <o.Ol), had a sign&~&y higher ratio of men to women, and had psychiatric evaluations and psy- chological test scores that suggested si&&antly more psychopathology. Other biosocial and med- ical characteristics were similar. Postoperatively, the dieters and nondieters had similar rates for morbidity. Dieters and nondieters had no differ- ences in woundchealitq complications, and sub- groups who had collagen deptiition measured experimentally had similar amomti of hydroxy- proline accumulation in their wounds.
CONCLUSION: These resdts suggest that a preop- erative diet program appeals more to certain mbgroups of severely obese patients than to oth- ers. An aggressive preoperative weight loss pro- gram that encourages patients to lose an average of 17 kg is safe and can be accomplished practi- cally using available commercial products.
From the Departments of Surgery, Psychiatry, and Clinical Nutrition, and The University Weight Management Center, The Milton S. Hershey Medical Center, Hershey, Pennsylvania,
Supported in part by grant I-IL 01502 from the National Institutes of Health, Bethesda, Maryland.
Requests for reprints should be addressed to Louis F. Martin, MD. Louisiana State University School of Medicine, 1542 Tulane Avenue, New Orleans, Louisiana 70112.
Presented at the Sixth International Symposium on Obesity Surgery, Genoa, Italy, September 22, 1992.
0 ne of the most common recommendations that physi- cians dispense to patients is to lose weight. That is
not surprising, since at least 25% of Americans are over- weight.’ Persons who weigh more than 200% of their ideal body weight (IBW) are considered severely, or morbidly, obese1x2 and have dramatically higher prevalence rates for diseases such as coronary artery disease, diabetes, and hy- pertension, and shorter life expectancies.4
In 1965, Prem and associates5 reported mortality rates for hysterectomy for endometrial cancer among women grouped by weight and suggested that obese patients had a higher perioperative mortality than nonobese patients. Most surgeons intuitively agreed with these conclusions, although Pas&a and associate& have argued that the data presented in that report do not justify the conclusions that were reached. More recently, Epstein and coworkers7 re- ported that patients hospitalized for total hip or knee re- placement who were more than 185% of IBW had mean lengths of hospital stay and total charges that both were 30% or more above those for patients who were not that heavy. Although the differences were significant, the heav- ier group only included 10 patients.
In 1992, Pennsylvania released the mortality rates for all surgeons performing coronary artery bypass grafts on Medicare patients,8 and the state has collected similar data on length of stay and charges. The intent was to publicize the differences in outcomes between hospitals and indi- vidual surgeons. This release was criticized because the data were not adjusted for comorbidities (severity ad- justed),g and surgeons with high mortality rates were not given a chance to show whether these rates were due to poor technique, to poor patient selection, or to having pa- tients with more diseases. Although government agencies have agreed that data should not be released unless it is severity adjusted, businesses and the public continue to re- quest nonadjusted data because it is cheaper to produce and can be used in negotiations for lower reimbursement rates for hospitals and physician groups by insurance co- operatives. These reports suggest that in the future obese patients and other groups with comorbid conditions may be denied equal access to care if surgeons and their hos- pitals believe that complication rates or hospital charges will be higher for these groups adversely affecting their reputations if severity-adjusted data are deemed too ex- pensive to collect.
Surgeons have often recommended that obese patients lose weight preoperatively but no one has documented how much weight must be lost before perioperative weight-related problems diminish. Nor is there evidence to document that weight loss during the perioperative pe- riod can be accomplished without promoting wound-heal- ing problems or other problems in obese patients, although there is evidence that cardiac problems can develop if di-
THE AMERICAN JOURNAL OF SURGERY’ VOLUME 169 FEBRUARY 1995 245

WEIGHT LOSS BEFORE SURGERY/MARTIN ET AL -__----------.-
ets do not contain enough protein.‘O All the major surgi- cal texts have chapters on nutritional management and wound healing, but we are not aware of any that make recommendations or even discuss preoperative weight loss for obese patients.
1n 1984, we became convinced that severely obese indi- viduals could safely lose weight using a protein-sparing modified fast (PSMF).“‘12 This approach uses a diet high in protein (more than 1 g/kg per day to protect the patient’s lean body mass) but low in carbohydrate and fat to pro- mote lipolysis. I2 Improvements in metabolic parameters,” cardiovascular function,‘3*‘4 antithrombin III levels is fib- rinolytic activity,16 and pulmonary function” in obese pa- tients who can lose weight preoperatively using a PSMF have the potential to reduce operative risks. Others6s’8 had been recommending essentially similar programs for 30 years to prevent postoperative complications but no peri- operative data support these recommendations.
Several companies have developed liquid diet products that qualify as PSMF but the Federal Trade Commission has complained that few of these companies have collected adequate outcome data to show that their products are cost- effective’” and none recommend using their product pre- operativeIy. Most of these companies state that their diets should be stopped or reversed by administering glucose in- travenous solutions if an operation is required, although they admit they have no data to support their recommen- dations (personal communications with Sandoz Nutrition Corporation, Minneapolis. Minnesota, February 1984; and Ross Laboratories, Columbus, Ohio, June 1993). There- fore, we decided to test the hypothesis that a standard out- patient protein-sparing liquid diet program could safely be used to help morbidly obese patients lose weight preoper- atively without the development of wound-healing prob- lems or protein deficiency.
In 1986, we started a preoperative diet program for severely obese patients who requested antiobesity surgery and met the criteria suggested by the task force of the American Society for Clinical Nutrition.20 Based on pre- viously successful outpatient medical programs,” our model incorporated components of standard behavioral modification including problem solving, nutritional edu- cation, stimulus control. and slowing the eating process, and encouraged exercise and self-monitoring.“’ The be- havioral component did not include group meetings, how- ever, and was not standardized during the time course of this study.
This report documents our experience with 100 patients consecutively undergoing gastric bypass surgery who were asked to lose weight preoperatively. These data suggest that severely obese patients can safely lose 7 kg to 47 kg preoperatively on a PSMF using a standard liquid diet product exclusively until the night before the operation, when fluid depletion can be reversed with intravenous nor- mal saline without glucose.
PATIENTS AND METHODS Patients
Between March 21,1986 and August 7,1990,84 women and 16 men who were at least 210% of IBW (as deter- mined by the midpoint of the suggested weight for people
of medium frames from the 1983 height and weight tables of the Metropolitan Life Insurance Company2) were eval- uated and accepted for operative treatment for obesity at The Milton S. Hershey Medical Center of the Pennsylvania State University College of Medicine. These patients were all asked to participate in a preoperative weight loss pro- gram. Another 31 women and 2 men were evaluated and accepted for treatment during this time who were less than 210% of IBW. These patients were excluded from the study because preoperative weight loss might have placed them below the minimal weight criteria for reimbursement at their time of admission for surgery.
A standard preoperative protocol was followed that eval- uated physical, social, and psychological characteristics and required a minimum of 8 weeks to complete.*’ Our psychiatric evaluation included completion of the Minnesota Multiphasic Personality Inventory (MMPQ2” and two interviews. When the evaluation was completed, patients were assigned to one of three categories: no con- traindications to surgery, some reservations but no psy- chiatric intervention required preoperatively, or psychiatric treatment recommended before further evaluation as a sur- gical candidate.
Patients who decided to attempt weight loss preopera- tively were started on a PSMF using a liquid 420 Kcal, 70 g protein per day diet (Optifast 70 nutritional supplement, Sandoz Nutrition Corporation). Patients were asked to use the diet for at least 1 month and for not longer than 4 months, following the guidelines suggested by Vertes and colleagues” for outpatient therapy. Seventy of the 100 pa- tients reported here voluntarily agreed to attempt to lose weight after this prospective (but not randomized) weight loss protocol was explained. The amount of time each pa- tient pursued preoperative diet therapy was usually not de- cided initially although a subset (20 patients) agreed to try it for less than 1 month.
Patients were classified as dieters if they lost at least 7.5 kg in the month before surgery, stated they had fol- lowed the diet, and demonstrated ketones on urinalysis from their preoperative admission evaluation. These pa- tients were given at least 1 L normal saline intravenously the night before surgery for rehydration. These criteria were used to make sure our conclusions would be based on observations obtained from the aggressive use of a diet in the immediate preoperative period and to main- tain lipolysis perioperatively. The other patients were classified as nondieters.
Methods The operation and postoperative care have been previ-
ously described. 22 Briefly, all patients underwent Roux- en-Y gastric bypass connecting a 40-cm Roux limb of je- junum to a 20-mL proximal gastric pouch using an 11 -mm diameter hand-sewn gastrojejunostomy. Postoperatively, patients were maintained on the PSMF formula for the first 6 weeks before beginning a transition to a regular diet. Patients were instructed to take a multivitamin daily and received 1,000 mg of vitamin B i2 intramuscularly ev- ery 6 months.
Between March 1988 and December 1989 all patients, both those who indicated they would attempt weight loss
246 THE AMERICAN JOURNAL OF SURGERY”’ VOLUME 169 FEBRUARY 1995

and those who did not wish to try, were also asked to par- ticipate in a prospective study to examine wound healing that involved perioperative measurement of hydroxypro- line accumulation in subcutaneously implanted polyte- trafluoroethylene (PTFE) tubes.
We measured accumulation of hydroxyproline in PTFE tubing as an index of collagen formation using the tech- nique described by Goodson and Hunt.24 This method mea- sures the ingrowth of granulation tissue into a wound cylin- der (the PTFE tubing) after a standard wound is created. The tubing was placed on the day of operation and re- moved 7 days later. The specimens were handled as pre- viously describedz4 to measure hydroxyproline. The hy- droxyproline content of each tube was then multiplied by 6.95 and this number divided by the length of the PTFE specimen to compute micrograms per centimeter of total
collagen. The rate of collagen forrmation has been corre- lated with the tensile strength of incised wounds.25
Medical, psychological, and digestive (or food ingestion) complications were categorized as described in our first pub- lication.22 We chose to group four postoperative complica- tions that should decrease with weight ioss and three others that could increase if weight loss adversely affected wound healing or destabilized bile. The complications we identi- fied as potentially decreasing included pulmonary, throm- botic, diabetic, and cardiovascular6 Complications that might increase after acute preoperative weight loss included gallstone formation~6~27 hernia, and wound infection.
Our success rate in maintaining contact with patients for 1 year was 96%. Eighty-seven of 100 patients were followed up for 2 years, 62 of 73 (85%) for 3 years, and 39 of 46 (85%) for 4 years. The average length of follow-up for this group was 42 months. Weight loss was measured by track- ing the percent of IBW and body mass index (BMI = kg/m2).
One patient died of metastatic disease from an extrem- ity sarcoma discovered more than 2 years after gastric by- pass. Another patient developed acute renal failure from a recurrence of kidney stones that caused bilateral obstruc- tion in the first postoperative year. He then developed chronic proteinuria and hypoalbuminemia but did not maintain contact with his physicians. He died of septic shock after developing a necrotizing fascitis from an ab- scessed tooth. All other patients lost weight and improved their general health.
Statistical calculations were performed on a computer (VAX 1 l/780, Digital Equipment Corporation, Maynard, Massachusetts) using a standard statistical package (SPSS- X, SPSS, Chicago, Illinois; BMDP, University of California Press, Berkeley). Student’s t-test, two-way anal- ysis of variance, analysis of covariance, chi-square analy- sis, correlation analysis, and multiple logistic regression were used as indicated. Differences were considered sig- nificant at P values of less than 0.05. All values are ex- pressed as mean rt SD.
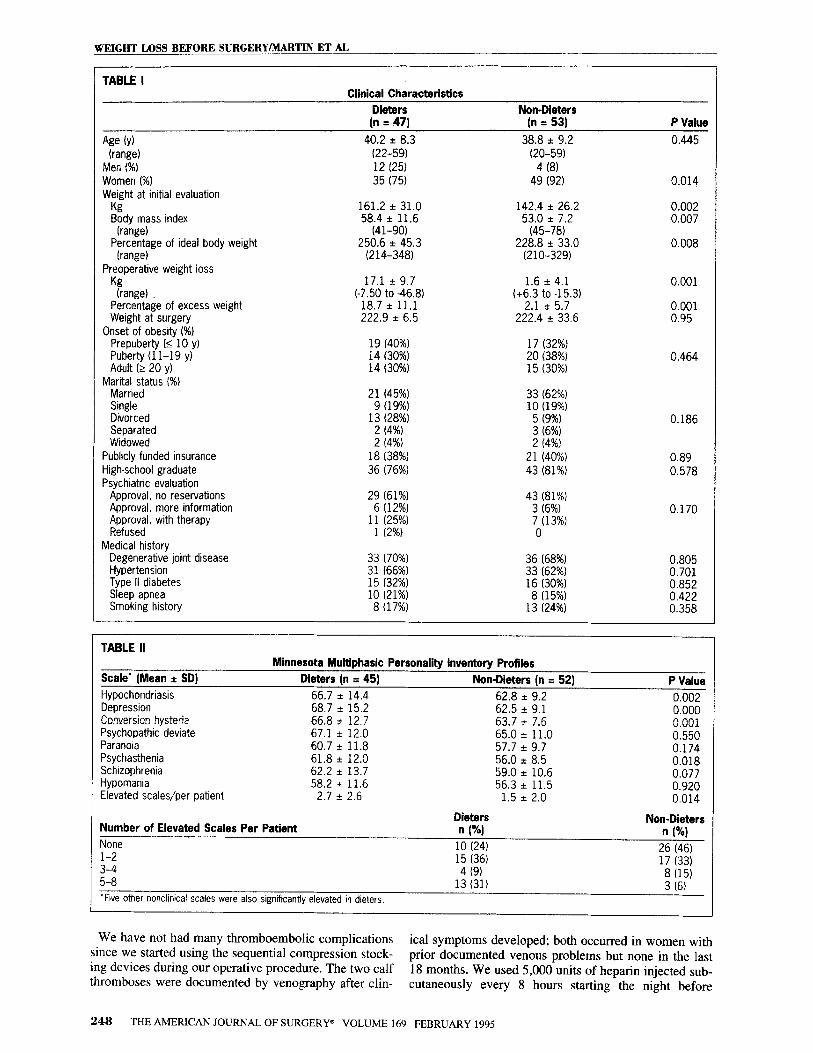
RESULTS The clinical characteristics of the 100 consecutive pa-
tients who proceeded with gastric bypass after completing our initial evaluation are listed in Table I. Forty-seven pa- tients met our criteria to be placed in the dieter group. Of the 53 patients who did not meet the criteria, only 9 pa-
tients lost more than 5 kg between the initial visit and their operation. Three of these patients lost between 7.5 kg and 10 kg during the first month of the PSMF but then began supplementing their liquid diet during the second and thud months with other food items while trying to decide when to proceed with surgery. They therefore stabilized at a new maintenance weight (the maximum weight loss was 15.3 kg) without further weight loss, were not ketotic at oper- ation, and were obviously not in a semifasted state at op- eration. Another 6 patients refused to diet for more than 14 days and lost less than 7.5 kg. We did not include these patients since this was less than a 5% decrease in weight for each of them.
The dieter and the nondieter groups are not perfectly matched. A significantly higher percentage of men suc- cessfully lost weight preoperatively. Fifteen of the 16 men attempted to diet and 11 were successful. The patients who successfully dieted were also significantly heavier initially, although by the operative date the patients in the dieter group had lost enough weight to match the nondieter group for mean percentage of IBW and BMI.
Table II presents personality data collected using the MMPI.23 All patients completed an MMPI; however, 3 pa- tients met criteria that made their test invalid.23 The dieter group exhibited several highly significant indicators sug- gesting more psychopathology. The mean score on all eight clinical scales was higher for the dieters (P co.05 by the sign test), with three of the scales having significantly higher means by the t-test. Additionally, there were sig- nificantly more patients in the dieter group who had patho- logically elevated MMPI (t score of 70 or greater) scores, The overall percentage of patients who fell into each of our psychiatric categories (Table I) after their psychiatric interviews also suggested that the dieter group had more psychopathology, although the chi-square analysis did not distinguish significant differences.
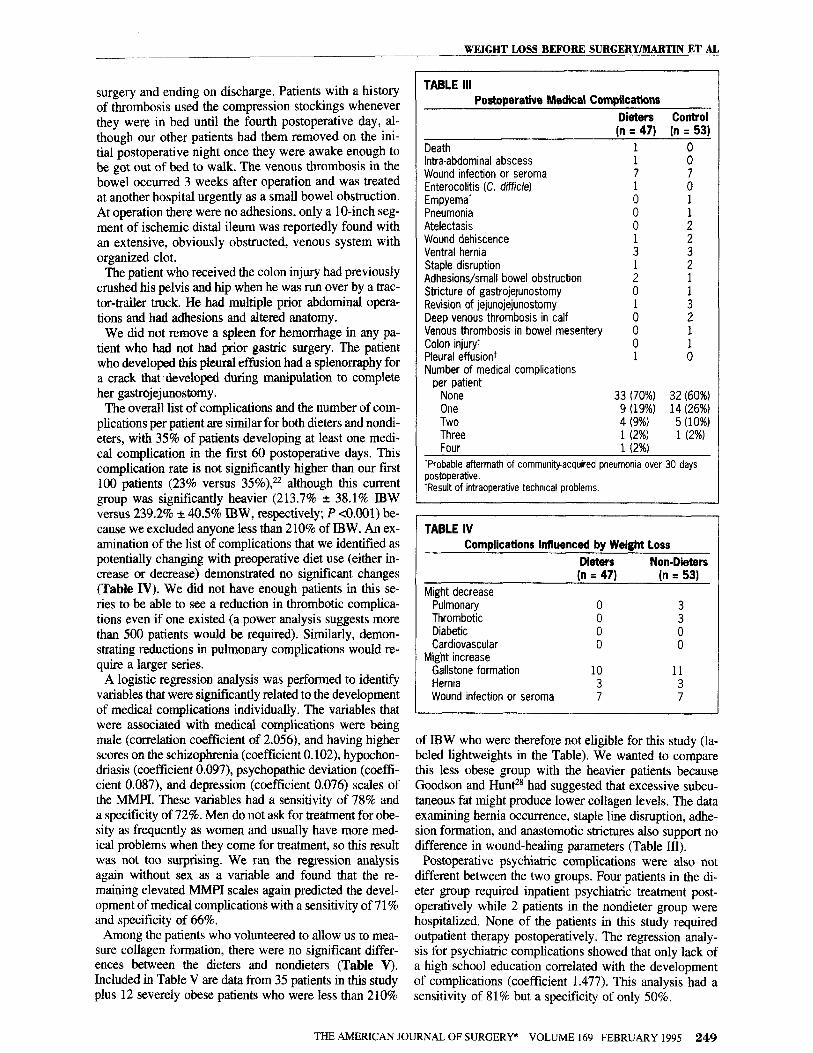
Table III lists the medical complications for dieters and nondieters. Several of the complications need some ex- planation Our wound infection seroma rate is high, but we count all wound separations in this category and in- form patients of this rate since even a minor alteration in surface wound healing disturbs our population. Almost all gastric bypass patients will have atelectasis on a postop- erative chest radiograph, which should be documented to help the hospital get a better reimbursement rate. The 2 patients in this series listed with this complication were both smokers who decreased their cigarette consumption preoperatively but had atelectasis that compromised their oxygenation and prolonged hospitalization for several days, requiring percussion and postural drainage treat- ments. The pneumonia also occurred in a smoker. There were fever, changes in sputum production, radiographic changes, and a positive culture for Staphylococcus aureus
from a sample with no epithelial cells, and a sheet of white blood cells with gram-positive cocci. Since our first studyz2. documented a significant association between smoking and postoperative complications, we warn patients of this association and make smoking cessation our number-one preoperative priority even above dieting (no patient we treated thought they could both stop smoking and diet pre- operatively, an assessment we agree with).
WEIGHT LOSS BEFORE SURGERY/MARTIN ET AL __ ._________-___-__ __-
THE AMERICAN JOURNAL OF SURGERY” VOLUME 169 FEBRUARY 1995 247
WEIGHT LOSS BEFORE SURGERY/MARTIN ET AL
TABLE I Clinical Characteristics
Dieters Non-Dieters
Age (Y)
(range) Men (%I Women (%I
W;$t at initial evaluation Body mass index
(range) Percentage of ideal body weight
(range) Preoperative weight loss
Kg (range)
Percentage of excess weight Weight at surgery
Onset of obesity (%I Prepuberty f< 10 y) Puberty (11-19 y) Adult (2 20 y)
Marital status (%I Married Single Divorced Separated Widowed
Publicly funded insurance High-school graduate Psychiatric evaluation
Approval, no reservations Approval, more information A$;p;;l, with therapy
Medical history Degenerative joint disease Hypertension Type II diabetes Sleep apnea Smoking history
(n = 47)
40.2 i 8.3 (22-59) 12 (25) 35 (75)
161.2 i 31.0 58.4 + 11.6
(41-90) 250.6 i 45.3
(214-348)
17.1 * 9.7 t;g t,” ;‘p$
222.9 2 6:5
19 (40%) 14 130%) 14 (30%)
21 (45%) 9 (19%)
13 (28%) 2 (4%) 2 (4%)
18 (38%) 36 (76%)
29 (61%) 6 (12%)
11 1 (2%) (25%)
33 (70%) ;; yp%;
10 (21%) 8 (17%)
(n = 53)
38.8 * 9.2 (20-59)
4 (8) 49 (92)
142.4 zt 26.2 53.0 zt 7.2
(45-78) 228.8 zt 33.0
1210-329)
1.6 i 4.1 “6.; ; -5l;.31 222.4 i 33.6
17 (32%) 20 (38%) 15 (30%)
;; I@$
5 (9%; 3 (6%) 2 14%)
21 (40%) 43 (81%)
43 (81%) 3 (6%) 7 0 (13%)
36 (68%) 33 (62%) 16 (30%) 8 (15%)
13 (24%)
P Value
0.445
0.014
0.002 0.007
0.008
0.001
0.001 0.95
0.464
0.186
0.89 0.578
0.170
0.805 0.701 0.852 0.422 0.358
TABLE ii
Scale’ (Mean t SD)
Hypochondriasis Depression Conversion hysteria Psychopathic deviate Paranoia Psychasthenia Schizophrenia Hypomania Elevated scales/per patient
Minnesota Muitiphasic Personality inventory Profiles Dieters (n = 45) Non-Dieters (n = 52)
66.7 + 14.4 62.8 e 9.2 68.7 zt 15.2 62.5 2 9.1 66.8 i 12.7 63.7 2 7.6 67.1 * 12.0 65.0 + 11.0 60.7 i 11.8 57.7 + 9.7 61.8 + 12.0 56.0 + 8.5 62.2 * 13.7 59.0 i 10.6 58.2 + 11.6 56.3 i 11.5
2.7 -c 2.6 1.5 32 2.0
P Value 0.002 0.000 0.001 0.550 0.174 0.018 0.077 0.920 0.014
I Dieters lumber of Elevated Scales Per Patient
Non-Dieters n I%1 n fYJ ~ I
None 10 (24) 5% IA&I l-2 3-4 5-8 ‘Five other nonclinical scales were also significantly elevated in dieters.
15 i36j 4 (9)
13 (31)
- ” > ‘V,
17 (33) 8 (15) 3 (6)
We have not had many thromboembolic complications since we started using the sequential compression stock-
ical symptoms developed; both occurred in women with
ing devices during our operative procedure. The two calf prior documented venous problems but none in the last
thromboses were documented by venography after clin- 18 months. We used 5,000 units of heparin injected sub- cutaneously every 8 hours starting the night before
248 THE AMERICAN JOURNAL OF SURGERY” VOLUME 169 FEBRUARY 1995
surgery and ending on discharge. Patients with a history of thrombosis used the compression stockings whenever they were in bed until the fourth postoperative day, al- though our other patients had them removed on the ini- tial postoperative night once they were awake enough to be got out of bed to walk. The venous thrombosis in the bowel occurred 3 weeks after operation and was treated at another hospital urgently as a small bowel obstruction. At operation there were no adhesions, only a lo-inch seg- ment of ischemic distal ileum was reportedly found with an extensive, obviously obstructed, venous system with organized clot.
The patient who received the colon injury had previously crushed his pelvis and hip when he was run over by a trac- tor-trailer truck. He had multiple prior abdominal opera- tions and had adhesions and altered anatomy.
We did not remove a spleen for hemorrhage in any pa- tient who had not had prior gastric surgery. The patient who developed this pleural effision had a splenormphy for a crack that developed during manipulation to complete her gastrojejunostomy.
The overall list of complications and the number of com- plications per patient are similar for both dieters and nondi- eters, with 35% of patients developing at least one medi- cal complication in the first 60 postoperative days. This complication rate is not significantly higher than our first 100 patients (23% versus 35%),” although this current group was significantly heavier (213.7% + 38.1% lBW versus 239.2% f 40.5% IBW, respectively; P ~0.001) be- cause we excluded anyone less than 210% of IBW. An ex- amination of the list of complications that we identified as potentially changing with preoperative diet use (either in- crease or decrease) demonstrated no significant changes (Table IV). We did not have enough patients in this se- ries to be able to see a reduction in thrombotic complica- tions even if one existed (a power analysis suggests more than 500 patients would be required). Similarly, demon- strating reductions in pulmonary complications would re- quire a larger series.
A logistic regression analysis was performed to identify variables that were significantly related to the development of medical complications individually. The variables that were associated with medical complications were being male (correlation coefficient of 2.056) and having higher scores on the schizophrenia (coefficient 0.102), hypochon- driasis (coefficient 0.097), psychopathic deviation (coeffi- cient 0.087), and depression (coefficient 0.076) scales of the MMPI. These variables had a sensitivity of 78% and a specificity of 72%. Men do not ask for treatment for obe- sity as frequently as women and usually have more med- ical problems when they come for treatment, so this result was not too surprising. We ran the regression analysis again without sex as a variable and found that the re- maining elevated MMPI scales again predicted the devel- opment of medical complications with a sensitivity of 71% and specificity of 66%.
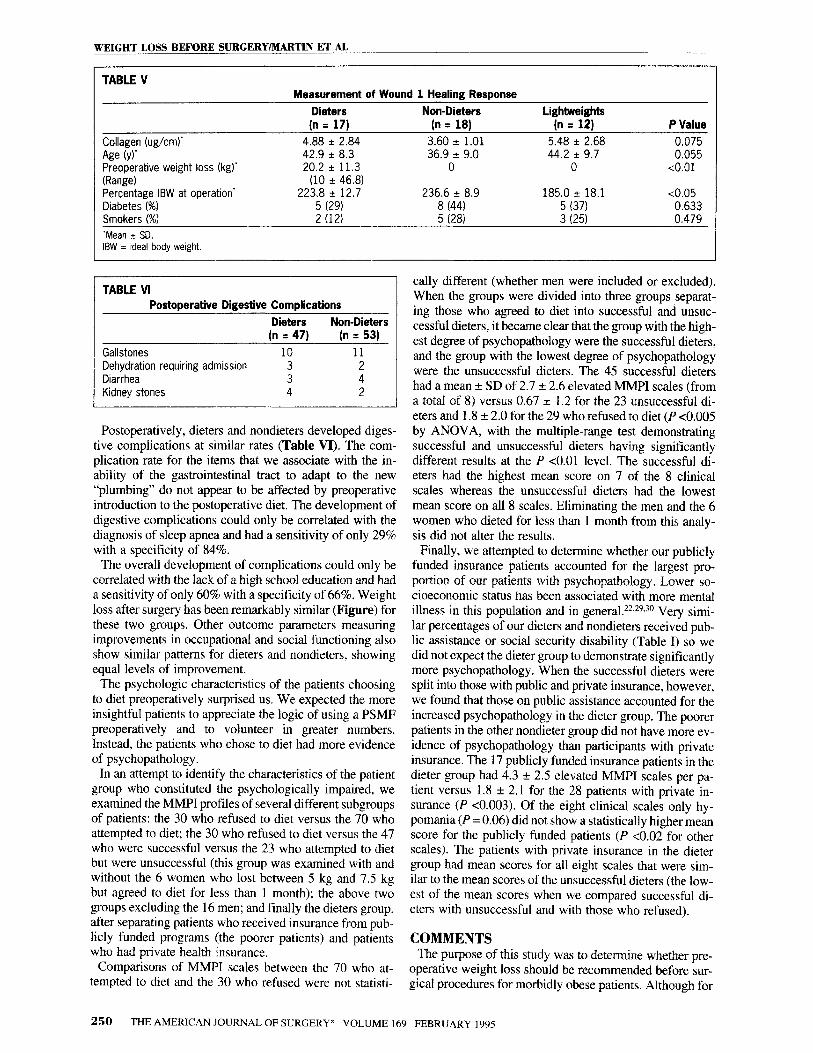
Among the patients who volunteered to allow us to mea- sure collagen formation, there were no significant differ- ences between the dieters and nondieters @able V). Included in Table V are data from 35 patients in this study plus 12 severely obese patients who were less than 210%
TABLE Ill Postoperative Medical Complications
Dieters Control (n = 47) (n = 53)
Death 1
Intra-abdominal abscess 1 Fi Wound infection or seroma 7 Enterocolitis (C. difficle) 1 : Empyema’ Pneumonia E ; Atelectasis 0 2 Wound dehiscence Ventral hernia i ; Staple disruption
: 2
Adhesions/small bowel obstruction 1 Stricture of gastrojejunostomy 0 Revision of jejunojejunostomy Deep venous thrombosis in calf :,
: 2
Venous thrombosis in bowel mesentery Colon injury+ i
1
Aeural effusion+ 1 :, Number of medical complications
per patient None 33 (70%) 32 (60%) One 9 (19%) 14 (26%) Two 4 (9%) 5 (10%) Three 1 (2%) 1 (2%) Four 1 (2%)
‘Probable aftermath of community-acquired pneumonia over 30 days postoperative. +Result of intraoperative technical problems.
WEIGHT LOSS BEFORE SURGERY/MARTIN ET AL ______
TABLE IV Complications Influenced by Weight Loss
Dieters Non-Dieters (n = 471 In = 531
Might decrease Pulmonary 0 3 Thrombotic Diabetic :: i Cardiovascular 0 0
Might increase Gallstone formation 10 11
Hernia 3 3 Wound infection or seroma 7 7
of IBW who were therefore not eligible for this study (la- beled lightweights in the Table). We wanted to compare this less obese group with the heavier patients because Goodson and Hur@ had suggested that excessive subcu- taneous fat might produce lower collagen levels. The data examining hernia occurrence, staple line disruption, adhe- sion formation, and anastomotic strictures also support no difference in wound-healing parameters (Table III).
Postoperative psychiatric complications were also not different between the two groups. Four patients in the di- eter group required inpatient psychiatric treatment post- operatively while 2 patients in the nondieter group were hospitalized. None of the patients in this study required outpatient therapy postoperatively. The regression analy- sis for psychiatric complications showed that only lack of a high school education correlated with the development of complications (coefficient 1.477). This analysis had a sensitivity of 8 1% but a specificity of only 50%.
THE AMERICAN JOURNAL OF SURGERY@ VOLUME 169 FEBRUARY 1995 249
WEIGHT LOSS BEFORE SURGERYMARTIN ET AL
TABLE V Measurement of Wound 1 Healing Response
Collagen (ug/cm)’ Age (~1’ Preoperative weight loss (kg)’ (Range) Percentage IBW at operation’ Diabetes (%I Smokers (%I ‘Mean * SD. IBW = Ideal body weight.
Dieters (n = 17)
4.88 r 2.84 42.9 r 8.3 20.2 * 11.3
(10 + 46.8) 223.8 zt 12.7
5 (29) 2 (12)
Non-Dieters Lightweights (n = 18) (n = 12)
3.60 zt 1.01 5.48 i 2.68 36.9 2 9.0 44.2 i 9.7
0 0
236.6 + 8.9 185.0 * 18.1 8 (44) 5 (37) 5 (28) 3 (25)
P Value
0.075 0.055
<O.Ol
<0.05 0.633 0.479
TABLE VI Postoperative Digestive Complications
Dieters Non-Dieters (n q 47) (n = 53)
Gallstones 10 11 Dehydration requiring admission 3 2 Diarrhea 3 4 Kidney stones 4 2
Postoperatively, dieters and nondieters developed diges- tive complications at similar rates (Table VI). The com- plication rate for the items that we associate with the in- ability of the gastrointestinal tract to adapt to the new “plumbing” do not appear to be affected by preoperative introduction to the postoperative diet. The development of digestive complications could only be correlated with the diagnosis of sleep apnea and had a sensitivity of only 29% with a specificity of 84%.
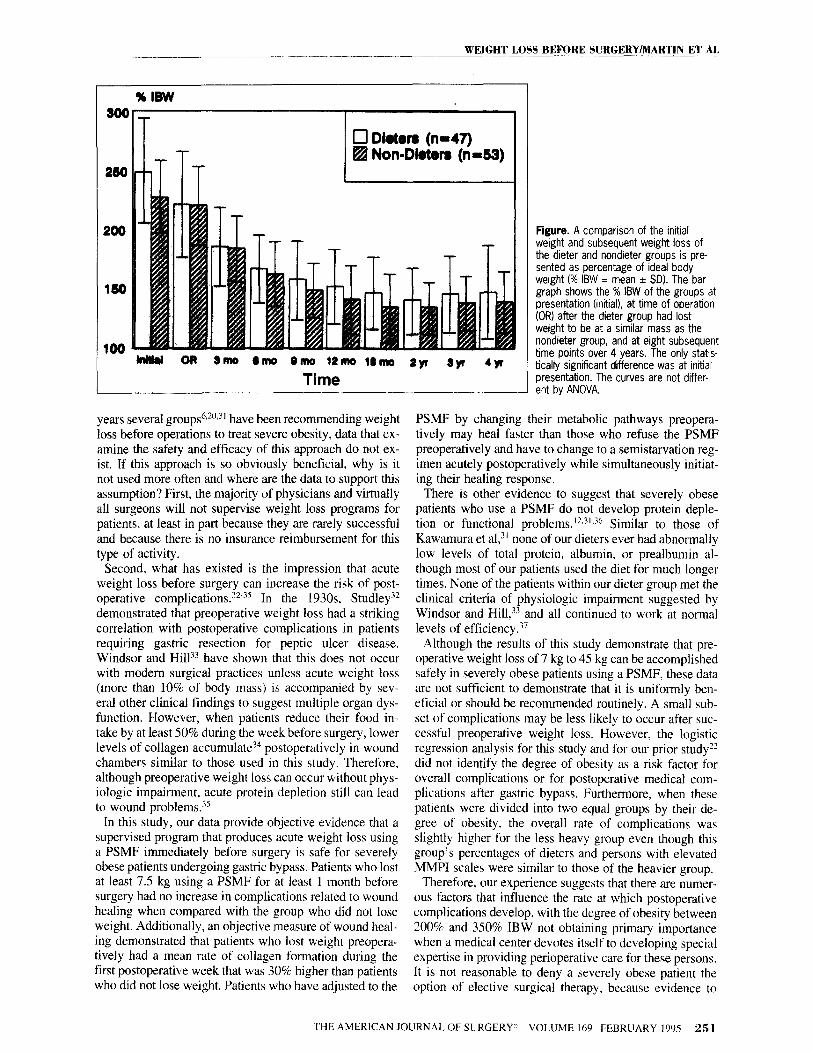
The overall development of complications could only be correlated with the lack of a high school education and had a sensitivity of only 60% with a specificity of 66%. Weight loss after surgery has been remarkably similar (Figure) for these two groups. Other outcome parameters measuring improvements in occupational and social functioning also show similar patterns for dieters and nondieters. showing equal levels of improvement.
The psychologic characteristics of the patients choosing to diet preoperatively surprised us. We expected the more insightful patients to appreciate the logic of using a PSMF preoperatively and to volunteer in greater numbers. Instead, the patients who chose to diet had more evidence of psychopathology.
In an attempt to identify the characteristics of the patient group who constituted the psychologically impaired, we examined the MMPI profiles of several different subgroups of patients: the 30 who refused to diet versus the 70 who attempted to diet; the 30 who refused to diet versus the 47 who were successful versus the 23 who attempted to diet but were unsuccessful (this group was examined with and without the 6 women who lost between 5 kg and 7.5 kg but agreed to diet for less than 1 month); the above two groups excluding the 16 men; and finally the dieters group. after separating patients who received insurance from pub- licly funded programs (the poorer patients) and patients who had private health insurance.
Comparisons of MMPI scales between the 70 who at- tempted to diet and the 30 who refused were not statisti-
tally different (whether men were included or excluded). When the groups were divided into three groups separat- ing those who agreed to diet into successful and unsuc- cessful dieters, it became clear that the group with the high- est degree of psychopathology were the successful dieters, and the group with the lowest degree of psychopathology were the unsuccessful dieters. The 45 successful dieters had a mean + SD of 2.7 2 2.6 elevated MMPI scales (from a total of 8) versus 0.67 f 1.2 for the 23 unsuccessful di- eters and 1.8 + 2.0 for the 29 who refused to diet (P co.005 by ANOVA, with the multiple-range test demonstrating successful and unsuccessful dieters having significantly different results at the P co.01 level. The successful di- eters had the highest mean score on 7 of the 8 clinical scales whereas the unsuccessful dieters had the lowest mean score on all 8 scales. Eliminating the men and the 6 women who dieted for less than 1 month from this analy- sis did not alter the results. Finally, we attempted to determine whether our publicly
funded insurance patients accounted for the largest pro- portion of our patients with psychopathology. Lower so- cioeconomic status has been associated with more mental illness in this population and in general.22,29J0 Very simi- lar percentages of our dieters and nondieters received pub- lic assistance or social security disability (Table I) so we did not expect the dieter group to demonstrate significantly more psychopathology. When the successful dieters were split into those with public and private insurance, however, we found that those on public assistance accounted for the increased psychopathology in the dieter group. The poorer patients in the other nondieter group did not have more ev- idence of psychopathology than participants with private insurance. The 17 publicly funded insurance patients in the dieter group had 4.3 5 2.5 elevated MMPI scales per pa- tient versus 1.8 + 2.1 for the 28 patients with private in- surance (P <0.003). Of the eight clinical scales only hy- pomania (P = 0.06) did not show a statistically higher mean score for the publicly funded patients (P co.02 for other scales). The patients with private insurance in the dieter group had mean scores for all eight scales that were sim- ilar to the mean scores of the unsuccessful dieters (the low- est of the mean scores when we compared successful di- eters with unsuccessful and with those who refused).
COMMENTS The purpose of this study was to determine whether pre-
operative weight loss should be recommended before sur- gical procedures for morbidly obese patients. Although for
250 THE AMERICAN JOURNAL OF SURGERYe VOLUME 169 FEBRUARY 1995
WEIGHT LOSS BEFORE SI;RGERYlMARTIN ET AL __~---
100 w OR smo 6mo orno 14mo lbmo 4yr syt 4yr
Time
years several groups h~20,31 have been recommending weight loss before operations to treat severe obesity, data that ex- amine the safety and efficacy of this approach do not ex- ist. If this approach is so obviously beneficial, why is it not used more often and where are the data to support this assumption? First, the majority of physicians and virtually all surgeons will not supervise weight loss programs for patients, at least in part because they are rarely successful and because there is no insurance reimbursement for this type of activity.
Second, what has existed is the impression that acute weight loss before surgery can increase the risk of post- operative complications.“2-‘5 In the 1930s Studley”? demonstrated that preoperative weight loss had a striking correlation with postoperative complications in patients requiring gastric resection for peptic ulcer disease. Windsor and Hill”” have shown that this does not occur with modern surgical practices unless acute weight loss (more than 10% of body mass) is accompanied by sev- eral other clinical findings to suggest multiple organ dys- function. However, when patients reduce their food in- take by at least 50% during the week before surgery, lower levels of collagen accumulate34 postoperatively in wound chambers similar to those used in this study. Therefore, although preoperative weight loss can occur without phys- iologic impairment, acute protein depletion still can lead to wound problems.“”
In this study, our data provide objective evidence that a supervised program that produces acute weight loss using a PSMF immediately before surgery is safe for severely obese patients undergoing gastric bypass. Patients who lost at least 7.5 kg using a PSMF for at least 1 month before surgery had no increase in complications related to wound healing when compared with the group who did not lose weight. Additionally, an objective measure of wound heal- ing demonstrated that patients who lost weight preopera- tively had a mean rate of collagen formation during the first postoperative week that was 30% higher than patients who did not lose weight. Patients who have adjusted to the
Figure. A comparison of the initial weight and subsequent weight loss of the dieter and nondieter groups is pre- sented as percentage of ideal body weight f% IBW = mean * SD). The bar graph shows the % IBW of the groups at presentation (initial), at time of operation (OR) after the dieter group had lost weight to be at a similar mass as the nondieter group, and at eight subsequent time points over 4 years. The only statis- tically significant difference was at initial presentation. The curves are not differ- ent by ANOVA.
PSMF by changing their metabolic pathways preopera- tively may heal faster than those who refuse the PSMF preoperatively and have to change to a semistarvation reg- imen acutely postoperatively while simultaneously initiat- ing their healing response.
There is other evidence to suggest that severely obese patients who use a PSMP do not develop protein deple- tion or functional problems.11J’J6 Similar to those of Kawamura et a13’ none of our dieters ever had abnormally low levels of total protein, albumin, or prealbumin al- though most of our patients used the diet for much longer times. None of the patients within our dieter group met the clinical criteria of physiologic impairment suggested by Windsor and Hill,“” and all continued to work at normal levels of efficiency.” Although the results of this study demonstrate that pre-
operative weight loss of 7 kg to 45 kg can be accomplished safely in severely obese patients using a PSMF, these data are not sufficient to demonstrate that it is uniformly ben- eficial or should be recommended routinely. A small sub- set of complications may be less likely to occur after suc- cessful preoperative weight loss. However, the logistic regression analysis for this study and for our prior study?? did not identify the degree of obesity as a risk factor for overall complications or for postoperative medical com- plications after gastric bypass. Furthermore, when these patients were divided into two equal groups by their de- gree of obesity, the overall rate of complications was slightly higher for the less heavy group even though this group’s percentages of dieters and persons with elevated MMPI scales were similar to those of the heavier group.
Therefore, our experience suggests that there are numer- ous factors that influence the raie at which postoperative complications develop, with the degree of obesity between 200% and 350% IBW not obtaining primary importance when a medical center devotes itself to developing special expertise in providing perioperative care for these persons. It is not reasonable to deny a severely obese patient the option of elective surgical therapy, because evidence to
THE AMERlCAN JOURNAL OF SURGERY” VOLUME 169 FEBRUARY 1995 25 1

WEIGHT LOSS BEFORE SURGERY/MARTIN ET AL - ___- --
suggest that obesity is a major risk for surgical complica- tions is insufficient.h
On the other hand, the public, businesses, and govem- ment agencies now want access to surgeons’ procedure- specific outcome results even though the data currently be- ing collected are not severity adjusted for comorbidities.8 For joint replacement procedures, there are data to suggest that patients who are 185% of IBW or higher incur a sig- nificantly longer length of stay and higher charges than less obese patients7 Surgeons treating a higher proportion of severely obese patients, therefore, might have worse out- comes for length of stay and hospital charges than those treating only less heavy patients. Surgeons need to care- fully determine which comorbidities influence outcomes’ and which preoperative strategies can be used to success- fully improve outcomes for various comorbid conditions, especially since unsuccessful outcomes may limit partici- pation in various programs.‘8 We also do not want to need- lessly discriminate against obese patients by refusing them necessary procedures if we find that weight loss does not change morbidity rates.
We used an outpatient approach” to reducing weight, in- cluding a liquid diet product and behavior modification ad- vice, that is very similar to currently available programs from companies such as Sandoz Nutrition Corporation, Health Management Resources, and Ross Laboratories. These companies contract to provide services to physician- supervised multispecialty groups. These programs are widely available, and collaborative relationships could be established by surgeons to help obese patients requiring operations to lose weight without the surgeons having to develop expertise in weight loss management.
Not all our patients were willing to pursue diet therapy preoperatively and not all who attempted to diet were suc- cessful. Any researcher trying to answer the question whether diet will decrease complications needs to re- member that the patients attracted to this option in our study had more evidence of psychopathology, especially in the patient population dependent on the Medicaid and Medicare programs. Patients with psychopathology have the highest risk of postoperative complications after gas- tric bypass using logistic regression analysis,‘2 so if they are overrepresented in one treatment group they can in- fluence outcome. Although surgeons have not routinely correlated preoperative evidence of psychopathology with postoperative outcomes, our evidence and that of Frasure- Smith and coworkers,“” who demonstrated that the pres- ence of depression following myocardial infarct directly affects survival over the next 6 months, suggest that psy- chological conditions should be included in severity-ad- justed mortality and morbidity data.
We still do not have a very complete understanding of why patients choose certain treatments and how that in- fluences our treatment outcomes,38.40 but it is important for surgeons to remember that “patients tend to be more averse to risks than physicians.“38 Our experience using a PSMF and a limited amount of behavioral modification suggests that a group of poorer patients with evidence of psy- chopathology use the preoperative period to confront a range of behaviors that are self-defeating, responding to suggestions from the behavioral modification program.
Doing so reduces their anxiety and may make them better surgical candidates.
Proving that a preoperative weight loss program will improve outcomes-especially since it will increase costs-will require randomized prospective trials of PSMF and behavior modification with patients needing specific procedures who agree to attempt such a program. We found that patients who dieted for at least 1 month and lost at least 7.5 kg began to make lifestyle changes that potentially helped them to adjust to the new postop- erative behaviors that a gastric bypass require. Our ex- perience in conducting this study has convinced us that severely obese patients can safely lose up to 45 kg im- mediately preoperatively, that commercial PSMF pro- grams help make this amount of weight loss feasible, and that losing weight may help improve the outcome of some procedures (especially regarding length of hospital stay and costs) for severely obese patients who complete a preoperative weight loss program.
REFERENCES I. Kuczmarski RJ. Prevalence of overweight and weight gain in the United States. Am J Clin Nutr. 1992;(suppl):495S-502s. 2. 1983 Metropolitan height and weight tables. Stat Bull Merropol Lije Ins Coo. 1984;64:2-9. 3. SjBstriim LV. Morbidity of severely obese subjects. Am J Clin Nutr. 1992;55:5088-5158. 4. SjGstr6m LV. Mortality of severely obese subjects. Am J Clin Nutr. 1992;55:516S-5238. 5. Prem KA, Mensheha NM, McKelvey JL. Operative treatment of adenocaxinoma of the endometrium in obese women. Am .I Obscet Cynecul. 1965;92: 16-22. 6. Pasulka PS, Bistrian RR, Benotti PN, Blackbum GL. The risk of surgery in obese patients. Ann Intern Med. 1986;104:540-546. 7. Epstein AM, Read JL, Hoefer M. The relationship of body weight to length of stay and charges for hospital services for patients un- dergoing elective surgery: a study of two procedures. Am J Pub Health. 1987;77:993-997. 8. Winslow R. State rates heart surgeons by mortality. Wall Street Journal, November 20, 1992;Bl. BIO. 9. Greenfield S, Aronow HV, Elashoff RM, Watanabe D. Flaws in mortality data. The hazards of ignoring comorbid disease. JAMA. 1988;260:2253-2255. 10. Wadden TA, Van Itallie TB. Blackbum GL. Responsible and ir- responsible use of very-low-calorie diets in the treatment of obesity. JAMA. 1990;263:83-85. 11. Vertes V, Genuth SM, Hazelton IM. Supplemented fasting as a large scale outpatient program. JAMA. 1977;238:2152-2153. 12. Hoffer LJ, Bistrian BR, Young VR, et al. Metabolic effects of very low calorie weight reduction diets. J CIin Invesr. 1984;73: 750-758. 13. Eliahou HFE, Iaina A, Goant L, et al. Body weight reduction necessary to attain normotension in the overweight hypertensive pa- tient. Int J Obes. 1981;5:157-163. 14. Reisin E, Frohlich ED, Messerli FH. et al. Cardiovascular changes after weight reduction in obesity hypertension. Ann Intern Med. 1983;98:315-319, 15. Batist G, Bothe A Jr, Bern M, et al. Low antithrombin III in mor- bid obesity: return to normal with weight reduction. JP.&V. 1983;7: 447-449. 16. Grace CS. Fibrinolysis and obesity: the effect of weight reduc- tion. Austral Ann Med. 1969;18:32-35. 17. Thomas PS, Owen ERTC, Hulands G, Milledge JS. Respiratory function in the morbidly obese before and after weight loss. Thorax. 1989;44:382-386.
252 THE AMERICAN JOURNAL OF SURGERY i VOLUME 169 FEBRUARY 1995

WEIGHT LOSS BEFORE~~IJRGERY/MARTIN ET AL
18. Catenacci AJ, Anderson JD, Boersma D. Anesthetic hazards of obesity. JAMA. 1961;175:111-119. 19. The Facts About Weight Lass Products and Programs. Federal
Trade Commission, Food and Drug Administration, and National Association of Attorneys General. DHHS Publication No. (FDA) 92-l 189. 20. Task Force of the American Society for Clinical Nutrition. Guidelines for surgery for morbid obesity. Am J Clin Nutr. 1985;42: 904405. 21. Wadden TA, Bell ST. Obesity. In: Bellack AS, Hersen M, Kazdin AE, eds. International Handbook of Behavioral ModrjTcation and Therapy. New York: Plenum Press; 1990:449-473. 22. Martin LF, Tan TL, Holmes PA, et al. Preoperative insurance status influences postoperative complication rates for gastric bypass. Am J Surg. 1991;161:625-634. 23. Hathaway SR, McKinley JC. Minnesota Multiphasic Personality
Inventory Manual. New York: The Psychological Corporation; 1967. 24. Goodson WH III, Hunt TK. Development of a new miniature method of the study of wound healing in human subjects. J Surg Res.
1982;33:394-401. 25. Viljanto J. Biochemical basis of tensile strength in wound heal- ing: an experimental study with viscose cellulose sponges in rats. Acta Chir Sca-nd. 1964;33(suppl): 1101. 26. Broomfield PH, Chopra R, Scheinbaum RC, et al. Effects of ur- sodeoxycholic acid and aspirin on the formation of lithogenic bile and gallstones during weight loss. NEJM. 1988;319: 1567-1572. 27. Liddle RA, Goldstein RB, Saxon J. Gallstone formation during weight reduction dieting. Arch Intern Med. 1989;149: 1750-I 753. 28. Goodson WH III, Hunt TK. Wound collagen accumulation in obese hyperglycemic mice. Diabetes. 1986;33:491-495.
29. Hollingshead AB, Redlich FC. Social Class and Mental Illness.
New York: Wiley & Sons; 1958:387-397. 30. Dohrenwend BP, Levav I, Shrout PE, et al. Socioeconomic sta- tus and psychiatric disorders: the causation-selection issue. Science.
1992;255:94&95 1. 31. Kawamura I, Chen CC, Yamazaki K, et al. A clinical study of protein sparing modified fast (PSMF) administered preoperatively to morbidly obese patients: comparison of PSMF with natural food products to originally prepared PSMF. Obes Surg. 1992;2:33-40. 32. Studley HO. Percentage of weight loss. A basic indicator of sur- gical risk in patients with chronic peptic ulcer. JAMA. 1936;106: 458-460. 33. Windsor JA, Hill GL. Weight loss with physiologic impairment: a basic indication of surgical risk. Ann Surg. 1988;207:29@-296. 34. Windsor JA, Knight GS, Hill GL. Wound-healing response in surgical patients: recent food intake is more important than nutri- tional status. Br J Surg. 1988;75: 13% 137. 35. Windsor JA. Underweight patients and the risks of major surgery. World JSurg. 1993;17:165-172. 36. Fisler JS, Kaptein EM, Drenick El, et al. Metabolic and hor- monal factors as predictors of nitrogen retention in obese men con- suming very low calorie diets. Metabolism. 1985;34:101-105. 37. Taylor HL, Keys A. Criteria for fitness and comments on nega- tive nitrogen balance. Ann NY Acad Sri. 1958;73:465-475. 38. Wennberg JE. Outcomes research, cost containment, and the fear of health care rationing. NEYM. 1990;323: 1202-1204. 39. Frasure-Smith N, Lesperance F, Talajic M. Depression follow- ing myocardial infarction. Impact on six-month survival. JAMA.
1993;270:1819-1825. 40. Wennberg JE. Which rate is right? NEJM 1986;3 14:3 10-311.
THE AMERICAN JOURNAL OF SURGERY* VOLUME 169 FEBRUARY 1995 253