bullying and suicide. a review
TRANSCRIPT

©Freund Publishing House Ltd. Int J Adolesc Med Health 2008;20(2):133-154
Bullying and suicide. A review Young Shin Kim, MD, MS, MPH, PhD and Bennett Leventhal, MD
2.3
1Child Study Center, Yale University School of Medicine, New Haven, CT;
2Center
for Child Mental Health and Developmental Neuroscience Institute for Juvenile Research; and
3Institute for Juvenile Research, University of Illinois College of
Medicine, Chicago, IL; United States of America
Abstract: Being a victim or perpetrator of school bullying, the most common type of school violence,
has been frequently associated with a broad spectrum of behavioral, emotional, and social problems.
Suicide is third leading cause of mortality in children and adolescent in the United States of America
and around the world. This paper provides a systematic review of the previous 37 studies conducted
in children and adolescents from communities, as well as in special populations that examined the
association between bullying experiences and suicide, with an emphasis on the strengths and
limitations of the study designs. Despite methodological and other differences and limitations, it is
increasingly clear that any participation in bullying increases the risk of suicidal ideations and/or
behaviors in a broad spectrum of youth.
Keywords: Bullying, school, suicide
Correspondence: Assistant Professor Young Shin Kim, MD, PhD, Child Study Center, Yale University
School of Medicine, 230 S Frontage Rd, POBox 207900, New Haven, CT 06520-7900 United States. Tel:
203-785-2198; Fax: 203-785-7402; E-mail: [email protected]
Submitted: January 01, 2008. Revised: January 16, 2008. Accepted: January 17, 2008.
INTRODUCTION
Bullying is an aggressive behavior in which
individuals in a dominant position intend to
cause mental and/or physical suffering to
others (1). Bullying is a serious public health
problem, with the international prevalence
ranging from 9% to 54% (2-4). All
participants in bullying are reported to be at
substantially increased risk for significant
mental and/or physical sequelae of bullying.
Victimized children are reported to have a
myriad of clinical problems, including bed
wetting, sleep difficulties, anxiety, depres-
sion, school phobia, feelings of insecurity,
and unhappiness at school; they may also
have low self-esteem, loneliness, isolation,
and somatic symptoms (5-12). In contrast,
perpetrators of bullying are reported to have
more depression and are more likely than are
their peers to be involved with antisocial
behaviors and legal problems later in adult-
hood (10,13). Victim-perpetrators, (aggressive
victims) are considered a distinct subtype of
school bullying, experiencing more psycho-
pathology, as well as problematic family and
educational profiles that differ from the other
two school bullying subtypes (14).
Suicide, the third leading cause of
mortality for adolescents in the United
States of America (US) and around the
world, is one of the most serious symptoms
of psychopathology (15). For example, a
recent, large scale, epidemiologic study in
the US suggested that in the past year, 19%
of high school students had serious suicidal
ideation, 15% made a specific plan to
BULLYING AND SUICIDE 134
attempt suicide, 8.8% reported suicidal
attempts, and 2.6% made a suicide attempt
that was serious enough to require significant
medical attention (16). Similarly, a 2001
Korean study found that the rate of com-
pleted suicides for adolescents (from 11 to
19 years) was 15.5 per 100,000, making
suicide the third leading cause of death, after
car accidents and cancer (17). For children at
greater risk for suicide, perceived peer rejec-
tion, being bullied, and being perpetrators of
bullying were associated, directly and
indirectly, with major depression, substance
use, and antisocial behavior with severe
suicidal ideation (18-20).
The goals of this review paper were (1)
to provide a systematic review of previous
studies that examined the association
between bullying experiences and suicide,
with an emphasis on the strengths and
limitations of the study designs; and (2) to
shed light on directions for future research.
METHODS
Identification of relevant literature
A literature search was carried out using six
databases, without date specification: Web
of Science, SCOPUS, EMBASE, PubMed,
PsychInfo, and Ovid Medline. The search
terminology included the following:
1. bullying included either bully*, peer
victimization, peer aggression,
relational aggression, peer relation,
school violence, school aggression,
social dominant*, social hierarchy* or
peer abuse; and
2. suicide included either suicide, suicide
attempt, suicide ideation, suicide
behavior, self-harm or self-injurious
behavior.
The subsequent literature search resulted in
867 papers, which was narrowed to 103
relevant papers by further review of the
abstracts. Among the 103 papers, 37 papers
that met our inclusion criteria (below) were
finally selected for this review paper.
Inclusion criteria
Studies were included in the review if they
met the following criteria:
1. the age of study participants is
younger than or equal to high school
students in the general population and
all age ranges in special populations,
including populations with develop-
mental disorders, behavioral disorders,
of homosexual and/or bi-sexual
orientation or at detention centers;
2. the statistical methods were described
so that the appropriateness of the
analyses could be evaluated;
3. quantitative research that provided
numerical data regarding bullying/
peer victimization exposure and suicidal
risks;
4. the measures for bullying or peer
victimization were described; and,
5. the measures of suicidal behaviors,
ideations or self-injurious behaviors
were described.
Exclusion criteria
Studies were excluded in the review when:
(1) no quantitative data were provided; or
(2) suicidal risks were not compared between
bullying and non-bullying groups.
Grouping of studies
The studies were grouped according to the
characteristics of the study population:
(1) children and adolescents of the general
population; and, (2) a special population,
including people with Asperger Disorder
(AD), Learning Disorders (LD), behavioral
disorders, homosexual and/or bisexual
orientation, or at detention centers. Within
each group, suicidal risks were categorized
by the types of suicidality: (1) suicidal
ideation including suicidal thoughts and

YS KIM AND B LEVENTHAL 135
suicidal plans; (2) suicidal attempts, including
suicidal behaviors and self-injurious/self-
harm behaviors; and, (3) a composite
variable of any suicidality.
Summary of findings
Because this review paper aims to provide a
systematic review of the previous studies
that investigated the association between
bullying experience and suicide risks rather
than to create a statistical summary of
suicidal risks in people with bullying
experience, the authors did not perform a
meta-analysis.
The authors selected odds ratios (ORs)
with 95% confidence intervals (CIs) for
presenting suicidal risks in the summary
tables because (1) ORs are the most
common risk ratios researchers used in their
original studies; (2) ORs are conceptually
intuitive to understand for most readers;
and, (3) Suicidal risks represented by ORs
can be easily translated into clinical practice
for the children and/or their families. In
those instances when ORs were not
available, the statistical method and findings
that were used in individual research were
noted in footnotes.
In examining the relations between
bullying and suicidality, adjustments must
be made for several confounding factors.
These factors include: (1) gender; (2)
psychopathology (depression, aggressive-
impulsive behaviors and disruptive
behaviors); (3) a history of suicide; (4)
parental divorce; and (5) sociodemographic
disadvantage. In this review, covariates that
were controlled in the analyses to examine
the relations between bullying experience
and suicide were examined and listed in the
summary tables.
RESULTS
The nature of the studies
The search strategy identified 37 studies as
eligible for inclusion in this review. Two
reports included separate results for either
subgroup of study sample (23) or same
sample (26,28). These two studies were
reviewed separately under the same author
list.
Researchers from 16 countries in 5
continents have conducted research on the
bullying and suicide. Approximately one
half of the studies were conducted in the
US, one third in Europe, and the rest in
Australia, South Korea, Japan, South
Africa, and Canada. Of the 17 US studies
(53%), 9 used data from the Youth Risk
Behavior Survey (YRBS). To monitor
priority health-risk behaviors among youth
and young adults, Center for Disease
Control (CDC) developed the Youth Risk
Behavior Surveillance System (YRBSS)
(21). YRBSS includes national, state, and
local school-based surveys of students in
grades 9–12 that have been conducted
biennially since 1991. YRBS is based on
data from these ongoing YRBSS surveys.
All 37 studies were cross-sectional
surveys. Of these studies, 73% were
conducted in children and adolescents in
their communities; the rest were performed
in special populations, such as populations
with developmental disorders (AD and
LD), drug problems, legal problems, and
homosexual or bisexual orientations (see
table 1.)
Measurement of predictors: Bullying
Ninety-two percent of research measured
bullying using self-report: 5% (two studies)
(22, 23) used peer nomination to identify
bullying and another 3% (one study) of
research interviewed children with Kiddie-
Schedule for Affective Disorders and
Schizophrenia-Present and Lifetime (K-
SADS-PL) (24) to identify bullying
experience in the study populations (see
table 2.) The time-frame of the bullying
BULLYING AND SUICIDE 136
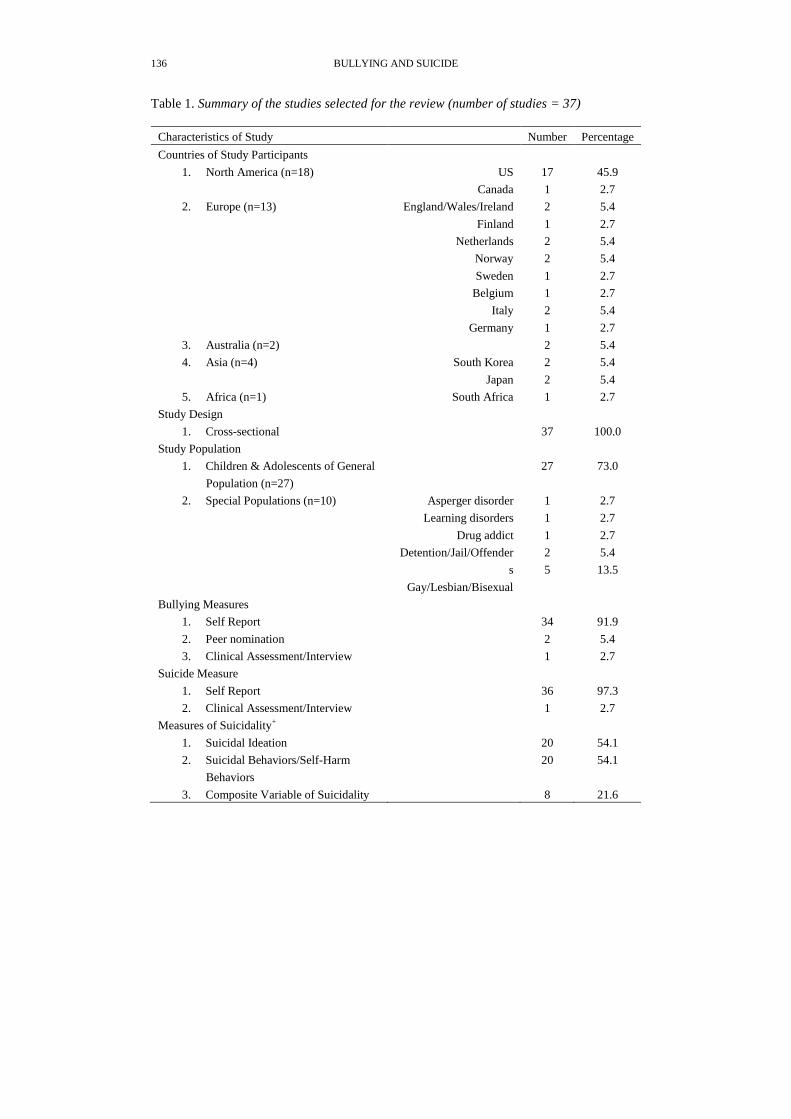
Table 1. Summary of the studies selected for the review (number of studies = 37)
Characteristics of Study Number Percentage
Countries of Study Participants
1. North America (n=18)
US
Canada
17
1
45.9
2.7
2. Europe (n=13)
England/Wales/Ireland
Finland
Netherlands
Norway
Sweden
Belgium
Italy
Germany
2
1
2
2
1
1
2
1
5.4
2.7
5.4
5.4
2.7
2.7
5.4
2.7
3. Australia (n=2) 2 5.4
4. Asia (n=4)
South Korea
Japan
2
2
5.4
5.4
5. Africa (n=1) South Africa 1 2.7
Study Design
1. Cross-sectional 37 100.0
Study Population
1. Children & Adolescents of General
Population (n=27)
27 73.0
2. Special Populations (n=10)
Asperger disorder
Learning disorders
Drug addict
Detention/Jail/Offender
s
Gay/Lesbian/Bisexual
1
1
1
2
5
2.7
2.7
2.7
5.4
13.5
Bullying Measures
1. Self Report 34 91.9
2. Peer nomination 2 5.4
3. Clinical Assessment/Interview 1 2.7
Suicide Measure
1. Self Report 36 97.3
2. Clinical Assessment/Interview 1 2.7
Measures of Suicidality+
1. Suicidal Ideation 20 54.1
2. Suicidal Behaviors/Self-Harm
Behaviors
20 54.1
3. Composite Variable of Suicidality 8 21.6
YS KIM AND B LEVENTHAL 137
+: Sum of each item is greater than 100% because some studies measured multiple aspects of
suicidality including suicidal ideation, attempts and/or self-harm behaviors
Table 2 landscape
P 1

BULLYING AND SUICIDE 138

YS KIM AND B LEVENTHAL 139
Table 2 landscap
P 3
BULLYING AND SUICIDE 140
experience inquired ranged from „ever in
the past‟, „for the last six months‟ to
„weekly experience.‟ The self-reports of
bullying can be further divided into three
categories:
Self-reports designed to identify
bullying experience with items de-
scribing specific bullying behaviors.
Items in these self-reports include
o Physical bullying such as pushing,
shoving, grabbing, kicking, biting
or hitting;
o Verbal bullying such as insulting,
threatening, calling names or
spreading rumors; and,
o Exclusion such as being ignored,
being rejected, or no talking.
The number of items included in this
category of self-reports varies across studies,
ranging from one (25) to 40 items (26).
This category is represented by 13 studies
(23,25-33).
Self-reports designed to identify a
broader range of behavioral aspects of
bullying and the experiences of
children and adolescents that resemble
bullying behaviors, peer abuse or peer
victimization. Examples of this type of
self-report of bullying include the use
of items from YRBS survey. Included
were YRBS survey items -
o How many days did you not go to
school because you felt you would
be unsafe at school or on your way
to or from school?;
o How many times has someone
threatened or injured you with a
weapon such as a gun, knife or
club on school property?;
o How many times has someone
stolen or deliberately damaged
your property such as your car,
clothing or books on school
property?;
o How often they had started a fight;
o Have you ever threatened to use a
weapon to get something from
someone; and,
o Have you ever used a weapon to
threaten or assault someone.
Sixteen studies used this type of self-report
to identify bullying experience (34-49).
Self-report designed to identify
bullying experience with direct inquiry
about „bullying‟ experiences with or
without the provision of a definition of
bullying. The bullying survey in WHO
Youth Health Study is an example. In
this study, children and adolescents
were asked how frequently they had
bullied others/been bullied during the
current term and whether these actions
occurred many times per week, once
per week, less frequently, or not at all,
after the definition of bullying was
provided. Eight studies used this form
of bullying self-report (50-57).
The peer nomination method was used in
two studies. Kim et al (22) used Korean-
Peer Nomination Inventory to identify four
types of victims, and/or perpetrators, using
the 17 items. Rigby and Slee (23) also used
Peer Rating Measures, using the eight items
to identify victims and bullies.
In one study, a direct interview was
conducted using one item from K-SADS-
PL interview to identify bullying experience
in children and adolescents (24).

YS KIM AND B LEVENTHAL 141
Measurement of outcomes: Suicide
Self-report and interviews were used to
measure suicidality in children and adoles-
cents. Three types of suicidality were
measured: suicidal ideation, suicidal behavior
including self-harm/self-injurious behaviors
and composite variable of any suicidality
(see table 2). Self-report of suicidality were
measured in following ways:
Suicidal Ideation: Suicidal ideations
that were measured in the selected studies
included: “tired of life/occasional thoughts
of suicide,” “for last 6 month, thought about
committing suicide,” “I have explicit plans
of suicide/preparations for suicide.” The
time-frame covered for suicidal ideations
included: “ever,” “past 12 months,” “past 6
months,” “past 2 months,” “past 2 weeks,”
and “current suicidal thoughts.” Suicidal
ideations were identified using suicide
inquiring questions that were created for the
surveys, including the YRBS and the EAT
(25-28,31,39,42,43,48,51,54), a part of the
existing questionnaires, or interview scales,
including Youth Self-Report (YSR), Beck
Depression Inventory, Goldberg Health
Questionnaire (22,23,50,53), or suicide
specific questionnaires, such as Suicidal
Ideation Questionnaire (49,56).
Suicidal behavior: Suicidal Attempts
included in this review paper were
measured by items such as, “Have you ever
on purpose tried to take your own life?” and
“Have you attempted suicide in the past 12
months that resulted in an injury requiring
medical attention?” Suicidal attempts were
identified using suicide inquiry questions
that were created for the particular survey,
including the YRBS survey (25,31,33,35,
37,39,40,43,45-48,51,53), or a part of
existing questionnaires or interview scales
including YSR, or Diagnostic Interview
Schedule for Children (22,56). Self-
harm/injurious behaviors were identified by
self-harm/injurious behavior questions that
were created for the survey (52), or a part of
existing interview scales such as K-SADS-
PL (57). Items assessing self-harm/injurious
behaviors that were identified in the
selected papers ranged from “Have you cut
your wrist and/or arm more than once?” to
“Have you deliberately taken an overdose
of medication or tried to harm yourself in
some other way?”
Composite score of any suicidality:
Eight studies created a single composite
score of suicidality based on the responses
to the multiple questions on suicidal
ideations and/or suicidal behaviors asked of
study participants. This composite variable
of suicidality became the outcome of interest
(29,30,32,34,36,38,41,44).
Interviews were performed in one study to
measure suicidal ideations and behaviors.
Mill et al (24) conducted interviews using
the 19-item Scale for Suicide Ideation to
measure current and past suicide ideations,
and 19-item Suicide Intent Scale to quantify
suicide intent and attempts. One study did
not describe how it measured suicidal
ideations and attempts (55).
Covariates adjusted in analyses examining
associations between bullying and suicide
Covariates that were adjusted in the
examination of the association between
bullying and suicide are summarized in
table 3 and 4. Among the studies conducted
in the general populations of children and
adolescents, 23 of 27 studies adjusted for
gender, whereas 5 out of 10 studies in
special populations controlled for gender in
the examination of the relation between
bullying and suicide. Eight studies
conducted in the general population, as well
BULLYING AND SUICIDE 142
as four studies of special population,
adjusted for other psychopathological risk
factors for suicide. These risk factors
included depression, substance abuse, or
emotional/psychological distress.
Table 3 landscape
P 1
YS KIM AND B LEVENTHAL 143
Table 3 landscape
P 2

BULLYING AND SUICIDE 144

YS KIM AND B LEVENTHAL 145

BULLYING AND SUICIDE 146

YS KIM AND B LEVENTHAL 147

BULLYING AND SUICIDE 148

YS KIM AND B LEVENTHAL 149
Only a single study of the total 37
studies considered past suicide history as a
covariate in its analysis (54). Seven studies
using a general population adjusted for
parental divorce or family structure as a
proxy for parental divorce in their analyses,
whereas none of the studies of special
populations did so. Additionally, 21 studies
of the general population, as well as 6
studies of special populations, controlled
for socioeconomic disadvantages, including
SES, poverty, exposure to violence, social
capital/social support, and demographic
information, such as age and race.
Suicide risks in children and adolescents
with bullying experience
Risks of suicidal ideations, suicidal attempts,
and composite risks of any suicidality that
were associated with bullying experience are
summarized in two tables: Table 3 summa-
rizes 27 studies in a general population of
children and adolescents and table 4 sum-
marizes 10 studies in special populations.
Using 15 samples from the general
population, studies examined the risks of
suicidal ideations in the victims of school
bullying. Whereas 3 studies reported no
association, 12 reported increased risks of
suicidal ideations in the victims of bullying,
with ORs ranging from 1.4 to 5.6. One
study reported a statistically significant
interaction with gender: female victims
were at a greater risk of suicidal ideations
than male victims (22). Additionally, three
studies reported dose-response-relations:
frequent victimization was associated with
higher risks for suicidal ideations than less-
frequent victimizations (26,50,56). Eight of
10 studies that examined the risks of
suicidal ideations in the bullying perpetrators
from the general population reported
increased suicidal risks, with ORs ranging
from 1.4 to 9.0. One study (22) reported
significantly higher risks of suicidal
ideations in female perpetrators than in
male perpetrators, and three studies (26,50,
56) reported dose-response-relations for
frequency of perpetrating behaviors and
suicidal risks. All five studies that
examined risks of suicidal ideations in the
victim-perpetrators (VPs) of school bullying
in the general population reported increased
risks, with ORs ranging from 1.9 to 10.0.
The suicidal risks in VPs were highest
among all the groups involved with
bullying in four studies (22,53,55,56), and
one study reported higher suicidal risk in
female VPs compared with male VPs (22).
Thirteen studies examined risks of
suicidal attempts, including self-injurious
behaviors, in the victims of bullying in
general population and twelve studies
reported increased risks, with ORs ranging
from 1.5 to 5.4. One study reported signifi-
cant interactions between suicidal risks and
female gender (25), and one showed dose-
response-relations (56). Two studies (53,56)
of the four that examined risks of suicidal
attempts in the perpetrators of bullying in
the general population reported increased
suicidal risks, with ORs ranging from 2.3 to
9.9. One study also reported dose-response-
relations between perpetrating behaviors
and suicidal risks (56). All five studies that
examined the composite risks of any
suicidality in victims of bullying in the
general population reported increased risks
of suicidality, with ORs ranging from 1.7 to
2.5. Two studies also examined the risks of
composite suicidality in perpetrators and
reported increased risks with ORs ranging
from 1.3-1.4.
Five studies examined risks of suicidal

BULLYING AND SUICIDE 150
ideations in victims of bullying in special
populations, and four studies reported
increased risks in juvenile offenders,
persons with LD, and lesbian/gay/bisexual
(LGB) sexual orientation, with ORs ranging
from 1.7 to 2.1. One study that examined
the risks of suicidal ideations in perpe-
trators of bullying among juvenile offenders
reported lowered risks compared with the
ones not involved with bullying (31).
Seven studies investigated the risks of
suicidal attempts and self-injurious behaviors
in the victims of bullying in special
populations, and six reported increased
risks, with ORs ranging from 1.4 to 4.6.
The special populations with increased
suicidal risks included individuals with LD,
drug abuse, juvenile delinquency, and of
LGB sexual orientation. Additionally, one
study reported increased risk of suicidal
attempts in the perpetrators of the children
and adolescents with LD with OR 2.7 (37).
Additionally, one study examined the
composite risks of any suicidality in
persons with LGB sexual orientation and
reported that bullying had a mediating role
between gender role conformity and
suicidal risk (32).
DISCUSSION
Suicidality, the third leading cause of
mortality for adolescents (16), has been
examined in relation to bullying in 37
studies conducted in various countries.
Most of these studies reported positive
associations between all bullying types and
suicidal risks, with strongest risks in
Victim-Perpetrators, both in general popu-
lations of children and adolescents and in
populations with specials needs (behavioral
problems or of LGB sexual orientation.) In
addition, a few studies found that suicidal
risks differed based on gender, as well as
with regard to dose-response-relations. The
ORs for suicidal risks associated with
bullying experience ranged from 1.4 to
10.0. Nevertheless, these prior findings
must be interpreted with caution because of
three important, methodological problems:
1. When examining the relation between
bullying and suicidality, most studies
failed to control for other well-
established suicide risk factors,
including gender, psychopathology
(depression, aggressive-impulsive
behaviors and disruptive behaviors),
and a history of suicide (58). Twenty
eight of the thirty-seven studies
controlled for gender. Twelve studies
also controlled for psychopathological
risk factors for suicide, including
depression, substance abuse, or
emotional/psychological distress. Only
a single study controlled for gender,
depression, and prior suicidal history;
this paper reported a negative associ-
ation between bullying and suicide
(54). Taken together, the interpretation
of the observed positive associations
between bullying and suicide in these
studies is seriously limited because
uncontrolled risk factors may have
confounded the relation between
bullying and suicide.
2. The interpretation of these findings is
complicated by the shared method
variance caused by the use of the same
informants to identify both bullying
status and suicidal behaviors/ideations
(59-60). In those instances, self-reports
of bullying are based on the
individuals‟ own perception of the
social circumstances, a situation in
which it is possible that the psycho-
pathological characteristics of the
reporter can lead to the misinterpreta-
tion of otherwise normal social events.
This can result in a confounded
relation between suicide and bullying.
Two of the thirty-seven studies used
YS KIM AND B LEVENTHAL 151
peer nomination to identify indepen-
dently bullying type and self-reports
for delineating suicidal thoughts/
behaviors; both studies reported an
increased risk of suicide in students
with bullying experience (22-23).
3. All 37 studies were cross-sectional,
making it impossible to make causal
inferences or conclusions that experi-
encing bullying increases suicide
risks.
Future studies should address these
major methodological limitations to establish
causal relations between bullying and risks
of suicide. Ideally, future studies should be
long-term, prospective in large community
samples of children and adolescents, as well
as in special populations, and with multiple
informants to identify predictors and out-
comes. The analyses should be planned and
conducted carefully to control for con-
founding effects of other well-established
suicidal risk factors. Findings should be
replicated by independent researchers in
independent study populations.
In the meantime, this systematic review
of 37 prior studies that were conducted in
various countries suggests that bullying is a
serious problem for our youth and our
communities. Not only does bullying inter-
fere with normal developmental and educa-
tional processes but also places adolescents
at an unnecessary and additional risk for
suicidal thoughts and actions. It seems clear
that these adolescents are at increased risk
for suicidal behaviors/ideations and deserve
our particular care and attention. Additionally,
the inclusion of screening and monitoring
of suicidal signs and symptoms in victims,
perpetrators, or victim-perpetrators in the
anti-bullying programs may be an effective
way to reduce suicidality in the children
and adolescents with bullying experience.
Finally, careful clinical evaluation for
suicidality in children with bullying
experience should be a standard practice
that is part of routine primary care visits.
Although many adolescents may experi-
ence bullying, either as participants or
observers, the observation that it is common
does not imply that it is „normal‟ and,
hence, an acceptable part of „normal devel-
opment‟. Indeed, the evidence from this
review suggests that exposure to bullying,
especially for participants, is harmful.
Therefore, it is imperative that there now be
a common goal to intervene actively to
reduce bullying in all communities and to
seek out both victims and perpetrators to
protect them from suicidality and other
potential lethal adverse consequences of
this serious public health problem.
REFERENCES
1. Olweus D. Bullying at school. Basic
facts and an effective intervention pro-
gramme. Promot Educ 1994;1(4):27-
31, 48.
2. Kim YS, Koh YJ, Leventhal BL.
Prevalence of school bullying in
Korean middle school students. Arch
Pediatr Adolesc Med 2004;158(8):
737-41.
3. Nansel TR, Craig W, Overpeck MD,
Saluja G, Ruan WJ. Cross-national
consistency in the relationship between
bullying behaviors and psychosocial
adjustment. Arch Pediatr Adolesc Med
2004;158(8):730-6.
4. Nansel TR, Overpeck M, Pilla RS,
Ruan WJ, Simons-Morton B, Scheidt
P. Bullying behaviors among US
youth: prevalence and association with
psychosocial adjustment. JAMA 2001;
285 (16):2094-100.
5. Boulton MJ, Underwood K. Bully/
victim problems among middle school
children. Br J Educ Psychol 1992;62
BULLYING AND SUICIDE 152
(Pt 1):73-87.
6. Boulton MJ, Smith PK. Bully/victim
problems in middle-school children:
stability, self-perceived competence,
peer rejection and peer acceptance. Br
J Dev Psychol 1994;12:315-29.
7. Byrne B. Bullies and victims in a
school setting with reference to some
Dublin schools. Irish J Psychol 1994;
15:574-86.
8. Rigby K, Slee P. Dimensions of inter-
personal relation among Australian
children and implications for psycho-
logical well-being. J Soc Psychol 1993;
133:33-42.
9. Rigby K. The relationship between
reported health and involvement in
bully/victim problems at school
among male and female secondary
school children. J Health Psychol
1998;3:465-76.
10. Salmon G, James A, Smith DM.
Bullying in schools: self reported
anxiety, depression, and self esteem in
secondary school children [see com-
ments]. BMJ 1996;317(7163):924-5.
11. Slee PT. Situational and interpersonal
correlates of anxiety associated with
peer victimisation. Child Psychiatry
Hum Dev 1994;25(2):97-107.
12. Williams K, Chambers M, Logan S,
Robinson D. Association of common
health symptoms with bullying in
primary school children. BMJ 1996;
313(7048):17-9.
13. Olweus D. Bullying at school: basic
facts and effects of a school based
intervention program. J Child Psychol
Psychiatry 1994;35(7):1171-90.
14. Schwartz D. Subtypes of victims and
aggressors in children‟s peer groups. J
Abnorm Child Psychol 2000;28:181-
92.
15. Anderson R. Deaths: leading causes
for 2000. Natl Vital Stat Rep 2002;
50(16):1-85.
16. Grunbaum J, Kann L, Kinchen S et al.
Youth risk behavior surveillance--
United States, 2001. MMWR Surveill
Summ. 2002;51(4):1-62.
17. Lee JW. Mortality statistics, 2001.
Daejeon: Korea Nat Stat Office, 2002.
18. Kaltiala-Heino R, Rimpela M, Mart-
tunen M, Rimpela A, Rantanen P.
Bullying, depression, and suicidal
ideation in Finnish adolescents: school
survey [see comments]. BMJ 1999;
319(7206):348-51.
19. Prinstein MJ, Boergers J, Spirito A,
Little TD, Grapentine WL. Peer
functioning, family dysfunction and
psychological symptoms in a risk
factor model for adolescent inpatients'
suicidal ideation severity. J Clin Child
Psychol 2000;29(3):392-405.
20. Shaffer D, Garland A, Gould MS,
Fisher P, Trautman P. Preventing teen-
age suicide: A clinical review. J Am
Acad Child Adolesc Psychiatry 1988;
27:675-87.
21. Brener ND, Kann L, Kinchen SA, et
al. Methodology of the youth risk
behavior surveillance system. MMWR
Recomm Rep 2004;53(RR-12):1-13.
22. Kim YS, Koh YJ, Leventhal B, Kim
YS, Koh Y-J, Leventhal B. School
bullying and suicidal risk in Korean
middle school students. Pediatrics
2005;115(2):357-63.
23. Rigby K, Slee P. Suicidal ideation
among adolescent school children,
involvement in bully-victim problems,
and perceived social support. Suicide
Life Threat Behav 1999;29(2):119-30.
24. Mills C, Guerin S, Lynch F, Daly I,
Fitzpatrick C. The relationship between
bullying, depression and suicidal
thoughts/behaviour in Irish adoles-
cents. Irish J Psychol Med 2004;21
(4):112-6.
25. Eisenberg ME, Neumark-Sztainer D,
Story M. Associations of weight-based
teasing and emotional well-being
among adolescents. Arch Pediatr
YS KIM AND B LEVENTHAL 153
Adolesc Med 2003;157(8):733-8.
26. van der Wal MF, de Wit CA, Hirasing
RA. Psychosocial health among young
victims and offenders of direct and
indirect bullying. Pediatrics 2003;111
(6 Pt 1):1312-7.
27. Roland E. Bullying, depressive symp-
toms and suicidal thoughts. Educ Res
2002;44(1):55-67.
28. van der Wal MF, van der Wal MF.
There is bullying and bullying. Eur J
Pediatrics 2005;164(2):117-8.
29. Baldry AC, Winkel FW. Direct and
vicarious victimization at school and at
home as risk factors for suicidal
cognition among Italian adolescents. J
Adolesc 2003;26(6):703-16.
30. Adelmann PK. Social environmental
factors and preteen health-related be-
haviors. J Adolesc Health 2005;36(1):
36-47.
31. Viljoen JL, O'Neill ML, Sidhu A.
Bullying behaviors in female and male
adolescent offenders: Prevalence,
types, and association with psycho-
social adjustment. Aggress Behav
2005;31(6): 521-36.
32. Friedman MS, Koeske GF, Silvestre
AJ, Korr WS, Sites EW. The impact of
gender-role nonconforming behavior,
bullying, and social support on suici-
dality among gay male youth. J
Adolesc Health 2006;38(5):621-3.
33. Hidaka Y, Operario D. Attempted
suicide, psychological health and ex-
posure to harassment among Japanese
homosexual, bisexual or other men
questioning their sexual orientation
recruited via the internet. J Epidemiol
Community Health 2006;60(11):962-7.
34. Woods ER, Lin YG, Middleman A,
Beckford P, Chase L, DuRant RH. The
associations of suicide attempts in ado-
lescents. Pediatrics 1997;99(6):791-6.
35. Garofalo R, Wolf RC, Wissow LS,
Woods ER, Goodman E. Sexual
orientation and risk of suicide attempts
among a representative sample of
youth. Arch Pediatr Adolesc Med 1999;
153(5):487-93.
36. Cleary SD. Adolescent victimization and
associated suicidal and violent behav-
iors. Adolescence 2000;35(140):671-82.
37. Svetaz MV, Ireland M, Blum R.
Adolescents with learning disabilities:
Risk and protective factors associated
with emotional well-being: Findings
from the National Longitudinal Study
of Adolescent Health. J Adolesc Health
2000;27(5):340-8.
38. Evans WP, Marte RM, Betts S,
Silliman B. Adolescent suicide risk
and peer-related violent behaviors and
victimization. J Interpers Violence
2001;16(12):1330-48.
39. Russell ST, Joyner K. Adolescent
sexual orientation and suicide risk:
Evidence from a national study. Am J
Public Health 2001;91(8):1276-81.
40. Bontempo DE, D'Augelli AR. Effects
of at-school victimization and sexual
orientation on lesbian, gay, or bisexual
youths' health risk behavior. J Adolesc
Health 2002;30(5):364-74.
41. Vermeiren R, Schwab-Stone M, Ruch-
kin VV, King RA, Van Heeringen C,
Deboutte D. Suicidal behavior and
violence in male adolescents: A
school-based study. J Am Acad Child
Adolesc Psychiatry 2003;42(1):41-8.
42. Huebner DM, Rebchook GM, Kegeles
SM. Experiences of harassment,
discrimination, and physical violence
among young gay and bisexual men.
Am J Public Health 2004;94(7):1200-3.
43. Warner J, McKeown E, Griffin M et
al. Rates and predictors of mental
illness in gay men, lesbians and bi-
sexual men and women: Results from
a survey based in England and Wales.
Br J Psychiatry 2004;185:479-85.
44. Bae S, Ye R, Chen S, Rivers PA,
Singh KP. Risky behaviors and factors
associated with suicide attempt in
BULLYING AND SUICIDE 154
adolescents. Arch Suicide Res 2005;
9(2): 193-202.
45. Goodenow C, Szalacha L, Westheimer
K. School support groups, other school
factors, and the safety of sexual
minority adolescents. Psychol Schools
2006;43(5):573-89.
46. Hacker KA, Suglia SF, Fried LE,
Rappaport N, Cabral H. Develop-
mental differences in risk factors for
suicide attempts between ninth and
eleventh graders. Suicide Life Threat
Behav 2006;36(2):154-66.
47. Haynie DL, South SJ, Bose S. Resi-
dential mobility and attempted suicide
among adolescents: An individual-
level analysis. Sociol Q 2006;47(4):
693-21.
48. Romito P, Grassi M. Does violence
affect one gender more than the other?
The mental health impact of violence
among male and female university
students. Soc Sci Med 2007;65(6):
1222-34.
49. Shtayermman O. Peer victimization in
adolescents and young adults diagnosed
with Asperger's Syndrome: A link to
depressive symptomatology, anxiety
symptomatology and suicidal ideation.
Issues Compr Pediatr Nurs 2007;30(3):
87-107.
50. Kaltiala-Heino R, Rimpela M, Marttu-
nen M, Rimpela A, Rantanen P.
Bullying, depression, and suicidal
ideation in Finnish adolescents: school
survey. BMJ 1999;319(7206):348-51.
51. Rossow I, Lauritzen G. Shattered
childhood: a key issue in suicidal be-
havior among drug addicts? Addiction
2001;96(2):227-40.
52. Matsumoto T, Yamaguchi A, Chiba Y,
Asami T, Iseki E, Hirayasu Y. Patterns
of self-cutting: A preliminary study on
differences in clinical implications
between wrist- and arm-cutting using a
Japanese juvenile detention center
sample. Psychiatr Clin Neurosci 2004;
58(4):377-82.
53. Ivarsson T, Broberg AG, Arvidsson T,
Gillberg C. Bullying in adolescence:
Psychiatric problems in victims and
bullies as measured by the youth self
report (YSR) and the depression self-
rating scale (DSRS). Nordic J Psychi-
atry 2005;59(5):365-73.
54. Park HS, Schepp KG, Jang EH, Koo
HY. Predictors of suicidal ideation
among high school students by gender
in South Korea. J Sch Health 2006;
76(5):181-8.
55. Liang H, Flisher AJ, Lombard CJ.
Bullying, violence, and risk behavior
in South African school students.
Child Abuse Negl 2007;31(2):161-71.
56. Brunstein Klomek A, Marrocco F,
Kleinman M, et al. Bullying, depres-
sion, and suicidality in adolescents. J
Am Acad Child Adolesc Psychiatry
2007;46(1):40-9.
57. Brunner R, Parzer P, Haffner J et al.
Prevalence and psychological correlates
of occasional and repetitive deliberate
self-harm in adolescents. Arch Pediatr
Adolesc Med 2007;161(7):641-9.
58. Gould MS, Greenberg T, Velting DM,
Shaffer D. Youth suicide risk and pre-
ventive interventions: a review of the
past 10 years. J Am Acad Child
Adolesc Psychiatry 2003;42(4):386-
405.
59. Crick NR, Bigbee MA. Relational and
overt forms of peer victimization: a
multiinformant approach. J Consult
Clin Psychol 1998;66(2):337-47.
60. Hawker DS, Boulton MJ. Twenty
years' research on peer victimization
and psychosocial maladjustment: a
meta-analytic review of cross-sectional
studies. J Child Psychol Psychiatry
2000;41(4):441-55.