bone formation within alumina tubes: effect of calcium, manganese, and chromium dopants
TRANSCRIPT

Biomaterials 25 (2004) 4901–4910
ARTICLE IN PRESS
*Correspondin
ing, The Univer
Kensington, Syd
9385-4437; fax: +
E-mail addres
o.standard@uns1Present addre
of Bath, Bath BA
0142-9612/$ - see
doi:10.1016/j.bio
Bone formation within alumina tubes: effect of calcium,manganese, and chromium dopants
Moreica B. Pabbruwea,b,1, Owen C. Standarda,*, Charles C. Sorrella, C Rolfe Howlettb
aSchool of Materials Science and Engineering, Faculty of Science, The University of New South Wales, Sydney, NSW 2052, AustraliabBone Biomaterial Unit, School of Pathology, Faculty of Medicine, The University of New South Wales, Sydney, NSW 2052, Australia
Received 15 December 2003; accepted 27 December 2003
Abstract
Alumina tubes (1.3mm outer diameter, 0.6mm inner diameter, 15mm length) doped with Ca, Mn, or Cr at nominal
concentrations of 0.5 and 5.0mol% were implanted into femoral medullary canals of female rats for 16 weeks. Tissue formation
within tubes was determined by histology and histomorphometry. Addition of Ca to alumina promoted hypertrophic bone
formation at the advancing tissue fronts and tube entrances, and appeared to retard angiogenesis by limiting ongoing cellular
migration into the tube. It is speculated that the presence of a secondary phase of calcium hexaluminate, probably having a
solubility greater than that of alumina, possibly increased the level of extracellular Ca and, consequently, stimulated osteoclastic
activity at the bone–ceramic interface. Addition of Mn significantly enhanced osteogenesis within the tubes. However, it is not
possible to determine whether phase composition or microstructure of the ceramic was responsible for this because both were
significantly altered by Mn addition. Addition of Cr to the alumina apparently stimulated bone remodelling as indicated by
increased cellular activity and bone resorption at the tissue-implant interface. Cr was incorporated into the alumina as a solid
solution and the tissue response was speculated to be an effect of surface chemistry rather than microstructure. The work
demonstrates that doping a bioinert ceramic with small amounts of specific elements can significantly alter tissue ingrowth,
differentiation, and osteogenesis within a porous implant.
r 2004 Elsevier Ltd. All rights reserved.
Keywords: Alumina; Bone ingrowth; Bone remodelling; Osteogenesis; Porosity; Surface modification
1. Introduction
The long-term success of orthopaedic joint prostheses,such as hip and knee arthroplasties, is criticallydependent on the formation and subsequent mainte-nance of a strong and stable interface between aprosthesis and skeletal tissue of the host. Asepticloosening, due to the presence of implant-derived weardebris, remains the major long-term clinical problemand is a primary cause for revision surgery [1]. Onestrategy to improve clinical longevity of non-cemented
g author. School of Materials Science and Engineer-
sity of New South Wales, Via Gate 2 High Street
ney, New South Wales 2033, Australia. Tel.: +61-2-
61-2-9385-5956.
ses: [email protected] (M.B. Pabbruwe),
w.edu.au (O.C. Standard).
ss. Department of Chemical Engineering, University
2 7AY, UK.
front matter r 2004 Elsevier Ltd. All rights reserved.
materials.2004.01.005
prostheses is to improve osseointegration at the im-plant–tissue interface. This may be achieved by promot-ing the initial ingrowth of osseous tissue into the outerporous or roughened structure and then to maintain thequality and quantity of this tissue within the porous orroughened domains. Such an approach serves not onlyto improve directly the strength and stability of theinterface but also to restrict access of particulate weardebris to the interface.Osseointegration is influenced strongly by surface
composition and topography [2,3]. A popular approachto promote osseointegration of relatively bioinertimplant surfaces is to apply a thin coating of a bioactivematerial [4,5]. More subtle modifications of surfacecomposition and resultant tissue response can beachieved by incorporating small amounts of selectedelements into a biomaterial [6–8]. Although the additionof a particular element may, in some cases, favourbone apposition, fundamental understanding of the
ARTICLE IN PRESSM.B. Pabbruwe et al. / Biomaterials 25 (2004) 4901–49104902
mechanism by which dopant elements influence thetissue response remains limited. It is known that Ca[9] and some trace elements, including Cr [10–12], Si[13–15], and Mn [16–19], are essential for normal growthand metabolism of skeletal tissue in vertebrates and canbe detected as minor constituents in teeth and bone.In contrast, implant-derived Ti, Co, and Cr (presentas wear particles or soluble salts) inhibit functions suchas alkaline phosphatase activity, extracellular calcifica-tion, and bone-specific gene expression of bone-derivedcells [20–23]. Considering the role of specific elementsin osteogenesis and bone remodelling, it is postulatedthat their incorporation in an almost inert bio-material, such as alumina, may affect the cellularresponse at the bone–implant interface and, in parti-cular, osteogenesis within porous domains. This hypoth-esis was tested by quantifying bone ingrowth anddifferentiation within cylindrical tubes (15mm long,0.6mm internal diameter) of pure alumina and aluminadoped with Ca, Mn, or Cr implanted in the medullarycanal of adult rats.
2. Materials and methods
2.1. Fabrication of ceramic tubes
Ceramic tubes having dimensions (after sintering) ofB1.3mm (outer diameter) �B0.6mm (inner diameter)�B15mm (length) and composed of high-purityalumina or alumina doped with either Ca, Mn, or Crat a concentration of 0.5 or 5.0mol% were used. Theinternal diameter of B0.6mm was selected fromprevious animal studies involving pure alumina tubesbecause it gave the best discrimination in osteogenesis atearly timepoints [24]. The doped-alumina batches weremade by ball-milling alumina powder (99.6% puritywith 0.04 wt% MgO sintering aid, Sumitomo Corp.,Japan) with an appropriate amount of CaCO3 (99.9%purity; Ajax Chemicals, Australia), MnO2 (99.5%purity; BDH Ltd., England), or Cr2O3 (99.9% purity;BDH Ltd., England) powder in deionised water usingalumina grinding media and a high-density polyethylenemill chamber. Tubes were formed by dipping a paper-coated mandrel into a suspension consisting of 55.47wt% ceramic powder, 44.37 wt% water, and 0.16 wt%sodium carboxymethylcellulose (Daicel Chemical In-dustries, Japan), the latter used as a deflocculant/binder.After casting, the tubes were removed from themandrels, dried, and then sintered in air in an electricfurnace at 1600�C for 6 h.
2.2. Characterisation of ceramic tubes
The bulk density of the sintered tubes was determinedby hydrostatic weighing [25]. The average grain size
of each ceramic was calculated from micrographs,obtained by field emission scanning electron microscopy(FESEM; S4500, Hitachi, Japan) of fracture surfaces,using a line-intercept method [26]. The internal surfaceof the sintered tubes was accessed by sectioning tubeslongitudinally and the surface microstructure wasexamined using FESEM. The average surface roughnessðRaÞ of the internal surface was determined by atomicforce microscopy (AFM; Dimension 3000, DigitalInstruments, USA) using standard Si3N4 probes incontact mode over a scan area of 100 mm2. The overallchemical composition of the sintered tubes was deter-mined by induction coupled plasma atomic emissionspectroscopy (ICP-AES; Australian Laboratory Ser-vices, Australia). The elemental distribution of Al, O,and individual dopant element (Ca, Mn, or Cr) withineach ceramic was determined using electron microprobeanalysis (EPMA; SX-50, Cameca, France). The phasecomposition was analysed by X-ray diffraction (XRD)using a powder-type X-ray diffractometer (D5000Diffractometer, Siemens, Germany) employing CuKaradiation. Leaching of dopant elements from theceramics was determined by ageing samples at 37�Cfor up to 28 days in sterile cell culture medium with theconcentration of dopant elements in the media beingmeasured by ICP-AES (Australian Laboratory Services,Australia). Also, the concentration of dopant elementsin tissues adjacent to tubes implanted in vivo wasmeasured by EPMA (EPMA was done on unstainedsections prepared in Section 2.4).
2.3. Surgical procedure
Ceramic tubes were implanted into the femoralmedullary canals of 12-week-old (B250 g) femaleSprague–Dawley rats. For the pure alumina controlmaterial and each of the seven doped alumina composi-tions, six tubes were implanted bilaterally in three rats,giving a total of 21 rats in the study. Australianguidelines for the care and use of laboratory animalswere followed [27]. The surgical procedure has beendescribed in detail elsewhere [24]. Briefly, after makingan incision medial to the patella, the knee jointwas dislocated and a hole drilled through the inter-condylar notch to access the femoral medullary canal.The canal was flushed with saline and a ceramictube inserted. The hole was sealed with bone cement,the patella relocated, and the joint capsule andskin were sutured closed. No postoperative compli-cations occurred and all rats were able to standfollowing recovery from anaesthesia. Postoperativeanalgesia (buprenorphine, Reckitt and Colman, UK)was administered for 48 h after surgery. Animals wereeuthanised at 16 weeks using intraperitoneal sodiumpentobarbitone.

ARTICLE IN PRESSM.B. Pabbruwe et al. / Biomaterials 25 (2004) 4901–4910 4903
2.4. Embedding and staining techniques
After retrieval, femurs were dissected free of softtissues, fixed in 95% ethanol, and embedded inpolymethylmethacrylate. Sections parallel to the long-itudinal axis of the femur and B100 mm thick wereprepared using a precision cutting system (Exakt 300CL,Exakt Apparatebau, Germany). The sections werestained using a modified version of Lee’s methyleneblue/basic fuchsin protocol for undecalcified embeddedtissue sections [28].
2.5. Histology and histomorphometry
Polished sections were examined using transmissionoptical microscopy. Tissues were identified on thebasis of morphology only; no complementary histo-chemical analyses were done. The extent of boneformation within the implanted tubes was quantifiedby image analysis (Leica Q500, Leica, Cambridge, UK)of sections, involving interactive selection of tissuedistances and areas at a magnification of 40� ,according to the following parameters:
1. Bone ingrowth area: area of bone (no distinctionbetween woven bone and lamellar bone) and marrowwithin a tube, expressed as a percentage of thetotal internal longitudinal cross-sectional area of thetube.
2. Bone penetration distance: longitudinal distance ofbone penetration into a tube (averaged between thedistal and proximal ends of each tube).
3. Affinity index: linear length of bone directly adjacentto the longitudinal length of the internal surface ofthe tube expressed as a fraction of the total long-itudinal length of the bone/implant interface.
These parameters were measured three times for eachsection. All data were analysed using statistical software(PRISM 3.0, Graphpad Software, San Diego, USA).
Table 1
Summary of the characteristics of the sintered tubes
Material Characteristics
Dopant (mol%)BD GS Ra
(kg/m3) (mm) (nm)
Pure alumina 4000760 1.9970.42 305.2
0.5mol% Ca (0.55mol%) 39507260 2.9770.23�,�� 370.0
5.0 mol% Ca (5.86mol%) 34707550 1.5070.22�,�� 265.6
0.5mol% Mn (0.24mol%) 3770770�,�� 1.6470.30� 145.2
5.0mol% Mn (2.54mol%) 33407100�,�� 2.0770.39 229.2
0.5mol% Cr (0.24mol%) 37807280 1.2870.25� 218.1
5.0mol% Cr (2.06mol%) 37907220 1.2470.47� 220.6
For the doped tubes, the dopant concentration is listed as the nominal conce
density (BD) and grain size (GS) are each reported 7one standard deviatio�Significant differences (po0.01) in characteristics between a dopant and��Significant differences (po0.01) in characteristics between concentratio
The effect of ceramic composition on each histomor-phometric parameter was determined by analysis ofvariance (ANOVA) and significant differences weredetermined using the Student–Newmann–Keuls post-test. Values of po0:05 were considered to be statisticallysignificant.
3. Results
3.1. Characterisation of sintered tubes
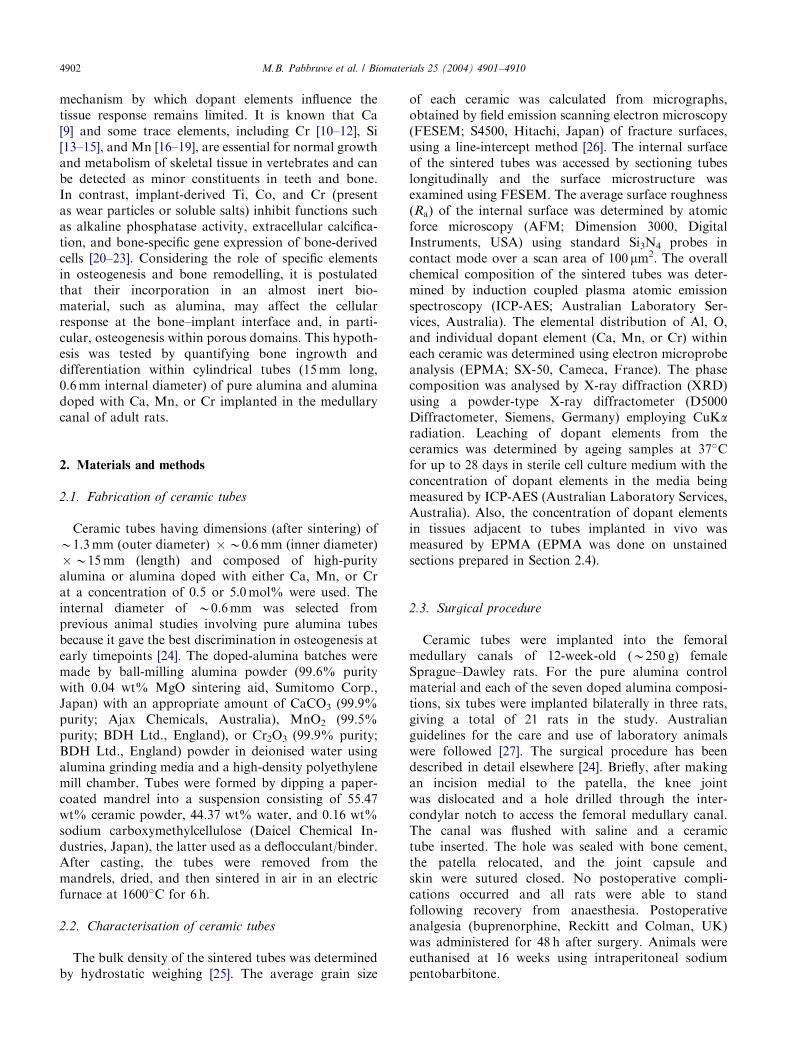
The chemical and physical properties of the sinteredceramic tubes are summarised in Table 1. The amountsof Ca in the sintered tubes were close to the nominalcompositions. The amounts of Mn and Cr in thesintered tubes were significantly less than those addedto the initial mixed-oxide powder batches (Table 1)which is attributed to volatilisation of the Mn and Croxides during sintering owing to their relatively highvapour pressure [29]. For the sake of consistency, thenominal dopant levels of 0.5 and 5.0mol% are still usedhereafter to identify the tubes. The microstructures ofthe internal surface of the ceramic tubes are shown inFig. 1. The internal surface of the implants was simplythe natural grain structure of the as-sintered surface.The internal surface roughness ranged from 145.0 to370.0 nm and correlated reasonably well with thechanges in grain size. EPMA and XRD data showedthe dopant in the Cr-doped tubes to be distributedhomogeneously within the a-Al2O3 grains whereas Caand Mn were incorporated as secondary phases. Fortubes doped with Mn and Cr, the concentration ofdopant elements in serum after aging in vitro was belowthe level of detection (0.01 ppm) of ICP-AES and theseelements were not detected by EPMA in tissues adjacentto the tubes in vivo. These leaching data indicate thatdissolution of these ceramics was not significant. Theconcentration of Ca in both serum and osseous tissue is
Phase composition
Polyhedral a-Al2O3 grainsPolyhedral a-Al2O3 grainsPolyhedral a-Al2O3 grains with some CaO � 6Al2O3 grainsPolyhedral a-Al2O3 grains with needle-shaped MnAl2O4 spinelgrains and globular MnO and Mn2O3 grains
Polyhedral a-Al2O3 grainsPolyhedral a-Al2O3 grains
ntration and the actual concentration is given in parentheses. The bulk
n.
pure alumina are indicated by asterisks.
ns of a particular dopant.
ARTICLE IN PRESS
Fig. 1. Microstructure of the internal surface of: (a) pure alumina tube; (b) 0.5mol% Ca-doped alumina tube; (c) 5.0mol% Ca-doped alumina tube;
(d) 0.5mol% Mn-doped alumina tube; (e) 5.0mol% Mn-doped alumina tube; (f) 0.5mol% Cr-doped alumina tube; and (g) 5.0mol% Cr-doped
alumina tube. The scale bar in each micrograph is equal to 5 mm.
M.B. Pabbruwe et al. / Biomaterials 25 (2004) 4901–49104904
significant and, whilst there were no significant changein Ca concentration of either the serum after agingin vitro or in the tissues adjacent to the implant in vivo,it was not possible to determine if there was biologicallysignificant leaching from the Ca-doped tubes.
3.2. Histology of tissues formed within ceramic tubes
Pure alumina tubes: The distal section of a purealumina tube implanted for 16 weeks is shown in Fig. 2.
Tissue migration occurred in the form of two advancingtissue fronts, one from each end of each tube. Each frontconsisted of a mixture of undifferentiated vascularmesenchymal tissue, osteoid, marrow, and trabeculaeof woven bone and lamellar bone. The region betweenthe two fronts was filled with plasma proteins (assumedto be mainly fibrin). Extending from each advancingtissue front towards the tube entrance, was a thincontinuous layer of lamellar bone lining the tube surfacethat enclosed a central lumen of marrow. This lamellar

ARTICLE IN PRESS
Fig. 2. Section of the distal end of a pure alumina tube implanted
for 16 weeks in the medullary canal of a rat femur (stained with
methylene blue and basic fuchsin) showing an advancing tissue front
consisting of areas of undifferentiated mesenchymal tissue (UMT);
undifferentiated mesenchymal tissue and woven bone (UMT+WB);
undifferentiated mesenchymal tissue, woven bone, and lamellar bone
(UMT+WB+LB); woven bone and marrow (WB+M); woven bone,
lamellar bone, and marrow (WB+LB+M). The region ahead of this
advancing tissue front consisted of plasma proteins whereas behind the
front bone had remodelled into lamellar bone (LB) appositioned along
the tube surface and enclosing a lumen of marrow (M).
Fig. 3. Section of the distal end of Ca-doped alumina tubes (stained
with methylene blue and basic fuchsin) showing: (a) hypertrophic
lamellar bone (LB) completely obstructing the entrance of a 0.5mol%
Ca tube with marrow (M) located further into the tube and minimal
bone resorption (white arrow) evident at the bone-implant interface;
(b) advancing tissue front in a 5.0mol% Ca tube consisting of
trabeculae of lamellar bone (LB) with the occasional osteoid seam
(OD) located on the trabecular surface and some undifferentiated
mesenchymal tissue (UMT) further inside the tube; and (c) resorption
site (white arrow) containing undifferentiated mesenchymal tissue
located at the bone-implant interface of a 5.0mol% Ca tube; cement
lines (black arrows) are indicative of a number of appositional deposits
of bone (the space between the bone and the tissue (Ar) is an artefact of
section preparation).
M.B. Pabbruwe et al. / Biomaterials 25 (2004) 4901–4910 4905
bone contained osteoclasts in Howship’s lacunae andnumerous cement lines indicating that it was in theprocess of being remodelled. In three tubes, theadvancing tissue fronts had met to leave small amountsof woven and lamellar bone trabeculae at the midpointof the tube length with lamellar bone lining the entiretube length back to the entrances.
Calcium-doped alumina tubes: In both the 0.5 and5.0mol% Ca-doped tubes, the advancing tissue frontsconsisted of thick layers of lamellar bone with a fewsmall foci of woven bone and osteoid (Fig. 3). Tubeentrances were lined with hypertrophic lamellar bone(Fig. 3a) such that two of the six 0.5mol% Ca-dopedtubes and three of the six 5.0mol% Ca-doped tubes hadentrances that were completely occluded by plugs oflamellar bone (Fig. 3b) with the remainder of the tubeinterior filled completely with undifferentiated mesench-ymal tissue and small amounts of plasma proteins. Atthe bone–ceramic interface of the 0.5mol% Ca-dopedtubes, direct apposition of bone occurred, with a fewresorption sites located towards the tube entrances.Interfaces between bone and 5.0mol% Ca-doped tubeswere characterised by either direct apposition oflamellar bone or scalloped bone resulting from resorp-tion sites (three of six tubes). The latter were partiallyfilled with new bone (Fig. 3c).
Manganese-doped alumina tubes: The pattern of tissueformation was similar in the 0.5 and 5.0mol% Mn-doped tubes in that the advancing tissue fronts hadeither (a) met and remodelled such that only a smallamount of woven/lamellar bone trabeculae remained atthe midpoint of the tube length, or (b) were close tomeeting, with the volume separating them filled withundifferentiated mesenchymal tissue. Differentiation oftissues in the Mn-doped alumina tubes appeared tooccur more promptly and completely than in the pure
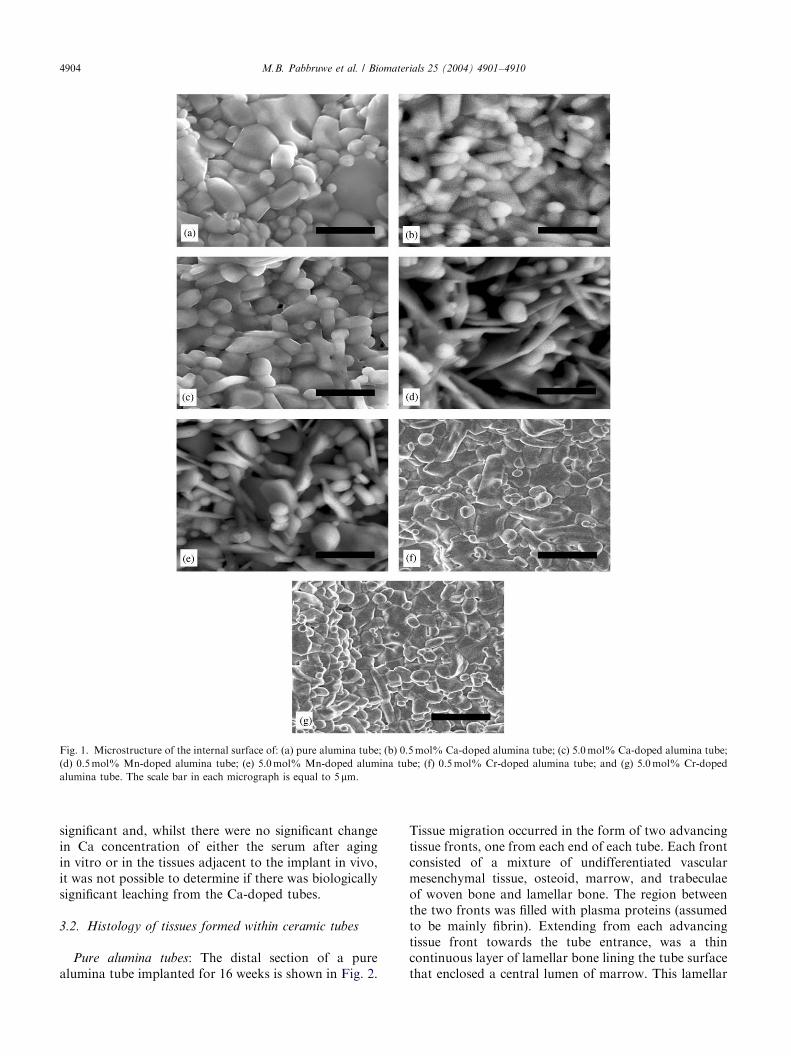
alumina tubes as evidenced by: (i) the absence of anyplasma proteins in the region between advancing tissuefronts (where still present) in the Mn-doped tubes, thisregion instead containing mainly undifferentiated me-senchymal tissue; (ii) the osseous tissues in the Mn-doped tubes consisted mainly of lamellar bone andmarrow; (iii) the lamellar bone lining the inner aspect ofthe Mn-doped tubes (at both concentrations) tendedto be thinner and more compact than that lining thepure alumina tubes Fig. (4); and (iv) unlike purealumina, there was virtually no evidence of cellularactivity or resorption activity along the entire internalbone–ceramic interface of the Mn-doped tubes andinstead the interface was characterised by direct bone
ARTICLE IN PRESS
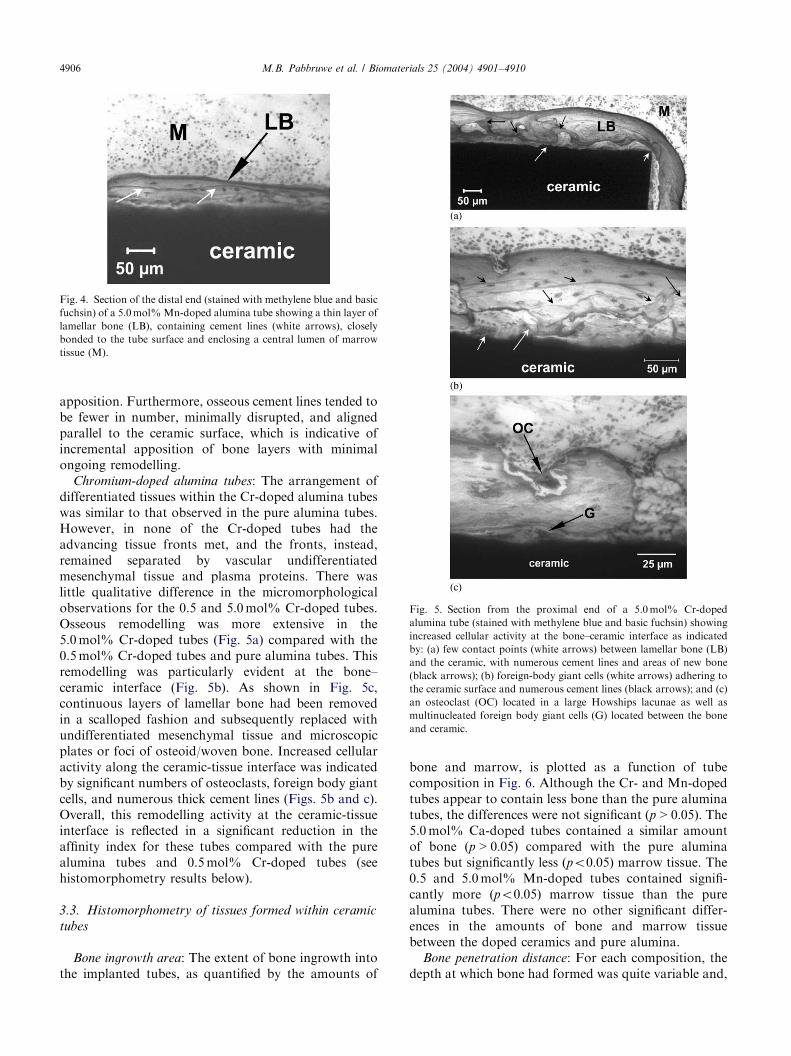
Fig. 5. Section from the proximal end of a 5.0mol% Cr-doped
alumina tube (stained with methylene blue and basic fuchsin) showing
increased cellular activity at the bone–ceramic interface as indicated
by: (a) few contact points (white arrows) between lamellar bone (LB)
and the ceramic, with numerous cement lines and areas of new bone
(black arrows); (b) foreign-body giant cells (white arrows) adhering to
the ceramic surface and numerous cement lines (black arrows); and (c)
an osteoclast (OC) located in a large Howships lacunae as well as
multinucleated foreign body giant cells (G) located between the bone
and ceramic.
Fig. 4. Section of the distal end (stained with methylene blue and basic
fuchsin) of a 5.0mol%Mn-doped alumina tube showing a thin layer of
lamellar bone (LB), containing cement lines (white arrows), closely
bonded to the tube surface and enclosing a central lumen of marrow
tissue (M).
M.B. Pabbruwe et al. / Biomaterials 25 (2004) 4901–49104906
apposition. Furthermore, osseous cement lines tended tobe fewer in number, minimally disrupted, and alignedparallel to the ceramic surface, which is indicative ofincremental apposition of bone layers with minimalongoing remodelling.
Chromium-doped alumina tubes: The arrangement ofdifferentiated tissues within the Cr-doped alumina tubeswas similar to that observed in the pure alumina tubes.However, in none of the Cr-doped tubes had theadvancing tissue fronts met, and the fronts, instead,remained separated by vascular undifferentiatedmesenchymal tissue and plasma proteins. There waslittle qualitative difference in the micromorphologicalobservations for the 0.5 and 5.0mol% Cr-doped tubes.Osseous remodelling was more extensive in the5.0mol% Cr-doped tubes (Fig. 5a) compared with the0.5mol% Cr-doped tubes and pure alumina tubes. Thisremodelling was particularly evident at the bone–ceramic interface (Fig. 5b). As shown in Fig. 5c,continuous layers of lamellar bone had been removedin a scalloped fashion and subsequently replaced withundifferentiated mesenchymal tissue and microscopicplates or foci of osteoid/woven bone. Increased cellularactivity along the ceramic-tissue interface was indicatedby significant numbers of osteoclasts, foreign body giantcells, and numerous thick cement lines (Figs. 5b and c).Overall, this remodelling activity at the ceramic-tissueinterface is reflected in a significant reduction in theaffinity index for these tubes compared with the purealumina tubes and 0.5mol% Cr-doped tubes (seehistomorphometry results below).
3.3. Histomorphometry of tissues formed within ceramic
tubes
Bone ingrowth area: The extent of bone ingrowth intothe implanted tubes, as quantified by the amounts of
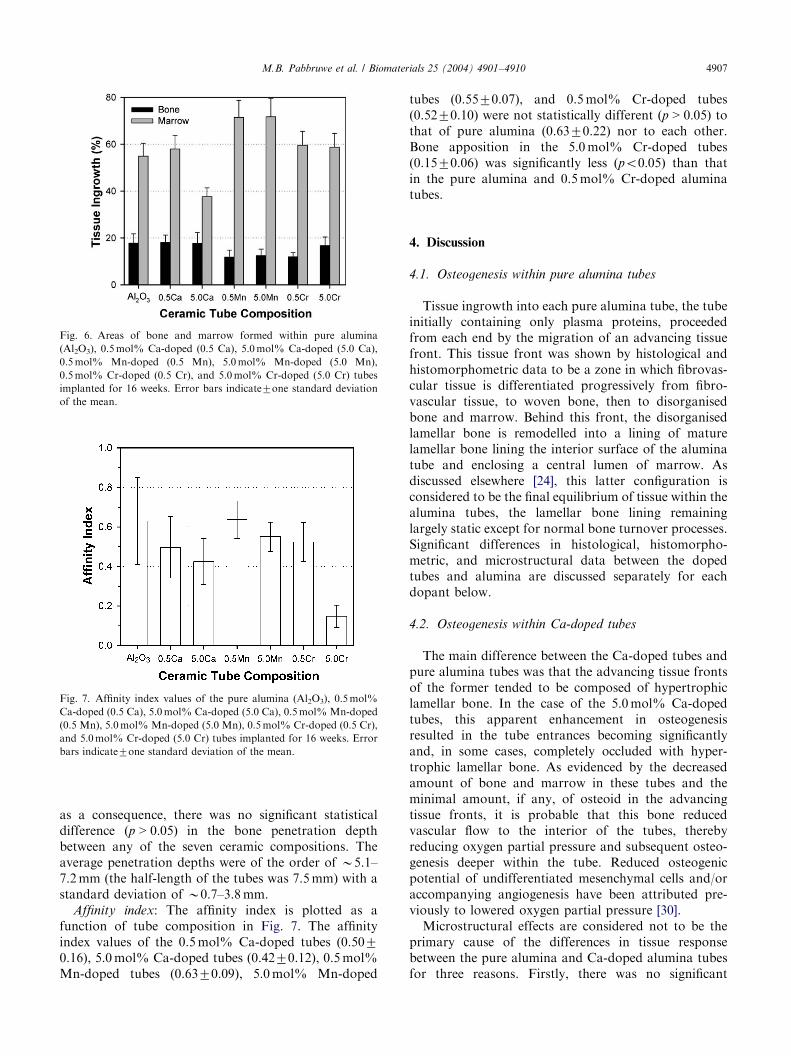
bone and marrow, is plotted as a function of tubecomposition in Fig. 6. Although the Cr- and Mn-dopedtubes appear to contain less bone than the pure aluminatubes, the differences were not significant ðp > 0:05Þ: The5.0mol% Ca-doped tubes contained a similar amountof bone ðp > 0:05Þ compared with the pure aluminatubes but significantly less ðpo0:05Þ marrow tissue. The0.5 and 5.0mol% Mn-doped tubes contained signifi-cantly more ðpo0:05Þ marrow tissue than the purealumina tubes. There were no other significant differ-ences in the amounts of bone and marrow tissuebetween the doped ceramics and pure alumina.
Bone penetration distance: For each composition, thedepth at which bone had formed was quite variable and,
ARTICLE IN PRESS
Fig. 6. Areas of bone and marrow formed within pure alumina
(Al2O3), 0.5mol% Ca-doped (0.5 Ca), 5.0mol% Ca-doped (5.0 Ca),
0.5mol% Mn-doped (0.5 Mn), 5.0mol% Mn-doped (5.0 Mn),
0.5mol% Cr-doped (0.5 Cr), and 5.0mol% Cr-doped (5.0 Cr) tubes
implanted for 16 weeks. Error bars indicate7one standard deviationof the mean.
Fig. 7. Affinity index values of the pure alumina (Al2O3), 0.5mol%
Ca-doped (0.5 Ca), 5.0mol% Ca-doped (5.0 Ca), 0.5mol% Mn-doped
(0.5 Mn), 5.0mol% Mn-doped (5.0 Mn), 0.5mol% Cr-doped (0.5 Cr),
and 5.0mol% Cr-doped (5.0 Cr) tubes implanted for 16 weeks. Error
bars indicate7one standard deviation of the mean.
M.B. Pabbruwe et al. / Biomaterials 25 (2004) 4901–4910 4907
as a consequence, there was no significant statisticaldifference ðp > 0:05Þ in the bone penetration depthbetween any of the seven ceramic compositions. Theaverage penetration depths were of the order of B5.1–7.2mm (the half-length of the tubes was 7.5mm) with astandard deviation of B0.7–3.8mm.
Affinity index: The affinity index is plotted as afunction of tube composition in Fig. 7. The affinityindex values of the 0.5mol% Ca-doped tubes (0.5070.16), 5.0mol% Ca-doped tubes (0.4270.12), 0.5mol%Mn-doped tubes (0.6370.09), 5.0mol% Mn-doped
tubes (0.5570.07), and 0.5mol% Cr-doped tubes(0.5270.10) were not statistically different ðp > 0:05Þ tothat of pure alumina (0.6370.22) nor to each other.Bone apposition in the 5.0mol% Cr-doped tubes(0.1570.06) was significantly less ðpo0:05Þ than thatin the pure alumina and 0.5mol% Cr-doped aluminatubes.
4. Discussion
4.1. Osteogenesis within pure alumina tubes
Tissue ingrowth into each pure alumina tube, the tubeinitially containing only plasma proteins, proceededfrom each end by the migration of an advancing tissuefront. This tissue front was shown by histological andhistomorphometric data to be a zone in which fibrovas-cular tissue is differentiated progressively from fibro-vascular tissue, to woven bone, then to disorganisedbone and marrow. Behind this front, the disorganisedlamellar bone is remodelled into a lining of maturelamellar bone lining the interior surface of the aluminatube and enclosing a central lumen of marrow. Asdiscussed elsewhere [24], this latter configuration isconsidered to be the final equilibrium of tissue within thealumina tubes, the lamellar bone lining remaininglargely static except for normal bone turnover processes.Significant differences in histological, histomorpho-metric, and microstructural data between the dopedtubes and alumina are discussed separately for eachdopant below.
4.2. Osteogenesis within Ca-doped tubes
The main difference between the Ca-doped tubes andpure alumina tubes was that the advancing tissue frontsof the former tended to be composed of hypertrophiclamellar bone. In the case of the 5.0mol% Ca-dopedtubes, this apparent enhancement in osteogenesisresulted in the tube entrances becoming significantlyand, in some cases, completely occluded with hyper-trophic lamellar bone. As evidenced by the decreasedamount of bone and marrow in these tubes and theminimal amount, if any, of osteoid in the advancingtissue fronts, it is probable that this bone reducedvascular flow to the interior of the tubes, therebyreducing oxygen partial pressure and subsequent osteo-genesis deeper within the tube. Reduced osteogenicpotential of undifferentiated mesenchymal cells and/oraccompanying angiogenesis have been attributed pre-viously to lowered oxygen partial pressure [30].Microstructural effects are considered not to be the
primary cause of the differences in tissue responsebetween the pure alumina and Ca-doped alumina tubesfor three reasons. Firstly, there was no significant

ARTICLE IN PRESSM.B. Pabbruwe et al. / Biomaterials 25 (2004) 4901–49104908
difference ðp > 0:01Þ in bulk density (or apparentporosity) between these three groups of tubes. Secondly,the grain size (and surface roughness) of the 0.5mol%Ca and 5.0mol% Ca tubes was significantly greater andsmaller, respectively, than that of the pure aluminatubes. Thus, a systematic variation in microstructuralproperties, with which to correlate with the differencesin tissue response to the tubes, was not apparent.Instead, variations in chemical composition and phasecomposition need to be considered.It is probable that, at both Ca concentrations, Ca was
incorporated in the alumina tubes as discrete precipi-tates of CaO � 6Al2O3 at the grain boundaries. Althoughnot identified in this work, it is likely that Ca wasincorporated also as an impurity-derived, thin (B10 nm)layer of calcium silicate or calcium aluminosilicate glasswetting the grain boundaries [31] and as CaO dissolvedwithin the Al2O3 grains (upto B0.01 wt% [32]) butenriched at the grain surfacesB10 times compared withthe bulk [33,34]. Although the solubilities of these Ca-containing phases in vitro or in vivo have not beenreported (and although there was no significant increasein Ca concentration in either the serum used to age thetubes in vitro or the tissues surrounding the tubesin vivo), consideration of physical and mechanicalproperties of these phases suggests that they are lesschemically stable than pure alumina and consequentlyshould have higher solubilities. It is possible that anydissolution of these phases in vivo could increase theextracellular concentration of Ca in the immediatevicinity of the implant surface. In vitro studies involvingisolated rat osteoclasts have shown that osteoclasticactivity and bone resorption are regulated downwardsby the release of soluble Ca into the extracellularenvironment by actively resorbing osteoclasts [35,36].Thus, it is speculated that the formation of hypertrophicbone in the advancing tissue fronts of the Ca-dopedtubes was caused by a downturn in osteoclastic activitytriggered by an increase in local extracellular Caconcentration arising from Ca leaching from thetubes, but leaving the osteoblastic phase proceedingat the normal rate, hence favouring a net formationof bone.
4.3. Osteogenesis within Mn-doped tubes
The apparent enhancement of tissue differentiationcascade within the Mn-doped tubes can be ascribedpotentially to changes in the chemical composition,phase composition, and surface microstructure of thetubes. The main effect of Mn addition was to producediscrete Mn-rich intergranular phases (MnO �Al2O3,MnO, and Mn3O4) of different morphologies (globulesand needles) in addition to the main a-alumina phase (inapproximate agreement with the MnO–Al2O3 phasediagram [37]). Also, Mn addition significantly inhibited
densification of the alumina and, correspondingly, therewas a greater amount of porosity in the Mn-dopedtubes. Although the surface topography of the mixed-phase microstructure appeared to be more complex andirregular than that of the pure alumina tubes, the scaleof the morphology was actually finer, as indicated by thesurface roughness values (Table 1).Considering firstly surface microstructure, given that
microstructural features at the submicron/micron levelappear to favour interlocking between bone and theimplant [38], it is possible that the changes in the natureand scale of the surface topography, compared with thepure alumina tubes, favoured tissue ingrowth anddifferentiation within the Mn-doped tubes. Also, themore open microstructure of the Mn-doped tubes mayhave provided enhanced nutrient penetration into thetube leading to enhanced tissue differentiation withinthe tubes.From a chemical point of view, Mn is important in
the synthesis of mucopolysaccharides [19] and Mndeficiency impairs the synthesis of cartilaginous organicmatrix, which, in turn, retards endochondral osteogen-esis [18,19] and causes skeletal abnormalities, such asthickening and shortening of long bones as well as jointdeformities [18]. Mn deficiency in rats has been shown toimpair osteoblastic activity, leading to increased boneresorption [39,40] as well as reducing proteoglycansynthesis [19,41]. In man, Mn deficiency has beenimplicated in osteoporosis, suggesting that Mn isinvolved in the maintenance of bone mass [42]. Thiselement appears to be involved in the regulation of boneremodelling [43] because its deficiency has been corre-lated with increases in extracellular Ca, phosphate, andalkaline phosphatase concentrations. Given the impor-tant role of Mn in bone formation and maintenance, it isspeculated that osteogenesis at the bone–ceramic inter-face of the Mn-doped tubes may have been enhanced bythe presence of Mn, either in the form of Mn-containingphases in the alumina or as extracellular Mn derivedfrom leaching from the ceramic (although in vitro andin vivo leaching data demonstrate that Mn leachingwas zero).Given that the incorporation of Mn altered the
chemical composition, phase composition, and surfacemicrostructure of the alumina, it was impossible todetermine which of these characteristics is responsiblefor the enhanced tissue differentiation. Nonetheless, thetissue responses to the two Mn concentrations weresimilar to each other but were significantly differentfrom that for alumina which indicates that whateverthe changes in material characteristics responsible forthe enhanced tissue response, they were effective by thelower Mn content. This investigation demonstrates, forthe first time, that incorporation of small amounts ofMn into alumina has a significant effect on the tissueresponse at the bone-ceramic interface.

ARTICLE IN PRESSM.B. Pabbruwe et al. / Biomaterials 25 (2004) 4901–4910 4909
4.4. Osteogenesis within Cr-doped tubes
Compared with pure alumina, the addition of0.5mol% Cr had no significant effect on the types,amounts, or arrangement of tissues inside the tubes, butit did decrease significantly the bulk density, grain size,and surface roughness of the ceramic. Increasing the Crlevel from 0.5 to 5.0mol% noticeably increased theextent of bone remodelling activity (as evidenced bynumerous bone resorption sites, usually occupied byosteoclasts and foreign-body giant cells, as well as areasof recently deposited bone) along the bone/implantinterface but did not affect significantly the bulk density,grain size, or surface roughness of the ceramic. Theseobservations are consistent with the affinity index valueobtained for the 5.0mol% Cr-doped tubes beingsignificantly lower ðpo0:05Þ than those of the purealumina and 0.5mol% Cr-doped tubes.Since the tissue response was similar for the different
microstructures of the 0.5mol% Cr doped and pure-Al2O3 tubes (these having a small difference incomposition) but was significantly different for the 0.5and 5.0mol% Cr doped-tubes (these having similarmicrostructures), it is reasonable to conclude thatcomposition (Cr content) rather than microstructurewas responsible for the increased cellular activity.Furthermore, since Cr2O3 is completely soluble in a-Al2O3 [44,45], does not segregate to the grain boundaries[34], and does not change the a-Al2O3 lattice parametersfor additions up to B8mol% Cr2O3 [46], the additionsof Cr2O3 in this work would be expected to change thechemical composition, but not the phase compositionnor crystal structure, of the alumina. Therefore, theincreased cellular activity at the interface of the5.0mol% Cr-doped tubes can be ascribed mainly to achange in chemical composition. Furthermore, it can bededuced that the compositional threshold for increasedcellular activity lies somewhere between the actual Crcontents of 0.24 and 2.06mol% Cr.Given that Cr has been implicated in enhanced
collagen production by osteoblasts and in bone resorp-tion (in osteoporotic patients) [10–12], it is possible thatthe resorption at the bone-ceramic interface wasstimulated directly by the Cr ions (at the higherconcentration) in solid solution with the alumina atthe ceramic surface. Similarly, it is possible that theincrease in cellular activity was due to a change insurface energy caused by the isovalent substitution ofAl with Cr in the a-Al2O3. Alternatively, given thatthe serum concentration of Cr is only 0.01–0.03 mg/L[10–12], it is possible that there was sufficient surfacedissolution of the ceramic to increase the Cr serumconcentration such that cellular activity at the bone–ceramic interface was stimulated. However, sincealumina (and Cr-alumina solid solution) is exceedinglyinsoluble, as demonstrated by the complete absence of
detectable Cr in the leached samples, this latterexplanation is probably unlikely. Although the mechan-ism is unclear, the data show that cellular activity at thebone–ceramic interface was affected significantly by theaddition of Cr to the alumina ceramic.
5. Conclusions
The single-pore model has enabled the processes oftissue formation, osteogenesis, and bone remodellingwithin a porous bioinert structure to be quantifiedand enabled the effects on tissue responses of incorpor-ating specific elements to be determined. Althoughalumina is considered to be a bioinert ceramic withno direct bone-bonding ability [47], the incorporationof small amounts (nominally 0.5 or 5.0mol%) ofCa, Mn, or Cr in the ceramic significantly influencedtissue differentiation and osteogenesis within thetubes. This work suggests that the cellular response toa bioinert material, such as alumina, can be modulatedby the incorporation of small amounts of dopantelements. More investigation is needed to elucidate themechanism by which specific elements, either addeddeliberately or present as impurities, affect the cellularresponse and bone formation around orthopaedicimplants.
Acknowledgements
The authors gratefully acknowledge the NationalHealth and Medical Research Council, Australia forfunding this work.
References
[1] Al-Saffar N, Revell PA. Pathology of the bone-implant interfaces.
J Long-term Effects Medical Implants 1999;9:319–47.
[2] Masuda T, Yliheikkil.a PK, Felton DA, Cooper LF. General-
izations regarding the process and phenomenon of osseointegra-
tion, Part. I. In vivo studies. Int J Oral Maxillofac Implants
1998;13:17–29.
[3] Wieland M, Sittig C, Brunette DM, Textor M, Spencer ND.
Measurement and evaluation of the chemical composition and
topography of titanium implant surfaces. In: Davies JE, editor.
Bone engineering. Toronto: Em2 Inc, 2000. p. 163–82.
[4] Rothman RH, Hozack WJ, Ranawat A, Moriarty L. Hydro-
xyapatite-coated femoral stems. J Bone Joint Surg Am 1996;
78A:319–24.
[5] Klein CPAT, Patka P, van der Lubbe HB, Wolke JG, de Groot
K. Plasma-sprayed coatings of tetracalcium phosphate, hydro-
xyapatite and alpha-TCP on titanium: an interface study.
J Biomed Mater Res 1991;25:53–65.
[6] Ergun C, Webster TJ, Bizios R, Doremus RH. Hydroxylapatite
with substituted magnesium, zinc, cadmium, and yttrium. II.
Mechanisms of osteoblast adhesion. J Biomed Mater Res 2002;
59:312–7.
ARTICLE IN PRESSM.B. Pabbruwe et al. / Biomaterials 25 (2004) 4901–49104910
[7] Serre CM, Papillard M, Chavassieux P, Voegel JC, Boivin G.
Influence of magnesium substitution on a collagen-apatite
biomaterial on the production of a calcifying matrix by human
osteoblasts. J Biomed Mater Res 1998;42:626–33.
[8] Zhao Q, Zhai G-J, Ng DHL, Zhang X-Z, Chen Z-Q. Surface
modification of Al2O3 bioceramic by NH2+ ion implantation.
Biomaterials 1999;20:595–9.
[9] Heaney RP. Skeletal development and maintenance: the role of
calcium and vitamin d. Adv Endocrinol Metab 1995;6:17–38.
[10] Anderson RA. Chromium. In: Mertz W, editor. Trace elements in
human and animal nutrition, vol. 1. 5th ed. San Diego: Academic
Press; 1987. p. 225–44.
[11] Costa M. Toxicity and carcinogenicity of Cr (VI) in animal
models and humans. Crit Rev Toxicol 1997;27:431–42.
[12] McCarty MF. Anabolic effects of insulin on bone suggest a role
for chromium picolinate in preservation of bone density. Medical
Hypotheses 1995;45:241–6.
[13] Carlisle EM. Silicon. In: Mertz W, editor. Trace elements in
human and animal nutrition, vol. 2, 5th ed. San Diego: Academic
Press; 1987. p. 373–90.
[14] Carlisle EM. Biochemical and morphological changes associated
with long bone abnormalities in silicon deficiency. J Nutr
1980;110:1046–56.
[15] Carlisle EM. Silicon as an essential element for the chick. Science
1972;178:619–21.
[16] Hurley LS, Keen CL. Manganese. In: Mertz W, editor. Trace
elements in human and animal nutrition, vol. 1, 5th ed. San
Diego: Academic Press; 1987. p. 185–223.
[17] Clausen T, Dorup I. Micronutrients, minerals and growth
control. Bibl Nutritio Dieta 1998;54:84–92.
[18] Cashman K, Flynn A. Trace elements and bone metabolism. Bibl
Nutritio Dieta 1998;54:150–64.
[19] Saltman PD, Strause LG. The role of trace minerals in
osteoporosis. J Am College Nutrition 1993;12:384–9.
[20] Morais S, Souse JP, Fernandes MH, Carvalho GS. In vitro
biomineralization by osteoblast-like cells. Retardation of tissue
mineralization by metal salts. Biomat 1998;19:13–21.
[21] Wang JY, Wicklund BH, Gustilo RB, Tsukayama DT. Prosthetic
metals interfere with the functions of human osteoblast cells
in vitro. Clin Orthop Rel Res 1997;339:216–26.
[22] Sun ZL, Wataha JC, Hanks CT. Effects of metal ions on
osteoblast-like cell metabolism and differentiation. J Biomed
Mater Res 1997;34:29–37.
[23] Allen MJ, Myer BJ, Millet PJ, Rushton N. The effects of
particulate cobalt, chromium and cobalt-chromium alloy on
human osteoblast-like cells in vitro. J Bone Joint Surg Br
1997;79:475–82.
[24] Pabbruwe MB, Standard OC, Sorrell CC, Howlett CR. Use of an
intramedullary in vivo model to study bone formation and
maintenance in ceramic porous domains. J Biomed Mater Res
2004;68A:305–13.
[25] AS1774.5. Refractories and refractory materials—physical test
methods. Method 5: the determination of density, porosity and
water absorption. Sydney: Standards Association of Australia,
1989.
[26] ASTM E112-96. Standard test methods for determining average
grain size. West Conshohocken, PA: American Society for Testing
and Materials, 1996.
[27] National Health and Medical Research Council. The Australian
code of practice for the care, use of animals for scientific purposes,
6th ed. Canberra: Australian Government Publishing Services,
1997.
[28] Bennett HS, Wyrick AD, Lee SW, McNeil JH. Science and art in
preparing tissues embedded in plastic for light microscopy, with
special reference to glycol methacrylate, glass, knives and simple
stains. Stain Tech 1976;51:71–97.
[29] Nishikawa A. Technology of monolithic refractories. Tokyo:
Plibrico Japan Company Ltd.; 1984.
[30] Marks SC, Herney DC. The structure and development of bone.
In: Bilezikan JP, Raisz LG, Rodan GA, editors. Principles of
bone biology. San Diego: Academic Press; 1996. p. 9.
[31] Hansen SC, Phillips DS. Grain boundary microstructures in a
liquid-phase sintered alumina. Philos Mag 1983;47:209–34.
[32] Bae SI, Baik S. Determination of critical concentrations of silica
and/or calcia for abnormal grain growth in alumina. J Am Ceram
Soc 1993;76:1065–7.
[33] McCune RC, Ku RC. Calcium segregation to MgO and a-Al2O2surfaces. In: Kingery WD, editor. Advances in ceramics, vol. 10.
Structure and properties of MgO and Al2O2 ceramics. OH:
American Ceramic Society; 1984. p. 217–37.
[34] Li CW, Kingery WD. Solute segregation at grain boundaries in
polycrystalline alumina. In: Kingery WD, editor. Advances in
ceramics, vol. 10. structure and properties of MgO and Al2O2
ceramics. OH: American Ceramic Society; 1984. p. 368–78.
[35] Datta HK, MacIntyre I, Zaidi M. The effect of extracellular
calcium elevation on morphology and function of isolated rat
osteoclasts. Bioscience Rep 1989;9:747–51.
[36] Zaidi M, Kerby J, Huang CL, Alam T, Rathod H, Chambers TJ,
Moonga BS. Divalent cations mimic the inhibitory effect of
extracellular ionised calcium on bone resorption by isolated rat
osteoclasts: further evidence for a calcium receptor. J Cellular
Phys 1991;149:422–7.
[37] Levin EM, Robbins CR, McMurdie HF. Phase diagrams for
ceramists. OH: American Ceramic Society Inc.; 1986. p. 114.
[38] Wieland M, Sittig C, Brunette DM, Textor M, Spencer ND.
Measurement and evaluation of the chemical composition and
topography of titanium implant surfaces. In: Davies JE, editor.
Bone engineering. Toronto: Em2 Inc.; 2000. p. 163–82.
[39] Strause L, Saltman P, Glowacki J. The effect of deficiencies of
manganese and copper on osteoinduction and on resorption of
bone particles in rats. Calc Tiss Int 1987;41:145–50.
[40] Strause L, Hegenauer J, Saltman P, Cone R, Resnick D. Effects of
long-term dietary manganese and copper deficiency on rat
skeleton. J Nutr 1986;116:135–41.
[41] Leach RM, Gay CV. Role of epiphysial cartilage in endochondral
bone formation. J Nutr 1987;117:784–90.
[42] Reginster JY, Strause LG, Saltman P, Franchimont P. Trace
elements and postmenopausal osteoporosis: a preliminary study
of decreased serum manganese. Med Sci Res 1988;16:337–8.
[43] Friedman BJ, Freeland-Graves JH, Bales CW, Behmardi F,
Shorey-Kutschke RL, Willis RA, Crosby JB, Trickett PC,
Houston SD. Manganese balance and clinical observations in
young men fed a manganese-deficient diet. J Nutr 1987;117:
133–43.
[44] Bunting EN. Phase equilibrium in the system Cr2O3–Al2O3. Bur
Stds J Res 1931;6:947–9.
[45] Bondioli F, Ferrari AM, Leonelli C, Manfredini T, Linati L,
Mustarelli P. Reaction mechanism in alumina/chromia
(Al2O3–Cr2O3) solid solutions obtained by coprecipitation.
J Am Ceram Soc 2000;83:2036–40.
[46] Ryshkewitch E. Oxide ceramics. New York: Academic Press;
1960.
[47] Hench LL, Wilson J. Introduction to bioceramics. Singapore:
World Scientific; 1993.