blind runner
TRANSCRIPT

SURVEY OF OPHTHALMOLOGY VOLUME 57 � NUMBER 5 � SEPTEMBER–OCTOBER 2012
CLINICAL CHALLENGESPETER SAVINO AND HELEN DANESH-MEYER, EDITORS
Blind RunnerLaura Pelegrın, MD,1 Marina Mesquida, MD,1 Amanda Rey, MD,1
Bernardo Sanchez-Dalmau, MD,1 and Larry Frohman, MD2
1Department of Ophthalmology, Hospital Clınic de Barcelona, Barcelona, Spain; and 2Institute of Ophthalmology andVisual Science, New Jersey Medical School, Newark, New Jersey, USA
� 201All rig
(In keeping with the format of a clinical pathologic conference,the abstract and key words appear at the end of the article.)
Case Report
A 42-year-old man born in Pakistan was referredfor a painless, gradual decline in visual acuity over4 months in both eyes. He had no history ofdiabetes, hypertension, or other systemic diseases.His best-corrected visual acuity was 20/25 right eyeand 20/200 left eye. He had no relative afferentpupillary defect (RAPD), but his pupils reactedsluggishly to light, the left eye more than the right.Adnexae and ocular motility were normal. Slit lampexamination revealed bilateral neovascularizationof the iris with peripheral anterior synechiae ongonioscopy (Fig. 1A and B). The intraocular pres-sure was 10 mmHg in the right eye and 6 mmHg inthe left eye. Fundus examination showed numerousmicroaneurysms in the mid-peripheral retina andposterior pole, arteriovenous shunts between thesuperior and inferotemporal vessels of the arcade,arteriolar narrowing, and venous dilation withoutbeading in both eyes. In the left eye, neovasculari-zation of the optic disc and preretinal and vitreoushemorrhage were also present (Fig. 1C and D).
What is your initial formulation of this patient?
486
2 by Elsevier Inc.hts reserved.
Comments
COMMENTS BY LARRY FROHMAN, MD
This patient had no significant medical history,and developed iris neovascularization, synechiae (I donot know if uveitis was also present.), mid-peripheralmicroaneurysms, arteriovenous shunts, optic disc neo-vascularization, and preretinal and vitreous hemor-rhage. The lack of a RAPD suggests that there wasbilateral, relatively symmetric optic nerve involvement,which might be evident upon perimetry. This constel-lation of signs and symptoms suggests the presence ofocular ischemic syndrome (OIS). One possible cause ishigh grade atherosclerotic disease of the carotids. Wecould start the evaluation with carotid Doppler, butno matter what it would show, magnetic resonanceangiography (MRA) or computed tomographic angi-ography is also indicated. The selection of initial studymight be made based upon relative contraindications(not present in this patient) as well as the quality of thestudies at your facility. It would be unusual to havebilateral, although somewhat asymmetric, OIS bilater-ally on a carotid atherosclerotic basis in the absence of
0039-6257/$ - see front matterdoi:10.1016/j.survophthal.2011.06.004

Fig. 1. A and B: Anterior segment image of both eyes shows a prominent neovascularization of the iris stroma as a resultof anterior segment chronic ischemia. Gonioscopy also revealed angle neovascularization. C: Retinography of right eyeshowing numerous microaneurysms all over the posterior pole and the mid-peripheral retina with venous engorgement.D: Retinography of left eye showing neovascularization and aneurysmal dilatation on the optic disc, with preretinal andvitreous hemorrhage. Posterior pole shows multiple microaneurysms, venous dilation, and arterial narrowing. Note thedark coloration of retinal veins. E: Fundus fluorescein angiography of right eye shows staining of vascular walls,microaneurysms formation, and peripheral capillary nonperfusion. F: Fundus fluorescein angiography of left eye showsproliferative retinopathy with neovascularization of the optic disc and dye leakage. Blockage of colorant due to preretinalhemorrhage. There are staining of vascular walls and peripheral ischemia.
BLIND RUNNER 487
systemic disease that particularly targets these vessels.Furthermore, although atherosclerotic aortic diseaseproximal to the carotid takeoff could cause bilateral
ocular ischemia, it would be quite unusual to have thiswithout other neurologic signs or symptoms. I wouldask about symptoms related to global intermittent loss

TABLE 1
Differential Diagnosis
1) Atherosclerosisa) Primaryb) Coagulopathy induced
2) Posttraumatica) Dissections
3) Neoplasm/mass causing vasculopathy
488 Surv Ophthalmol 57 (5) September--October 2012 PELEGRIN ET AL
of perfusion of the brain, such as syncope or nearsyncope when arising from a lying or sitting position,memory deficits, etc. I would also inquire aboutsymptoms with changes in head position, neck flexion,or extension. The presence of arteriovenous shuntsindicates that this is a chronic process. In this case, theshunts are not the classic, wreath-like ring around thedisc described in OIS.37
a) Direct compression of large vessels by massb) Infiltrative (e.g., lymphoma, leukemia)
i) Angiocentric/hybrid entities(1) Lymphomatoid granulomatosis(2) Angioendotheliomatosis
4) Posttherapy (radiation induced)5) Infection
a) Syphilis6) Inflammation
a) Vasculitisi) Giant cell arteritisii) Cogan syndromeiii) Necrotizing vasculitides
(1) Polyarteritis nodosa(2) Wegener granulomatosis
iv) Kawasaki disease (e.g., if child with aorticinvolvement)
v) Takayasu arteritis7) Other
Case Report (Continued)
He was lost to follow-up until a few weeks later,when he presented to the emergency room withsudden, painless loss of vision in his left eye. He alsoreported headache, transient visual loss in his righteye for about 1 minute, and a syncopal attack. Hisacuities were 20/40 in his right eye and countingfingers in his left eye. His right pupil reacted poorly,and his left pupil was fixed and dilated. In addition tohis previously described findings, he also had a densecataract in his left eye. His fundus was unchanged.
Does this change your initial impressions?What further tests would you perform?
a) Susac syndromeb) Moyamoya
Comments (Continued)
COMMENTS BY DR. FROHMAN
With the history and examination, and nowsyncope and headache indicating intermittent cere-bral hypoperfusion, the differential diagnosis maybe framed by the usual categories of atherosclerosisor compromise of vascular lumen—either primaryor secondary to a coagulopathy—trauma, neoplasm,infection, inflammation, or other (Table 1).
OIS is caused by severe narrowing of the internalcarotid or its branches. This can be secondary toatherosclerosis, a coagulopathy, or possibly a traumaticlesion such as a dissection. Extrinsic compression of thecarotid by a mass such as an intracavernous meningi-oma may occasionally reduce carotid flow withoutfostering adequate collateral formation, inducing OIS.
On occasion, other neoplastic or related entities,such as lymphoma, leukemia, neoplastic angioendo-theliomatosis, or lymphomatoid granulomatosis,mayocclude vessels. If the carotid artery was in a priorfield of radiation, consideration must be given toradiation-induced vasculopathy.
Note that there were no pulses detected over bothradial and carotid arteries; this patient was pulseless.This indicates multifocality, making the infectious/inflammatory causes such as syphilis or vasculitismore likely. Pulselessness, in combination with theother clinical features and radiologic findings, willlikely lead to the diagnosis of Takayasu aterteritis(TA). Although giant cell arteritis has typically been
classified as a different vasculitis than TA, this maybe different phenotypic expressions of the samedisease.25 Other vasculitides, such as periarteritisnodosa or Wegener granulomatosis, can generally bedistinguished from TA by the organs affected and bycharacteristic histologic features. Kawasaki diseasewould rarely be mistaken for TA. When it has aorticinvolvement, this is typically in a very young child.Cogan syndrome is another vasculitis that can havea similar presentation to TA, but typically has morevestibular findings than does TA.5,11 Susac syndromeof encephalopathy, visual field defects from branchretinal artery occlusions, and hearing loss mayclinically overlap with TA, but does have radiologicevidence of large vessel disease.9 Moyamoya diseasemay have similar clinical features to TA, but is not aninflammatory condition and has a more limiteddistribution of involvement of the distal carotidsand proximal cerebral vessels than TA.20
I divide the investigations into those that may beperformed in my examination room, those that Imight perform within an ophthalmology depart-ment, and those serologic, radiologic, and otherinvestigations that would be performed outside ofthe department (Table 2). Not all tests are neededin all cases, and those in Group V will largely beordered by consulting physicians.
Pipitone et al give amore complete reviewof the useof various imagingmodalities (angiography, magnetic

TABLE 2
Evaluation Strategy
1) Group I—exam room testsa) Digital pulsations—do the central retinal arteries collapse with too gentle pressure?b) Ophthalmodynamometryc) Blood pressure, both armsd) Listen for axillary and carotid bruits
2) Group II—‘‘Ocular down the hall’’ testsa) Fluorescein angiography with transit time
3) Group III—Ocular ‘‘exotic’’ testsa) Color orbital Dopplerb) Oculoplethysmographyc) Laser Doppler flowmetry32
4) Group IV—Ocular delayed/secondary testinga) Electroretinography
5) Group V—‘‘Out of the office or building’’ testsa) Bloodwork
i) First stage(1) ESR, C-reactive protein, complete blood count with platelet count, VDRL, FTA-abs
ii) Second stage(1) ANA, ANCA, Lupus anticoagulant, antiphospholipid antibodies, serum protein electrophoresis,
cryoglobulins, complement studies, coagulopathy workup (in conjunction with hemotologist)b) Carotid Dopplersc) Dopplers Of Limbsd) B-mode ultrasonography
i) Raninen discussed the utility of measuring great vessel wall thickness, specifically looking at intimal, media,adventitial, and total wall thickness as a sign of TA.31
e) Echocardiographyf) Tilt testg) MRI brain with and without contrast with optic nerve viewsh) CTA or MRA or catheter angiographyi) PET scan
ANA 5 antinuclear antibody; ANCA5 antinuclear cytoplasmic antibody; CTA 5 computed tomographic angiography;ESR 5 erythrocyte sedimentation rate; FTA-abs 5 fluorescent treponemal antibody-absorption; MRA 5 magneticresonance angiography; MRI 5 magnetic resonace imaging; PET 5 positron emission tomography; TA 5 Takayasuarteritis; VDRL5 venereal disease research laboratory.
BLIND RUNNER 489
resonance imaging [MRI], computed tomography,ultrasound, positron emission tomographic [PET]scans) for both diagnosis and monitoring therapeuticefficacy in the large vessel vasculitides (TA and giantcell arteritis).30
Case Report (Continued)
Fundus fluorescein angiography revealed bilater-ally delayed arm to retina time (30 seconds),delayed and patchy choroidal filling, prolongedarteriovenous transit time, microaneurysms in mid-peripheral retina and posterior pole, and peripheralcapillary nonperfusion. Neovascularization over theleft disc was also evident (Fig. 1E and F).
Physical examination revealed bilterally absentradial and carotid pulses, and a bruit was heard inthe neck. Carotid duplex showed complete bilateralcommon carotid artery occlusion and severe steno-sis in the right subclavian artery.
Laboratory studies including completebloodcount,renal and liver function, clotting factors, antinuclearantibodies, antineutrophil cytoplasmatic antibodies,
rheumatoid factor, syphilis serology, antihuman im-munodeficiency virus, antihepatitis C virus and hepa-titis B surface antigen, andurinary sedimentationwerenormal. Abnormalities were a minor b-thalasemia, anerythrocyte sedimentation rate (ESR) of 40mm/hour,and a C-reactive protein of 3.20 mg/dL.
MRI disclosed microinfarctions in the cerebralparenchyma. An MRA showed no significant in-tracranial stenosis. Digital subtraction angiographyof the aorta and its branches demonstrated a severestenosis in the brachiocephalic trunk and leftsubclavian artery, filiform structures in the axillaryarteries, occlusion of both common carotid arteriesand the left vertebral artery, and hypertrophictirocervicoscapular trunk (Fig. 2). Echocardiogra-phy showed mild aortic root dilatation.
Which is your diagnosis now?
Comments (Continued)
COMMENTS BY DR. FROHMAN
My diagnosis is bilateral OIS from large vesselinvolvement in TA. In 1990, the American College

Fig. 2. Arteriography of aorta and its major branchesdemonstrated severe stenosis of the brachiocephalic trunkand the left subclavian artery, with obliteration of bothright and left common carotid arteries. It also demon-strated an hypertrophic tirocervicoscapular trunk withdevelopment of collateral circulation.
490 Surv Ophthalmol 57 (5) September--October 2012 PELEGRIN ET AL
of Rheumatology proposed six criteria for TA.2
Three are needed for diagnosis: 1) age !40 years,2) extremity claudication, 3) decreased brachialartery pulse, 4) $10 mm Hg difference in bloodpressure between the arms, 5) subclavian or aorticbruit, and 6) abnormal angiography of the aorta orits proximal branches.
Sharma et al proposed revisions to the 1988diagnostic criteria published by Ishikawa and to theAmerican College of Rheumatology criteria.13,35 Intheir schema, there was a high probability of having TAif one has either two major criteria, one major and twominor criteria, or four minor criteria: 1) major criteria:a) left mid subclavian artery lesion, b) right midsubclavian artery lesion, and c) characteristic signsand symptoms for at least 1 month; and 2) minorcriteria: a) high ESR, b) carotid artery tenderness, c)hypertension, d) aortic regurgitation, e) annuloaorticectasia, f) pulmonary artery lesion, g) leftmid commoncarotid lesion, h) distal brachiocephalic trunk lesion, i)descending thoracic aorta lesion, j) abdominal aorta
lesion, and k) coronary artery lesion. In Sharma et al’sseries of 106 cases, there was 92.5% sensitivity and 95%specificity, which was better than both the Ishikawa andthe 1990 American College of Rheumatology criteria.Nonetheless, it is clear that as newdiagnosticmodalitiesare available (e.g., PET scans) that these criteria willonce again need be modified.
It would be nice to see the reportedly normalMRA images to see if there was a quality or technicalissue that precluded making the diagnosis of TA inthis case. One series by Yamada et al concluded thatthe specificity and sensitivity of MRA for making thediagnosis of TA were both 100%.44 There is anemerging literature on the potential utility ofPET scanning, in conjunction with either MRI orcomputed tomography, as a means of both di-agnosing and monitoring disease activity in cases ofTA. Lee et al published a series on 32 patients withTA who underwent F-18 fluorodeoxyglucose PET--computed tomography. Some of the patients werescanned after they began immunosuppressive ther-apy. They determined that the sensitivity of PET was78% and the specificity was 87%. They also founda correlation between elevated ESR and C-reactiveprotein with having an abnormal PET--CT.23 Yet ina series by Arnaud et al, only 47% of TA patients hadan abnormal PET scan.3
Bartels et al reported a 24-year-old woman whohad negative MRI and MRA scans. A PET--MRI,detected disease activity in the vertebral arteries.4
This demonstrated that despite the Yamada series,the sensitivity of MRA was not 100%.
What treatments would you initiate?
Comments (Continued)
COMMENTS BY DR. FROHMAN
Prednisone, typically started at 0.5--1.0mg/kg/day,is the mainstay of systemic therapy for TA. Mainte-nance dosages of at least 15 mg/day are usuallyrequired to suppress disease activity.24 Immunosup-pressants such as methotrexate, azathioprine, andmycophenolate mofetil (MM) have been used suc-cessfully. Rodrıguez-Hurtado et al’s case of TA withocular involvement responded to monthly intrave-nous cyclophosphamide monotherapy.33 Goel et alhad a series of patients with TA who were bettercontrolled when treated with MM.12 Molloy et alfound that the antitumor necrosis factor agentsinfliximab and etanercept in TA allowed 60%of casesto be tapered off prednisone, and an additional 28%to decrease their maintenance dose below 10 mg.27
Beyond immunosuppression, a recent retrospec-tive study by deSouza et al suggested a salutary effectof antiplatelet drugs in preventing arterial ischemic

BLIND RUNNER 491
events in TA.8 Thus, in this case, presenting ata relatively advanced stage, I would begin medicaltherapy with 5 days of intravenous methylpredniso-lone at 1 g/day. This would be followed with long-term maintenance therapy beginning with 1 mg/kgof prednisone. I would also put the patient onaspirin. I would consult with rheumatology as towhat immunosuppressive or immunomodulatorthey prefer and would expect them to recommendmethotrexate, azathioprine, or MM. In this rapidlyprogressive and relatively advanced case, however, Imight push for intravenous cyclophosphamide asthe initial adjunct immunosuppressive, as its timeuntil onset of action is much more rapid than theother agents mentioned. If available, I would haveserum amyloid A drawn before starting treatment, asit may be a marker for disease activity duringtherapy.18 Another method of assessing systemictherapeutic efficacy may be a repeat PET scan, as inthe case of Iwabu’s patient, where PET after 6 weeksof therapy showed improvement as clinical symp-toms disappeared and the C-reactive proteinnormalized.14
There is a second arm of the therapeutic regimento consider. Besides systemic therapy, there isincreasing interest in developing surgery for thecerebral occlusive disease of TA. These includestents, transluminal angioplasty, and bypass grafts.One of the reasons that these therapies may berequired in many cases is that, by the time diagnosisof TA is made, significant vascular compromise ofthe cerebral vessels is already present. Furthermore,even when felt to be in remission, new vascularlesions can be demonstrated in 61% of cases of TA.Yet another reason is that despite medical therapywith prednisone and cytotoxic agents, most TApatients will experience progression of their vascu-lar disease. Liang and Hoffman list the indicationsto consider surgical therapy as: 1) cerebrovasculardisease due to cervicocranial vessel stenosis, 2)coronary artery disease, 3) moderate to severe aorticregurgitation, 4) severe coarctation of the aorta, 5)renovascular hypertension, 6) limb claudication,and 7) progressive aneurysm enlargement with riskof rupture or dissection.15,24
Endovascular therapy, with or without stenting,has been tried in TA. In cases that were felt to beinactive, Lee et al reported that endovasculartherapy with stenting provided a durable therapeu-tic response in 48 cases.21 Zhang et al reported onascending aorta to bilateral internal carotid arterybypass as a means of increasing cerebral perfusion,but raised the spectre of a potentially fatal reperfu-sion syndrome.45
Surgical options also exist in TA patients withlarge vessel disease of the cervical/cerebral vessels.
Moncada et al reported a case of TA refractory tohigh dose steroids who underwent two bypass-grafts.The first one, a GoreTex, 8 mm in diameter, thinwall, stretch type with ring-bypass graft, from the leftexternal iliac artery to the ipsilateral axillary artery.The second one, an autologous reverse saphenousvein graft from the left subclavian artery to theipsilateral common carotid artery, and showed greatimprovement.28
Visionmight improve after surgical reconstruction.Slusher and Richards reported a 25-year-old womanwith TA who underwent an ascending aorta to distalcommon carotid artery bypass.36 She had improve-ment in both her acuity bilaterally and a decrease inthe frequency of her amaurotic episodes withina month. Disc neovascularization regressed, andretinal circulatory disturbances improved.36 Yet, suchsurgical therapy is not without risk; Koz et al’s patientdied during bypass surgery.19 Fields et al reportedlong-term results in a series of 42 TA patients whorequired surgical therapy. His group found that at 5years, the percentage who did not require surgicalrevision was 100% in those who did not requiresteroids, and 95% in thosewhodid; the numbers at 10years were 100% and 81%, respectively.10
In this case, because this is severe multifocal greatvessel disease (brachiocephalic trunk, left subclavianartery, both common carotid arteries and the leftvertebral artery, as well as dilatation of the aorticroot), it mandates consultation with cardiothoracicand vascular services. Tracci and Cherry recentlyreviewed surgical therapies in TA.41
The standard approach to ocular treatment is toperform panretinal photocoagulation to reducemetabolic demands for oxygen. Chun et al remindedus that if systemic or surgical therapy significantlyimproves ocular perfusion, then intraocular pressuremay suddenly rise as the result of improved ciliarybody function. Adjunct therapies for glaucomamight be required.6 Whether there are indicationsfor local anti-vascular endothelial growth factor(VEGF) therapy, and whether these indications arecomplementary to surgical and/or endovascularreperfusion techniques are unanswered questions.
Case Report (Concluded)
This patient fulfills the American College ofRheumatology’s diagnostic criteria for TA.2 He hadOIS in both eyes and ischemic optic neuropathy inhis left eye. He was placed on prednisolone 60 mg/day, aspirin 100 mg/day, and oral methotrexate20 mg/week.
Because of opaque media in his left eye, panretinalphotocoagulation was not possible, so cataract surgery
492 Surv Ophthalmol 57 (5) September--October 2012 PELEGRIN ET AL
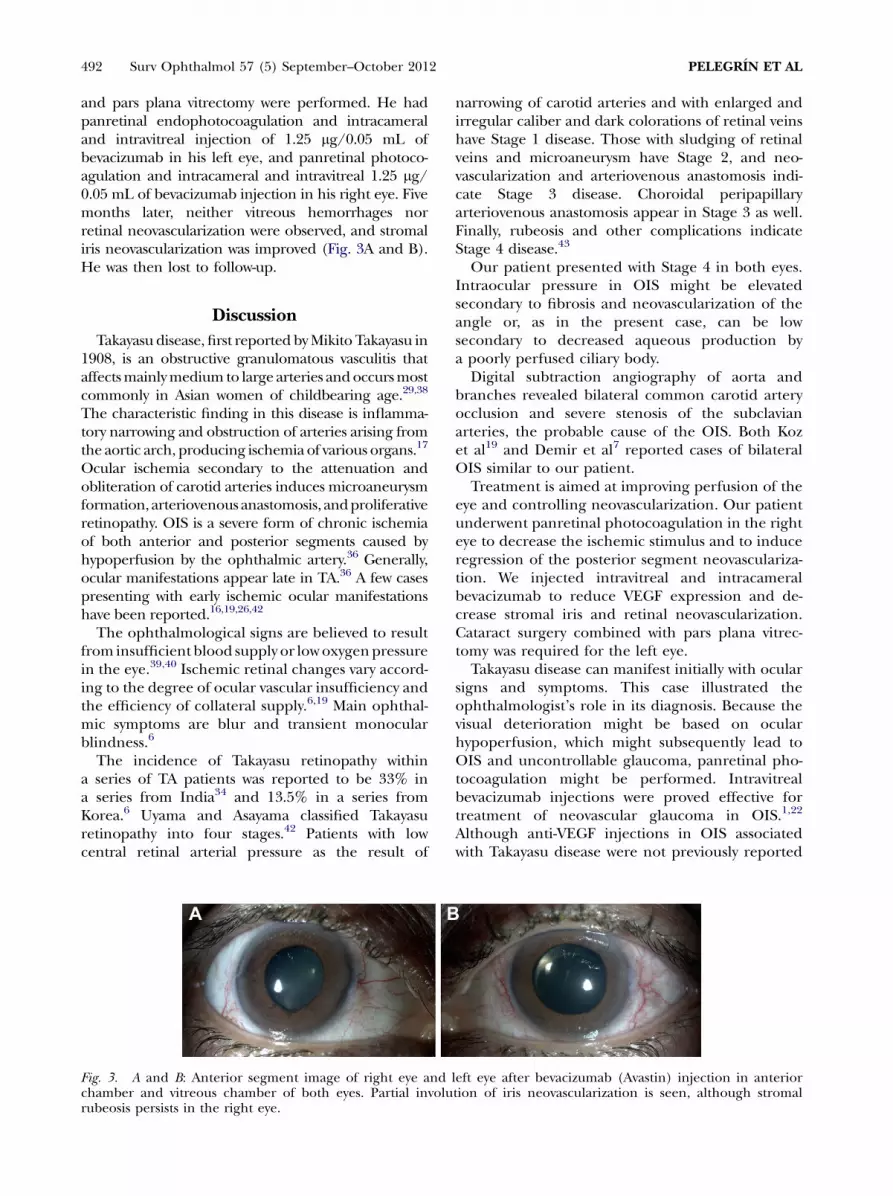
and pars plana vitrectomy were performed. He hadpanretinal endophotocoagulation and intracameraland intravitreal injection of 1.25 mg/0.05 mL ofbevacizumab in his left eye, and panretinal photoco-agulation and intracameral and intravitreal 1.25 mg/0.05 mL of bevacizumab injection in his right eye. Fivemonths later, neither vitreous hemorrhages norretinal neovascularization were observed, and stromaliris neovascularization was improved (Fig. 3A and B).He was then lost to follow-up.
Discussion
Takayasu disease, first reported byMikitoTakayasu in1908, is an obstructive granulomatous vasculitis thataffectsmainlymedium to large arteries andoccursmostcommonly in Asian women of childbearing age.29,38
The characteristic finding in this disease is inflamma-tory narrowing and obstruction of arteries arising fromthe aortic arch, producing ischemia of various organs.17
Ocular ischemia secondary to the attenuation andobliteration of carotid arteries induces microaneurysmformation, arteriovenous anastomosis, andproliferativeretinopathy. OIS is a severe form of chronic ischemiaof both anterior and posterior segments caused byhypoperfusion by the ophthalmic artery.36 Generally,ocular manifestations appear late in TA.36 A few casespresenting with early ischemic ocular manifestationshave been reported.16,19,26,42
The ophthalmological signs are believed to resultfrom insufficient blood supply or lowoxygenpressurein the eye.39,40 Ischemic retinal changes vary accord-ing to the degree of ocular vascular insufficiency andthe efficiency of collateral supply.6,19 Main ophthal-mic symptoms are blur and transient monocularblindness.6
The incidence of Takayasu retinopathy withina series of TA patients was reported to be 33% ina series from India34 and 13.5% in a series fromKorea.6 Uyama and Asayama classified Takayasuretinopathy into four stages.42 Patients with lowcentral retinal arterial pressure as the result of
Fig. 3. A and B: Anterior segment image of right eye andchamber and vitreous chamber of both eyes. Partial involurubeosis persists in the right eye.
narrowing of carotid arteries and with enlarged andirregular caliber and dark colorations of retinal veinshave Stage 1 disease. Those with sludging of retinalveins and microaneurysm have Stage 2, and neo-vascularization and arteriovenous anastomosis indi-cate Stage 3 disease. Choroidal peripapillaryarteriovenous anastomosis appear in Stage 3 as well.Finally, rubeosis and other complications indicateStage 4 disease.43
Our patient presented with Stage 4 in both eyes.Intraocular pressure in OIS might be elevatedsecondary to fibrosis and neovascularization of theangle or, as in the present case, can be lowsecondary to decreased aqueous production bya poorly perfused ciliary body.
Digital subtraction angiography of aorta andbranches revealed bilateral common carotid arteryocclusion and severe stenosis of the subclavianarteries, the probable cause of the OIS. Both Kozet al19 and Demir et al7 reported cases of bilateralOIS similar to our patient.
Treatment is aimed at improving perfusion of theeye and controlling neovascularization. Our patientunderwent panretinal photocoagulation in the righteye to decrease the ischemic stimulus and to induceregression of the posterior segment neovasculariza-tion. We injected intravitreal and intracameralbevacizumab to reduce VEGF expression and de-crease stromal iris and retinal neovascularization.Cataract surgery combined with pars plana vitrec-tomy was required for the left eye.
Takayasu disease can manifest initially with ocularsigns and symptoms. This case illustrated theophthalmologist’s role in its diagnosis. Because thevisual deterioration might be based on ocularhypoperfusion, which might subsequently lead toOIS and uncontrollable glaucoma, panretinal pho-tocoagulation might be performed. Intravitrealbevacizumab injections were proved effective fortreatment of neovascular glaucoma in OIS.1,22
Although anti-VEGF injections in OIS associatedwith Takayasu disease were not previously reported
left eye after bevacizumab (Avastin) injection in anteriortion of iris neovascularization is seen, although stromal

BLIND RUNNER 493
and further studies are needed, these appeared toinduce regression of neovascularization in this case.
Disclosure
The authors report no proprietary or commercialinterest in any product mentioned or conceptdiscussed in this article.
References
1. Amselem L, Montero J, Diaz-Llopis M, et al. Intravitrealbevacizumab (Avastin) injection in ocular ischemic syn-drome. Am J Ophthalmol. 2007;144:122--4
2. Arend WP, Michel BA, Bloch DA, et al. The AmericanCollege of Rheumatology 1990 criteria for the classifica-tion of Takayasu’s arteritis. Arthriotis Rheum. 1990;33:1129--34
3. Arnaud L, Haroche J, Malek Z, et al. Is (18)F-fluorodeox-yglucose positron emission tomography scanning a reliableway to assess disease activity in Takayasu arteritis? ArthritisRheumatol. 2009;60:1193--200
4. Bartels AL, Zeebregts CJ, Bijl M, et al. Fused FDG-PET andMRI imaging of Takayasu arteritis in vertebral arteries. AnnNucl Med. 2009;23:753--6
5. Bielory LB, Conti J, Frohman LP. Cogan’s Syndrome.J Allergy Clin Immunol. 1990;85:808--15
6. Chun YS, Park SJ, Park IK, et al. The clinical and ocularmanifestations of Takayasu arteritis. Retina. 2001;21:132--140
7. Demir MN, Hazirolan D, Altiparmak UE, et al. Takayasu’sdisease and secondary ocular ischemic syndrome. J PediatrOphthalmol Strabismus. 2010;47:54--7
8. de Souza AW, Machado NP, Pereira VM, et al.Antiplatelet therapy for the prevention of arterialischemic events in Takayasu arteritis. Circulation. 2010;74:1236--41
9. Dorr J, Radbruch H, Bock M, et al. Encephalopathy,visual disturbance and hearing loss-recognizing thesymptoms of Susac syndrome. Nat Rev Neurosc. 2009;5:683--8
10. Fields CE, Bower TC, Cooper LT, et al. Takayasu’s arteritis:operative results and influence of disease activity. J VascSurg. 2006;43:64--71
11. Gaubitz M, Lubben B, Seidel M, et al. Cogan’s syndrome:organ-specific autoimmune disease or systemic vasculitis? Areport of two cases and review of the literature. Clin ExpRheumatol. 2001;19:463--9
12. Goel R, Danda D, Matthew J, Edwin N. Mycophenolatemofetil in Takayasu’s arteritis. Clin Rheumatol. 2010;29:329--32
13. Ishikawa K. Diagnostic approach and proposed criteria forthe clinical diagnosis of Takayasu’s arteriopathy. J Am CollCardiol. 1988;12:964--72
14. Iwabu M, Yamamoto Y, Dobashi H, et al. F-18 FDG PETfindings of Takayasu arteritis before and after immunosup-pressive therapy. Clin Nucl Med. 2008;33:872--3
15. Kerr GS, Hallahan CW, Giordano J, et al. Takayasu arteritis.Ann Intern Med. 1994;120:919--29
16. Kimura H, Masai H, Kashii S. Anterior ischemic opticneuropathy associated with pulseless disease. Ophthalmo-logica. 1995;209:346--8
17. Kiyosawa M, Baba T. Ophthalmological findings in patientswith Takayasu disease. Int J Cardiol. 1998;66:141--7
18. Koga T, Nishino Y, Makiyama J, et al. Serum amyloid A isa useful marker to evaluate the disease activity of Takayasu’sarteritis. Rheumatol Int. 2010;30:561--3
19. Koz OG, Ates A, Alp MN, et al. Bilateral ocular ischemicsyndrome as an initial manifestation of Takayasu’s arteritis
associated with carotid steal syndrome. Rheumatol Int. 2007;27:299--302
20. Kraemer M, Berlit P. Primary central nervous systemvasculitis and moyamoya disease: similarities and differ-ences. J Neurol. 2010;257:816--9
21. Lee BB, Laredo J, Neville R, Villavicencio JL. Endovascularmanagement of Takayasu arteritis: is it a durable option?Vascular. 2009;17:138--46
22. Lee SJ, Lee JJ, Kim SY, Kim SD. Intravitreal bevacizumab(Avastin) treatment of neovascular glaucoma in ocularischemic syndrome. Korean J Ophthalmol. 2009;23:132--134
23. Lee SG, Ryu JS, Kim HO, et al. Evaluation of disease activityusing F-18 FDG PET-CT in patients with Takayasu arteritis.Clin Nucl Med. 2009;34:749--52
24. Liang P, Hoffman GS. Advances in the medical and surgicaltreatment of Takayasu arteritis. Curr Opin Rheumatol. 2005;17:16--24
25. Maksimowicz-McKinnon K, Clark TM, Hoffman GS. Takaya-su arteritis and giant cell arteritis: a spectrum within thesame disease? Medicine. 2009;88:221--6
26. Malik KP, Kapoor K, Mehta A, et al. Bilateral anteriorischaemic optic neuropathy in Takayasu arteritis. IndianJ Ophthalmol. 2002;50:52--4
27. MolloyES,LangfordCA,ClarkTM,et al. Anti-tumournecrosisfactor therapy in patients with refractory Takayasu arteritis:long-term follow-up. Ann Rheum Dis. 2008;67:1567--9
28. Moncada G, Kobayashi Y, Kaneko E, et al. Subclavian stealsyndrome secondary to Takayasu arteritis. Int J Cardiol.1998;66(suppl 1):S231--6
29. Nasu T. Pathology of pulseless disease. A systematic studyand critical review of twenty-one autopsy cases reported inJapan. Angiology. 1963;14:225--42
30. Pipitone N, Versari A, Salvarani C. Role of imaging studies inthe diagnosis and follow-up of large-vesselv asculitis: anupdate. Rheumatology. 2008;47:403--8
31. Raninen RO, Kupari MM, Pamilo M, et al. Arterial wallthickness measurements by B mode ultrasonography inpatients with Takayasu’s arteritis. Ann Rheum Dis. 1996;55(7):461--5
32. Riva CE, Geiser M, Petrig BL, for the Ocular Blood FlowResearch Association. Ocular blood flow assessment usingcontinuous laser Doppler flowmetry. Acta Ophthalmol.2010;88:622--9
33. Rodrıguez-Hurtado FJ, Sabio JM, Lucena J, Jimenez-Alonso J. Ocular involvement in Takayasu’s arteritis: re-sponse to cyclophosphamide therapy. Euro J Med Res. 2002;7:128--30
34. Sagar S, Kar S, Gupta A, Sharma BK. Ocular changes inTakayasu’s arteritis in India. Jpn J Ophthalmol. 1994;38:97--102
35. Sharma BK, Jain S, Suri S, Numano F. Diagnostic criteriafor Takayasu arteritis. Int J Cardiol. 1996;54(suppl 1):S127--S133
36. Slusher MM, Richards CP. Postsurgical alterations in visualacuity, retinal vasculature, and retinal circulation times inTakayasu’s disease. Retina. 2002;22:116--7
37. Sugiyama K, Ijiri S, Tagawa S, Shimizu K. Takayasu diseaseon the centenary of its discovery. Jpn J Ophthalmol. 2009;53:81--91
38. Takayasu M. A case with peculiar changes of central retinalvessels. Acta Soc Ophthal Jpn. 1908;12:554--5
39. Tanaka T, Muraoka K, Tokui K. Retinal arteriovenous shuntat the arteriovenous crossing. Ophthalmology. 1998;105:1251--8
40. Tanaka T, Shimizu K. Retinal arteriovenous shunts inTakayasu disease. Ophthalmology. 1987;94:1380--8
41. Tracci MC, Cherry KJ. Surgical treatment of great vesselocclusive disease. Surg Clin N Am. 2009;89:821--36, viii.
42. Uyama M, Asayama K. Retinal vascular changes in Takayasu’sdisease (pulseless disease), occurrence and evolution of thelesion, in De Laey JJ (ed) International symposium onfluorescein angiography: The Ghent, March 28--April 1,1976. Hague, W Junk, 1976, pp 549--54

494 Surv Ophthalmol 57 (5) September--October 2012 PELEGRIN ET AL
43. Worrall M, Atebara N, Travis M, Mann E. Bilateralocular ischemic syndrome in Takayasu disease. Retina.2001;21:75--6
44. Yamada I, Nakagawa T, Himeno Y, et al. Takayasu arteritis:diagnosis with breath-hold contrast-enhanced three-dimensional MR angiography. J Magn Reson Imaging.2000;11:481--7
45. Zhang B, Wang Z, Huang Y, et al. Aortobilateral axillarybypass to treat severe cerebral ischemia due to Takayasu’sarteritis. Ann Vasc Surg. 2009;23:689.e7--10
Reprint address:LauraPelegrın,MD, InstitutClınicd’Oftalmologia(ICOF),Hospital Clınic i Provincial deBarcelona, C/SabinoAranan�1, 08028, Barcelona, Spain. e-mail: [email protected].
Abstract. Bilateral ocular ischemic syndrome and ischemic optic neuropathy have rarely beenreported as initial manifestations of Takayasu arteritis (TA). Appearance of ocular symptoms in TA isrelated to the extent and severity of involvement of the aorta and its major branches. We report a caseof bilateral ocular ischemic syndrome with unilateral ischemic optic neuropathy secondary to TA ina 42-year-old Pakistani man who had severe ocular and cerebral ischemia. (Surv Ophthalmol 57:486--494, 2012. � 2012 Elsevier Inc. All rights reserved.)
Key words. ischemic optic neuropathy � ocular ischemic syndrome � Takayasu arteritis �Takayasu retinopathy