barriers to evidence‐based nursing: a focus group study
TRANSCRIPT

Barriers to evidence-based nursing: a focus group study
Karin Hannes, Jo Vandersmissen, Liesbeth De Blaeser, Gert Peeters, Jo Goedhuys & Bert Aertgeerts
Accepted for publication 15 June 2007
Correspondence to K. Hannes:
e-mail: [email protected]
K. Hannes MSc
Research Fellow
Belgian Centre for Evidence-Based Medicine,
Belgian Branch of the Cochrane
Collaboration, Leuven, Belgium
J. Vandersmissen MSc RN
Staff Member, Nursing Unit
University Hospital Leuven, Leuven, Belgium
L. De Blaeser MSc RN
Staff Member, Nursing Unit
University Hospital Leuven, Leuven, Belgium
G. Peeters MSc RN
Program Coordinator
Belgian Health Care Knowledge Centre,
Brussels, Belgium
J. Goedhuys PhD
Professor
Catholic University Leuven-Academic Centre
for General Practice, Leuven, Belgium
B. Aertgeerts PhD MD
Professor
Belgian Centre for Evidence-Based Medicine,
Belgian Branch of the Cochrane
Collaboration, Leuven, Belgium and Catholic
University Leuven-Academic Centre for
General Practice, Leuven, Belgium
HANNES KHANNES K., VANDERSMISSEN JVANDERSMISSEN J., DEDE BLAESER LBLAESER L., PEETERS GPEETERS G., GOEDHUYS J.GOEDHUYS J.
&& AERTGEERTS B. (2007)AERTGEERTS B. (2007) Barriers to evidence-based nursing: a focus group
study. Journal of Advanced Nursing 60(2), 162–171
doi: 10.1111/j.1365-2648.2007.04389.x
AbstractTitle. Barriers to evidence-based nursing: a focus group study
Aim. This paper reports a study to explore the barriers to evidence-based nursing
among Flemish (Belgian) nurses.
Background. Barriers obstructing the call for an increase in evidence-based nursing
have been explored in many countries, mostly through quantitative study designs.
Authors report on lack of time, resources, evidence, authority, support, motivation
and resistance to change. Relationships between barriers are seldom presented.
Methods. We used a grounded theory approach, and five focus groups were
organized between September 2004 and April 2005 in Belgium. We used purposeful
sampling to recruit 53 nurses working in different settings. A problem tree was
developed to establish links between codes that emerged from the data.
Findings. The majority of the barriers were consistent with previous findings.
Flemish (Belgian) nurses added a potential lack of responsibility in the uptake of
evidence-based nursing, their ‘guest’ position in a patient’s environment leading to a
culture of adaptation, and a future ‘two tier’ nursing practice, which refers to the
different education levels of nurses. The problem tree developed serves as (1) a basic
model for other researchers who want to explore barriers within their own
healthcare system and (2) a useful tool for orienting change management processes.
Conclusion. Despite the fact that the problem tree presented is context-specific for
Flanders (Belgium), it gives an opportunity to develop clear objectives and targeted
strategies for tackling obstacles to evidence-based nursing.
Keywords: barriers, empirical research report, evidence-based nursing, focus
groups, qualitative research
Background
Over the past few years, concerns have been growing about
the use of evidence-based nursing (EBN) in health care.
Nurses at all levels are increasingly expected to use evidence
in a conscientious, explicit and judicious way. In Flanders
(Belgium), many barriers obstruct the calls for an increase in
EBN. We searched The Cochrane Database of Systematic
Reviews, ACP Journal Club, DARE, Medline, Sociological
Abstracts and CINAHL from 1998 up until spring 2006 to
gain insight into the reasons why nurses are not using
evidence in daily practice.
We found more than 25 quantitative studies that had used
the BARRIERS scale, developed and tested by Funk et al.
ORIGINAL RESEARCHJAN
162 � 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd

(1991a, 1991b, 1995a, 1995b). French (2005) has summar-
ized most of these contributions. There is a high degree of
consistency in reporting ‘setting’ or ‘environment’ as an
important barrier. Setting includes inadequacy of facilities or
available equipment, lack of resources and time, lack of
support or cooperation from doctors and supervisors and
lack of authority to handle clinical problems. Problems such
as a lack of relevant evidence, conflicting results in literature,
information overload, lack of computer skills, difficulties in
interpreting statistical data, difficulties in generalizing re-
search results and applying them to daily practice are also
frequently mentioned. Similar outcomes are reported by other
authors using the BARRIERS scale or other quantitative
techniques (Walsh 1997, Sitzia 2001, McCleary 2003, Olade
2003, Sommer 2003, Kirshbaum et al. 2004, McKnight
2004, Mazurek Melnyk et al. 2004, Micevski et al. 2004,
Kenny 2005, Paramonczic 2005, Pravikoff et al. 2005).
Additional barriers reported include limited funding for
nursing research and a lack of incentives for evidence-based
action (Tsai 2000, Olade 2003, Pravikoff et al. 2005). Some
barriers relate to nurses themselves: attitudes, unwillingness
to participate in the EBN process, an anti-research culture or
anti-teamwork spirit, lack of motivation and fear of change
(Retsas 2000, Andrew & Kinn 2001, Sitzia 2001, Bryar et al.
2003, Carrion et al. 2004, Kirshbaum et al. 2004, Mazurek
Melnyk et al. 2004).
We found a limited number of qualitative studies addres-
sing barriers to EBN. The majority of the findings were
consistent with the results from quantitative studies (Adams
2001, McCaughan et al. 2002, Adamsen et al. 2003) . Some
additional barriers were mentioned, such as the influence of
pharmaceutical companies (French 2005), the time-delay
between publication of research results and their implemen-
tation in practice (Thompson 2003), a culture that favours
‘acting’ over ‘thinking’, a strong hierarchical structure,
difficulties in managing innovation and an inadequate system
for personal and professional development (Newman et al.
1998), patients’ experience as the driving force for nurses
(Rycroft-Malone et al. 2004), resistance to change and lack
of motivation (Ring et al. 2005). Few qualitative studies have
discussed relationships between the different barriers inven-
toried. Opportunities to develop targeted strategies to tackle
the obstacles experienced by nurses are therefore limited.
The study
Aim
The aim of this study was to explore the barriers to EBN
among Flemish (Belgian) nurses. The research objectives
were: (1) to make sense of the meaning, expectations,
attitudes and suggestions Flemish (Belgian) nurses bring to
EBN; (2) to explore whether the results of the study matched
previous insights from international research; (3) to develop a
problem tree linking all barriers so as to contribute to the
discussion about which obstacles can be tackled before nurses
will be able to integrate EBN in daily practice.
Methodology
The methodology was guided by a ‘grounded theory
approach’ (Strauss & Corbin 1997). Rather than beginning
with a particular theory on the implementation of EBN, we
started by examining problems in daily nursing practice,
using focus groups, and developed a conceptual framework
consistent with what we were observing. Data collection and
data analysis were concurrent. Data were collected and
analysed between October 2004 and October 2005.
Participants
Purposive sampling was used to recruit a total of 53 nurses,
based on four criteria: (1) variability of interest in EBN, (2)
variability of expertise in EBN, (3) geographical variability
and (4) variability in ‘setting’. We recruited between six and
12 participants for each focus group. Group I consisted of
seven academics who were chosen for their reputation as
good informants on EBN. Group II consisted of eight nurses
working in a hospital setting. Group III consisted of 12 nurses
providing home care. In Group IV, nine nurses who were
enrolled in an educational programme in pain management
participated, and for group V seven nurses working with
older patients participated.
Data collection
Five focus groups were conducted. An independent moder-
ator was hired to facilitate the discussions, using a semi-
structured interview guide. Two researchers took notes on the
non-verbal behaviour of participants. These notes are pre-
sented alongside the citations used in the findings section
below. Two major topics were discussed: (1) Applicability of
EBN and (2) Specific barriers to implement EBN. The focus
group discussions lasted between 1Æ5 and 2 hours.
Validity and reliability
Reliability was assured by recording and transcribing the
interview excerpts, using independent researchers from dif-
ferent disciplines to code data. Inter-rater agreement between
JAN: ORIGINAL RESEARCH Barriers to evidence-based practice
� 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd 163
researchers ranged from 87% to 92%. Validity was assured
by describing the sample, the process of data collection and
analysis in detail. We used an independent moderator to
ensure that no influences from the research team occurred
during the focus group interviews. The results were validated
through a process of triangulation with existing literature.
Ethical considerations
All nurses in the sample had given their consent to participate
in the focus group. The research team presented a written
statement, in which they guaranteed that all data were to be
analysed anonymously and explained that individual talks
with members of the research team were possible, after the
focus group had finished.
Data analysis
We used the software program ATLAS-ti (5Æ0) (The ATLAS-ti
Center, Berlin, Germany) to analyse the data. A thematic
analysis was conducted (Benner 1985, Leininger 1985) and
refined by an inductive process of open and axial coding. We
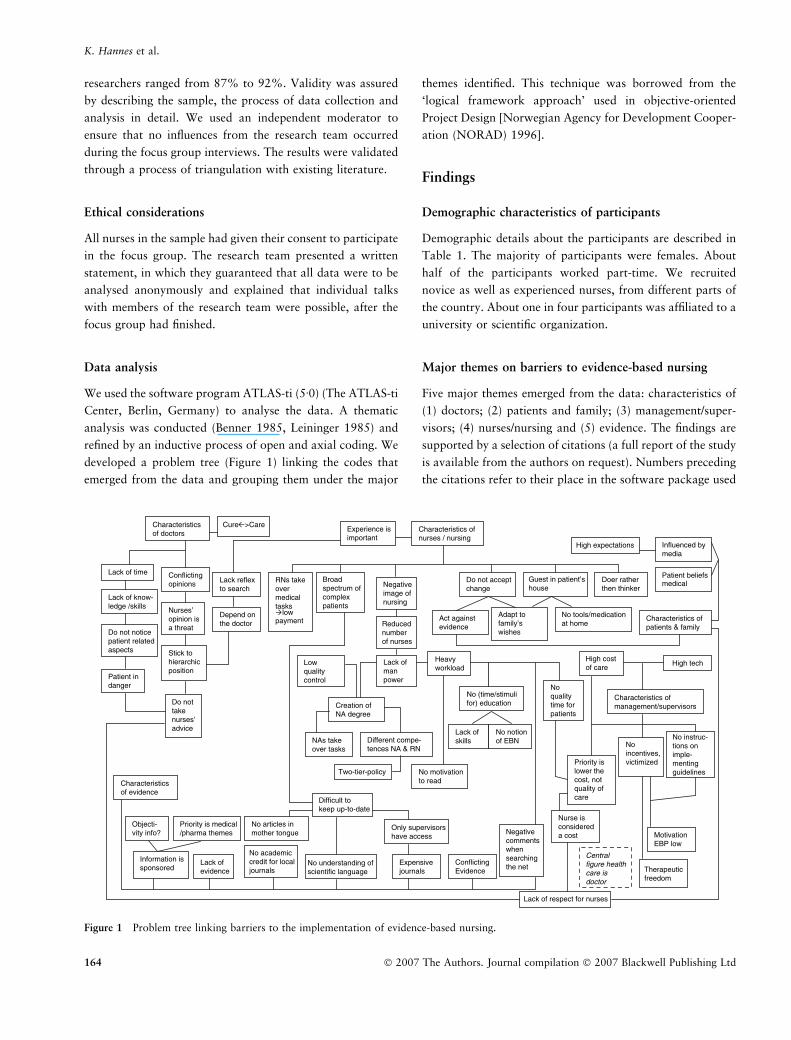
developed a problem tree (Figure 1) linking the codes that
emerged from the data and grouping them under the major
themes identified. This technique was borrowed from the
‘logical framework approach’ used in objective-oriented
Project Design [Norwegian Agency for Development Cooper-
ation (NORAD) 1996].
Findings
Demographic characteristics of participants
Demographic details about the participants are described in
Table 1. The majority of participants were females. About
half of the participants worked part-time. We recruited
novice as well as experienced nurses, from different parts of
the country. About one in four participants was affiliated to a
university or scientific organization.
Major themes on barriers to evidence-based nursing
Five major themes emerged from the data: characteristics of
(1) doctors; (2) patients and family; (3) management/super-
visors; (4) nurses/nursing and (5) evidence. The findings are
supported by a selection of citations (a full report of the study
is available from the authors on request). Numbers preceding
the citations refer to their place in the software package used
Lack of time
Characteristicsof doctors
Characteristics ofpatients & family
Characteristics ofnurses / nursing
Characteristicsof evidence
Characteristics ofmanagement/supervisors
Do not acceptchange
Patient beliefs medical
Act againstevidence
Lack of know-ledge /skills
Influenced bymedia
High expectations
No academiccredit for local journals
No articles inmother tongue
No understanding ofscientific language
No motivationto read
Expensivejournals
Only supervisorshave access
Broadspectrum ofcomplexpatients
Noincentives,victimized
Nurses’opinion isa threat
Do not noticepatient relatedaspects
Do nottakenurses’advice
Patient indanger
Stick tohierarchicposition
Difficult to keep up-to-date
ConflictingEvidence
Lack ofevidence
Guest in patient’shouse
Adapt tofamily’swishes
No tools/medicationat home
Experience isimportant
Lack reflexto search
Depend onthe doctor
Negativeimage ofnursing
Reducednumberof nurses
Lack of respect for nurses
Heavyworkload
Negativecommentswhensearchingthe net
Lack ofmanpower
Noqualitytime forpatients
No (time/stimulifor) education
No notionof EBN
Lack ofskillsNAs take
over tasks
Two-tier-policy
Different compe-tences NA & RN
High costof care
Nurse isconsidereda cost
No instruc-tions onimple-mentingguidelines
Priority islower thecost, notquality ofcare
Information issponsored
Objecti-vity info?
Priority is medical/pharma themes
Creation of NA degree
RNs takeovermedicaltasks
lowpayment
Doer ratherthen thinker
MotivationEBP low
Lowqualitycontrol
Conflictingopinions
Centralfigure healthcare is doctor
Cure >Care
High tech
Therapeuticfreedom
Figure 1 Problem tree linking barriers to the implementation of evidence-based nursing.
K. Hannes et al.
164 � 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd

and include (1) the focus group, (2) the statement made and
(3) the ID of the participant. Abbreviations used in the
citations refer to codes used by the observers: I is agreement,
O is denial and G is type of behaviour, followed by the ID-
number of a participant.
Characteristics of doctors
In general, nurses work under the supervision of doctors,
leading to a very dependent position with limited space for
autonomous decisions. Contradicting doctors’ opinions is ex-
tremely difficult, particularly for the older generation of nurses:
2:62:3: A number of doctors would consider it strange if you as a
nurse were to say ‘Yes but doctor, it is the rule here to keep patients
in bed for 12 hours after a heart catheterization’…If we take a look
in the literature…6 hours are sufficient. And then comes the reaction;
yes but where do you suddenly get that from…I am the one who…
Nurses doubt the ability of doctors to remain up-to-date on
important issues of daily practice. Additionally, doctors do
not always notice important patient-related aspects. It could
lead to a potentially dangerous situation for the patient as
well as the care provider:
10:105:3: I see things in the file that the physician has simply
disregarded and then I think about allergies or a previous operation and
hepatitis for the protection of the nurse…things that just do not interest
them or they have just passed over in the electronic dossier…(G: I: 2).
Proposals for the development of clinical pathways and
nurses’ opinions are sometimes experienced as a threat.
Doctors may deliberately decide to do the opposite in order
to reaffirm their dominant position, even in domains where
nurses have gained specific expertise:
5:17:2: On the subject of wound care, among other things…we are
actually regularly overruled. Would you believe it? We often find that
we have more insight into wound care than they do, but they do not
acknowledge that and would like to enforce their own way of
thinking.
From the nurses’ perspective, doctors are more willing to take
or ask advice from physiotherapists or dieticians. While
doctors tend to focus on cure, nurses give more attention to
comfort and care. According to some participants this
contributes to the incongruity of opinions. In response to
their position on the hierarchical ladder, nurses admit lacking
the reflex to search for solutions themselves and automatic-
ally delegate responsibility to the doctor. It places them in a
dependent position:
2:37:3: If they get round to serious discussions, then they will very
often refer the problem to another care provider; hence, ‘We need a
doctor for this problem’ not always the reflex of ‘What added value
can I offer as a nurse?’
Nurses also address the gap between the younger generation
of doctors and the rigid older generation, a problem that
should solve itself in the long term.
Characteristics of patients and family
Relations with patients differ between different types of
nurses. Nurses providing home-based care seem more likely
to compromise on ‘evidence’ because they considered them-
selves ‘guests’ in the private world of the patients:
5:53:10: In a hospital patients enter into your world, but you enter
their world and I think that however you try and get round it (G: I:
4), you will always have to make some concessions, you have to learn
to accept a bit; you can explain something, you can be occupied for
weeks or months with something, but you are dealing with human
nature…Yes, somehow introduce ‘respect’. These people are not little
children.
Sometimes, the patients do not have the right equipment,
tools or medicine at home, which is another obstacle to
providing the best possible care. Nurses often adapt to
patients’ wishes and expectations, even though the solution a
nurse proposes makes more sense. Some patients act entirely
against the advice that is given, or the patient’s family has
insisted on different treatment. In the case of a significant
change in scientific knowledge regarding certain treatments,
it seems particularly hard to convince patients and those
around them to accept it:
Table 1 Participant demographics (n = 53)
Sex
Male (%) 7 16Æ7Female (%) 35 83Æ3
Average age (min/max) 35 21/49
Average year of graduation (SDSD) 1991 8Æ708
Province
Antwerp (%) 3 7Æ1Brabant (%) 13 31
Limburg (%) 5 11Æ9East Flanders (%) 16 38Æ1West Flanders (%) 5 11Æ9
Average years of practice (SDSD) 12Æ39 8Æ203
% Present in practice*
Full-time (%) 18 42Æ9Part-time (%) 15 45Æ5
Affiliated with university or
scientific organization�
Yes (%) 11 26Æ2No (%) 29 69
*Nine missing values, mostly from academics working for univer-
sities; �Two missing values.
JAN: ORIGINAL RESEARCH Barriers to evidence-based practice
� 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd 165

6:27:2: Once again it is the grandparent or the family who also from
their experience have other ideas, the general public’s view. Also,
when science has changed you really have to slog away to convince
people to get them to be with you on this point. (G: I: 5, 6).
Keeping up-to-date with scientific literature is extremely
difficult. Nurses work with patients with multiple patholo-
gies, especially those in home-based care settings or geriatric
units. Several nurses mention the lack of respect for their
work, from doctors as well as patients and their families.
Patients value doctors’ advice more than nurses’ opinions:
11:213:7: The more I look, the more I see nurses being treated as
fools (G: smiles: 6, 02) by many people and that really grieves me. I
notice that my people have a real need for appreciation, to feel they
are a full partner in the dialogue, to be respected and that on all sides
they are no longer accorded that respect, neither by the patients, not
in the least by the visitors but also not always by the doctors, and yet
we still go on trying to bring about that joint ownership with doctors.
Patients are also heavily influenced by less objective infor-
mation presented through the media. These messages result in
high expectations that cannot be fulfilled:
2:48:3: I think that many patients do generate an area of tension for
nurses. They can come up with a solution that they have seen in
[popular magazine] or on the internet or in a journal. ‘I have seen
there that such-and-such offers a solution; can you help me with
this?’ (G: smile: 6, 7). Actually, it is really an additional obstacle to
delivering evidence-based (EB) health care because you are confron-
ted with expectations of your patient and their family that do not
directly match with what you are doing…
Characteristics of management/supervisors
Management priorities differ from those of nurses. Managers
are mainly interested in how to control the costs of health
care. Nurses seem to be more concerned with the quality of
care. When targets in a certain unit of a hospital or institute
are not reached, it is the nursing staff that decreases, while the
medical staff remains the same. Nurses state that they are too
easily reduced to a cost:
11:131:6: And now I am just going to speak for hospitals. If we do
not achieve the targets that we have been set, then we get fewer
people, but the staff of physicians remains the same. In the end they
determine what the targets are (G: I: 4)…everything revolves around
the physician, this is exactly our feeling; who is here and now still
central, the patient or the physician? (G: I: 2).
Many managers and supervisors are proponents of imposing
guidelines. However, there are no clear instructions on how
to integrate them into daily care. Even if the guidelines are
feasible in practice there are no penalties for those who act
otherwise. According to some nurses, doctors still use their
therapeutic freedom as an excuse to neglect guidelines:
11:225:02: Would it not help doctors and other health workers if
they begin to appreciate that everything that appears in the literature
in guidelines, for example, regarding pain and so forth, is really a
restriction of their therapeutic freedom? If that is good practice, then
you as a doctor can surely not permit yourself to say ‘and now I am
going to do it differently’. If I did it differently, I would be
committing a professional error.
Characteristics of nurses/nursing
The general culture of practice. There is a strong resistance
and low interest within the group of nurses to adapt to
evidence-based treatments. According to a supervising nurse,
the resistance is greater for routine treatments than for
recently developed treatments:
11:184:3: The nearer it (evidence) comes to what you routinely
undertake, the more resistance you experience to changing things.
Washing, for example every day everyone must be washed, that is
something that you cannot discuss with nurses, because we have been
doing that for years. Every day we wash everyone from top to toe and
so this practice continues unchanged…On the other hand, things
such as analgesia, palliative care, things that were added on later, are
much easier to discuss (G: I: 1, 2, 4/laughter: 5).
Nurses who are motivated to invest in an evidence-based
approach fear the negative comments of others, for example,
when searching the web, because it creates a bigger work-
load. A reference nurse providing home-based care, as well as
several nurses working in a geriatric setting, state that they
mostly rely on experience. They tend to look back at the
process they have gone through with former patients to solve
a problem, instead of taking into account results from
theoretical studies:
11:180:5: What I also see is that some decisions are taken informally
in a rest home (G: I: 4)…nurses see a particular problem and then
they are going to link that back to residents that they have known:
‘What problem have we had there, what was important at that time,
what did not go well in order to start?’ They use this information to
handle the problem with which they are dealing today. They do not
keep a record of it, but they are certainly going to reach back to their
experience. I think that it differs from hospitals, because you see the
patients for such a short time. (G: I: 1, 2, 3, 4).
Changing the attitude of nurses to a more scientifically based
approach seems to be difficult, as most of them value ‘acting’
above ‘reading and interpreting research’. The lack of time is
one of the major obstacles of a general uptake of EBN. Some
nurses blame their own unwilling attitude in the ongoing
K. Hannes et al.
166 � 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd

debate on the implementation of EBN, where time is often
used as an excuse:
6:35:5: The aspect ‘time’…nurses do have a full programme indeed,
but at the same time we cannot deny that nurses take it for granted: ‘I
am a nurse, so I do not have time’. That it becomes a synonym,
something to hide behind (G: I: 2).
Education. In recent years, there has been a decrease in the
number of registered nurses (RNs) and nursing students. The
acute need for more nurses forced the government into the
decision (1) to stimulate physiotherapists (too many in
Belgium) and health care practitioners from other disciplines
to re-educate themselves to become nurses and (2) to allow
nursing assistants (NAs) to fulfill some nursing tasks in
hospitals and other institutes. The position of NAs has been
legalized. The lack of RNs is considered a facilitating factor
in the development of guidelines in daily care, to be used by
NAs under supervision, especially in geriatric institutions
where NAs seem to be well integrated in daily care. It
contributes to the discussion about which tasks can be taken
on by NAs and which tasks can only be performed by RNs,
because of the specific expertise needed:
11:185:6: I have thrown my weight behind the introduction of
carers (NAs) in an acute setting. We were 100% behind this step.
Nevertheless, we have found that delegating tasks to NAs is a
difficult step. You must go about introducing this system almost in
terms of a directive; in this case you do such-and-such and in that
case you do so-and-so…it is not easy…At that time we used a
formula: ‘If the patient’s skin is touched in any way whatsoever,
this must be discussed. So washing: yes, taking a tablet: no’. (G:
private discussion 1, 2/seeks confirmation with 01 and 6: 7).
There is a difference in knowledge between RNs with a
master’s degree and bedside RNs (bachelor’s degree). Differ-
ences between the groups become most clear in the response
to the introductory question: ‘What is EBN?’ While the
concept is well known to the group of nurses working on an
academic level, RNs in at least one of the five focus groups
have no notion of the concept. Nurses working in an
institutional setting seem to be more aware of the content
than those working independently. Nurses not only address
their own lack of knowledge and skills, but also the limited
capacities of their fellow care providers, supervisors or
teachers:
2:22:4: If I think about college then I think about the level of the
lecturers in the first place. If you have a body of lecturers fewer than
half of whom have a master’s degree. I believe that they cannot pass
EBN on to the students.
Differences between the scientific capabilities of nurses are
the subject of mixed feelings. Some nurses feel there is no
problem having two groups with different skills, while
others doubt there will be any progress in the implemen-
tation of EBN in bedside nursing if the staff performing the
latter is not scientifically trained. Older nurses seem to be
aware of some changes in the curriculum. Expectations
regarding nursing students changed from ‘having gained the
right skills’ under the supervision of experienced colleagues
to ‘having the skills to find out how to handle’ a specific
problem in practice:
10:249:9: Training is now a bit minimalist as regards techniques (G:
I: 3, 4, 6). Consequently, the assumption is probably higher that
students should take a look themselves at ‘How are we going to do
that?’…Perhaps they have indeed learned the way in which they must
find things out, but their baggage is definitely smaller and perhaps the
need to find things out is greater.
Payment. Nurses state that there is no compensation or
support of any kind for their efforts to carry out evidence-
based practice. Another aspect that bothers them is the
incongruity in the payment between doctors and nurses.
Nurses acting under the doctors’ supervision are not allowed
to earn a payment for the clinical act. On the other hand,
doctors performing clinical services that can be provided by
nurses let the patient pay for this consultation, which leads to
financial malpractice that should be avoided in an evidence-
based culture:
10:161:5: If you now just look at injections that people have to have;
some of the doctors pass them on spontaneously and say, that is a
nursing job, but other doctors invite the patient to come to their surgery
every day and actually charge for a consultation. Where are we?
Characteristics of evidence
Several nurses lack the necessary knowledge and skills to
be able to implement EBN in daily practice. They are not
encouraged to gain computer skills, access keys to scientific
information are preserved for supervisors only, quality lit-
erature in Dutch language is scarce, statistical language is
difficult, subscriptions to important journals are often too
expensive and the motivation to read is generally low.
Nurses who do read are discouraged owing to conflicting
opinions or vague answers. They also complain about a
lack of evidence for both their clinical and ethical ques-
tions:
11:188:7: We have quite a few problems with people who are sent to
us with nutritional problems…Then you say, ok, we would like to do
JAN: ORIGINAL RESEARCH Barriers to evidence-based practice
� 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd 167

something. What are the guidelines about doing a gastrostomy? You
find damn all about it in the literature, but pragmatically speaking the
one thing that is clear is ‘We must give preventive antibiotics
prophylactically’. But which antibiotics do they have to take…and
then I have not looked at everything else associated with this topic,
such as ethical issues…Do we have to or continue to treat those with
terminal dementia? To what extent do we have to go along with the
family? It has not yet been discussed. (G: I: 1, 3, 4/dreaming: 3, 4).
Several nurses doubt the objectivity and quality of the
scientific studies produced within their domains of interest.
Commercial firms sponsor many of the studies:
6:25:6: Just take the whole item about the breast-feeding story; in
society, enormous interest groups jump on the bandwagon. I just
want to say that if Nestle did a study you can indeed ask yourself
about the distortion or what those results really mean. You, as an
independent individual and professional, are perhaps more likely to
come to other conclusions.
What also bothers nurses is the impression that existing
evidence seems to give priority to popular medical themes,
mostly related to pharmaceutical products.
The problem tree
In the problem tree presented in Figure 1, relationships
between the barriers mentioned by the study population and
the context in which they are working are explored. The tree
is presented as a web of ideas, in which the codes within each
major theme are linked, grounded in the data. Links that
conflict with findings from previous studies are discussed in
the paragraph below. The tree adds value to the thematic
analysis by revealing relationships that cross the borders of
the major themes and thus presents a more nuanced picture
of the data. This illustrates the complexity of implementing
EBN and creates an opportunity to translate problems into
specific targets on which to focus.
Discussion
Methodological aspects
We decided to complete our focus group-based research
project before searching the literature, so as to be able to look
at the data with an open mind, free from the boundaries of
perspectives from other researchers. Some of our participants
had little or no notion of EBN. This finding is consistent with
previous studies (Sams & Gannon 2000, Micevski et al.
2004, Bahtsevani et al. 2005, Mott et al. 2005). The lack of
awareness of the EBN concept in some focus groups
contributed to the complexity of the moderator’s task.
Valuable time was spent on clarifying basic principles. The
focus group methodology was considered appropriate for
identifying barriers. However, in some groups, the education
level of nurses differed, leading to dominant voices from, for
example, expert nurses or nurses working on an academic
level. We cannot guarantee that all voices were sufficiently
heard.
The 53 nurses who participated formed a small sample of
Flemish (Belgian) nurses. The sample was neither random nor
representative. Instead, we chose to engage nurses working in
different settings, such as hospitals, home care and elder care.
As most settings were represented in only one or two focus
groups, comparisons between nurses working in different
settings is problematic. Future research could focus on an in-
depth study of barriers within each setting.
Finally, we would like to draw attention to some meth-
odological issues that developed on the problem tree. It
differs from the original concept in the logical framework
approach to Project Design. Although the focus group
participants identified all barriers and provided the ingredi-
ents, researchers have developed the final tree. Furthermore,
the tree does not aim to determine cause and effect relation-
ships, as is the case in the logical framework approach.
Instead, it reveals potential relationships that can be tested in
future research projects.
Contributions to EBN
The major findings of our study seem to be consistent with
findings from previous studies. Findings report a lack of time,
a difficult access to resources, a hierarchical structure, a lack
of support from doctors or management, a lack of relevant
studies for nursing, a lack of computer and other skills, little
motivation to carry out evidence-based practice, a reluctance
to change practice, the impact of pharmaceutical companies
on evidence, a culture promoting ‘acting’ instead of ‘research-
ing’ and the experience of patients as an important outcome
measure for evaluating clinical practice. However, Flemish
(Belgian) nurses added some topics that were not fully
addressed in previous research.
Some participants seemed to argue that nurses themselves
have a big responsibility to claim autonomy and authority for
decisions regarding patients. The hierarchical structure of
clinical professions, in which nurses’ position appears to be
close to the bottom, is reflected in differences in status,
power, authority and salary. Elements of ‘power’ also play a
part in Flemish (Belgian) nurses’ relationship with patients.
Nurses in home-based care are especially sensitive to the
K. Hannes et al.
168 � 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd

demands of patients, as they consider themselves to be
‘guests’ in the environment of the patient. The lack of respect
experienced by Flemish (Belgian) nurses from, for example,
allied health care practitioners and the fact that doctors do
not recognize the importance of nursing interventions have
been reported in a previous study (Siebens et al. 2006).
However, 91% of the nurses in Siebens’ study (Belgium)
stated that they were seen as an equal partner across
disciplines. In addition, managers tend to treat nurses simply
as a cost in the process of health care instead of a valuable
partner. Newman et al. (1998) also reported that nurses were
blamed or punished when patients complained, even when
the primary cause of an incident may have been an underlying
organizational procedure.
Evidence-based nursing has the potential to empower
nurses in their decision-making processes (Zeitz & McCutch-
eon 2003). However, the majority of Flemish (Belgian) nurses
do not achieve a sufficient level of mastery in applying EBN.
The peer pressure felt, for example, when searching for
information on the internet during working hours is consis-
tent with McKnight’s (2006) finding that taking time to read
on duty is difficult and, in some cases, felt as ethically wrong.
The lack of time to invest in the evidence-based movement
might be related to a lack of staff. Difficulties in recruiting
and retaining nurses have been mentioned by other authors
(Newman et al. 1998, Tsai 2000, Kirshbaum et al. 2004,
Pravikoff et al. 2005, Milissen et al. 2006). In Flanders
(Belgium), NAs have filled in the gap. Currently, they seem to
be more active in elder care institutions than in hospitals.
RNs in the focus groups still have their doubts about the
quality of the work NAs deliver. However, previous research
found that 43% of Belgian RNs considered the impact of
NAs positive. Only 15% reported a worsening of the quality
of care (Milissen et al. 2006). Some Flemish (Belgian) nurses
fear the whole situation will lead to a ‘two-tier’ education
and practice policy for nurses, a discussion previously
initiated by White and Taylor (2002). At least some of the
nurses in our sample tend to support Castledine’s (1997)
opinion that maybe not all nurses need to become research-
ers, but there is no excuse for them not to develop a research-
minded mentality. Nevertheless, it will be difficult for some
groups of nurses to engage themselves in the evidence-based
movement, especially those working in rural areas with
limited access to medical information and stakeholders, such
as librarians, methodological experts and well-trained expert
nurses.
Conclusion
In this study, we describe the barriers mentioned by Flemish
(Belgian) nurses. To our knowledge, no other study in the
field of nursing has proposed a problem tree, in which
barriers are linked and can easily be located. The tree has the
potential to be transformed into a tree of objectives, which
will be the focus of a subsequent research project. It will
enable us to identify clusters of strategies to tackle the
problems. We feel the tree is of relevance to the international
community of nurses and those who promote EBN. It could
function as a useful tool to orient change management
processes and serve as a model for other researchers who
explore barriers within their own healthcare system. How-
ever, one should bear in mind that the tree is context-specific
for Flanders (Belgium).
Acknowledgements
We wish to acknowledge the time and enthusiasm of the
nurses who took part in the focus groups and Prof. Dr. E.
Vermeire for his advice on the analysis of data.
Author contributions
KH was responsible for the study conception and design and
the drafting of the manuscript. KH, JV and GP performed the
data collection and KH, LD, JG and BA performed the data
What is already known about this topic
• Known external barriers to the use of evidence-based
nursing include a lack of time, resources, evidence,
authority and support.
• Known internal barriers include a lack of motivation
and resistance to change.
What this paper adds
• Nurses acknowledge a lack of responsibility in the
uptake of evidence-based nursing.
• Elements of power are visible in nurses’ relationships
with doctors, managers and patients, the latter being
more outspoken with nurses providing home-based
care who consider themselves ‘guests’ in the patient’s
environment.
• Different education levels might lead to ‘two-tier’
nursing practice.
• Relationships between barriers to evidence-based nur-
sing are presented in a problem tree, which facilitates
the development of clear objectives and targeted
strategies.
JAN: ORIGINAL RESEARCH Barriers to evidence-based practice
� 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd 169

analysis. BA obtained funding and provided administrative
support. JV, JG and BA made critical revisions to the paper.
JG and BA supervised the study.
References
Adams D. (2001) Breaking down the barriers: perceptions of factors
that influence the use of evidence in practice. Journal of Ortho-
paedic Nursing 5, 170–175.
Adamsen L., Larsen K., Bjerregaard L. & Madsen J.K. (2003) Danish
research-active clinical nurses overcome barriers in research util-
ization. Scandinavian Journal of Caring Science 17(1), 57–65.
Andrew N. & Kinn S. (2001) Are nurses receptive to an evidence-
based newsletter? Nursing Times 97(44), 32–33.
Bahtsevani C., Khalaf A. & Willman A. (2005) Evaluating psychi-
atric nurses’ awareness of evidence-based nursing publications.
Worldviews on Evidence-Based Nursing 2(4), 196–206.
Benner P. (1985) Quality of life: a phenomenological perspective on
explanation, prediction and understanding in nursing science.
Advances in Nursing Science 8(1), 1–14.
Bryar R.M., Closs S.J., Baum G., Cooke J., Griffiths J., Hotsick T.,
Kelly S., Knight S., Marshall K. & Thompson D.R. (2003) The
Yorkshire BARRIERS project: diagnostic analysis of barriers to
research utilization. International Journal of Nursing Studies 40,
73–84.
Carrion M., Woods P. & Norman I. (2004) Barriers to research
utilization among forensic mental health nurses. International
Journal of Nursing Studies 41(6), 613–619.
Castledine G. (1997) Barriers to evidence-based nursing care. British
Journal of Nursing 6(18), 1077.
French B. (2005) Contextual factors influencing research use in
nursing. Worldviews on Evidence-Based Nursing 4, 172–183.
Funk S.G., Champagne M.T., Wiese R.A. & Tornquist E.M. (1991a)
Barriers to using research findings in practice: the clinicians’ per-
spective. Applied Nursing Research 4, 90–95.
Funk S.G., Champagne M.T., Wiese R.A. & Tornquist E.M. (1991b)
BARRIERS; the barriers to research utilization scale. Applied
Nursing Research 4, 39–45.
Funk S.G., Champagne M.T., Tornquist E.M. & Wiese R.A. (1995a)
Administrators’ views on barriers to research utilization. Applied
Nursing Research 8, 44–49.
Funk S.G., Tornquist E.M. & Champagne M.T. (1995b) Barriers and
facilitators of research utilization: an integrative review. Nursing
Clinics of North America 30, 395–704.
Kenny D.J. (2005) Nurses’ use of research in practice at three US
Army hospitals. Canadian Journal of Nursing Leadership 18(3),
45–67.
Kirshbaum M., Beaver K. & Luker K.A. (2004) Perspectives of breast
care nurses on research dissemination and utilization. Clinical
Effectiveness in Nursing 8, 47–58.
Leininger M.M. (1985) Ethography and ethnonursing: models and
modes of qualitative data analysis. In Qualitative Research Meth-
ods in Nursing (Leininger M.M., ed.), Grune & Stratton, Orlando,
FL, pp. 33–72.
Mazurek Melnyk B., Fineout Overholt E., Fishbeck Feinstein N.,
Hong L., Small L., Wilcox L. & Kraus R. (2004) Nurses’ perceived
knowledge, beliefs, skills and needs regarding evidence-based
practice: implications for accelerating the paradigm shift. World-
views on Evidence-Based Nursing 3, 185–191.
McCaughan D., Thompson C., Cullum N., Sheldon T.A. &
Thompson D.R. (2002) Acute care nurses’ perceptions of barriers
to using research information in clinical decision-making. Journal
of Advanced Nursing 39(1), 46–60.
McCleary L. (2003) Barriers to paediatric nurses’ research utilization.
Journal of Advanced Nursing 42(4), 364–372.
McKnight M. (2004) Hospital nurses; no time to read on duty.
Journal of Electronic Resources in Medical Libraries 1(3), 13–23.
McKnight M. (2006) The information seeking of on-duty critical care
nurses: evidence from participant observation and in-context inter-
views. Journal of the Medical Library Association 94(2), 145–151.
Micevski V., Sarkissian S., Byrne J. & Smirnis J. (2004) Identification
of barriers and facilitators to utilizing research in nursing practice.
Worldviews on Evidence-Based Nursing 1(4), 229.
Milissen K., Abraham I., Siebens K., Darras E., Dierckx de Casterle
B., representing the BELIMAGE group (2006) Work environment
and workforce problems: a cross-sectional questionnaire survey of
hospital nurses in Belgium. International Journal of Nursing
Studies 43, 745–754.
Mott B., Nolan J., Zarb N., Arnison V., Chan R., Codner T., Casey
T., Jenkins B., Ulrych G., Blackburn C., Glanfield L., Halcomb E.
& Davidson P.M. (2005) Clinical nurses’ knowledge of evidence-
based practice: constructing a framework to evaluate a multifac-
eted intervention for implementing EBP. Contemporary Nurse
19(1–2), 96–104.
Newman M., Papadopoulos I. & Sigsworth J. (1998) Barriers to
evidence-based practice. Intensive & Critical Care Nursing 14(5),
231–238.
Norwegian Agency for Development Cooperation (NORAD) (1996)
The Logical Framework Approach (LFA) A Handbook for
Objective-Oriented Planning. Tempus, Norway.
Olade R.A. (2003) Attitudes and factors affecting research utiliza-
tion. Nursing Forum 38(4), 5–15.
Paramonczic A. (2005) Barriers to implementing research in clinical
practice. Canadian Nurse 101(3), 12–15.
Pravikoff D.S., Tanner A.B. & Pierce S.T. (2005) Readiness of U.S.
nurses for evidence-based practice. The American Journal of
Nursing 105(9), 40–51.
Retsas A. (2000) Barriers to using research evidence in nursing
practice. Journal of Advanced Nursing 31(3), 599–606.
Ring N., Malcolm C., Coull A., Murphy T. & Watterson A. (2005)
Nursing best practice statements: an exploration of their imple-
mentation in clinical practice. Journal of Clinical Nursing 14,
1048–1058.
Rycroft-Malone J., Harvey G., Seers K., Kitson A., Mccormack B. &
Titchen A. (2004) An exploration of the factors that influence the
implementation of evidence into practice. Journal of Clinical
Nursing 13, 913–924.
Sams L. & Gannon M.E. (2000) Evidence-based practice and
clinical work assessment. Seminars in Perioperative Nursing 9(3),
125–132.
Siebens K., Dierckx de Casterle B., Abraham I., Dierckx K., Braes T.,
Darras E., Dubois Y., Milisen K., representing the BELIMAGE
group (2006) The professional self-image of nurses in Belgian
hospitals: a cross-sectional questionnaire survey. International
Journal of Nursing Studies 43, 71–82.
K. Hannes et al.
170 � 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd

Sitzia J. (2001) Barriers to research utilization: the clinical setting and
nurses themselves. European Journal Oncology Nursing 5(3), 154–
164.
Sommer S.K.(2003) An Investigation of the Barriers and Facilitators
of Research Utilization among a Sample of Registered Nurses. PhD
thesis, Loyola University of Chicago, Chicago, IL, pp. 136.
Strauss A. & Corbin J. (1997) Grounded Theory in Practice. Sage
Publications, California.
Thompson C. (2003) Clinical experience as evidence in evidence-
based practice. Journal of Advanced Nursing 43(3), 230–237.
Tsai S.L. (2000) Nurses’ participation and utilization of research in
the Republic of China. International Journal of Nursing Studies 37,
435–444.
Walsh M. (1997) Barriers to research utilization and evi-
dence based practice in A&E nursing. Emergency Nurse 5(2),
24–27.
White R. & Taylor S. (2002) Nursing practice should be informed by
the best available evidence, but should all first level nurses be
competent at research appraisal and utilization? Nurse Education
Today 22, 220–224.
Zeitz K. & McCutcheon H. (2003) Evidence-based practice: to be or
not to be, this is the question! International Journal of Nursing
Practice 9, 272–279.
JAN: ORIGINAL RESEARCH Barriers to evidence-based practice
� 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd 171