assessment of the skeletal status by mr relaxometry techniques of the lumbar spine: comparison with...
TRANSCRIPT

European Journal of Radiology 50 (2004) 245–256
Assessment of the skeletal status by MR relaxometry techniquesof the lumbar spine: comparison with dual X-ray absorptiometry
Thomas G. Marisa,∗, John Damilakisa, Liana Sideria, Michael Deimlingb,Georgios Papadokostakisc, Olympia Papakonstantinoud, Nikos Gourtsoyiannisd
a Departement of Medical Physics, Faculty of Medicine, University Hospital of Heraklion, P.O. Box 1352, 71110 Stavrakia, Heraklion, Crete, Greeceb MR Research and Development, MREA, Siemens, Erlangen, Germany
c Department of Orthopedics, Faculty of Medicine, University of Crete, Crete, Greeced Department of Radiology, Faculty of Medicine, University of Crete, Crete, Greece
Received 11 January 2004; received in revised form 13 January 2004; accepted 16 January 2004
Abstract
Purpose: To measure lumbar spineT2*, T2, T2′ andT1 MR relaxometry parameters and compare them with lumbar spine bone mineraldensity (BMD) in a group of postmenopausal women.Materials and methods: Lumbar spineT2*, T2,T2′ andT1 MR relaxometry parametersand BMD values were assessed in 101 postmenopausal women (mean age: 61.8±7.1 (1 S.D.) years); of them 63 referred to as control subjects(group A, BMD T-scores≥ −2.5 S.D.) and 38 as osteoporotic (group B, BMD T-scores< −2.5 S.D.). All magnetic resonance imaging(MRI) examinations were performed on an 1.5 T imaging system using: (a) a 2D single slice multi echo (32 echoes) gradient echo (MEGRE)sequence (TR/TE1/TE32/FA: 160/2.7/74.93 ms/25◦) for theT2* measurement, (b) a respiratory gated 2D single slice Multi Echo (16 echoes)Spin Echo (MESE) sequence (TR/TE1/TE16/FA: 2000–2500/22.5/360 ms/90◦) for the T2 measurement and (c) a 2D single slice multi TI(18 repeats) turbo Fast Low Angle Shot (turbo FLASH) sequence (TR/TE/TI1/TI16/FA: 11/4.2/10/5000 ms/10◦) for theT1 measurement.T2′
was calculated from its definition equation: (1/T2′ = 1/T2* − 1/T2). Lumbar spine BMD was assessed using DXA.Results: All measuredparameters showed statistically significant differences between groups A and B (fromP < 0.05 to<0.001). All parameters showed significantassociations with subject’s age ranging fromr = 0.245 (P < 0.05) for theT2 up tor = 0.377 (P < 0.001) for theT2*. All parameters showedsignificant associations with subject’s BMD measurements ranging fromr = −0.184 (P < 0.05) for theR1 = (1/T1) up tor = −0.345(P < 0.0005) for theT2. Conclusion: Among the MR relaxometry parameters studied,T2* andT2 showed better discrimination of patientswith osteoporosis from control subjects.© 2004 Elsevier Ireland Ltd. All rights reserved.
Keywords: Magnetic resonance imaging; MR relaxometry; Dual energy X-ray absorptiometry; Osteoporosis
1. Introduction
Clinical and experimental research studies performed overthe last decade have shown that magnetic resonance imag-ing (MRI) has the potential to be a useful method for thestudy of trabecular bone. Two approaches have been devel-oped. The first is referred to direct 2D or 3D imaging ofthe trabecular bone network utilizing high resolution MRI[1–4]. With this technique MR images with in plane spatialresolution as high as 80�m can be used to study the trabec-ular bone architecture directly[5,6]. The second approach
∗ Corresponding author. Tel.:+30-2810-392797;fax: +30-2810-542095.
E-mail address: [email protected] (T.G. Maris).
is referred to indirect MR imaging of the trabecular boneutilizing the physical MR signal related relaxometric param-eters [T2*, R2* = (T2*)−1, T2, R2 = (T2)−1, T2′ and R2′= (T2′)−1] to study the density and quality of the trabecularbone network (MR relaxometry)[7–13]. Direct high reso-lution MRI requires advanced MRI systems equipped withsophisticated hardware and software and is time consumingwhereas MR relaxometry methods can be performed utiliz-ing standard imaging techniques on conventional MR sys-tems and lesser time expenditures.
The general concept of the MR relaxometry strategy ad-dressed for the study of trabecular bone is the differences inmagnetic susceptibilities between the inter-surfaces of tra-becular structures and bone marrow material[14,15]. Whena quantitative estimation of theT2* of the bone marrow is
0720-048X/$ – see front matter © 2004 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.ejrad.2004.01.021

246 T.G. Maris et al. / European Journal of Radiology 50 (2004) 245–256
desirable, the susceptibility differences at the interface be-tween trabecular bone and bone marrow result in additionalspatial inhomogeneities of the static magnetic field. In thisway the reversible bone marrow transverse relaxation timeT2′ and eventuallyT2* are both affected: (T2*)−1 = (T2)−1
+ (T2′)−1. Static field inhomogeneities imposed by the pres-ence of trabecular bone result in additional dephasing ofT2′,which finally leads to a decrease in the bone marrowT2*values[15]. The change (decrease or increase) in bone mar-row T2* and its decay scheme provides information whichis indirectly related to the density and the structure of thesurrounding trabecular network[15]. In early reports, dif-ferent techniques were used to assessT2* [7,14–16]all ofthem based on multi echo GRadient Echo (GRE) sequences.Quite recently new MRI sequences (GES-FIDE techniques)[17] were designed and used for direct assessment of theT2′and theT2 parameter of trabecular bone in vitro and in vivo[9,17]. Trabecular bone quality is also evaluated with theuse of multiple spin echo (MSE) techniques at the presenceof correlation gradients[18].
In vivo correlations ofT2′andT2* (or the correspondingR2′ andR2*) and BMD as measured by dual energy X-rayabsorptiometry (DXA) methods were observed in differentappendicular skeletal sites namely: the calcaneus[13,19],the distal radius[16] and the femoral neck[8,13]. There islimited literature referred to in vivo comparative studies ofDXA and MR relaxometry for the lumbar spine[7,13]. Inall skeletal sites a positive association of eitherT2* or T2′and BMD values was observed.
The objectives of the current study were to (a) introducea new methodology for the quantitative assessment of lum-bar spineT2* which is partly based on the application of anew MRI sequence (MEGRE) and on theT2* signal decayweighted regression analysis procedures, (b) apply a con-ventional MESE and a conventional turboFLASH MRI se-quences for the calculation ofT2 andT1 of the lumbar spine,respectively and (c) perform a preliminary study to com-pare lumbar spine MR relaxometric parameters with lumbarspine BMD measurements.
2. Materials and methods
2.1. Study subject group
One hundred one (n = 101) postmenopausal women,aged 43–77 [61.8 ± 7.1 (1 S.D.)] years were included inthe present open perspective study during a 2-year-period.All women had no history of bone disease, low energy frac-tures, and trauma or bone malignancies. They were also notsubjected to any medical treatment with drugs that might in-fluence their bone metabolism. Data were collected on thebasis of a routine medical interview. For each subject, height(H), weight (W) and body mass index (BMI) (BMI= W/H2)were obtained. Informed consent was obtained from all sub-jects prior to DXA and MRI examinations.
The whole study population was divided into two groupsaccording to their DXA lumbar spine average BMD (L1-L4)and their T-scores following WHO recommendations[20].These were: (Group A): non-osteoporotic (either normal orosteopenic) postmenopausal women (n = 63), aged 43–77[60.4 ± 7.1 (1 S.D.)] years with T-scores≥ −2.5 S.D. ascompared to the young adult normal mean. (Group B): os-teoporotic postmenopausal women (n = 38), aged 51–76[61.2 ± 6.2 (1 S.D.)] years with T-scores<−2.5 S.D. ascompared to the young adult normal mean.
2.2. DXA measurements
DXA measurements for the estimation of the average lum-bar spine areal BMD were performed using a DXA appara-tus (QDR 1000 plus, Hologic, Watham, MA). BMD of thelumbar spine was measured from anteroposterior projectionsfor all women and was expressed as an average from theBMD of the four first lumbar vertebrae (L1 to L4). The aver-age T-score obtained from the first four vertebrae (L1 to L4)was used as the index for the subject group classification.
2.3. MR imaging technique
MR imaging for all subjects and phantoms was performedusing a standard clinical 1.5 T whole-body supercon-ducting imaging system (Vision Plus, Siemens/Erlangen),equipped with high performance 25 mT/m gradients. Stan-dard quadrature RF body coil (64 cm diameter) was usedin all measurements for both excitation and signal detec-tion. All participants were placed in supine position on thesystem’s scanning bed. A respiratory belt wrapped aroundthe subject’s body was used for the respiratory triggeringMR imaging technique.
2.3.1. MR phantom studiesA 10 mM gadolinium diethylenetriamine pentaacetic
acid (Gd-DTPA, MagnevistTM, Shering, Germany), para-magnetic solution was prepared in deionized water. ThisGd-DTPA solution, which was used as a calibration phantommaterial, is expected to giveT1 andT2 relaxivities (RV1 andRV2) at 1.5 T field strength calculated by the coefficients:RV1 = 4.59 ± 0.03 (mM s)−1 and RV2 = 5.15 ± 0.03(mM s)−1 [21]. A T1 value of 22 ms and aT2 value of19 ms are expected from a 10 mM Gd-DTPA solution whenmeasured at room temperature conditions (23◦C) [21].
Gd-DTPA solution was positioned in a 35-ml plastic cylin-drical vial (calibration vial: diameter: 1.5 cm, length: 6 cm)and stored in the magnet room for 24 h prior to measure-ments for temperature stabilization. Calibration vial wasplaced in a thermally isolated coat and positioned behindthe subject’s back at the level of the first lumbar spine verte-brae (L1) prior to examination (Fig. 1). There was no impactof the calibration vial and the subject’s body. The vial wasincluded in all measurements, and was used to evaluate ac-tual image background and structural noise figures (Fig. 2)

T.G. Maris et al. / European Journal of Radiology 50 (2004) 245–256 247
Fig. 1. The three first echo images from the 32 echo MEGRE sequence obtained from an osteoporotic subject (53 years BMDT = −3.5). Images (a), (b)and (c) are obtained at TEs: 2.70, 5.03 and 7.36 ms, respectively. Images (a) and (c) are referred to as fat-water out of phase images, whereas image (b) isa fat-water in phase image of the lumbar spine. ROI-1 to ROI-4 are positioned on the L1 to L4 vertebrae, respectively, and are used for theT2* calculation.ROI-5 is positioned on the calibration vial phantom and is used for the calculation of the 32 image stack background and structured noise figures.
as well as short and long term precision of the MR system.Calibration vial measurement temperature was (23± 1)◦Cthroughout the whole examination.
Short and long term in vitro precision for theT2*, T2, T2′and theT1 values of the calibration vial were assessed us-ing the data obtained for approximately 2-year-period. Shortterm in vitro precision refers to the measurements of thevial parameters (T2*, T2, T2′ andT1) averaged over 1 day(five different successive subjects). Long term in vitro pre-cision refers to the measurements of vial parameters (T2*,T2, T2′ andT1) averaged over the maximum possible time(2 years). Both precision figures are expressed as coefficientof variation (CV%) for each sample.
0 20 40 60 800
50
100
150
200
250
Sign
al
e28 e32
65.61 74.93TE (ms)
Fig. 2. Estimation of image stack background (Bg) and structured noise figures (σS) for T2* measurements from the calibration vialT2* decay data[ Bg(T2*) and σS(T2*) ]. Signal Intensities and their standard deviations (error bars) are averaged from the 28th to the 32th echo. (Bg(T2*) = 15.4,�S(T2*) = 7.2). TheT2* of the calibration vial using the same decay scheme is 10.2 ± 0.8 ms.
2.3.2. MR subject studiesA series of conventional GRadient Echo (GRE)T1
weighted imaging sequences were applied in axial, sagittaland coronal planes and used to locate the lumbar regionof the spine. Once localized, a set of sagittal images wasobtained with the use of a 2D GRET1 weighted multi-slicefast low angle shot (FLASH) sequence[22] (TR/TE/Flipangle(FA): 120 ms/4 ms/70◦) for 13 contiguous spacefilling sagittal slices with 5 mm slice thickness. Spatialpre-saturation slabs were utilized in oblique coronal planesfor motion related artifacts suppression. These images werereviewed by an on site skeletal radiologist (O.P.) in order toassess any vertebral deformities. Consequently, the sixth of

248 T.G. Maris et al. / European Journal of Radiology 50 (2004) 245–256
the thirteen sagittal slices (reference middle sagittal slice)was selected and three sets of quantitative MRI sequenceprotocols were applied in reference to that slice.
For the quantitative estimation of the lumbar bone mar-row T2* a 2D single-slice multi echo GRadient Echo(MEGRE) pulse train sequence was applied for the refer-ence middle sagittal slice in 32 symmetrically repeatablegradient echoes. The first TE was 2.7 ms (out of phasecondition) and 31 gradient echoes were sampled there-after every 2.33 ms. TEs: (2.70, 5.03, 7.36, 9.69, 12.02,14.35, 16.68, 19.01, 21.34, 23.67, 26, 28.33, 30.66, 32.99,35.32, 37.65, 39.98, 42.31, 44.64, 46.97, 49.30, 51.63,53.96, 56.29, 58.62, 60.95, 63.28, 65.61, 67.94, 70.27,72.60 and 74.93) ms. With the above chosen parameters anin-phase out-of phase half modulation period of 2.33 msand a full modulation period (distance between two sub-sequent in phase maxima) of 4.66 ms were obtained. Thiscorresponds to the expected chemical shift separation of215 Hz for fat and water protons at 1.5 T field strength.MEGRE sequence contrast related initial parameterswere: (TR/TE1/TE32/FA: 160 ms/2.7 ms/74.93 ms/25◦).Three signal averages were used and the total examina-tion time for the MEGRE sequence was approximately1 min.
Consequently, for the quantitative estimation of the lum-bar bone marrowT2 a respiratory-gated 2D single-slicemulti echo spin echo (MESE) pulse train sequence (PHAPStechnique)[23] was applied for the same middle sagittalslice in 16 symmetrically repeatable radiofrequency (RF)spin echoes. The first TE was 22.5 ms and 15 RF spinechoes echoes were sampled thereafter every 22.5 ms. TE’s:(22.5, 45, 67.5, 90, 112.5, 135, 157.5, 180, 202.5, 225,247.5, 270, 292.5, 315, 337.5 and 360) ms. MESE sequencecontrast related initial parameters were: (TR/TE1/TE16/FA:2000–2500 ms/22.5 ms/360 ms/90◦). One signal average wasused and the total examination time for the MESE sequencewas approximately 7 min.
Finally, for the quantitative estimation of the lumbar bonemarrowT1, a 2D single-slice multi TI turbo-FLASH pulsesequence (Snapshot-FLASH technique)[24] using centricphase encoding order was applied for the reference middlesagittal slice in 18 distinct TI intervals. TI: (10, 20, 50, 100,200, 300, 400, 500, 600, 700, 800, 900, 1000, 1500, 2000,3000, 4000, and 5000) ms. Turbo-FLASH sequence con-trast related initial parameters were: (TR/TE/TI1/TI16/FA:11 ms/4.2 ms/10 ms/5000 ms/10◦). One signal average wasused and the total examination time for the turbo-FLASHsequence (all TIs) was approximately 6 min.
For all quantitative sequences a 10 mm slice thickness anda rectangular field of view covering an area of 200 mm×320mm was used. The image reconstruction matrix was160×256 pixels, respectively, to the FOV dimensions, corre-sponding to a pixel matrix with pixel dimensions 1.25 mm×1.25 mm. The longer anatomical axis (Head to Feet direc-tion) was chosen as the frequency encoding axis and theshorter (anterior to posterior direction) as the phase encod-
ing axis. A small receiver bandwidth (< 150 Hz/pixel) wasused in all sequences in order to improve signal to noise ratio(SNR). Spatial pre-saturation slabs were utilized in obliquecoronal planes in all three quantitative MR sequences foradjacent to spine tissue suppression and blood flow artifactssuppression. The total examination time was 35 min.
2.3.3. MR data handling and quantitative image analysisAll quantitative MR image data were transferred to
a PC Workstation for further analysis. Standard imagepost-processing routines (image cropping, image segmenta-tion, image archiving) were performed utilizing the imageanalysis software ImageJ (http://www.rsb.info.nih.gov/ij/).A numerical fitting and MR image analysis software con-structed by one of the authors (T.G.M) was used for thecalculation ofT2*, T2 andT1 values. Five regions of inter-est (ROI) corresponding to the first four lumbar vertebrae(L1 to L4) (ROI-1 to ROI-4) and the calibration vial sample(ROI-5) were outlined for all quantitative measurements(T2*, T2 andT1) (Fig. 1).
For the T2* and theT2 evaluations data analysis wasperformed on the five ROI meanT2* and meanT2 de-cay data curves, respectively. In eitherT2* or T2 measure-ments relaxation decay curves were analyzed assuming amono-exponential decay behavior with the presence of sig-nal offset (actual image background).T2* andT2 signal de-cay data were fitted to the equations (Eq. (1)) and (Eq. (2)),respectively
S(TE) = Bg + M0(T1, ρ) e−TE/T2∗ ⇔ ln[S(TE) − Bg]
= ln M0(T1, ρ) −(
1
T2∗)
TE (1)
S(TE) = Bg + M0(T1, ρ) e−TE/T2 ⇔ ln[S(TE) − Bg]
= ln M0(T1, ρ) −(
1
T2
)TE (2)
Numerical fits were performed using a simple weighted lin-ear regression analysis-fitting algorithm. The termM0(T1,ρ)is a signal saturation factor (pseudodensity) and term Bgstands for the actual image background offset. For all fitsr2
was >0.8.The term Bg inEqs. (1) and (2)was calculated from
the calibration vial signal decay data curves obtained fromROI-5 as an average of the five latest echo ROI’s [Echoes:(28–32) forT2* and echoes: (12–16) forT2 measurements].The same five latest echo ROIs were used for the estimationof the average image noise figureσS (averaged standard de-viation of the five latest echo ROIs) which can be assumedas the noise figure of whole base image stack data for ei-ther T2*: [σS(T2*)] or T2: [σS(T2)] (Fig. 2). This can bemathematically expressed using the equations:
σS(T2∗) = [< (Rf σSe) >]e=32e=28,
σS(T2) = [< (Rf σSe) >]e=16e=12 (3)
T.G. Maris et al. / European Journal of Radiology 50 (2004) 245–256 249
whereσSe is the standard deviation (structured noise) ob-tained from ROI-5 on the echo (e) of the base image stack.The Rf factor (Rf = 1.53) is known as the Rayleigh factorand arises when any gaussian noise (random noise) presenton the raw data is centered about zero. The raw data areFourier transformed in order to create a magnitude imagewith all positive values; therefore the noise distribution isskewed at the vicinity of zero.Rf factor accounts for thiseffect [25].
Each signal dataSi from the ROIs decay curves(ROI-1-ROI-5) were weightedSi (w) prior to the linear fitfor T2* (Eq. (4)) andT2 (Eq. (5)) calculation, respectively.The relevant weighting factorsw(T2*) and w(T2) can beexpressed as follows[26]:
Si(w) = w(T2∗)Siw(T2∗) =[
1
[< (Rf σSe) >]e=32e=28
]2
(4)
Si(w) = w(T2)Siw(T2) =[
1
[< (Rf σSe) >]e=16e=12
]2
(5)
where Rf is the Rayleigh correction factor as mentionedpreviously.
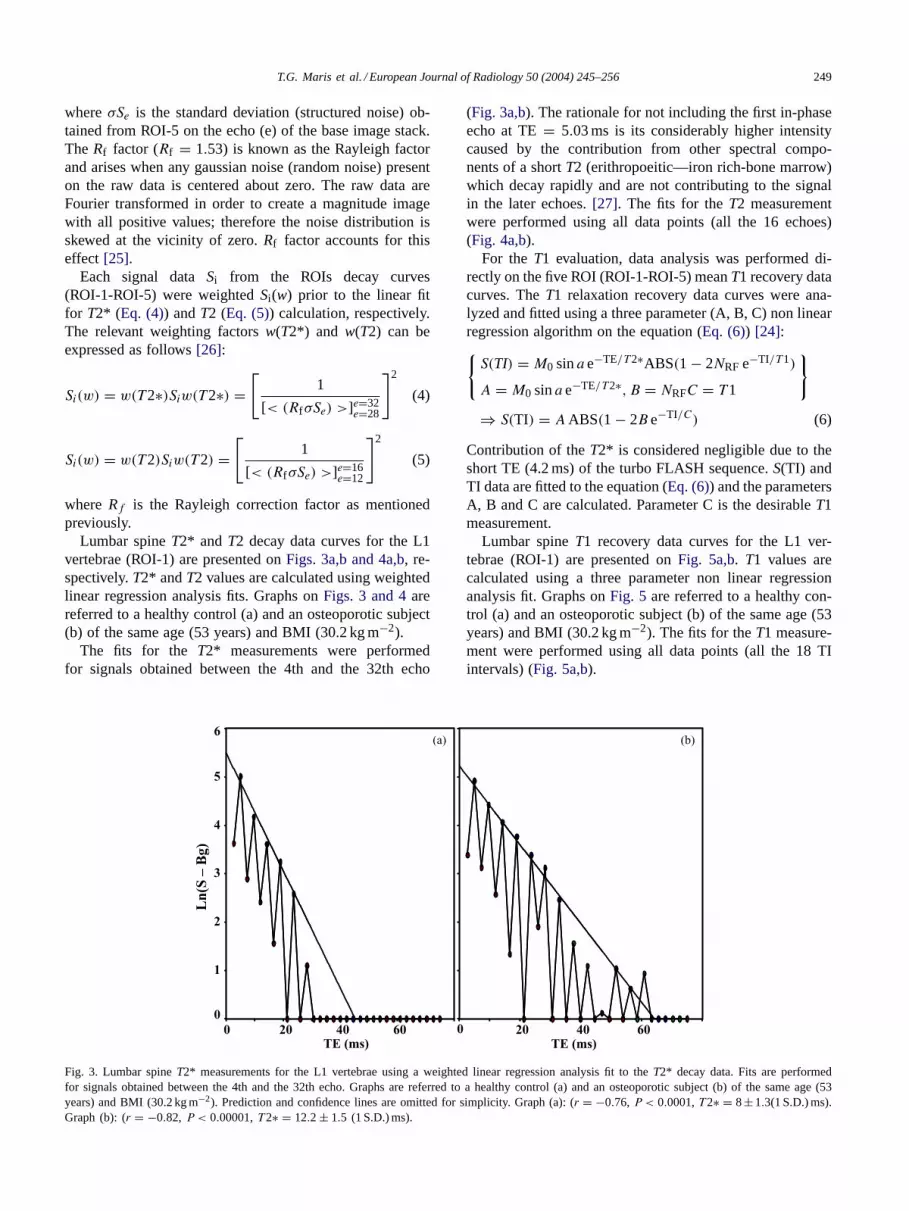
Lumbar spineT2* and T2 decay data curves for the L1vertebrae (ROI-1) are presented onFigs. 3a,b and 4a,b, re-spectively.T2* andT2 values are calculated using weightedlinear regression analysis fits. Graphs onFigs. 3 and 4arereferred to a healthy control (a) and an osteoporotic subject(b) of the same age (53 years) and BMI (30.2 kg m−2).
The fits for the T2* measurements were performedfor signals obtained between the 4th and the 32th echo
2
3
4
5
6
0 20 40 60TE (ms)
0
1
20 40 60
Ln(
S –
Bg)
0TE (ms)
(a) (b)
Fig. 3. Lumbar spineT2* measurements for the L1 vertebrae using a weighted linear regression analysis fit to theT2* decay data. Fits are performedfor signals obtained between the 4th and the 32th echo. Graphs are referred to a healthy control (a) and an osteoporotic subject (b) of the same age (53years) and BMI (30.2 kg m−2). Prediction and confidence lines are omitted for simplicity. Graph (a): (r = −0.76, P < 0.0001,T2∗ = 8± 1.3(1 S.D.) ms).Graph (b): (r = −0.82, P < 0.00001,T2∗ = 12.2 ± 1.5 (1 S.D.) ms).
(Fig. 3a,b). The rationale for not including the first in-phaseecho at TE= 5.03 ms is its considerably higher intensitycaused by the contribution from other spectral compo-nents of a shortT2 (erithropoeitic—iron rich-bone marrow)which decay rapidly and are not contributing to the signalin the later echoes.[27]. The fits for theT2 measurementwere performed using all data points (all the 16 echoes)(Fig. 4a,b).
For theT1 evaluation, data analysis was performed di-rectly on the five ROI (ROI-1-ROI-5) meanT1 recovery datacurves. TheT1 relaxation recovery data curves were ana-lyzed and fitted using a three parameter (A, B, C) non linearregression algorithm on the equation (Eq. (6)) [24]:{
S(TI) = M0 sina e−TE/T2∗ABS(1 − 2NRF e−TI/T1)
A = M0 sina e−TE/T2∗, B = NRFC = T1
}
⇒ S(TI) = A ABS(1 − 2B e−TI/C) (6)
Contribution of theT2* is considered negligible due to theshort TE (4.2 ms) of the turbo FLASH sequence.S(TI) andTI data are fitted to the equation (Eq. (6)) and the parametersA, B and C are calculated. Parameter C is the desirableT1measurement.
Lumbar spineT1 recovery data curves for the L1 ver-tebrae (ROI-1) are presented onFig. 5a,b. T1 values arecalculated using a three parameter non linear regressionanalysis fit. Graphs onFig. 5 are referred to a healthy con-trol (a) and an osteoporotic subject (b) of the same age (53years) and BMI (30.2 kg m−2). The fits for theT1 measure-ment were performed using all data points (all the 18 TIintervals) (Fig. 5a,b).

250 T.G. Maris et al. / European Journal of Radiology 50 (2004) 245–256
0 100 200 3000 100 200 3001
1.5
2
2.5
3
3.5
4
4.5
5
5.5
Ln(
S –
Bg)
TE (ms) TE (ms)
(a) (b)
Fig. 4. Lumbar spineT2 measurements for the L1 vertebrae using a weighted linear regression analysis fit to theT2 decay data. Fits are performed forsignals obtained between the 1st and the 16th echo. Graphs are referred to a healthy control (a) and an osteoporotic subject (b) of the same age (53 years)and BMI (30.2 kg m−2). Graph (a): (r = −0.99, P < 0.00001,T2 = 73.6 ± 1.7 (1 S.D.) ms). Graph (b): (r = −0.99, P < 0.00001,T2 = 79.4 ± 3.6(1 S.D.) ms).
Calculations of the reversible transverse relaxation timeT2′ and the reversible transverse relaxation rateR2′ wereperformed using the formulas (Eq. (7)):
1
T2∗ = 1
T2+ 1
T2′ , R2∗ = R2 + R2′ (7)
T2′ andR2′ were calculated for all ROIs (ROI-1− ROI-5)in each subject (Fig. 1).
(a) (b)
0 1000 2000 3000 4000TI (ms)
0 1000 2000 3000 40000
50
100
150
200
250
300
350
Sign
al
TI (ms)
Fig. 5. Lumbar spineT1 measurements for the L1 vertebrae using a non linear regression analysis fit to theT1 recovery data. Fits are performed forsignals obtained between the 1st and the 18th TI interval. Graphs are referred to a control subject (a) and an osteoporotic subject (b) of the same age (53years) and BMI (30.2 kg m−2). Graph (a): (r = 0.89, P < 0.00001,T1 = 685.7±47.4 (1 S.D.) ms). Graph (b): (r = 0.96, P < 0.00001,T1 = 659.5±53.6(1 S.D.) ms).
2.4. Subject data handling and analysis
Subject and MR parameter measurement data were han-dled and analyzed using MedCalc (MedCalc Software, 9030Mariakerke, Belgium) and TableCurve 2D (Systat, SoftwareInc., Chicago, IL, USA) software. All anthropometric dataare expressed as mean± standard deviation (S.D.). AllMR measurement parameter data are expressed as mean±standard error (S.E.). The normality of the data samples

T.G. Maris et al. / European Journal of Radiology 50 (2004) 245–256 251
Table 1Comparison of anthropometric variables between groups A and B
Parameter Group A (n = 63) Group B (n = 38)
Age (years) 60.4± 7.1 64.6± 6.2Weight (kg) 74.3± 11.1 66.9± 11.7Height (cm) 156.1± 6.3 153± 5.1BMI (kg m−2) 30.4 ± 4.3 28.5± 4.6YPM (years) 15.2± 5.4 17.1± 8.1
Note: mean± standard deviation. YPM: years post-menopause.
was tested using the Kolmogorov–Smirnov test. UnpairedStudent’st-test was used to assess the statistical signifi-cance between data means of the MR measured parametersamongst the study groups. Correlations amongst measurableparameters were estimated by means of normal linear regres-sion analysis. Estimations of sensitivity and specificity fig-ures for all measurable parameters in terms of differentiatingpostmenopausal osteoporotic women from postmenopausalcontrol subjects were performed by means of ROC analysiscurves.
3. Results
The short term (ST) and long term (LT) in vitro precisionfigures for the calibration vial were: (T2*: ST = 1.1% andLT = 3.9%), (T2: ST= 2.3% andLT = 5.5%), (T2′: ST =1.8% andLT = 4.5%), (T1: ST= 3.1% andLT = 7.4%).
All but two subjects underwent both examinations (DXAand MRI) and provided acceptable image quality for quan-titative analysis.Table 1lists the anthropometric variables[age, weight, height BMI and years post-menopause (YPM)]obtained from the two study groups (Group A) and (GroupB) in this study.
All calculated MR relaxometry parameters showed statis-tically significant differences between group A and group B(Table 2). Differences in BMD values between the two studygroups are also presented for comparisons. Differences inlumbar spineT2 andR2 values between the two groups (Aand B) were considered significant at a level: (P < 0.001).Lumbar spineT2*, R2*, T2′, R2′, T1 andR1 values showed
Table 2Unpairedt-tests for the means of BMD,T2*, R2*, T2, R2, T2′, R2′, T1and R1 parameters between the groups A and B
Parameter Group A(n = 63)
Group B(n = 38)
t P
BMD (g cm−2) 0.885± 0.01 0.692± 0.009 11.14 <0.0001T2* (ms) 12.6± 0.9 14.3± 0.4 −2.19 <0.05R2* (s−1) 85.7 ± 6.3 72.2± 2.2 2.54 <0.05T2 (ms) 82.5± 2 90.6± 1.2 −3.61 <0.001R2 (s−1) 12.2 ± 0.3 11.1± 0.1 3.65 <0.001T2′ (ms) 15.2± 0.8 17.1± 0.6 −2.09 <0.05R2′ (s−1) 73.5 ± 6.2 61.1± 7.2 2.36 <0.05T1 (ms) 612.3± 42.9 544.2± 20.5 1.61 <0.05R1 (s−1) 1.75 ± 0.13 1.93± 0.07 −1.33 <0.05
Note: mean± standard error.
Table 3Correlations of BMD,T2*, R2*, T2, R2, T2′, R2′, T1 andR1 parameterswith age for all subjects
Parameter All subjects (n = 101)
Slope r P
BMD(g cm−2)
−0.008± 0.001(g cm−2 per year) −0.452 <0.00001
T2* (ms) 0.153± 0.04 (ms per year) 0.377 <0.001R2* (s−1) −0.993± 0.25(s−1 per year) −0.283 <0.001T2 (ms) 0.308± 0.12 (ms per year) 0.245 <0.05R2 (s−1) −0.05 ± 0.02 (s−1 per year) −0.264 <0.01T2′ (ms) 0.203± 0.05 (ms per year) 0.351 <0.001R2′ (s−1) −0.943± 0.249 (s−1 per year) −0.355 <0.001T1 (ms) −6.5 ± 1.87 (ms per year) −0.329 <0.001R1 (s−1) 0.02 ± 0.006 (s−1 per year) 0.335 <0.001
Note: mean± standard error.
statistically significant differences at a level: (P < 0.05) be-tween the two study groups.
The correlations of all MR relaxometry measured param-eters with subject’s age for both study groups (all subjects)are presented onTable 3. The same correlations concern-ing group A and group B independently are presented onTable 4. Correlations of lumbar spine BMD values withsubject’s age are also presented for comparisons onTables 3and 4. All parameters showed significant associations withsubject’s age ranging from (r = 0.245, P < 0.05) for theT2 up to (r = 0.377, P < 0.001) for theT2* when bothstudy groups are studied as one sample (all subjects,n =101). Results for theT2*, T2 and theT1 parameter werepresented graphically onFigs. 6a, 7a and 8a, respectively.Only T2* and R2* parameters showed significant correla-tions with subject’s age when group A (n = 63) and groupB (n = 38) are studied independently. Their correlations arecomparable with those obtained from the reference BMDmeasurements in both study groups (Table 4).
The correlations of all MR relaxometry measured param-eters with subject’s lumbar spine BMD measurements forboth study groups (all subjects) are presented onTable 5.All parameters showed significant associations with subjectsBMD measurements ranging from (r = −0.184,P < 0.05)for theR1 up to (r = −0.345,P < 0.0005) for theT2 whenboth study groups are studied as one sample (all subjects,n = 101). Results for theT2*, T2 and theT1 parameter werepresented graphically onFigs. 6b, 7b and 8b, respectively.
ROC analysis results for theT2*, R2*, T2, R2, T2′, R2′,T1 and R1 parameters for assessing their discriminationability between postmenopausal osteoporosis (group B) andpostmenopausal control (group A) subject groups are pre-sented onTable 6. Maximum accuracy criteria, sensitivityand specificity figures as well as area under curve (AUC) es-timations are summarized onTable 6. All parameters showedAUC values ranging from 0.611 (95% CI: 0.509–0.707)for T2′ up to 0.744 (95% CI: 0.647–0.825) and were ableto discriminate the postmenopausal osteoporotic from thepostmenopausal control group. Amongst all parametersT2*

252 T.G. Maris et al. / European Journal of Radiology 50 (2004) 245–256
Table 4Correlations of BMD,T2*, R2*, T2, R2, T2′, R2′, T1 andR1 parameters with subject’s age for the groups A and B
Parameter Group A (n = 63) Group B (n = 38)
r slope P r slope P
BMD (g cm−2) −0.365 <0.005 −0.308 <0.05−0.0050 (g cm−2 per year) −0.0027 (g cm−2 per year)
T2* (ms) 0.362 <0.005 0.293 <0.050.154 (ms per year) 0.119 (ms per year)
R2* (s−1) −0.348 <0.005 −0.285 <0.05−1.045 (s−1 per year) −0.623 (s−1 per year)
T2 (ms) 0.173 NS 0.06 NSR2 (s−1) −0.202 NS −0.07 NST2’ (ms) 0.338 NS 0.293 NSR2’(s−1) −0.338 NS −0.281 NST1 (ms) 0.290 NS 0.237 NSR1 (s−1) 0.285 NS 0.279 NS
Note: mean± standard error. NS: not significant.
andT2′ presented the maximum measured sensitivities (84.2and 86.8, respectively), whereasT2 presented the maximummeasured specificity (85.7) in discriminating the two groups.Sensitivity and specificity figures for theT1 parameter weremoderate (63.2 and 68.3, respectively). ROC analysis curvesfor theT2*, T2, T2′ and theT1 parameters are presented onFig. 9.
4. Discussion
In most in vivo MR relaxometry studies of the spine andbone marrow the phased array coil was used routinely[7,13].The rationale for this choice is the increased SNR at thevicinity of the coil and locally at the position of the spine.In this study and for all MR relaxometry techniques thestandard quadrature RF body coil was used for both exci-
20
22
24
T2*
(m
s)
Age (yrs)0,5 0,6 0,7 0,8 0,9 1,0 1,1 1,2
4
6
8
10
12
14
16
18
40 45 50 55 60 65 70 75
BMD (g/cm2)
(a) (b)
Fig. 6. Linear regression ofT2* vs. age (a) and BMD (b) for all subjects (n = 101). A positive correlation (a) ofT2* with subject’s age was observed:(slope = 0.153 ms per year,r = 0.377, P < 0.001). A negative correlation (b) ofT2* with subject’s BMD was observed: (slope =−6.1 ms g−1 cm2,r = −0.266, P < 0.005).
tation and signal detection. This might result in lower SNRas compared with the standard phase array surface coils forroutine MR imaging of the spine, but ensures excellent SNRuniformity throughout the whole imaging scanned volume.Moreover, no image post processing filtering are applied forSNR uniformity correction, a procedure that is routinely ap-plied when using surface coils. Body coil was therefore usedfor the measurements ofT2*, T2 andT1 parameters of thelumbar spine.
Moreover, the short initial TE’s used for the measurementof lumbar spineT2* (2.7–10 ms) are responsible for the im-proved SNR on images obtained at the initial echoes (Fig. 1).In addition, the use of coronal oblique pre-saturation slabsanterior to the spine suppresses motion artifacts (cardiacmovement and blood flow) as well as any adjacent signalproducing tissue anterior to the spine. Finally, the use of theweighted regression analysis fit enforces the points, which

T.G. Maris et al. / European Journal of Radiology 50 (2004) 245–256 253
0,5 0,6 0,7 0,8 0,9 1,0 1,1 1,2
T2
(ms)
40 45 50 55 60 65 70 7550
60
70
80
90
100
110
Age (yrs) BMD (g/cm2)
(a) (b)
Fig. 7. Linear regression ofT2 vs. age (a) and BMD (b) for all subjects (n = 101). A positive correlation (a) ofT2 with subject’s age was observed: (slope= 0.308 ms per year,r = 0.245, P < 0.05). A negative correlation (b) ofT2 with subject’s BMD was observed: (slope =−24.6 ms g−1 cm2, r = −0.345,P < 0.0005).
were measured with acceptable SNR (initial points on theT2* decay curve) (Fig. 3) as compared to those obtained onthe latest echoes. As a result only the initial in-phase echopoints (2nd, 4th, 6th, 8th, and 10th) echo of theT2* decaycurve actually contribute to the weighted fit for the calcula-tion of T2* in the non osteoporotic lumbar spine (Fig. 3).
Respiratory triggering and pre-saturation slabs applied inoblique coronal directions anterior to the spine were usedfor the measurement of lumbar spineT2. Respiratory trig-gering is used for the elimination any respiratory artifactsdue to patient breathing. Presaturation slabs help to suppresssignals and motion related artifacts (cardiac movement andblood flow) of the tissues adjacent to the spine.
40 45 50 55 60 65 70 75
3
4
5
6
7
8
9
10
11
T1
(ms)
(X 103)
0,5 0,6 0,7 0 8 0,9 1,0 1,1 1 2
Age (yrs) BMD (g/cm2)
(b)(a)
Fig. 8. Linear regression ofT1 vs. age (a) and BMD (b) for all subjects (n = 101). A negative correlation (a) ofT1 with subject’s age was observed:(slope =−6.50 ms per year,r = −0.329, P < 0.001). A positive correlation (b) ofT1 with subject’s BMD was observed: (slope = 237 ms g−1cm2,r = 0.212, P < 0.05).
In all of the MR sequences designed for bone marrowT2*measurements the fat contribution from the fatty marrow tothe signal decay signal was eliminated by carefully selectingthe inter-echo intervals of the GRE sequence[7,8,9,11,12].In this way only the water in-phase images were acquired;therefore signal modulation on the expected signalT2* de-cay interferogram was minimal[7,11,12]. T2* decay datawere then fitted by simplified single or bi-exponential mod-els for the calculation ofT2* [7,8,11].
In this study the concept was reversed. The fat con-tribution from the fatty marrow to theT2* signal decaywas not suppressed. Thirty-two gradient echoes were gath-ered duringT2* decay therefore resulting in a modulated

254 T.G. Maris et al. / European Journal of Radiology 50 (2004) 245–256
Table 5Correlations ofT2*, R2*, T2, R2, T2′, R2′, T1 andR1 parameters withBMDs for all subjects
Parameter All subjects (101)
Slope r p
T2* (ms) −6.10 ± 1.8 (ms g−1 cm2) −0.266 <0.005R2* (s−1) 43.1 ± 11.6 (s−1 g−1 cm2) 0.283 <0.005T2 (ms) −24.6 ± 5.9 (ms g−1 cm2) −0.345 <0.0005R2 (s−1) 3.54 ± 0.8 (s−1 g−1 cm2) 0.332 <0.0005T2′ (ms) −7.45 ± 2.49 (ms g−1 cm2) −0.228 <0.05R2′ (s−1) 39.6 ± 11.3 (s−1 g−1 cm2) 0.264 <0.001T1 (ms) 237± 89.8 (ms g−1 cm2) 0.212 <0.05R1 (s−1) −0.66 ± 0.3 (s−1 g−1 cm2) −0.184 <0.05
Note: mean± standard error.
interferogram pattern (Fig. 3). Information obtained fromthis interferogram pattern might be useful for quantitativeestimations concerning the fatty marrow content that isfound to be pronounced in the lumbar spine bone marrow.Quantification of the modulation, time series analysis oreven fractal analysis for estimating the complexity of theT2* signal decay curve might be valuable means for indi-rect assessment of osteoporosis and bone strength. One theother hand the presence of this modulation is not affectingthe measurement procedure of theT2* mainly because ofthe weighted linear regression analysis technique (in phaseechoes still are the determinants of theT2* values).
Results in the present study show a significant increasein the lumbar spineT2* and T2′ measurements in postmenopausal osteoporotic women as compared with a post-menopausal control subject group (Table 2). Our results areconsistent with those published in the literature from previ-
Table 6ROC analysis results for theT2*, R2*, T2, R2, T2′, R2′, T1 andR1 parameters.
Parameter Group A (n = 63) and Group B (n = 38)
Maximum accuracy criterion Sensitivity 95% CI Specificity 95% CI AUC 95% CI
T2* (ms) >12.5 (ms) 84.2 42.9 0.624± 0.06(68.7 − 93.9) (30.5− 56) (0.523− 0.719)
R2* (s−1) ≤79.4 (s−1) 84.2 42.9 0.624± 0.06(68.7 − 93.9) (30.5− 56) (0.523− 0.719)
T2 (ms) >91.1 (ms) 55.3 85.7 0.744± 0.05(38.3 − 71.4) (74.6− 93.2) (0.647− 0.825)
R2 (s−1) ≤11 (s−1) 55.3 85.7 0.744± 0.05(38.3 − 71.4) (74.6− 93.2) (0.647− 0.825)
T2′ (ms) >14.4 (ms) 86.8 39.7 0.611± 0.06(71.9 − 95.5) (27.6− 52.8) (0.509− 0.707)
R2′(s−1) ≤69.1 (s−1) 86.8 39.7 0.611± 0.06(71.9 − 95.5) (27.6− 52.8) (0.509− 0.707)
T1 (ms) ≤570.6 (ms) 63.2 68.3 0.652± 0.06(46 − 78.2) (55.3− 79.4) (0.550− 0.744)
R1 (s−1) >1.7 (s−1) 63.2 68.3 0.652± 0.06(46 − 78.2) (55.3− 79.4) (0.550− 0.744)
Assessment of their discrimination ability between Group A and Group B as compared with DXA measurements. AUC: area under curve.
T2*T2T2’T1
100-Specificity
Sens
itiv
ity
0 20 40 60 80 100
100
80
60
40
20
0
Fig. 9. ROC curves of theT2*, T2, T2′ and T1 parameters for the dis-crimination of postmenopausal osteoporotic from postmenopausal controlsubjects.T2* and T2′ measurements presented increased sensitivity (84.2,86.8, respectively),T2 measurements presented increased specificity (85.7)andT1 measurements presented moderate sensitivity and specificity (63.2,68.3) for the assessment of postmenopausal lumbar spine osteoporosis.
ous researchers[7,13]. The lesser value ofT2* in the osteo-porotic group (14.3 ms) as compared to that published byWehrli et al. [7] (18.4 ms) is partly due to the applicationof a different measurement strategy and on the fact that os-teoporotic women with low energy fractures were excludedfrom the present study (increased overall trabeculation).
Bone marrowT2* is also influenced from the non re-versible transverse relaxation timeT2 through its definition(Eq. (7)). The T2 and theT2* parameters of the trabecular

T.G. Maris et al. / European Journal of Radiology 50 (2004) 245–256 255
bone itself are in the order of�s and therefore they do notcontribute to either theT2 orT2* signal decay schemes esti-mated by the present MRI methods. The interest is thereforeaddressed to the measurement of theT2 of the bone marrowitself, which has to be assumed as a mixture of erithropoeiticand fatty marrow constituents each one having its ownT2value.
The change in lumbar spineT2 and thereforeR2 measure-ments was observed previously in an in vitro study[9]. Inthis study, Brismar et al. reported a relationship betweenR2and bone mineral measurement parameters. It was also sug-gested that the variation of bone marrow composition prob-ably affectsR2 and thereforeT2, to a greater extent than theamount of trabecular bone in clinical situations. The sameresearcher (Brismar TB) in an in vivo study[13] has reporteda significant positive correlation (r = 0.52,P < 0.05) of R2and areal BMDL1-L4 but this result was finally consideredto be a random observation. Early in vivo studies utilizingfat suppression imaging and spectroscopy techniques couldnot observe any significant difference inR2 between osteo-porotic and normal individuals[28].
In the present study where no fat suppression tech-niques were used a significant increase inT2 (significantdecrease inR2) between postmenopausal osteoporotic andpostmenopausal control subjects was observed. This resultcan be explained by applying Bloemengern’s Purcell andPound (BPP) theory considerations[29]. It is obvious thatthe presence of bone marrow plays a crucial role in theassessment of osteoporosis of the spine. The MR signalproducing spongy part of the vertebrae can be assumed as amixture of trabecular bone, erithropoeitic marrow and fattymarrow with a specific weighted average physical density,which resembles the physical density of a viscous liquid.Neither multi exponential behavior nor signal modulationwas observed in any of theT2 decay curves (Fig. 4a and b);therefore one average singleT2 value can be thus associatedwith each measurement.
According to the BPP theory[29], it is the translationaland rotational molecular correlation times (τc) of bone mar-row hydrogen protons and their natural precession frequency(�), which finally modulate bone marrowT1 andT2 values.In the normal clinical situation the condition of (ωτc > 1)is fulfilled [29]. As the BMD decreases (ageing or osteo-porosis) the physical density of the measurable spongy partof the vertebrae is getting lesser. This will eventually affect(τc) of the bone marrow hydrogen protons, which in turnwill affect bone marrowT1 andT2 values. As the physicaldensity decreasesT2 should monotonously increase (ωτc >
1, ωτc∼= 1, ωτc < 1) whereasT1 should initially decrease
(ωτc > 1), pass through a minimum (ωτc∼= 1, most effec-
tive fatty T1 relaxation) and then increase again (ωτc > 1,post traumatic edema present on non violent fractures).
Results in the present study show a significant positivecorrelation of lumbar spineT2* and T2′ with subject’s age(Table 3, Fig. 6a). Our results are consistent with thosepublished in the literature from previous researchers[7,13].
Bone marrowT2* andT2′ increase with age, correspondingto the known fact that mineral density decreases as one getsolder [7].
The increase of lumbar spineT2 (Table 3, Fig. 7a) aswell as the decrease of lumbar spineT1 (Table 3, Fig. 8a)with ageing is consistent with the predictions of BPP theory(less dense vertebrae). It is the authors’ suggestion that theobserved effect of increasingT2 and decreasingT1 withageing is mainly due to the presence of fatty bone marrow,which fills the intertrabecular space of the spongy part of thevertebrae resulting in a less dense vertebrae. The increase offatty marrow with ageing was confirmed from early in vitroquantitative histological studies[30] and recent in vivo MRspectroscopy studies[31].
Results in the present study show a significant negativecorrelation of lumbar spineT2* andT2′ with subject’s BMDmeasurements (Table 5, Fig. 6b). From these results it ap-pears that only a small percentage of the variability of MRImeasurements can be explained by BMD. The remaindermay be determined by other properties of bone related tobone strength. Our results are consistent with those pub-lished in the literature from previous researchers[7,13]. Thedecrease of lumbar spineT2 (Table 5, Fig. 7b) as well as theincrease of lumbar spineT1 (Table 5, Fig. 8b) with BMDmeasurements is also consistent with the predictions of BPPtheory (less dense vertebrae).
Again the presence of fatty marrow filling the intertra-becular space can be assumed to be responsible for the ob-served decrease ofT2 and concomitant increase ofT1 withBMD. The observed prolonged signal modulation inT2* de-cay curves (Fig. 3b) is in accordance with this assumption.A more pronounce effect should be expected (greater slopesfor T2 decrease and decrease ofT1 with BMD) when posttraumatic edema related to non violent fractures is present.In this caseT2* decay signal modulation should be minimal.
Of all MR relaxometry measured parameters lumbar spineT2* and T2′ are directly related to the osteoporosis sta-tus. The fact that according to BPP theory bone marrowT2should monotonously increase as the vertebrae is getting lessdense makesT2 a valuable means for the indirect estimationof osteoporosis. This is not the case for the bone marrowT1, which according to BPP theory should pass through aminimum as the vertebrae is getting less dense. This facteventually makes theT1 parameter less sensitive in the in-direct estimation of osteoporosis.T2* and T2′ were provedto be more sensitive parameters in differentiation of osteo-porotic from control subjects (Table 6, Fig. 9). One the otherhand,T2 was proved to be more specific (Table 6, Fig. 9).T1 was not either sensitive or specific in estimating osteo-porosis status (Table 6, Fig. 9).
5. Conclusion
In conclusion, this study has shown thatT2*, T2, T2′and T1 MR relaxometry techniques can detect age-related

256 T.G. Maris et al. / European Journal of Radiology 50 (2004) 245–256
influences on bone status.T2 had a stronger relationship withBMD than the other MR parameters examined in the currentstudy. Lumbar spineT2* andT2′ are more sensitive whereasT2 is more specific in assessing lumbar spine osteoporosiswith reference to BMD status.
References
[1] Majumdar S, Genant HK, Grampp S, et al. Correlation of tra-becular bone structure with age, bone, mineral density, and osteo-porotic status: in vivo studies in the distal radius using high reso-lution magnetic resonance imaging. J Bone Miner Res 1997;12(1):111–8.
[2] Link T, Majumdar S, Grampp S, Guglielmi G, van Kuijk C, ImhofH, et al. Imaging of trabecular bone structure in osteoporosis. EurRadiol 1999;9:1781–8.
[3] Vieth V, Link T, Lotter A, Persigehl T, Newitt D, Heindel W, etal. Does the trabecular bone structure depicted by high resolutionMRI of the calcaneus reflect the true bone structure. Invest Radiol2001;36(4):210–6.
[4] Bourty N, Cortet B, Dubois P, Marchandise X, Cotten A. Trabecularbone structure of the calcaneus: preliminary in vivo MR imagingassessment in men with osteoporosis. Radiology 2003;227:708–17.
[5] Jara H, Wehrli F, Chung H, Ford J. High resolution variable flipangle 3D MR imaging of trabecular microstructure in vivo. MagnReson Med 1993;29:528–39.
[6] Hipp J, Jansujwicz A, Simmons C, Snyder B. Trabecular bonemorphology from micro-magnetic resonance imaging. J Bone MinerRes 1996;11:286–92.
[7] Wehrli FW, Ford CJ, Haddad GJ. Osteoporosis: clinical assessmentwith quantitative MR imaging in diagnosis. Radiology 1995;196:631–41.
[8] Link MT, Majumdar S, Augat P, et al. Proximal femur: assessmentfor osteoporosis withT2* decay characteristics at MR imaging.Radiology 1998;209:531–6.
[9] Brismar TB, Karlsson M, Li TQ, Ringertz H. The correlation betweenR2′ and bone mineral measurements in human vertebrae: an in vitrostudy. Eur Radiol 1999;9:141–4.
[10] Fransson A, Grampp S, Imhof H. Effects of trabecular bone onmarrow relaxation in the tibia. Mag Reson Imag 1999;17(1):69–82.
[11] Machann J, Schnatterbeck P, Raible A, Lutz O, Claussen CD, SchickF. Magnetic resonance osteodensitometry in human heel bones. Cor-relation with quantitative computed tomography using different mea-suring parameters. Invest Radiol 2000;35(7):393–400.
[12] Wehrli FW, Hopkins JA, Hwang SN, Song HK, Snyder PJ, HaddadJC. Cross-sectional study of osteopenia with quantitative MR imagingand bone densitometry. Radiology 2000;217:527–38.
[13] Brismar TB. MR relaxometry of lumbar spine, hip and calca-neus in healthy premenopausal women: relationship with dual en-
ergy X-ray absorptiometry and quantitative ultrasound. Eur Radiol2000;10:1215–21.
[14] Davis CA, Genant HK, Dunham JS. The effects of bone on pro-ton NMR relaxation times of surrounding liquids. Invest Radiol1986;21:472–7.
[15] Sebag GH, Moore SG. Effects of trabecular bone on the appearanceof marrow in gradient echo imaging of the appendicular skeleton.Radiology 1990;174:855–9.
[16] Grampp S, Majumdar S, Jergas M, Lang P, Gies A, Genant HK. MRIof bone marrow in the distal radius: in vivo precision of effectivetransverse relaxation times.
[17] Ma J, Wehrli FW. Method for image-based measurerement of thereversible and irreversible contribution to the transverse relaxationrate. J Magn Reson Ser B 1996;111:61–9.
[18] Capuani S, Alessandri FM, Bifone A, Maraviglia B. Multiple spinechoes for the evaluation of trabecular bone quality. MAGMA2002;14:3–9.
[19] Kang C, Paley M, Ordidge R, Speller R. In vivo MRI measurementsof bone quality in the calcaneus: a comparison with DXA andultrasound. Osteoporosis Int 1999;9:65–74.
[20] Assessment of fracture risk and its application to screening forpostmenopausal osteoporosis: report of a WHO study group. GenevaSwitzerland, Technical Report Series, WHO 1994; no. 843.
[21] Reichenbach JR, Hacklander T, Hofer M, Rassek M, Modder U.1H T1 and T2 measurements of the MR imaging contrast agentsGd-DTPA and Gd-DTPA BMA at 1.5T. Eur Radiol 1997;7:264–74.
[22] Haase A, Frahm J, Matthaei D, Haenicke W, Merbolt KD. FLASHimaging. Rapid NMR imaging using low flip angle pulses. J MagnReson 1986;67:258–66.
[23] Graumann R, Oppelt A, Stetter E. Multiple-spin-echo imaging witha 2D Fourier method. Magn Reson Med 1984;3:707–21.
[24] Haase A. Snapshot FLASH MRI. Applications toT1, T2, and chem-ical shift imaging. Magn Reson Med 1990;13:77–89.
[25] Kaufman L, Kramer DM, Crooks EL, Ortendahl DA. Measuringsignal to noise ratios in MR imaging. Radiology 1989;173:265–7.
[26] Bevington PR. Data reduction and error analysis for the physicalsciences, New York: McGraw-Hill; 1969.
[27] Wehrli FW, Ma J, Hopkins JA, Song HK. Measurement ofR2’ in thepresense of multiple spectral components using reference spectrumdeconvolution. J Magn Reson 1998;131:61–8.
[28] Traber F, Block W, Layer G, Braucker G, Giesecke J, Kretzer S, etal. Determination of1H relaxation times of water in human bonemarrow by fat suppressed turbo spin echo in comparison to MRspectroscopic methods. J Magn Reson Imaging 1996;6:541–8.
[29] Bloembergen N, Purcell ME, Pound VR. Relaxation effects in nuclearmagnetic resonance absorption. Phys Rev 1948;73(7):679–712.
[30] Dunhill MS, Anderson JA, Whitehead R. Quantitative histologicalstudies on age changes in bone. J Pathol Bact 1967;94:275–91.
[31] Schellinger D, Lin CS, Fertikh D, Lee JS, Lauerman WC, HendersonF, et al. Normal lumbar vertebrae: anatomic, age, and sex variance insubjects at proton MR spectroscopy—initial experience. Radiology2000;215:910–6.