assessing phlebitis: caution advised
TRANSCRIPT

Assessing phlebi,s: Cau,on advised!
Gillian Ray-‐Barruel, RN, BSN, Grad Cert ICU Nursing, BA(Honours) Senior Research Assistant, OMG PIVC Study PI and Coordinator AVATAR Group, Menzies Health Ins,tute Queensland, Griffith University
4th SEHA Interna.onal Nursing Conference Abu Dhabi, UAE, November 24-‐25, 2015

Session objec,ves 1. Describe the current challenges for achieving excellence in the care provided to the pa,ent with a PIVC. 2. Review the role of nursing research in promo,ng the development of innova,ve strategies to achieve excellence in healthcare seZngs. 3. Propose steps for developing innova,ve strategies to achieve excellence in pa,ent care considering the various challenges nurses are encountering.

RCTs
Cochrane Reviews
Micro lab studies
Prac,ce surveys, Cohort studies
Knowledge transla,on, Educa,on
Health Economics
Pilot trials, Simula,on
Professor Claire Rickard, AVATAR Founder and Head

• Over a billion PIVCs inserted annually worldwide • Most common clinical procedure
• Blood sampling • Emergency admission / resuscita,on • Parenteral medica,on • IV fluids
• >60% of hospital inpa,ents have a PIVC during admission
• Phlebi,s significantly increases risk of future phlebi,s (Hadaway 2012; Gallant et al, 2006; Palefski et al, 2001)
Why should we care about PIVCs?

Examined phlebi,s scoring tools and signs/symptoms for reliability, validity, feasibility, responsiveness.
COSMIN guidelines (COnsensus-‐based Standards for the selec,on of health Measurement Instruments)
Phlebi,s Scales Systema,c Review

Results v 233 studies reported infusion phlebi,s as the primary outcome
measure v 53 of these provided no defini,on of phlebi,s, despite the study
measuring phlebi,s v 180 studies reported measuring phlebi,s incidence or severity
and gave a defini,on v Of these, 101 used an assessment scale v 79 used a defini,on only
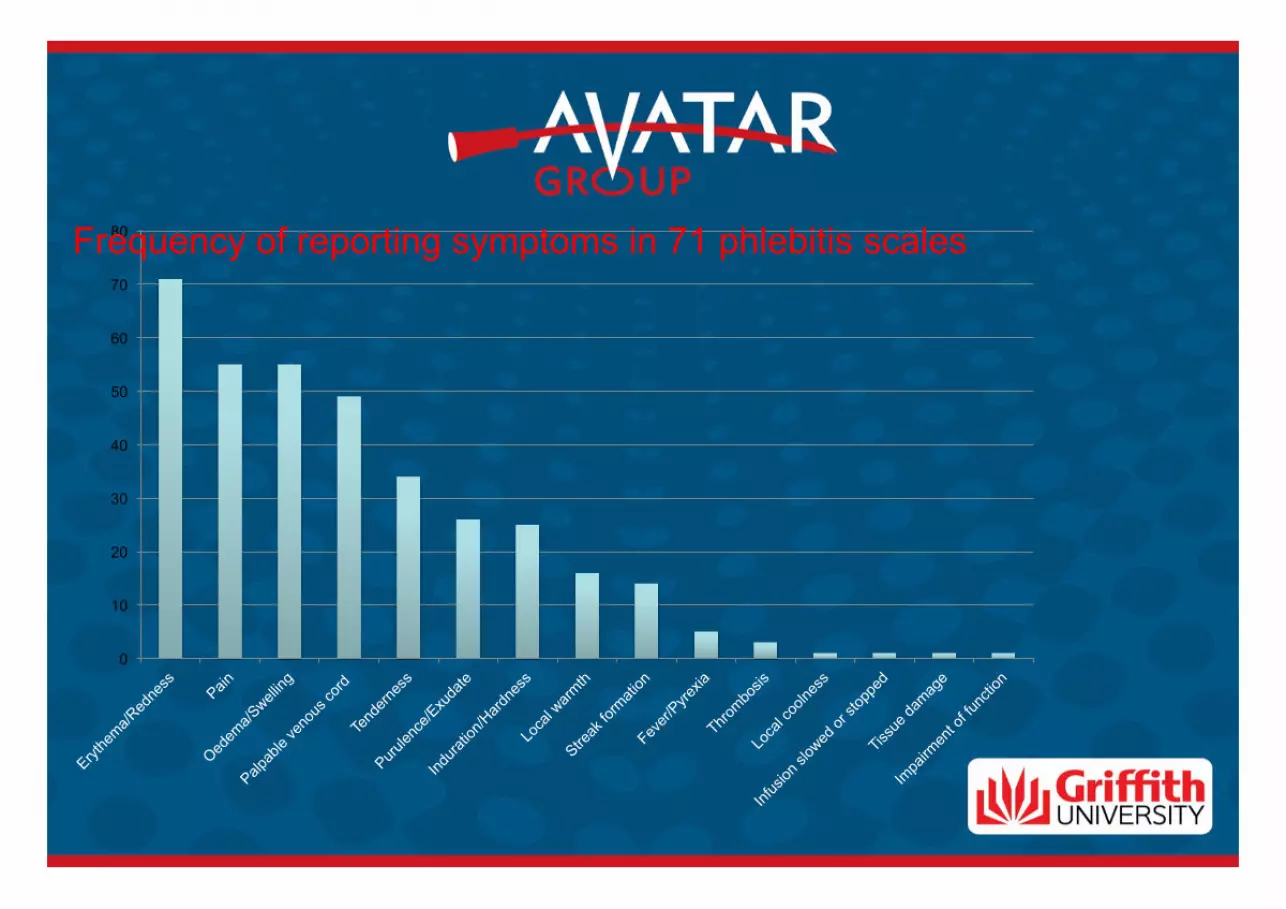
§ 71 different phlebi,s scales § 15 different signs/symptoms
0
10
20
30
40
50
60
70
80 Frequency of reporting symptoms in 71 phlebitis scales

Reported phlebi,s prevalence • 0-‐91% for studies using a scale • 0-‐100% for studies using a defini,on alone • Repor,ng measures varied widely
• (per PIVC, per pa,ent, per catheter day) Lack of consistency in measuring phlebi6s likely contributes to the variability in reported phlebi6s rates

Results
• Many phlebi,s scales and tools exist, but none has been properly validated for use in the clinical seZng.
• Studies that reported tes,ng the psychometric proper,es of scales (VIP, INS, PVC ASSESS, etc.) all had several major limita,ons.

Inter-‐rater study of phlebi,s signs • Subset of a large mul,centre RCT (3283 pa,ents, 5907 PIVCs) (Rickard et al, Lancet, 2012)
• 210 pa,ents, 3 hospitals, 246 sets of paired observa,ons undertaken within a 10 min ,meframe.
• Blinded observa,on, 2 RN raters, 5 min apart
• 7 signs & symptoms (pain, tenderness, erythema, swelling, warmth, purulent discharge, and palpable cord

Inter-‐rater study • The inter-‐rater data were modelled into phlebi,s scores using 10 different scoring tools
• (Barker, Baxter, Catney, Curran, Lanbeck, Maki, Rickard, Rinenberg, Van Donk, and Visual Infusion Phlebi,s [VIP] scales).
• Only published phlebi,s tools that used the 7 symptoms our nurses assessed could be included in the modelling.
• Propor,ons of specific agreement (e.g. posi,ve, nega,ve), observed and expected agreements, Cohen’s kappa, the maximum achievable kappa, prevalence-‐ and bias-‐adjusted kappa were calculated.
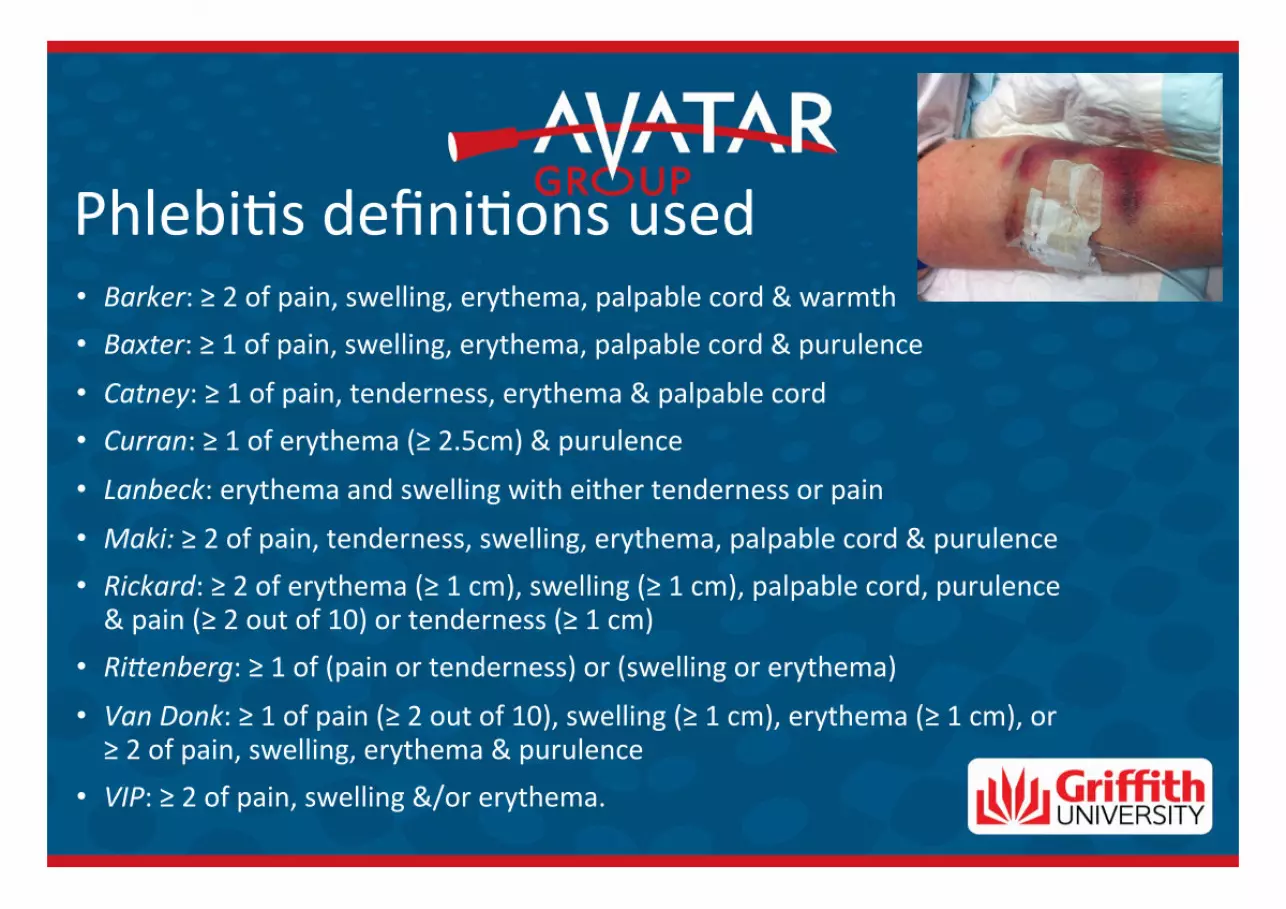
• Barker: ≥ 2 of pain, swelling, erythema, palpable cord & warmth • Baxter: ≥ 1 of pain, swelling, erythema, palpable cord & purulence
• Catney: ≥ 1 of pain, tenderness, erythema & palpable cord • Curran: ≥ 1 of erythema (≥ 2.5cm) & purulence
• Lanbeck: erythema and swelling with either tenderness or pain
• Maki: ≥ 2 of pain, tenderness, swelling, erythema, palpable cord & purulence • Rickard: ≥ 2 of erythema (≥ 1 cm), swelling (≥ 1 cm), palpable cord, purulence & pain (≥ 2 out of 10) or tenderness (≥ 1 cm)
• Ri?enberg: ≥ 1 of (pain or tenderness) or (swelling or erythema)
• Van Donk: ≥ 1 of pain (≥ 2 out of 10), swelling (≥ 1 cm), erythema (≥ 1 cm), or ≥ 2 of pain, swelling, erythema & purulence
• VIP: ≥ 2 of pain, swelling &/or erythema.
Phlebi,s defini,ons used

Findings
• The most prevalent symptom was tenderness: 47/246 observa,ons (19.1%).
• The Catney and Rinenberg scales were the most sensi,ve (phlebi,s in > 20% of observa,ons)
• Barker and VIP scales were the most restric,ve (no phlebi,s detected).
• Only ‘tenderness’ ‘erythema’, and the Catney and Rinenberg scales had acceptable (66.7%) levels of inter-‐rater agreement.

Summary
• Inter-‐rater agreement for phlebi,s assessment signs/symptoms and scales is generally low.
• Poor agreement likely contributes to the high degree of variability in phlebi,s rates in the literature.
• Further research and new approaches to assessing vein irrita,on are needed.

No exis,ng phlebi,s scale or defini,on can be recommended
XINS Phlebitis Scale Grade 0 – No symptoms Grade 1 – Erythema at access site with or without pain Grade 2 – Pain at access site with erythema and/or edema Grade 3 – Pain at access site with erythema and/or edema, streak formation, palpable venous cord. Grade 4 – Pain at access site with erythema and/or edema, streak formation, palpable venous cord greater than 1 in in length; purulent drainage. X

Regular assessment of the PIVC site is key! Use clinical judgement!
• Is it needed? Ø If not, remove it. Don’t leave it there, just in case.
• Is it tolerated by the patient? Ø If not, remove it. Consider other access (e.g. oral, PICC)
• Is it working? Ø If not, remove it. Resite IV or insert PICC.
• Is there any evidence of infection from an unknown source? Ø If so, remove the cannula.

• 5,907 PIVCs from 3,283 pa,ents
• Post-‐infusion phlebi,s at 48 hours was diagnosed in 59 (1.8%) pa,ents.
• Fiteen (25.4%) of these pa,ents had phlebi,s at removal and also at 48 hours ater removal.
• Even ater the catheter is removed, the site should be checked daily for at least 48 hours.
Post-‐infusion Phlebi,s

References Marsh N, Mihala G, Ray-‐Barruel G, Webster J, Wallis MC, Rickard CM. Inter-‐rater agreement on PIVC-‐associated phlebi,s signs, symptoms and scales. J Eval Clin Pract. 2015;21(5):893-‐9. Ray-‐Barruel G, Polit DF, Murfield JE, Rickard CM. Infusion phlebi,s assessment measures: a systema,c review. J Eval Clin Pract. 2014;20(2):191-‐202. Rickard CM, Webster J, Wallis MC, Marsh N, McGrail MR, French V, et al. Rou,ne versus clinically indicated replacement of peripheral intravenous catheters: a randomised controlled equivalence trial. Lancet. 2012;380(9847):1066-‐74. Webster J, McGrail M, Marsh N, Wallis MC, Ray-‐Barruel G, Rickard CM. Pos,nfusion Phlebi,s: Incidence and Risk Factors. Nurs Res Pract. 2015;2015:691934.

For more informa,on or to get involved in IV research, please contact us: www.avatargroup.org.au
Ques,ons?