anesthesia breathing systems
TRANSCRIPT

+
Anesthesia Breathing SystemsProf. Karen Haddock, CRNA
+ Anesthesia Breathing Systems Purpose
To deliver anesthetic gases and oxygen Offer a means to deliver anesthesia without significant increase in airway resistance
To offer a convenient and safe method of delivering inhaled anesthetic agents
+ Anesthesia Breathing Systems Basic Principles
All anesthesia breathing systems have 2 fundamental purposesDelivery of O2/Anesthetic gasesElimination of CO2 (either by washout with adequate fresh gas flow (FGF) or by soda lime absorption)
+ Anesthesia Breathing SystemsResistance to flow can be minimized by:Reducing the circuit’s lengthIncreasing the diameter Avoiding the use of sharp bendsEliminating unnecessary valvesMaintaining laminar flow
+ Anesthesia Breathing SystemsClassifications (controversial)Traditional attempts to classify circuits combine functional aspects (eg, extent of rebreathing) with physical characteristics (eg, presence of valves)
Based on the presence or absence ofA gas reservoir bagRebreathing of exhaled gasesMeans to chemically neutralize CO2
Unidirectional valves
+ Anesthesia Breathing SystemsClassifications
OpenSemiopenSemiclosedClosed
+ Anesthesia Breathing Systems
+ Anesthesia Breathing SystemsClassifications
OpenNo reservoirNo rebreathingNo neutralization of CO2No unidirectional valves
+ Anesthesia Breathing SystemsClassifications
OpenNasal cannulaOpen drop etherThink of it as anything where there is NO rebreathing and NO scavenging

+ Anesthesia Breathing SystemsClassifications
SemiopenGas reservoir bad presentNO rebreathingNo neutralization of CO2No unidirectional valvesFresh gas flow exceeds minute ventilation
Examples includeMapleson A, B, C, DBainJackson-Rees
+ Anesthesia Breathing SystemsNon-rebreathing circuits
Mapleson – 1954 Mapleson D still commonly used Mapleson F is better known as Jackson-Rees Modified Mapleson D is also called Bain
Used almost exclusively in children Very low resistance to breathing The degree of rebreathing is influenced by method of ventilation
Adjustable overflow valve Delivery of FGF should be at least 2x the minute volume
+ Non-rebreathing Circuits
All non-rebreathing (NRB) circuits lack unidirectional valves and soda lime CO2 absorption
Amount of rebreathing is highly dependent on fresh gas flow (FGF)
Work of breathing is low (no unidirectional valves or soda lime granules to create resistance)
+ Anesthesia Breathing SystemsClassifications
Closed Always has a gas reservoir bag Allows for TOTAL rebreathing of exhaled gases Always provides for chemical neutralization of CO2
Always contains unidirectional valves We don’t use these….Suffice to say you can do this with the machines we have now if you keep your fresh gas flow to metabolic requirements around 150ml/min
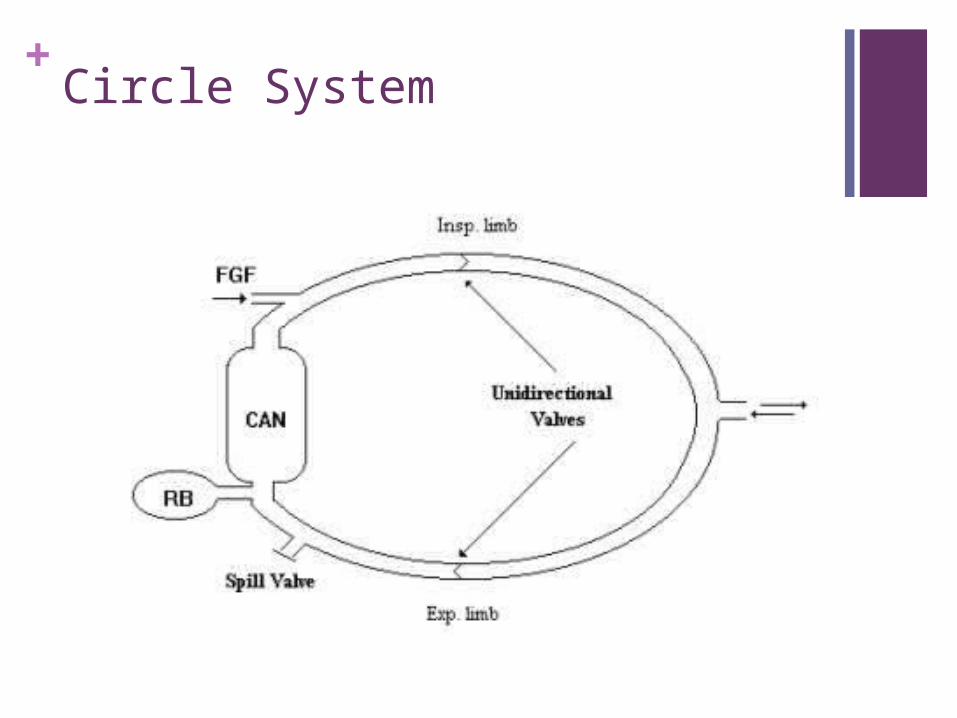
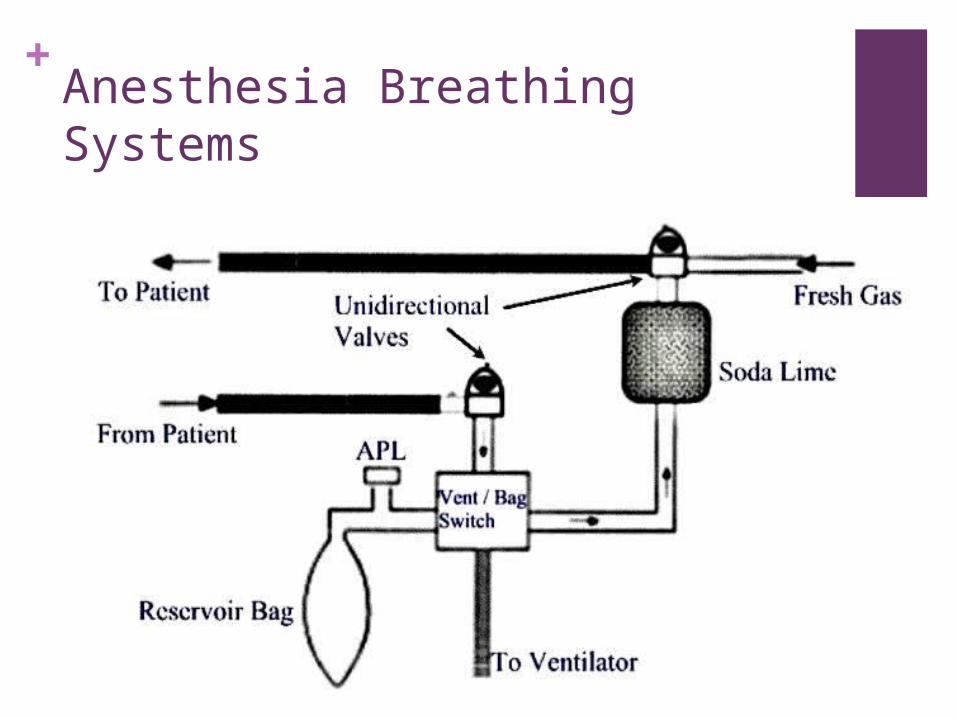
+ Circle System
+ Optimization of Circle Design Unidirectional Valves
Close to pt to prevent backflow into inspiratory limb if circuit leak develops.
Fresh Gas Inlet Placed between absorber & inspiratory valve. If placed downstream from insp valve, it would allow FG to bypass pt during exhalation and be wasted. FG placed between expiration valve and absorber would be diluted by recirculating gas
+ Optimization of Circle Design APL valve
Placed immediately before absorber to conserve absorption capacity and to minimize venting of FG
Breathing Bag Placed in expiratory limb to decrease resistance to exhalation. Bag compression during controlled ventilation will vent alveolar gas thru APL valve, conserving absorbent
+ Circle system can be:
closed (fresh gas inflow exactly equal to patient uptake, complete rebreathing after carbon dioxide absorbed, and pop-off closed)
semi-closed (some rebreathing occurs, FGF and pop-off settings at intermediate values), or
semi-open (no rebreathing, high fresh gas flow)
+ Anesthesia Breathing Systems Circle systems
Unidirectional valves Prevent inhalation of exhaled gases until they have passed through the CO2 absorber (enforced pattern of flow)
Incompetent valve will allow rebreathing of CO2
Hypercarbia and failure of ETCO2 wave to return to baseline
Pop off (APL) Valve Allows pressure control of inspiratory controlled ventilation
Allows for manual and assisted ventilation with mask, LMA, or ETT
+ Anesthesia Breathing SystemsCircle systems
Most commonly usedAdult and child appropriate sizes
Can be semiopen, semiclosed, or closed dependent solely on fresh gas flow (FGF)
Uses chemical neutralization of CO2
Conservation of moisture and body heat

+ Anesthesia Breathing SystemsCircle system
Allows for mechanical ventilation of the lungs using the attached ventilator
Allows for adjustment of ventilatory pressure
Is easily scavenged to avoid pollution of OR environment
Low FGF’s saves money
+ Anesthesia Breathing Systems Advantages of rebreathing
Cost reduction (use less agent and O2) Increased tracheal warmth and humidity Decreased exposure of OR personnel to waste gases
Decreased pollution of the environment REMEMBER that the degree of rebreathing in an anesthesia circuit is increased as the fresh gas flow (FGF) supplied to the circuit is decreased
+ Anesthesia Breathing Systems
+ Anesthesia Breathing Systems
Dead space Increases with the use of any anesthesia system Unlike Mapleson circuits, the length of the breathing tube of a circle system DOES NOT directly affect dead space
Like Mapleson’s, length DOES affect circuit compliance (affecting amount of TV lost to the circuit during mech vent)
Increasing dead space increases rebreathing of CO2 To avoid hypercarbia in the face of an acute increase in dead space, a patient must increase minute ventilation
Dead space ends where the inspiratory and expiratory gas streams converge

+ Anesthesia Breathing Systems
Carbon dioxide neutralizationInfluenced by
Size of granules Presence or absence of channeling in the canister (areas of loosely packed granules, minimized by baffle system)
Tidal volume in comparison to void space of the canister
Ph sensitive dye Ethyl violet indicator turns purple when soda lime exhausted (change when 50-70% has changed color)
Regeneration: Exhausted granules may revert to original color if rested, no significant recovery of absorptive capacity occurs
+ Anesthesia Breathing SystemsCarbon dioxide neutralization
Maximum absorbent capacity 23-26L of CO2/100g granules
Granules designated by Mesh size (4-8 mesh)A compromise between higher absorptive surface area of small granules & the lower resistance to gas flow of larger granules
Toxic byproductsThe drier the soda lime, the more likely it will absorb & degrade volatile anesthetics
+ Disadvantages of Circle SystemGreater size, less portabilityIncreased complexity
Higher risk of disconnection or malfunction
Increased resistanceDissuading use in Pediatrics
Difficulty of predicting inspired gas concentration during low fresh gas flow
+ Anesthesia Breathing Systems
Airway Humidity Concerns Anesthesia machine FGF dry and cold
Medical gas delivery systems supply dehumidified gases at room temp.
Exhaled gas is saturated with H2O at body temp High flows (5 L/min) low humidity Low flows (<0.5 L/min) allow greater H2O saturation Absorbent granules: significant source of heat/moisture (soda lime 14-19% water content)
Normal upper airway humidification bypassed under General Anesthesia
Passive heat and humidity (“Artificial Nose”) Active heat and humidity (electrically heated humidifier)
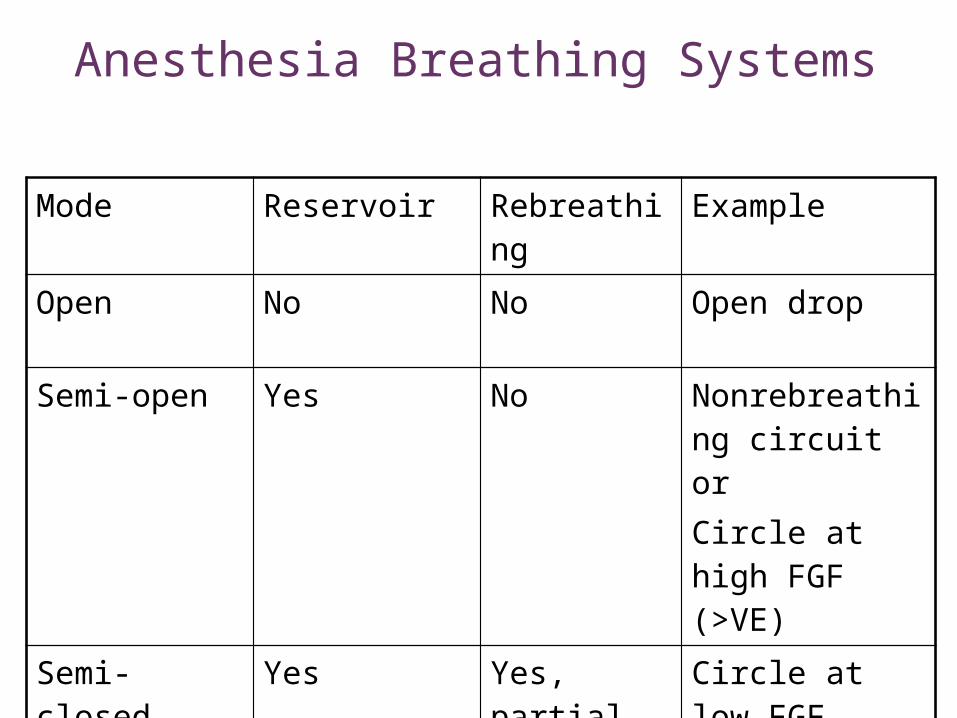
Anesthesia Breathing Systems
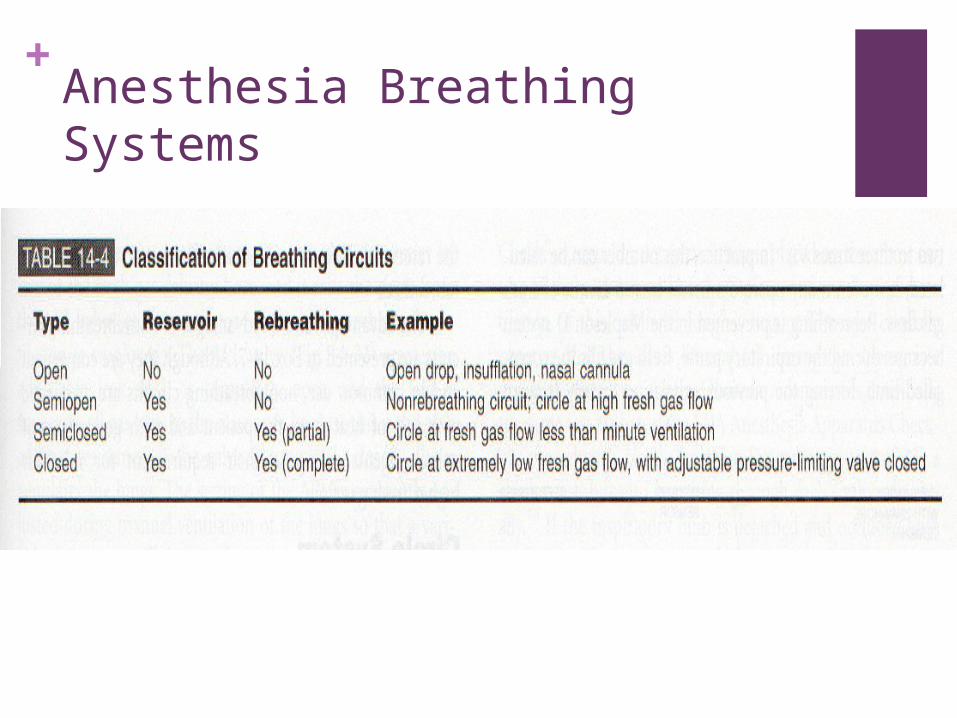
Mode Reservoir Rebreathing
Example
Open No No Open drop
Semi-open Yes No Nonrebreathing circuit or Circle at high FGF (>VE)
Semi-closed
Yes Yes, partial
Circle at low FGF (<VE)
Closed Yes Yes, complete
Circle (if APL valve closed)
+Reference
Morgan, G. E., Mikhail, M. S., Murray, M. J., & Larson, P. C. , (2013). Clinical anesthesiology (4rd ed.). New York: The McGraw-Hill Companies, Inc..
Stoelting, R. K., Miller, R. D. ,(2007). Basic of Anesthesia (5th ed.). New York: Churchill Livingstone Elsevier, Inc. (2011). MemoryMaster. Des Moines: