an e-learning platform for aerospace medicine
TRANSCRIPT

15HIPPOKRATIA 2008, 12 (Suppl 1)HIPPOKRATIA 2008, 12 (Suppl 1): 15-22
ORIGINAL ARTICLE
The appeal of online education through distance
learning as an educational alternative is ever increasing.
Technological advances in medicine, aerospace, agricul-
ture, the environment, communications and education
permeate the world we live in. To support and accommo-
date the over-specialized knowledge available by differ-
ent experts, information technology can be employed to
develop virtual distributed pools of autonomous special-
ized educational modules and provide the mechanisms
for searching, retrieving, evaluating and rating, adapting
and revising educational content. In addition, research
has predicted that in the future more people will complete
their studies at home, as distance learning concepts con-
tinue to evolve. E-learning offers both synchronous and
asynchronous modes of learning thus enabling a student
to access information from anywhere and at anytime.
E-learning environments have generally been suc-
cessful and, therefore, nowadays the majority of the uni-
versities provide online courses in some way. Numerous
efforts to create e-learning courses have also been spent
within medical education as well, covering various the-
matic areas, including aviation and aerospace medicine.
However, there exist limited efforts attempting to cre-
ate an e-learning course on aviation and aerospace medi-
cine conformant and compliant with the international
Standard SCORM (Shareable Content Object Reference
Model). Furthermore, and to the best of our knowledge,
there has been no attempt in complementing a SCORM
compliant course on aviation and aerospace medicine
with the so called Healthcare Learning Object Metadata.
The remainder of this paper is structured as follows.
In section 2 we provide a brief account on current trends
and approaches in online Medical Education with empha-
sis in aviation medicine, while in section 3, a brief over-
view of the modules necessary for the creation of courses
compliant and conformant with SCORM is provided. The
following two sections focus on the technological issues
involved in creating the SCORM compliant course on
pulmonary disorders in aviation medicine, together with
the structure and the educational details of the speciic course, while in the last section, a discussion on key is-
sues of concern is augmented with insights into future
work.
Background Information
The importance of online courses and e-learning in
post secondary career oriented medical education has
been identiied in some recent studies alongside with the beneits of and demand for offering continuing education to health professionals1,2. Moreover, some researchers
conclude that e-learning may be a very useful tool, but
emphasis has to be placed upon appropriate designs tak-
ing care of the fact that certain educational goals have to
be met3 irrespective of the media used4; such educational
goals, however, may be electronically linked to online
material itself by utilizing the SCORM standard5,6.
An e-learning platform for Aerospace Medicine
Bamidis PD1,2, Konstantinidis S1, Papadelis CL1,2, Perantoni E2, Styliadis C1,2, Kourtidou-Papadeli C2, Pappas C1
1 Lab of Medical Informatics, Medical School, Aristotle University of Thessaloniki, Thessaloniki, Greece2 Greek Aerospace Medical Association and Space Research
Abstract
The appeal of online education and distance learning as an educational alternative is ever increasing. To support and
accommodate the over-specialized knowledge available by different experts, information technology can be employed
to develop virtual distributed pools of autonomous specialized educational modules and provide the mechanisms for
retrieving and sharing them. New educational standards such as SCORM and Healthcare LOM enhance this process of
sharing by offering qualities like interoperability, accessibility, and reusability, so that learning material remains credible,
up-to-date and tracks changes and developments of medical techniques and standards through time. Given that only a
few e-learning courses exist in aerospace medicine the material of which may be exchanged among teachers, the aim
of this paper is to illustrate the procedure of creating a SCORM compliant course that incorporates notions of recent
advances in social web technologies. The course is in accordance with main educational and technological details and
is speciic to pulmonary disorders in aerospace medicine. As new educational trends place much emphasis in continuing medical education, the expansion of a general practitioner’s knowledge in topics such as aviation and aerospace pulmo-
nary disorders for crew and passengers becomes a societal requirement. Hippokratia 2008; 12 (Suppl 1): 15-22
Keywords: SCORM, Healthcare LOM, IEEE LOM, Continuing Medical Education, CPD, aviation medicine, online
education, aerospace medicine, pulmonary disorders
Corresponding author: Bamidis PD; Lab of Medical Informatics, Medical School, Aristotle University of Thessaloniki, Greece, Tel: +30-
2310-999310, e-mail: [email protected]

16 BAMIDIS PD
An interesting aspect that is under continuous scien-
tiic discussions and developments over the last few years is the enhancement of medical education with 3D virtual
environments7-9, with the majority of them targeting to a
speciic area, e.g. mental illness10, or rheumatology11. It
seems that the use of such Internet-connected graphics
environments holds promise for public education as evi-
denced by research on the learners’ reactions12,13.
The ield of Aviation Medicine is not an exception in this evolving story. Many countries are currently using
e-learning courses to train medical doctors in the ield of aviation and aerospace medicine (USA, UK, Taiwan,
Germany, the Netherlands and others). Federal Aviation
Authorities in USA are offering online training courses to
international aviation medical examiners enabling them
to renew their authorization. In addition, British Airways
(BA) in the UK provide light and cabin crews with e-Learning projects. Aviation medicine programs have also
been delivered on CD-ROMs, designed to increase efi-
ciency when used in parallel with the Flight Crew simula-
tor check, but also achieve cost reductions by eliminating
the necessity for a medical trainer presence around the
clock. Such programs aim to provide light crew with up-to-date information about medical equipment on board
aircraft, life-saving skills, personal health advice and the
use of the MedLink service. BA had designed a one hour
training course which would be produced by Maxim14-16.
The 6th Panhellenic Clinical Aviation Medicine semi-
nar was organised in Skiathos Island, Greece, in late
August 2007, during the 5th International conference of
Aerospace Medicine organized by GASMA, the Greek
Aerospace Medical Association and Space Research. It
was accredited with 13 CME credits by the Hellenic Na-
tional Medical Association. This course was motivated by
the recent observation that a number of universities and
colleges have shown interest in developing courses in the
ield of aviation; however, there usually exists an inher-ent dificulty in achieving this, as only a few qualiied lecturers can be found among faculty members in most
universities and colleges. Since aviation technology en-
compasses various subjects in engineering, management,
medicine, and regulations, it is almost impossible to ind a lecturer who is qualiied to cover such a wide range of areas. On the other hand, providing students with a com-
prehensive knowledge background of aviation is deemed
very essential. Thus, a course at the entry-level, with the
scope of introducing various areas of aviation medicine
seems meaningful, as it may serve as a basic introductory
course for an aviation curriculum, currently under devel-
opment in various universities and colleges.
Moreover, postgraduate education is moving towards
blended learning solutions combining high-quality e-
learning with a mixture of paper-based material, classi-
cal or online meetings, CDs and other digital content, as
well as, material uploaded on the internet. This is true for
continuous medical education too; for example, what a
General Practitioner usually needs, is a real combination
of learning media and modes, well packaged and associ-
ated with appropriate learning objectives and outcomes,
and linked with formal routes to professional accredita-
tion5,17.
Material and Methods
E-learning environments
An e-learning environment can be characterized as
a Learning Management System (LMS) complemented
with synchronous and asynchronous communication
tools. Furthermore, an LMS compliant with SCORM18
refers to a suite of functionalities designed to deliver,
track, report on and manage learning content, learner
progress and learner interactions.
Two main user roles are encountered in learning envi-
ronments: “Student” and “Teacher”. Individual needs of
each role are obviously clear within classical educational
procedures, but those needs should also be reinforced and
transferred to speciications of interactive e-learning en-
vironments. The addition of a third use role, the “admin-
istrator”, is mandatory in such role-based e-environments
(Student, Teacher, and Administrator).
The user–Teacher should have the capability to
implement the following tasks:
1. Add/Modify Resources
2. Create/Update Glossary
3. Add/Invite User-Learner
4. Add/Participate to a Communication Module
5. Reset the Course
On the other hand, some other actions should be made
available to the learner (user-Student):
1. View Course Events
2. Add/Modify Personal Events
3. View/ Add to Glossary (depending on the proper-
ties of Glossary set by the User-Teacher)
4. View/Get Resources (Topic Labels, Text Pages,
Web Pages, Files or Web Sites and Directories having a
group of Files) that are available by the User-Teacher
5. Submit Tasks within a speciic time limit.6. Get Notiication for: Submitting Tasks, updated or
new Resources, announcements of Grades and Commu-
nication Modules that have been initialised or providing
new (updated) information.
7. Interact in Communication Modules:
• Create a new Forum (depending on the settings)
• Participate to a Forum
• Participate to a Live Chat
• Communicate through messages.
Security in e-learning environments usually follows
the Role-Based control model (RBAC), where there are
user to role and role to role relationships or, in some
cases, the Access Matrix Model19. In this front, continu-
ous research efforts are devoted to the social aspects of
security, the importance of identity20 or the provision
of new security and privacy frameworks and architec-
tures21,22.
Taking the above into account, one may be lost in
seeking for appropriate software tools that fulill the

17HIPPOKRATIA 2008, 12 (Suppl 1)
stringent educational requirements. The existence of
open source software environments like “Moodle”23, that
provide simultaneous use of synchronous and asynchro-
nous communications tools and SCORM compliance in
a reliable e-learning setting, meeting the needs of online
medical education, is not only a nice coincidence, but a
real opportunity to exploit24. Moodle is utilised by a large
community of users and supports numerous languages; it
has more than 38,500 registered sites.
E-learning Standards
The existence of educational material in one LMS
does not necessarily imply, that it is easily transferable
to other LMSs, due to compatibility, as well as, lack
of teaching attribute information. Teachers may cre-
ate their educational material according to the require-
ments of the LMS to be used for uploading their mate-
rial. To this extend the absence of common approaches
for creation, description and distribution of learning
objects creates compact borders for their eficient and effective use.
It was for this reason that Advanced Distributed
Learning (ADL), a U.S. Government initiative, devel-
oped SCORM18, enabling the production of learning ma-
terial fulilling requirements such as Interoperability, Ac-
cessibility, Reusability, Durability, Maintainability and
Adaptability; in this way, the learning material remains
credible, up-to-date and follows changes and develop-
ments of medical techniques and standards through time.
In the published SCORM book, ADL described the
Content Aggregation Model25, where it is depicted how
a SCORM object is divided into many Sharable Content
Objects (SCOs); furthermore, each SCO consists of ei-
ther one or many Assets. Asset is the basic building block
of a learning resource; the latter may be composed by
all those iles and different formats containing text, im-
ages, sound, animation, video that can be viewed through
a web browser.
Moreover, all Assets and SCOs are described in the
Manifest ile, an XML (eXtensible Markup Language) ile, named imsmanifest.xml along with the fundamental iles format. This special ile describes also the content structure and, therefore, it must exist in the root of the
content package (a package usually in ZIP format that
contains all the physical iles).One or more SCOs can be considered as a Learning
Object (LO); each learning object can be associated with
one or many educational objectives. A course composed
of one or many LOs and may also be given an overall
educational objective. A complete course composed of
many LOs with high cohesion and where the content is
integrated, may not easily be reusable. On the other hand
assets are reusable, but they do not provide a structured
content. SCORM offers the ability to have a coherent
course and at the same time to have access to the indi-
vidual assets. In this respect, reusability is maintained at a
higher level within a SCORM conformant and compliant
course (Figure 2).
Figure 2: Reusability vs Coherence.
SCORM and Web 2.0 tools
Over the last few years the emergence of Web 2.0
tools, namely wikis, blogs, podcasts and vodcasts, have
changed the way internet is used. Their application in
education was inevitable and is incrementally exploited
in various contexts of Medical Education26,27.
Such new educational tools may also be included in
SCORM either as a stand alone asset or within a SCO,
but always described by appropriate metadata (see Fig-
ure 3).
Figure 1: E-learning Environment Actions.

18 BAMIDIS PD
Figure 3: Web 2.0 tools in SCORM.
Learning Object Metadata
According to Wikipedia28 metadata are data about
data. An item of metadata may describe an individual
datum, or content item, or a collection of data includ-
ing multiple content items. Furthermore, in e-learning,
metadata can be used to discover resources, to organize
electronic resources, to facilitate interoperability, to pro-
vide digital identiication and to support archiving and preservation.
SCORM uses the IEEE Learning Object Metadata
(LOM)29 deinitions in order to achieve a description of the content package as a whole, but also contain metadata
about:
• Content Aggregation
• Content Organization
• Activities
• SCOs and
• Assets
Special demands and needs in medical education drove
the foundation of the MedBiquitous Consortium through
which SCORM for Healthcare is developed30. The major
(and only) difference from the “simple” SCORM is in the
metadata. That is, SCORM for Healthcare uses Health-
care Learning Objects Metadata(LOM)31, which extended
IEEE LOM with one more category, namely, “Healthcare
Metadata”, where “health-oriented” information, as well
as, information speciic to a medical course is described (e.g. CME credits).
Creation of SCORM course
A course compliant and conformant with SCORM
could be created either from scratch, creating the inde-
pendent html pages with the necessary scripts, the ims-
manifest.xml and the appropriate java scripts for the
communication with the E-learning platforms, or by the
use of a SCORM editor.
There exist both open source and proprietary SCORM
editors. One of the most known ones, that supports
Greek Language too, is eXe, the eLearning XHTML edi-
tor32. Furthermore, eXe is an authoring application that
assists teachers and academics in the publishing of web
content without their needing to become proicient in HTML or XML markup. It is primarily written in the
Python programming language and is based upon the
open source web browser Firefox; it has been developed
around formal elements, called instructional devices or
iDevices. These instructional devices include a range of
pedagogical forms e.g. objectives, advance organizers,
and learning activities which constitute the equivalent of
the ‘teacher talk’ in content resources designed for on-
line learning32.
The course creator (usually the teacher), creates by
the use of this SCORM editor the SCORM package, usu-
ally in a ZIP format. This Content Package contains all
the necessary iles, so as for the online course to be fully working. The only action that should be taken in order to
run the course in the e-learning environment is to upload
this Content Package into the environment. The content
package is then unzipped into its directory and it is ready
for use.
To this extend the users, learners and teachers, can use
the web 2.0 tools and the synchronous and asynchronous
modules that are provided by the e-learning environment.
All users are connected to the e-learning environment
through an appropriate interface provided via the internet
(Figure 4).
Figure 4: Overall creation of SCORM course.
Metadata Creation
The metadata decided to be used for the purposes of
this piece of work were those deined in the Healthcare Learning Object Metadata as proposed by the MedBiq-
uitous Consortium30, and following the http://ltsc.ieee.
org/xsd/LOM healthcarelom.xsd XML Schema Deini-tion.
Figures 5, 6 and 7 illustrate some of the categories
can be observed as an example. Figure 5 depicts the gen-
eral category containing the title, the course description,
the keywords, etc.

19HIPPOKRATIA 2008, 12 (Suppl 1)
Figure 5: Healthcare LOM – general category.
Figure 6 shows the educational category that groups
the educational and pedagogic characteristics of the
learning object; the way the course should be delivered
and the different kinds of features/items (modules) that
the course is composed of.
Last but not least, the classiication category among others contains all the educational objectives of the
course. It is very important that the description of educa-
tional objectives accompany the learning material itself.
(Figure 7).
Figure 7: Healthcare LOM – classiication category
Course Content Background
As already mentioned above, this piece of work ne-
cessitated the collaboration of researchers from the Labo-
ratory of Medical Informatics of AUTh and the qualiied specialists of the Greek Aerospace Medical Association
and Space Research , as well as, other professionals from
bodies such as the Hellenic Civil Aviation Authority and
the Aeromedical Center “IASI”. The common efforts of
these were essential in building up the quality standards,
and a structure for Professional Development Series of
seminars.
The irst course developed for this purpose, name-
ly, “pulmonary disorders in aerospace medicine”, is
presented below. The content of the course deals with
topics such as asthma, sarcoidosis, pneumothorax, trau-
matic pneumothorax, Chronic Airway Obstruction, pul-
monary blisters and lung bleds, pulmonary tuberculo-
sis, atypical mycobacterioum diseases, Interstitial Lung
Diseases, bronchiectasis, Lung Neoplasias and Malig-
nancies, lung thromboembolism disease, and obstruc-
tive sleep apnea.
Technically speaking, the modules used by the e-
learning environment are: text, slides, video, forums,
wikis; last but not least, multiple choice questions were
used for the assessing the learning outcomes on the learn-
ers’ side.
The educational goals of this course of the CME
activity were:
1. Update and improve the clinical skills of Pri-
mary Care Practitioners in Pulmonary Medicine. This Figure 6: Healthcare LOM – educational category.
20 BAMIDIS PD
stemmed from the fact that new treatments for Asthma,
chronic obstructive pulmonary disorders, deep venous
thrombosis, Sleep Disorders and Critical Care Medi-
cine are rapidly developing and become available. This
CME activity addresses these needs and satisies the need to improve the abilities of practitioners to diag-
nose, treat and properly refer necessary pulmonary
conditions.
2. Understand and evaluate the conditions under
which a pilot or a traveler with chronic or acute pul-
monary disease may fly, as well as, the precautions
they should take before their exposure to high alti-
tudes.
3. Comprehend the restrictions under which an ap-
plicant may become it to ly.
At the end of this course in pulmonary medicine, at-
tendants will have the knowledge to understand which
pulmonary disease is related to aviator’s health and per-
formance, measures to prevent derangements during
light and where to address in case a related problem oc-
curs.
Figure 8: The entry to the e-learning Environment.
Figure 9: A “Presentation module” of the SCORM compli-
ant and conformant e-learning environment.
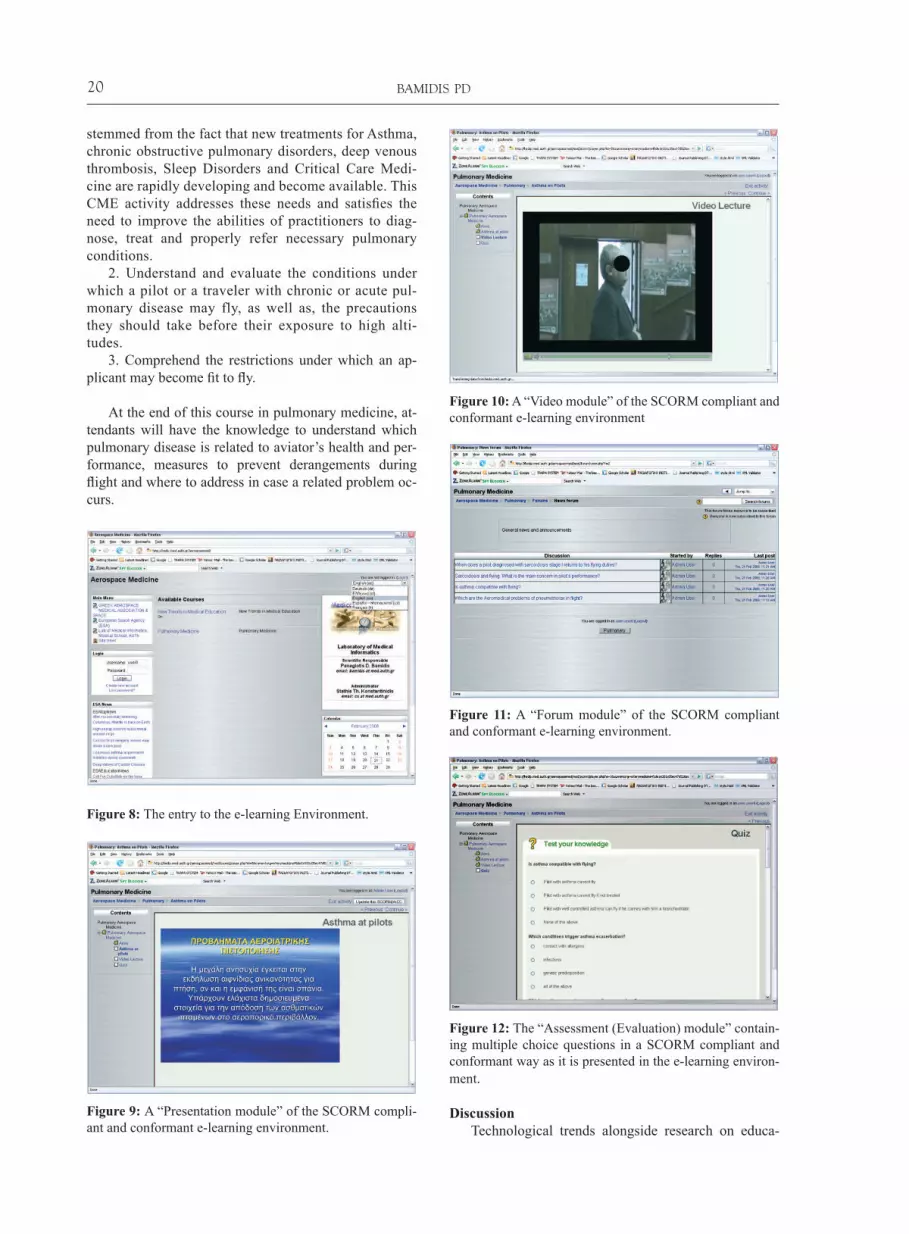
Figure 10: A “Video module” of the SCORM compliant and
conformant e-learning environment
Figure 11: A “Forum module” of the SCORM compliant
and conformant e-learning environment.
Figure 12: The “Assessment (Evaluation) module” contain-
ing multiple choice questions in a SCORM compliant and
conformant way as it is presented in the e-learning environ-
ment.
Discussion
Technological trends alongside research on educa-

21HIPPOKRATIA 2008, 12 (Suppl 1)
tional and teaching strategies appear as key issues for
the advancement of continuing medical education34,35.
This paper outlined some of the efforts undertaken in
order to provide contemporary medical aviation topics
in e-learning forms by the use of the international stan-
dard SCORM. Such an approach facilitates the future
exchange of this highly specialized educational material
among the limited, anyway, specialist educators.
The paper illustrated the elements composing the
open source e-learning environment, MOODLE, which
accommodated the medical aviation course on pulmo-
nary disorders. The approach was lead by the notion of
creating the necessary procedures that can act as a guide-
line and pattern for future course developments.
To this extent, continuing medical education is fa-
cilitated with all those tools and standards required so
as to allow not only the electronic provision of CME
but its sharing among educators as well. Physicians and
general practitioners could use this e-learning environ-
ment to extend their medical knowledge and update
their professional level in terms of aerospace medicine.
Accordingly, specialised educators of aerospace and
aviation medicine may exploit the availability of this
environment in order to share highly specialized educa-
tional material31,36.
The impact of such an environment to the aerospace
medicine community, the health professional associa-
tions, as well as, society on the whole will become obvi-
ous in future years and after meticulous evaluations. In
this respect, this paper has not touched upon any of these
important issues, as its focus was on providing the neces-
sary procedures for enabling such an e-learning course
infrastructure, rather evaluating it. Evidently though, any
such effort must adhere to certain quality criteria in order
to become acceptable and to this end, the paper has dem-
onstrated the use of a standardized process that facilitates
this quality. In addition, national accreditation authorities
have deined a framework concerning such educational activities, and medical associations are proposing poli-
cies in order to promote CME through the Internet or oth-
er spatial and temporal distance technologies. In conclud-
ing, it has to be mentioned that our plan is to create and
evaluate the e-learning educational procedure through an
accreditation framework proposed by Bamidis et al17.
Acknowledgement
This work has been beneited from an INTERREG IIIA Greece - Bulgaria (Decision 300531/YD4388
01/11/2005; CrossBorderHealth project), and an IN-
TERREG IIIA/ARCHIMED grand (Contract Number
A.1.087; IntraMEDnet project) by the European Union
and the Greek Government.
References1. Duplaga M, Juszkiewicz K, Kwolek B, et al. Enhancing Medical
Education through Telelearning. In: Zieliński K, Duplaga M, Ingram D (eds). Information Technology Solutions for Health-
care. Springer, London 2006; pp 302-327
2. Childs S, Blenkinsopp E, Hall A, Walton G. Effective e-learning
for health professionals and students—barriers and their solu-
tions. A systematic review of the literature-indings from the HeXL project. Health Info Libr J 2005; 2: 20-32
3. Cook DA, McDonald FS. E-Learning is there anything special
about the “e”? Persp Biol Med 2008; 51: 5-21
4. Olson CA, Shershneva MB. Setting quality standards for web-
based continuing medical education. J Contin Educ Health Prof
2004; 24: 100-111
5. Konstantinidis ST, Nikolaidou MM, Bamidis PD, Pappas C.
Distance Continuing Medical Education in cross border areas
of Greece and Bulgaria – The CrossBorderHealth project ex-
ample. Proceedings of the 4th International Conference in Open
and Distance Learning - ICODL 2007, Athens, Greece, 2007,
B: 73-79
6. Marolov SS, Konstantinidis ST, Bamidis P D, Nikolaidou M,
Pappas C. Cross-Border Collaboration Between Greece And
Bulgaria: The Use Of ICT In Improving Social Medicine Edu-
cation. Proceedings of the 3rd Balkan Conference in Informatics
BCI’2007, Soia, Bulgaria, 2007, 2: 281-2907. Sten L, Annita F. New tools in Social Practice: Learning, Medi-
cal Education and 3D Environments. Outlines 2001; 2: 5-23
8. Lu J, Pan Z, Lin H, et al. Virtual learning environment for medi-
cal education based on VRML and VTK. Computers & Graph-
ics 2005; 29: 283-288
9. Heinrichs W, Youngblood P, Harter P, et al. Simulation for
Team Training and Assessment: Case Studies of Online Train-
ing with Virtual Worlds. World Journal of Surgery 2008; 32:
161-170
10. Yellowlees PM, Cook JN. Education about hallucinations using
an internet virtual reality system: a qualitative survey. Acad Psy-
chiatry 2006; 30: 543-549
11. Wilson AS, Goodall JE, Ambrosini G, et al. Development of an
interactive learning tool for teaching rheumatology-a simulated
clinical case studies program. Rheumatology 2006; 9: 1158-
1161
12. Yee N, Bailenson JN, Urbanek M, et al. The unbearable like-
ness of being digital: the persistence of nonverbal social norms
in online virtual environments. Cyberpsychol Behav 2007; 10:
115-121
13. Fried MP, Uribe JI, Sadoughi B. The role of virtual reality in
surgical training in otorhinolaryngology. Curr Opin Otolaryngol
Head Neck Surg 2007; 15: 163-169
14. Miau JJ, Wu J, Chiu HH, et al. Promoting University-Industry
and International Collaborations in Aerospace Engineering Edu-
cation in Taiwan. Proceedings of the ICEE 2001, Oslo/Bergen,
Norway, 2001
15. Institute of Aerospace Medicine, RWTH Aachen University,
Germany Telemedicine for the mobile society: First results of the
TEMOS. www.t-online.de
16. Shirley A. E-learning developments and experiences. Education
and Training 2001; 43: 240-248
17. Bamidis PD, Nikolaidou MM, Konstantinidis ST, et al. A Pro-
posed Framework for Accreditation of Online Continuing Medi-
cal Education. Proceedings of the Twentieth IEEE International
Symposium on Computer-Based Medical Systems - CBMS ‘07,
2007, pp 693-700
18. SCORM 2004 3rd Edition Overview Version 1.0, 2006, Ad-
vanced Distributed Learning(ADL), www.adl.org
19. Sandhu R, Samarati P. Access control: Principles and practice.
IEEE Communications 1994; 32: 40–48
20. Raitman R, Ngo L, Augar N, et al. Security in the online e-learn-
ing environment. Proceedings of the ifth IEEE International Conference on Advanced Learning Technologies – ICALT, 2005
21. Franz E, Wahrig H, Boettcher A, et al. Access control in a pri-
vacy-aware eLearning environment. Proceedings of the First In-
ternational Conference on Availability, Reliability and Security
–ARES, 2006
22. Lin NH, Korba L, Yee G, et al. Security and privacy technolo-
gies for distance education applications. Proceedings of the 18th

22 BAMIDIS PD
International Conference on Advanced Information Networking
and Applications – AINA, 2004
23. Moodle: Modular Object-Oriented Dynamic Learning Environ-
ment. www.moodle.org
24. Antoniou P, Papaioakeim M, Kaldoudi E, et al. Deliverable 1.1:
Critical Review of Current State in E-Learning Technologies
and Applications. IntraMEDnet: A Mediterranean Research and
Higher Education Intranet in Medical and Biological Sciences,
http://www2.cs.ucy.ac.cy/intramednet
25. Content Aggregation Model 1.0, SCORM 2004 3rd Edition,
2006. Advanced Distributed Learning (ADL). 2006, last visited
10/1/2008
26. Boulos MNK, Maramba I, Wheeler S. Wikis, blogs and pod-
casts: a new generation of Web-based tools for virtual collab-
orative clinical practice and education. BMC Medical Education
2006; 6: 41
27. Boulos MNK, Wheeler S. The emerging Web 2.0 social soft-
ware: an enabling suite of sociable technologies in health and
health care education. Health Inform Libr J 2007; 24: 2–23
28. Metadata in Wikipedia, http://en.wikipedia.org/wiki/Metadata
29. Draft Standard for Learning Object Metadata. Learning
Technology Standards Committee of the IEEE, 2002, http://
ltsc.ieee.org/wg12/files/LOM_1484_12_1_v1_Final_Draft.
pdf, last visited 10/02/2008
30. Smothers V. Healthcare Learning Object Metadata Speciica-
tions and Description Document,v0.9. MedBiquitous Consortium
2007, http://www.medbiq.org/working_groups/learning_objects/
HealthcareLOMSpeciication.pdf
31. Smoothers V, Greene P, Ellaway R, Detmer DE. Sharing inno-
vation: the case for technology standards in health professions
education. Medical Teacher 2008; 30: 150-154
32. eXe: eLearning XHTML editor, in http://www.exelearning.org/
33. Greek Aerospace Medical Association and Space Research.
www.gasma.gr
34. Radon K, Kolb S, Reichert J, et al. Case-based e-learning in
occupational medicine-The NetWoRM Project in Germany. Ann
Agric Environ Med 2006; 13: 93-98
35. Vollmar1 HC, Schόrer-Maly CC, Frahne J, Lelgemann M, Butzlaff M. An E-learning Platform for Guideline Implemen-
tation – Evidence- and Case-based Knowledge Translation via
the Internet. Methods of Information in Medicine 2006; 45:
389-396
36. Kaldoudi E, Papaioakeim M, Bamidis PD, Vargemezis V. To-
wards expert content sharing in medical education. Proceedings
of the International Technology Education and Development
Conference, INTED 2008, In press