aka: ald, “lorenzo's oil disease”, amn - hunter's hope
TRANSCRIPT
Adrenoleukodystrophy:AKA: ALD, “Lorenzo’s Oil Disease”, AMN
2020 Winter MeetingMarch 3, 2020
SpeakersSpeakers
Family Presenters: Robert Rauner, President of United Leukodystrophy Foundation
Clinical Coordinator Presenters: Catherine Becker, NP MGH Kim Hollandsworth BSN, RN, CPN, Kennedy Krieger
} Adreno-pertaining to the adrenal gland
} Leuko- comes from Greek word meaning “white”
} Dystrophy-condition of abnormal development or degeneration
} ALD- generally refers to the childhood form of the disease
} AMN- adult on-set of symptoms involving the spinal cord
What’s in a name? FdafaffdadsagsdAdrenoleukodystrophy
ALD
• “X-linked ALD is a genetically determined disorder that mainly affects the nervous system, white matter, adrenal cortex, and testis. The principle biochemical abnormality is the accumulation in tissues and body fluids of saturated unbranched Very Long Chain Fatty Acids, VLCFA, due to mutations in the peroxisomal fatty acid transport.” ABCD1, is located on the terminal end of the X-chromosome
Genetics of ALD
• Occurs one in 13,500 births
• Most commonly inherited Leukodystrophy
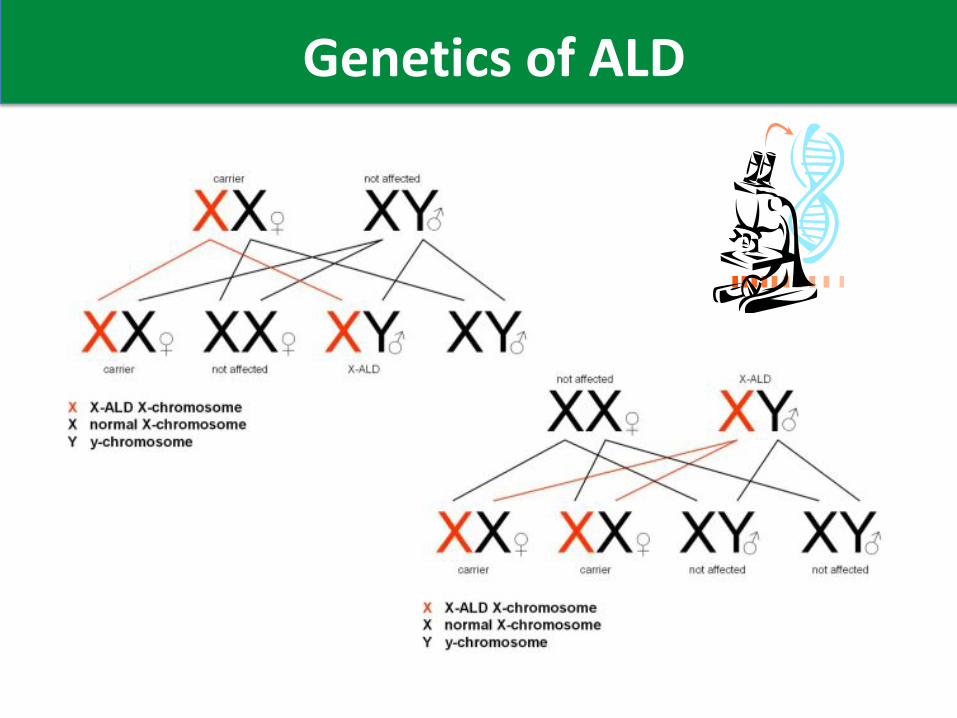
• ALD is passed on the X chromosome
• Women carriers have a 50% affected child
• Risk does not decrease with subsequent pregnancies
• CVS and Amniocentesis can be done prenatally at ~12-16 weeks
• PGD with invitro is available to ensure child without ALD gene
• Genetic counseling is strongly encouraged
Genetics of ALD
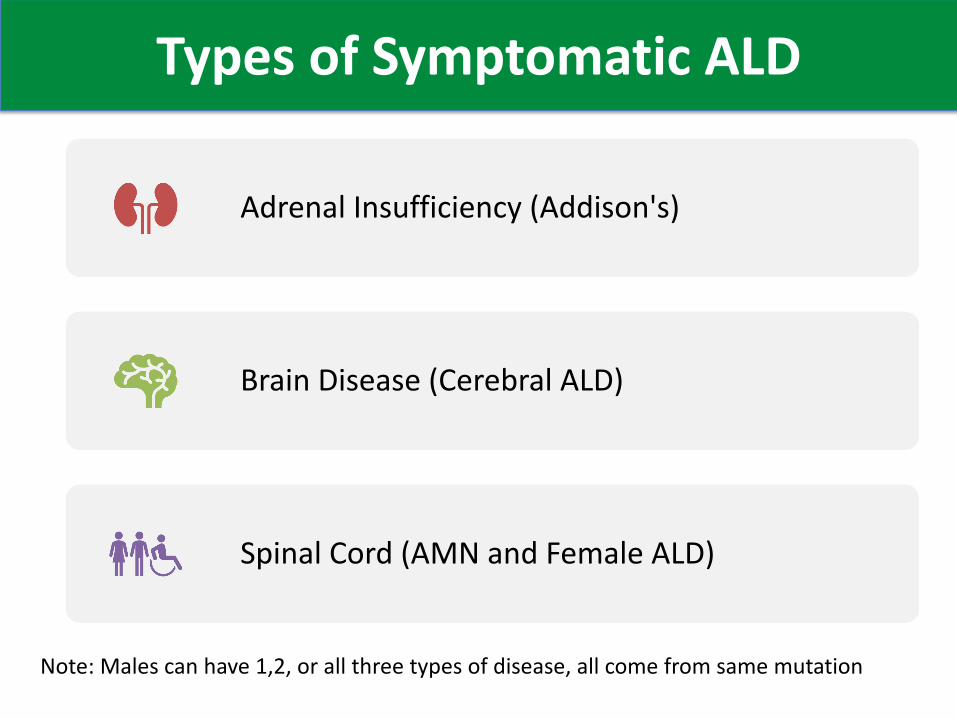
Types of Symptomatic ALD
Adrenal Insufficiency (Addison's)
Brain Disease (Cerebral ALD)
Spinal Cord (AMN and Female ALD)
Note: Males can have 1,2, or all three types of disease, all come from same mutation
• Dried blood spot test for C26:0-LPC , a VLCFA phospholipid done by LCMSMS
• Dried blood spot test done by LCMSMS is 100% for males and 97% for females
• As of February 2020, 16 states and DC screen for ALD, representing about 50% of births in the USA
Newborn Screeningfor ALD
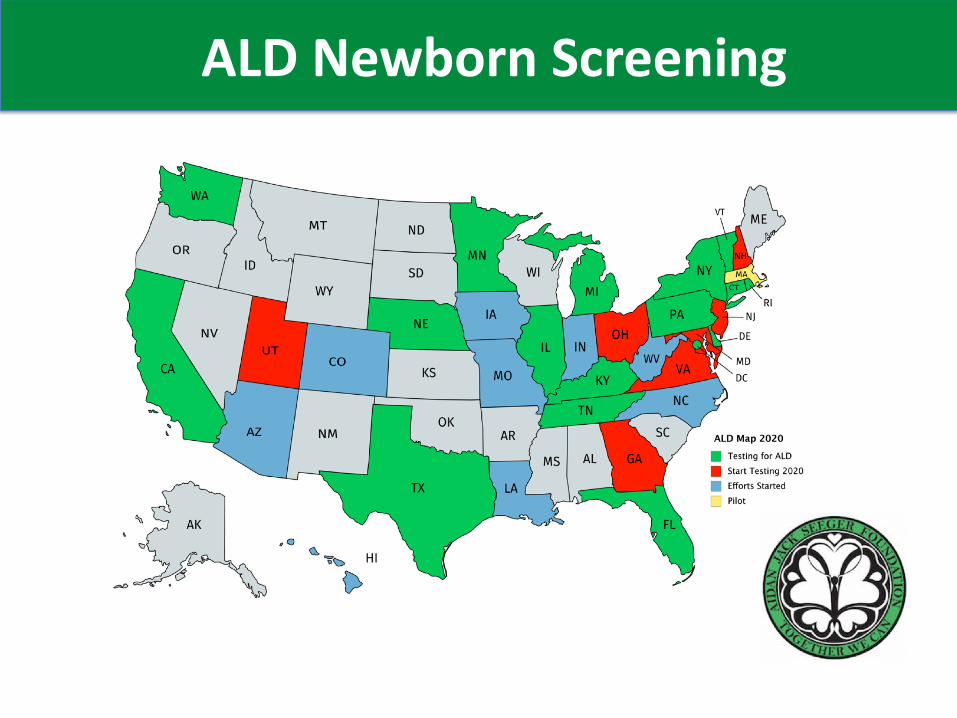
ALD Newborn Screening
Female ALDAt least 80% of women are also symptomatic:
- Female ALD has been under studied and under recognized- Likely is different then Male AMN- In some families women are more severely affected by AMN- No drug trials to date in female ALDHuffnagel, et.al., Disease progression in women with X-linked adrenoleukodystrophy is slow, Orphanet Journal of Rare disease, 2019
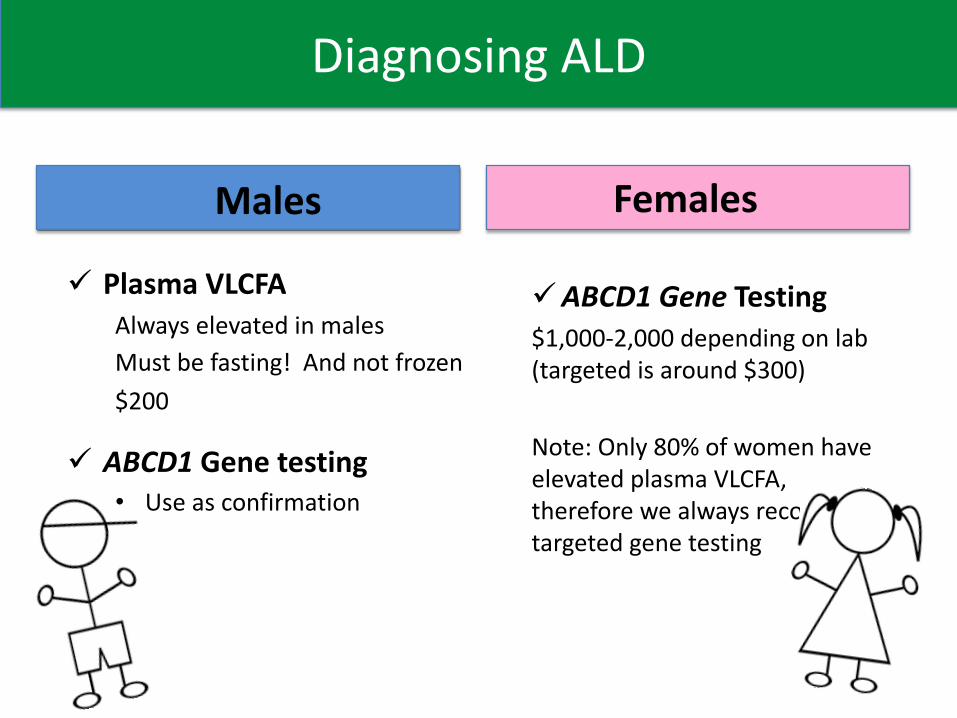
Diagnosing ALD
Males
ü Plasma VLCFAAlways elevated in malesMust be fasting! And not frozen$200
ü ABCD1 Gene testing • Use as confirmation
Females
üABCD1 Gene Testing$1,000-2,000 depending on lab (targeted is around $300)
Note: Only 80% of women have elevated plasma VLCFA, therefore we always recommend targeted gene testing
ABCD1 Gene
Over 1100 mutations have been identified in ABCD1 gene
No Genotype Phenotype correlation v Identical twins can present with different phenotypes
Adrenoleukodystrophy.info v Website listing every mutation reported in the ABCD1 genev Run by Stephan Kemp PhD
Faces of Cerebral ALD
Krabbe Disease affects both the central and peripheral nervous systems, which are responsible for all of the body’s voluntary and involuntary functions.
More…
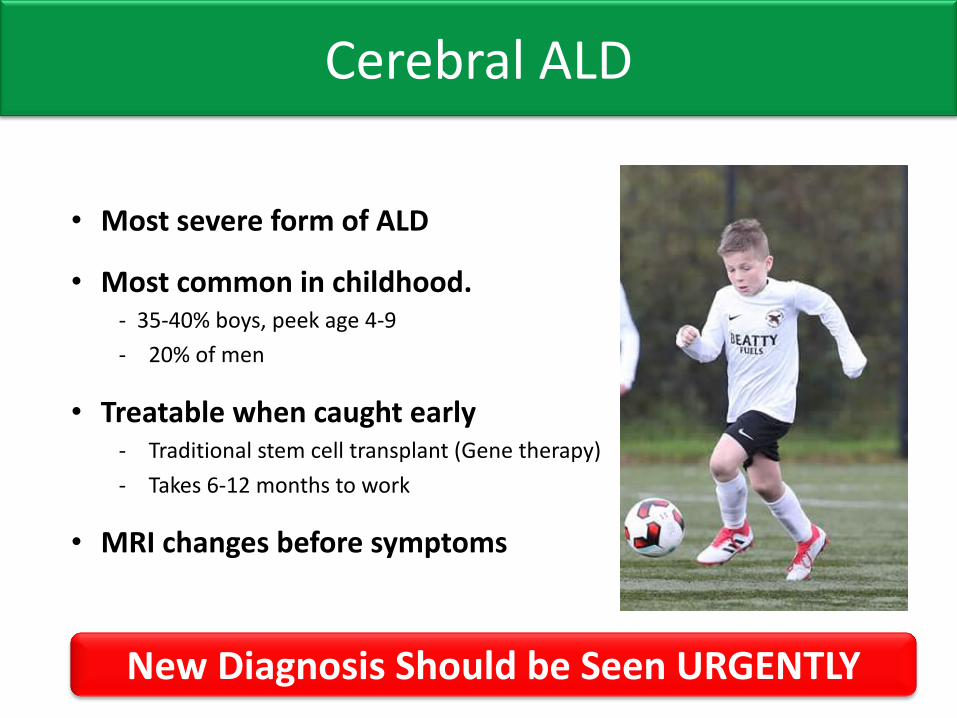
Cerebral ALD
• Most severe form of ALD
• Most common in childhood. - 35-40% boys, peek age 4-9
- 20% of men
• Treatable when caught early- Traditional stem cell transplant (Gene therapy)
- Takes 6-12 months to work
• MRI changes before symptoms
New Diagnosis Should be Seen URGENTLY
15
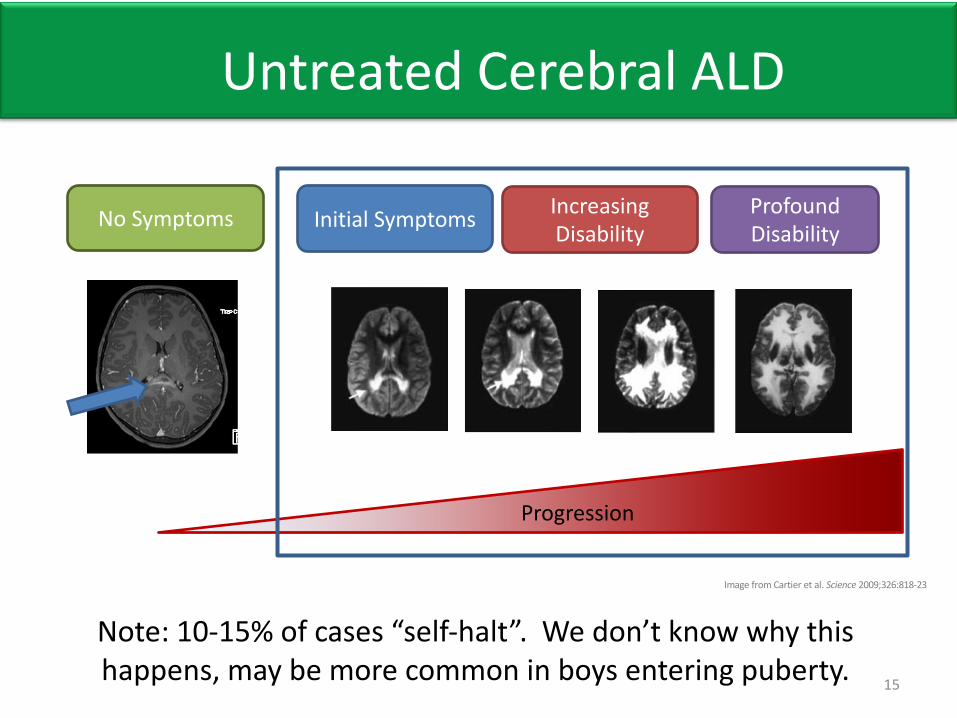
Progression
Initial Symptoms Increasing Disability
Profound Disability
Image from Cartier et al. Science 2009;326:818-23
No Symptoms
Untreated Cerebral ALD
Note: 10-15% of cases “self-halt”. We don’t know why this happens, may be more common in boys entering puberty.
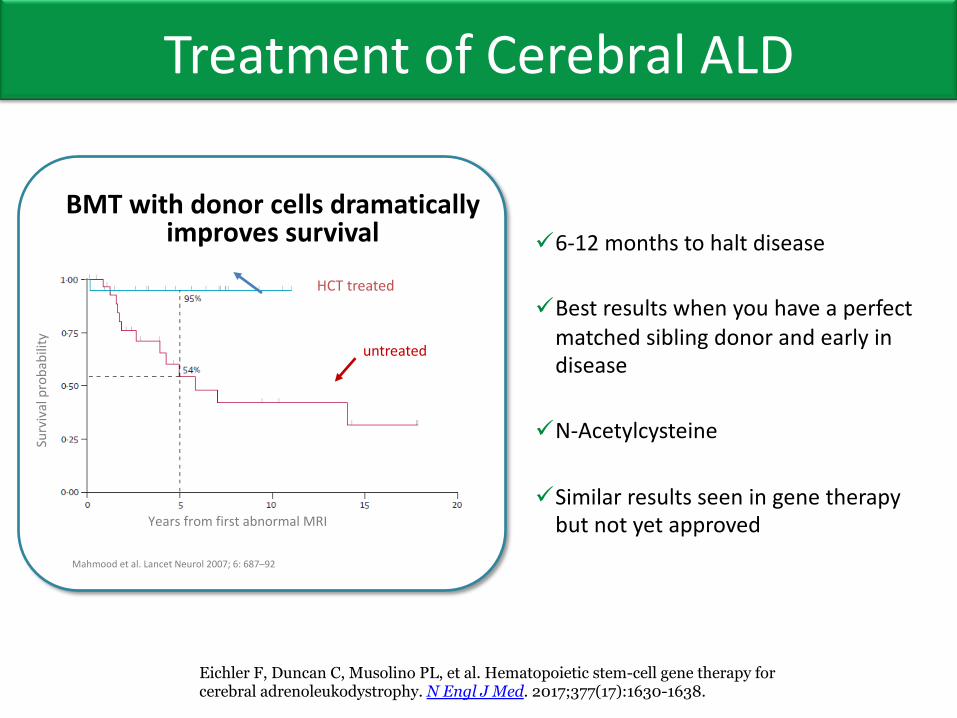
Treatment of Cerebral ALD
BMT with donor cells dramatically improves survival
untreated
HCT treated
Surv
ival
pro
babi
lity
Years from first abnormal MRI
Mahmood et al. Lancet Neurol 2007; 6: 687–92
ü6-12 months to halt disease
üBest results when you have a perfect matched sibling donor and early in disease
üN-Acetylcysteine
üSimilar results seen in gene therapy but not yet approved
Eichler F, Duncan C, Musolino PL, et al. Hematopoietic stem-cell gene therapy for cerebral adrenoleukodystrophy. N Engl J Med. 2017;377(17):1630-1638.
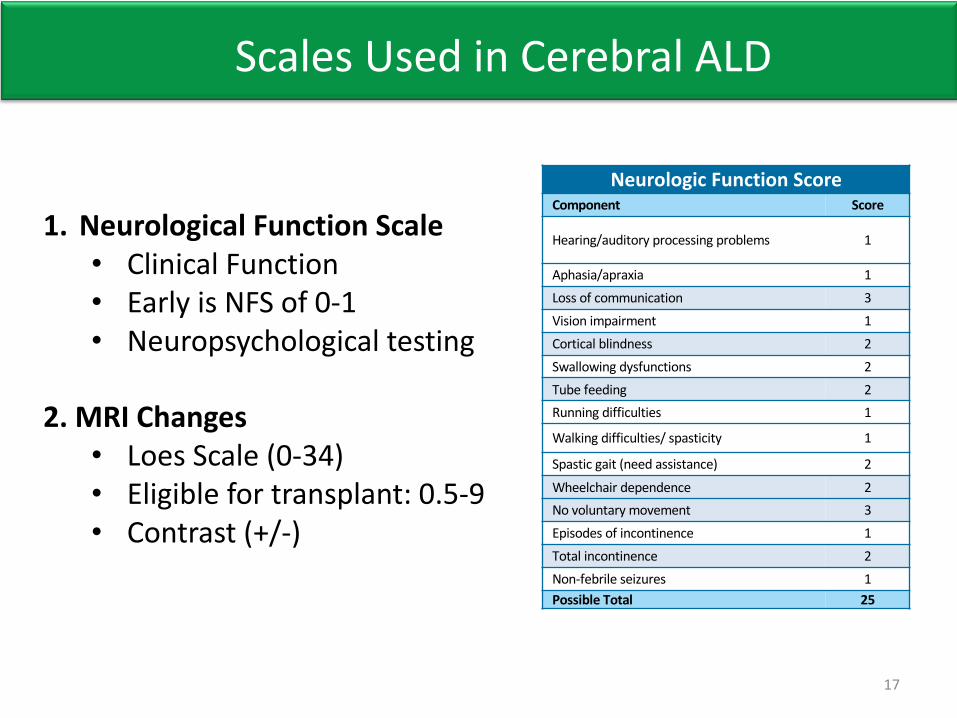
Scales Used in Cerebral ALD
17
ADHD = attention deficit hyperactivity disorder
1. Neurological Function Scale• Clinical Function
• Early is NFS of 0-1
• Neuropsychological testing
2. MRI Changes• Loes Scale (0-34)
• Eligible for transplant: 0.5-9
• Contrast (+/-)
Neurologic Function ScoreComponent Score
Hearing/auditory processing problems 1
Aphasia/apraxia 1
Loss of communication 3
Vision impairment 1
Cortical blindness 2
Swallowing dysfunctions 2
Tube feeding 2
Running difficulties 1
Walking difficulties/ spasticity 1
Spastic gait (need assistance) 2
Wheelchair dependence 2
No voluntary movement 3
Episodes of incontinence 1
Total incontinence 2
Non-febrile seizures 1
Possible Total 25
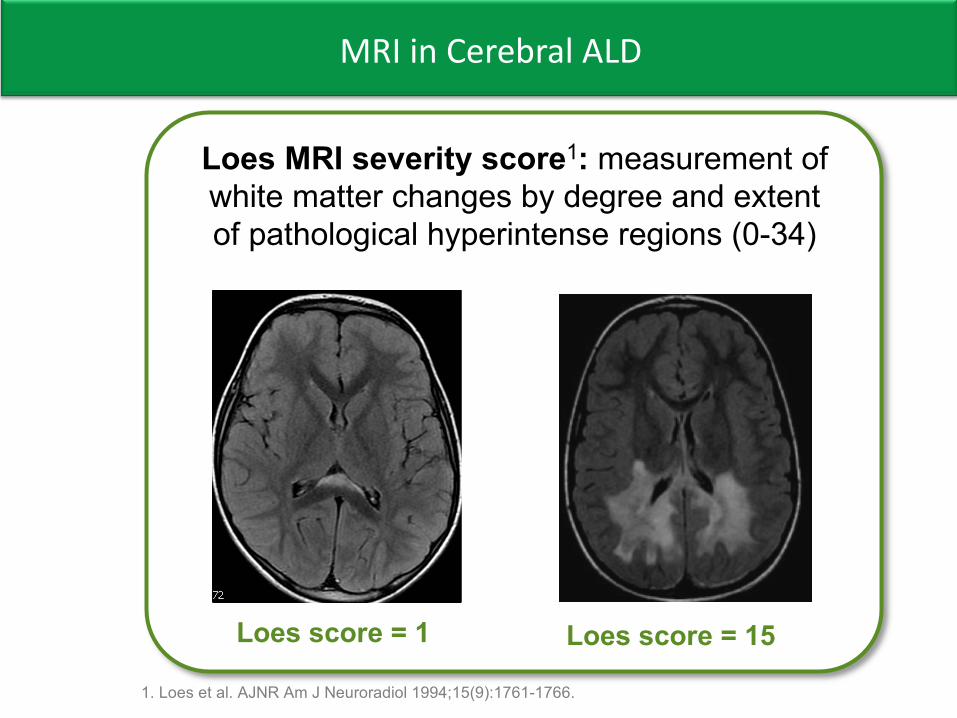
MRI in Cerebral ALD
Gadolinium*enhancement:indicator)of)active)inflammation)in)
untreated)patients)(+/5)
Loes*score*=*1 Loes*score*=*15
Loes*MRI*severity*score1:*measurement)of)white)matter)changes)by)degree)and)extent)of)pathological)hyperintense regions)(0534)
GdE+
1.)Loes)et)al.)AJNR)Am)J)Neuroradiol)1994H15(9):176151766.
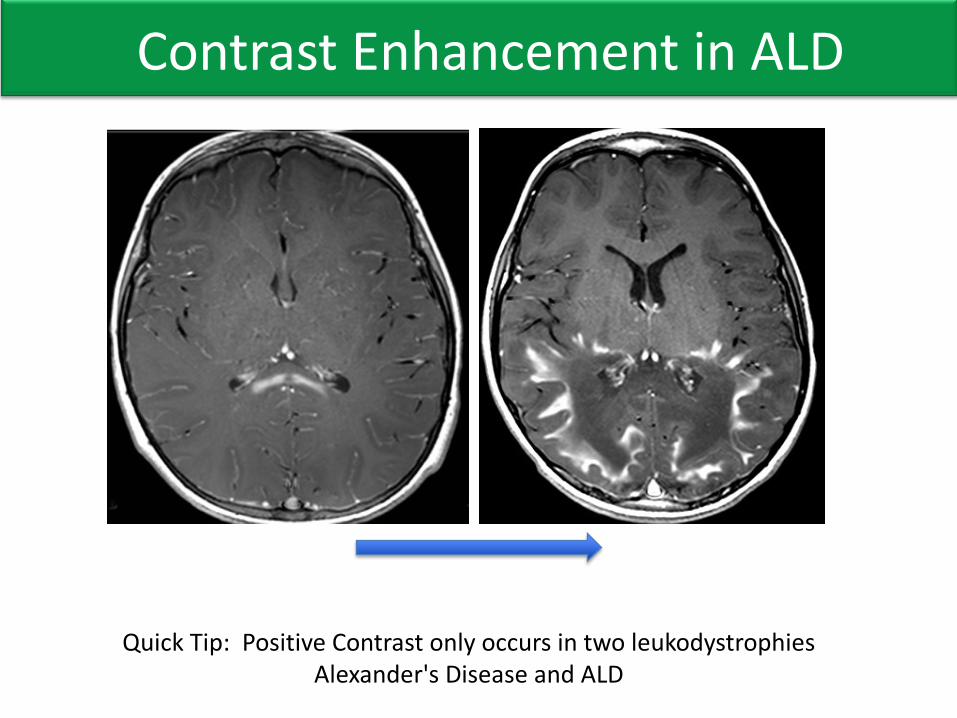
Contrast Enhancement in ALD
Quick Tip: Positive Contrast only occurs in two leukodystrophiesAlexander's Disease and ALD
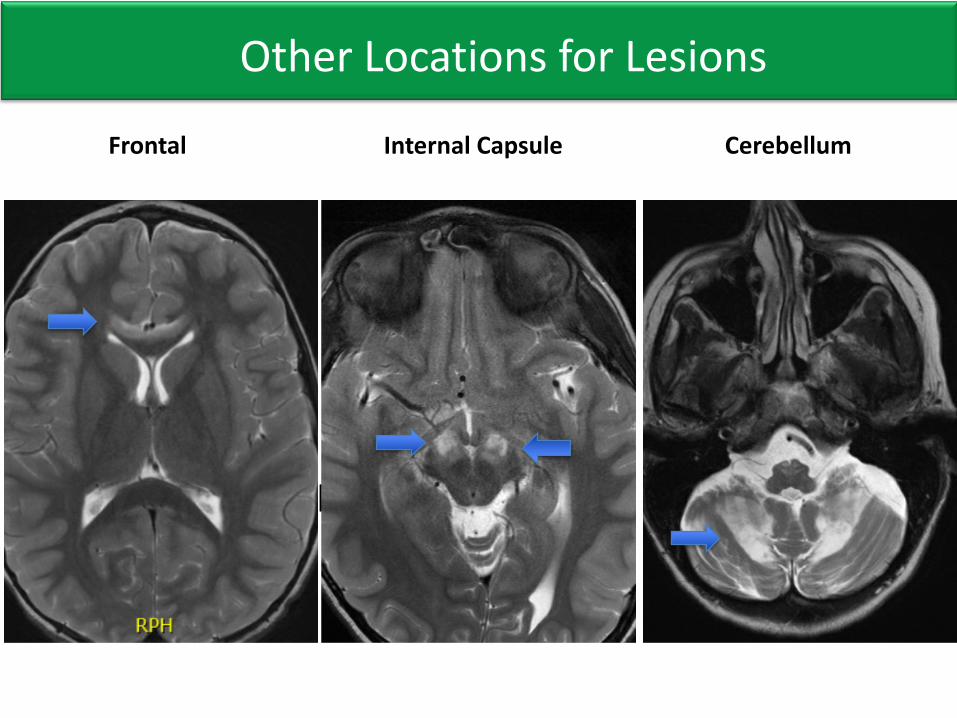
Other Cerebral Lesion
Frontal Internal Capsule Cerebellum
Other Locations for Lesions
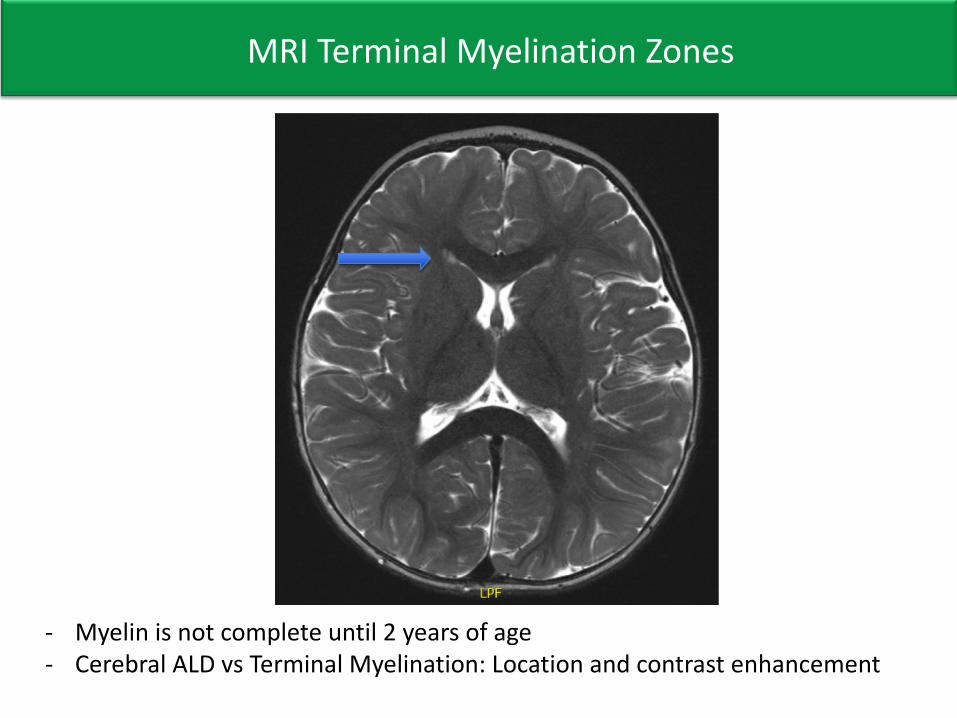
MRI Terminal Myelination Zones
- Myelin is not complete until 2 years of age- Cerebral ALD vs Terminal Myelination: Location and contrast enhancement
High Risk Cerebral ALD
22
ADHD = attention deficit hyperactivity disorder
High risk if any of the following:
ü Clinically symptomatic
ü Non-febrile seizure
ü MRI Loes Score >9
ü Incontinence (risk of urosepsis)
Treatment Options:
ü N-Acetylcysteine and move fast once decision made
ü Counsel on added risks of treatment
ü ? Seizure prevention (no data to support)
While there are many devastating stories of ALD, there are also stories of hope…..18 months post high risk transplant
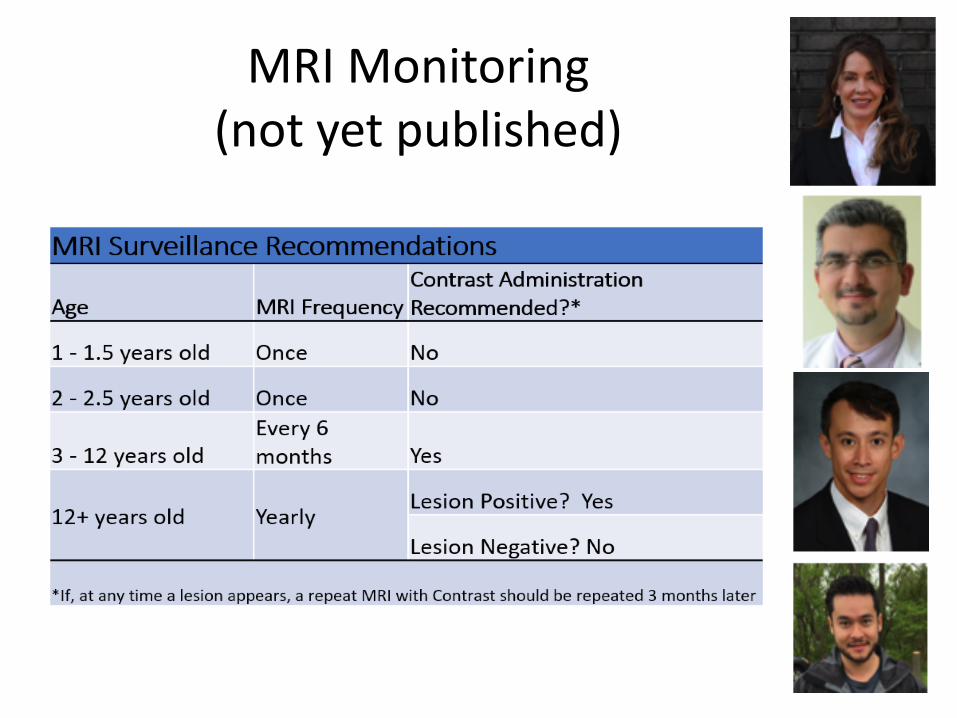
MRI Monitoring (not yet published)
NBS Follow-up Protocols for Krabbe?
Explain…
Adrenal Insufficiency
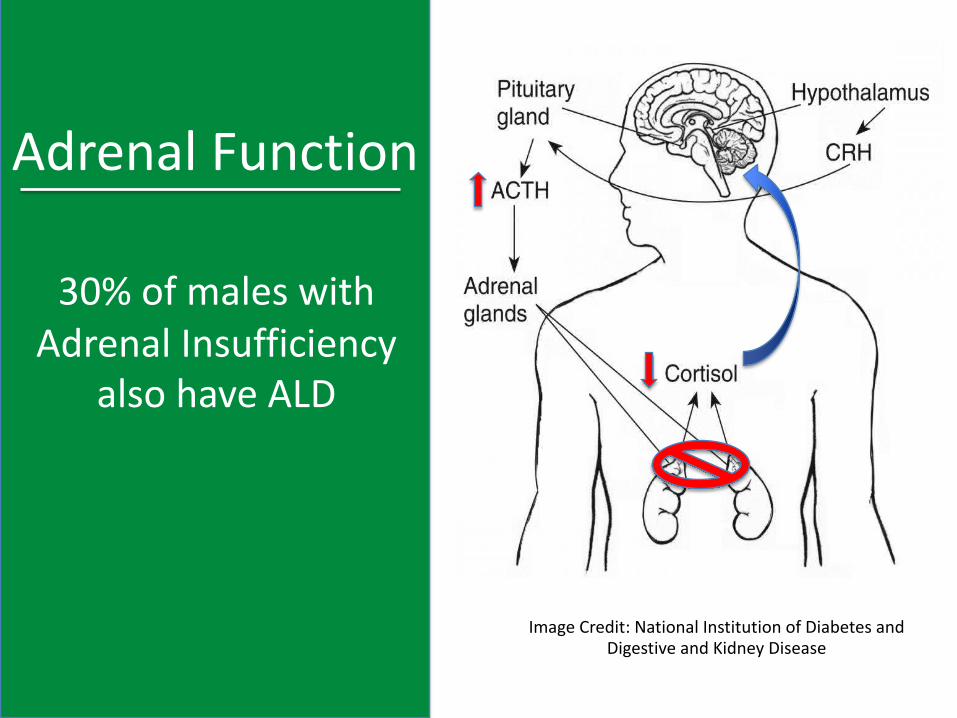
Adrenal Function
Image Credit: National Institution of Diabetes and Digestive and Kidney Disease
30% of males with Adrenal Insufficiency
also have ALD
Adrenal Insufficiency
• 80% risk over lifetime
• Usually starts in first decade of life- 47% developed between 0-10 years- 28% developed between age 10 and 40- 5% developed after age 40Huffnagel, et.al., The Natural History of Adrenal Insufficiency in X-Linked Adrenoleukodystrophy: and International Collaboration, J Clin Endocrin Metab, January 2019
• Very treatable with oral medication
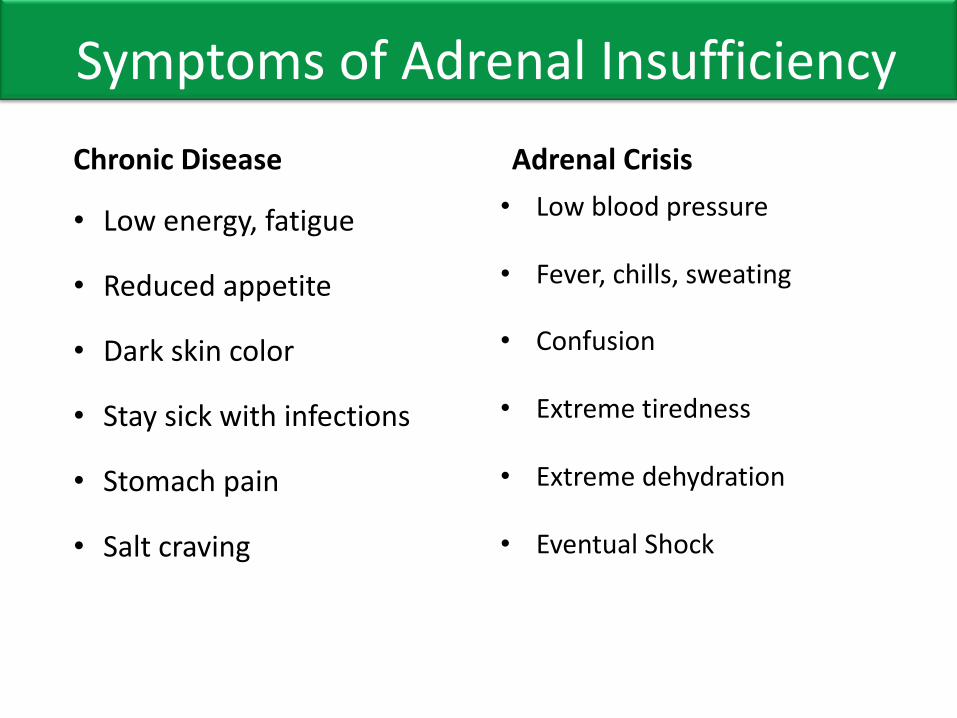
Symptoms of Adrenal Insufficiency Chronic Disease
• Low energy, fatigue
• Reduced appetite
• Dark skin color
• Stay sick with infections
• Stomach pain
• Salt craving
Adrenal Crisis • Low blood pressure
• Fever, chills, sweating
• Confusion
• Extreme tiredness
• Extreme dehydration
• Eventual Shock
Medical IssuesMonitoring for Adrenal Insufficiency
Published in 2018
Agreed on screening for boys identified with ALD through newborn screening
Specifics:• What labs to test and when
• Follow-up testing
• When to start treatments
30
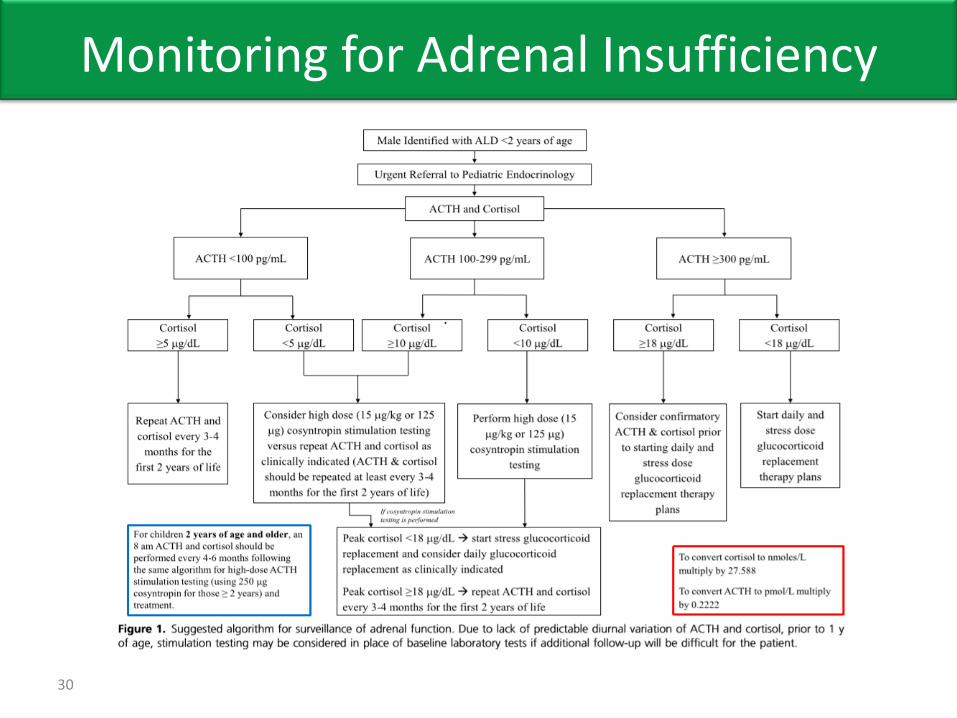
Monitoring for Adrenal Insufficiency
Adrenomeyloneuropathy (AMN)
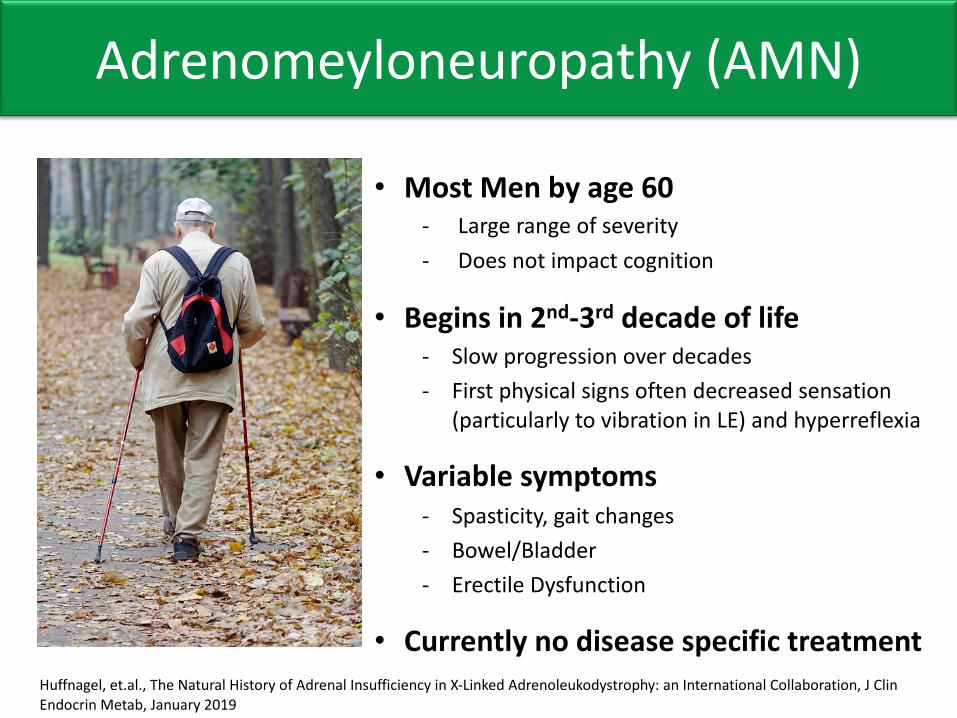
• Most Men by age 60- Large range of severity- Does not impact cognition
• Begins in 2nd-3rd decade of life- Slow progression over decades- First physical signs often decreased sensation
(particularly to vibration in LE) and hyperreflexia
• Variable symptoms- Spasticity, gait changes- Bowel/Bladder- Erectile Dysfunction
• Currently no disease specific treatmentHuffnagel, et.al., The Natural History of Adrenal Insufficiency in X-Linked Adrenoleukodystrophy: an International Collaboration, J Clin Endocrin Metab, January 2019
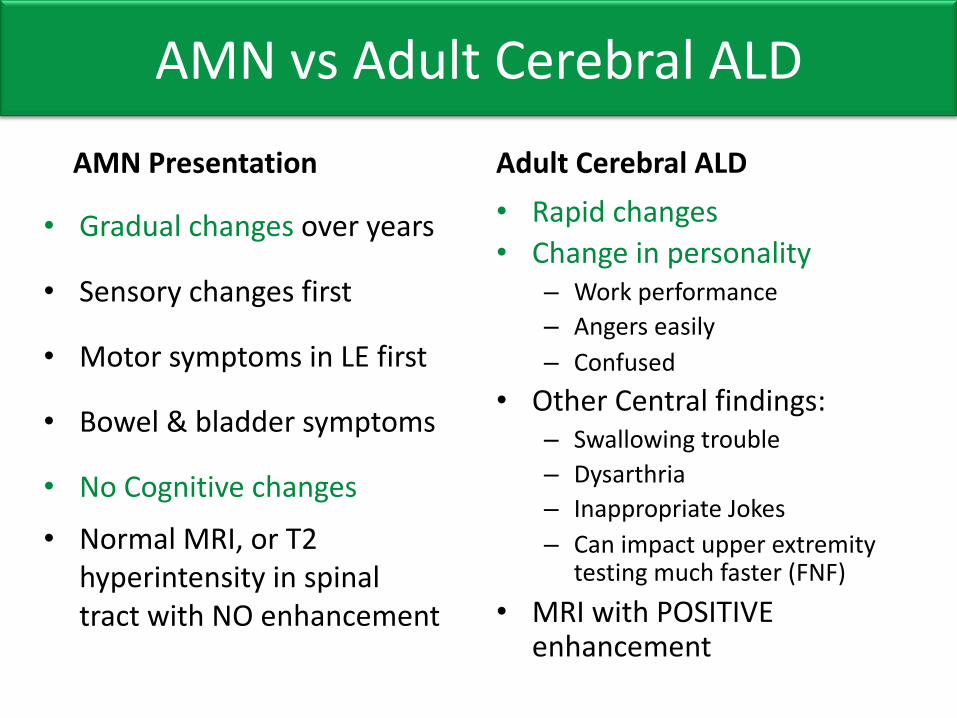
AMN vs Adult Cerebral ALDAMN Presentation
• Gradual changes over years
• Sensory changes first
• Motor symptoms in LE first
• Bowel & bladder symptoms
• No Cognitive changes• Normal MRI, or T2
hyperintensity in spinal tract with NO enhancement
Adult Cerebral ALD• Rapid changes• Change in personality
– Work performance– Angers easily– Confused
• Other Central findings:– Swallowing trouble– Dysarthria– Inappropriate Jokes– Can impact upper extremity
testing much faster (FNF)• MRI with POSITIVE
enhancement
Active Clinical TrialsGeneral ALD
- Pilot Vitamin D study based out of Stanford California
Childhood Cerebral ALD • BlueBird Bio: Lenti-Viral Exvivo Gene Therapy
– 1st study complete and being prepared for FDA, results published– 2nd study Actively enrolling – Must be early child with early cerebral ALD with contrast enhancement
• Minoryx Theraputics: Leriglitazone– Open in Europe only– Cerebral lesion with or without contrast enhancement– Strategy would be to prevent development of enhancement through
anti inflammatory property and reduced oxidative stress
Active Clinical TrialsGeneral Transplant: including Cerebral ALD• Magenta Therapeutics: MGTA-456
– Cerebral ALD undergoing cord blood transplant, work to expand volume of the cord blood
– University of Minnesota , Emory University, Duke University
• UCB Transplant with intrathecal UCB Derived Oligodendrocyte-Like Cells (DUOC-01)– Cerebral lesion going for cord blood transplant– Duke University
Active ResearchGeneral ALD• Minnesota ALD Registry Study (MARS)• Several Natural History and Biomarker Studies
– Stanford, KKI, MGH, Minnesota, University of Pittsburg, GainsvilleFlorida, UCLA, Boston Children’s…..
• Upcoming NIH sponsored Multi-Center Natural History Study (GLIA-CTN)– CHOP, KKI, MGH will include studies for men and women with ALD
AMN• Minoryx Theraputics: Leriglitazone
– Double blind study ending this summer– No data yet available
ALD Centers
Most Common QuestionsAsymptomatic ALD
Can we just do a transplant now?
Transplant is ONLY recommended when we see active cerebral disease for several reasons:
1. Transplant has serious risks. While it’s come a long way there is still significant risk of transplant that makes it too dangerous unless we see active cerebral disease. Only 30-40% of boys will ever develop cerebral ALD
2. We don’t know if it works without active diseaseWe don’t actually know if transplant can even prevent cerebral disease. The active inflammation and breakdown of blood brain barrier may help tell the new cells where to go.
Should we look for HLA Match NOW?
1. If there are siblings, SOME families choose to do testing for a perfect sibling match (only if family wants to)
2. Donor pool changes: So it is NOT recommended to do ahead of seeing a lesion, because the donor pool will change over time
3. We have time: As long as we stay on top of the MRI schedule, we have time.
Lorenzo’s Oil/Fat?
Lorenzo’s Oil is not available in the US.
Current recommendation is a normal healthy diet. Fat is important in laying down new myelin especially in first 2 years of life. Whole milk is still recommended in these years!
Few things to remember:• There is no association between how high your VLCFA are
and developing CCALD• We have transplanted many boys who were strictly
following the Lorenzo’s Oil diet and still developed CCALD• Most important thing is staying on top of the brain MRIs
What happens if he falls and hits his head?
There is some evidence that severe head trauma (that results in breaking the blood brain barrier) can increase risk of cerebral ALD
- Major traumatic brain injury- Brain surgery (shunt placement, biopsy, etc)
While we recommend avoiding direct head contact supports (football, ice hockey, etc.), there is no evidence that minor head injury causes CCALD
All children fall and bump their heads, many have had stitches. It is OK! They need to be able to play and explore for normal development. We only want to avoid high risk activities. Head trauma that results in a LOC is what we are trying to avoid.
Resources for Families
United Leukodystrophy Foundation Leukodystrophy Care NetworkHunter’s Hope Foundation – Family CareAidan Seeger FoundationALD FoundationALD Life (UK)Brian’s HopeCure ALD FoundationEthan Zakes FoundationThe Myelin ProjectStop ALDALD Connect
Resources for Medical Professionals
Leukodystrophy Care Networkhttps://adrenoleukodystrophy.info/Published care guideline on endocrine monitoring Soon to be published guideline on MRI schedule:
LCN Care Coordinator Shared Files for ALD
ALD Phenotypes Urodynamic Information
Scales for Cerebral ALD:ALD Loes Score templateNFS scale template
Adult ALD: AMN Note template
Publications:Adrenal monitoring for ALDGene TherapyN-Acetylcystine
Thank you!