adapting enactments to couple reactivity: five developmental stages
TRANSCRIPT

Journal of Marital and Family Therapy July 2003,Vol. 29,No. 3,311-327
ADAPTING ENACTMENTS TO COUPLE REACTIVITY: FIVE DEVELOPMENTAL STAGES
Mark H. Butler Brigham Young University
Brandt C. Gardner Texas Tech University
Interest in change interventions that are common to different models of relationship therapy has spurred investigation of enactments as one such candidate. In change-focused enactments, therapists structure and coach couplefamily interaction, as opposed to channeling interaction through the therapist. Still, varying levels of couplefamily distress, volatility, and reactivity mean that readiness for enactment intervention varies along a broad continuum and changes over the course of therapy. This suggests the need for diyerentiated enactments. Currently, howevel; no model exists for adapting enactments to changing relationship conditions. We propose ajve-stage developmental model of clinical operations in couple therapy that adapts the process and structure of enactments to changing levels of relationship distress, interactional volatility, and emotional reactivity. The model increases the possibility for therapists to use enactments successfilly over the entire course of couple therapy. Issues to be considered in using the couple enactments model as a template for the development of enactment models for other relationship systems are noted.
Interest in change mechanisms that function across different models of therapy has spurred consid- eration of enactments as a possible common operation in relationship-oriented therapy. We propose a model of enactments developed from our clinical work with couples. In this setting, enactments seem to be a critical dimension of “best practice,” providing a structure and process crucial to relationship mediation concerned with healing, enriching, strengthening, and empowering relationships. In addition, enactments- which are inherently relationally focused-may be viewed as a defining clinical operation that is unique and essential to relational therapies.
Therapist-centered and therapist-anchored clinical interaction, by concentrating and converging clinical dialogue and interaction in the therapist, is, as Bowen discovered and articulated (Kerr & Bowen, 1988), a straightforward approach to attempting to regulate negative affect and contain destructive expression- expression that readily leads to volatile, escalating in-session episodes, which have been linked to poorer clinical outcomes (Butler & Bird, 2000; Shields, Sprenkle, & Constantine, 1991). However, this simple resort, if employed over the entire course of therapy, may ultimately disempower couples or families, either leaving the system essentially unimproved at termination or permanently establishing the therapeutic system, interposing the therapist as an essential additional member of a viable couple system. Gottman and Gottman (1999) concur, and further warn that making the therapist “irreplaceable . . . may maximize the couple’s relapse once therapy terminates” (p. 3 10). Therapist-anchored clinical process may facilitate containing and structuring couple/family interaction, but may ultimately be disempowering and counter- productive. Therefore, a more complex clinical technology appears to be necessary to enable therapists to
Mark H. Butler, PhD, Marriage and Family Therapy Department, Brigham Young University; Brandt C. Gardner, MS, Marriage and Family Therapy Program, Texas Tech University.
Correspondence concerning this article should be addressed to Mark Butler, Marriage and Family Therapy Department, School of Family Life, Brigham Young University, 262 TLRB, PO Box 28601, Provo, Utah, 84602. E-mail: [email protected]
July 2003 JOURNAL OF MARITAL AND FMILY THERAPY 311
empower couples/families through successful interactional experiences carefully promoted, structured, and coached by the therapist.
Sophisticated use of enactments may provide one means for therapists to regulate and guide the clinical experience, while still sustaining client-anchored clinical interaction. For this to be possible, however, clinicians need a dynamic, developmental model of enactments that adapts its operations and interventions to varying levels of clients’ distress, volatility, and reactivity. Enactments have recently received significant attention (Allen-Eckert, Fong, Nichols, Watson, & Liddle, 2001; Davis & Butler, 2002; Nichols & Fellenberg, 2000), yet critical gaps in our theoretical understanding and clinical implementation still need to be remedied.
LIMITATIONS IN STATE-OF-THE-ART CONCEPTUALIZATION OF ENACTMENTS
Enactments are broadly conceptualized as therapist-coached couple/family interaction. Enactments are interventions that target interaction patterns for change and use those same interaction experiences to effect deeper attitudinal, attributional, emotional, and attachment shifts or changes. Thus, through enactments, interaction is both a change target and change mechanism.
Based on our clinical experience, which is significantly informed by attachment theory (Cassidy & Shaver, 1999) and emotionally focused therapy (Johnson, 1996), we propose that, within the context of couple therapy, the goal of enactments is couples’ self-reliant interaction that (a) results in successful resolution of problems; (b) promotes secure attachment; and (c) promotes mutual positive self-concept. We view perceived threats to secure attachment and/or positive self-concept as the two primary existential threats that typically derail successful couple interaction and lead to personal and relationship distress. In addition, we apply Gottman and Levenson’s ( I 992; 19996) recommendations for therapy process generally to enactments as well: [Enactments] should reduce physiological arousal and reactivity (Gottman & Levenson, 1992; 19996); facilitate positive interaction around discussions of disagreements, differences, and problems (Gottman & Levenson, 1999b); increase display of positive behaviordaffect, together with the other’s ability to recognize those positive displays (Gottman & Levenson, 2000); reduce defensiveness, stubbornness, withdrawal, anger, and conflict engagement (Gottman & Levenson, 1992); increase expressed interest in each other (Gottman & Levenson, 1999~); and increase ability to step back and see their partner’s point of view (Levenson & Gottman, 1983). We also think it critical that the couple learn to monitor their own interaction process from a metaperspective and regulate it for the well-being of the relationship. Enactments may be one tool therapists can use to promote couples’ development toward this kind of self- reliant interaction.
Risk Associated with State-of-the-Art Enactments Yet clients entering therapy range along a broad continuum in terms of their relationship distress and
their vulnerability to volatile, emotionally reactive interaction. In addition, these relationship attributes may fluctuate considerably during therapy. Assessment of and adaptation to these conditions needs to inform clinical practice generally and the use of enactments specifically. To apply enactments monolithically and blithely engage distressed couples in interaction while the therapist removes himself, abdicating process to the couple, is to invite them to “argue among themselves as they may do at home” (Shields et al., 1991, p. 13). Such unstructured interaction is predictive of poorer clinical outcomes (Butler & Bird, 2000; Shields et al., 1991). If enactments do not correspond to critical relationship conditions, the intervention may explode or implode as interaction escalates destructively or shuts down. Conversely, therapists who are concerned about the possibility of enactments deteriorating may altogether cease to use them, even with moderately distressed couples, and thus forfeit potential clinical benefits.
Dynamically Adapting Enactments to Levels of Distress, Volatility, and Reactivity All this makes the use of invariant, direct couple interaction (enactments) for achieving the goals listed
earlier potentially problematic, and presupposes the need for an adaptive, differentiated model of enactments that fit5 enactment process and structure to current relationship conditions. It is critical to differ- entiate or adapt enactments to “fit” changing couple dynamics. Theoretical, clinical, and empirical guidance
312 JOURNAL OF MARITAL AND FAMILY THERAPY July 2003
needs to be applied in the process of developing enactments capable of addressing the interaction goals listed earlier, while simultaneously adapting them to the ever-changing interaction possibilities and potential couples present therapists with. Again, we limit our focus here specifically to enactment5 for couple relationships; there are additional issues unique to other relationship configurations that are beyond our scope here.
Currently, however, no model exists for fitting the process and structure of enactments to different degrees of relationship distress, interactional volatility, and emotional reactivity, even though these dynamic conditions vary considerably between couples, as well as over the course of therapy. Again, an invariant model of enactments, understmctured in terms of couple distress, volatility, and emotional reactivity, risks unraveling and becoming destructive. Conversely, a monolithic approach to enactments risks tedium and frustration if they are overstructured relative to couple dynamics.
We propose a five-stage developmental model that adapts the process and structure of enactments to changing levels of couple relationship distress, interactional volatility, and emotional reactivity over the course of therapy. The five-stage model of enactments is fluid, dynamic, and adaptive to a couple’s changing presentation from session to session. Thus, our five-stage model operationally differentiates enactments to address these changing dynamics in couple relationships throughout therapy. Our purpose in developing an adaptive stage model of enactments is to enable therapists to use enactments from the earliest to latest stages of therapy. Nevertheless, pro forma use of any of the stages of enactments as a matter of rote is neither necessary nor desirable. Each stage is only used as indicated by concordant levels of distress, volatility, and reactivity. Further, it is not uncommon for a couple to regress situationally from time to time. More provocative issues lead to situationally heightened distress, volatility, and reactivity. In these instances, the therapist may find it useful to return to a previous enactment stage. The model is not rigidly linear.
Our adaptive, developmental model of enactments over the course of therapy is designed to dovetail with contemporary models of the component operations-separate steps or processes-af single enactments (Davis & Butler, 2002; Nichols & Fellenberg, 2000). The five-stage model adds a developmental perspective to our current freeze-frame profile of enactments, thereby allowing therapists to evolve and employ enactments successfully throughout therapy. Our conceptual, clinical, and empirical understanding of couple therapy is the basis for our model of enactments. Consequently, the generalizability of this model of enactments to other relationship systems is uncertain. Dynamics unique to other systems-for example, developmentally based hierarchy and power differences, unique family relationship structures, such as triangles (Butler & Harper, 1994)-lead us to suggest the model’s potentially limited generalizability to couple therapy. Before our model can be more broadly applied, careful analysis of the unique structural and interaction dynamics of these other systems must inform modifications and stipulations to the couple-based enactment template. This model may, nevertheless, provide such a template.
ENACTMENTS IN FIVE DEVELOPMENTAL STAGES
Across all stages of enactments, the therapist’s focus is on coaching interaction as opposed to advice giving. The presumption is that when therapy goes well, couples will usually be able to craft idiosyncratic solutions that are better adapted to their values, beliefs, and relationship styles than any the therapist might propose. Thus, generally speaking, interaction process, not problem content is the purview or province of the therapist using enactments.
In enactments, the therapist’s global objectives are twofold: First, to situate herself within the couple relationship so as to be able to regulate the interactional proximity (how directly they interact), emotional intensity (how high-pitched their interaction is), and verbal autonomy (how freely they interact). This allows the therapist to regulate couples’ immediate levels of relationship distress, interactional volatility, and emotional reactivity. As couples progress through the five stages of enactments, proximity, intensity, and autonomy are all incrementally increased. This structuring (Shields et al., 1999) does not mean the therapist keeps a tight lid on affect, but she or he does filter, buffer, and dampen destructive exchanges. Passion is not problematic, but relationship-corroding hostility, negativity, and contempt (Gottman, 1999) are not left unchecked. We recommend that enactments be carefully structured and regulated so as to yield positive in- session experiences.
July 2003 JOURliAL OF MARITAL AND FMILY THERAPY 313
The second global objective in enactments is to coach progress in process that enables the couple to interact in a satisfying way that is increasingly independent of the therapist’s assistance. In our approach to enactments, successful interaction means that primary emotions are shared in ways that address and facilitate secure attachment (Cassidy & Shaver, 1999) and positive self-worth, and all of these conditions empower the resolution of specific relationship problems. When couple interaction is self-reliant-meaning their process (how they interact), although occasionally volatile, is attended to and sensitively managed, so that it neither leads to relationship injury nor derails problem-solving-therapy will be ready for closure.
Our operational description of five stages of enactments will be exemplified in a hypothetical couple therapy case based on our clinical experience. Martha and Raphael are a married couple in their 30s. They have been married for 7 years and have two children. Martha is a sales representative in a large, interna- tional corporation, and Raphael is on the fast track to a partnership in a prestigious law fm. The pace of their respective careers frequently keeps them apart. For the last several years, when they are together both are usually emotionally and physically drained and barely have enough energy to engage in essential task- oriented conversations related to rearing their children and keeping their household running. Given the demands both face, disagreements about childrearing and household responsibilities have not been uncommon and have increasingly escalated into conflict. With both of them feeling that the other is “protecting their own turf,” but without the time, energy, or solitude to work things through, an emotional and physical distance has opened up between Raphael and Martha. Both tend to become defensive or hostile and shut dowdwithdraw or attack when their interests are threatened. Both feel that their partner is insensitive to their feelings or needs. Recently, Martha has started having regular private lunches with a male coworker. When Raphael challenges her about this, she becomes defensive and conflict erupts, only increasing the distance between them, along with Raphael’s fears. Martha now spends more time at work, much of it with her coworker. Following their most recent argument, Martha and Raphael decide to seek therapy from Samuel, a licensed MET to whom they were referred by their pastor.
STAGE ONE: SHIELDED ENACTMENTS
Initial observations and impressions suggest to Samuel that Martha and Raphael are currently highly distressed, volatile, and reactive. Consequently, he determines to begin enacting their relationship using stage one, shielded enactments. We use the term shielded to signify that therapist operations in this stage shield or protect each spouse from direct, face-to-face experience of their distressing relationship and volatile couple interaction.
Process and Structure The use of stage one, shielded enactments signifies the therapist’s tacit assessment that Martha and
Raphael are currently not interactionally self-reliant. In shielded enactments, 100% of the interaction is passed through the therapist. The acting partner “passes” herhis thoughts and emotions to the therapist, and the attending partner is invited to listen and understand through the therapist. Also in stage one, coaching- the central therapist operation in enactments-is primarily through modeling. Indirect coaching by modeling includes therapist reframing in terms of primary emotions, as well as attachment and self-concept needs, and therapist attending in terms of the same, and it predominates over direct coaching (inviting or soliciting the acting partner to so restate himself and the attending partner to hear in terms of primary emotions and attachment or self-concept needs or distress). When modeling for either the acting partner or attending partner, the therapist is more likely to suggest and represent than to elicit and coach conciliatory expression or hearing anchored in primary emotions and attachment or self-concept needs. Only occasionally is coaching direct, with the therapist assisting partners in altering expression and listening, respectively. Direct coaching is more characteristic of enactments from stage two forward.
Samuel: Raphael and Martha, the experiences that have brought you to therapy are obviously serious, and provoke intense feelings for each of you. I could try to “take care of’ your relationship, but experience suggests that you’ll be better off if I help you do that.
314 JOURNAL OF MARITAL AND F M I L Y THEKAPY July 2003
Nevertheless, to begin with, I’ll try to help in that process. For a little while, I’m going to provide each of you with a little emotional space, to shield you from the intensity that has sparked harmful experiences in your attempts to work through this problem. I’ll do that by having your conversation with each other pass through me. Please remember, though, that your conversation is with your partner, not me. Your purpose is not my understanding, or empathy, or validation, or change, but your own. Only that will heal your relationship. So think of me as a conduit and a coach for your relationship. As we progress, you’ll be interacting more and more directly with each other, until-as before-you’re satisfied with your interaction and relationship, even while sharing these things that are at the very heart and soul of your personal lives and relationship. In your interaction, there will be an acting partner and an attending partner. To help your conversation stay on track, I’m going to keep these two roles separate for a while. We won’t be shifting back and forth a lot. Raphael, I’d like you attending first. Martha, you’ll be speaking.
Samuel (to Raphael): Raphael, could you please slide your chair back a little bit, and turn it so you aren’t facing Martha. Lean back in your chair, breathe deeply, and allow yourself to relax. As the attending partner, that’s your first objective. Martha’s going to share some intense feelings and provocative thoughts, but I’ll be the one “catching” all that. I’ll hold on to them so that you won’t have to. This will enable you to focus on understanding. That’s your second objective. In seeking understanding, the important thing is not to think that there’s a right or a wrong to be discovered here. What you each want is to get close again. To do that, you need a window on her world, and she, yours. Work to accept that her experience of things-however much it may differ from yours-is nonetheless truly her experience. There can be two truths-your experience and her experience-and to get close you need to have that window on each other’s world. That window will help you see how to take care of each other; that’s our work here, not to determine a “right” or “wrong.” And now that you see that her experience of things doesn’t threaten the truthfulness of your experience, you‘ll feel less provoked to either contradict her experience or defend yours. You can understand, accept, and eventually respond in a way that’s consistent with her experience. That’s how you’ll achieve a satisfying marriage again.
Samuel (to Martha): Martha, the same view of things will change the way you carry out your part, too. As the acting partner, your job is to help Raphael understand. You won’t think of it as arguing or defending your case like an attorney or advocate in a win-lose proposition. Rather, you’re just giving Raphael that window on your world, in preparation for a win-win resolution. So you’ll find you can use soothing and softening expressions-telling Raphael more about your hurt and sadness than your anger, more about your experience, disappointment, and hopes than about being blameless or right. Shall we begin?
Using the skeletal outline of this hypothetical example, we will flesh out the defining process and structure of stage one, shielded enactments. Elements of each of the five stages are listed in Table 1. A central component of shielded enactment structuring consists of keeping acting and attending roles spaced and distinct. Escalation is the product of exchanges. The potential for escalation is high when both partners are brought into the communication mix as simultaneous “actors” with no “audience.” Conversely, the potential for escalation is greatly reduced when acting and attending roles are separated and not simultaneous. Deescalation is more likely. Although this structuring stilts typical, free-form exchanges and is often tedious and frustrating to couples, what is also frustrated is combative engagement with one another. Evidence suggests that this is highly advantageous (Butler & Bird, 2000; Shields et al., 1991).
A second component in shielded enactments is that the therapist structures interaction so as to make
July 2003 JOURNAL OF MARITAL AND FAMILY THERAPY 315
himself a conduit, or pass-through for the interaction experience of both the acting and attending partner. Thus, the therapist explicitly separates both the acting and the attending partner from the currently overwhelming (Kerr & Bowen, 1988) demands of direct, face-to-face interaction. Martha expresses her thoughts and feelings in the comparatively safer context of the therapist conduit. As the attending partner, Raphael is an active, neutral (explained below) listener; he is encouraged to key in to the therapist as his pass-through access to Martha’s world.
While carrying out their respective roles, Raphael is simultaneously an observer of the interaction between the therapist and Martha; and Martha observes how Samuel reframes messages as he passes her expressions along to Raphael. This is coaching through modeling. As the conduit, the therapist usually filters both the acting and attending partner’s expressions and hearing. Thus, the therapist uses reframing to translate expressions into the language of primary emotions and attachment and self-concept needs, which are more likely to be heard and responded to positively-with deescalation, softening, and empathy.
Martha: Samuel:
For so long, you haven’t been there for me; of course his attention attracted me! Martha, . . . [therapist pauses] what I hear in your words is, “I’ve missed our relationship. I love you and need to be close to you. I’ve felt unneeded and lonely, and hurt” [modeling]. Does that fit your feeling? [Martha nods.] Perhaps Raphael could be receptive to your loneliness and respond to your desire to be close again if you say it that way. Would you?
Martha: He’s so selfish with his time. I have responsibilities too, you know. Samuel (to Martha): Martha, I hear your frustration in trying to manage an almost overwhelming
schedule and pace. You chose Raphael and would like to be able to lean on him for help. I wonder if Raphael is able to hear what you’re trying to say, given the words. Is there a way to share the same feelings differently, to better help Raphael hear them [coaching].
Samuel (to Raphael): Raphael, how can you “hear” what Martha just said, different than the actual words, so as to help you feel calm, and keep focused on your purpose of gaining a window on her world-as opposed, perhaps, to being provoked by the words themselves [coaching]. Do you think the “translation” I offered is useful [modeling]? Can you work from my own or your “softened” translation rather than the actual words?
After a while, the therapist will reverse Martha’s and Raphael’s roles. When Raphael becomes the acting spouse, the therapist will explicitly monitor and coach his communications to ensure that they are not reactive or even responsive to Martha’s expressions, particularly in a defensive or combative way-what Raphael might refer to as “explanation” or “clarification.”
Raphael: Samuel:
Well, to begin with, I’d like to “clarify” some of the things Martha said. Raphael, it’s not as important as you may think for me to “understand.” Martha needs to understand you. She wants to connect with your experience, as you did with hers. Organizing your thoughts as a counter to some of the things she said might make that difficult. Instead, simply begin at your beginning and share your feelings, fears, hopes, and needs, without “reacting,” to what she’s said. It’s her, not me. I’m just your conduit for the time being.
In shielded enactments, in addition to the therapist facilitating, modeling, and coaching expression, process for the acting partner includes facilitating partner perspective and problem-solving responsibility as well.
Martha, now that you’ve both had a chance to get a better window on each other’s lived experience of the marriage, can you help him see the window that you have on his world as well. Please share your understanding, and feeling, for his experience.
Samuel:
316 JOURhHL OF MARITAL AND F M I L Y THERAPY
Martha: Samuel:
[Shares Raphael’s perspective as she understands it.] Finally, Martha, in all this, what do you feel you could choose to do to improve the situation? [Therapist invites neutrality (self-change perspective).]
In addition to features of shielded enactments already noted, certain other process elements deserve mention. As depicted in our example, initiation of stage-one enactments requires more preparatory explanation than do later enactments for two reasons. First, distressed couples are least prepared at this point to engage with one another productively and charitably. They are helped by a careful, explicit description of what a satisfying experience will require of them, accompanied by encouragement. Second, a thorough explanation sets the stage for the entire therapy and the developmental progression of enactments over its course. The therapist paints the picture of satisfying couple interaction that all enactments will aim for.
Preparatory explanation of enactments to couples, including shielded enactments, includes descriptions that point to and presuppose desired interaction patterns, as in the example above. These descriptions play a limited but specific role in eliciting positive interaction. In describing what the process and outcome of the enactment episode can be, the therapist emphasizes the acting partner’s focus on conciliatory, relationship- oriented expression, and the attending partner’s emphasis of empathic, nondefensive listening. Both are invited to maintain calm, using methods including self-soothing, thus preventing confounding physiological arousal.
Another structuring intervention in shielded enactments, complementary to presuppositional descriptions, is containment or regulation of inciting words, emotions, and nonverbal expressions. With partners that are highly distressed, volatile, and reactive, the therapist may ask the attending partner to turn so as to minimize eye contact. This helps prevent nonverbal expressions from either the acting or attending partner from inciting a reaction and disrupting a focus on attachment-oriented expression and empathic listening and understanding. In all these ways, therapist intervention is used to minimize the impact of charged statements, emotions, and expressions, and empower softening expressions while couples remain volatile.
In shielded enactments, Samuel does not disconnect the couple relationship, but ‘‘brings” the relationship to them. This process and structure allows him to act as both a passive container and active checkpoint and filter for Martha and Raphael’s interaction process. In this manner, couple interaction proximity, emotional intensity, and verbal autonomy are constrained, filtered, and regulated. As a result, we anticipate that each partner will attain a neutral “window on the other’s world” that promotes deescalation, softening, and nascent empathy. These outcomes are made possible by each partner being offered a compar- atively nonprovocative interaction experience, the result of therapist pass-through positioning that filters and contains otherwise inciting interaction. A second anticipated outcome is interaction skills development through therapist modeling.
STAGE TWO: BUFFERED ENACTMENTS
The term buffered signifies that therapist operations in this stage buffer or filter spouses’ interaction, changing meaning and experience in ways that facilitate softening and allow couple interaction to proceed and constructive understanding to develop. Therapist positive connotation, reframes, and interpretations accomplish this buffering of otherwise volatile exchanges.
Indicators for Transition Progress prerequisite for transition from stage one (shielded enactments) to stage two (buffered
enactments) is minimal. We recommend that therapists shift from stages one and two to stage-three enactments as quickly as possible to avoid solidifying therapist pass-through interaction process. Minimal indicators for transition to stage two include calming, manifest in diminished physiological arousal (see Gottman, 1993, 1999, for observable markers of diffuse physiological arousal [DPA]), and softening (Johnson, 1996), manifest in conciliatory self-expression in the acting partner and receptivity in the attending partner.
July 2003 JOURNAL OF MARITAL AND FAMILY THERAPY 317
Process and Structure With immediate volatility and reactivity abated, attachment and self-concept needddistress coming
into focus, and relationship regard renewed, the therapist shifts to stage- two, buffered enactments. Structurally, as in stage one, 100% of the interaction is still brought to Martha and Raphael via the therapist conduit. In stage one, process coaching consisted of modeling, whereas in stage two, process is elicited and coached directly. The therapist elicits and coaches their conciliatory expression and hearing. The attending partner is increasingly engaged in formulating an understanding of acting-partner statements in terms of primary emotions and attachment or self-concept needddistress. The acting partner is increasingly relied on to articulate the conversation in these same relationship terms. The therapist elicits and coaches, but forebears modeling-thereby shuffling himself one step back from the couple’s relationship. Nevertheless, the therapist remains a structural conduit for Martha and Raphael’s interaction.
A second way in which process changes is that the therapist shifts between the acting partner and the attending partner more frequently now. Rather than listening for quite a while and only occasionally shifting attention to the attending partner, the therapist shifts with increasing frequency until only several talk turns pass between therapist shifts. This pass-through shifting brings couple interaction closer to real-time exchanges. Nevertheless, the relationship still passes through the therapist 100% of the time. The therapist remains interposed between them.
Raphael:
Martha: Samuel:
Martha: Raphael: Samuel:
Raphael:
Samuel:
I wish Martha could hear herself talk, then she’d understand just how selfish, unreasonable, and demanding she’s being. You can see that, can’t you? Raphael, I’d like to pause the conversation and invite you to edit it for me, so that it’s easier to hear without hurt or anger. First, remember that your object is not to challenge Martha’s experience or defend your version of reality, but to get a window on each other’s world so as to make it easier to connect. So, instead of passing your agreement or disagreement with Martha’s experience through me, just share your own. Try to share it in terms of “primary” emotions underneath it all-what we’ve talked about-and in terms of what you hope for in your relationship with Martha. [Nods.] I guess I feel hurt, and offended, that Martha doesn’t seem to see my needs as being as important as hers. Bottom line, I guess that threatens me, because I wonder if she would put her own wants and needs ahead of mine . . . o r . . . ahead of our relationship. That doubt makes me feel particularly anxious and vulnerable about this guy at work. But there’s nothing between us! Martha, 1’11 come to you. 1’11 bring the conversation to you in a moment, okay. Focus on attending, too, not defending. Remember, Raphael’s not attacking your experience, just sharing his own, and both are real! That window on his world is your passport inside. [Expresses assent.] [Continues to share his experience.] [Turns to Martha.] Martha, you’ve lived and loved with Raphael for 7 years. You sense his meaning. From listening, what do you know about Raphael’s experience? What feelings do you hear-behind any criticism or anger? What needs may lie underneath it all?
Noted in the example above was a neutrality threat-Raphael’s solicitation of therapist agreement/alliance (Butler & Harper, 1994). The therapist responded by treating it as a nonproductive attempt to persuade Martha (not the therapist) to his point of view, rather than focusing on “windowing” his experience of the relationship for Martha. Samuel does not allow himself to be engaged by alliance solici- tations, but maintains his pass-through positioning. He is a facilitator of their relationship, not a third party judging the situation, nor intending to form any separate, independent relationship with Raphael or Martha. He functions as a coach, mediator, and facilitator, not judge, ally, or substitute. Finally, in addition to facili-
318 JOURNAL OF MARITAL AND F M I L Y THE‘RAPY July 2003
tating and coaching acting and attending in terms of primary emotions and attachment or self-concept needddistress, Samuel foreshadows stage-three enactments by presupposing additional interaction skills that will need to be practiced, for example, reflecting, clarifying, validating, and so forth.
Samuel: [As part of lengthy enactment.] Martha, responding sensitively to Raphael right now, how would you go about making sure you understand him? How could you respond to him in a way that shows you care, and that you value his feelings, even if you don’t fully agree? How might you show Raphael your commitment to solving the problem as opposed to determining fault? How will you convey willingness to “do your part?’
To review, in stage two, enactment structure is identical to stage one, with 100% of couple interaction passed through the therapist (see Table 1 ). Procedurally, however, coaching supplants modeling, and pass- through shifting from the acting to attending partner is more frequent, bringing couple interaction closer to real-time exchanges. By these means, the response capacity of each partner toward the other increases. Buffered enactments presuppose that the couple system is still in need of patient coaching and significant buffering of residual negative emotions, negative sentiment ovemde, and emotional intensity. Relationship distress, interactional volatility, and emotional reactivity still dictate pass-through enacting of their relationship, but as this dissipates, behavior signaling readiness for stage three (defined below) will be observed.
Interaction proximity and emotional intensity increase in stage-two enactments, as couple interaction is brought closer to real-time, unreframed exchanges. Nevertheless, therapist pass-through positioning continues to limit verbal autonomy, maintaining therapy as a safe haven for relationship interaction. As stage-two enactments progress, couples’ capacity and skills for emotionally focused and attachment-based sharing are anticipated to increase considerably. In addition, therapist coaching helps couples to master basic communication skills.
STAGE THREE: FACE-TO-FACE TALK-TURN ENACTMENTS
The terms face-to-face and talk-turn refer to therapist operations focused on intensive coaching of direct spouse-to-spouse interaction, up to and including talk-turn-by-talk-turn intervention, thus allowing the therapist to regulate couple distress, reactivity, and volatility during stage three face-to-face enactments. The process level of interaction for these enactments is the individual speech act (Greenberg, 1986).
Indicators for Transition Stage-three prerequisites include the couple’s willingness to relate to each other in a conciliatory,
receptive, vulnerable, and relationship-focused manner, together with their willingness to listen without interruption, genuinely attend, seek partner perspective, validate, and empathize. With these rudimentary elements for successful interaction in place, successful stage-three enactments are possible. Helpful, but not essential, for stage three is nascent skill in expressing (acting partner) or discerning (attending partner) primary emotion and attachment or self-concept needddistress.
Despite a significant shift in the structure of the enactment (explained below), stage-three enactments remain relatively easy to regulate. Hence, we recommend that therapists attempt these enactments as early in therapy as possible. Indeed, the distress, volatility, and reactivity of a significant proportion of couples will be low enough that stage-three enactments will be possible early on, if not from the start. In such instances, pro forma use of stage-one and stage-two enactments as a matter of rote is neither necessary nor desirable. As previously indicated, each stage is only used as indicated by concordant levels of distress, volatility, and reactivity.
Process and Structure Although the primary shift between stage-one and stage-two enactments is processual-from modeling
to coaching-the main difference between stages two and three is structural. From stage two forward,
July 2003 JOCJRNAL OF MARITAL AND FAMILY THERAPY 319

enactment process conqists of coaching, rather than modeling. In stage two, however, coaching is pass- through. At stage three a significant structural shift is made-the therapist no longer interposes himself, bringing the relationship to the couple. He sets aside pass-through positioning and situates himself to coach interaction from outside the relationship. All couple interaction will now pass directly between Raphael and Martha. Still, coaching-at the level of individual speech acts-remains the substance of stage-three enactment process.
This structural shift means that therapist operations shift from shielding or buffering couples’ affective reactivity and attachment distress or self-concept threats to simply coaching and facilitating them in working through it themselves. Thus, in stage three they will be coached in managing their own interaction volatility, primarily through the discipline of basic communication skills, but also through increasing ability to articulate and be receptive to their emotional experience and attachment andor self-concept needddistress and bring about softening. Stage-three enactments mark an observable shift toward couple responsibility (Butler & Harper, 1994) and self-reliance.
Consequently, to begin stage three, Martha and Raphael are invited to turn toward and face each other. Before, visual contact was either obstructed-as where the spouse not engaged with the therapist was asked to face away from the interaction-or minimal, as where each spouse was focused on the therapist. Now, the spouses are invited to look directly at each other. Given their growing awareness and ability to track multiple levels of interaction, Martha and Raphael’s ability to maintain discerning visual (and sometimes physical) contact, and to do so less reactively than before, is very useful now. The couple may directly exchange verbal, nonverbal, and physical expressions of caring and love, as long as they do not intrude on the distance one’s partner still needs or invalidate their partner’s emotions by attempting to soothe and push hurt and anger aside prematurely, before they have had a chance to express and work through it.
Martha: [Reaches for Raphael’s hand.] Raphael: [Withdraws his hand.] Samuel: Martha: Samuel:
Martha, what do you hear Raphael saying when he pulls his hand away? I think he’s trying to punish me still. I wonder if it might be that Raphael wants to be close to you, but he wants it to be real, not “play-acting,” and something’s still missing for him. [Turning to Raphael.] Raphael, I’m sure you can understand how easy it is for Martha to misread your gesture. Can you make sure you clearly share with her what it means, and reassure her of your desire to work through whatever it is and be close again?
I haven’t finished telling you how deeply I’ve been hurt, and how angry I’ve been. I want you to hear me first.
Martha: What is it Raphael? Raphael:
Martha and Raphael interact directly with one another and are commended for the progress that has made this possible. In stage-three, speech-act enactments, the therapist provides microprocess coaching to create and maintain successful sequences and episodes. Samuel explains that his role in the enactment is to coach and micromanage their direct interaction. He informs the couple that initially he will be very engaged, active, and hopefully serviceable to their interaction, but his “intrusiveness” will decrease as time goes on. The couple is encouraged to be patient for the time being with speech-act-by-speech-act interruption and intervention .
Samuel: Raphael, Martha, I know this is tedious having me interrupt and coach “every step of the way.” But I’m confident if we get the foundation right, you’ll be able to share emotions and experiences and your deepest intimacy issues, and solve problems, without getting derailed.
The therapist notes that sometimes his intense engagement and active role, or the intensity of the enactment experience, or some of the things that are on their minds (e.g., complaints, for which a partner
320 JOURNAL OF MARITAL AND FAMILY THERAPY July 2003

may seek alliance connection with the therapist), may elicit their speaking directly to the therapist again. A reliable index to whether Martha and Raphael are relating with each other or the therapist will be whether they use third person (he, she, him, her) or first person (you, Raphael, Martha) pronouns. Such shifts are responded to by therapist redirection. When Martha and Raphael attempt to engage with Samuel, he will gesture, ask, or otherwise redirect their conversation back into the relationship.
Martha:
Raphael:
Samuel:
I just don’t know if I can stay with a man who won’t trust me, and who tries to keep such a tight rein on me. You see, she always does this, threatens divorce if I won’t just close my eyes. She pays no attention to what that’s asking of me. Raphael and Martha, I can see that you’re facing each other, but I sense you’re talking to me instead of each other. Remember it’s not me you want to get close to, or have understand you, but your partner. Talk to each other. But first, perhaps you’re sensing that the conversation is becoming a little intense again, and engaging with me is a “plea for help,” to help keep things under control. It’s appropriate at times to invite a mediator to help-as long as he cares about your relationship, can be neutral, and invites you to be responsible for resolving problems. Nevertheless, I’m confident you will work through this one yourselves. I’ll coach you a little, but only as much as you really need.
When partners attempt to reengage the therapist conduit, Samuel asks whether threatening thoughts or intense emotions have been provoked and whether the enactment feels as though it could get out of their control. If so, Samuel facilitates the couple in soothing self and other and calming their interaction for themselves. The therapist’s goal is to utilize stage three structure to keep the “problem in the relationship from which it is attempting to escape,” (Kerr & Bowen, 1988, p. 161) and work for resolution there. A final component of stage-three enactments is proxy expression, or speaking in the client’s voice, as described below. Although Martha and Raphael are mastering basic communication skills, more complex psycho- logical dynamics and affect, as well as underlying attachment or self-concept distress, may at times be present but beyond their articulation, though not beyond operation in the relationship. As these become apparent to Samuel, he may intervene by assuming a proxy position. Sliding his chair behind the acting or attending spouse, he asks permission to try to “speak in your voice” for a moment. Samuel invites the spouse for whom he is taking a proxy position to listen carefully so that she or he can correct andor confirm. If a partner indicates that Samuel has accurately traced and illuminated obscured dynamics, Samuel invites the spouse to rephrase the proxy voice in his or her words, offering corrections as needed, and then to continue the enactment.
In stage-three, face-to-face enactments, although coaching remains the substance of enactment process, the structural shift leads to meaningful differences in Martha and Raphael’s experience of enactments. With Samuel no longer bringing the interaction and relationship to them, no longer providing pass-through interventions that mediate exchanges, interaction proximity, emotional intensity, and verbal autonomy all increase significantly. At this point, however, proximity and intensity are less and less problematic, but rather increasingly positive and desirable, allowing intimate, emotional and attachment-focused interaction that is all the more powehl and healing for its being direct-unmediated and undiluted by a therapist conduit. Nevertheless, the limitation in verbal autonomy afforded by speech-act level intervention provides essential therapist maneuverability to promote and sustain positive couple interaction.
Anticipated positive outcomes of stage-three enactments include (a) couples’ increasing consistency in practicing basic communication skills; (b) attentiveness and responsiveness to emotions; and (c) increasing awareness, identification, and attentiveness to attachment and self-concept distress as important trigger points in relationship interaction. Finally, we note that stage-three, speech-act enactments intrude the discipline of focused relationship practice and skills development on the natural rhythm and flow of intimate interaction. Couples’ impatience with this tedium often leads them to work hard to develop the virtues (Fowers, 2001) and adopt the skills that will bring transition to enactments, allowing a more natural flow of interaction. We recommend transition from stage-three to stage-four enactments as early as possible.
July 2003 JOURNAL OF MARITAL AND FAMILY THERAPY 321

STAGE FOUR: EPISODE ENACTMENTS
The term episode (Greenberg, 1986) highlights stage-four transition to enactment episodes, or vignettes, in which spouses interact without significant therapist coaching for extended periods, followed by therapist-facilitated couple evaluation or processing of their interaction.
Indicators for Transition Three hallmark advances signal readiness for stage-four enactments: reasonable use of basic communi-
cation skills, self-awareness of interaction process, and resiliency. Martha and Raphael’s speech-act-by-speech-act exchanges should manifest mastery of the basic communication skills listed previously. Second, couples should manifest increasing in vivo or in-the-moment awareness of their interaction process. This includes being attuned and attentive to emotions and to attachment or self-concept triggers and distress, and they should make attention to these a priority, even while their interaction is ostensibly aimed at resolving specific problems. Within single episodes, distress, volatility, and reactivity should not usually overwhelm them and they should be able to prevent destructive escalation. On occasions where they do get caught up in their emotion, and their process again assumes a (destructive) life of its own, they should be able to red-flag their escalation patterns and prevent or exit negative sequences. With therapist assistance in lowering intensity, after a brief respite they will search and discover ways to preemp- tively identify, calm and soothe, and exit incipient negative cycles. Overall, they will be catching on to the particular dynamics of their relationship and, within that framework, will develop strategies for managing emotions, attending to attachment and self-concept distress, and solving problems. They apply these strategies in an idiosyncratic way in their own relationship.
Altogether, the therapist observes both that the couple’s interaction is objectively less provocative, and each partner is subjectively less apt to be provoked. As a couple, they are more resilient. They are thus prepared to navigate difficult issues without the distraction of speech-act-by-speech-act intervention, but also without serious risk of interaction explosion or implosion-fight or flight. Fulfillment of this constel- lation of developmental tasks signals readiness for stage-four, episode enactments in which their developmental task is to choreograph entire episodes of interaction on their own, followed by evaluation or processing.
Process and Structure In stage four, as in stage three, the couple interacts directly 100% of the time. The structure present in
stages one and two no longer shields or buffers couples’ affective reactivity and attachment distress or self- concept threats. In place of stage-one and stage-two pass-through structure, the therapist coaches and facilitates Raphael and Martha in working through their reactivity and distress themselves. Whereas in stage three this occurred speech-act-by-speech-act, stage-four coaching occurs at the episode level of interaction process. Thus, stage-four enactments are episode enactments, and the primary change between stages three and four is in terms of process. Shifting from speech-act to episode-level coaching is more than merely a decreased frequency of therapist intervention, though. The therapist allows Martha and Raphael’s interaction to run its course, thereby allowing them to run up against some real obstacles and challenges. Thus, stage four exposes Martha and Raphael to whatever emotionally provocative exchanges they offer without early intervention or interruption (as would be offered in stage three). They thereby test and strengthen their interaction, relationship, and attachment abilities, especially their ability to monitor and manage their process and exit negative sequences.
In stage four, as explained below, the most significant therapist intervention usually occurs at the conclusion of the enactment episode. However, the therapist-suspending the flow of interaction as little as possible-may occasionally offer brief asides to either Martha or Raphael to keep their interaction on course. This represents transitional (stage-three to stage-four) intervention. These asides invite the couple to fine tune their interaction process andor keep them attentive, sensitive, and responsive to emotionally focused interaction and to opportunities for attachment- or self-concept-focused acting and attending. On rare occasions, the therapist may offer proxy perspective in addition to an aside, as in stage three, but only as needed for the couple to access and understand their relationship at a deeper level than they are discerning
322 JOURNAL OF MARITAL AND FAMILY THERAPY July 2003
or articulating. Very rarely, the therapist will interrupt the enactment if the couple’s interaction escalates to destructive proportions and if it appears that they have dangerously neglected to track and exit their own negative process.
Martha: Samuel: Martha: Samuel: Martha:
Samuel:
Oooh, I just bristle when Raphael tries to control me. [Slides chair behind Martha, speaks only to her.] Strong feelings signal what? That he’s touched a raw nerve. But he doesn’t know what it is; I need to tell him. And . . . can you reframe his “control” in terms of attachment needs, or fears? Yes, I can see it. Okay. And deal with the problem as attachment, not “control.” I can do that. [Martha reengages with Raphael and continues the conversation.] [Slides his chair away and “busies” himself writing notes.]
After the episode enactment, the therapist facilitates Martha and Raphael in processing or evaluating their experience of the enactment. Postepisode evaluation is the primary stage-four intervention. Processing is through inductive dialogue, rather than didactic discourse (Butler & Bird, 2000). Thus again, the process shift of stage-four enactments is not only in terms of the intervention interval (speech-act vs. episode), but also in terms of the method of intervention (postenactment evaluation through inductive dialogue, rather than modeling or direct coaching during the enactment). As they evaluate/process the enactment, couples are encouraged to: (a) renew awareness of overarching relationship goals-secure attachment and helpful self-concept; (b) assess/evaluate the episode in light of these goals, beginning with affirmation of couple successes and following with sensitive critique; and (c) commit to mutual improvement.
As exemplified, the developmental progression of enactments is toward increasing couple self-reliance. Each incremental step by the couple is matched by enactment operations that, in terms of both structure and process, remove the therapist as a mediator. As the couple progress, clinical operations in the five stages of developmentally sequenced enactments are designed to respect their independence and defer to their increasingly self-reliant interaction process. Even as he withdraws from their relationship, though, Samuel offers collegial affirmation and encouragement.
Samuel: Raphael and Martha, I’m impressed with how well each of you took care of each other in that episode. But more important than my impressions are your own. Remember your goals when you came into therapy? Yes. I wanted my marriage back. I wanted to stop the pain every time we talked. Reflect on the episode you just completed. You were sharing your thoughts and feelings about some thorny issues. How well did your interaction conform to your goals? Commend each other for what you did well and for changes you’ve made. Give yourself personal credit, too. Then, make note of lapses, your own first. It’s often helpful to pay particular attention to moments when your emotions may have been pricked, or sparked. Those can be clues to exchanges that you might still be able to improve. Apologizing can be an important part, t o p rearming your relationship, building resiliency, and helping the next episode go better. [Samuel attends while Martha and Raphael discuss their enactment episode.]
Ruphael: Martha: Samuel:
During postenactment processing, Samuel facilitates Martha and Raphael in tracing or predicting both short- and long-term outcomes of their process, and then in identifying areas for change. As Martha and Raphael’s interaction process and outcome in stage four enactments increasingly demonstrates ability to (a) monitor and manage their own process, (b) address affect, attachment, and self-concept in positive ways, and (c) resolve problems, postenactment coaching and facilitating are eclipsed by mere affirmation, at which point the need for therapy itself has been eclipsed by the couple’s success.
Interaction proximity is unchanged between talk-turn and episode enactments-the couple interact directly in both-while emotional intensity and verbal autonomy increase significantly. Ideally, this increase
July 2003 JOURNAL OF MARITAL AND FAMILY THERAPY 323
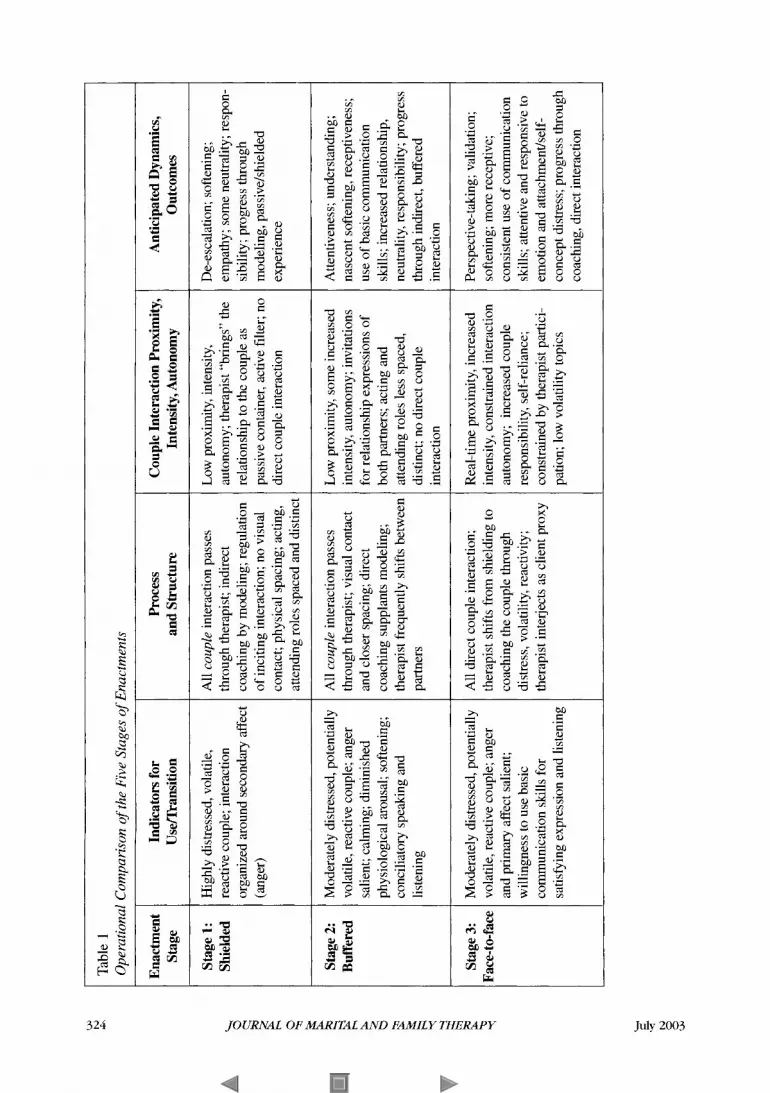
Table 1 Operational Comparison of the Five Stages of Enactments
All couple interaction passes through therapist; indirect coaching by modeling; regulation of inciting interaction; no visual contact; physical spacing; acting, attending roles spaced and distinct
All couple interaction passes through therapist; visual contact and closer spacing; direct coaching supplants modeling; therapist frequently shifts between partners
Enactment Stage
Low proximity, intensity, autonomy; therapist “brings” the relationship to the couple as passive container, active filter; no direct couple interaction
Low proximity, some increased intensity, autonomy; invitations for relationship expressions of both partners; acting and attending roles less spaced, distinct; no direct couple interaction
Stage 1: Shielded
All direct couple interaction; therapist shifts from shielding to coaching the couple through distress, volatility, reactivity; therapist interjects as client proxy
Stage 2: Buffered
Real-time proximity, increased intensity, constrained interaction autonomy; increased couple responsibility, self-reliance; constrained by therapist partici- pation; low volatility topics
Stage 3: pace-to-face
Indicators for Usernansition
Highly distressed, volatile, reactive couple; interaction organized around secondary affect (anger)
Moderately distressed, potentially volatile, reactive couple; anger salient; calming; diminished physiological arousal; softening; conciliatory speaking and listening
Moderately distressed, potentially volatile, reactive couple; anger and primary affect salient; willingness to use basic communication skills for satisfying expression and listening
Process and Structure
Couple Interaction Proximity, Intensity, Autonomy
Anticipated Dynamics, Outcomes
De-escalation; softening; empathy; some neutrality; respon- sibility; progress through modeling, passivekhielded experience
Attentiveness; understanding; nascent softening, receptiveness; use of basic communication skills; increased relationship, neutrality, responsibility; progress through indirect, buffered interaction
Perspective-taking; validation; softening; more receptive; consistent use of communication skills; attentive and responsive to emotion and attachmentkelf- concept distress; progress through coaching, direct interaction
N 0 0 w
324JO
UR
NA
L O
F M
AR
ITA
L A
ND
FA
MIL
Y T
HE
RA
PY
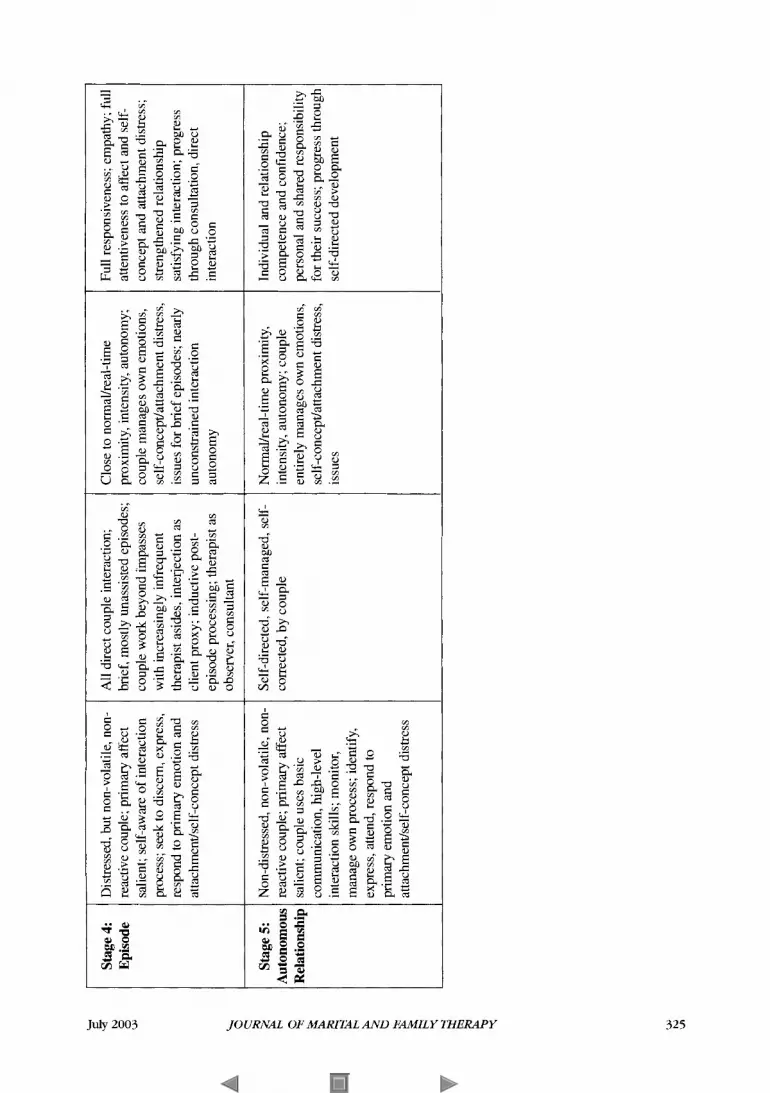
Stage 4: Episode
Stage 5: 4utonomous
Distressed, but non-volatile, non- reactive couple; primary affect salient; self-aware of interaction process; seek to discern, express, respond to primary emotion and attachmenuself-concept distress
Non-distressed, non-volatile, non- reactive couple; primary affect salient; couple uses basic communication, high-level interaction skills; monitor, manage own process; identify, express, attend, respond to primary emotion and attachmenuself-concept distress
All direct couple interaction; brief, mostly unassisted episodes; couple work beyond impasses with increasingly infrequent therapist asides, interjection as client proxy; inductive post- episode processing; therapist as observer, consultant
Self-directed, self-managed, self- corrected, by couple
Close to normalheal-time proximity, intensity, autonomy; couple manages own emotions, self-concept/attachment distress, issues for brief episodes; nearly unconstrained interaction autonomy
Normdreal-time proximity, intensity, autonomy; couple entirely manages own emotions, self-concept/attachment distress, issues
Full responsiveness; empathy; full attentiveness to affect and self- concept and attachment distress; strengthened relationship satisfying interaction; progress through consultation, direct interaction
Individual and relationship competence and confidence; personal and shared responsibility for their success; progress through self-directed development
W N 'U
JOU
RN
AL
OF
MA
RIT
AL
AN
D F
AM
ILY
TH
ER
AP
Y
in intensity and autonomy is to their advantage now, with their successes resulting in increased relationship mastery, confidence, and intimacy. Although they will certainly step on each other’s toes now and again, they catch themselves sooner, regain their composure and balance, and resume positive interaction. Specific problem resolution, strengthening of individual self-concept, and secure attachment are all anticipated outcomes of increasingly successful stage-four enactments. The couple are relationally self-reliant the majority of the time. The therapist-mediator thus removes himself completely from the couple’s relationship, inviting the end of therapy. “It is clear when the therapy process is complete, because the couple is able to exit from negative cycles in the session, to sustain emotional engagement, and to be accessible and responsive to each other” (Johnson & Greenberg, 1995, p. 130).
STAGE FIVE: AUTONOMOUS RELATIONSHIP ENACTMENTS
Autonomous relationship enactments signify enactments in which the couple’s self-reliant interaction has become consistently relationship enhancing and is satisfying to them in terms of both process and outcome. These couples are engaged with and by each other and their issues and simultaneously maintain a metaperspective on their interaction. Monitoring their interaction process, even while they wrestle with content, allows them to track and attend to affect and underlying attachment or self-concept issues, and to recognize and exit destructive sequences. In this manner, problem resolution and relationship healing and bonding are not derailed by the provocation of attachment or self-concept distress, with its attendant negative affect. Problems are resolved and the process of that resolution, as well as the resolution itself, confirms and strengthens each partner’s secure attachment and positive self-concept. Other observational indicators of readiness for relationship-level (Greenberg, 1986) enactment and therapy closure include demonstrations of ability to manage physiological arousal (soothe self and other, soften, become emotionally receptive); reduction of contingency in negative exchanges, accompanied by ability to exit escalating cycles of negative exchange; and a trend toward prioritizing emotionally focused and attachment- and self-concept-based expression, leading to deescalation and softening that catalyzes more successful subsequent problem solving.
In stage five, interaction proximity and emotional intensity are at that level characteristic of intimate relationships, and the couple is satisfied with the process and outcome of their autonomous interactions. Through enactment-based therapy, couples are anticipated to depart therapy with high hope, individual and relationship competence and confidence, and the satisfaction of mutual credit for their success.
INTEGRATING THE DEVELOPMENTAL MODEL WITH STATIC COMPONENT MODELS OF ENACTMENTS
The five-stage model provides a dynamic, developmental model for enactments over the course of therapy, linking structure and process to couples’ changing levels of relationship distress, interactional volatility, and emotional reactivity. We believe the five-stage model provides a developmental refinement essential to successful use of enactments over the entire course of therapy. Without the five-stage model, therapists are likely to either fail to use enactments at all in early or other volatile sessions of therapy or prematurely implement later-stage enactment process and structure, with potentially destructive outcomes for both the couple and for therapy itself, which again may lead to therapists foregoing enactments altogether and to couples becoming discouraged about therapy and their relationship. The five-stage model provides both an overarching focus for therapy process (relationship interaction) and outcome (relationship self-reliance), anchored fundamentally to positive emotional, attachment, and self-concept processes and experiences. We invite the investigation of enactments as a potential tool to invite, promote, and guide intimate relationship experiences between the very people whose softening, healing, positive self-worth, and secure attachment is, after all, the focus of therapy. Finally, we again caution that the exclusive basis for the development of the five-stage model has been couple therapy. We are thus not currently prepared to generalize its application to other relationship systems. Unique hierarchical and developmental differences among members of these systems, together with other dynamics unique to these systems (such as
326 JOURNAL OF MARITAL AND FAMILY THERAPY July 2003

relationship triangles), undoubtedly need to illuminate and inform the development of enactments suited to these relationship systems.
Contraindications to the Use of Enactments Finally, contraindications to the use of enactments need to be considered. We recommend, for example,
that enactments not be used in relationships significantly characterized and organized by power differences between partners (e.g., domestically violent, emotionally abusive, or economically exploitive relationships). In these situations, the assertiveness, emotional expression, and disclosure typically facilitated in enactments can compromise a disempowered partner. Therapist advocacy seems a more relevant therapist positioning in such situations. With these and other prudent stipulations, cautions, and issues considered and attended to, therapists may, we judge, effectively use enactments across the course of therapy by applying the adaptive, five-stage developmental model.
REFERENCES
Allen-Eckert, H., Fong, E., Nichols, M. P., Watson, N., & Liddle, H. A. (2001). Development of the Family Therapy Enactment
Butler, M. H., & Bird, M. H. (2000). Narrative and interactional process for preventing harmful struggle in therapy: An
Butler, M. H., & Harper, J. M. (1994). The divine triangle: God in the marital system of religious couples. Family Process, 33,
Cassidy, J., & Shaver, P. R. (Eds.). (1999). Handbook of attachment: Theory, research, and clinical applications. New York:
Davis, S. D., & Butler, M. H. (2002). Enacting relationships in M F T A conceptual and operational definition of on enactmmt.
Fowers, B. J . (2001). The limits of a technical concept of a good marriage: Exploring the role of virtue in communication skills.
Gottman J. M. (1993). A theory of marital dissolution and stability. Journal of Family Psychology, 7, 57-75. Gottman, J. M. (1999). The marriage clinic: A scientifically based marital therapy. New York Norton. Gottman, J. M., & Gottman, J. S. (1999). The marriage survival kit: A research-based marital therapy. In R. Berger & M. T.
Gottman, J. M.. & Levenson, R. W. (1992). Marital processes predictive of later dissolution: Behavior, physiology, and health.
Gottman, J. M., & Levenson, R. W. (1999a). Rebound from marital conflict and divorce prediction. Family Process, 38,
Gottman, J. M., & Levenson, R. W. (1999h). What predicts change in marital interaction over time? A study of alternative
Gottman, J. M., & Levenson, R. W. (2000). The timing of divorce: Predicting when a couple will divorce over a 14-year period.
Greenberg, L. S. (1986). Change process research. Journal of Consulting and Clinical Psychology, 54, 4-9. Johnson, S. M. (1996). The practice of emotionally ,focused marital therapy: Creating connection. Philadelphia, PA:
Johnson, S. M., & Greenberg, L. S. (1995). The emotionally focused approach to problems in adult attachment. In N. S.
Ken; M. E., & Bowen, M. (1988). Family evaluation. New York: Norton. Levenson, R. W., & Gottman, J. M. (1983). Marital interaction: Physiological linkage and affective exchange. Journal of
Nichols, M. P. & Fellenberg, S. (2000). The effective use of enactments in family therapy: A discovery-oriented process study.
Shields, C. G.. Sprenkle, D. H., & Constantine, J. A. (1991). Anatomy of an initial interview: The importance of joining and
Rating Scale. Family Process, 40, 469-478.
integrative empirical model. Journal of Marital and Family Therapy, 26, 123-142.
277-286.
Guilford.
Manuscript submitted for publication.
Journal of Marital and Family Therapy, 27, 321-340.
Hannah (Eds.), Preventive approaches in couples therapy (pp. 304-330). Philadelphia, PA: BrunnerMazel.
Journal of Personality and Social Psycholog)\ 63, 221-233.
287-292.
models. Family Process, 38, 143-158.
Journal of Marriage and the Family, 62, 737-745.
BrunnerMazel.
Jacobson &A. S. Gurman (Eds.), Clinical handbook of couple therapy (pp. 121-141). New York Guilford.
Personality and Social Psychology, 45, 587-597.
Journal of Marital and Family Therapy, 26, 143-152.
structuring skills. American Journal of Family Therapy, 19, 3-1 8.
July 2003 JOURNAL OF MARITAL AND FAMILY THERAPY 327