a review of the medication pathway in rural queensland, australia
TRANSCRIPT
A review of the medication pathway in ruralQueensland, AustraliaAmy Chen Wee Tana, Lynne Emmertona,c and Hendrika Laetitia Hattinghb,c
aSchool of Pharmacy, The University of Queensland, Brisbane, bSchool of Pharmacy, Griffith University, Gold Coast, Qld and cSchool of Pharmacy,Curtin University, Perth, WA, Australia
Keywordslegislation; pharmacist; pharmacy; policy;Quality Use of Medicines
CorrespondenceDr Lynne Emmerton, School of Pharmacy,Curtin University, GPO Box U1987, Perth, WA6845, Australia.E-mail: [email protected]
Received August 10, 2011Accepted January 15, 2012
doi: 10.1111/j.2042-7174.2012.00193.x
Abstract
Objectives It is well established that rural areas have compromised access to healthservices, including medication services. This paper reviews the practice develop-ments for rural health professionals in relation to medication processes, with a focuson regulatory provisions in Queensland, Australia, and a view to identifying oppor-tunities for enhanced pharmacy involvement.Methods Literature referring to ‘medication/medicine’, ‘rural/remote’, ‘Australia’and ‘pharmacy/pharmacist/pharmaceutical’ was identified via EBSCOhost, Ovid,Informit, Pubmed, Embase and The Cochrane Library. Australian Governmentreports and conference proceedings were sourced from relevant websites. Legisla-tive and policy documents reviewed include drugs and poisons legislation,the National Medicines Policy and the Australian Pharmaceutical Advisory Councilguidelines.Key findings The following developments enhance access to medication services inrural Queensland: (1) endorsement of various non-medical prescribers, (2) autho-risation of registered nurses, midwives, paramedics and Indigenous health workersto supply medications in sites without pharmacists, (3) skill-mixing of nursing staffin rural areas to ease medication administration tasks, (4) establishment ofpharmacist-mediated medication review services, (5) electronic transfer of medicalorders or prescriptions and (6) enhanced transfer of medication informationbetween metropolitan and rural, and public and private facilities.Conclusions This review identified a divide between medication access and medica-tion management services. Initiatives aiming to improve supply of (access to) medica-tions focus on scopes of practice and endorsements for non-pharmacist ruralhealthcare providers. Medication management remains the domain of pharmacists,and is less well addressed by current initiatives. Pharmacists’ involvement in ruralcommunities could be enhanced through tele-pharmacy, outreach support andsessional support.
Introduction
Medications are used for symptom relief,cure or managementof conditions, or as supplementation, particularly with theincreased burden of chronic diseases with the aging popula-tion. Yet, medications have the potential for unwantedeffects.[1] Therefore, it is important for healthcare providers toassist consumers or patients in managing their use of medica-tions. Medication management is a complex process thatinvolvesarangeof healthcareproviders.Figure 1illustrates the
nine major ‘steps’ identified in the medication management‘pathway’.[2]
In Australia, provision of medication services is compli-cated by the division of regulatory aspects of healthcare deliv-ery between the Commonwealth (national) Government andstate/territory governments. Currently, the CommonwealthGovernment oversees registration of healthcare practitioners(including scopes of practice), subsidy of pharmaceuticals
bs_bs_banner
International Journal of
Pharmacy PracticeInternational Journal of Pharmacy Practice 2012, 20, pp. 324–339
Review Article
© 2012 The Authors. IJPP © 2012 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2012, 20, pp. 324–339

under the Pharmaceuticals Benefits Scheme (PBS) and theimplementation of the National Medicines Policy.[3,4] On theother hand, the state/territory governments manage regula-tory aspects relevant to drugs and poisons and healthcareproviders not licensed under the national registration ofhealthcare practitioners (e.g. paramedics, Indigenous healthworkers).[4,5] The division of responsibilities and funding,including for public health services, between the Common-wealth and state/territory governments further complicatesthe delivery of healthcare services, including medicationservices.[4]
The medication pathway is further compromised in ruralareas, with consumers’ access to healthcare services restricteddue to limited health workforce capacity as well as geographi-cal, professional and social isolation.[4,6,7] This essentially chal-lenges the existing rural healthcare providers to consistentlyfulfil the ‘steps’ in the medication pathway and to providethe necessary medication support to consumers. This is ofconcern in rural areas where there is a lack of services offeringalternative or adjunct therapy, which could lead to increasedreliance on medication therapy. Rural healthcare alsodoes not provide a favourable environment to comply withkey objectives outlined in the National Medicines Policy,specifically (1) timely access to affordable medications,
(2) responsible and quality delivery of medication serviceswith best-practice regulatory systems in place and (3) QualityUse of Medicines (QUM), which encompasses judicious,appropriate, safe and efficacious use of medications.[3,4,6,7]
The dynamics of rural health have been shown to fosterchanging or extended clinical roles or skills and differentialhealthcare models to cope with rural health demands.[6]
However, few studies have explored the effect of rural loca-tion on the medication pathway in Australia and how ruralhealthcare providers are coping with the medication needsof consumers or patients. The majority of publishedstudies reviewing rural QUM processes have been limited toindividual professions (e.g. medical, nursing, pharmacy,Indigenous health), key tasks (e.g. prescribing, dispensing,administration, management) or specific medical categories(e.g. mental health, cardiovascular health, asthma, diabetes).
This paper reviews roles and practice initiatives relevant tothe medication pathway that are facilitated by current legisla-tion and policy. Specific objectives were to critique:1. rolesandpractice initiatives inruralQueensland,Australia,2. medication-related provisions according to Australian
(Commonwealth) and Queensland (state) legislation,3. how the legislation addresses or inhibits key objectives of
Australia’s National Medicines Policy,
Figure 1 Overview of the medication pathway. For the Regulation, see reference [5].
Amy Chen Wee Tan et al. 325
© 2012 The Authors. IJPP © 2012 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2012, 20, pp. 324–339

4. key areas where a medication support system appears tobe lacking, and potential delivery models for pharmacy(i.e. pharmacists and pharmacy support staff) to providesuch support to other rural healthcare providers.
Method
A review of the Health (Drugs and Poisons) Regulation 1996(Qld) [5] (here referred to as the Regulation) was conducted toexplore medication-related authorities and roles for relevanthealthcare providers in Queensland, as illustrated in Figure 1.This Regulation is subordinate legislation under the HealthAct 1937 (Qld) and contains detailed provisions regardingthe handling of medicines, referred to as ‘drugs’ in the Regula-tion. The review also referred to Commonwealth Govern-ment documents, including legislative provisions relevant tothe PBS, the National Medicines Policy[3] and the AustralianPharmaceutical Advisory Council (APAC) Guiding Principlesto Achieve Continuity in Medication Management.[8] Thereview refers to schedules (classifications) of medicines inAustralia. These are defined by the Standard for the UniformScheduling of Medicines and Poisons, and relevant schedulesare Schedule 2 (S2) or Pharmacy Medicines, Schedule 3 (S3)or Pharmacist Only Medicines, Schedule 4 (S4) or Prescrip-tion Medicines, and Schedule 8 (S8) or Controlled Drugs.[5]
This review of legislative and policy documents wassupplemented with a review of published and grey literature.Published articles, including research articles, review articlesand commentaries, were identified from EBSCOhost,Ovid, Informit, Pubmed, Embase and The Cochrane Librarydatabases. The search parameter was limited to abstractsto broaden potential search results. Search terms usedwere ‘medication/medicine’, ‘rural/remote’, ‘Australia’ and‘pharmacy/pharmacist/pharmaceutical’ (Figure 2). Uponidentifying relevant abstracts, the full papers were screenedfor relevance to healthcare providers’ role(s), medicationprocesses and healthcare provision models, with a particularfocus in rural Australian settings. Grey literature that wasnot available through the aforementioned databases, such asGovernment reports, research reports and conference pro-ceedings, were sourced online from the Australian Govern-ment Department of Health and Ageing, Medicare Australia,National Prescribing Service, the Pharmacy Guild of Austra-lia and the National Rural Health Conference. Online docu-ments were manually screened for their relevance to thereview by referring to the title, abstract or executive summaryand then the full report. A ‘snowballing’ technique was usedto locate further references from the identified papers.
Preference was given to English papers published between2000 and 2011, with the assumption that medication issuesreported prior to this period are not applicable to currenthealthcare settings and policy. Resources were excludedif they (1) were not within the focus of the search strategy,
(2) did not discuss development or implications in ruralareas, (3) focused on particular pharmacotherapy or amedical condition with little reference to rural practice orthe medication process involved (from Figure 1) and/or (4)described practices that were not applicable to the area ofinterest (e.g. irrelevant overseas model).
Results
The research coverage shown in Figure 2 suggests that there isoverall limited published research exploring medication pro-cesses in rural areas of Australia. A total of 204 citations rel-evant to the review were identified from sections D–J ofFigure 2, with 49 of those articles included in this review.The key findings relevant to medication initiatives, provisionsand support systems are categorised into key steps in themedication pathway as illustrated in Figure 1. This is followedwith subsequent reporting of pharmacy-mediated supportsystems and potential delivery models for pharmacy.
The medication pathway
Decision to treat and prescribe
The initial step involves prescribers making informed deci-sions on appropriate treatment for patients.[2]
Figure 2 Numbers of references identified in the literature search.
326 Medication pathway in rural Australia
© 2012 The Authors. IJPP © 2012 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2012, 20, pp. 324–339

The recent expansion of prescribing authority to a rangeof health practitioners aimed to provide continuity of, andtimely access to, pharmaceutical therapy or medications.Since 2005, the Regulation has been amended to include pro-visions to endorse a number of non-medical prescribers:surgical podiatrists, nurse practitioners (NPs), physician’sassistants (PAs),‘Therapeutically Endorsed’ optometrists and‘Eligible Midwives’.[5] The details of these endorsements aresummarised in Table 1.[9–13]
In addition to medical doctors and dentists, ‘Therapeuti-cally Endorsed’ (known as ‘authorised’) optometrists, NPsand Eligible Midwives also have PBS prescribing authority,which further improves consumers’ access to affordablemedications. This allows the healthcare providers to prescribe
a specific list of Australian government-subsidised medicationsrelevant to their profession as of 1 January 2008 (authorisedoptometrists) or 1 November 2010 (NPs and midwives).[9,14]
It has been claimed that certain inconsistencies existbetween Commonwealth (national) Government PBS autho-risations and state- or territory-based legislation. Theseinconsistencies exist because jurisdictions need to addressspecific local needs.[4] However, the peculiarities of the stateand territory legislation and (national) PBS provisions interms of prescribing can cause confusion among healthcareproviders who are trained in the legislation of their homestate or territory. The confusion is compounded by thenationalisation of health practitioner registration (July2010), enabling health professionals to practise interstate.[4]
Table 1 Recently endorsed prescribers
Prescriber Provisions in Queensland/notes
‘TherapeuticallyEndorsed’optometrists
In 2005, the Regulation was amended to allow optometrists to obtain, possess, administer, supply or prescribe restricteddrugs (S4 medications) in Queensland, according to the conditions specified in the Ocular Therapeutics Protocol.[9] Tobe eligible for this authorisation or endorsement, optometrists are required to complete an approved programme ofstudy/certificate course of training or have successfully completed an assessment in ocular therapeutics approved bythe Optometry Board of Australia.[5,9]
Surgical podiatrists Queensland’s Regulation was amended in 2006 to allow surgical podiatrists to prescribe, supply or administer accordingto a specific formulary containing limited S4 medications and one S8 medication (oxycodone).[5,10] This is provided thesurgical podiatrist hold Fellowship with the Australasian College of Podiatric Surgeons or have completed one of theaccreditation pathways for ‘endorsement for scheduled medicines’ as outlined by the Podiatry Board of Australia.[10]
The inconsistencies in terms of authorisations for podiatrists and surgical podiatrists have led to the introduction ofvarious endorsements by the Board.[10]
Nurse practitioners(NPs)
NPs were introduced into Queensland in 2006 and are now integrated state-wide in a range of healthcare settings.[11] Tobe eligible for an NP endorsement, a registered nurse is required to demonstrate ‘advanced nursing practice in a clinicalleadership role in the area of practice’ within the past 5 years and complete the requisite Master’s qualificationapproved by the Nursing and Midwifery Board of Australia.[11] The role of an NP includes prescribing, ordering ofpathology or radiology, providing clinics for disease management and issuing of Workers’ Compensation certificates.[11]
The NP role is anticipated to assist medical workforce cope with the increasing healthcare demand, ease access tohealth services which are unavailable to certain communities or groups of interest as well as fulfill gaps and scarcitywithin the rural healthcare services.[11] In Queensland, the prescribing authority of an NP is restricted to within the DrugTherapy Protocol of Nurse Practitioners, applicable to both rural and metropolitan settings.[11]
Eligible midwives In 2007, midwives under general registration are authorised to administer or supply prescription medicines (S4 or S8medications) under the condition of Drug Therapy Protocol, regardless of area of practice in Queensland.[5]
As of July 2010, midwives can apply for endorsement as an Eligible Midwife, which allows the midwife to apply for aMedicare provider number to provide relevant health services. Requirements to be endorsed as an Eligible Midwifeinclude equivalent of 3 years of practice experience full-time post initial registration as a midwife and successfulcompletion of an accredited/approved programme of study determined by the Nursing and Midwifery Board ofAustralia.[12] Eligible midwives who are authorised to prescribe scheduled medicines in accordance with state andterritory legislation may apply for endorsement for scheduled medicines.[12] As of 2011, eligible midwives are allowedto prescribe restricted drugs (S4 medications) in Queensland.[5]
Physician’s assistants(PAs) (role notrecognised by theAustralian HealthPractitionerRegulation Agency)
The PA role was originally developed in the USA in 1960s, utilising trained military medics returning from active duty inrural areas.[13] The Regulation was amended to accommodate the pilot PA project in rural Queensland between May2009 and May 2010, with five US-trained PAs recruited into Queensland Health.[13] The defined role of five PAsrecruited varied depending on location of practice and type of care involved, such as emergency, specialist ward orprimary care. In general, the role involved assisting medical doctors in assessing, diagnosing and treating patients, asPAs are required to work under the supervision of a medical doctor.[5,13] Benefits reported included sharing of case-load,streamlining patients, easing of medical workforce and the flexibility of the role to adapt to gaps in service deliverywithin the relevant area of practice.[13] Some of the barriers to establishing the role included reducing the opportunitiesof advanced nursing to expand, competition with junior doctors in terms of learning and employment, and limitedprescribing authority.[13]
Amy Chen Wee Tan et al. 327
© 2012 The Authors. IJPP © 2012 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2012, 20, pp. 324–339

In rural Queensland, NPs, registered nurses (RNs), ruraland isolated practice RNs, midwives, Indigenous healthworkers and isolated practice area paramedics are allowedto initiate administration or supply of medication using adrug therapy protocol (DTP), when prescribers, specificallymedical doctors, PAs and NPs, are not available (Table 2).[5,15]
The DTP is a document containing a list of drugs that havebeen approved for use in rural hospitals or isolated practiceareas by endorsed/authorised healthcare providers, and statesthe conditions and restrictions under which the drugs can beused.[5,15] The Primary Clinical Care Manual[15] provides clearand concise clinical care guidelines in accordance with theRegulation for rural healthcare providers to implement theDTP.
Although prescribing roles have been established for arange of healthcare providers, pharmacists in Australia cur-rently do not have prescribing endorsements for PrescriptionMedicines, even in rural areas. The recently released Austra-lian Pharmacy Council (APC) report from the Remote RuralPharmacists Project has identified that legislation inhibitspharmacists by not allowing them to prescribe medicationsfor the management of chronic disease.[4] The APC reporttherefore recommended that remote pharmacists be autho-rised to prescribe by protocol.[4] While the debate about,and development of, pharmacists’ prescribing is stillunderway,[16,17] the Fifth Community Pharmacy Agreementbetween the Department of Health and Ageing and the Phar-macy Guild of Australia has recommended a ‘medicationcontinuance protocol’ for community pharmacists to initiatecontinuing therapy (i.e. supply based on previous prescrip-tion or medication order) of a 1-month or single-pack supplyof medication, provided that the patient has been stabilisedon the medication therapy.[17] A similar model (the Medica-tion Maintenance model) was proposed in 2007 for aged-caresettings.[16] While this framework is developed for both met-ropolitan and rural setting, this is anticipated to temporarilyease access to medications when or where prescribers areunavailable and the consumer is in short supply. It is foreseenthat the implementation of this initiative would attract PBSsubsidy, which would require changes to the PBS. It wouldalso require the current drugs and poisons legislation (theRegulation in Queensland) to be amended to allow pharma-cists to implement the protocol without an existing or validprescription.
Record of medication order or prescription
This step involves information transfer from the prescriber tothe subsequent healthcare providers involved in the medica-tion pathway, adhering to the legal prescribing and prescrip-tion requirements within the jurisdiction of practice.[2]
In addition to the extended prescribing rights, provisionsin the Regulation also allow some flexibility to facilitate
prescribing and dispensing of medications, which is appli-cable to both metropolitan and rural areas. The Regulationallows for verbal or facsimile orders from prescribers, pro-vided that a written order is received by the dispensingpharmacy within 7 days (sections 81, 97, 192).[5] In recogni-tion of technology, electronic prescribing has been a recentestablishment in the hospital setting to enhance informa-tion transfer and reduce errors on prescriptions.[1,18,19] Inte-gration of electronic prescribing in hospital, communityand aged-care settings has been trialled, and national imple-mentation, in line with the development of national elec-tronic health records, is currently under review.[20] However,the implementation of electronic prescribing requires train-ing for healthcare staff, funding, technological resources andcompatibility with the existing medication recording sys-tem,[1,19,20] limiting the potential for expansion in rural areas.Relevant exploratory research for implementation in ruralareas is lacking.
Review of medication order or prescription
It is crucial to review medication orders or prescriptionsfor compliance with legislative or PBS requirements andclinical appropriateness prior to supply or administration ofthe medication, a task commonly undertaken by pharma-cists. The Regulation specifies that pharmacists must followQuality Standards during dispensing of medications to con-sumers (section 4A).[5] The standards that apply are the Phar-maceutical Society of Australia (PSA) Professional PracticeStandards.[21] Specifically, the pharmacist should review themedication order by considering the patient’s medicationhistory, drug interactions or appropriateness of dosingregimen when dispensing the prescribed medication.[2,21,22]
Studies have shown that the support from a pharmacist inreviewing prescribing decisions is perceived by prescribers asvaluable.[19,23–25]
Electronic transfer of prescriptions (under development inAustralia) has integrated computer-based clinical decision-support systems for checking of the patient’s medicationhistory for interactions, allergies and duplicate ordering, toenhance appropriate prescribing and patient safety.[1,8,19,26]
Although studies exploring such systems have been limited tocertain settings or institutions,[1,26] the implementation ofnationwide electronic health records will allow a consistentand complete set of patients’ medication records to improveprovision of healthcare.[20] While the benefits of supportsystems in assisting with prescribing have been reported,some of the shortcomings identified in the literature wereblocking features for privacy, excessive or inappropriate alert-ing systems and variability or inconsistencies across prod-ucts.[1,19,20] Although research and evidence is lacking in termsof the superiority of computerised systems as opposed topharmacotherapeutic knowledge of an actual healthcare
328 Medication pathway in rural Australia
© 2012 The Authors. IJPP © 2012 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2012, 20, pp. 324–339

provider, such as a pharmacist, adjunct use of such supportsystems has the potential to improve the process of reviewingmedication orders.
No reports were identified involving non-pharmacists’review of prescribing decisions in a rural setting, althoughnursing staff were reported to perform occasional clarifica-tion of medication orders.[30]
Medication supply
The previous step generally leads to the dispensing and/orextemporaneous compounding by a pharmacist.[2] Inrural areas, where pharmacists are not available, other health-care providers (Figure 1) are endorsed to ‘supply’ medica-tions.[5,6,31] Rural-specific provisions are summarised in
Table 2.[27–29] These healthcare providers do not need toconform to the quality standards under which pharmacistspractise, although they are bound by the requirements inthe Regulation for labelling and recording of medicationsissued.[5,32] Research has highlighted that these healthcareproviders require support systems amidst the scarcity ofpharmacists and lack of technological support in rural areas,particularly in terms of complying with legislative require-ments, clinical drug knowledge and provision of medicationinformation.[4,31,33–36] While medical doctors are endorsed todispense or supply medications under the Regulation, theymay only provide PBS medications as ‘a convenient and effi-cient pharmaceutical service’ in a rural location where there isno pharmacist-approved location under the National HealthAct 1953 (Cth).[32]
Table 2 Specific provisions in accordance to the Regulation for rural healthcare providers
Authorised entity Provisions in Queensland/notes
Registered nurses(RNs)
Under general conditions, an RN may initiate and administer an S2 or S3 medication; and administer an S4 or S8medication under an oral or written instruction from a medical doctor, physician’s assistant (PA) or nursepractitioner (NP).[5,15]
An RN practising in a rural hospital may supply an S2, S3, S4 or S8 medication under an oral or written instruction from amedical doctor, PA or NP, provided the rural hospital does not employ a pharmacist or the pharmacist is absent from thehospital at the time the medication(s) is/are supplied.[5,15]
An RN practising in an isolated practice area may supply an S2, S3, S4 or S8 medication under an oral or written instructionfrom a medical doctor, PA or NP.[5,15]
Midwives Under general conditions, a midwife may initiate and administer an S2 or S3.A midwife may supply an S2 or S3 medication in a rural hospital or an isolated practice area.In addition to authorisations granted to an RN, a midwife may supply or administer an S4 or S8 medication under the drug
therapy protocol (DTP).[5,15]
Rural and isolatedpractice registerednurse (RIPRN)
A RIPRN is an RN whose registration is endorsed under the national Health Practitioner Regulation National Law (Cth) asbeing qualified to administer or supply certain approved medications for practising nursing in a rural or isolatedpractice area.[5]
In Queensland, in addition to authorisations granted to an RN, a RIPRN practising in an isolated practice area or ruralhospital may supply or administer an S4 or S8 medication under the DTP.[5,15]
Indigenous healthworker (IHW)
An IHW is a person who holds a Diploma of Health Science Aboriginal and Torres Strait Islander Primary Health Care(Generalist) or certified equivalent qualification and has successfully completed the North Queensland Rural HealthTraining Unit Isolated Practice Health (Drugs and Poisons) Regulation 1996 Course or a certified equivalent course oftraining for the accreditation of Registered Nurses for practice in an isolated practice area.[5]
An IHW practicing in an Aboriginal and Torres Strait Islander community in an isolated practice area may administer S8 andsupply or administer an S2, S3 or S4 medication under the DTP.[5,15]
Isolated practice areaparamedic (IPAP)
An IPAP is an ambulance officer who has successfully completed the training course Graduate Certificate of Rural andRemote Paramedic Practice, and is classified by the Queensland Ambulance Service as a paramedic 3, 3(ECP) or 4.[5]
An IPAP working in an isolated practice area may supply or administer an S2, S3, S4 or S8 medication, either under an oralor written instruction from a medical doctor, PA or NP, or under the DTP.[5,15]
Royal Flying DoctorService (RFDS)medical chests
The RFDS medical chests are available and located at RFDS outposts in recognition of the need to manage acute clinicalconditions in remote areas.[27–29] In Queensland, these chests contain medications to be supplied by a person in charge ofan RFDS outpost under the oral or written instruction of a medical doctor, PA or NP.[5,27] The medication supplied can beself-administered or administered by the person in charge of the RFDS outpost.[5] Conditions include that the chest is‘assigned to a person living and working in the same location for greater than six months, and the location is greaterthan 80 km from the nearest health service’.[27,28].
Authorised premises Authorised premises in Queensland, such as convenience or grocery stores, can obtain ‘general poison license’ tosell S2 medications. This is provided the premise is located at a place more than 25 km by road from a pharmacy(Sections 19, 231).[5]
Amy Chen Wee Tan et al. 329
© 2012 The Authors. IJPP © 2012 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2012, 20, pp. 324–339

The Regulation allows pharmacists to supply 3 days’ worthof Prescription Medicines without a prescription under theEmergency Supply provision (section 194). The pharmacist,however, is required to ascertain that an emergency exists,that the patient has used the medication previously and thepatient is in need of that medication.[5] This provisionis applicable to both metropolitan and rural settings inQueensland. Unlike some other rural healthcare providers(Figure 1), pharmacists do not have additional endorsementsin rural areas. Under the national PBS arrangements,however, Regulation 24 of the National Health (Pharmaceu-tical Benefits) Regulations 1960 (Cth) allows pharmacists tosupply original and repeat supplies of prescription medica-tions at the same time if the doctor has endorsed the prescrip-tion with ‘Regulation 24’. This is on the condition that (1)the maximum PBS quantity per supply is insufficient for thepatient’s treatment, (2) the patient lives in a remote areawhere medications access is limited and (3) the patient hasgreat difficulties in obtaining the medications on separateoccasions.[9]
The APC report identified that the legislation concerningpharmacy premises and the allocation of PBS providernumbers inhibits pharmacists from dispensing in, and claim-ing PBS benefits from, non-approved premises such asremote clinics with pharmacy outstations. In order to supplyPBS medications, pharmacies, medical practitioners and hos-pital authorities are required to seek approval from Medicare,and this is specified under sections 90, 92 and 94 of theNational Health Act 1953 (Cth), respectively.[9,14] Under thePBS, pharmacists may only dispense and claim Pharmaceuti-cal Benefits from a pharmacy or dispensary located at pre-mises with a Medicare Australia approval number.[4] Thisincreases the need to rely on non-pharmacists to ‘supply’medications in rural areas. In the Northern Territory, anexemption was approved under the Schedule 8 of HealthPractitioners Act 2004 (NT), allowing pharmacists to providepharmacy services at remote Aboriginal clinics to improveaccess to both medications and medication consultation.[4]
The APC report recommended such exemption to be consid-ered in other states, including Queensland.[4]
It is well established that maintaining Indigenoushealth imposes a challenge to healthcare delivery.[36,37] Aspecial arrangement under Section 100 (S100) of theNational Health Act 1953 (Cth) was introduced in 1999 by theAustralian Government to supply free medications to, andimprove medications access at, Aboriginal Health Services(AHSs). This allows for the AHSs to order bulk supplies ofPBS medications from a participating community pharmacy,and the AHSs then supply the medications to Indigenousand non-Indigenous patients treated at the AHSs.[4,28,37,38] Anexpansion of the S100 provisions to include all AHSs, regard-less of location or remoteness, has been proposed to furtherincrease medication access to all Indigenous people.[36,37]
However, the S100 scheme facilitates medication accesswithout providing opportunity for medication consultationbetween a pharmacist (bulk supplier) and the patient, as themedication supply task is now undertaken by a health workerat the AHS.[4,36] While there are developments to improveQUM in Indigenous communities, such as the PharmacyGuild’s ‘S100 Pharmacy Support Allowance’ and NationalPrescribing Service education sessions, the call forpharmacist-facilitated QUM education sessions, medicationconsultation in AHSs and pharmacist-AHS health workerliaison are restricted by inadequate funding, logistical issuesand scarcity of pharmacists in rural areas.[4,28,36,37,39]
Provision of medication information
Provision of consumer-specific information about the medi-cation supplied forms a significant component of QUM. Thisis usually incorporated in a pharmacist’s dispensing processand is detailed in the PSA Professional Practice Standards,specifying that the pharmacist should work with the con-sumer ‘to provide tailored verbal and written information toensure that consumers have sufficient knowledge and under-standing of their medications and therapeutic devices tofacilitate safe and effective use’.[21] A common written infor-mation tool is Consumer Medicine Information (or CMI)which provides brand-specific medication information pro-duced by the relevant pharmaceutical company, in accordancewith the Therapeutic Goods Regulations.[8,21] Pharmacists arerequired to provide Consumer Medicine Information leafletsunder certain circumstances, for example when the medica-tion is first provided to a consumer.[40] While non-pharmacistswith medication responsibilities do not have to conform tothe professional standards or guidelines outlined for pharma-cists, the APAC guidelines[8] and the PSA’s position statementDispensing by Other Health Professionals[32] suggest all health-care providers have the responsibility to provide sufficientinformation to patients and/or their carers to support them inmanaging their medications.
Numerous reports[7,23,26,41,42] have demonstrated that theinvolvement of a pharmacist in providing medication consul-tation can influence patients’ self-management of their medi-cations. Reports have also shown that nurses were able toprovide basic medication information, including the action ofmedications and common side effects, although the informa-tion provided was not as comprehensive as that provided bypharmacists.[30,31] This is because nursing staff, with specificreference to rural nursing staff, often supply and/or adminis-ter medications, raising the need for them to have pharmaco-therapeutic knowledge when monitoring patients’ responseto medications to ensure patients’ safety.[30,31]
It should be noted that the rural legislative provisions inFigure 1 and Table 2 improve timely access to medicationsand expand the range of healthcare providers involved in the
330 Medication pathway in rural Australia
© 2012 The Authors. IJPP © 2012 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2012, 20, pp. 324–339

medication pathway in rural areas. While the increase inaccess addresses one aim of QUM, there is a sub-optimal levelof assistance for rural consumers to manage their medica-tions, particularly when quality standards for dispensingare not applied and adequate and appropriate medicationinformation is not provided. Reports have shown that ruralsole pharmacists experience high workloads from dispensingand pharmacy management, impeding their involvementin medication consultations.[4,7,28,43,44] In addition, non-pharmacists involved in medication supply have limitedscope of practice in the provision of medication informationand medication management.[4,31,36] Training packages devel-oped to up-skill non-pharmacists in their medication knowl-edge have been limited due to the costs of time and travel,high turnover of rural staff and scarcity of rural pharmaciststo train these healthcare providers.[4,33,36] This reiterates theneed to provide medication support systems (ideallypharmacist-mediated) for both rural pharmacists and non-pharmacists to improve and optimise QUM in rural areas.
Distribution and storage of medications
Once issued, the medications are distributed to consumers orcarers for storage at home, or to healthcare delivery areaswithin an aged-care facility or hospital.[2] The process of dis-tribution and handling of medications in healthcare facilitiesis important, due to the potential involvement of severalhealthcare workers in the facility before the medicationreaches the patient. Apart from specific provisions in theRegulation regarding healthcare providers authorised toobtain or possess medications with the higher levels ofrestrictions, and storage specifications surrounding Con-trolled Drugs,[5] the literature search did not identify anyAustralian studies specifically referring to ordering anddistribution of medications in rural areas.
Care should be taken, particularly for perishable medica-tions, to preserve efficacy of medications, as lack of refrigera-tion, lack of knowledge about storage conditions and long-distance transportation without appropriate temperaturecontrol are some of the reported issues in rural Austra-lia.[4,36,39] Pharmacists have a role in providing medicationinformation, as discussed in the previous section, on han-dling and storage of medications to consumers and ruralhealthcare providers.
Administration of medications
This step involves medication selection, preparation andadministration (by the consumer, carer or healthcare pro-vider).[2] Rural-specific provisions are summarised in Table 2.
The nursing profession in Australia comprises a hierarchydepending on qualification of the nurse, and thus his/herresponsibilities and authority. Under the Regulation, RNs and
midwives are authorised to administer an S2 or S3 medica-tion without a medical order, but require a medical doctor’s,PA’s or NP’s instructions to administer an S4 or S8 medica-tion.[5,15] A medication-endorsed enrolled nurse (EEN) is ableto administer an S2, S3, S4 or S8 medication under the delega-tion and supervision of an RN, midwife, dentist or medicaldoctor. An EEN may not delegate any other person to admin-ister medications or initiate or supply any medications. Whileall enrolled nurses now graduate with medication endorse-ment, practising enrolled nurses without this endorsementmay not administer medications, initiate any medications orhelp patients take dispensed medication.[45,46] Unlicensednursing staff including assistants-in-nursing and personalcarers may not administer medications.[5,46]
Despite the apparent abundance of nursing career paths,nursing staff in rural areas are challenged with higher work-load and lower staffing levels. This results in the healthcareproviders practising in a skill-mix setting, and either stretch-ing their roles or undertaking tasks beyond their scope ofpractice and/or legal authority.[35,45,47] A further layer of com-plexity is that the defined tasks of these nursing roles, includ-ing clinical roles and medication roles, can differ betweenjurisdictions and between workplaces.[4,45] This, again, cancause confusion between healthcare providers practisinginterstate, given the recent nationalisation of health practitio-ner registration. For example, legislation changes in Tasmaniain 2009 allowed personal carers employed in aged-care facili-ties to administer medications, provided they have completeda Certificate IV in Aged Care.[48] Existing policies in Queen-sland do not allow personal carers to administer medication,but rather provide for physical assistance to patients in medi-cation administration.[5] The extent of ‘assisting’ with medi-cations may vary between facilities and between public andprivate settings.While legislation and workplace protocols setboundaries to promote safe practice, it can also inhibit theprovision of the required services in rural areas, where health-care workforce is limited.[6,35] Some reports have drawn atten-tion to the blurring of nursing roles, often out of necessity inpractice, and raised concerns about medication administra-tion, clinical monitoring of patients’ responses and medica-tion safety.[31,35,45,47]
Of concern is research that has indicated that medicationadministration errors and near-miss incidents in the hospitalsetting are common.[19] Another area of concern is that medi-cation dosage forms are often modified, for example crushedand mixed into food or beverage, to aid medication adminis-tration, and nursing staff may not be aware of the potentialclinical effect of these alterations.[49,50] Pharmacists play amajor role in providing drug information in relation to medi-cation administration and educating healthcare providersabout problems resulting from altering medication dosageforms.[19,30,49,50] Pharmacists can also be involved in extempo-raneous preparations to compound or manufacture dosage
Amy Chen Wee Tan et al. 331
© 2012 The Authors. IJPP © 2012 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2012, 20, pp. 324–339

forms that are not commercially available and to ensure safeadministration of the medication.[19,50] This, again, raises theimportance of medication support systems for rural health-care providers in non-pharmacist sites, as highlighted abovein previous steps.
Monitor for response
Following administration or supply of medication,healthcare providers, carers and patients themselves havethe responsibility to monitor the patient’s response (positiveand/or negative) to a given medication.[2] Generally, anymedications administered by a healthcare provider (e.g.nursing staff) are closely monitored for effectiveness andadverse reactions at the facility where the administrationoccurred.[30,35] The extent of such monitoring may differbetween healthcare providers and between workplaces.
Pharmacist-mediated medication review services havebeen demonstrated as valuable in enhancing the managementof patients’ medications.[23,25,26,41,51] Established servicesinclude Home Medicines Reviews (HMRs) and ResidentialMedication Management Reviews (RMMRs), which allowaccredited pharmacists to provide detailed medication reviewservices to patients using multiple medications at the patient’shome (HMR) or aged-care facility (RMMR).[23,28,41] This notonly incorporates monitoring of patients’ responses to theirmedication regimen, but also involves other components ofthe medication pathway such as review of prescribing, provi-sion of medication information to the patient, transfer ofinformation/recommendation(s) to the general practitioner(GP), and finally, the GP developing a management planbased on the pharmacist’s recommendation(s).[23,25,41] Asimilar medication review service for post-discharge patientshas been proposed and the hospital referral pathway is cur-rently being explored.[19,26]
Available studies on pharmacist-mediated medicationreview services were focused in metropolitan areas; remu-neration, workforce issues and ‘territorial issues’ with localGPs have been cited as barriers to the service.[1,19,26,52] To assistin better collaboration between GPs and accredited pharma-cists, the Fifth Community Pharmacy Agreement has devel-oped a number of changes to HMR and RMMR services, forimplementation from October 2011. These include allowingdirect HMR referral from GP to accredited pharmacist(instead of via the community pharmacy as an intermediatechannel) and imposing that RMMR has to be collaborative(involving the participation of both the GP and accreditedpharmacist in the review process).[53,54] Medication reviewsled by medical doctors or nurses have also been explored.While disease management is the key focus in the studies,ambiguous results have been reported relating to manage-ment of adverse drug events or medication managementplans.[26]
Barriers to the implementation of pharmacist-mediatedmedication review services in rural areas have been reported,including travel costs for training and limited remunerationfor travel to patients’ homes or aged-care facilities.[28] Inaddition, the need for a GP’s referral challenges the provi-sion of such services in rural areas where access to a GP isoften limited.[28] The inability to engage an accredited phar-macist in a timely matter has also been reported.[19] Thiswarrants further research to extend referral pathway to ruralhealthcare providers (e.g. nurses) and to explore remunera-tion framework or career pathway for accredited pharma-cists in rural areas.
Transfer of verified information
The transfer of medication information to relevanthealthcare providers is crucial to ensure optimal ongoingcare and therapy for the patient.[2] Research suggests thatmedication errors in this step are common, as changes topatients’ medication regimens are often not communicatedeffectively between the hospital, specialist, GP, pharmacist,other healthcare provider(s), carer(s) and patients them-selves.[1,8,18,19,30,42,52,55,56] One such case highlighted the confu-sion of a rural patient about his medications, which resultedfrom ineffective information transfer and the inability for hisvarious healthcare providers to provide comprehensivecare.[55] Information transfer is crucial during each transitionin a patient’s care. A role has been proposed for pharmaciststo act as a liaison between healthcare providers to facilitatemedication reconciliation and information transfer betweenhealthcare providers;[19,21,52,56] more research should be under-taken to explore this role to develop an appropriate frame-work to be implemented in rural areas.
Some studies have explored information transfer andmedication reconciliation processes (on admission andon discharge) between hospitals and the primary care set-ting.[18,19,42,56] Prior to the PBS Public Hospital PharmaceuticalReforms, 3–7 days’ worth of discharge medications were sup-plied by Queensland public hospitals. During this period, thedischarged patient was responsible to visit a GP to obtain newprescriptions for continuing therapy.[42] This was particularlychallenging for patients in areas where timely access to GPservices was lacking, resulting in patients potentially missingdoses of medication(s).
Public Hospital Pharmaceutical Reforms adopted by somestates (including Queensland) aim to improve the continuitybetween hospital and community sectors in relation to cogni-tive medication services and discharge medication supply, asoutlined in the APAC guidelines.[8,42,56] Under this arrange-ment, public hospitals are able to dispense 1 month’s worth ofdischarge medications under the PBS, extending the time fora patient to access a GP for repeat prescriptions. Ideally, aclinical pharmacist’s services should also be included under
332 Medication pathway in rural Australia
© 2012 The Authors. IJPP © 2012 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2012, 20, pp. 324–339

this arrangement to promote QUM via medication reconcili-ation and information provision.[8,22,35,42,43] However, with thelimited pharmacy/dispensing services in rural hospitals, themajority of PBS prescriptions generated by these hospitals aredispensed by community pharmacies with no medicationssupplied from the hospital on discharge.[42] Limitationsto this arrangement include patients not being able to havetheir prescriptions filled immediately upon discharge, whenlimited by access to pharmacy services in rural areas or mobil-ity issues. In addition, community pharmacists dispensingthe medication do not have access to hospital medical recordsto review the patient’s medication history.[42,52] More researchis warranted to explore this issue in rural areas. As describedin the previous section, post-discharge hospital pharmacistmedication review services have been proposed to enhancecontinuity of care and medication management, although theincorporation of this service within the current medicationsupply and management arrangements is unknown.
In both cases above, patients are relied on to communicatethe information from the hospital to the primary care setting,and this has been shown to be less effective compared toinformation transfer by a healthcare provider.[18,52] There hasbeen the development of state-wide software such as theEnterprise-wide Liaison Medication System (eLMS) to facili-tate medication reconciliation processes in Queenslandpublic hospitals and to the primary care setting.[57] eLMS is aweb-based application that produces a discharge medicationrecord (DMR) that contains medication information forpatients discharged from public hospitals in Queensland.Information on a DMR includes new, current and ceasedmedications, as well as written directions on how to take themedications. The DMR is also provided to the patient’selected community health practitioners (e.g. GPs, commu-nity pharmacists) to enhance the process of medicationreconciliation and to facilitate exchange of medication infor-mation between health practitioners.[57] Medical doctors,nursing staff and pharmacists are often involved in facilitat-ing information transfer; however, the implementation ofmedication reconciliation processes and the processing ofDMRs are traditionally undertaken by pharmacists.[18,19,56]
There is a lack of research exploring such processes in ruralareas, particularly in areas without pharmacy services. Thereare similar systems in place in other states, and a nationalshared electronic medication record is under development toease medication information communication.[1,6,19,20]
Pharmacy-mediated support
The majority of rural healthcare providers are sole practitio-ners with a lack of professional support from their ownprofession and other healthcare providers.[4,35] Given thecomplexity of the medication pathway, medication-relatedproblems and errors may occur at any stage. The Australian
Commission on Safety and Quality in Health Care indeedidentified that 2–3% of Australian hospital admissionsare related to problems with medications (approximately140 000 annual admissions), originating either in the com-munity or in hospital, and costing about AUD$380 millionper year in the public hospital system alone.[1] Researchershave argued that pharmacists have extensive knowledge of,and expertise in, medications, and should play a major roleto promote QUM, ensure safe medication practices andsupport rural healthcare providers throughout the medica-tion pathway.[26,35,44]
A key problem, however, is a recognised shortage ofpharmacists and pharmacy services in rural areas, limitingthe potential for pharmacists to enhance medication ser-vices.[7,44,57] It has been reported that over half (75 of 116) ofQueensland’s public hospitals have no pharmacist on site,and less than one-quarter of these non-pharmacist sites (18of 75) have limited outreach pharmacist support.[57] Manyrural outpatient clinics and healthcare centres are serviced bysole nurses or health workers, who also undertake medicationsupply and stock control in these facilities. These facilitiesoften do not have the capacity to employ pharmacists, or arenot within the vicinity of a pharmacy service, and hencereceive minimal input from pharmacists.[7,34,57]
About one-third of Queensland’s public hospitals that doemploy pharmacists (15 of 41) are reportedly serviced by solepharmacists.[57] It has been postulated that cost-shifting forpublic hospitals from state-based to Commonwealth-basedmanagement, as proposed as part of major PBS Public Hospi-tal Pharmaceutical Reforms in Australia, would improvefunding and therefore clinical pharmacy services in rural orregional hospitals.[43] Workforce studies have confirmedaging of the pharmacy workforce and high rates of sole phar-macy practice in rural areas, in both hospital and communitysettings.[7,28] Some of the contributing factors for the low ratesof younger pharmacists in rural areas include the perceivedhigher workload and shortfalls in support (e.g. mentoringand training) systems in rural areas.[4,28,58]
The limited pharmacy workforce restricts the provision ofextended medication services or enhanced pharmacy ser-vices, meaning that rural pharmacists are often focused oncore services such as dispensing and drug distribution, as wellas pharmacy supervision and management.[4,28,43,44,59,60] SomeAustralian studies reviewed and/or trialled several deliverymodels to enhance medication support to rural healthcareproviders, including pharmacists. This includes remotesupport via video technology, outreach support, sessionalsupport and involvement of pharmacy support staff, asdescribed below, to compensate for the pharmacy workforceshortage in rural areas. The literature search did not identifyreports of established models or framework to supportextended delivery of medication services by pharmacists inrural areas.
Amy Chen Wee Tan et al. 333
© 2012 The Authors. IJPP © 2012 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2012, 20, pp. 324–339

Remote support via technology
The use of video-conferencing in tele-pharmacy has beenestablished in the USA to provide pharmacy services remotelyby a pharmacist to a patient or healthcare provider in a ruralcommunity, with the aim of improving medication servicesin rural areas.[4,51] The initial tele-pharmacy concept inQueensland utilises medical practitioners to provide diagno-sis and dispense medications, without the support of a phar-macist, over the telephone to patients located at an outpost inremote areas, where a ‘medical chest’ is located (Table 2).[27,61]
Tele-pharmacy utilising video technology and the medica-tion expertise of a pharmacist is under development, andtrials conducted in Queensland and Victoria (Table 3, section3.1)[51,57,61,62] may have significant impact if the nationalbroadband communications network is strengthened in ruralareas. Benefits reported for trials of such tele-pharmacysystem include capacity for supervision of pharmacy supportstaff (e.g. technicians), patient counselling, case-conferencingand associated recommendations, mentoring of ruralpharmacists, distance dispensing and distance medicationreviews.[51,61] In Victoria, tele-pharmacy introduces greaterpotential for pharmacists’ involvement and added value tothe ‘pharmacy depot’ system, in which medications aredispensed by, or under the supervision of, a pharmacist at apharmacy and then transported to a rural depot for collectionby the patients.[4] Barriers to implementation of tele-pharmacy in Australia include costs, training, location issuesand the need to comply with legislation.[51,61]
Outreach services
In an attempt to provide medication assistance to ruralhealth services, pharmacists have been commissionedto visit non-pharmacist sites, as described in Table 3(section 3.2).[30,33,39,43,63] The majority focused on providingmedication-related educational sessions and health promo-tion to local healthcare providers and consumers. Inconsis-tency in terms of the frequency of visits and the communitiescoveredbytheoutreachsupportresultedfromruralworkforceshortages, funding issues for pharmacists and/or logistical dif-ficulties.[28,33,39]
Sessional services (shared employment)
Shared employment across multiple health sectors (e.g. hos-pital, general practice, aged care) is a model commonly uti-lised in rural settings to maximise the existing healthcareworkforce. One example of a health professional working ona sessional basis is rural GPs who are often also the medicaldoctors employed at their local hospital.[13,23] Similarly, alliedhealthcare providers who practise privately are often alsoemployed by the public sector or provide sessional private
services in several towns within their district(s) of practice toexpand allied health services within the rural region.[4]
Studies illustrated in Table 3 (section 3.3)[7,25,52] provide someexamples of pharmacy-based sessional services; however,there is no formal establishment of such employment modelsacross rural areas of Queensland. Further research into thesessional model for pharmacists, including a remunerationpathway, is warranted as an option to enhance medicationservices with the existing rural pharmacy workforce.
Pharmacy support staff
Enhancement of pharmacy support staff (pharmacy assis-tants and technicians) capacity and roles in medicationsupply and delivery systems may enable the available phar-macists to provide extended services such as medicationmanagement or clinical services, both in hospital and com-munity settings.[22,28,43,60,64] The Regulation allows pharmacystaff some involvement in the provision of non-prescriptionmedications (S2 and S3 medications), assembling/labellingmedications, data entry and daily stock control, under thedirection and personal supervision of a pharmacist.[5,21,60]
This requirement for supervision is the limiting factor in theutilisation of pharmacy support staff in rural areas, althougha recent change in the Regulation, allowing ‘supervision’ viatechnology, such as video-conferencing,[5] warrants investiga-tion. Other limiting factors include lack of a career pathway,liability issues and variations in workplace roles and train-ing.[22] In certain countries, for example New Zealand, theUSA and the UK, there are formalised frameworks and legis-lation in place to allow pharmacy technicians to be moreactively involved in the entire dispensing process under theauthorisation of the supervising pharmacist.[22,65] Similarextended roles should be explored in Australia, specifically inareas lacking pharmacists or with limited pharmacy work-force capacity, which would also require amendment of legis-lation, standardised training procedures and development ofprofessional standards.
Discussion
This review drew on roles and practice initiatives in ruralareas to improve the provision of medication services alongthe medication pathway (Figure 1). The review focused onthe legal framework and medication provisions of Common-wealth (national) and Queensland (state). The review alsoidentified the value of pharmacists and potential pharmacy-mediated support systems to further enhance QUM in ruralcommunities. The strength of this review lies in the review ofboth published literature identified through databases andunpublished (grey) literature identified through other onlinesources. The combination ensured a comprehensive review ofthe topics amidst the lack of research in provision of medica-
334 Medication pathway in rural Australia
© 2012 The Authors. IJPP © 2012 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2012, 20, pp. 324–339
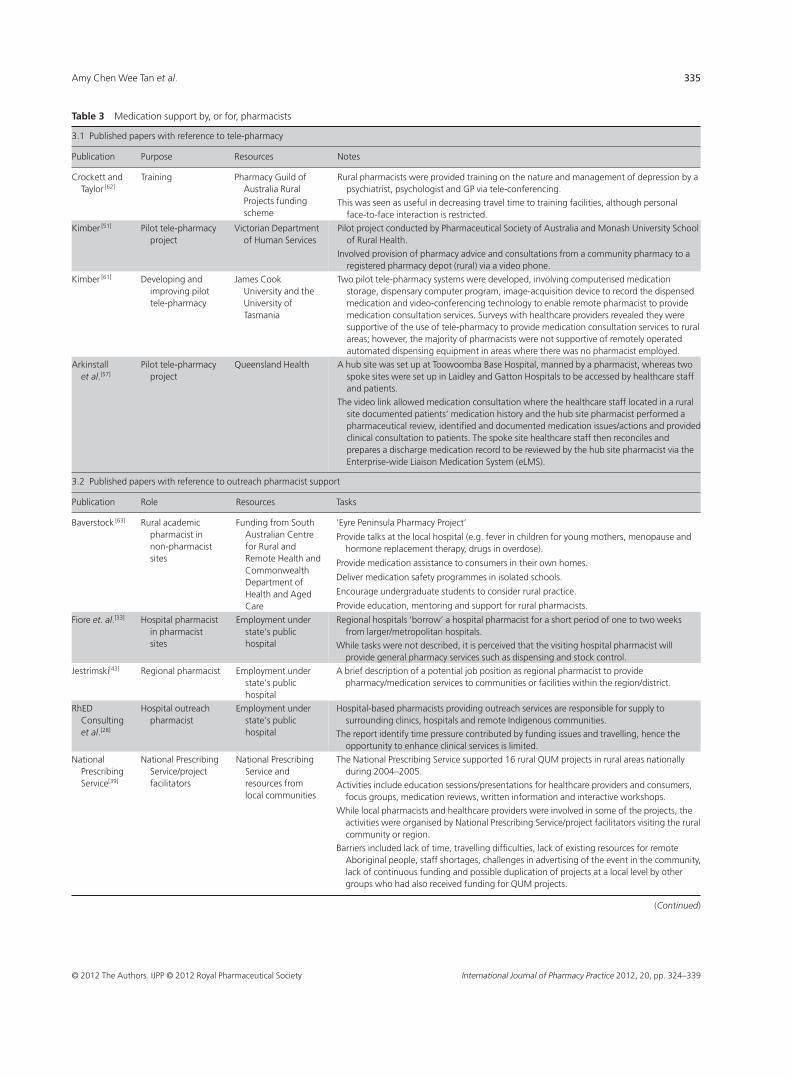
Table 3 Medication support by, or for, pharmacists
3.1 Published papers with reference to tele-pharmacy
Publication Purpose Resources Notes
Crockett andTaylor [62]
Training Pharmacy Guild ofAustralia RuralProjects fundingscheme
Rural pharmacists were provided training on the nature and management of depression by apsychiatrist, psychologist and GP via tele-conferencing.
This was seen as useful in decreasing travel time to training facilities, although personalface-to-face interaction is restricted.
Kimber [51] Pilot tele-pharmacyproject
Victorian Departmentof Human Services
Pilot project conducted by Pharmaceutical Society of Australia and Monash University Schoolof Rural Health.
Involved provision of pharmacy advice and consultations from a community pharmacy to aregistered pharmacy depot (rural) via a video phone.
Kimber [61] Developing andimproving pilottele-pharmacy
James CookUniversity and theUniversity ofTasmania
Two pilot tele-pharmacy systems were developed, involving computerised medicationstorage, dispensary computer program, image-acquisition device to record the dispensedmedication and video-conferencing technology to enable remote pharmacist to providemedication consultation services. Surveys with healthcare providers revealed they weresupportive of the use of tele-pharmacy to provide medication consultation services to ruralareas; however, the majority of pharmacists were not supportive of remotely operatedautomated dispensing equipment in areas where there was no pharmacist employed.
Arkinstallet al.[57]
Pilot tele-pharmacyproject
Queensland Health A hub site was set up at Toowoomba Base Hospital, manned by a pharmacist, whereas twospoke sites were set up in Laidley and Gatton Hospitals to be accessed by healthcare staffand patients.
The video link allowed medication consultation where the healthcare staff located in a ruralsite documented patients’ medication history and the hub site pharmacist performed apharmaceutical review, identified and documented medication issues/actions and providedclinical consultation to patients. The spoke site healthcare staff then reconciles andprepares a discharge medication record to be reviewed by the hub site pharmacist via theEnterprise-wide Liaison Medication System (eLMS).
3.2 Published papers with reference to outreach pharmacist support
Publication Role Resources Tasks
Baverstock [63] Rural academicpharmacist innon-pharmacistsites
Funding from SouthAustralian Centrefor Rural andRemote Health andCommonwealthDepartment ofHealth and AgedCare
‘Eyre Peninsula Pharmacy Project’
Provide talks at the local hospital (e.g. fever in children for young mothers, menopause andhormone replacement therapy, drugs in overdose).
Provide medication assistance to consumers in their own homes.
Deliver medication safety programmes in isolated schools.
Encourage undergraduate students to consider rural practice.
Provide education, mentoring and support for rural pharmacists.
Fiore et. al.[33] Hospital pharmacistin pharmacistsites
Employment understate’s publichospital
Regional hospitals ‘borrow’ a hospital pharmacist for a short period of one to two weeksfrom larger/metropolitan hospitals.
While tasks were not described, it is perceived that the visiting hospital pharmacist willprovide general pharmacy services such as dispensing and stock control.
Jestrimski[43] Regional pharmacist Employment understate’s publichospital
A brief description of a potential job position as regional pharmacist to providepharmacy/medication services to communities or facilities within the region/district.
RhEDConsultinget al.[28]
Hospital outreachpharmacist
Employment understate’s publichospital
Hospital-based pharmacists providing outreach services are responsible for supply tosurrounding clinics, hospitals and remote Indigenous communities.
The report identify time pressure contributed by funding issues and travelling, hence theopportunity to enhance clinical services is limited.
NationalPrescribingService[39]
National PrescribingService/projectfacilitators
National PrescribingService andresources fromlocal communities
The National Prescribing Service supported 16 rural QUM projects in rural areas nationallyduring 2004–2005.
Activities include education sessions/presentations for healthcare providers and consumers,focus groups, medication reviews, written information and interactive workshops.
While local pharmacists and healthcare providers were involved in some of the projects, theactivities were organised by National Prescribing Service/project facilitators visiting the ruralcommunity or region.
Barriers included lack of time, travelling difficulties, lack of existing resources for remoteAboriginal people, staff shortages, challenges in advertising of the event in the community,lack of continuous funding and possible duplication of projects at a local level by othergroups who had also received funding for QUM projects.
(Continued)
Amy Chen Wee Tan et al. 335
© 2012 The Authors. IJPP © 2012 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2012, 20, pp. 324–339

tion services in rural areas. One of the limitations of thisreview is the focus on roles, practice and legislative develop-ments in the State of Queensland, Australia, and focused onmedication issues. It should be noted that the legal frame-work and certain state-specific initiatives (e.g. eLMS) differbetween states and territories of Australia. However, theoverall concept of improving QUM should still be applicablenationally and internationally. Apart from role, practice andlegislative developments, there is also considerable effortto address rural health workforce shortages, which is notexplored in detail in this review. These efforts include theestablishment of rural clinical schools, rural placements,scholarships, financial incentives and locum services to copewith rural healthcare demands.[6,28]
Identified reports have shown that in order to enhanceconsumers’ continuing access to medications in rural areas,potentially valuable solutions appear to involve:
• increasing the range of healthcare providers authorised toprescribe or supply medications,
• broadening the scope of practice of healthcare providers toinclude medication tasks, and/or
• improving prescription and medication informationtransfer.It should be noted that extending the role or scope of prac-
tice could increase the workload of existing healthcare pro-viders, considering the workforce shortage in rural areas.[6,35]
In any extension of any healthcare provider’s role, consider-ation should be given to define the scope of practice, deter-mine financial and professional support, and ensure qualityassurance and ongoing training, all which could be morechallenging in rural areas.[6,31,35] Medication support mecha-nisms, ideally from pharmacists, should also be consideredto promote safe and quality practices, specifically when the
medication roles are not within traditional training of therural healthcare providers.
This paper has also identified potential steps of the medica-tion pathway where pharmacy support could enhance QUMand medication management. Alternative service deliverymodels could be potentially explored to expand pharmacyworkforce capacity in rural areas to provide medicationsupport and/or consultation services in rural communities.Models worthy of further exploration include tele-pharmacyutilising video technology, outreach services by visiting phar-macists, sessional services via shared employment of a phar-macist and role extension for pharmacy support staff. Thedevelopment of medication management service deliverymodels can be complicated by the logistics of conductingtrials in a healthcare environment which is at the mercy offunding changes and often a high turnover of rural staff, andis likely to be located some distance from a research cen-tre.[6,23,43] The challenge is raised to researchers to engage witha rural community, and commit to an intensive programmeof research that identifies the community’s healthcare needsand potential solutions to assist or support existing ruralhealthcare providers, and subsequently establish a sustain-able delivery model that can be applied to the majority of, ifnot all, rural areas.
Conclusions
It is well established that timely and quality access to medica-tion services remains a significant and growing problem inrural communities.While current initiatives involve roles andpractice developments of rural healthcare providers, there ispotential to further enhance medication services in ruralareas. The review has also shown the value of pharmacy along
Table 3 (Continued)
3.3 Published papers with reference to shared employment for pharmacists
Publication Setting Resources Tasks
Sunderlandet al.[7]
Shared-carebetween twocommunitypharmacies
Employmentbetween twocommunitypharmacies
The author described a pharmacist servicing two towns via shared-employment. Thepharmacist was reported to service one town in the mornings and the other town in theafternoons.
This was seen as a potential solution to increase pharmacy services in rural areas that do notoffer sufficient workload capacity to financially support a full-time pharmacy service.
Bonner andWatson[25]
Shared-carebetween medicalpractice andhospital
Regional networkof GPs
A clinical pharmacist (hospital-based) provided sessional medication review services at a localmedical practice.
The pharmacist-GP collaboration took four 1-h sessions over a period of 2 months.
This collaboration have been further developed into Home Medicines Review (HMR) andResidential Medication Management Review (RMMR) services; however, such sharedemployment can also be seen as a potential solution to increase medication support to GPsin rural areas.
Vuong andMarriott [52]
Shared-carebetween hospitaland communitypharmacy
Part-time salarypackages
While no job description has been provided, the author identified a pharmacist who workedpart-time in both hospital and community pharmacy.
This can be seen as a partial workforce solution to enhance both community and hospitalpharmacy services in areas lacking pharmacists.
336 Medication pathway in rural Australia
© 2012 The Authors. IJPP © 2012 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2012, 20, pp. 324–339

the medication pathway, and there is potential to betterinvolve pharmacy to provide support mechanisms and/ormedication consultation services.
Declarations
Conflict of interest
The Authors declare that they have no conflicts of interest todisclose.
Funding
This work was supported by the Pharmacists Board of Queen-sland Pharmacy College Trust (grant number 2010000973).
Acknowledgements
The authors gratefully acknowledge technical assistance fromVictoria Jarvis, BPharm MPS.
References
1. Australian Council for Safety andQuality in Health Care. SecondNational Report on Patient Safety –Improving Medication Safety. Can-berra: Australian Council for Safetyand Quality in Health Care, 2002.
2. Stowasser D et al. Understanding themedicines management pathway. JPharm Pract Res 2004; 34: 293–296.
3. Australian Government Department ofHealth and Ageing. The National Strat-egy for Quality Use of Medicines. Can-berra: Commonwealth of Australia,2002.
4. Australian Pharmacy Council. Remoterural pharmacists project. 2009. www.pharmacycouncil.org.au/PDF/Rural%20Remote%20Final%20Report%20June%2009.pdf (accessed 12 July 2011).
5. Health (Drugs and Poisons) Regulation1996 (Qld).
6. Productivity Commission. Australia’sHealth Workforce. Research Report.Canberra: Productivity Commission,2005.
7. Sunderland V et al. A comparativeevaluation of phamacy services insingle and no pharmacy towns. Aust NZ Health Policy 2006; 3: 8–17.
8. Australian Pharmaceutical AdvisoryCouncil. Guiding Principles to AchieveContinuity in Medication Management.Canberra: Commonwealth of Austra-lia, 2005.
9. Australian Government Department ofHealth and Ageing. Health professional– explanatory notes. Commonwealthof Australia. 2011. www.pbs.gov.au/info/healthpro/explanatory-notes/(accessed 20 January 2011).
10. Borthwick AM et al. Non-medicalprescribing in Australasia and the UK:the case of podiatry. J Foot Ankle Res2010; 3: 1–10.
11. Queensland Health. Clinical Gover-nance for Nurse Practitioners in Queen-sland: A Guide. Brisbane: The State ofQueensland, 2011.
12. Australian Health Practitioner Regula-tion Agency. Guidelines for educationrequirements for recognition as Eli-gible Midwives and accreditation stan-dards for programs of study leading toendorsement for scheduled medicinesfor Eligible Midwives. Nursing andMidwifery Board of Australia; 2011.www.nursingmidwiferyboard.gov.au/Accreditation.aspx (accessed 22 Febru-ary 2012).
13. Kurti L et al. Physician’s assistants: aworkforce solution for Australia? Aust JPrim Health 2011; 17: 23–28.
14. National Health Act 1953 (Cth).15. Queensland Health and the Royal
Flying Doctor Service (QueenslandSection).PrimaryClinicalCareManual,6th edn. Cairns: Queensland Healthand the Royal Flying Doctor Service,2009.
16. Emmerton L et al. Reforming thequality use of medicines in Australianaged care facilities: a new pharmacypractice model. Int J Pharm Pract 2007;15: 331–337.
17. Pharmacy Guild of Australia. TheRoadmap – The Strategic Direction forCommunity Pharmacy. Barton: Phar-macy Guild of Australia, 2010.
18. Pierce D, Fraser G. An investigationof medication information transferand application in aged care facilitiesin an Australian rural setting. Rural
Remote Health 2009; 9: 1090. www.rrh.org.au/articles/showarticlenew.asp?ArticleID=1090 (accessed 22 Feb-ruary 2012).
19. Semple SJ, Roughead E. Medicationsafety in acute care in Australia: whereare we now? Part 2: a review of strate-gies and activities for improvingmedication safety 2002–2008. Aust N ZHealth Policy 2009; 6: 24.
20. Australian Government Department ofHealth and Ageing. MediConnect FieldTest Evaluation Findings [Final Report].Canberra: Commonwealth of Austra-lia, 2005.
21. Pharmaceutical Society of Australia.Professional Practice Standards, 4th edn.Deakin: Pharmaceutical Society ofAustralia, 2010.
22. Carroll M et al. Potential support rolesfor pharmacy technicians in provisionof clinical pharmacy services. J PharmPract Res 2003; 33: 186–193.
23. Graffen M et al. Quality use of medi-cines in the rural ambulant elderly:a pilot study. Rural Remote Health2004; 4: 184. www.rrh.org.au/articles/showarticlenew.asp?ArticleID=184(accessed 22 February 2012).
24. Cutts C, Tett SE. Influences on doctors’prescribing: is geographical remotenessa factor? Aust J Rural Health 2003; 11:124–130.
25. Bonner C, Watson PG. Therapeutichousekeeping: a case study involvingcollaboration between a medical prac-titioner and a clinical pharmacist in amedication management program forelderly patients. J Soc Admin Pharm2001; 18: 97–102.
26. Easton K et al. Medication Safety in theCommunity: A Review of the Literature.
Amy Chen Wee Tan et al. 337
© 2012 The Authors. IJPP © 2012 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2012, 20, pp. 324–339

Sydney: National Prescribing Service,2009.
27. Margolis S, Ypinazar VA. Tele-pharmacy in remote medical practice:theRoyalFlyingDoctorServiceMedicalChest Program. Rural Remote Health2008; 8: 937. www.rrh.org.au/articles/showarticlenew.asp?ArticleID=937(accessed 22 February 2012).
28. RhED Consulting et al. Research totrack the rural pharmacy workforce andidentify the role that rural programs haveon retention of the rural pharmacy work-force. Final report. Canberra: PharmacyGuild of Australia, 2010.
29. Royal Flying Doctor Service. Medicalchests. Royal Flying Doctor Service;2011. www.flyingdoctor.org.au/Health-Services/Remote-Services/Medical-Chests/ (accessed 18 February 2011).
30. Manias E et al. Graduate nurses’ com-munication with health professionalswhen managing patients’ medications.J Clin Nurs 2005; 14: 354–362.
31. Hegney D et al. Patient educationand consumer medicine information: astudy of provision by Queensland ruraland remote are Registered Nurses. JClin Nurs 2004; 14: 855–862.
32. Pharmaceutical Society of Australia.Dispensing by other health profession-als. 2006. www.psa.org.au/download/policies/dispensing-by-other-health-professionals.pdf (accessed 22 Feb-ruary 2012).
33. Fiore S et al. Support needs ofsupply nurses in rural and remoteQueensland. Aust J Rural Health 2005;13: 10–13.
34. Craig M. Development of Career Path-ways for Indigenous People, to ProvideMedication Support Services in RemoteHealth Service Settings. Alice Springs:Centre for Remote Health, 2009.
35. Fogarty G, McKeon CM. Patient safetyduring medication administration:the influence of organizational andindividual variables on unsafe workpractices and medication errors. Ergon2006; 49: 444–456.
36. Stoneman J,Taylor SJ. Improving accessto medicines in urban, regional andrural Aboriginal communities – isexpansion of Section 100 the answer?Rural Remote Health 2007; 7: 738. www.
rrh.org.au/articles/showarticlenew.asp?ArticleID=738 (accessed 22 Febru-ary 2012).
37. Stoneman J, Taylor SJ. Pharmacist’sviews on Indigenous health: is theremore that can be done? Rural RemoteHealth 2007; 7: 743. www.rrh.org.au/articles/showarticlenew.asp?ArticleID=743 (accessed 22 February2012).
38. Couzos S. PBS medications – improv-ing access for Aboriginal and TorresStrait Islander peoples. Aust Fam Physi-cian 2005; 34: 841–844.
39. National Prescribing Service. RuralProject Schemes 2004-05: Summaryof Activity and Evaluation Reports.Sydney: National Prescribing Service,2006.
40. Pharmaceutical Society of Australia.Consumer medicine informationand the pharmacist – guidelines forpharmacists. 2007. www.psa.org.au/supporting-practice/guidelines(accessed 22 February 2012).
41. Khalil H. A review of pharmacist rec-ommendations in an aged care facility.Aust J Prim Health 2011; 17: 35–39.
42. Couch G et al. Continuity of medica-tion supply and provision of patientinformation on discharge. J PharmPract Res 2007; 37: 210–213.
43. JestrimskiK.Managementchallenges inlarge rural hospital pharmacy depart-ments.Aust JHospPharm1999;29:202–205.
44. Wibowo Y et al. Analysis of enhancedpharmacy services in rural communitypharmacies in Western Australia. RuralRemote Health 2010; 10: 1400. www.rrh.org.au/articles/showarticlenew.asp?ArticleID=1400 (accessed 22 Feb-ruary 2012).
45. Blay N, Donoghue J. Enrolled nurseskill extension: metropolitan myth orrural reality? Aust J Adv Nurs 2007; 24:38–42.
46. Queensland Health. Medication man-agement – administration, handling,storage and supply of medication (Too-woomba and Darling Downs HealthService District). Brisbane: Queen-sland Health, 2008.
47. Hegney D et al. The Administration andSupply of Controlled and Restricted
Medications by Queensland Rural andRemote Nurses. Project report. Too-woomba: University of SouthernQueensland, 2003.
48. Anon. Keep RNs in aged care. Aust NursJ 2010; 17: 6.
49. Barnes L et al. Making sure theresidents get their tablets: medicationadministration in care homes for olderpeople. Nurs Health Manag Policy 2006;56: 190–199.
50. Nissen L et al. Solid medication dosageform modification at the bedside andin the pharmacy of Queensland hospi-tals. J Pharm Pract Res 2009; 39: 129–134.
51. Kimber M. Telepharmacy-enablingtechnology to provide quality phar-macy services in rural and remote com-munities. J Pharm Pract Res 2006; 36:128–133.
52. Vuong T, Marriott JL. Potential roleof the community liaison pharmacist:stakeholder views. Int J Pharm 2006; 14:135–148.
53. Australian Government Depart-ment of Health and Ageing. Residen-tial medication management review(RMMR) Factsheet. Pharmacy Guildof Australia. 2011. www.5cpa.com.au/5CPA/Information_and_Resources/Information+and+Resources.page?(accessed 20 July 2011).
54. Australian Government Departmentof Health and Ageing. Home medicinesreview (HMR) Factsheet. PharmacyGuild of Australia. 2011. www.5cpa.com.au/5CPA/Information_and_Resources/Information+and+Resources.page? (accessed 20 July2011).
55. Smith JD. The case of Brian – a realitycheck on the safe use of medicines inrural Australia. Aust Pharm 2010; 29:835–838.
56. O’Leary K et al. Survey of implementa-tion levels and pharmacy requirementsfor the continuum of quality use ofmedicines between hospital and com-munity. J Pharm Pract Res 2003; 33:93–100.
57. Arkinstall R et al. Supporting ruralnurses in safe and appropriatemedication management. Associationof Queensland Nurse Leaders; 2007.
338 Medication pathway in rural Australia
© 2012 The Authors. IJPP © 2012 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2012, 20, pp. 324–339

www.aqnl.org.au/default.asp?PageID=79&n=2007+Conference+Speakers+Papers (accessed 15 March 2011).
58. Australian Government Departmentof Health and Ageing. Report on theAudit of Health Workforce in Rural andRegional Australia. Canberra: Com-monwealth of Australia, 2008.
59. Harding A et al. Factors affecting therecruitment and retention of pharma-cists to practice sites in rural andremote areas of New South Wales: aqualitative study. Aust J Rural Health2006; 14: 214–218.
60. Leversha A et al. Ward pharmacy tech-nicians assist clinical pharmacists withadmissions. Aust J Hosp Pharm 2001;31: 130–132.
61. Kimber M. The application of telephar-macy as an enabling technology tofacilitate the provision of quality phar-maceutical services to rural and remoteareas of Australia. PhD thesis, JamesCook University, Townsville, 2007.
62. Crockett J, Taylor S. Rural pharmacistperceptions of a project assessing theirrole in the management of depression.Aust J Rural Health 2009; 17: 236–243.
63. Baverstock K. Rural academic pharma-cists – working with rural and remotecommunities. Aust Health Consum2001; 1: 33–34.
64. Seaton SM, Adams RC. Impact of ahospital pharmacy technician facili-tated medication delivery system. JPharm Pract Res 2010; 40: 199–202.
65. Kinrade W. Workforce and CareerOptions for Pharmacy Assistants. Finalreport. Barton: Pharmacy Guild of
Australia; 2004.
Amy Chen Wee Tan et al. 339
© 2012 The Authors. IJPP © 2012 Royal Pharmaceutical Society International Journal of Pharmacy Practice 2012, 20, pp. 324–339