a rapid, fully automated, molecular-based assay accurately analyzes sentinel lymph nodes for the...
TRANSCRIPT

ORIGINAL ARTICLES
A Rapid, Fully Automated, Molecular-Based AssayAccurately Analyzes Sentinel Lymph Nodes for the
Presence of Metastatic Breast Cancer
Steven J. Hughes, MD,* Liqiang Xi, PhD,* Siva Raja, MD, PhD,* William Gooding, MS,†David J. Cole, MD,§ William E. Gillanders, MD,§ Keidi Mikhitarian, MD,§
Kenneth McCarty, MD, PhD,‡ Susan Silver, MD,‡ Jesus Ching, PhD,� William McMillan, PhD,�James D. Luketich, MD,* and Tony E. Godfrey, PhD*
Objective: To develop a fully automated, rapid, molecular-basedassay that accurately and objectively evaluates sentinel lymph nodes(SLN) from breast cancer patients.Summary Background Data: Intraoperative analysis for the pres-ence of metastatic cancer in SLNs from breast cancer patients lackssensitivity. Even with immunohistochemical staining (IHC) andtime-consuming review, alarming discordance in the interpretationof SLN has been observed.Methods: A total of 43 potential markers were evaluated for theability to accurately characterize lymph node specimens from breastcancer patients as compared with complete histologic analysis in-cluding IHC. Selected markers then underwent external validationon 90 independent SLN specimens using rapid, multiplex quantita-tive reverse transcription-polymerase chain reaction (QRT-PCR)assays. Finally, 18 SLNs were analyzed using a completely auto-mated RNA isolation, reverse transcription, and quantitative PCRinstrument (GeneXpert).Results: Following analysis of potential markers, promising mark-ers were evaluated to establish relative level of expression cutoffvalues that maximized classification accuracy. A validation set of 90SLNs from breast cancer patients was prospectively characterizedusing 4 markers individually or in combinations, and the resultscompared with histologic analysis. A 2-marker assay was found tobe 97.8% accurate (94% sensitive, 100% specific) compared withhistologic analysis. The fully automated GeneXpert instrument pro-duced comparable and reproducible results in less than 35 minutes.Conclusions: A rapid, fully automated QRT-PCR assay definitivelycharacterizes breast cancer SLN with accuracy equal to conventional
pathology. This approach is superior to intraoperative SLN analysisand can provide standardized, objective results to assist in patho-logic diagnosis.
(Ann Surg 2006;243: 389–398)
In breast cancer and other malignancies, involvement ofregional lymph nodes is a strong prognostic indicator and
greatly influences staging and clinical management.1–4 Onebenefit from the implementation of sentinel lymph nodebiopsy (SLNB) techniques is the identification of metastaticfoci of cancer in 10% to 15% of patients that would have beenpreviously staged as node-negative (pN0) by conventio-nal methods.5,6 This improved sensitivity is attributed to boththe addition of immunohistochemical staining (IHC) and toan increase in sampling volume.5,6 Many of these additionalpositive nodes contain only micrometastatic foci of tumor.However, the clinical significance of micrometastatic diseaseidentified by SLNB techniques is highly controversial.7–11
Nonetheless, SLNB techniques are now widely used in breastcancer and melanoma and are being applied with increasingfrequency to other tumors, including colorectal, oropharyn-geal, prostate, lung, and other solid organ cancers.12–15
Another clear advantage to the SLNB technique is thatin the majority of breast cancer patients, SLNB safely avoidsaxillary lymph node dissection (ALND) and the associatedmorbidity when the SLN is negative for metastatic disease.16
However, rapid, frozen-section analysis of SLN for metasta-sis is only 50% to 70% sensitive for the detection of metas-tasis compared with the permanent histologic sections andIHC of the same lymph node,17,18 and complete analysis ofthe SLNB specimen currently requires extensive preparationand time-consuming review.8 Even in experienced hands, 10%of SLNB specimens are later found to contain metastases.19 Asa result, these patients have required a second surgical procedureto complete the ALND. This is clearly an undesirable algorithmfor the patient, the healthcare provider, and the healthcare payer,and this dilemma has contributed to a new controversy; if theSLNB is positive, does a completion ALND confer a therapeutic
From the Departments of *Surgery, †Biostatistics, and ‡Pathology, HillmanCancer Center, University of Pittsburgh, Pittsburgh, PA; the §Depart-ment of Surgery, Medical University of South Carolina, Charleston, SC;and �Cepheid, Sunnyvale, CA.
Supported in part by NIH CA-01958 (S.J.H.), NIH CA-099123 (J.C., T.E.G.,S.J.H.), Department of Defense N00014-99-1-0784 (D.J.C., W.E.G., K.M.),and a cooperative research and development grant from Cepheid (T.E.G.).
Reprints: Steven J. Hughes, MD, Department of Surgery, University ofPittsburgh, 497 Scaife Hall, 3550 Terrace Street, Pittsburgh, PA 15261.E-mail: [email protected].
Copyright © 2006 by Lippincott Williams & WilkinsISSN: 0003-4932/06/24303-0389DOI: 10.1097/01.sla.0000201541.68577.6a
Annals of Surgery • Volume 243, Number 3, March 2006 389

or staging benefit to the patient? Until ongoing multicenter trialsdetermine whether completing the ALND when the SLNB ispositive for metastasis benefits the patient, it is clear that the timerequired to accurately evaluate SLNB specimens has significantimplications.20
It must also be recognized that, even with adequatetime, the accurate histologic analysis of lymph nodes formetastatic disease is challenging, and discordance in theinterpretation of these materials is a well-known clinicalproblem. Indeed, a recent study found alarming disparityamong pathologists in the analysis of SLNB specimens.21
Furthermore, protocols for SLNB specimen analysis varywidely between healthcare centers.22 Thus, current methodsof lymph node analysis clearly lack standardization, aredependent in part on subjective criteria, and are subject tohuman error.
We and others have shown that a real-time, quantitativeRT-PCR (QRT-PCR) analysis of lymph nodes can be moreaccurate than conventional histologic analysis in predict-ing prognosis for solid organ malignancies,23,24 and we havepreviously reported our development of a rapid QRT-PCRprocedure that can be completed (including RNA isolation)in less than 25 minutes.25 Importantly, a revolutionary toolfor molecular-based assays called the GeneXpert (Cepheid,Sunnyvale, CA) is in the final stages of development. Thisinstrument fully automates sample preparation, RNA isola-tion and purification, and QRT-PCR in a single-use, car-tridge-based format that removes the major obstacles limitingroutine use of molecular-based assays. Thus, we aimed todetermine if a rapid, fully automated, internally controlledQRT-PCR assay performed by a prototype GeneXpert instru-ment could produce equivalent results to histologic tech-niques of SLNB analysis, including IHC. This assay couldproduce significant benefits to patients and healthcare provid-ers by definitively analyzing lymph nodes using objectivecriteria in a time frame that allows intraoperative use, reducespatient psychologic distress, and improves standardizationbetween healthcare centers.
MATERIALS AND METHODS
Experimental DesignLiterature and database surveys identified potential
mRNA markers for detection of breast cancer metastases. Aprimary screen analyzed the expression of 43 markers in 6primary breast carcinomas and 10 benign lymph nodes frompatients without cancer. Six markers showed good character-istics for lymph node metastasis detection and entered asecondary screening phase where expression was analyzed in25 primary tumors, 27 lymph nodes histologically positivefor cancer, and 21 benign lymph nodes (73 individual pa-tients). Based on classification characteristics, 4 markers wereselected for an external validation study of 90 SLN from 90individual breast cancer patients using a rapid, multiplexreal-time PCR assay. Finally, 9 histologically negative and 9histologically positive lymph nodes were analyzed using acompletely automated and rapid RNA isolation and QRT-PCR assay on the GeneXpert instrument.
Source of TissuesAll tissues were collected through IRB approved pro-
tocols. Tissues for marker screening and GeneXpert studieswere obtained from tissue banks at the University of Pitts-burgh Medical Center and SLN for the marker validationstudy were obtained from the Minimally Invasive MolecularStaging of Breast Cancer Trial.
Tissue Preparation and Histologic AnalysisAll tissues were snap-frozen in liquid nitrogen and
stored at �80°C until use, when they were embedded in OCTcompound for frozen sectioning on a cryostat. For the markerscreening and GeneXpert studies, 45-�m sections were cutfor RNA isolation. Additional sections from the beginning,middle, and end of the sections for RNA isolation were cutfor hematoxylin and eosin and IHC (AE1/AE3 pancytokera-tin antibodies) analysis. All slides from each specimen wereindependently reviewed by 2 pathologists.
For the validation study, 115 sequentially obtainedSLN specimens from individual patients were identified.Five-micron serial sections were cut from each SLN, and theinitial and final 2 tissue sections were mounted on slides forhistologic analysis with hematoxylin and eosin staining andpancytokeratin IHC. The intervening sections were distrib-uted 4:1:4:1:4 etc., such that 4 sections were immediatelyplaced in chaotropic lysis buffer for RNA isolation and everyfifth section was mounted on a slide for histologic review(total of 50–60 sections). Review to confirm adequate pres-ervation of histology for pathologic analysis resulted in theexclusion of 25 specimens, principally due to freeze-dryingartifact. For the remaining 90 SLNs, sections from 3 levelsunderwent pathologic review with both hematoxylin andeosin and IHC staining, and remaining slides were reviewedas needed.
All specimens were independently evaluated by 2 pa-thologists with extensive experience interpreting breast can-cer specimens. The pathologists determined the presence orabsence of tumor, the percentage of tumor present, and thepresence of any contaminating tissues (eg, normal breasttissue). A single discordantly interpreted specimen was ob-served and was reviewed by both pathologists with a consen-sus reached that a single focus of metastatic tumor waspresent on only 2 of the 10 sections examined for that SLN.
RNA IsolationFor the screening and validation studies, RNA was
isolated using the RNeasy minikit (Qiagen, Valencia, CA) asdescribed by the manufacturer. The only modification wasthat the volume of lysis reagent was doubled and loaded onthe column in 2 steps. All RNAs were DNAse treated usingthe DNA-free Kit from Ambion.
Quantitative RT-PCR AnalysisFor the marker screening study, cDNA was synthesized
using random hexamers as previously described.26 Quantita-tive real-time PCR was performed on the ABI Prism 7700Sequence Detection instrument and expression of eachmarker gene was measured relative to the endogenous controlgene �-glucuronidase using �Ct calculations.23,27 The pri-
Hughes et al Annals of Surgery • Volume 243, Number 3, March 2006
© 2006 Lippincott Williams & Wilkins390

mary screen was performed using quantification with SYBRgreen.26 In the secondary screen, 5� nuclease hybridiza-tion probes were used to increase assay specificity.26 Allassays were designed using the ABI Primer Express Version2.0 software and, where possible, amplicons spanned exonjunctions to provide cDNA specificity. Negative controlswere included in each PCR plate. A mixture of UniversalHuman Reference RNA (Stratagene, La Jolla, CA) and RNAsfrom human placenta, thyroid, heart, colon, PCI13 cell line,and SKBR3 cell line served as a universal positive expressioncontrol for all the genes in the marker screening process.
Analysis in the marker validation study was performedusing rapid, multiplex (endogenous control gene and targetgene) QRT-PCR on the SmartCycler (Cepheid) as previouslydescribed.25,28 RNA input for each lymph node sample was 50to 200 ng per QRT-PCR reaction, and all reactions were per-formed in duplicate. Each reaction incorporated an internalpositive control oligonucleotide to demonstrate adequate assaysensitivity in the case of negative results.28 Gene specific reversetranscription primer sequences and PCR primer and probe se-quences are published as supplemental data on-line at http://www.mssm.edu/labs/godfrt01/publications/index.html.
GeneXpert AnalysisTwenty-four, 5-�m sections of OCT-embedded tissue
were sectioned into 800 mL of GeneXpert lysis buffer (Ce-pheid). The lysis buffer was filtered through a 0.22-�msyringe filter (Osmonics Inc, West Borough, MA) and loadedinto a GeneXpert cartridge. The automated processes ofRNA isolation, reverse transcription, and QRT-PCR on theGeneXpert are described elsewhere (Raja S et al Clin Chem.in press).
Statistical AnalysesThe characteristics used to evaluate markers were sen-
sitivity, specificity, classification accuracy and negative andpositive predictive values. The evaluation included charac-terizing the distributions of the markers and testing the fit ofthe data to the log-normal distribution. For individual mark-ers, a cutoff value was determined that maximized the clas-sification accuracy. In cases where classification accuracywas 100%, the cutoff was set at the midpoint between thehighest expressing benign node and the lowest expressinghistologically positive node. Markers were also evaluated inpaired combinations and a linear prediction rule was gener-ated for each pair. The rule was equivalent to the linearpredictor that equalized the fitted probabilities above andbelow the linear boundary. That is, points on the boundaryline had a predicted probability midway between the numericscores assigned to positive and negative nodes.
Properties of single and paired marker prediction ruleswere also investigated by examining the distributional prop-erties of the expression levels and by applying parametricbootstrap validation. Data were simulated from the lognormaland bivariate lognormal distributions using moment estima-tors for mean, variance, and correlation between markerpairs. A total of 500 parametric samples of the original datawere obtained and the prediction for each bootstrap samplewas applied to the original data. Using Efron’s improved
bootstrap for prediction error,29 the difference between theobserved classification accuracy and the average bootstrapclassification accuracy was used to estimate the optimism inthe resubstitution prediction rules. The single marker anddouble marker decision rules were then applied to data fromthe marker validation study and classification characteristicswere calculated.
Prediction characteristics of marker combinations werealso determined by generating equal probability contours. Inthis method, the joint distributions of marker pairs wereassumed to follow a bivariate log-normal distribution. Fromestimates of the means, variances, and covariances of benignnodes, equal probability contours were constructed aroundthe estimated mean values obtained for relative level ofexpression in benign lymph nodes. Observed values werethen plotted against these equal probability ellipsoids andcompared with contours for the more extreme quantiles,including the 95th, 99th, and 99.9th percentiles. This methodof analyzing the data attaches a value to each point that is theapproximate probability that the plotted node is benign.
RESULTS
Primary Marker ScreenMedian relative expression in primary tumors and in
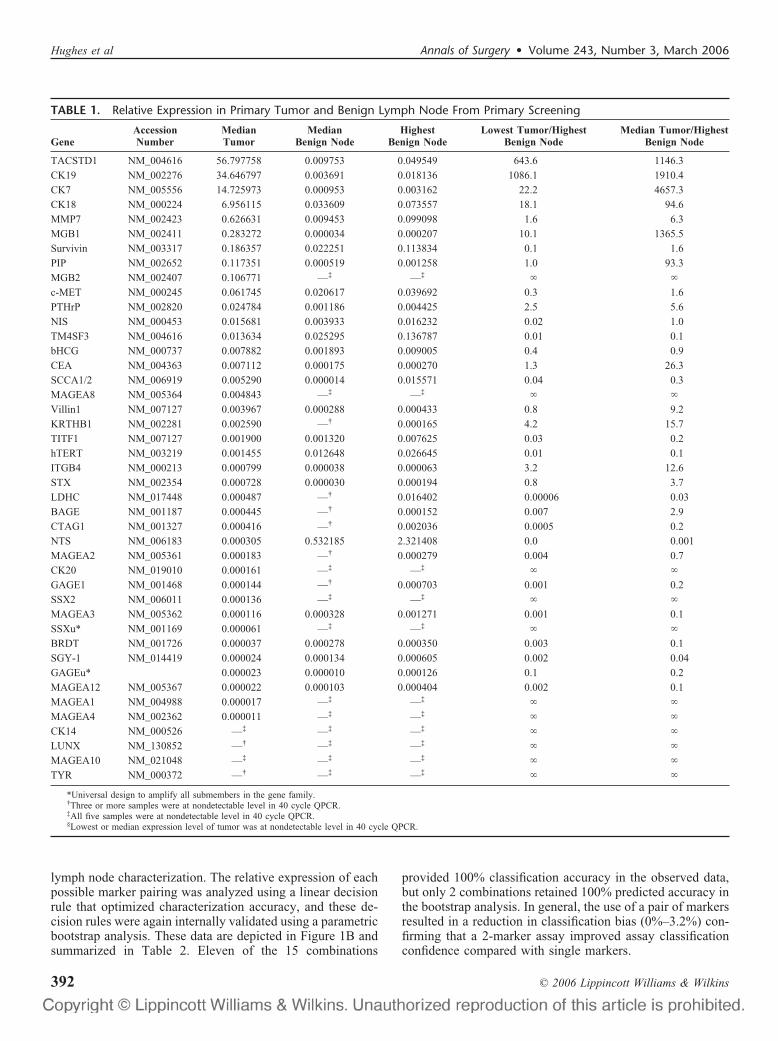
benign lymph nodes was calculated for all 43 potentialmarkers included in the primary screen (Table 1). In addition,we also calculated the ratio between the median expression intumors and the highest expressing benign node and betweenthe lowest expressing tumor and the highest expressing be-nign node. When using median expression in the tumors asthe numerator, 4 genes, TACSTD1, cytokeratin 7 (CK7),cytokeratin 19 (CK19), and mammoglobin 1 (MGB1), stoodout as having tumor/benign node ratios greater than 1000.Thus, these 4 markers were selected for further evaluation.Mammoglobin 2 (MGB2) and prolactin inducible protein(PIP) were also selected based on the primary screen data aswell as previously published data regarding these markers.30
The other 37 markers were excluded from further evaluation.
Secondary Marker ScreenHistologic evaluation of the 25 primary breast cancer
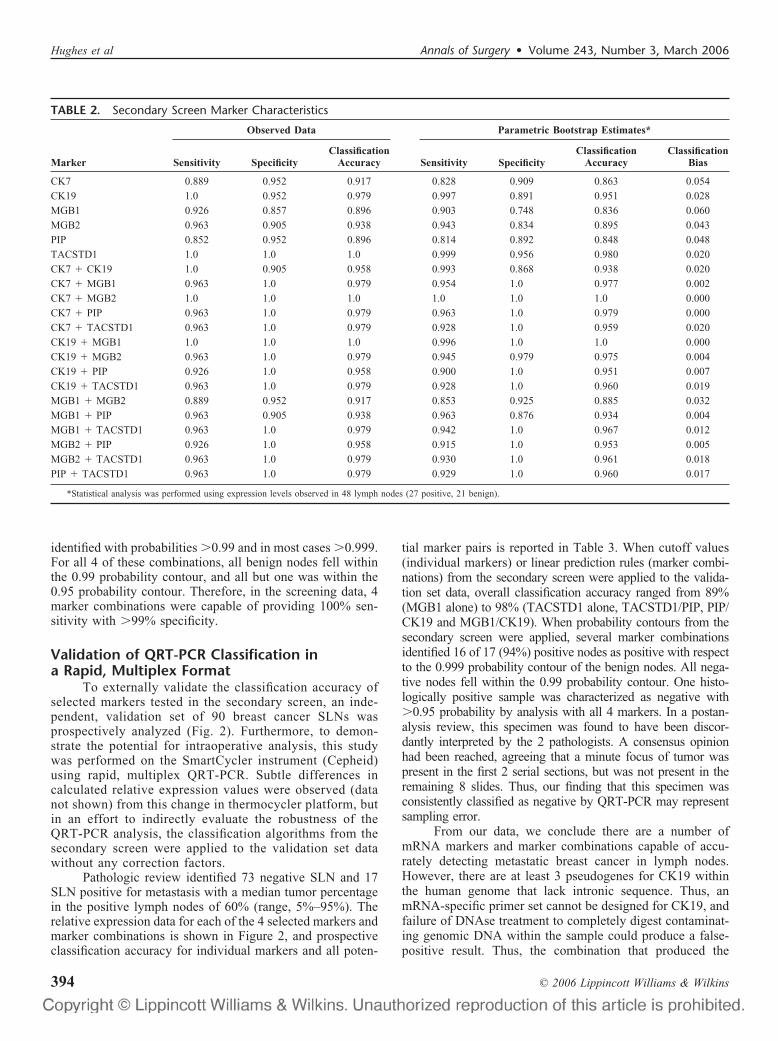
specimens used in the secondary screen revealed a mediantumor percentage of 75% (range, 5%–95%). The mediantumor percentage in the 27 histologically positive nodes was80% (range, 5%–95%). The relative expression of the 6markers included in the secondary screen in breast tumors,positive lymph nodes, and benign lymph nodes are shown inFigure 1A. The classification characteristics of each marker(compared with pathology review) are summarized in Table 2.The observed classification accuracies ranged from 89.6%(MGB1 and PIP) to 100% (TACSTD1). Parametric bootstrapanalysis of these data is also shown in Table 2, and the estimatesof classification bias ranged from 2% (TACSTD1) to 6%(MGB1). Thus, the relative expression level cutoffs establishedfor each individual marker in the screening set should accuratelycharacterize subsequently analyzed lymph nodes.
We examined all possible combinations of marker pairsto determine if a 2-marker assay produces a more robust
Annals of Surgery • Volume 243, Number 3, March 2006 QRT-PCR Analysis of Lymph Nodes in Breast Cancer
© 2006 Lippincott Williams & Wilkins 391
lymph node characterization. The relative expression of eachpossible marker pairing was analyzed using a linear decisionrule that optimized characterization accuracy, and these de-cision rules were again internally validated using a parametricbootstrap analysis. These data are depicted in Figure 1B andsummarized in Table 2. Eleven of the 15 combinations
provided 100% classification accuracy in the observed data,but only 2 combinations retained 100% predicted accuracy inthe bootstrap analysis. In general, the use of a pair of markersresulted in a reduction in classification bias (0%–3.2%) con-firming that a 2-marker assay improved assay classificationconfidence compared with single markers.
TABLE 1. Relative Expression in Primary Tumor and Benign Lymph Node From Primary Screening
GeneAccessionNumber
MedianTumor
MedianBenign Node
HighestBenign Node
Lowest Tumor/HighestBenign Node
Median Tumor/HighestBenign Node
TACSTD1 NM_004616 56.797758 0.009753 0.049549 643.6 1146.3
CK19 NM_002276 34.646797 0.003691 0.018136 1086.1 1910.4
CK7 NM_005556 14.725973 0.000953 0.003162 22.2 4657.3
CK18 NM_000224 6.956115 0.033609 0.073557 18.1 94.6
MMP7 NM_002423 0.626631 0.009453 0.099098 1.6 6.3
MGB1 NM_002411 0.283272 0.000034 0.000207 10.1 1365.5
Survivin NM_003317 0.186357 0.022251 0.113834 0.1 1.6
PIP NM_002652 0.117351 0.000519 0.001258 1.0 93.3
MGB2 NM_002407 0.106771 —‡ —‡ � �
c-MET NM_000245 0.061745 0.020617 0.039692 0.3 1.6
PTHrP NM_002820 0.024784 0.001186 0.004425 2.5 5.6
NIS NM_000453 0.015681 0.003933 0.016232 0.02 1.0
TM4SF3 NM_004616 0.013634 0.025295 0.136787 0.01 0.1
bHCG NM_000737 0.007882 0.001893 0.009005 0.4 0.9
CEA NM_004363 0.007112 0.000175 0.000270 1.3 26.3
SCCA1/2 NM_006919 0.005290 0.000014 0.015571 0.04 0.3
MAGEA8 NM_005364 0.004843 —‡ —‡ � �
Villin1 NM_007127 0.003967 0.000288 0.000433 0.8 9.2
KRTHB1 NM_002281 0.002590 —† 0.000165 4.2 15.7
TITF1 NM_007127 0.001900 0.001320 0.007625 0.03 0.2
hTERT NM_003219 0.001455 0.012648 0.026645 0.01 0.1
ITGB4 NM_000213 0.000799 0.000038 0.000063 3.2 12.6
STX NM_002354 0.000728 0.000030 0.000194 0.8 3.7
LDHC NM_017448 0.000487 —† 0.016402 0.00006 0.03
BAGE NM_001187 0.000445 —† 0.000152 0.007 2.9
CTAG1 NM_001327 0.000416 —† 0.002036 0.0005 0.2
NTS NM_006183 0.000305 0.532185 2.321408 0.0 0.001
MAGEA2 NM_005361 0.000183 —† 0.000279 0.004 0.7
CK20 NM_019010 0.000161 —‡ —‡ � �
GAGE1 NM_001468 0.000144 —† 0.000703 0.001 0.2
SSX2 NM_006011 0.000136 —‡ —‡ � �
MAGEA3 NM_005362 0.000116 0.000328 0.001271 0.001 0.1
SSXu* NM_001169 0.000061 —‡ —‡ � �
BRDT NM_001726 0.000037 0.000278 0.000350 0.003 0.1
SGY-1 NM_014419 0.000024 0.000134 0.000605 0.002 0.04
GAGEu* 0.000023 0.000010 0.000126 0.1 0.2
MAGEA12 NM_005367 0.000022 0.000103 0.000404 0.002 0.1
MAGEA1 NM_004988 0.000017 —‡ —‡ � �
MAGEA4 NM_002362 0.000011 —‡ —‡ � �
CK14 NM_000526 —‡ —‡ —‡ � �
LUNX NM_130852 —† —‡ —‡ � �
MAGEA10 NM_021048 —‡ —‡ —‡ � �
TYR NM_000372 —† —‡ —‡ � �
*Universal design to amplify all submembers in the gene family.†Three or more samples were at nondetectable level in 40 cycle QPCR.‡All five samples were at nondetectable level in 40 cycle QPCR.§Lowest or median expression level of tumor was at nondetectable level in 40 cycle QPCR.
Hughes et al Annals of Surgery • Volume 243, Number 3, March 2006
© 2006 Lippincott Williams & Wilkins392
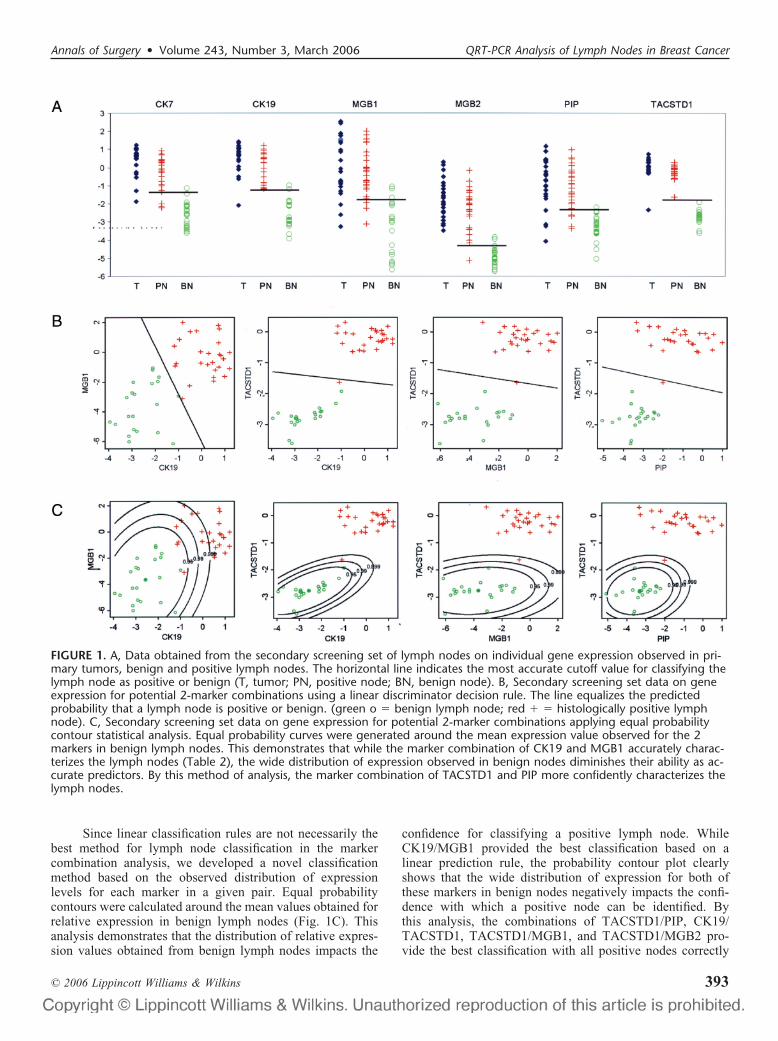
Since linear classification rules are not necessarily thebest method for lymph node classification in the markercombination analysis, we developed a novel classificationmethod based on the observed distribution of expressionlevels for each marker in a given pair. Equal probabilitycontours were calculated around the mean values obtained forrelative expression in benign lymph nodes (Fig. 1C). Thisanalysis demonstrates that the distribution of relative expres-sion values obtained from benign lymph nodes impacts the
confidence for classifying a positive lymph node. WhileCK19/MGB1 provided the best classification based on alinear prediction rule, the probability contour plot clearlyshows that the wide distribution of expression for both ofthese markers in benign nodes negatively impacts the confi-dence with which a positive node can be identified. Bythis analysis, the combinations of TACSTD1/PIP, CK19/TACSTD1, TACSTD1/MGB1, and TACSTD1/MGB2 pro-vide the best classification with all positive nodes correctly
FIGURE 1. A, Data obtained from the secondary screening set of lymph nodes on individual gene expression observed in pri-mary tumors, benign and positive lymph nodes. The horizontal line indicates the most accurate cutoff value for classifying thelymph node as positive or benign (T, tumor; PN, positive node; BN, benign node). B, Secondary screening set data on geneexpression for potential 2-marker combinations using a linear discriminator decision rule. The line equalizes the predictedprobability that a lymph node is positive or benign. (green o � benign lymph node; red � � histologically positive lymphnode). C, Secondary screening set data on gene expression for potential 2-marker combinations applying equal probabilitycontour statistical analysis. Equal probability curves were generated around the mean expression value observed for the 2markers in benign lymph nodes. This demonstrates that while the marker combination of CK19 and MGB1 accurately charac-terizes the lymph nodes (Table 2), the wide distribution of expression observed in benign nodes diminishes their ability as ac-curate predictors. By this method of analysis, the marker combination of TACSTD1 and PIP more confidently characterizes thelymph nodes.
Annals of Surgery • Volume 243, Number 3, March 2006 QRT-PCR Analysis of Lymph Nodes in Breast Cancer
© 2006 Lippincott Williams & Wilkins 393
identified with probabilities �0.99 and in most cases �0.999.For all 4 of these combinations, all benign nodes fell withinthe 0.99 probability contour, and all but one was within the0.95 probability contour. Therefore, in the screening data, 4marker combinations were capable of providing 100% sen-sitivity with �99% specificity.
Validation of QRT-PCR Classification ina Rapid, Multiplex Format
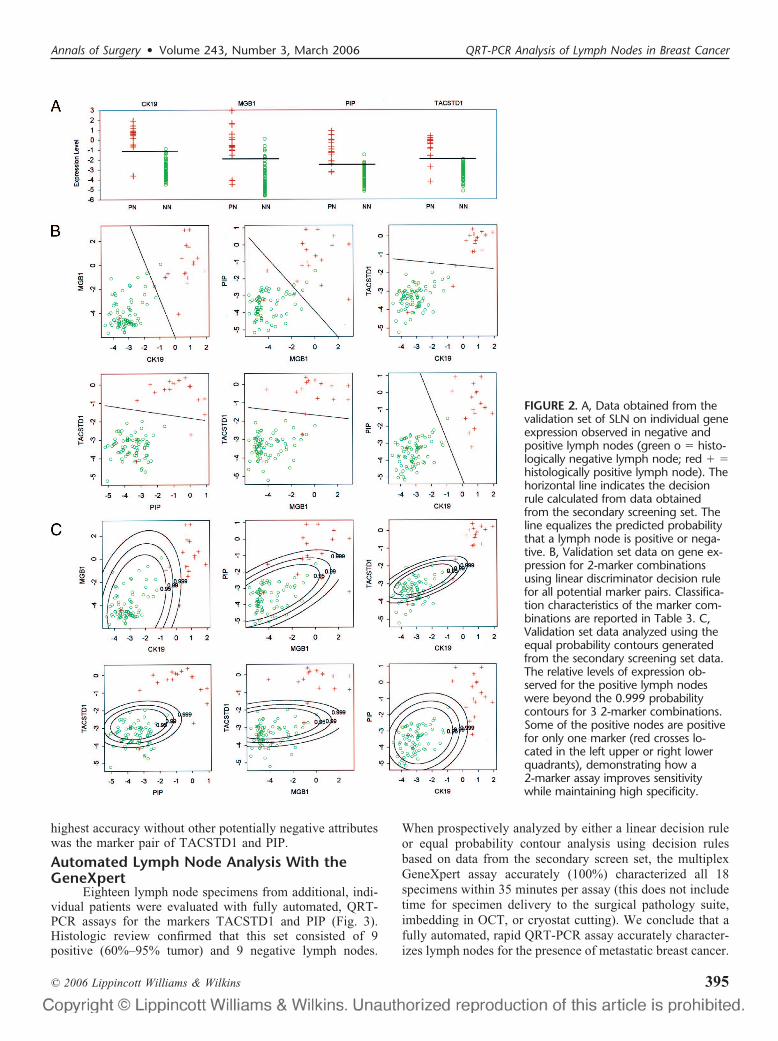
To externally validate the classification accuracy ofselected markers tested in the secondary screen, an inde-pendent, validation set of 90 breast cancer SLNs wasprospectively analyzed (Fig. 2). Furthermore, to demon-strate the potential for intraoperative analysis, this studywas performed on the SmartCycler instrument (Cepheid)using rapid, multiplex QRT-PCR. Subtle differences incalculated relative expression values were observed (datanot shown) from this change in thermocycler platform, butin an effort to indirectly evaluate the robustness of theQRT-PCR analysis, the classification algorithms from thesecondary screen were applied to the validation set datawithout any correction factors.
Pathologic review identified 73 negative SLN and 17SLN positive for metastasis with a median tumor percentagein the positive lymph nodes of 60% (range, 5%–95%). Therelative expression data for each of the 4 selected markers andmarker combinations is shown in Figure 2, and prospectiveclassification accuracy for individual markers and all poten-
tial marker pairs is reported in Table 3. When cutoff values(individual markers) or linear prediction rules (marker combi-nations) from the secondary screen were applied to the valida-tion set data, overall classification accuracy ranged from 89%(MGB1 alone) to 98% (TACSTD1 alone, TACSTD1/PIP, PIP/CK19 and MGB1/CK19). When probability contours from thesecondary screen were applied, several marker combinationsidentified 16 of 17 (94%) positive nodes as positive with respectto the 0.999 probability contour of the benign nodes. All nega-tive nodes fell within the 0.99 probability contour. One histo-logically positive sample was characterized as negative with�0.95 probability by analysis with all 4 markers. In a postan-alysis review, this specimen was found to have been discor-dantly interpreted by the 2 pathologists. A consensus opinionhad been reached, agreeing that a minute focus of tumor waspresent in the first 2 serial sections, but was not present in theremaining 8 slides. Thus, our finding that this specimen wasconsistently classified as negative by QRT-PCR may representsampling error.
From our data, we conclude there are a number ofmRNA markers and marker combinations capable of accu-rately detecting metastatic breast cancer in lymph nodes.However, there are at least 3 pseudogenes for CK19 withinthe human genome that lack intronic sequence. Thus, anmRNA-specific primer set cannot be designed for CK19, andfailure of DNAse treatment to completely digest contaminat-ing genomic DNA within the sample could produce a false-positive result. Thus, the combination that produced the
TABLE 2. Secondary Screen Marker Characteristics
Observed Data Parametric Bootstrap Estimates*
Marker Sensitivity SpecificityClassification
Accuracy Sensitivity SpecificityClassification
AccuracyClassification
Bias
CK7 0.889 0.952 0.917 0.828 0.909 0.863 0.054
CK19 1.0 0.952 0.979 0.997 0.891 0.951 0.028
MGB1 0.926 0.857 0.896 0.903 0.748 0.836 0.060
MGB2 0.963 0.905 0.938 0.943 0.834 0.895 0.043
PIP 0.852 0.952 0.896 0.814 0.892 0.848 0.048
TACSTD1 1.0 1.0 1.0 0.999 0.956 0.980 0.020
CK7 � CK19 1.0 0.905 0.958 0.993 0.868 0.938 0.020
CK7 � MGB1 0.963 1.0 0.979 0.954 1.0 0.977 0.002
CK7 � MGB2 1.0 1.0 1.0 1.0 1.0 1.0 0.000
CK7 � PIP 0.963 1.0 0.979 0.963 1.0 0.979 0.000
CK7 � TACSTD1 0.963 1.0 0.979 0.928 1.0 0.959 0.020
CK19 � MGB1 1.0 1.0 1.0 0.996 1.0 1.0 0.000
CK19 � MGB2 0.963 1.0 0.979 0.945 0.979 0.975 0.004
CK19 � PIP 0.926 1.0 0.958 0.900 1.0 0.951 0.007
CK19 � TACSTD1 0.963 1.0 0.979 0.928 1.0 0.960 0.019
MGB1 � MGB2 0.889 0.952 0.917 0.853 0.925 0.885 0.032
MGB1 � PIP 0.963 0.905 0.938 0.963 0.876 0.934 0.004
MGB1 � TACSTD1 0.963 1.0 0.979 0.942 1.0 0.967 0.012
MGB2 � PIP 0.926 1.0 0.958 0.915 1.0 0.953 0.005
MGB2 � TACSTD1 0.963 1.0 0.979 0.930 1.0 0.961 0.018
PIP � TACSTD1 0.963 1.0 0.979 0.929 1.0 0.960 0.017
*Statistical analysis was performed using expression levels observed in 48 lymph nodes (27 positive, 21 benign).
Hughes et al Annals of Surgery • Volume 243, Number 3, March 2006
© 2006 Lippincott Williams & Wilkins394
highest accuracy without other potentially negative attributeswas the marker pair of TACSTD1 and PIP.
Automated Lymph Node Analysis With theGeneXpert
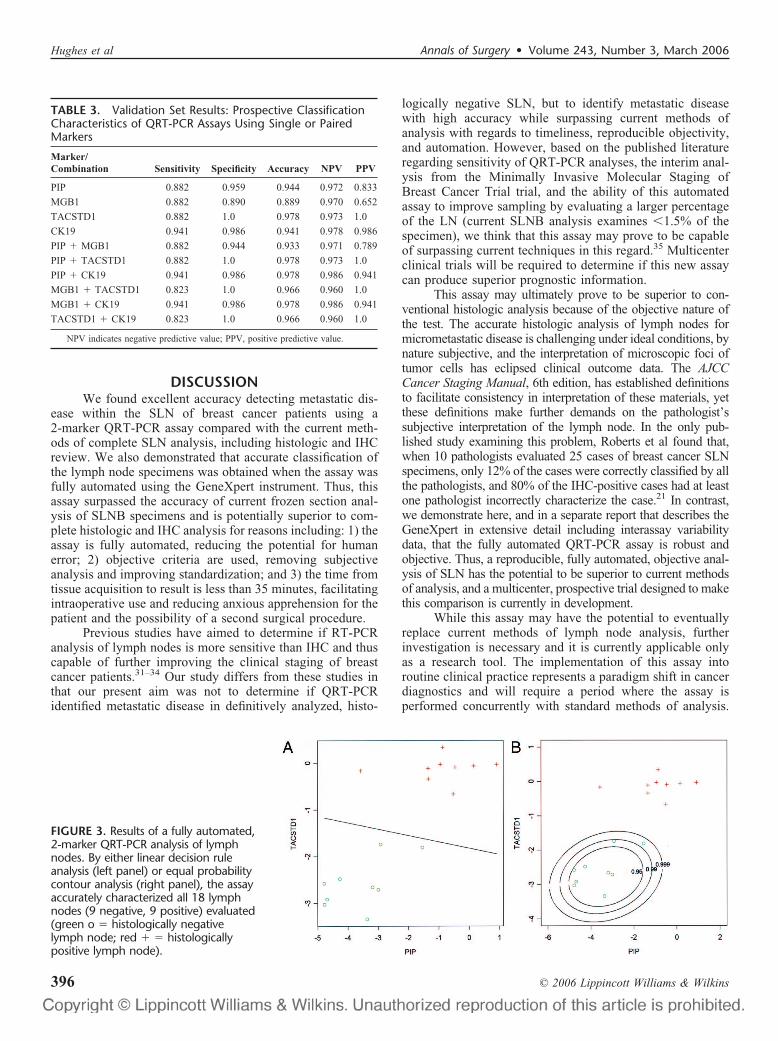
Eighteen lymph node specimens from additional, indi-vidual patients were evaluated with fully automated, QRT-PCR assays for the markers TACSTD1 and PIP (Fig. 3).Histologic review confirmed that this set consisted of 9positive (60%–95% tumor) and 9 negative lymph nodes.
When prospectively analyzed by either a linear decision ruleor equal probability contour analysis using decision rulesbased on data from the secondary screen set, the multiplexGeneXpert assay accurately (100%) characterized all 18specimens within 35 minutes per assay (this does not includetime for specimen delivery to the surgical pathology suite,imbedding in OCT, or cryostat cutting). We conclude that afully automated, rapid QRT-PCR assay accurately character-izes lymph nodes for the presence of metastatic breast cancer.
FIGURE 2. A, Data obtained from thevalidation set of SLN on individual geneexpression observed in negative andpositive lymph nodes (green o � histo-logically negative lymph node; red � �histologically positive lymph node). Thehorizontal line indicates the decisionrule calculated from data obtainedfrom the secondary screening set. Theline equalizes the predicted probabilitythat a lymph node is positive or nega-tive. B, Validation set data on gene ex-pression for 2-marker combinationsusing linear discriminator decision rulefor all potential marker pairs. Classifica-tion characteristics of the marker com-binations are reported in Table 3. C,Validation set data analyzed using theequal probability contours generatedfrom the secondary screening set data.The relative levels of expression ob-served for the positive lymph nodeswere beyond the 0.999 probabilitycontours for 3 2-marker combinations.Some of the positive nodes are positivefor only one marker (red crosses lo-cated in the left upper or right lowerquadrants), demonstrating how a2-marker assay improves sensitivitywhile maintaining high specificity.
Annals of Surgery • Volume 243, Number 3, March 2006 QRT-PCR Analysis of Lymph Nodes in Breast Cancer
© 2006 Lippincott Williams & Wilkins 395
DISCUSSIONWe found excellent accuracy detecting metastatic dis-
ease within the SLN of breast cancer patients using a2-marker QRT-PCR assay compared with the current meth-ods of complete SLN analysis, including histologic and IHCreview. We also demonstrated that accurate classification ofthe lymph node specimens was obtained when the assay wasfully automated using the GeneXpert instrument. Thus, thisassay surpassed the accuracy of current frozen section anal-ysis of SLNB specimens and is potentially superior to com-plete histologic and IHC analysis for reasons including: 1) theassay is fully automated, reducing the potential for humanerror; 2) objective criteria are used, removing subjectiveanalysis and improving standardization; and 3) the time fromtissue acquisition to result is less than 35 minutes, facilitatingintraoperative use and reducing anxious apprehension for thepatient and the possibility of a second surgical procedure.
Previous studies have aimed to determine if RT-PCRanalysis of lymph nodes is more sensitive than IHC and thuscapable of further improving the clinical staging of breastcancer patients.31–34 Our study differs from these studies inthat our present aim was not to determine if QRT-PCRidentified metastatic disease in definitively analyzed, histo-
logically negative SLN, but to identify metastatic diseasewith high accuracy while surpassing current methods ofanalysis with regards to timeliness, reproducible objectivity,and automation. However, based on the published literatureregarding sensitivity of QRT-PCR analyses, the interim anal-ysis from the Minimally Invasive Molecular Staging ofBreast Cancer Trial trial, and the ability of this automatedassay to improve sampling by evaluating a larger percentageof the LN (current SLNB analysis examines �1.5% of thespecimen), we think that this assay may prove to be capableof surpassing current techniques in this regard.35 Multicenterclinical trials will be required to determine if this new assaycan produce superior prognostic information.
This assay may ultimately prove to be superior to con-ventional histologic analysis because of the objective nature ofthe test. The accurate histologic analysis of lymph nodes formicrometastatic disease is challenging under ideal conditions, bynature subjective, and the interpretation of microscopic foci oftumor cells has eclipsed clinical outcome data. The AJCCCancer Staging Manual, 6th edition, has established definitionsto facilitate consistency in interpretation of these materials, yetthese definitions make further demands on the pathologist’ssubjective interpretation of the lymph node. In the only pub-lished study examining this problem, Roberts et al found that,when 10 pathologists evaluated 25 cases of breast cancer SLNspecimens, only 12% of the cases were correctly classified by allthe pathologists, and 80% of the IHC-positive cases had at leastone pathologist incorrectly characterize the case.21 In contrast,we demonstrate here, and in a separate report that describes theGeneXpert in extensive detail including interassay variabilitydata, that the fully automated QRT-PCR assay is robust andobjective. Thus, a reproducible, fully automated, objective anal-ysis of SLN has the potential to be superior to current methodsof analysis, and a multicenter, prospective trial designed to makethis comparison is currently in development.
While this assay may have the potential to eventuallyreplace current methods of lymph node analysis, furtherinvestigation is necessary and it is currently applicable onlyas a research tool. The implementation of this assay intoroutine clinical practice represents a paradigm shift in cancerdiagnostics and will require a period where the assay isperformed concurrently with standard methods of analysis.
FIGURE 3. Results of a fully automated,2-marker QRT-PCR analysis of lymphnodes. By either linear decision ruleanalysis (left panel) or equal probabilitycontour analysis (right panel), the assayaccurately characterized all 18 lymphnodes (9 negative, 9 positive) evaluated(green o � histologically negativelymph node; red � � histologicallypositive lymph node).
TABLE 3. Validation Set Results: Prospective ClassificationCharacteristics of QRT-PCR Assays Using Single or PairedMarkers
Marker/Combination Sensitivity Specificity Accuracy NPV PPV
PIP 0.882 0.959 0.944 0.972 0.833
MGB1 0.882 0.890 0.889 0.970 0.652
TACSTD1 0.882 1.0 0.978 0.973 1.0
CK19 0.941 0.986 0.941 0.978 0.986
PIP � MGB1 0.882 0.944 0.933 0.971 0.789
PIP � TACSTD1 0.882 1.0 0.978 0.973 1.0
PIP � CK19 0.941 0.986 0.978 0.986 0.941
MGB1 � TACSTD1 0.823 1.0 0.966 0.960 1.0
MGB1 � CK19 0.941 0.986 0.978 0.986 0.941
TACSTD1 � CK19 0.823 1.0 0.966 0.960 1.0
NPV indicates negative predictive value; PPV, positive predictive value.
Hughes et al Annals of Surgery • Volume 243, Number 3, March 2006
© 2006 Lippincott Williams & Wilkins396
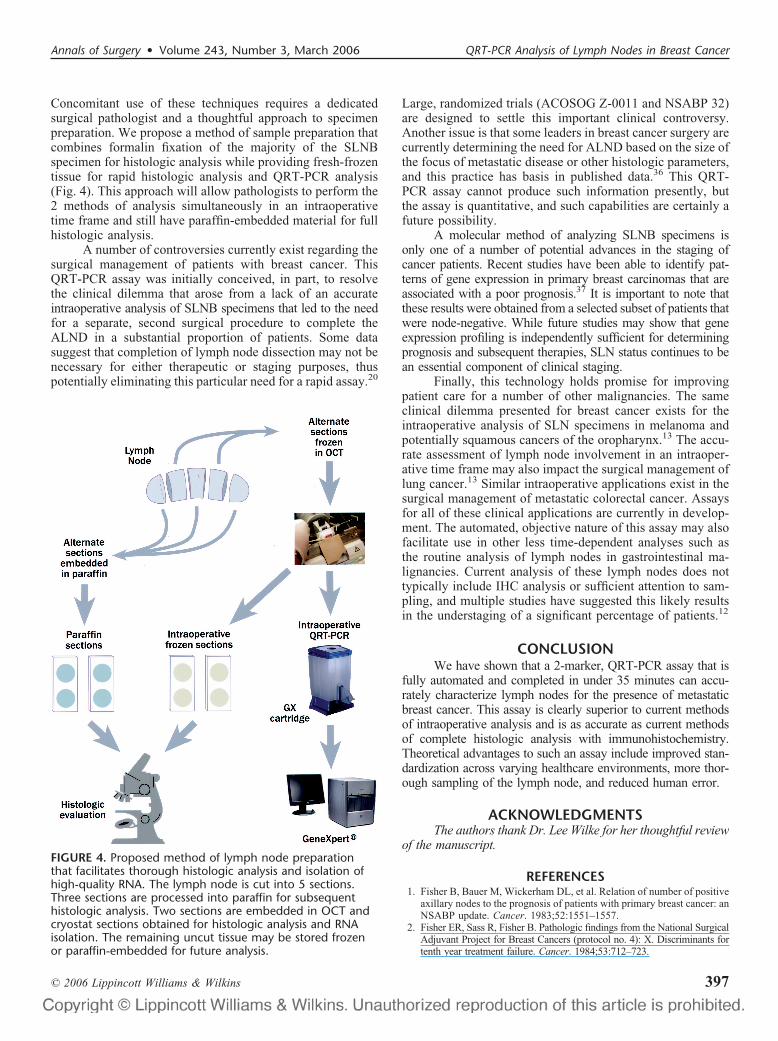
Concomitant use of these techniques requires a dedicatedsurgical pathologist and a thoughtful approach to specimenpreparation. We propose a method of sample preparation thatcombines formalin fixation of the majority of the SLNBspecimen for histologic analysis while providing fresh-frozentissue for rapid histologic analysis and QRT-PCR analysis(Fig. 4). This approach will allow pathologists to perform the2 methods of analysis simultaneously in an intraoperativetime frame and still have paraffin-embedded material for fullhistologic analysis.
A number of controversies currently exist regarding thesurgical management of patients with breast cancer. ThisQRT-PCR assay was initially conceived, in part, to resolvethe clinical dilemma that arose from a lack of an accurateintraoperative analysis of SLNB specimens that led to the needfor a separate, second surgical procedure to complete theALND in a substantial proportion of patients. Some datasuggest that completion of lymph node dissection may not benecessary for either therapeutic or staging purposes, thuspotentially eliminating this particular need for a rapid assay.20
Large, randomized trials (ACOSOG Z-0011 and NSABP 32)are designed to settle this important clinical controversy.Another issue is that some leaders in breast cancer surgery arecurrently determining the need for ALND based on the size ofthe focus of metastatic disease or other histologic parameters,and this practice has basis in published data.36 This QRT-PCR assay cannot produce such information presently, butthe assay is quantitative, and such capabilities are certainly afuture possibility.
A molecular method of analyzing SLNB specimens isonly one of a number of potential advances in the staging ofcancer patients. Recent studies have been able to identify pat-terns of gene expression in primary breast carcinomas that areassociated with a poor prognosis.37 It is important to note thatthese results were obtained from a selected subset of patients thatwere node-negative. While future studies may show that geneexpression profiling is independently sufficient for determiningprognosis and subsequent therapies, SLN status continues to bean essential component of clinical staging.
Finally, this technology holds promise for improvingpatient care for a number of other malignancies. The sameclinical dilemma presented for breast cancer exists for theintraoperative analysis of SLN specimens in melanoma andpotentially squamous cancers of the oropharynx.13 The accu-rate assessment of lymph node involvement in an intraoper-ative time frame may also impact the surgical management oflung cancer.13 Similar intraoperative applications exist in thesurgical management of metastatic colorectal cancer. Assaysfor all of these clinical applications are currently in develop-ment. The automated, objective nature of this assay may alsofacilitate use in other less time-dependent analyses such asthe routine analysis of lymph nodes in gastrointestinal ma-lignancies. Current analysis of these lymph nodes does nottypically include IHC analysis or sufficient attention to sam-pling, and multiple studies have suggested this likely resultsin the understaging of a significant percentage of patients.12
CONCLUSIONWe have shown that a 2-marker, QRT-PCR assay that is
fully automated and completed in under 35 minutes can accu-rately characterize lymph nodes for the presence of metastaticbreast cancer. This assay is clearly superior to current methodsof intraoperative analysis and is as accurate as current methodsof complete histologic analysis with immunohistochemistry.Theoretical advantages to such an assay include improved stan-dardization across varying healthcare environments, more thor-ough sampling of the lymph node, and reduced human error.
ACKNOWLEDGMENTSThe authors thank Dr. Lee Wilke for her thoughtful review
of the manuscript.
REFERENCES1. Fisher B, Bauer M, Wickerham DL, et al. Relation of number of positive
axillary nodes to the prognosis of patients with primary breast cancer: anNSABP update. Cancer. 1983;52:1551–1557.
2. Fisher ER, Sass R, Fisher B. Pathologic findings from the National SurgicalAdjuvant Project for Breast Cancers (protocol no. 4): X. Discriminants fortenth year treatment failure. Cancer. 1984;53:712–723.
FIGURE 4. Proposed method of lymph node preparationthat facilitates thorough histologic analysis and isolation ofhigh-quality RNA. The lymph node is cut into 5 sections.Three sections are processed into paraffin for subsequenthistologic analysis. Two sections are embedded in OCT andcryostat sections obtained for histologic analysis and RNAisolation. The remaining uncut tissue may be stored frozenor paraffin-embedded for future analysis.
Annals of Surgery • Volume 243, Number 3, March 2006 QRT-PCR Analysis of Lymph Nodes in Breast Cancer
© 2006 Lippincott Williams & Wilkins 397

3. Fisher ER, Costantino J, Fisher B, et al. Pathologic findings from theNational Surgical Adjuvant Breast Project (Protocol 4): Discriminantsfor 15-year survival. National Surgical Adjuvant Breast and BowelProject Investigators. Cancer. 1993;71:2141–2150.
4. Siziopikou KP, Schnitt SJ, Connolly JL, et al. Detection and significanceof occult axillary metastatic disease in breast cancer patients. Breast J.1999;5:221–229.
5. Turner RR, Ollila DW, Krasne DL, et al. Histopathologic validation ofthe sentinel lymph node hypothesis for breast carcinoma. Ann Surg.1997;226:271–276.
6. Cote RJ, Peterson HF, Chaiwun B, et al. Role of immunohistochemicaldetection of lymph-node metastases in management of breast cancer.Lancet. 1999;354:896–900.
7. de Mascarel I, Bonichon F, Coindre JM, et al. Prognostic significance ofbreast cancer axillary lymph node micrometastases assessed by twospecial techniques: reevaluation with longer follow-up. Br J Cancer.1992;66:523–527.
8. Giuliano AE, Dale PS, Turner RR, et al. Improved axillary staging of breastcancer with sentinel lymphadenectomy. Ann Surg. 1995;222:394–399.
9. Leong AS. The prognostic dilemma of nodal micrometastases in breastcarcinoma. Gan To Kagaku Ryoho. 2000;27(suppl 2):315–320.
10. Noguchi M. Therapeutic relevance of breast cancer micrometastases insentinel lymph nodes. Br J Surg. 2002;89:1505–1515.
11. Weaver DL. Sentinel lymph nodes and breast carcinoma: which microme-tastases are clinically significant? Am J Surg Pathol. 2003;27:842–845.
12. Saha S, Dan AG, Bilchik AJ, et al. Historical review of lymphaticmapping in gastrointestinal malignancies. Ann Surg Oncol. 2004;11(suppl):245–249.
13. Goyal A, Mansel RE. Current status of sentinel lymph node biopsy insolid malignancies. World J Surg Oncol. 2004;2:9.
14. Ross GL, Soutar DS, MacDonald DG, et al. Improved staging of cervicalmetastases in clinically node-negative patients with head and necksquamous cell carcinoma. Ann Surg Oncol. 2004;11:213–218.
15. Wawroschek F, Vogt H, Weckermann D, et al. The sentinel lymph nodeconcept in prostate cancer: first results of gamma probe-guided sentinellymph node identification. Eur Urol. 1999;36:595–600.
16. Giuliano AE, Haigh PI, Brennan MB, et al. Prospective observationalstudy of sentinel lymphadenectomy without further axillary dissection inpatients with sentinel node-negative breast cancer. J Clin Oncol. 2000;18:2553–2559.
17. Chao C, Wong SL, Ackermann D, et al. Utility of intraoperative frozensection analysis of sentinel lymph nodes in breast cancer. Am J Surg.2001;182:609–615.
18. Gulec SA, Su J, O’Leary JP, et al. Clinical utility of frozen section insentinel node biopsy in breast cancer. Am Surg. 2001;67:529–532.
19. Gemignani ML, Cody HS III, Fey JV, et al. Impact of sentinel lymphnode mapping on relative charges in patients with early-stage breastcancer. Ann Surg Oncol. 2000;7:575–580.
20. Wilke LG, Giuliano A. Sentinel lymph node biopsy in patients withearly-stage breast cancer: status of the National Clinical Trials. Surg ClinNorth Am. 2003;83:901–910.
21. Roberts CA, Beitsch PD, Litz CE, et al. Interpretive disparity among
pathologists in breast sentinel lymph node evaluation. Am J Surg.2003;186:324–329.
22. Hunt JL, Baloch ZW, LiVolsi VA. Sentinel lymph node evaluation fortumor metastasis. Semin Diagn Pathol. 2002;19:263–277.
23. Godfrey TE, Raja S, Finkelstein SD, et al. Prognostic value of quantitativereverse transcription-polymerase chain reaction in lymph node-negativeesophageal cancer patients. Clin Cancer Res. 2001;7:4041–4048.
24. Liefers GJ, Cleton-Jansen AM, van de Velde CJ, et al. Micrometastases andsurvival in stage II colorectal cancer. N Engl J Med. 1998;339:223–228.
25. Raja S, Luketich JD, Kelly LA, et al. Rapid, quantitative reversetranscriptase-polymerase chain reaction: application to intraoperativemolecular detection of occult metastases in esophageal cancer. J ThoracCardiovasc Surg. 2002;123:475–482.
26. Xi L, Raja S, Gooding W, et al. Molecular staging of lymph nodes frompatient’s with esophageal adenocarcinoma. Clin Cancer Res. in press.
27. Tassone F, Hagerman RJ, Taylor AK, et al. Elevated levels of FMR1mRNA in carrier males: a new mechanism of involvement in thefragile-X syndrome. Am J Hum Genet. 2000;66:6–15.
28. Raja S, El Hefnawy T, Kelly LA, et al. Temperature-controlled primerlimit for multiplexing of rapid, quantitative reverse transcription-PCRassays: application to intraoperative cancer diagnostics. Clin Chem.2002;48:1329–1337.
29. Efron B. An Introduction to the Bootstrap. Boca Raton, FL: Chapmanand Hall, 1993:247–252.
30. Mitas M, Mikhitarian K, Walters C, et al. Quantitative real-time RT-PCR detection of breast cancer micrometastasis using a multigenemarker panel. Int J Cancer. 2001;93:162–171.
31. Bostick PJ, Huynh KT, Sarantou T, et al. Detection of metastases insentinel lymph nodes of breast cancer patients by multiple-markerRT-PCR. Int J Cancer. 1998;79:645–651.
32. Bostick PJ, Chatterjee S, Chi DD, et al. Limitations of specific reverse-transcriptase polymerase chain reaction markers in the detection ofmetastases in the lymph nodes and blood of breast cancer patients. J ClinOncol. 1998;16:2632–2640.
33. Mori M, Mimori K, Inoue H, et al. Detection of cancer micrometastasesin lymph nodes by reverse transcriptase-polymerase chain reaction.Cancer Res. 1995;55:3417–3420.
34. Schoenfeld A, Luqmani Y, Smith D, et al. Detection of breast cancermicrometastases in axillary lymph nodes by using polymerase chainreaction. Cancer Res. 1994;54:2986–2990.
35. Gillanders WE, Mikhitarian K, Hebert R, et al. Molecular detection ofmicrometastatic breast cancer in histopathology-negative axillary lymphnodes correlates with traditional predictors of prognosis: an interimanalysis of a prospective multi-institutional cohort study. Ann Surg.2004;239:828–837.
36. Van Zee KJ, Manasseh DM, Bevilacqua JL, et al. A nomogram forpredicting the likelihood of additional nodal metastases in breast cancerpatients with a positive sentinel node biopsy. Ann Surg Oncol. 2003;10:1140–1151.
37. van de Vijver M, Van’t Veer LJ, Dai H, et al. Gene expression profilingof breast cancer accurately predicts clinical outcome of disease. ModPathol. 2002;15:55A.
Hughes et al Annals of Surgery • Volume 243, Number 3, March 2006
© 2006 Lippincott Williams & Wilkins398