a randomised phase 2 trial of dexamethasone versus prednisolone in castration-resistant prostate...
TRANSCRIPT
E U R O P E A N U R O L O G Y 6 7 ( 2 0 1 5 ) 6 7 3 – 6 7 9
ava i lable at www.sciencedirect .com
journal homepage: www.europeanurology.com
Platinum Priority – Prostate CancerEditorial by Camillo Porta, Sergio Bracarda and Romano Danesi on pp. 680–681 of this issue
A Randomised Phase 2 Trial of Dexamethasone Versus
Prednisolone in Castration-resistant Prostate Cancer
Ramachandran Venkitaraman a, David Lorente b, Vedang Murthy c, Karen Thomas d,Lydia Parker b, Ruth Ahiabor b, David Dearnaley b, Robert Huddart b, Johann De Bono b,Chris Parker d,*
a Ipswich Hospital NHS and University Campus Suffolk, Ipswich, UK; b Institute of Cancer Research, Sutton, UK; c Advanced Centre for Treatment Research and
Education in Cancer (ACTREC), Tata Memorial Centre, Mumbai, India; d Royal Marsden Hospital, Sutton, UK
Article info
Article history:
Accepted October 1, 2014
Keywords:
Prostate cancer
Dexamethasone
Prednisolone
Please visit
www.eu-acme.org/
europeanurology to read and
answer questions on-line.
The EU-ACME credits will
then be attributed
automatically.
Abstract
Background: Prednisolone is widely used as secondary hormonal treatment for castra-tion-resistant prostate cancer (CRPC). We hypothesised that dexamethasone, anothercorticosteroid, is more active.Objective: To compare the activity of prednisolone and dexamethasone in CRPC.Design, setting, and participants: This single-centre, randomised, phase 2 trial wasperformed in 82 men with chemotherapy-naıve CRPC enrolled from 2006 to 2010.Intervention: Prednisolone 5 mg twice daily versus dexamethasone 0.5 mg once dailyversus intermittent dexamethasone 8 mg twice daily on days 1–3 every 3 wk.Outcome measurements and statistical analysis: The main end point was prostate-specific antigen (PSA) response rate. Secondary end points included time to PSAprogression, radiologic response rate using Response Evaluation Criteria In Solid Tumors(RECIST), and safety.Results and limitations: The intermittent dexamethasone arm was dropped after noresponse was seen in seven patients. By intention to treat, confirmed PSA response wasseen in 41% versus 22% for daily dexamethasone versus prednisolone, respectively( p = 0.08). In evaluable patients, the PSA response rates were 47% versus 24% fordexamethasone and prednisolone, respectively ( p = 0.05). Median time to PSA progres-sion was 9.7 mo on dexamethasone versus 5.1 mo on prednisolone (hazard ratio: 1.6;95% confidence interval, 0.9–2.8). In 43 patients with measurable disease, the responserate by RECIST was 15% and 6% for dexamethasone and prednisolone, respectively( p = 0.6). Of 23 patients who crossed over at PSA progression on prednisolone, 7 of the19 evaluable (37%) had a confirmed PSA response to dexamethasone. Clinically signifi-cant toxicities were rare.Conclusions: Dexamethasone may be more active than prednisolone in CRPC. In theabsence of more definitive trials, dexamethasone should be used in preference toprednisolone.Patient summary: We compared two different steroids used for treating men withadvanced prostate cancer. Our results suggest that dexamethasone may be moreeffective than prednisolone and that both are well tolerated.Clinical trial registry: EUDRAC 2005-006018-16
# 2014 European Association of Urology. Published by Elsevier B.V. All rights reserved.
. Royal Marsden Hospital, Academic Urology Unit, Downs Road, Sutton, SM2661 3425; Fax: +44 020 8643 8809.
* Corresponding author5PT, UK. Tel. +44 020 8
E-mail address: chris.parkehttp://dx.doi.org/10.1016/j.eururo.2014.10.0040302-2838/# 2014 European Association of Urology. Published by Elsevier
[email protected] (C. Parker).
B.V. All rights reserved.
E U R O P E A N U R O L O G Y 6 7 ( 2 0 1 5 ) 6 7 3 – 6 7 9674
1. Introduction
Prednisolone is widely used as secondary hormonal treat-
ment for patients with castration-resistant prostate cancer
(CRPC) [1]. Several corticosteroids, including hydrocortisone
and dexamethasone, have also achieved favourable symp-
tomatic, biochemical, and radiologic responses [2–4]. It has
been assumed that corticosteroids are active in CRPC by
suppression of adrenal androgen production. Hence, one
would expect any corticosteroid that suppresses adrenocor-
ticotrophic hormone (ACTH) to be equally effective [1]. Pred-
nisolone is also used in combination with cytotoxic
chemotherapy and with abiraterone to ameliorate the
toxicities of treatment in patients with metastatic CRPC [5,6].
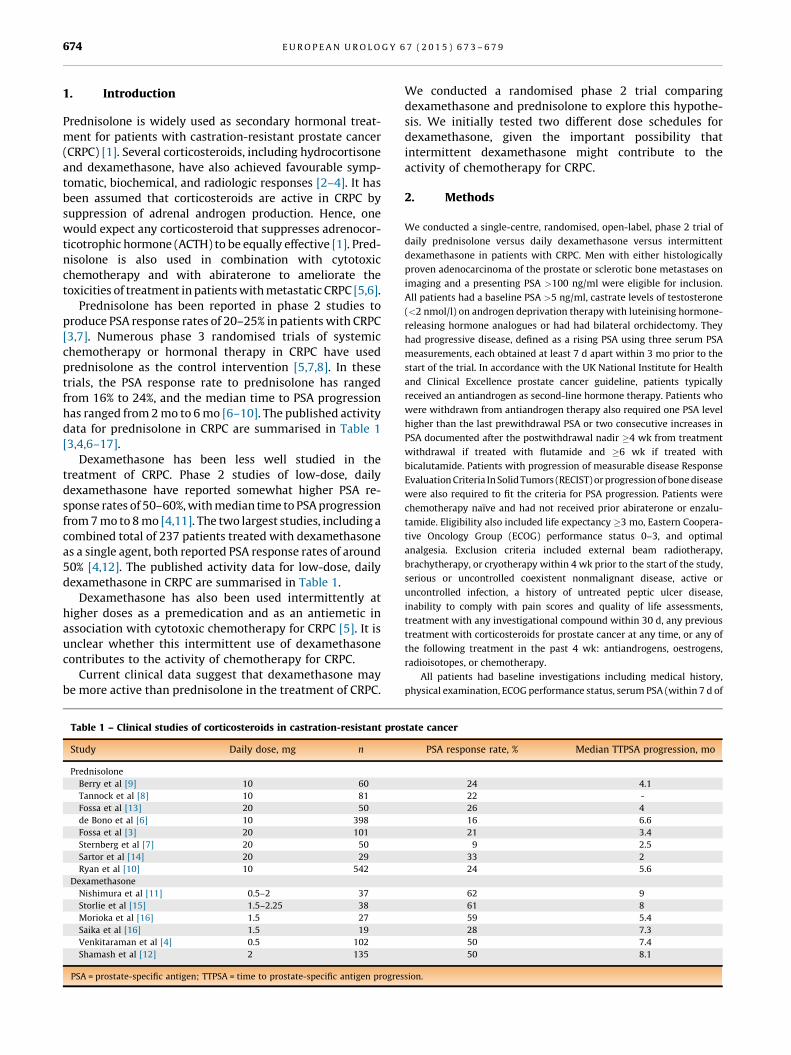
Prednisolone has been reported in phase 2 studies to
produce PSA response rates of 20–25% in patients with CRPC
[3,7]. Numerous phase 3 randomised trials of systemic
chemotherapy or hormonal therapy in CRPC have used
prednisolone as the control intervention [5,7,8]. In these
trials, the PSA response rate to prednisolone has ranged
from 16% to 24%, and the median time to PSA progression
has ranged from 2 mo to 6 mo [6–10]. The published activity
data for prednisolone in CRPC are summarised in Table 1
[3,4,6–17].
Dexamethasone has been less well studied in the
treatment of CRPC. Phase 2 studies of low-dose, daily
dexamethasone have reported somewhat higher PSA re-
sponse rates of 50–60%, with median time to PSA progression
from 7 mo to 8 mo [4,11]. The two largest studies, including a
combined total of 237 patients treated with dexamethasone
as a single agent, both reported PSA response rates of around
50% [4,12]. The published activity data for low-dose, daily
dexamethasone in CRPC are summarised in Table 1.
Dexamethasone has also been used intermittently at
higher doses as a premedication and as an antiemetic in
association with cytotoxic chemotherapy for CRPC [5]. It is
unclear whether this intermittent use of dexamethasone
contributes to the activity of chemotherapy for CRPC.
Current clinical data suggest that dexamethasone may
be more active than prednisolone in the treatment of CRPC.
Table 1 – Clinical studies of corticosteroids in castration-resistant pro
Study Daily dose, mg n
Prednisolone
Berry et al [9] 10 60
Tannock et al [8] 10 81
Fossa et al [13] 20 50
de Bono et al [6] 10 398
Fossa et al [3] 20 101
Sternberg et al [7] 20 50
Sartor et al [14] 20 29
Ryan et al [10] 10 542
Dexamethasone
Nishimura et al [11] 0.5–2 37
Storlie et al [15] 1.5–2.25 38
Morioka et al [16] 1.5 27
Saika et al [16] 1.5 19
Venkitaraman et al [4] 0.5 102
Shamash et al [12] 2 135
PSA = prostate-specific antigen; TTPSA = time to prostate-specific antigen progres
We conducted a randomised phase 2 trial comparing
dexamethasone and prednisolone to explore this hypothe-
sis. We initially tested two different dose schedules for
dexamethasone, given the important possibility that
intermittent dexamethasone might contribute to the
activity of chemotherapy for CRPC.
2. Methods
We conducted a single-centre, randomised, open-label, phase 2 trial of
daily prednisolone versus daily dexamethasone versus intermittent
dexamethasone in patients with CRPC. Men with either histologically
proven adenocarcinoma of the prostate or sclerotic bone metastases on
imaging and a presenting PSA >100 ng/ml were eligible for inclusion.
All patients had a baseline PSA >5 ng/ml, castrate levels of testosterone
(<2 nmol/l) on androgen deprivation therapy with luteinising hormone-
releasing hormone analogues or had had bilateral orchidectomy. They
had progressive disease, defined as a rising PSA using three serum PSA
measurements, each obtained at least 7 d apart within 3 mo prior to the
start of the trial. In accordance with the UK National Institute for Health
and Clinical Excellence prostate cancer guideline, patients typically
received an antiandrogen as second-line hormone therapy. Patients who
were withdrawn from antiandrogen therapy also required one PSA level
higher than the last prewithdrawal PSA or two consecutive increases in
PSA documented after the postwithdrawal nadir �4 wk from treatment
withdrawal if treated with flutamide and �6 wk if treated with
bicalutamide. Patients with progression of measurable disease Response
Evaluation Criteria In Solid Tumors (RECIST) or progression of bone disease
were also required to fit the criteria for PSA progression. Patients were
chemotherapy naıve and had not received prior abiraterone or enzalu-
tamide. Eligibility also included life expectancy �3 mo, Eastern Coopera-
tive Oncology Group (ECOG) performance status 0–3, and optimal
analgesia. Exclusion criteria included external beam radiotherapy,
brachytherapy, or cryotherapy within 4 wk prior to the start of the study,
serious or uncontrolled coexistent nonmalignant disease, active or
uncontrolled infection, a history of untreated peptic ulcer disease,
inability to comply with pain scores and quality of life assessments,
treatment with any investigational compound within 30 d, any previous
treatment with corticosteroids for prostate cancer at any time, or any of
the following treatment in the past 4 wk: antiandrogens, oestrogens,
radioisotopes, or chemotherapy.
All patients had baseline investigations including medical history,
physical examination, ECOG performance status, serum PSA (within 7 d of
state cancer
PSA response rate, % Median TTPSA progression, mo
24 4.1
22 -
26 4
16 6.6
21 3.4
9 2.5
33 2
24 5.6
62 9
61 8
59 5.4
28 7.3
50 7.4
50 8.1
sion.
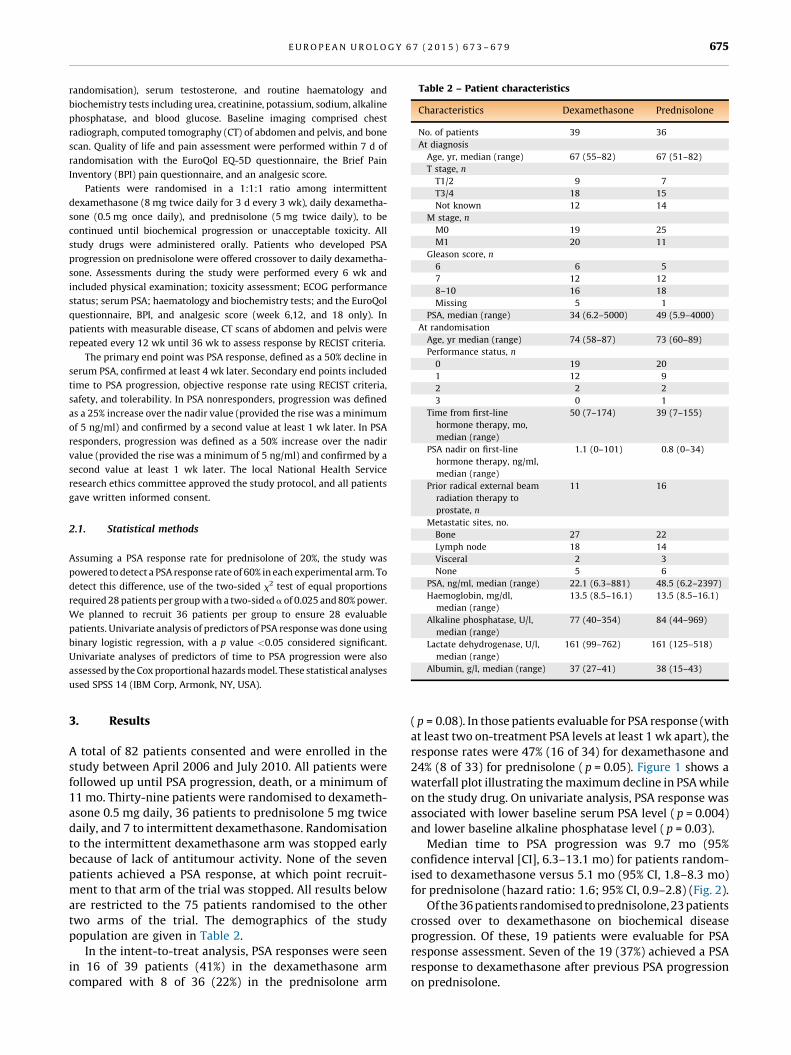
Table 2 – Patient characteristics
Characteristics Dexamethasone Prednisolone
No. of patients 39 36
At diagnosis
Age, yr, median (range) 67 (55–82) 67 (51–82)
T stage, n
T1/2 9 7
T3/4 18 15
Not known 12 14
M stage, n
M0 19 25
M1 20 11
Gleason score, n
6 6 5
7 12 12
8–10 16 18
Missing 5 1
PSA, median (range) 34 (6.2–5000) 49 (5.9–4000)
At randomisation
Age, yr median (range) 74 (58–87) 73 (60–89)
Performance status, n
0 19 20
1 12 9
2 2 2
3 0 1
Time from first-line
hormone therapy, mo,
median (range)
50 (7–174) 39 (7–155)
PSA nadir on first-line
hormone therapy, ng/ml,
median (range)
1.1 (0–101) 0.8 (0–34)
Prior radical external beam
radiation therapy to
prostate, n
11 16
Metastatic sites, no.
Bone 27 22
Lymph node 18 14
Visceral 2 3
None 5 6
PSA, ng/ml, median (range) 22.1 (6.3–881) 48.5 (6.2–2397)
Haemoglobin, mg/dl,
median (range)
13.5 (8.5–16.1) 13.5 (8.5–16.1)
Alkaline phosphatase, U/l,
median (range)
77 (40–354) 84 (44–969)
Lactate dehydrogenase, U/l,
median (range)
161 (99–762) 161 (125–518)
Albumin, g/l, median (range) 37 (27–41) 38 (15–43)
E U R O P E A N U R O L O G Y 6 7 ( 2 0 1 5 ) 6 7 3 – 6 7 9 675
randomisation), serum testosterone, and routine haematology and
biochemistry tests including urea, creatinine, potassium, sodium, alkaline
phosphatase, and blood glucose. Baseline imaging comprised chest
radiograph, computed tomography (CT) of abdomen and pelvis, and bone
scan. Quality of life and pain assessment were performed within 7 d of
randomisation with the EuroQol EQ-5D questionnaire, the Brief Pain
Inventory (BPI) pain questionnaire, and an analgesic score.
Patients were randomised in a 1:1:1 ratio among intermittent
dexamethasone (8 mg twice daily for 3 d every 3 wk), daily dexametha-
sone (0.5 mg once daily), and prednisolone (5 mg twice daily), to be
continued until biochemical progression or unacceptable toxicity. All
study drugs were administered orally. Patients who developed PSA
progression on prednisolone were offered crossover to daily dexametha-
sone. Assessments during the study were performed every 6 wk and
included physical examination; toxicity assessment; ECOG performance
status; serum PSA; haematology and biochemistry tests; and the EuroQol
questionnaire, BPI, and analgesic score (week 6,12, and 18 only). In
patients with measurable disease, CT scans of abdomen and pelvis were
repeated every 12 wk until 36 wk to assess response by RECIST criteria.
The primary end point was PSA response, defined as a 50% decline in
serum PSA, confirmed at least 4 wk later. Secondary end points included
time to PSA progression, objective response rate using RECIST criteria,
safety, and tolerability. In PSA nonresponders, progression was defined
as a 25% increase over the nadir value (provided the rise was a minimum
of 5 ng/ml) and confirmed by a second value at least 1 wk later. In PSA
responders, progression was defined as a 50% increase over the nadir
value (provided the rise was a minimum of 5 ng/ml) and confirmed by a
second value at least 1 wk later. The local National Health Service
research ethics committee approved the study protocol, and all patients
gave written informed consent.
2.1. Statistical methods
Assuming a PSA response rate for prednisolone of 20%, the study was
powered to detect a PSA response rate of 60% in each experimental arm. To
detect this difference, use of the two-sided x2 test of equal proportions
required 28 patients per group with a two-sided a of 0.025 and 80% power.
We planned to recruit 36 patients per group to ensure 28 evaluable
patients. Univariate analysis of predictors of PSA response was done using
binary logistic regression, with a p value <0.05 considered significant.
Univariate analyses of predictors of time to PSA progression were also
assessed by the Cox proportional hazards model. These statistical analyses
used SPSS 14 (IBM Corp, Armonk, NY, USA).
3. Results
A total of 82 patients consented and were enrolled in the
study between April 2006 and July 2010. All patients were
followed up until PSA progression, death, or a minimum of
11 mo. Thirty-nine patients were randomised to dexameth-
asone 0.5 mg daily, 36 patients to prednisolone 5 mg twice
daily, and 7 to intermittent dexamethasone. Randomisation
to the intermittent dexamethasone arm was stopped early
because of lack of antitumour activity. None of the seven
patients achieved a PSA response, at which point recruit-
ment to that arm of the trial was stopped. All results below
are restricted to the 75 patients randomised to the other
two arms of the trial. The demographics of the study
population are given in Table 2.
In the intent-to-treat analysis, PSA responses were seen
in 16 of 39 patients (41%) in the dexamethasone arm
compared with 8 of 36 (22%) in the prednisolone arm
( p = 0.08). In those patients evaluable for PSA response (with
at least two on-treatment PSA levels at least 1 wk apart), the
response rates were 47% (16 of 34) for dexamethasone and
24% (8 of 33) for prednisolone ( p = 0.05). Figure 1 shows a
waterfall plot illustrating the maximum decline in PSA while
on the study drug. On univariate analysis, PSA response was
associated with lower baseline serum PSA level ( p = 0.004)
and lower baseline alkaline phosphatase level ( p = 0.03).
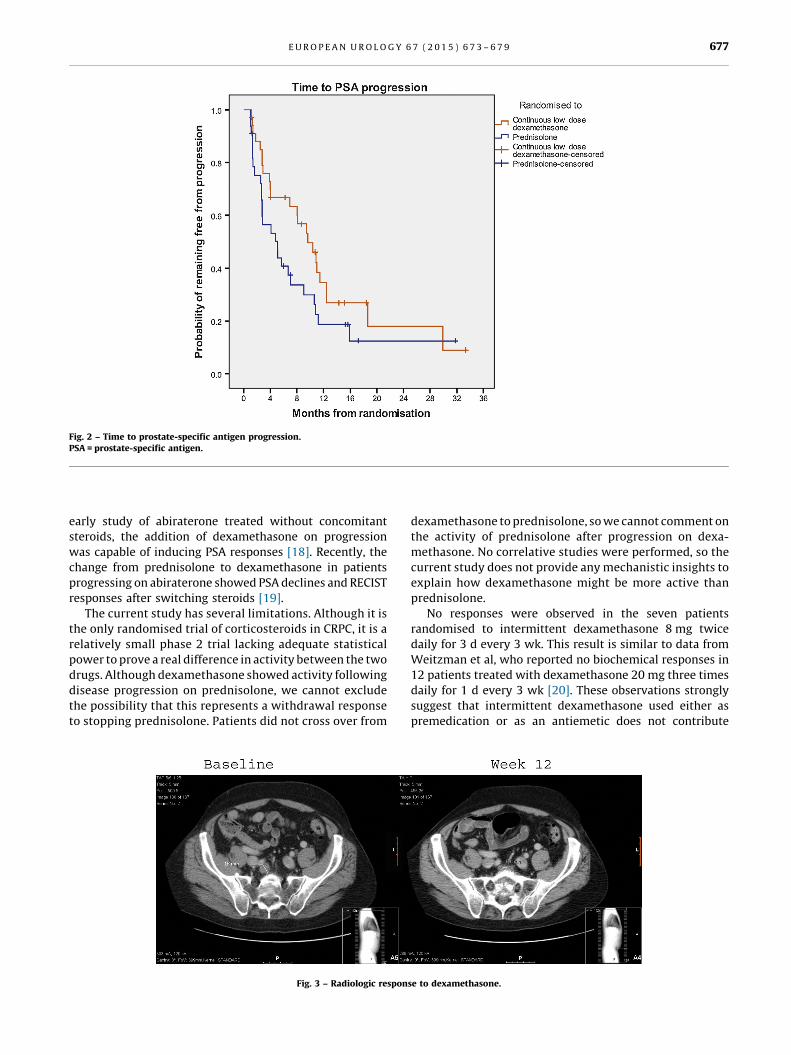
Median time to PSA progression was 9.7 mo (95%
confidence interval [CI], 6.3–13.1 mo) for patients random-
ised to dexamethasone versus 5.1 mo (95% CI, 1.8–8.3 mo)
for prednisolone (hazard ratio: 1.6; 95% CI, 0.9–2.8) (Fig. 2).
Of the 36 patients randomised to prednisolone, 23 patients
crossed over to dexamethasone on biochemical disease
progression. Of these, 19 patients were evaluable for PSA
response assessment. Seven of the 19 (37%) achieved a PSA
response to dexamethasone after previous PSA progression
on prednisolone.
[(Fig._1)TD$FIG]
100%(a)
(b)
80%
60%
40%
20%
0%
-20%
-40%
-60%
-80%
-100%
100%
80%
60%
40%
20%
0%
-20%
-40%
-60%
-80%
-100%
Per
cent
cha
nge
from
bas
elin
e to
nad
irP
erce
nt c
hang
e fro
m b
asel
ine
to n
adir
Continuous low dose dexamethasone
Continuous low dose dexamethasonePrednisolone
Prednisolone
Maximum PSA fall from baseline
Maximum PSA fall from baseline to 12 wk
Fig. 1 – Maximum prostate-specific antigen decline by study drug (a) at any time on initial study drug treatment and (b) within the first 12 wk.PSA = prostate-specific antigen.
E U R O P E A N U R O L O G Y 6 7 ( 2 0 1 5 ) 6 7 3 – 6 7 9676
A total of 43 patients had measurable disease at baseline.
The objective response rates by RECIST criteria were 15%
(3 of 20) and 6% (1 of 18) for dexamethasone and
prednisolone, respectively ( p = 0.6). Figure 3 illustrates an
objective response to dexamethasone. This patient, with a
pretreatment PSA of 47 ng/ml, obtained a complete response
to dexamethasone on CT scan and an undetectable PSA of
<0.04 ng/ml. His serum PSA remains undetectable after
treatment with dexamethasone for 44 mo.
Thirteen patients in each treatment group were on
analgesia at baseline. Pain scores, analgesic use, and EQ-5D
health scores improved during study treatment, with no
significant difference between treatments but with a trend
for greater improvement in pain for dexamethasone rather
than prednisolone (Table 3). Clinically significant toxicities
were uncommon (Table 4). No significant difference was
seen between the two study drugs with regard to safety and
tolerability. Fifty-one patients were normoglycaemic at
baseline. Of these, 14 of 25 on dexamethasone had at least
one glucose level >6 mmol/l versus 20 of 26 on predniso-
lone. Three patients on prednisolone versus none on
dexamethasone had at least one random glucose level
>12 mmol/l.
4. Discussion
This study is the only completed randomised comparison of
different corticosteroids in CRPC. The results are consistent
with the hypothesis that dexamethasone 0.5 mg daily is
more active than prednisolone 10 mg daily in the treatment
of CRPC. It is noteworthy that a significant proportion of
patients (7 of 19, 36%) achieved a PSA response to
dexamethasone after PSA progression on prednisolone.
The data are in keeping with the previously reported
activity of these agents in nonrandomised clinical trials of
prednisolone and dexamethasone in CRPC (Table 1). In an
[(Fig._2)TD$FIG]
Fig. 2 – Time to prostate-specific antigen progression.PSA = prostate-specific antigen.
E U R O P E A N U R O L O G Y 6 7 ( 2 0 1 5 ) 6 7 3 – 6 7 9 677
early study of abiraterone treated without concomitant
steroids, the addition of dexamethasone on progression
was capable of inducing PSA responses [18]. Recently, the
change from prednisolone to dexamethasone in patients
progressing on abiraterone showed PSA declines and RECIST
responses after switching steroids [19].
The current study has several limitations. Although it is
the only randomised trial of corticosteroids in CRPC, it is a
relatively small phase 2 trial lacking adequate statistical
power to prove a real difference in activity between the two
drugs. Although dexamethasone showed activity following
disease progression on prednisolone, we cannot exclude
the possibility that this represents a withdrawal response
to stopping prednisolone. Patients did not cross over from
[(Fig._3)TD$FIG]
Fig. 3 – Radiologic respon
dexamethasone to prednisolone, so we cannot comment on
the activity of prednisolone after progression on dexa-
methasone. No correlative studies were performed, so the
current study does not provide any mechanistic insights to
explain how dexamethasone might be more active than
prednisolone.
No responses were observed in the seven patients
randomised to intermittent dexamethasone 8 mg twice
daily for 3 d every 3 wk. This result is similar to data from
Weitzman et al, who reported no biochemical responses in
12 patients treated with dexamethasone 20 mg three times
daily for 1 d every 3 wk [20]. These observations strongly
suggest that intermittent dexamethasone used either as
premedication or as an antiemetic does not contribute
se to dexamethasone.
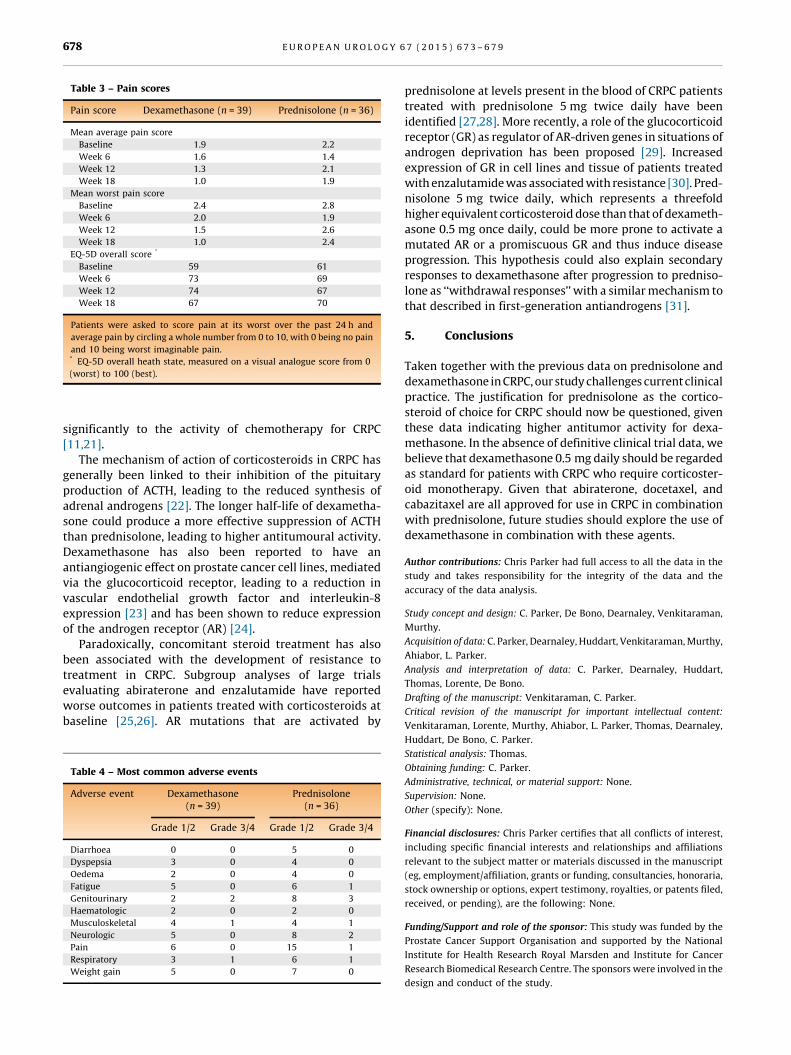
Table 3 – Pain scores
Pain score Dexamethasone (n = 39) Prednisolone (n = 36)
Mean average pain score
Baseline 1.9 2.2
Week 6 1.6 1.4
Week 12 1.3 2.1
Week 18 1.0 1.9
Mean worst pain score
Baseline 2.4 2.8
Week 6 2.0 1.9
Week 12 1.5 2.6
Week 18 1.0 2.4
EQ-5D overall score *
Baseline 59 61
Week 6 73 69
Week 12 74 67
Week 18 67 70
Patients were asked to score pain at its worst over the past 24 h and
average pain by circling a whole number from 0 to 10, with 0 being no pain
and 10 being worst imaginable pain.* EQ-5D overall heath state, measured on a visual analogue score from 0
(worst) to 100 (best).
E U R O P E A N U R O L O G Y 6 7 ( 2 0 1 5 ) 6 7 3 – 6 7 9678
significantly to the activity of chemotherapy for CRPC
[11,21].
The mechanism of action of corticosteroids in CRPC has
generally been linked to their inhibition of the pituitary
production of ACTH, leading to the reduced synthesis of
adrenal androgens [22]. The longer half-life of dexametha-
sone could produce a more effective suppression of ACTH
than prednisolone, leading to higher antitumoural activity.
Dexamethasone has also been reported to have an
antiangiogenic effect on prostate cancer cell lines, mediated
via the glucocorticoid receptor, leading to a reduction in
vascular endothelial growth factor and interleukin-8
expression [23] and has been shown to reduce expression
of the androgen receptor (AR) [24].
Paradoxically, concomitant steroid treatment has also
been associated with the development of resistance to
treatment in CRPC. Subgroup analyses of large trials
evaluating abiraterone and enzalutamide have reported
worse outcomes in patients treated with corticosteroids at
baseline [25,26]. AR mutations that are activated by
Table 4 – Most common adverse events
Adverse event Dexamethasone(n = 39)
Prednisolone(n = 36)
Grade 1/2 Grade 3/4 Grade 1/2 Grade 3/4
Diarrhoea 0 0 5 0
Dyspepsia 3 0 4 0
Oedema 2 0 4 0
Fatigue 5 0 6 1
Genitourinary 2 2 8 3
Haematologic 2 0 2 0
Musculoskeletal 4 1 4 1
Neurologic 5 0 8 2
Pain 6 0 15 1
Respiratory 3 1 6 1
Weight gain 5 0 7 0
prednisolone at levels present in the blood of CRPC patients
treated with prednisolone 5 mg twice daily have been
identified [27,28]. More recently, a role of the glucocorticoid
receptor (GR) as regulator of AR-driven genes in situations of
androgen deprivation has been proposed [29]. Increased
expression of GR in cell lines and tissue of patients treated
with enzalutamide was associated with resistance [30]. Pred-
nisolone 5 mg twice daily, which represents a threefold
higher equivalent corticosteroid dose than that of dexameth-
asone 0.5 mg once daily, could be more prone to activate a
mutated AR or a promiscuous GR and thus induce disease
progression. This hypothesis could also explain secondary
responses to dexamethasone after progression to predniso-
lone as ‘‘withdrawal responses’’ with a similar mechanism to
that described in first-generation antiandrogens [31].
5. Conclusions
Taken together with the previous data on prednisolone and
dexamethasone in CRPC, our study challenges current clinical
practice. The justification for prednisolone as the cortico-
steroid of choice for CRPC should now be questioned, given
these data indicating higher antitumor activity for dexa-
methasone. In the absence of definitive clinical trial data, we
believe that dexamethasone 0.5 mg daily should be regarded
as standard for patients with CRPC who require corticoster-
oid monotherapy. Given that abiraterone, docetaxel, and
cabazitaxel are all approved for use in CRPC in combination
with prednisolone, future studies should explore the use of
dexamethasone in combination with these agents.
Author contributions: Chris Parker had full access to all the data in the
study and takes responsibility for the integrity of the data and the
accuracy of the data analysis.
Study concept and design: C. Parker, De Bono, Dearnaley, Venkitaraman,
Murthy.
Acquisition of data: C. Parker, Dearnaley, Huddart, Venkitaraman, Murthy,
Ahiabor, L. Parker.
Analysis and interpretation of data: C. Parker, Dearnaley, Huddart,
Thomas, Lorente, De Bono.
Drafting of the manuscript: Venkitaraman, C. Parker.
Critical revision of the manuscript for important intellectual content:
Venkitaraman, Lorente, Murthy, Ahiabor, L. Parker, Thomas, Dearnaley,
Huddart, De Bono, C. Parker.
Statistical analysis: Thomas.
Obtaining funding: C. Parker.
Administrative, technical, or material support: None.
Supervision: None.
Other (specify): None.
Financial disclosures: Chris Parker certifies that all conflicts of interest,
including specific financial interests and relationships and affiliations
relevant to the subject matter or materials discussed in the manuscript
(eg, employment/affiliation, grants or funding, consultancies, honoraria,
stock ownership or options, expert testimony, royalties, or patents filed,
received, or pending), are the following: None.
Funding/Support and role of the sponsor: This study was funded by the
Prostate Cancer Support Organisation and supported by the National
Institute for Health Research Royal Marsden and Institute for Cancer
Research Biomedical Research Centre. The sponsors were involved in the
design and conduct of the study.
E U R O P E A N U R O L O G Y 6 7 ( 2 0 1 5 ) 6 7 3 – 6 7 9 679
References
[1] Khandwala HM, Vassilopoulou-Sellin R, Logethetis CJ, Friend KE.
Corticosteroid-induced inhibition of adrenal androgen production
in selected patients with prostate cancer. Endocr Pract 2001;7:
11–5.
[2] Tannock I, Gospodarowicz M, Meakin W, Panzarella T, Stewart L,
Rider W. Treatment of metastatic prostatic cancer with low-dose
prednisone: evaluation of pain and quality of life as pragmatic
indices of response. J Clin Oncol 1989;7:590–7.
[3] Fossa SD, Slee PH, Brausi M, et al. Flutamide versus prednisone in
patients with prostate cancer symptomatically progressing after
androgen-ablative therapy: a phase III study of the European
organization for research and treatment of cancer genitourinary
group. J Clin Oncol 2001;19:62–71.
[4] Venkitaraman R, Thomas K, Huddart RA, Horwich A, Dearnaley DP,
Parker CC. Efficacy of low-dose dexamethasone in castration-re-
fractory prostate cancer. BJU Int 2008;101:440–3.
[5] Tannock IF, de Wit R, Berry WR, et al. Docetaxel plus prednisone or
mitoxantrone plus prednisone for advanced prostate cancer. N Engl
J Med 2004;351:1502–12.
[6] De Bono JS, Logothetis CJ, Molina A, et al. Abiraterone and increased
survival in metastatic prostate cancer. N Engl J Med 2011;364:
1995–2005.
[7] Sternberg CN, Whelan P, Hetherington J, et al. Phase III trial of
satraplatin, an oral platinum plus prednisone vs. prednisone alone
in patients with hormone-refractory prostate cancer. Oncology
2005;68:2–9.
[8] Tannock IF, Osoba D, Stockler MR, et al. Chemotherapy with mitox-
antrone plus prednisone or prednisone alone for symptomatic
hormone-resistant prostate cancer: a Canadian randomized trial
with palliative end points. J Clin Oncol 1996;14:1756–64.
[9] Berry W, Dakhil S, Modiano M, Gregurich M, Asmar L. Phase III study
of mitoxantrone plus low dose prednisone versus low dose predni-
sone alone in patients with asymptomatic hormone refractory
prostate cancer. J Urol 2002;168:2439–43.
[10] Ryan CJ, Smith MR, de Bono JS, et al. Abiraterone in metastatic
prostate cancer without previous chemotherapy. N Engl J Med
2013;368:138–48.
[11] Nishimura K, Nonomura N, Yasunaga Y, et al. Low doses of oral
dexamethasone for hormone-refractory prostate carcinoma. Can-
cer 2000;89:2570–6.
[12] Shamash J, Powles T, Sarker SJ, et al. A multi-centre randomised
phase III trial of dexamethasone vs dexamethasone and diethyl-
stilbestrol in castration-resistant prostate cancer: immediate vs
deferred diethylstilbestrol. Br J Cancer 2011;104:620–8.
[13] Fossa SD, Jacobsen A-B, Ginman C, et al. Weekly docetaxel and
prednisolone versus prednisolone alone in androgen-independent
prostate cancer: a randomized phase II study. Eur Urol 2007;52:
1691–9.
[14] Sartor O, Weinberger M, Moore A, Li A, Figg WD. Effect of predni-
sone on prostate-specific antigen in patients with hormone-refrac-
tory prostate cancer. Urology 1998;52:252–6.
[15] Storlie JA, Buckner JC, Wiseman GA, Burch PA, Hartmann LC,
Richardson RL. Prostate specific antigen levels and clinical response
to low dose dexamethasone for hormone-refractory metastatic
prostate carcinoma. Cancer 1995;76:96–100.
[16] Morioka M, Kobayashi T, Furukawa Y, et al. Prostate-specific antigen
levels and prognosis in patients with hormone-refractory prostate
cancer treated with low-dose dexamethasone. Urol Int 2002;68:10–5.
[17] Saika T, Kusaka N, Tsushima T, et al. Okayama Urological Cancer
Collaborating Group. Treatment of androgen-independent prostate
cancer with dexamethasone: a prospective study in stage D2
patients. Int J Urol 2001;8:290–4.
[18] Attard G, Reid AHM, de Bono JS. Abiraterone acetate is well toler-
ated without concomitant use of corticosteroids. J Clin Oncol
2010;28:e560–1, author reply e562.
[19] Lorente D, Weatherstone K, Omlin A, et al. Tumor responses after
steroid switch of prednisolone (P) to dexamethasone (D) in castra-
tion-resistant prostate cancer (CRPC) patients (pts) on abiraterone
acetate (AA) [abstract 2918]. Eur J Cancer 2013:49.
[20] Weitzman AL, Shelton G, Zuech N, et al. Dexamethasone does not
significantly contribute to the response rate of docetaxel and estra-
mustine in androgen independent prostate cancer. J Urol 2000;163:
834–7.
[21] Dorff TB, Crawford ED. Management and challenges of corticoster-
oid therapy in men with metastatic castrate-resistant prostate
cancer. Ann Oncol 2013;24:31–8.
[22] Eichholz A, Ferraldeschi R, Attard G, de Bono JS. Putting the brakes
on continued androgen receptor signaling in castration-resistant
prostate cancer. Mol Cell Endocrinol 2012;360:68–75.
[23] Yano A, Fujii Y, Iwai A, Kageyama Y, Kihara K. Glucocorticoids
suppress tumor angiogenesis and in vivo growth of prostate cancer
cells. Clin Cancer Res 2006;12:3003–9.
[24] Nishimura K, Nonomura N, Satoh E, et al. Potential mechanism for
the effects of dexamethasone on growth of androgen-independent
prostate cancer. J Natl Cancer Inst 2001;93:1739–46.
[25] Montgomery RB, Kheoh TS, Molina A, et al. Effect of corticosteroid
(CS) use at baseline (CUB) on overall survival (OS) in patients (pts)
receiving abiraterone acetate (AA): Results from a randomized
study (COU-AA-301) in metastatic castration-resistant prostate
cancer (mCRPC) post-docetaxel (D) [abstract 5014]. J Clin Oncol
2013;31(Suppl).
[26] Scher HI, Fizazi K, Saad F, et al. Impact of on-study corticosteroid
use on efficacy and safety in the phase III AFFIRM study of enza-
lutamide (ENZA), an androgen receptor inhibitor [abstract 6]. J Clin
Oncol 2013;31(Suppl).
[27] Zhao XY, Malloy PJ, Krishnan AV, et al. Glucocorticoids can promote
androgen-independent growth of prostate cancer cells through a
mutated androgen receptor. Nat Med 2000;6:703–6.
[28] Richards J, Lim AC, Hay CW, et al. Interactions of abiraterone,
eplerenone, and prednisolone with wild-type and mutant androgen
receptor: a rationale for increasing abiraterone exposure or com-
bining with MDV3100. Cancer Res 2012;72:2176–82.
[29] Sahu B, Laakso M, Pihlajamaa P, et al. FoxA1 specifies unique
androgen and glucocorticoid receptor binding events in prostate
cancer cells. Cancer Res 2013;73:1570–80.
[30] Arora VK, Schenkein E, Murali R, et al. Glucocorticoid receptor
confers resistance to antiandrogens by bypassing androgen recep-
tor blockade. Cell 2013;155:1309–22.
[31] Small EJ, Halabi S, Dawson NA, et al. Antiandrogen withdrawal
alone or in combination with ketoconazole in androgen-indepen-
dent prostate cancer patients: a phase III trial (CALGB 9583). J Clin
Oncol 2004;22:1025–33.