a proposed glossary for dialysis kinetics
TRANSCRIPT

EDITORIAL OPINION
A Proposed Glossary for Dialysis Kinetics Joel D. Kopple, MD, Michael R. Jones, PhD, Prakash R. Keshaviah, PhD,
Jonas Bergstrijm, MD, Robert M. Lindsay, MD, John Moran, MD, Karl D. Nolph, MD, and Brendan P. Teehan, MD
0 Quantification of the dialysis dose and assessment of nutritional status and response to nutritional therapy have become standard parts of the management of the chronic dialysis patient. Atthough advances in these areas have led to a more rational basis for therapy, certain misconceptions and points of confusion appear to have occurred. Recognizing the importance of a standard nomenclature to the development of concepts and the communication of research findings, we have attempted to compile a list of terms that are commonly used in the field of dialysis. New terms have been proposed for current ones that do not seem adequate. In addition, we have discussed potential methodologies for obtaining more accurate data for dialysis kinetics and for precise monitoring of nutritional intake and status. lt is hoped that this glossary will stimulate discussion that will lead to refinements in terminology and concepts that will, in turn, improve research and practice in nephrology. It is anticipated that many of these definitions and recommendations will be modiii or superseded as the management of patients with renal failure continues to advance. 0 1995 by the National Kidney Foundation, Inc.
INDEX WORDS Protein catabolic rate; anthropometry; urea kinetics; urea nitrogen appearance; Protein equivalent of nitrogen appearance; dialysis dose; nutrition; hemodialysis; peritoneal dialysis; renal failure.
T HE DEVELOPMENT of a kinetic and quantitative approach to the prescription of
dialysis therapy and the assessment of adequacy of dialysis treatment by Gotch, Sargent, and other researchers was a major advance toward placing maintenance dialysis treatment on a rational ba- sis.‘-16 These innovative steps have resulted in a more systematic and rational approach to the management of patients with end-stage renal dis- ease. However, there appears to be some confu- sion regarding the terms used for dialysis quanti- fication and, hence, there is potential for both conceptual errors and misinterpretation of data. This is also true with regard to the calculation and normalization of estimates of dietary protein intake (DPI) and the characterization of body mass.
Due to these concerns, we have re-examined the terms used for the estimation of nitrogen out- put, DPI, and quantification of dialysis dose. The goal was to develop a glossary of terms that would be less confusing, more precise, and widely accepted by clinicians and investigators in this field. There appears to be consensus with regard to the definitions of some terms. However, there is considerable variance in the meaning and interpretation of other terms, particularly those concerning nutritional status. In the latter in- stances, we will discuss the issues surrounding the controversial terms and make recommenda- tions for their standardization. Many of the defi-
nitions of nutritional status are standard or com- monly used in the nutrition community. It is hoped that all the definitions in this glossary eventually will be validated by experimental studies.
Considerable discussion was devoted to the term “protein catabolic rate” (PCR) for estimat- ing DPI from urea appearance. In addition, par- ticular attention was given to the different meth- ods for standardizing protein intake and small molecule clearance to body mass or fluid volume. For example, the terms “body weight,” “ideal body weight,” and “dry weight” are used in different ways by investigators. Some of these terms have traditional and precise definitions in the nutrition literature. To use these terms in a different way for dialysis patients introduces the likelihood for confusion and error. For those
From Harbor-UCLA Medical Center, Torrance, CA, and UCLA Schools of Medicine and Public Health; Renal Divi- sion, Research Group, Baxter Healthcare, McGaw Park, IL: Karolinska Institute, Huddinge. Sweden; Victoria Hospital, London, Ontario, Canada; University of Missouri, Columbia, MO: and Lankenau Hospital, Philadelphia, PA.
Received August 8, 1995; accepted in revised form August 11, 1995.
Address reprint requests to Joel D. Kopple, MD, Division of Nephrology and Hypertension, Harbor-UCLA Medical Center, 1000 W Carson St, Torrance, CA 90509.
0 1995 by the National Kidney Foundation, Inc. 0272-6386/95/2606-0014$3.00/O
American Journal of Kidney Diseases, Vol26, No 6 (December), 1995: pp 963-981 963

964 KOPPLE ET AL
terms, such as relative or desirable body weight (DBW) and lean body mass, which have a well- defined meaning, the traditional definitions have been retained to be consistent with the other med- ical disciplines. We also have proposed some new definitions that are especially appropriate for the dialysis community. We therefore attempted to bring together, in one list, definitions of these and other quantities that are both accurate and practical. Although several excellent reviews and books have been written on kinetic modeling, to our knowledge, there is not a concise list of terms that can be referred to by investigators in the field.
It is hoped that these revised definitions and the attendant discussion concerning the rationale for the proposed changes will lead to improved clarity of thinking regarding dialysis-related treatment and research. We believe that the de- velopment of techniques for the quantification of dialysis therapy and the measurement of the uremic and nutritional status of renal failure pa- tients is an iterative process. These methods and definitions should continue to undergo revision as new information is developed and more effec- tive techniques for quantification are devised.
ANTHROPOMETRIC PARAMETERS
Anthropometric parameters are used to assess nutritional status and standardize the dose of dial- ysis therapy. There is general agreement as to the meaning and use of the terms discussed below.
Actual Body Weight
An individual’s actual (ie, current) body weight (aBW) is usually expressed in kilograms. No adjustment is made in the aBW for an abnor- mal proportion of total body water (TBW) or fat. For patients undergoing peritoneal dialysis, body weight should be measured with the abdomen drained of fluid. Patients should be weighed ac- cording to a standardized protocol that indicates the type and amount of clothing that individuals may wear during weighing.
Dry Body Weight or Edema-Free Body Weight
The body weight of an individual who has no edema fluid and no abnormally high or low fraction of body water is usually expressed in kilograms. In practice, dry body weight is almost always estimated using clinical criteria, although
direct measurement of TBW as a percentage of body weight may be more accurate. Examples of current usage are (1) a body weight that is not associated with edema or hypertension, and (2) the lowest body weight that is not associated with an increase in malaise or muscle cramps or, in an individual who is not receiving blood pressure- lowering medication, with hypotension. This as- sessment should be performed when the rate of fluid removal has not exceeded approximately 1.0 to 1.2 L/hr, because greater rates of fluid removal often cause these symptoms before the edema-free body weight is attained. Hemodialy- sis patients who have a marked increase in TBW are particularly likely to have symptoms before the desirable amount of fluid is removed. All operational definitions of dry body weight have limitations, and it is perhaps most important to define the method by which dry body weight is estimated. For hemodialysis patients, the weight obtained postdialysis rather than predialysis usu- ally is closer to the dry body weight.
It is recognized that the aBW or edema-free body weight of a dialysis patient may be mark- edly abnormal. There is confusion in the litera- ture as to the method for assigning a weight goal or a standard reference weight to a given patient. We propose a standard weight, referred to as “normal body weight” (nBW), based on data from the US National Health and Nutrition Eval- uation Survey (NHANES).“.‘*
Normal Body Weight
Defined as the median body weight of normal Americans with the same age range, height, sex, and skeletal frame size as the individual in ques- tion, the nBW is expressed in kilograms. The values for normal individuals are obtained from the NHANES data, which are periodically up- dated on the basis of new surveys.“~‘* The extent to which the NHANES data are normative for individuals living in other nations or societies is not known. However, similar types of data are available for the indigenous populations of a number of countries.
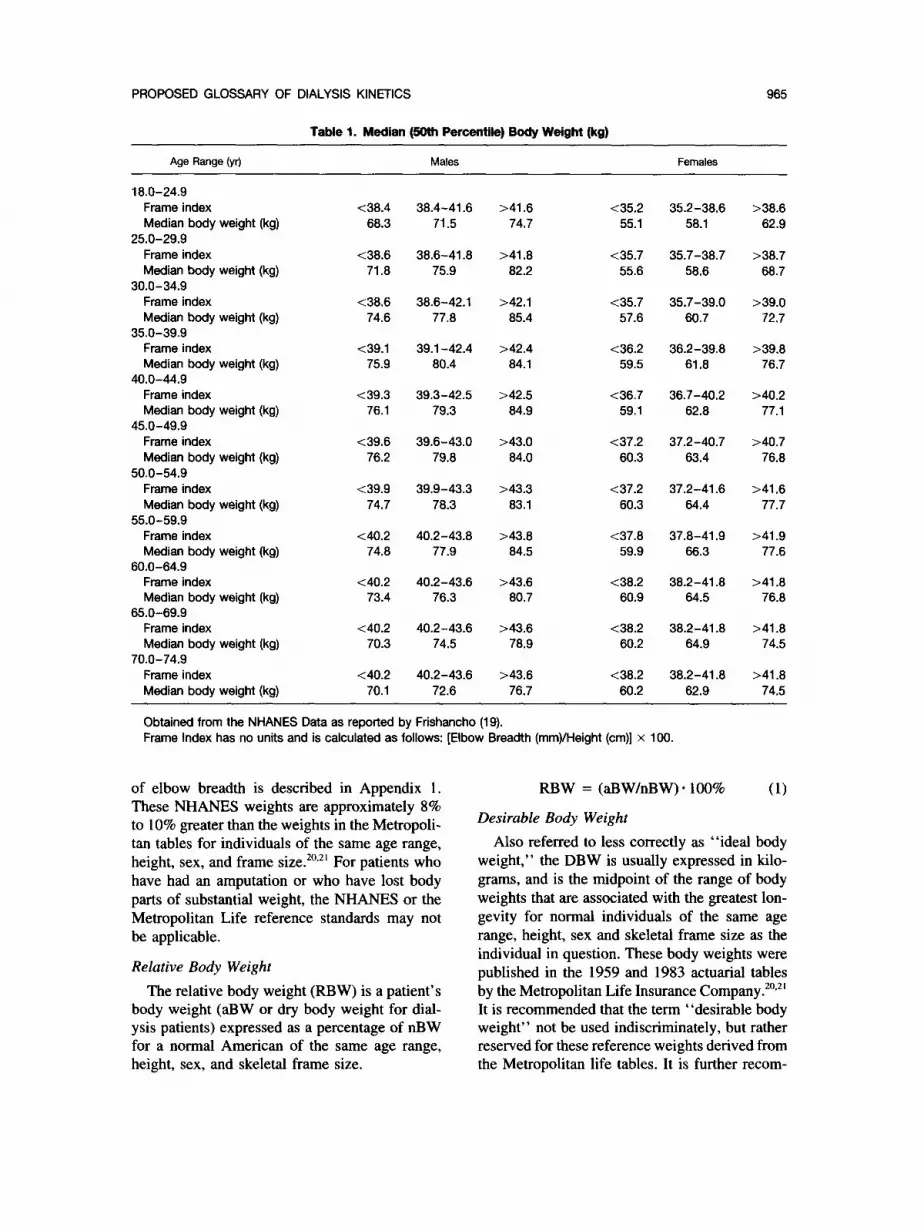
The reference median body weights obtained from the NHANES data are summarized in Table 1. It should be noted that height is not given in this table as a separate variable, but is combined with elbow breadth as an indicator of skeletal frame size” to give a frame index. Measurement
PROPOSED GLOSSARY OF DIALYSIS KINETICS
Table 1. Median (50th Percentile) BoUy Weight (kg)
965
Age Range(yr) Males Females
18.0-24.9 Frame index Median body weight (kg)
25.0-29.9 Frame index Median body weight (kg)
30.0-34.9 Frame index Median body weight (kg)
35.0-39.9 Frame index Median body weight (kg)
40.0-44.9 Frame index Median body weight (kg)
45.0-49.9 Frame index Median body weight (kg)
50.0-54.9 Frame index Median body weight (kg)
55.0-59.9 Frame index Median body weight (kg)
80.0-84.9 Frame index Median body weight (kg)
65.0-69.9 Frame index Median body weight (kg)
70.0-74.9 Frame index Median body weight (kg)
~38.4 38.4-41.6 >41.6 <35.2 35.2-38.6 >38.6 68.3 71.5 74.7 55.1 58.1 62.9
<38.6 38.6-41.8 >41.8 <35.7 35.7-38.7 >38.7 71.8 75.9 82.2 55.6 58.6 68.7
<38.6 38.6-42.1 >42.1 <35.7 35.7-39.0 >39.0 74.6 77.8 85.4 57.6 60.7 72.7
<39.1 39.1-42.4 >42.4 <36.2 36.2-39.8 >39.8 75.9 80.4 84.1 59.5 61.8 76.7
<39.3 39.3-42.5 >42.5 <36.7 36.7-40.2 >40.2 76.1 79.3 84.9 59.1 62.8 77.1
<39.6 39.6-43.0 >43.0 <37.2 37.2-40.7 >40.7 76.2 79.8 84.0 60.3 63.4 76.8
<39.9 39.9-43.3 >43.3 <37.2 37.2-41.6 >41.6 74.7 78.3 83.1 80.3 64.4 77.7
<40.2 40.2-43.6 >43.8 <37.8 37.8-41.9 >41.9 74.8 77.9 84.5 59.9 66.3 77.6
<40.2 40.2-43.6 73.4 76.3
<40.2 40.2-43.6 >43.6 <38.2 38.2-41.8 >41.8 70.3 74.5 78.9 60.2 84.9 74.5
<40.2 40.2-43.6 >43.8 <38.2 38.2-41.8 >41.8 70.1 72.6 76.7 60.2 62.9 74.5
>43.6 80.7
<38.2 60.9
38.2-41.8 >41.8 64.5 76.8
Obtained from the NHANES Data as reported by Frishancho (19). Frame Index has no units and is calculated as follows: [Elbow Breadth (mm)/Height (cm)] x 100.
of elbow breadth is described in Appendix 1. These NHANES weights are approximately 8% to 10% greater than the weights in the Metropoli- tan tables for individuals of the same age range, height, sex, and frame size.20s2’ For patients who have had an amputation or who have lost body parts of substantial weight, the NHANES or the Metropolitan Life reference standards may not be applicable.
Relative Body Weight The relative body weight (RBW) is a patient’s
body weight (aBW or dry body weight for dial- ysis patients) expressed as a percentage of nBW for a normal American of the same age range, height, sex, and skeletal frame size.
RBW = (aBW/nBW)* 100%
Desirable Body Weight
(1)
Also referred to less correctly as “ideal body weight,” the DBW is usually expressed in kilo- grams, and is the midpoint of the range of body weights that are associated with the greatest lon- gevity for normal individuals of the same age range, height, sex and skeletal frame size as the individual in question. These body weights were published in the 1959 and 1983 actuarial tables by the Metropolitan Life Insurance Company.20,2’ It is recommended that the term “desirable body weight” not be used indiscriminately, but rather reserved for these reference weights derived from the Metropolitan life tables. It is further recom-

966 KOPPLE ET AL
mended that the term “ideal body weight” not be used at all.
A patient’s aBW or dry weight may be ex- pressed as a percentage of DBW (%DBW):
%DBW = (aBW/DBW)* 100% (2)
In general, the nBW obtained from the NHANES data are preferable to the DBW from the Metropolitan Life data, primarily because of the quality of the information collected and the greater range of applicability to the whole popu- lation. An analysis of the strengths and weak- nesses of these databases, as reviewed by Robin- ett-Weiss et al,** is summarized in Appendix 2.
There is increasing use in the literature of the term “lean body mass.” We believe that this term, which often is used to denote nonobese body weight, edema-free body weight (ie, dry body weight), or muscle mass, has caused much confusion, and its use should be restricted to its precise, traditional definition.
Lean Body Mass
The total body mass or weight minus body fat is expressed in kilogram~.*~ Total body fat (kg) is estimated, usually from skinfold thickness measurements and equations relating these mea- surements to body fat.24 This definition of lean body mass is well-accepted and traditional, par- ticularly in the nutrition and body composition literature. Therefore, we believe that the defini- tion should not be changed. Lean body mass does not refer to muscle mass, body cell mass, dry body weight, nBW, or DBW. The use of lean body mass to indicate these latter meanings has caused much confusion. Since lean body mass, by definition, includes TBW, lean body mass will be large in edematous patients and small in dehy- drated or volume depleted individuals. For these reasons, we do not recommend that the protein equivalent of total nitrogen appearance (PNA; see below), DPI, or any dialysis kinetic measure- ments be normalized to lean body mass. Dry body weight, nBW, or DBW often will serve the purposes for which lean body mass has been currently used. Other parameters that might be used for standardization include total body nitro- gen, total body potassium, fat-free solids, or cre- atinine appearance. These latter parameters are not, as yet, widely accepted methods for charac-
terizing or standardizing body mass or muscle mass for patients with renal failure.
Body Su$ace Area
Body surface area (BSA) is the total surface area of the body, usually expressed in square meters and derived from height and weight. Body surface area can be estimated from a nomogram or the following equation?
BSA = 0.007 184 * aBW’.425 . Ht”.725 (3)
where aBW is expressed in kilograms and height (Ht) is expressed in centimeters.
Total Body Water
Total body water historically is estimated by the volume of distribution of labeled water or by underwater weighing and is usually expressed in liters.*” The use of tritiated or deuterated water to measure TBW is most accurate but is too labo- rious and expensive for routine clinical use. Total body water also may be measured by bioelectri- cal impedance, although currently there are some limitations to this method.27-2y In hemodialysis patients, urea kinetic modeling can be used to estimate TBW. The limitations to using urea ki- netic modeling to estimate TBW appear to be largely due to the time necessary for equilibration of the body urea pools with the plasma compart- ment and are discussed in the section below enti- tled Compartmental Disequilibrium. For perito- neal dialysis patients, estimates of TBW by urea kinetic modeling may be more difficult. In non- edematous hemodialysis or peritoneal dialysis patients, TBW may be estimated by the formula 0.58 * aBW (for men) or 0.55 * aBW (for women), or from the Watson or Hume-Weyers equa- tions.3.4”0’“l Although these methods are useful and probably sufficiently accurate under most circumstances, neither of these latter techniques has been carefully validated in chronic dialysis patients, and these approaches may not give an accurate estimate of TBW, at least for edema- tous, obese, or very thin dialysis patients.
Should Nutrient Intake and Dialysis Dose Be Related to Different Parameters of Body Mass?
A rationale can be advanced for relating nutri- tional requirements and dialysis dosage to differ- ent parameters of body mass. Many dietary nutri-

PROPOSED GLOSSARY OF DIALYSIS KINETICS 967
ent needs appear to be determined by body metabolic activity, which, in turn, may be related to the body pools of specific nutrients, especially protein.” Dietary energy requirements are de- fined by energy expenditure (eg, resting energy consumption, physical activity, the specific dy- namic action of foods, and, in growing individu- als, the energy requirement for growth”?). Dietary protein requirements are related to body protein mass. Thus, the prescription and assessment of adequacy of dietary energy and protein intake might be determined most physiologically ac- cording to the edema-free aBW, with modifica- tion for any special metabolic needs. Energy in- take should be further adjusted for physical activity. For patients who are obese or very thin, prescribing nutrient intake according to their aBW or nBW might lead to an excessively high or low intake. For example, a massively obese dialysis patient might be prescribed too much protein if the DPI were normalized to aBW or edema-free body weight. On the other hand, pre- scribing a DPI based on such an individual’s nBW might provide too little protein. The ad- justed body weight will help to rectify this di- lemma. For this reason, nutrient intake might be more appropriately normalized to an adjusted aBW. Such a method, which has been gaining in popularity but has not yet been validated by experimental data, is as follows’4:
Adjusted aBW = edema-free aBW
+ [(nBW - edema-free aBW) * 0.251 (4)
Since the current methods for prescribing or eval- uating dialysis dosage usually are based on urea removal (eg, KtN,,, and urea reduction ratio [URR], see below) and since urea seems to be a rather good marker of uremic toxicity, it seems appropriate to relate the dialysis urea clearance to the volume of distribution of urea (V).
ASSESSMENT OF DIETARY PROTEIN INTAKE
Dietary protein intake usually is measured or calculated for a 24-hour cycle. The DPI can be expressed in absolute units, such as grams of pro- tein per day, or may be factored by a number of terms, including the patient’s edema-free aBW, nBW, or adjusted aBW, as indicated above. We recommend that the method for weight adjustment of DPI always be clearly stated and that it be con-
sistent with the method of weight adjustment for the PNA (see below). There are direct and indirect methods for estimating the DPI, and these are dis- cussed in the following sections.
Direct Methods for Estimating Dietary Protein Intake
Dietary Diaries and Interviews .
Such diaries usually are collected for 2- to 7- day periods. Accuracy is increased by an inter- view based on the results of the diaries. Dietary diaries and interviews conducted by carefully trained personnel can provide rather accurate in- formation.‘53”6 The difference between the intake of nutrients reported in dietetic diaries and di- rectly observed in one large study was reported to be 10% or less in half of the subjects.“’ For energy, the reported intake was within 20% of observed in 85% of subjects; the accuracy was almost as good for protein. Group means were much closer. Twenty-four hour recall methods and food frequency questionnaires also can be used to assess dietary intake. The information obtained is entered into computer databases that will indicate the daily intake of many nutrients in addition to protein.
Indirect Methods for Estimating Dietary Protein Intake
Dietary protein intake also can be estimated from urea nitrogen appearance (UNA) and total nitrogen appearance (TNA). These terms and their use are described below.
Urea Nitrogen Appearance
Urea nitrogen appearance is the net production or appearance of urea nitrogen in body fluids and all measurable outputs (eg, urine, dialysate, fistula drainage). The term “urea nitrogen ap- pearance” is preferred over “urea production” or “urea generation” because some urea that is produced (or generated) is degraded in the intes- tinal tract; the ammonia thus released from urea is largely transported to the liver and converted back to urea.?’
UNA (g/d) = urinary urea N
+ dialysate urea N + Abody urea N (5)
ABody urea N = (SUNf - SUNi). aBWi * 0.58
+ (aBWf - aBWi)* SUNf (6)

968 KOPPLE ET AL
where i and f are the initial and final values for the period of measurement, respectively, SUN is serum urea nitrogen (g/L), aBW is actual body weight (kg), and 0.58 (or 0.60) is the fraction of body weight that is water.“” The proportion of body weight that is water may be increased in patients who are edematous or lean and de- creased in individuals who are obese or very young. If actual V is known from urea kinetics, it may be used instead of 0.58 * aBW. Changes in body weight during the I- to 3-day period of measurement of UNA are assumed to be due entirely to changes in body water.
When serum urea (SU) is expressed in milli- moles per liter, the change in body urea nitrogen (g/d) can be calculated as follows:
ABody urea N
= O.O28[(SUr - SUi) * aBWi 0 0.58
+ (aBWr - aBWi) * SUV] (7)
Urea nitrogen appearance can be calculated for maintenance hemodialysis patients as follows. In hemodialysis patients, the UNA is traditionally calculated using the single pool urea kinetic model requiring three blood samples: predialysis SUN (C,), postdialysis SUN (C,), and predialysis SUN for the next dialysis (C,) and the dialyzer clearance, &. There are two unknown values: V (volume of urea distribution) and UNA. To determine these two unknown values, two equa- tions are required. The first equation examines the change of body content of urea nitrogen dur- ing dialysis, and the second equation is related to the change of body content of urea nitrogen between two dialyses. In the more rigorous vari- able volume single-pool model, the influence of UNA on body content of urea nitrogen during dialysis as well as the influence of residual renal clearance, K,, on body content of urea nitrogen during dialysis and between dialyses are consid- ered. The resulting equations are rather complex and are presented in Appendix 3. For conceptual simplicity, we will consider the case of an aneph- ric patient with a relatively negligible change of body volume during dialysis (fixed volume model) and ignore the small impact of UNA on body content during the dialysis (because of the short duration involved):
c2 = c, . e-WIW (8)
where td and tad are dialytic and interdial, +ic time intervals, respectively, and C,, CZ, and CX are measured. K is measured in vivo or calculated for the operating conditions of blood and dialy- sate flow, knowing the in vivo mass transfer area coefficient of the dialyzer. The two equations are iteratively solved for the unknown V and UNA. If K,, is not explicitly known or measured, the equation can be solved for KJV and UNA/V.
Methods for estimating UNA from only two blood samples (C, and C,) have been derived recently. These approaches are discussed below in the Estimation of Dose of Dialysis Therapy section.
Urea nitrogen appearance can be calculated for patients undergoing continuous ambulatory peritoneal dialysis (CAPD) as follows:
UNA = (V, *DUN + V;UUN)t
+ Abody urea N (10)
where Vd and V, are dialysate and urine volumes, respectively (L), DUN and UUN are dialysate and urine concentrations of urea nitrogen (g/L), respectively, and t is the time of collection (typi- cally 1 day).3,4” Since with CAPD the daily changes in body urea nitrogen are usually negli- gible, the UNA can be estimated closely as fol- lows:
UNA (g/d) = (V,.DUN + V;UUN)/t (11)
Total Nitrogen Appearance
Total nitrogen appearance is the sum of all outputs of nitrogen from the body, including dial- ysate, urine, and feces, plus the change in body urea nitrogen, usually expressed in grams of ni- trogen per day. The TNA includes the nitrogen losses from the body in the form of urea, protein, peptides, amino acids, and all other nitrogen-con- taining compounds. In a patient who is in nitro- gen equilibrium, TNA plus any unmeasured ni- trogen losses should roughly equal total nitrogen intake. The latter quantity, when multiplied by the factor 6.25, should approximate protein in- take.
The TNA can be quantitated by measurement
PROPOSED GLOSSARY OF DIALYSIS KINETICS
of total nitrogen in urine, dialysate, and feces using rather laborious and expensive tech- niques.4’.42 The factor that has made the indirect methods for estimating protein intake more prac- ticable is the very strong correlation between TNA and UNA?‘a4” Thus, using relatively simple and inexpensive measurements of urea nitrogen, regression equations can be used to estimate TNA. It should be appreciated that although the correlation between TNA and UNA is strong, the 95% confidence limits for the regression equation are approximately 220% of the mean.’ The Y intercept for the regression of TNA on UNA is an average value for non-UNA. If a patient has unusually large protein losses into dialysate or a large urinary ammonium excretion, is in marked positive or negative protein balance, or is preg- nant, these regression equations may not accu- rately predict TNA for that individual.
Since not all nitrogen losses can be easily mea- sured (eg, skin desquamation, sweat, nail and hair loss, respiration, flatus), the TNA predicted by these equations underestimates actual nitrogen appearance by an unknown amount, thought to be at least 5 mg nitrogen/kg aBW/d in normal adults.47 This quantity has not been quantified in dialysis patients and could be larger because of unusual losses, such as methylamines in the breath!8 Moreover, there is some evidence that these unmeasured nitrogen losses may not be constant, but rather may increase with large pro- tein intake.49
In the dialysis literature, protein intake esti- mated from the UNA has been referred to as the “protein catabolic rate.” It was thus named in recognition of the fact that urea is the major ni- trogenous waste product from the breakdown of exogenous and endogenous proteins.44 We be- lieve that although it is a useful concept, the term “protein catabolic rate” is misleading because, first, intact proteins, peptides, and amino acids lost in dialysate and urine comprise a portion of the PCR, but they are not catabolized to urea or other nitrogenous products, and second, in clini- cal nutrition and metabolism, the term “protein catabolism” refers to the absolute rate of protein breakdown, commonly measured by isotopically labeled amino acids. The absolute rate of protein breakdown is much greater than the net degrada- tion of exogenous and endogenous proteins, which results in urea excretion. In healthy adults
weighing about 70 kg, protein synthesis and breakdown generally are measured to be approxi- mately 250 to 300 g protein/d,50~5’ whereas both the typical protein intake and the net rate of pro- tein breakdown estimated from the UNA are ap- proximately 50 to 100 g/d in such individuals.
Therefore, the new term “protein equivalent of total nitrogen appearance” (PNA) is proposed. This expression is more in keeping with the origi- nal definition suggested by Borah et al.““ The PNA is calculated exactly the same way as PCR. The advantage of the term “protein equivalent of total nitrogen appearance” is that it describes more cor- rectly the metabolic processes that it represents, whereas “protein catabolic rate” is a misnomer that may be more likely to cause confusion.
Protein Equivalent of Total Nitrogen Appearance
The PNA expresses TNA in terms of protein. The equivalent amount of protein lost, PNA is usually expressed in grams per day or grams per kilogram per day. The conversion of TNA to PNA (equation 12) is based on the fact that the nitrogen content of mixed proteins is relatively constant at 16%, and that, quantitatively, most of the nitrogenous compounds lost from the body are either metabolites of protein (eg, urea) or are proteins and peptides (eg, in peritoneal dialy- sate).
PNA (g protein/d) = 6.25 * TNA (g N/d) (12)
The PNA can be estimated from UNA in nondia- lyzed patients with chronic renal failure4’*45.46 and in maintenance dialysis patients as described be- low. The regression equations relating UNA to PNA differ slightly for hemodialysis and perito- neal dialysis patients. When originally published, these equations were expressed in the traditional terms of PCR and urea generation. They have been modified here to be consistent with the pro- posed nomenclature.
Hemodialysis patients.
PNA (g/d) = 6.49.UNA + 11.04 (13)
with UNA expressed in grams of nitrogen per day. Equation 13 was derived by Borah et al.““ The second term on the right-hand side is an average value for non-urea nitrogen losses ex- pressed in terms of protein (g protein/d). Since

970 KOPPLE ET AL
the average V in their patients was 38 L, these investigators lateti* modified the equation by di- viding the constant term by 38 L resulting in equation 14.
PNA (g/d) = 6.49.UNA + 0.294-V (14)
where V is the volume of distribution of urea (L) and the coefficient for the second term is expressed as grams of protein per liter per day. Since the second term represents non-urea losses, which vary primarily with body size, this modi- fication allows use of the equation for patients of various sizes.
Delayed equilibration of body urea pools after hemodialysis may lead to a disproportionately lower urea concentration in plasma compared with other body pools. Failure to adjust for the postdialysis plasma urea rebound may lead to an overestimation of the PNA of 10% or greater. This is especially likely to occur in patients who receive high-efficiency hemodialysis (see section below entitled Compartmental Disequilibrium).
Continuous ambulatory peritoneal dialysispa- tients.
PNA (g/d) = 6.49.UNA + 0.294. V
+ protein losses (15)
This is the modified equation of Borah et al (equation 14) further modified4’ by inclusion of a term for peritoneal protein losses, expressed in grams of protein per day.
PNA (g/d) = 10.76(0.69 * UNA + 1.46) (16)
Equation 16 is essentially the equation of Ran- derson et al?” which was derived from data col- lected in CAPD patients. In the original form of the equation, UNA was expressed as G,, (mg urea nitrogen/min). In equation 16, the recom- mended term UNA (g urea nitrogen/d) is used instead (G,, = UNA/1.44 = 0.69 * UNA).
PNA (g/d) = 6.25 (UNA + 1.81)
+ 0.031.aBw (17)
Equation 17 was derived by Teehan et al54 from data collected in CAPD patients. The second term ( 1.8 1 g nitrogen/d) -is an average value from the literature for protein and amino acid nitrogen losses in CAPD patients. The third term (0.031 g/kg/d) is an average value taken from the litera-
ture for non-urea losses. For a discussion of these various approaches for calculating the PNA in chronic peritoneal dialysis patients, see Kesha- viah and Nolph,40 who have reported that these equations, in general, give similar results. Berg- striim et al” have argued that the relationship between UNA and TNA may be different for hemodialysis and peritoneal dialysis patients. Since peritoneal losses of protein may vary sub- stantially from patient to patient, especially if peritoneal inflammation is present, it may be more accurate to use equation 15. This may be of more importance in research studies than in the clinical setting. Other investigators have pub- lished equations that can be used to calculate PNA in CAPD patients.56,57
Normalized Protein Equivalent of Total Nitrogen Appearance
For comparison of an individual patient’s PNA to published standards or data from other patient populations, PNA can be divided by aBW, nBW (as defined above), or a body weight derived from the urea distribution space (ie, V/0.58). The PNA may be useful for evaluating nitrogen out- put or intake (see below) using a normal refer- ence value for body mass. The PNA divided by aBW may provide useful information when pre- scribing a dietary intake or when evaluating the appropriateness of a patient’s actual nutritional intake, but may present special difficulties when the patient is edematous, obese, or emaciated (ie, when the actual and standard weights of a patient are very different). Division of PNA by V/O.58 is commonly used and has the advantage that it relates protein metabolism to the body’s com- partment of urea, the major nitrogenous metabo- lite of protein removed by dialysis. It has the disadvantage that the values obtained represent neither a standard body weight nor the patient’s aBW. In edematous, obese, or severely under- weight patients, the term V/O.58 may give mis- leading data. As always, clinical judgment must be used when the PNA is expressed as a function of body mass.
Limitations to the Estimation of Dietary Protein Intake by Indirect Methods
Because PNA, TNA, and UNA do not include nitrogen from unmeasured losses, PNA almost always underestimates the actual DPI. In nonure-

PROPOSED GLOSSARY OF DIALYSIS KINETICS 971
mic subjects the difference is approximately 2.5 to 7.5 g protein/d!7 For nondialyzed chronic re- nal failure, maintenance hemodialysis, or chronic peritoneal dialysis patients, less is known about the degree of underestimation of DPI by PNA, but it is probably of at least the same magnitude. Theoretically, because of the possibility of in- creased respiratory or dermal nitrogen losses in renal failure,48 it may be greater. The degree to which the PNA underestimates DPI is not en- tirely constant, and also may be greatly increased in individuals ingesting high nitrogen intakes49 or when protein or nitrogen balance is positive. In patients who are in negative protein or nitrogen balance, PNA may be greater than the DPI. Since transient periods of positive or negative nitrogen balance may be common, this may be a common source of error. To these sources of error must be added the variance intrinsic to UNA measure- ments. Clearly, PNA must be interpreted in light of the patient’s clinical condition. It is also appar- ent that more research is needed to define more precisely the relationships between UNA, TNA, PNA, and the DPI in chronic renal failure and maintenance dialysis patients.
Expression of Dietary Protein Intake
Since the PNA (formerly the PCR) often will be used to estimate the DPI, it is important to determine the relationship between DPI and PNA as precisely as possible. There are essentially no published data that directly examine this relation- ship. Until such information is forthcoming, it would seem reasonable to add 30 to 60 mg pro- tein/kg aBW/d to the PNA to approximate the usual unmeasured nitrogen losses.”
The DPI can be expressed in absolute units, such as grams of protein per day, or may be factored by a number of terms, including the pa- tient’s aBW, nBW, or V/0.58. We recommend that the methods for estimation of DPI (ie, direct or indirect) and for weight adjustment of DPI (ie, aBW, nBW, or V/0.58) always be clearly stated.
ESTIMATION OF DOSE OF DIALYSIS THERAPY
The dose of dialysis therapy is the product of clearance (K) and duration of therapy (t). The Kt product usually is normalized to reflect body size. For urea, it has become accepted practice to nor- malize Kt to the volume of urea distribution V,
resulting in the index of urea removal Kt/V, which has been shown to be a marker of dialysis morbidity and mortality.2~“~9 In peritoneal dial- ysis, in addition to the Kt/V urea index, an index based on weekly creatinine clearance normalized to BSA (expressed per 1.73 m2 of BSA), is often used to quantify the dose of dialysis therapy.
Clearance
Clearance (K) is the volume of a solution that is completely cleared or depleted of a solute dur- ing a given period of time. An alternate definition of clearance is the rate of mass transport per unit of concentration gradient.
For hemodialysis, the clearance of a solute from blood can be expressed as follows:
K = (Qin . G - Qout * GJG (18)
where Q and C represent blood flow rates and concentrations, respectively, the subscripts in and out represent the inflow and outflow sites for the measurement of blood flow and concentration, respectively, and QO,, = Qin - Q.r, where Quf is the rate of ultrafiltration.
It is common but incorrect for the concentra- tions C,,, and Ci” to be given as plasma concen- trations and Qin to be given as the whole blood flow rate. For a correct calculation of clearance, concentration and flow rate should be measured for the same solution that is being cleared of the solute. If K is a whole blood clearance, then Q and C should refer to the whole blood flow rate and the whole blood concentration.58 The whole blood concentration is calculated as follows:
CB = C,[(l - H) + H*Ea] (19)
where C, is the solute concentration in whole blood, Cp is the concentration in plasma, H is the hematocrit, and ER is an equilibrium ratio between red blood cell and plasma concentra- tions. Values for ER in the literature, for normal red blood cells, range from 0.76 to 0.96 (mean, 0.86) for urea and 0.70 to 0.76 (mean, 0.73) for creatinine.59.m For an inert solute that does not bind to blood components, the E, would be ex- pected to be 0.77 based on a red blood cell water fraction of 72% and a plasma water fraction of 92%. The measurements of ER for urea by Cheung et a16’ give a value of 0.76 for normal subjects and 0.77 for uremic patients. The data

972 KOPPLE ET AL
of Descombes et al”’ for dialysis patients are con- sistent with values of 0.77 for urea and 0.73 for creatinine.
Use of equation 19 to convert plasma concen- tration to whole blood concentration assumes that there is concentration equilibrium between red blood cells and plasma. For urea, this assumption is probably valid for blood both entering and leaving the dialyzer. However, for creatinine, while the assumption may be reasonable for blood entering the dialyzer, it is certainly not the case for blood leaving the dialyzer. Creatinine is preferentially removed from plasma during the transit of blood through the dialyzer, and little creatinine is removed from within the red blood cell. If the outflow blood is allowed to sit in a container, some degree of equilibration will oc- cur between the red blood cells and plasma. Ac- cording to Skalsky et al,63 the time for 95% equil- ibration of creatinine is on the order of 105 minutes. However, according to Descombes et al,” it may take as long as 6 to 12 hours for complete equilibration of creatinine between the red blood cells and plasma. Furthermore, Des- combes et al report that for creatinine, red blood cells and plasma are not in equilibrium even in the blood entering the dialyzer. A small but sig- nificant creatinine concentration increase of 4% was noted in inlet plasma allowed to equilibrate with inlet red blood cells at room temperature. This inlet disequilibrium was not seen in the data of Skalsky et aL6’ who used fairly low blood flow rates of approximately 150 rnL/min compared with 315 mL/min in the work of Descombes et a1.62 At the higher blood flow rates, the time inter- val between two successive transits of red blood cells through the dialyzer is decreased to as little as 12 to 15 minutes, an interval that may not be sufficient for red blood cell-plasma equilibration in vivo.
An alternate and preferred calculation for clearance is based on the measurement of solute concentrations in dialysate and incoming blood, as follows:
K = QD~ * G&Bin (20)
where QDo is the dialysate outflow flow rate, C, is the solute concentration in outflow, and Csi, is the solute concentration in inflow blood. The blood concentration can be calculated from the plasma concentration, hematocrit, and equilib-
rium concentration ratio as above. Since concen- trations in dialysate are often much lower than in blood, they need to be measured carefully with duplicate or triplicate determinations.
In equation 20, the numerator represents aque- ous flows and concentrations, whereas the de- nominator is a whole blood concentration. Some investigators therefore prefer to use a blood water concentration in the denominator. Thus calcu- lated, the clearance is a blood water clearance rather than a whole blood clearance.h4 In the in- flow blood, plasma water and red blood cell wa- ter are in equilibrium so that the plasma water concentration can be used in the denominator instead.
C pW = CJ(1 - 0.0107’ C,,,,iJ (21)
where Cp is the concentration of the solute in plasma and Cpmtein is the total plasma protein con- centration in grams per deciliter.“’ For Cprotein = 7 g/dL, Cpw = Cd0.925.
For peritoneal dialysis, the clearance of a sol- ute is usually measured as an average value for an entire exchange, as follows:
K = (V,*C,)/(C,*t) (22)
where Vd is the volume of drained dialysate, Cd is the solute concentration in drained dialysate, C, is the serum/plasma solute concentration dur- ing the exchange, and t is the time for that ex- change. Thus, the clearance usually reflects a se- rum/plasma clearance.
If it is desirable to calculate whole body clear- ance rather than blood clearance, C, should be replaced by CTBW, the concentration in TBW. Be- cause peritoneal dialysis is a slow transport pro- cess in which there is almost constant equilib- rium between TBW and plasma water (PW), Cpw (plasma water concentration) can be used instead of CTsW (equation 21).
For peritoneal dialysis, clearance is usually measured as an average value for an entire ex- change, but also may be measured as an average value based on the pooled volumes and concen- trations of a number of exchanges. This is usually the case for CAPD, in which the total drained volume for a 24-hour duration is pooled and the urea nitrogen concentration of this pooled sample is used in the calculation. It should be noted from equation 22 that the clearance-time product Kt

PROPOSED GLOSSARY OF DIALYSIS KINETICS 973
is equal to V,, * (C&Z,), ie, the drained volume times the dialysate to SUN concentration ratio.
Residual Renal Function
Residual renal function is the renal function in an individual with advanced renal failure who is usually receiving dialysis treatments. Residual renal function generally refers to the glomerular filtration rate (GFR), expressed in milliliters per minute or liters per day. The GFR may be accu- rately estimated by inulin, iothalamate, or EDTA clearances or, for patients with renal failure, somewhat less accurately by the mean of the uri- nary clearances of urea and creatinine.66.67 For urea kinetic modeling, the renal urea clearance may be more relevant than measurements of GFR. However, when calculating the weekly cre- atinine clearance normalized to 1.73 m* as an index of the dialysis dose, the use of GFR or estimate of GFR rather than the residual creati- nine clearance is recommended.
Kt/V
Kt/V is defined as the dose of dialysis treat- ment as determined by the solute clearance-time product normalized to the individual’s volume of urea distribution. Kt/V is a dimensionless param- eter that is dependent on K, the total clearance (dialytic plus residual renal clearance, mL/min), t, the duration of the dialysis (mm), and V, the volume of solute distribution (mL). Kt/V is most often expressed per dialysis treatment for hemo- dialysis and per day or per week for peritoneal dialysis, as discussed below. For clarity, the time basis for the Kt/V dose should be indicated (eg, Kt/V weekly). Kt/V was first introduced by Gotch and Sargent’ as a measurement of dialysis dose for the small solute urea, based on their reanalysis of the National Cooperative Dialysis Study data. However, Kt/V can be calculated for other solutes as well, if the volume of distribution and the intercompartmental equilibration rates for the solute are known.
Kt/V Hemodialysis
If Kt/V is calculated simply as the product of the measured total clearance (dialysis clearance I(d + residual renal clearance K,) and duration of dialysis (t) normalized to the volume of distri- bution (V), the result will overestimate the true delivered Kt/V because the delivered K is usually
less than (I<d + K,) for the reasons discussed below.
Access recirculation. If the blood flow rate set by the blood pump is higher than the access blood flow, some of the blood outflow from the dialyzer will be recirculated within the access, back into the inflow stream:* The blood flowing into the dialyzer will therefore be a mixture of “fresh” blood entering the access from the arte- rial segment and dialyzed blood recirculated from the “venous” needle. The actual blood clearance will therefore be less than the measured dialyzer clearance and an access recirculation correction will be necessary. Access recirculation and the reduction in clearance due to access recir- culation is calculated using the following equa- tions:
Access recirculation R (%)
= [(C, - C,)/(C, - C,)] x 100 (23)
where Cf is the solute concentration in “fresh” blood not contaminated by access recirculation and C, and C, are solute concentrations in the “arterial” and “venous” segments of the extra- corporeal blood circuit. Access recirculation is normally calculated using urea and/or creatinine concentrations. In the past, Cr was measured by drawing a peripheral venous blood sample, usu- ally from the nonaccess arm. However, it has been shown that because of a phenomenon known as cardiopulmonary recirculation,“9‘7’ which is described below, the peripheral blood sample is not representative of the fresh blood entering the access. The current procedure is to stop or slow down the blood pump so as to elimi- nate recirculation and to draw a sample from the arterial line of the extracorporeal circuit. With this stop-flow technique, the dead space in the arterial needle and connecting tubing between the access and the point of sampling must be flushed to obtain a representative sample.
%Reduction in Clearance
R =R+(l -R)/E
x 100 (24)
where R is expressed as a fraction of unity rather than as a percentage, and E, the dialyzer extrac- tion ratio, is equal to (1 - CJC,).

974 KOPPLE ET AL
Cardiopulmonary recirculation. In the case of access recirculation, blood from the “venous” needle is recirculated within the access back into the arterial needle and the “venous” blood di- lutes the solute concentration in the “fresh” blood entering the access. In the case of cardio- pulmonary recirculation, dialyzed blood from the venous outflow of the blood access is recirculated back into the arterial inflow of the blood access through a circulation loop that includes the cen- tral veins, right heart, lungs, and left heart7’ When the venous outflow blood mixes with the rest of the cardiac output in the central vein, there is dilution of solute concentration because the dialyzed venous outflow has a much lower solute concentration than the blood entering the central veins from the peripheral capillary beds. As a consequence of this recirculation within a larger blood loop than the access loop, the old method of drawing a peripheral blood sample to deter- mine recirculation exaggerates the actual access recirculation because this technique measures the combined effect of access and cardiopulmonary recirculation. Even in a good access with no ac- cess recirculation, the old technique would result in a recirculation value of 5% to lo%, represent- ing the contribution of cardiopulmonary recircu- lation. It is because of this phenomenon that one notices a very steep drop in “arterial” blood urea nitrogen (BUN) in the first few minutes of dial- ysis, representing the “dialysis” of the cardiopul- monary loop only and not of TBW. As with access recirculation, cardiopulmonary recirculation fur- ther reduces effective blood clearance.
Compartmental disequilibrium. The single- pool kinetic model assumes that solute is distrib- uted in a single, well-mixed homogenous body pool and that the dialyzer removes solute uni- formly from this total volume. In reality, the dia- lyzer removes solute preferentially from a pe- ripheral compartment, the central compartment lagging behind at a higher concentration than in the peripheral compartment. At the start of the dialysis procedure, both compartments are in equilibrium; the dialytic process perturbs this equilibrium. At the end of dialysis, the disequi- librium induced between body compartments is manifested by a rebound of solute concentration in the peripheral compartment as solute diffuses down the concentration gradient established by compartmental disequilibrium.72 Although it has
been speculated that rebound may be a manifes- tation of an increased UNA resulting from dial- ysis-induced hypercatabolism, the magnitude of increase in UNA that must be postulated to ac- count for the rapid rebound is too large to be plausible. While hypercatabolism may cause a small increase in UNA lasting for several hours following dialysis, the rapid rebound in the 30 to 45 minutes immediately following dialysis is, for the most part, a result of compartmental dis- equilibrium. This conclusion is strengthened by the correlation noted between the magnitude of the rebound and the efficiency of dialysis (K/V). The single-pool model assumes that blood solute concentrations represent concentrations in the en- tire body pool. As a consequence, the single pool estimation of clearance and, hence, Kt/V gives an overestimation of the true whole body clear- ance and whole body Kt/V. As long as V repre- sents the entire body pool of solute, K must rep- resent the clearance of this whole body pool and not merely blood clearance or dialyzer clearance. With the increasing use of high-efficiency and high-flux therapies, which require higher dialyzer clearances to compensate for the shorter time du- ration, the magnitude of this compartmental dis- equilibrium has become more significant; the overestimation of the actual dose of delivered dialysis may be 15% to 20% or greater.
Our understanding of compartmental disequi- librium introduced by dialysis is still very incom- plete. The mass transfer coefficient governing urea transfer between body compartments may be highly variable among patients and may even vary from day to day within a given patient. This variability may support a regional blood flow model of disequilibrium rather than an intracellu- lar to extracellular disequilibrium model. Erics- son et al7-1 and Kjellstrand et a174 suggest that deviation from single-pool behavior is greater in patients who are overhydrated and have labile blood pressures, pulse rates, and body tempera- tures. Shirai et a175 showed that urea, creatinine, and uric acid are removed more slowly from edema fluid than from plasma; concentrations of these solutes in plasma are 15% to 17% lower than in edema fluid at the end of dialysis. Silver et al,76 investigating the dialysis disequilibrium syndrome in a rat model, provided evidence that the increase in brain water observed during dial- ysis is related to the more rapid removal of urea

PROPOSED GLOSSARY OF DIALYSIS KINETICS 975
from plasma relative to its removal from the brain. The resulting osmotic gradient between plasma and the brain causes cerebral edema. Me- try et a177 used a novel microdialysis technique to measure interstitial concentrations of urea during dialysis, and noted a close correspondence be- tween urea concentrations in plasma and intersti- tial fluid during the course of dialysis. However, postdialysis, the urea rebound in plasma was complete in 2 hours, whereas urea rebound in interstitial fluid was delayed by approximately 60 minutes and continued for approximately 4 hours postdialysis. Metry et al speculate that the more rapid urea rebound in plasma may represent urea influx from the enterohepatic recirculation of urea nitrogen. All these studies emphasize that if urea nitrogen concentrations measured imme- diately postdialysis are used to measure the effi- ciency of the dialysis process, an overestimation of dialysis efficiency results. A more realistic appraisal of dialysis efficiency must take postdi- alysis rebound into consideration.
As can be seen from the above considerations, the calculation of Kt/V based on individual mea- surements of K, t, and V is complicated and not suited to routine clinical monitoring. We will now consider several approaches to measuring delivered Kt/V without explicitly measuring K.
Three-Point and Two-Point Serum Urea Nitrogen Methods for Measuring Kt/V for Hemodialysis
Using the single-pool urea kinetic model re- ported by Sargent et al,’ predialysis, postdialysis, and the next predialysis values of SUN and the clearance K are inputs, and the iterative solution of equations 8 and 9 results in V and UNA as outputs. If K is overestimated because the appro- priate corrections (eg, the blood water correction, recirculation correction) are not applied, then V also will be overestimated and the ratio K/V will only be slightly underestimated. If t is known accurately, then Kt/V can be calculated with rea- sonable accuracy despite the uncertainty in K and V as individual values. Even if K is not a mea- sured input, a reasonable estimate of K can be used as an input and a corresponding V can be derived. The ratio K/V will be reasonably accu- rate even with this approach. This approach is known as the three-SUN or three-point urea ki- netic model. It suffers from the invalid assump-
tion that the urea pool is a single, well-mixed pool. The Kt/V thus derived will therefore over- estimate whole body Kt/V. However, in the three-SUN model, if the SUN measured after a postdialysis rebound period of 30 to 60 minutes is used instead of the immediate postdialysis SUN, a more valid whole body Kt/V will be obtained.
Since the three-point SUN method with its it- erative solution was considered to be too com- plex for routine clinical use, a two-point SUN approach based on predialysis and postdialysis SUN levels has become popular. Several simple formulae have been proposed for calculating Kt/ V based on the post-SUN to pre-SUN ratio, R. A recent study78 comparing nine of these simplified formulae based on the same set of SUN measure- ments reports a resulting Kt/V range as wide as 1.0 to 1.5. One example of a simplified formula is as follows:
Kt/V = -In (R)
where In (R) is the natural logarithm of the post- SUN to pre-SUN ratio. This simple formula is valid if there is no ultrafiltration-induced volume change and if the UNA rate during dialysis is ignored. In the presence of ultrafiltration and with typical values for the UNA, this simple logarith- mic formula will underestimate Kt/V by as much as 20% to 30%.
Another simple formula for Kt/V that corrects the logarithmic approach for ultrafiltration and for UNA during dialysis has been proposed by Daugirdas79:
Kt/V = -In (R - 0.03)
+ (4 - 3.5 *R).UF/W (26)
where R is the ratio of the postdialysis to predial- ysis plasma urea nitrogen concentrations, UF is the ultrafiltration volume (L) removed during di- alysis, W is the postdialysis weight (kg), and the factor 0.03 is a constant that adjusts for UNA during dialysis. (Note that data concerning Kt/V should always indicate the method and equation used to calculate Kt/V.)
This formula results in Kt/V values that are very similar to those of the more rigorous three- point SUN method of Gotch and Sargent. As with the three-point SUN approach, if the postrebound SUN is used instead of the immediate postdial-

976 KOPPLE ET AL
ysis SUN in the Daugirdas formula, a more repre- sentative whole body Kt/V is derived.
As originally proposed, the two-point SUN method was useful only for estimating Kt/V but not the UNA or PCR. However, Depner” and Gotch’ proposed methods for calculating UNA and PCR (PNA in the proposed nomenclature) from the two-point BUN approach by assuming that the patient is in a steady state and calculating the average UNA over the duration of the weekly cycle that achieves the measured steady-state predialysis and postdialysis values of SUN. For example, in the Depner approach, if the Monday values of SUN predialysis and postdialysis are measured and the KtN is calculated, a value of UNA can be assumed that will allow calculation of the Wednesday and Friday predialysis and postdialysis SUN as well as the next Monday predialysis SUN. If too high a value for UNA is assumed, then the predialysis SUN on the next Monday will overestimate the predialysis SUN of the previous Monday. If too low a value of UNA is assumed, the next Monday predialysis SUN will be lower than the previous Monday’s predialysis SUN. By a trial-and-error or iterative approach, a value for UNA is arrived at that rep- resents the steady-state UNA over a l-week cy- cle. It must be noted that this estimation of UNA is based on a 7-day treatment cycle, whereas the three-point SUN approach calculates a UNA that applies to the interdialytic interval between the end of the first dialysis and the start of the next dialysis. This interdialytic value of UNA may not represent the steady-state UNA calculated by the Depner approach. The Gotch approach to cal- culating a UNA from two-point SUN measure- ments is similar conceptually to the Depner ap- proach in that it represents a steady-state UNA. However, the methodology used is different and is a graphical approach based on the Gotch do- main map that relates predialysis SUN, normal- ized PCR (PNA divided by aBW), and Kt/V. If predialysis SUN and Kt/V are known, then the appropriate Kt/V line of the domain map is iden- tified and the normalized PNA corresponding to the intercept of the predialysis SUN value with theappropriate Kt/V line can be read off the do- main map. Direct Dialysis Quanti$cation
In addition to the two-point SUN and three- point SUN kinetic approaches to calculating
Kt/V and PCR (PNA), these latter parameters may be determined from direct measurements of urea in the total effluent dialysate or in aliquots of the dialysate. Although some investigators consider the direct measurement of dialysate urea nitrogen to be the definitive standard for de- termining dialysis urea removal, there are also limitations to this technique. It has been laborious and time-consuming, and several measurements of the dialysate are required because a small error in the measurement becomes greatly magnified when it is multiplied by the dialysate volume. The direct measurement of effluent dialysate is probably more suitable for research procedures than for clinical use. Direct dialysis quantifica- tion requires the direct measurement of total ef- fluent or of representative aliquots and measure- ments of predialysis and 30- to 60minute postdialysis SUN.8’ Urinary urea excretion dur- ing the interdialytic interval and the subsequent predialysis SUN also are determined. From these data, two equations can be solved, one for the urea mass balance during dialysis and the other representing urea mass balance in the interdia- lytic interval. These two equations are similar in concept to equations 8 and 9, but represent a mass balance rather than a kinetic approach. As with equations 8 and 9, these mass balance equa- tions are solved for V and UNA. As originally proposed, the direct dialysis quantification meth- odology was flawed in that it did not take into account either volume changes during dialysis resulting from ultrafiltration or the postdialysis rebound.
Urea Reduction Ratio
Another simplified approach8* to quantifying the dose of hemodialysis is the URR.
t-RR(%) = (1 - postSUN/preSUN) * 100
(27)
The limitations to using the URR are that it does not take into account either the influence of vol- ume changes due to ultrafiltration on the dose of dialysis or the postdialysis rebound. Therefore, one cannot strictly correlate URR and whole body Kt/V without accounting for the volume ultrafiltered and the urea rebound postdialysis. Nevertheless, a target URR between 60% and 70% corresponds to a single pool Kt/V between

PROPOSED GLOSSARY OF DIALYSIS KINETICS 977
1 .l and 1.4. Using a large database, URR has been shown to be a significant predictor of mor- tality in hemodialysis patients with serum albu- min concentrations in the range of 3.0 to 3.9 g/dL.”
KtN Peritoneal Dialysis The delivered KtN for chronic peritoneal dial-
ysis indicates the patient’s solute clearance, nor- malized to the body’s volume of distribution for that solute, usually urea. Both clearance and the volume of distribution are expressed in liters; hence, the units of Kt/V for peritoneal dialysis are also dimensionless. The K includes contribu- tions from both the dialytic (K,) and renal (K,) clearances.
The dialytic contribution (K,t) is calculated as the product of the volume of dialysate outflow and the dialysate to plasma/serum water concen- tration ratio. The plasma/serum water solute con- centration can be calculated using equation 21. The dialysate sample should be obtained from a pooled, mixed, complete 24-hour collection. In the case of CAPD, this is simply equal to the 24- hour drained dialysate vohime. FOT nightperito- neal dialysis, this includes both the complete di- alysate volume drained overnight as well as any daytime dialysate outflow. Although the dialysis dwell times with night peritoneal dialysis may be less than 24 hours, if a daytime dwell is not used, the value for the clearance-time product K,t can still be expressed in liters per day since that is, in fact, the total peritoneal clearance for that 24-hour period. The procedure for dialysate collection for continuous cycling peritoneal dial- ysis is essentially the same as for night peritoneal dialysis. The residual renal contribution (K,t) is calculated from a 24-hour urine collection that should be obtained during the same day in which the dialysate is collected for the calculation of K,t.
The delivered Kt/V may be expressed as (K,t + K,t)N or simply Kp,t/V. Typical KtN,,,, val- ues for chronic peritoneal dialysis range from 0.21 to 0.32/d or 1.5 to 2.25/wk. It is more com- mon to express Kt/V on a weekly basis. The daily method, however, may be more useful for prescriptive purposes.
Standardization of KtN Values Kt/V values generally are expressed for a sin-
gle hemodialysis treatment. Studies correlating
Kt/V values with morbidity and mortality have been based on hemodialysis treatment schedules of three times per week. In the future, it is possi- ble that hemodialysis treatments may be per- formed at different frequencies. It is important to indicate, therefore, the frequency of hemodial- ysis treatments when expressing the Kt/V. It is recommended that a value for a weekly Kt/V also be given. Similarly, chronic peritoneal dialysis is not always performed with the same dialysis dose each day; thus, expressing Kt/V for peritoneal dialysis on a weekly basis is generally preferable for peritoneal dialysis as well. Expression of Kt/ V for both hemodialysis and peritoneal dialysis on a weekly basis also allows for much easier comparisons between these two dialysis treat- ments.
Prescribed KtN Versus Delivered KtN There is much evidence indicating that the pre-
scribed Kt/V is not delivered in the majority of clinical dialysis treatments.8” Thus, research or quality assurance data concerning the effects of actual dialysis treatments should refer only to the delivered Kt/V:
Weekly Creatinine Clearance
Weekly creatinine clearance, the urinary and dialysis creatinine clearance, is expressed in li- ters per week and is usually normalized to 1.73 m2 of BSA. This index of dialysis dose has been developed for chronic peritoneal dialysis on em- pirical grounds, and a minimum value of 40 to 50 L/week is recommended. Kb, is calculated as for urea by multiplying the volume of drained (24 hours) dialysate by the dialysate to plasma/ serum water concentration ratio and adding the amount contributed by renal function (if any). Since creatinine is at most a minor toxin, its clearance, per se, is not of particular interest, except as a marker for the clearance of other solutes, particularly those that are somewhat larger than urea. Renal tubular secretion of creati- nine accounts for a substantial fraction of renal creatinine clearance in patients with renal failure. Thus, an accurate estimate of GFR, rather than total renal creatinine clearance, should be used to estimate the renal contribution so that clear- ance of other molecules in this molecular weight range is not overestimated. It may be more appro- priate to use plasma water concentrations rather

978 KOPPLE ET AL
than plasma concentrations in this calculation, as discussed above. Weekly creatinine clearance for an individual with BSA is normalized to 1.73 m’, as shown in below:
Kb,(normalized to 1.73 m*) = Kb; 1.73/BSA
(28)
It has been shown that for peritoneal dialysis there is a high correlation between Kt/V,,, and the weekly creatinine clearance, as long as the residual renal contribution is correctly measured. The choice between Kt/V,,. and weekly creati- nine clearance as indices of the dose of peritoneal dialysis therapy may therefore be a personal one. However, the advantage of using urea as a marker of adequacy is that the same measure- ments also can be used to calculate UNA and PNA. In addition, laboratory measurements of creatinine in drained dialysate are complicated by the requirement for an appropriate dextrose correction.
ACKNOWLEDGMENT
That authors thank Baxter Healthcare Corporation, and es- pecially Stephen Garchow, for providing administrative sup- port for this project. In addition, discussions with Dr A. Ro- berto Frisancho regarding anthropometric standards were most helpful.
APPENDIX 1: MEASUREMENT OF ELBOW BREADTH
Measurement of elbow breadth has been described by Fri- sancho.” Briefly the subject’s right arm is raised forward to a horizontal position and then the forearm is bent to a 90- degree angle at the elbow with the palm facing the body. The examiner then measures the greatest width between the lateral and medial epicondyles using either a broadfaced sliding cali- per (Bicondylar Calipers; Seritex, Calstadt, NJ) or a Frameter (distributed by Health products, Ann Arbor, MI). The latter instrument requires less expertise and is less subject to errors in locating the proper anatomical landmarks or in positioning the caliper jaws.
APPENDIX 2: SELECTION OF A REFERENCE BODY WEIGHT
It is recommended that, in general, the NHANES data”-19 rather than the data in the Metropolitan tablesZaz’ be used as a reference standard for body weight for the following reasons:
1. The NHANBS reference values are based on data ob- tained from all major races and ethnic groups in the United States. The Metropolitan data are derived from a more afflu- ent segment of Americans, with a skewed representation to- ward males and certain races and ethnic groups (ie, those
who purchased life insurance in the 1950s through the 1970~“~‘) and are thus less representative.
2. The age range for adults in the NHANES data is 25 to 74 years; for the Metropolitan data, the age range is more limited, 2.5 to 59 years.
3. It is not known whether the DBWs reported in the Metropolitan tables are associated with greater longevity for races and ethnic groups that are not well represented in the Metropolitan tables or for chronically ill individuals, such as maintenance dialysis patients.
4. The NHANES data were frequently collected by health care professionals trained and committed to obtain accurate weights, heights, and frame sizes. With regard to the Metro- politan tables, these data generally were obtained by persons who were not specifically trained in the techniques of anthro- pometric data collection. Approximately 10% of the Metro- politan data were self-reported.”
5. The classification of individuals according to frame size is more scientifically based in the NHANES data than in the Metropolitan tables.
6. In addition to body weights, there are other anthropo- metric data obtained from the same individuals for the NHANES data that are available for comparison’7-‘9; this is not the case for the Metropolitan data.
7. The anthropometric data in the Metropolitan tables were obtained at one point in time. There is no information con- cerning how subsequent changes in body weight will affect the risk of mortality.
8. There are bodies of data similar to the NHANES data in other countries that can be used for comparisons; in con- trast, the type of data reported in the Metropolitan tables is largely confined to the United States.
APPENDIX 3: CALCULATION OF V AND UREA NITROGEN APPEARANCE FROM THE
VARIABLE VOLUME SINGLE-POOL MODEL THAT INCLUDES THE INFLUENCE OF K, AND
UREA NITROGEN APPEARANCE ON UREA MASS BALANCE
During hemodialysis, the rate of decline of body content of urea nitrogen reflects the balance between the rate of re- moval of urea nitrogen by the dialyzer and residual renal function and the UN’A. The solution of the differential equa- tion reflecting this balance is given below:
+(4+yeQ”f).(1 -$F) (1)
where C, and CZ are predialysis and postdialysis serum urea nitrogen concentrations, respectively, V, and VZ are predial- ysis and postdialysis volumes of urea distribution, respec- tively, I<d and K, are dialyzer and renal clearances, respec- tively, and Qur is the rate of ultrafiltration determined as the weight change during dialysis. I& is measured during dialysis, either from SUN concentrations at the dialyzer inlet and outlet or from outlet dialysate concentrations (see section on Clear-

PROPOSED GLOSSARY OF DIALYSIS KINETICS 979
ance). K, is determined by collecting urine between dialyses and measuring the volume and urea nitrogen concentration in this collected urine. V, is calculated as follows:
V, = VZ + Qur.b (2)
where b is the duration of dialysis. Between hemodialyses, the rate of accumulation of urea
nitrogen in the body reflects the balance between the UNA rate and removal by residual renal function. Solution of the differential equation expressing this mass balance yields the following formula:
(3)
where C, and C, are postdialysis and the next predialysis serum urea nitrogen concentrations, respectively, V, and V, are the corresponding volumes of urea distribution, and Qw is the rate of weight gain between dialyses. Vz is calculated as follows:
V, = Vr + Qw.t, (4)
where t is the duration between the two dialyses. C,, C2. and C, are measured by appropriate blood sampling. Qu is measured from the weight change between dialyses. The two remaining unknowns are UNA and V,. Equations 1 and 3 can he solved for these two unknowns.
REFERENCES
1. Sargent J, Gotch FA, Borah M, Piercy L, Spinozzi N, Schoenfeld P, Humphreys M: Urea kinetics: A guide to nutri- tional management of renal failure. Am J Clin Nutr 3 1: 1696- 1702, 1978
2. Gotch FA, Sargent JA: A mechanistic analysis of the National Cooperative Dialysis Study (NCDS). Kidney Int 28526-534, 1985
3. Keshaviah PR, Nolph KD, Prowant B, Moore H, Pon- ferrada L, Van Stone J, Twardowski ZJ, Khanna R: Defining adequacy of CAPD with urea kinetics. Adv Petit Dial 6: 173- 177, 1990
4. Teehan BP, Schleifer CR, Brown JM, Sigler MH, Rai- mondo J: Urea kinetic analysis and clinical outcome on CAPD. A five year longitudinal study. Adv Petit Dial 6: 18 l- 185, 1990
5. Gotch FA: Kinetic modeling in hemodialysis, in Nissen- son A, Fine R, Gentile D (eds): Clinical Dialysis (ed 2). Norwalk, CT, Appleton & Lange, pp 118-146, 1991
6. Lindsay RM, Spanner E: A hypothesis: The protein catabolic rate is dependent upon the type and amount of treatment in dialyzed uremic patients. Am J Kidney Dis I8:382-389, 1989
7. Gotch FA, Yarian S, Keen M: A kinetic survey of US hemodialysis prescriptions. Am J Kidney Dis 15:51 l-515, 1990
8. Levine J, Bernard DB: The role of urea kinetic model- ing, TAC.,,, and Kt/V in achieving optimal dialysis: A criti- cal reappraisal. Am J Kidney Dis 4:285-301, 1990
9. Hakim RM: Assessing the adequacy of dialysis. Kidney Int 37:822-832, 1990
10. Depner TA: Standards for dialysis adequacy. Semin Dial 4:245-252, 1991
11. Blake PG. Sombolos K, Abraham G, Weissgarten J, Pemberton R, Chu GL, Greopoulos DG: Lack of correlation between urea kinetic indices and clinical outcomes in CAPD patients. Kidney Int 39:700-706, 1991
12. Flanigan MJ, Fangman J, Lim VS: Quantitating hemo- dialysis: A comparison of three kinetic models. Am J Kidney Dis 17:295-302, 1991
13. Goldstein MB, Jindal KK, Levin A, Stinebaugh BF: Adequacy of hemodialysis: Assessment and achievement, in Jacobson H, Striker G, Klahr S (eds)L Principles and Practice of Nephrology. Philadelphia, PA, Decker, 1991, pp 749-757
14. Teehan BP, Brown JM, Schleifer CR Kinetic model- ing in peritoneal dialysis, in Nissenson A, Fine R, Gentile D (eds): Clinical Dialysis (ed 2). Norwalk, CT, Appleton & Lange, pp 319-329, 1991
15. Vonesh EF, Lysaght MJ, Moran J, Farrell P: Kinetic modeling as a prescription aid in peritoneal dialysis. Blood Purif 9:246-270, 1991
16. Vanholder RC, Ringoir SM: Adequacy of dialysis: A critical analysis. Kidney Int 42:540-558, 1992
17. Frisancho AR: New standards of weight and body composition by frame size and height for assessment of nutri- tional status of adults and the elderly. Am J Clin Nutr 40:808- 819, 1984
18. National Center for Health Statistics, NaJjar MF, Row- land M: Anthropometric reference data and prevalence of overweight, United States, 1976-1980. Vital and Health Sta- tistics, series 11, no. 238. DHHS publication no. (PHS) 87- 1688. Public Health Service. Washington, DC, US Govem- ment Printing Office, October 1987
19. Frisancho AR Anthropometric standards for the as- sessment of growth and nutritional status. Ann Arbor, MI, The University of Michigan Press, 1990
20. New weight standards for men and women. Stat Bull Metrop Life Insur Co 40: 1, 1959
21. 1983 Metropolitan height and weight tables. Stat Bull Metrop Life Insur Co 64:3, 1983
22. Robinett-Weiss N, Hixson ML, Keir B, Sieberg J: The Metropolitan height-weight tables: Perspectives for use. J Am Diet Assoc 84:1480-1481, 1984
23. Roubenhoff R, Kehayias JJ: The meaning and mea- surement of lean body mass. Nutr Rev 49:163-175, 1991
24. Dumin JVGA, Womersley J: Body fat assessed from total body density and its estimation from skinfold thickness; measurements on 481 men and women aged from 16 to 72 years. Br J Nutr 32:77-97, 1974
25. Dubois D, Dubois EF: A formula to estimate the ap- proximate surface area if height and weight be known. Arch Intern Med 17:863-871, 1916
26. Malina RM: Quantification of fat, muscle and bone in man. Clin Orthop 65:9-38, 1969
27. Co&ran WJ, Wong WW, Fiorotto ML, Sheng HP, Klein PD, Klish WJ: Total body water estimated by measur- ing total-body electrical conductivity. Am J Clin Nutr 48:946- 950, 1988
28. Kurtin PS, Shapiro AC, Tomita H, Raizman D: Vol- ume status and body composition of chronic dialysis patients: Utility of bioclectric impedance plethysmography. Am J Nephrol 10:363-367, 1990

980 KOPPLE ET AL
29. Guglielmi FW, Contento F, Laddaga L, Panella C, Francavilla A: Bioelectric impedance analysis: Experience with male patients with cirrhosis. Hepatology 13:892-895, 1991
30. Watson PE, Watson ID, Batt RD: Total body water volumes for adult males and females estimated from simple anthropometric measurements. Am J Clin Nutr 33:27-39, 1980
31. Hume R, Weyers E: Relationship between total body water and surface ama in normal and obese subjects. J Clin Path01 24234-238, 1971
32. Subcommittee on the Tenth Edition of the RDAs, Food and Nutrition Board, Commission on Life Sciences, National Research Council: Recommended Dietary Allowances (ed 10). Washington, DC, National Academy Press, 1989
33. Shils ME, Young VR: Modem Nutrition in Health and Disease (ed 7). Philadelphia, PA, Lea & Febiger, 1988
34. Wilkens K, Brouns-Schir K: Suggested Guidelines for Nutrition Care of Renal Patients. Chicago, IL, American Di- etetic Association, 1992, p 44
35. Krantzler NJ, Mullen BJ, Schutz HG, Grivetti LE, Holden CA, Meiselman HL: Validity of telephoned diet te- calls and records for assessment of individual food intake. Am J Clin Nutr 36:1234-1242, 1982
36. Gersovitz M, Madden JP, Smiciklas-Wright H: Vahd- ity of the 24-hr dietary recall and seven-day food record for group comparisons. J Am Diet Assoc 73:48-55, 1978
37. Karvetti R-L, Knuts L-R: Validity of the estimated food diary: Comparison of 2-day recorded and observed food and nutrient intakes. J Am Diet Assoc 92:580-584, 1992
38. Walser M: Urea metabolism in chronic renal failure. J Clin Invest 53:1385-1392, 1974
39. Kopple JD: Uses and limitations of the balance tech- nique. J Parenter Enter Nutr 11:79S-858 1987 (suppl 5)
40. Keshaviah PR, Nolph KD: Protein catabolic rate calcu- lations in CAPD patients. ASAJO Tram 37:M400-M402, 1991
41. Kjeldahl J: Neue methode zur bestimmung des stickoffs nin organ&hen Korpem. Z Anatytische Chemie 22:366-382, 1883
42. Grimble GK, West MFE, Acuti ABC, Rees RG, Hun- jan MK, Webster JD, Frost PG, Silk DBA: Assessment of an automated chemiluminescence nitrogen analyzer for rou- tine use in clinical nutrition. J Parenter Enter Nutr 12:100- 106, 1988
43. Cottini EP, Gallina DL, Dominguez JM: Urea excre- tion in adult humans with varying degrees of kidney malfunc- tion fed milk, egg or an amino acid mixture: Assessment of nitrogen balance. J Nutr 103:l I-19, 1973
44. Borah MF, Schoenfeld PY, Gotch FA, Sargent JA, Wolfson M, Humphreys MH: Nitrogen balance during inter- mittent dialysis therapy of uremia. Kidney lnt 14:491-500, 1978
45. Grodstein G, Kopple JD: Urea nitrogen appearance, a simple and practical indicator of total nitrogen output. Kidney lnt 16:953, 1979
46. Maroni BJ, Steinman Tl, Mitch WE: A method for estimating nitrogen intake of patients with chronic renal fail- ure. Kidney lnt 27:58-65, 1985
47. Calloway DH, Ode11 ACF, Margen S: Sweat and mis- cellaneous nitrogen losses in human balance studies. J Nutr 101:775-786, 1971
48. Simenhoff ML, Burke JF, Saukkonen JJ, Grdinario AT, Doty R: Biochemical profile of uremic breath. N Engl J Med 297:132-135, 1977
49. Oddoye EA, Margen S: Nitrogen balance studies in humans: Long-term effect of high nitrogen intake on nitrogen accretion. J Nutr 109:363-377, 1979
SO. Waterlow JC, Golden MHN, Garlick PJ: Protein tum- over in man measured with “N: Comparison of end products and dose regimes. Am J Physiol 23S:El65-E174, 1978
51. Matthews DE, Motil KJ, Rohrbaugh DK, Burke F, Young VR, Bier DM: Measurements of leucine metabolism in man from a primed, continuous infusion of L-[I-“C]leu- tine. Am J Physiol 238E473E479, 1980
52. Sargent J: Control of dialysis by a single-pool model. The National Cooperative Dialysis Study. Kidney lnt 23:519- 525, 1983 (suppl 13)
53. Randerson DH, Chapman GV, Farrell PC: Amino acid and dietary status in CAPD patients, in Atkins RC, Farrell PC, Thompson N (eds): Peritoneal Dialysis. Edinburgh, UK, Churchill Livingstone, pp 179-191, 1981
54. Teehan BP, Schleifer CR, Sigler MH, Gilgore GS: A quantitative approach to the CAPD prescription. Petit Dial Bull 5:152-156, 1985
55. Bergstrom J, Alvestrand A, Lindholm B, Tranaeus A, Fttrst P: Proceedings of VIth International Congress on Nutri- tion and Metabolism in Renal Disease, Harrogate, UK Au- gust 1991
56. Blumenkrantz MJ, Kopple JD, Moran JK, Grodstein GP, Cobum JW: Nitrogen and urea metabolism during con- tinuous ambulatory peritoneal dialysis. Kidney lnt 20:78-82, 1981
57. Bergstrom J, Fttrst P, Alvestrand A, Lindholm B: Pro- tein and energy intake, nitrogen balance and nitrogen losses in patients treated with continuous ambulatory peritoneal di- alysis. Kidney lnt 44:1048-1057, 1993
58. Shinaberger JH, Miller JH, Gardner PW: Characteris- tics of available hemodialyzers, in Nissenson A, Fine RN, Gentile D (eds): Clinical Dialysis (ed 2). Norwalk, CT, Ap- pleton & Lange, p 99, 1984
59. Colton CK, Smith KA, Merrill GW, Reece JM: Diffu- sion of organic solutes in stagnant plasma and red cell suspen- sion. Chem Eng Prog Symp 66:85-100, 1970
60. Colton C, Lowrie E: Hemodialysis: Physical principles and technical considerations, in Brenner BM, Rector FC (eds): The Kidney (ed 2). Philadelphia, PA, Saunders, pp 2425-2489, 1981
61. Cheung A, Alford M, Wilson M, Leypoldt J, Hender- son L: Urea movement across erythrocyte membrane during artificial kidney treatment. Kidney lnt 23:866-869, 1983
62. Descombes E, Perriard F, Fellay G: Diffusion kinetics of urea, creatinine and uric acid in blood during hemodialysis. Clinical implications. Clin Nephrol 40:286-295, 1993
63. Skalsky M, Schindhelm K, Farrell PC: Creatinine transfer between red cells and plasma: A comparison between normal and uremic subjects. Nephron 22:514-521, 1978
64. llstrup K, Hanson G, Shapiro W, Keshaviah P: Exam- ining the foundations of urea kinetics. Tram Am Sot Artif Intern Grgans 31:164-168, 1985
65. Colton C, Henderson L, Ford C, Lysaght M: Kinetics of hemodiafiltration of a follow-fiber blood ultrafilter. J Lab Clin Med 85:355-371, 1975

PROPOSED GLOSSARY OF DIALYSIS KINETICS 981
66. Lavender S, Hilton PJ, Jones NF: The measurement of glomerular filtration rate in renal disease. Lancet 2: 1216- 1218, 1969
67. Perrone RD, Steinman TI, Beck GJ, Skibinski CI, Royal HD, Lawlor M, Hunsicker LG: The Modification of Diet in Renal Disease Study: Utility of radioisotopic filtration markers in chronic renal insufficiency: Simultaneous compar- ison of ‘%iothalamate, ‘@?b-DTPA, ‘~Tc-DTPA and inulin. Am J Kidney Dis 16:224-235, 1990
68. Keshaviah P, Carlson G, Wathen R: In vitro and clini- cal evaluation of single needle dialysis. Tram Am Sot Artif Intern Organs 22:367-375, 1976
69. Depner TA, Rizwan S, Cheer AY, Wagner JM, Eder LA: High venous urea concentrations in the opposite arm: A consequence of hemodialysis-induced compartment disequilib rium. Tram Am Sot Artif Intern Organs 37:M141-M143,1991
70. Sherman RA: Recirculation revisited. Semin Dial 4:223, 1991 (editorial)
71. Schneditz D, Van Stone, JC, Daugirdas JT: A regional blood circulation alternative to in-series two compartment urea kinetic modeling. J Am Sot Artif Intern Organs 39:M573-M577, 1978
72. Pedrini LA, Zereik S, Rasmy S: Causes, kinetics and clinical implications of post-hemodialysis urea rebound. Kid- ney Int 34817-824, 1988
73. Ericsson F, Odar-Cederlof I, Eriksson C, Lindgren S, Kjellstrand C: Urea, cteatinine, uric acid, and phosphate spaces and their relationship to total body water during chronic hemodialysis. Tram Am Sot Artif Intern Organs 34:346-350, 1988
74. Kjellstrand C, Skroder R, Cederlof I, Ericsson, F,
Kjellstrand P, Jacobson S: Patient related factors leading to slow urea transfer in the body during dialysis. ASAIO J 40:164-170, 1994
75. Shirai D, Kajimoto Y, Ochi S, Tanaka Y, Wada A, Yano F, Izumi M, Fujita Y: Evaluation of hemodialysis effi- ciency by an edema fluid model. Ren Fail 1463-68, 1992
76. Silver S, DeSimone J, Smith D, Stems R: Dialysis disequilibrium syndrome (DDS) in the rat: Role of the “re- verse urea effect.” Kidney Int 42:161-166, 1992
77. Metry G, Attman P-O, Lomuoth P, Beshara S, Aurell M: Urea kinetics during hemodialysis measured by microdi- alysis-A novel technique. Kidney Int 44:622-629, 1993
78. Bosticardo GM, Alloatti S, Avalle U, Paternoster G, Cestonaro G, Giacchino F: Single-pool urea kinetic model (UKM) and simplified formulas: Comparison of results. J Am Sot Nephrol4:335, 1993 (abstr)
79. Daugirdas JT: Estimation of variable volume single- pool KtN when Kt/V > 1.5: Comparison of logarithmic formulas. J Am Sot Nephrol 3:361, 1992
80. Depner TA: Single compartment model, in Prescribing Hemodialysis: A Guide to Urea Modeling. Boston, MA, Kluwer Academic, pp 65-89, 1991
81. Malchesky P, Ellis P, Nosse C, Magnusson M, Lank- horst B, Nakamoto S: Direct quantification of dialysis. Dial Transplant 11:42-49, 1982
82. Owen WF, Lew NL, Liu Y, Lowrie EG, Lazarus JM: The urea reduction ratio and serum albumin concentration as predictors of mortality in patients undergoing hemodialysis. N Engl J Med 329:1001-1006, 1993
83. Lefebvre NJ, Spanner E, Heidenheim AP, Lindsay R: Kt/V: Patients do not get what the physician prescribes. Tram Am Sot Artif Intern Organs 37:132-133, 1991