document resume ed 396 510 ec 304 892 title · 2013-11-23 · document resume. ec 304 892....
TRANSCRIPT

ED 396 510
TITLE
INSTITUTIONREPORT NOPUB DATENOTEAVAILABLE FROM
PUB TYPE
EDRS PRICEDESCRIPTORS
ABSTRACT
DOCUMENT RESUME
EC 304 892
Improving the Social Skills of Children and Youthwith Emotional/Behavioral Disorders. RetrospectiveSeries on Critical Issues in Emotional/BehavioralDisorders.Council for Children with Behavioral Disorders.ISBN-0-86586-283-496I26p.
Council for Exceptional Children/Council for Childrenwith Behavioral Disorders, 1920 Association Drive,Reston, VA 22091 (CEC Stock No. D5158).Collected Works General (020) Books (010)Guides Non-Classroom Use (055)
MF01/PC06 Plus Postage.Behavior Change; *Behavior Disorders; CognitiveProcesses; Elementary Secondary Education; *EmotionalDisturbances; Family Environment; Generalization;Interaction Process Analysis; *InterpersonalCompetence; *Intervention; Maintenance; PeerRelationship; Preschool Education; PsychoeducationalMethods; Self Management; Social Experience;*Teaching Methods; Validity
The nine readings in this monograph focus on ways toimprove the social skills of students with emotional/behavioraldisorders. The following readings are included: (1) "Analysis ofLiterature on Social Competence of Behaviorally Disordered Childrenand Youth" (Sarup R. Mathur and Robert B. Rutherford, Jr.); (2) "A
Validation of Social Skills for Students with Behavioral Disorders"(Nancy Meadows and others); (3) "Social Interaction Research andFamilies of Behaviorally Disordered Children: A Critical Review andForward Look" (James Fox and Sarah Savelle); (4) "StructuredLearning: A Psychoeducational Approach for Teaching SocialCompetencies" (Arnold P. Goldstein and others); (5) "Use of CognitiveMediation Strategies for Social Skills Training: Theoretical andConceptual Issues" (John W. Maag); (6) "Using a Peer ConfrontationSystem in a Group Setting" (Spencer J. Salend and others); (7)"Social Interaction Training for Preschool Children with BehavioralDisorders" (Mary A. McEvoy and Samuel L. Odom); (8) "EntrapmentEffects and the Generalization and Maintenance of Social SkillsTraining for Elementary School Students with Behavioral Disorders"(Scott R. McConnell); and (9) "Structured Learning UsingSelf-Monitoring To Promote Maintenance and Generalization of SocialSkills across Settings for a Behaviorally Disordered Adolescent"(Cheryl Strobel Kiburz and others). (Individual readings containreferences.) (DB)
**********************************************************************
Reproductions supplied by EDRS are the best that can be madefrom the original document.
***********************************************************************

Impmving the
Social Skills of Child= and YouthWith Emotional/Behavioral
Disorders
U.S. DEPARTMENT OF EDUCATIOPit tip:* of Edwahonal Research and Imprownent
UCATIONAL RESOURCES INFORMATIONCENTER (ERIC)
This document has been reproduced asreceived from the person or organizationoriginating It.
0 Minor changes have been made toimprove reproduction quality.
Points of view or opinions stated in thisdocument do not necessarily representofficial OERI position or policy.
PERMISSION TO REPRODUCE ANCDISSEMINATE THIS MATERIAL
HAS BEEN GRANTED BYrTO THE EDUCATIONAL RESOURCE
INFORMATION CENTER (ERIC)
Lynda! M. Bullock, Robert A. Gable, Robert B. Rutherford, Jr.Series Editors
The Council for Children with Behavioral Disorders
Council forChildren withBehavioralDisorders
2
BEST COPY AVAILABLE

Retrospective Series on Critical Issues in Emotional/Behavioral Disorders
Improving theSocial Skills of Children and Youth
With Emotional/BehavioralDisorders
Lyndal M. Bullock, Robert A. Gable, Robert B. Rutherford, Jr.
Series Editors
The Council for Children with Behavioral Disorders1996
Council forChildren withBehavioralDisorders

About the Council for Childrenwith Behavioral Disorders (CCBD)
1:0131CCBD is an international professional organizationcommitted to promoting and facilitating the educationand general welfare of children/youth with behavioral andemotional disorders. CCBD, whose members includeeducators, parents, mental health personnel, and avariety of other professionals, actively pursues qualityeducational services and program alternatives for per-sons with behavioral disorders, advocates for the needs
of such children and youth, emphasizes research and professionalgrowth as vehicles for better understanding behavioral disorders, andprovides professional support for persons who are involved with andserve children and youth with behavioral disorders.
Council forChildren withBehavioralDisorders
In advocating for the professionals in the field of behavioral disorders,CCBD (a division of The Council for Exceptional Children) endorses theStandards for Professional Practice and Code of Ethics which wasadopted by the Delegate Assembly of The Council for ExceptionalChildren in 1983.
ISBN 0-86586-283-4
CEC Stock No. D5158
Copyright © 1996 by the Council for Children with Behavioral Disorders,
a Division of The Council for Exceptional Children, 1920 Association
Drive, Reston, VA 22091.
Printed in the United States of America
II / CCBD Retrospective Series

Contents
Foreword
Analysis of Literature on Social Competenceof Behaviorally Disordered Children and Youth 1
Sarup R. Mathur and Robert B. Rutherford, Jr.
A Validation of Social Skills for Students withBehavioral Disorders 13
Nancy Meadows, Richard S. Neel, Gerilyn Parkerand Kimberly Timo
Social Interaction Research and Familiesof Behaviorally Disordered Children:A Critical Review and Forward Look 27
James Fox and Sarah Save lie
Structured Learning: A Psychoeducational Approach forTeaching Social Competencies 47
Arnold P. Goldstein, Robert P. Sprafkin, Jane Gershawand Paul Klein
Use of Cognitive Mediation Strategies for Social SkillsTraining: Theoretical and Conceptual Issues 59
John W. Maag
Using a Peer Confrontation Systemin a Group Setting 73
Spencer J. Salend, Nancy Reid Jantzen, and Karen Giek
Social Interaction Training for Preschool Childrenwith Behavioral Disorders 83
Mary A. McEvoy and Samuel L. Odom
Entrapment Effects and the Generalization and Maintenanceof Social Skills Training for Elementary School Students with
Behavioral Disorders 95
Scott R. McConnell
Structured Learning Using Self-Monitoring to PromoteMaintenance and Generalization of Social Skills AcrossSettings for a Behaviorally Disordered Adolescent 111
Cheryl Strobel Kiburz, Sidney R. Miller, and Lonny W. Morrow
CCBD Retrospective Geries / iiimaimommimail

Foreword
This is the first in a series of monographs containing articlespreviously published by the Council for Children with Behavioral
Disorders (CCBD). The topics that together comprise the serieshave been identified by CCBD members as among the mostcritical in dealing with children and youth with emotional/behavioral disorders. This volume is devoted to the issue of
social skills.
There is little doubt that an intact repertoire of prosocial skills isindispensable to normal growth and development. In contrast, a
diminished capacity to initiate and sustain positive socialinteractions can have ruinous effects on life span adjustment.Unfortunately, both accumulated research and classroomexperience substantiate that many students categorized asseriously emotionally disturbed, emotionally handicapped, orbehaviorally disordered are deficient in the critical area of social
skills.
In this volume, we have attempted to provide a selection ofreadings that not only stand alone on merit but also share a
common purposeto furnish practitioners with the tools toimprove the social skills of students with emotional/behavioral
disorders.
Lyndal M. BullockRobert A. Gable
Robert B. Rutherford, Jr.
Series Editors
ti
Retrospective Series
on Critical Issues in
Emotional/BehavioralDisorders
miummimmoimmimmummoil
CCBD Retrospective Series / V

Analysis of Literatureon Social Competenceof Behaviorally DisorderedChildren and Youth
Sarup R. MathurRobert B. Rutherford, Jr.
ABSTRACT: The present review has been conducted to critically evaluate re-cent intervention research on the social competence ofbehaviorally disorderedchildren and adolescents. The purpose of this review was to analyze the conceptof social competence and to evaluate the efficacy of intervention proceduresused in the literature. The results of the review indicate that (a) research hasfailed to build a comprehensive conceptual base for social competence, (b) in-terveraions have resulted in positive behavioral change, and (c) generalizationof behavior across time, stimuli, and responses needs to be improved.
Social competence can be defined as having the social skills necessary tointeract in socially acceptable ways. Behaviorally disordered childrenoften demonstrate lack of appropriate social behaviors. Frequently, thisresults in social rejection by peers which further hampers the success ofmainstreaming (Gresham, 1982). Rejected children report feelings ofextreme loneliness (Asher & Wheeler, 1985) and they often are at-risk fordelinquency and psychosocial adjustment problems (Cowen, Pederson,Babigiari, Izzo, & Trost, 1973; Roff, Sells, & Golden, 1972).
To improve the social acceptance of behavioral ly disordered children inmainstream settings, social skills instruction is essential. Preparation for
social integration should be a necessary part of their educational program(Hollinger, 1987). If these students had acquired functional social compe-tence, they probably would not have been classified as behaviorallydisordered. Regular classroom placement of a behaviorally disorderedstudent without providing training to enhance social competence is askingfor failure. Available literature suggests that social skills training is aviable intervention to increase the successful mainstreaming of behavior-ally disordered children (LaNunziata, Hill, & Krause, 1981).
The purpose of this article is to (a) analyze the conceptual framework ofsocial competence, (b) analyze different approaches proposed for socialskills training that enhance social competence of behaviorally disorderedchildren, and (c) critically evaluate the success of these interventions interms of promoting generalization.
Reprinted from Monograph in
Behavioral Disorders, Vol. 12,
Summer 1989, pp. 72-86
There is a great variability inhow social competence and
social skills are defined; socialcompetence and social skillsdo not imply the same concept.
lowammilimmoor
2 / CCBD Retrospective Seriesaismarea
The present review focuses on thepast 5 years of social competenceresearch with behaviorally disorderedchildren and youth. It builds on anearlier review conducted by Schloss,Schloss, Wood, and Kiehl (1986)which analyzed 25 social skillsstudies with behaviorally disorderedstudents. The present review ana-lyzed 17 additional publishedarticles on social competence/socialskills interventions.
CONCEPTUALFRAMEWORK
Much attention has been givenrecently to training behaviorallydisordered children and youth insocial skills, but not to developing asound conceptual base of whatconstitutes social competence(Gresham, 1986; Gresham & Elliott,1987; Hollinger, 1987). Indeed, thereis a great variability in how socialcompetence and social skills aredefined; social competence andsocial skills do not imply the sameconcept. Social skills are specificbehaviors necessary for an individualto perform a task competently. Incontrast, social competence repre-sents an evaluative term based uponjudgment. given certain criteriathat a person has adequately per-formed a task (Gresham, 1986;McFall, 1982).
Social Competence
Although social competence encom-passes a wide area of cognitive andbehavioral skills, generally the termrefers to a person's effective partici-pation in a social setting. The termsocial competence has been definedin many ways that reflect the varyingperspectives of social theorists. Sometheorists have defined it as a combi-nation of adaptive behavior and socialskills (Gresham & Elliott, 1987;Leland, 1978), while others haveviewed it in terms of social interac-tion and social reciprocity (Gaylord-
Ross & Haring, 1987; Hollinger,1987). Meichenbaum, Butler, andGruson (1981) presented a theoreti-cal model of social competence basedon a cognitive behavior modificationparadigm that contends a focus onovert behaviors is necessary but notsufficient in studying social compe-tence. Meichenbaum and his col-leagues assert that the role ofcognitive process also must be takeninto account in viewing socialcompetence as a construct. From thisperspective, the acquisition of socialcompetence depends upon anindividual's cognitive awareness ofhis or her social situation.
These definitions reveal differencesin their relative emphasis. Thesedifferences may be best considered assemantic disagreements, becauseeach of these definitions refers toseparate constructs that may or maynot empirically relate to each other.
Social Skills
Social skills are viewed as part of theglobal construct known as socialcompetence. Gresham (1986) hasdescribed three types of social skillscomprising social competence whichinclude (a) peer acceptance, (b)behavioral skills, and (c) socialvalidity. Peer acceptance involvesmeasuring peer acceptability orpopularity to define children associally skilled. Few of the studiesreviewed focused upon the peeracceptance definition or usedsociometric assessment to evaluatethe effectiveness of interventions(Bierman, 1986; Sainato, Maheady, &Shook, 1986; Tiffen & Spence,1986).
When social skills are defined assituationally.specific observablebehaviors, the antecedents andconsequences of the particular socialbehaviors are identified, specified,and operationalized for the purpose ofassessment and intervention. Many

researchers have addressed socialskills in behavioral terms. Thebehavioral definitions of social skillsinclude: increasing rate of socialinitiation (Fox, Shores, Lindeman, &Strain, 1986), communicativeinteraction (Bierman, 1986; Gold-stein & Wickstrom, 1986), sharing,play organization (Odom & Strain,1986), eye contact, facial expression,body posture, voice tone; and givingand following instructions (Serna,Schumaker, Hazel, & Sheldon,1986). Although behavioral defini-tions identify the particular socialbehaviors, the social validity of thesebehaviors has not been ascertained.
The social validity definition not onlyspecifies behaviors in which thechild is deficient but also definesthese behaviors as socially skilled,based upon their relationship tosocially important outcomes. Twostudies in the present review men-tioned employing social validationmeasures to demonstrate the effec-tiveness of intervention (Christoff etal., 1985; Serna et al., 1986).
Definitions which are premised onthe global aspects of maladaptivebehavior in terms of social skillsdeficits are of limited usefulnessbecause of their lack of specificity.Rather, they become ambiguous andcomplex. The field needs a definitionthat incorporates a balance betweenbeing too global or too molecular.
Theoretical Basis
There are two main reasons for thelack of a sound conceptual base ofsocial competence: a lack of appro-priate definition, and a unified theoryof social competence that is bothpractical and coherent. A theoreticalconceptualization of social compe-tence emphasizing adaptive behaviorwas developed by Leland (1978).Adaptive behavior is comprised ofthree components: (a) independentfunctioning, (b) personal responsibil-
BEST COPY AVAILABLE
ity, and (c) social responsibility. Asocially responsible and sociallyskilled individual performs appropri-ate behavior in terms of societalexpectations. Due to the lack ofempirical data support, the validity ofLeland's (1978) conceptualization isstill in question.
In contrast to Leland's perspective,Hollinger (1987) proposed a morebalanced concept which incorporatesboth molar and molecular levels ofanalysis of social competence. Fromthe molecular perspective, theanalysis focuses on observablebehaviors, which entails an under-standing of the specific behaviors orsocial skills comprising socialcompetence. In contrast, the molarperspective focuses on broad dimen-sional analysis of social competence.
More recently, Gresham and Elliott(1987) conceptualized social compe-tence as being comprised of twointerrelated components: adaptivebehavior and social skills. Theeffectiveness and degree to which anindividual meets social/culturalstandards of personal independenceand social responsibility is reflectiveof the adaptive behavior. According toGresham and Elliott, an adaptivebehavior includes independentfunctioning skills, physical develop-ment, language development, andacademic competencies. Social skillsrepresent behaviors which in specificsituations predict important socialoutcomes. Due to a failure to provideclear distinctions between adaptivebehavior and social skill, theexplicitness of this conceptualizationis limited.
A recent concept in the field of socialcompetence is entrapment of behavior(McConnell, 1987). Entrapment isdescribed as a process through whichthe social behavior of a child comesunder the control of naturallyoccurring reinforcers. This can occurwhen changes in the social behavior
There are two main reasons forthe lack of a sound conceptual
base of social competence: alack of appropriate definition,and a unified theory of socialcompetence that is both
practical and coherent.
1110111111111=11111111111111
CCBD Retrospective Series / 3

Contemporary research onintervention procedures
reveals two main approachesof developing socialcompetence: social skillstraining and social problemsolving.
4 / CCBD Retrospective SeriesImilimmmemismi
of the child are reinforced by thesocial behavior of others duringinteractions in naturalistic settings.As a result, social skills developthrough an elaboration of thesebehaviors. However, to facilitate theentrapment of social interaction,attention is required to the selectionof target behavior and the use ofintervention procedures.
Viewed together, these aforemen-tioned conceptualizations representdiverse views of the construct ofsocial competence. However, acohesiveness noted within thediversity of views is the perception ofsocial competence as a globaljudgment of a person's adequatesocial functioning. Along withdeveloping a conceptual frameworkfor social competence, it is importantto consider how social skills thatconstitute social competence aretaught to behaviorally disorderedchildren.
INTERVENTIONRESEARCH
To examine the effectiveness ofintervention procedures in promotingthe social competence of behaviorallydisordered children and youth, 17articles relating to interventionresearch were reviewed. Each of thesestudies was analyzed according to thecomponents developed by Schloss etal. (1986) which include subjects,target lehavior, and proceduresemployed. In addition, setting,experimental design, and results wereincluded in the present analysis (seeTable 1).
Major Intervention Approaches
Contemporary research on interven-tion procedures revealed two mainapproaches of developing socialcompetence. One approach focuseson systematic teaching of specificprosocial behaviors to behaviorallydisordered children, and is referred
to as social skills training. Thisapproach employs direct instruction,modeling, prompting, rehearsal ofspecific social skills, and positivereinforcement.
A study conducted by Bierman(1986) illustrates this approach.Participating in the study were 27preadolescents who were perceived asunpopular and lacking conversationalskills. Each of these subjects engagedin cooperative activities with twosocially accepted classmates. Half ofthese triads received coaching insocial conversation skills, while theothers received nonspecific adultsupport. Children who received socialskills training displayed moreconversational skills and receivedmore peer support. Similar improve-ment in target behaviors of behavior-ally disordered children as a result ofsocial skills training has beendocumented in several other studies(Goldstein & Wickstrom, 1986;Kohler & Fowler, 1985; Tiffen &Spence, 1986).
A second approach to developingsocial competence identified in thepresent review focuses on socialcognitive processes and is referred toas social problem-solving. Forexample, Spivack and his colleagues(Spivack, Platt, & Shure, 1976;Spivack & Shure, 1974) initiated theuse of this approach in their studies.These studies reported that childrenwho received training in interperson-al cognitive problem-solving in-creased their abilities to generatealternative solutions and anticipateconsequences.
In the past, social problem-solvingwas considered to be a promisingtechnique for normal samples(without handicaps) as a preventivemeans of fostering social competence.However, a recent trend in theapplication of problem-solvinginterventions has occurred with
,c)inical populations. A tentativeh .1

evidence exists for its effect onacquisition of social skills with shy(Christoff et. al.,1985) and aggres-sive (Dubow, Huesmann, & Eron,1987; Vanghn, Ridley, & Bullock,1984) children. Success of thisapproach has also been demonstratedwith severely emotionally disturbedchildren (Amis, Gesten, Smith,Clark, & Stark, 1988; Yu, Harris,Solovitz, & Franklin, 1986).
Yu et al. (1986) employed a socialproblem-solving (SPS) procedurewith 7- to 12-year- dd boys who werechild psychiatric outpatients demon-strating behavioral problems. Theresults demonstrated that SPS trainedyoungsters generated more problemsolutions and showed greater reduc-tions in acting out behaviors relativeto those under traditional psychother-apy treatment. Similar findings wereobtained by Vaughn et al. (1984)using a social problem-solvingintervention with aggressive children.
Of the 17 studies reviewed, 12employed social skills training while5 studies used a problem-solvingtraining procedure, either by itself oralong with other procedures. Dubowet al. (1987) compared the effective-ness of cognitive training, behavioraltraining, cognitive-behavioraltraining, and play training. Theresults indicated that the childrenreceiving cognitive-behavioral andplay interventions significantlydecreased aggressive behavior andincreased prosocial behaviors thandid those exposed to either cogni,iveor behavioral training alone.
In general, the studies reviewed thatemployed a social problem-solving orsocial skills training approachproduced positive results. However,some of the authors indicated limitedsuccess because intervention did notresult in positive behavior change inall the subjects or in all the targetbehavior:. (Amish et al., 1988; Sasso,Mitchell, k Struthers, 1986; Serna et
al., 1986; Tiffen & Spence, 1985; Yuet al., 1986).
Peer-Mediated Interventions
Recently, researchers have begun toinvestigate the use of peer-mediatedapproaches to increasing socialcompetence (Brady et al., 1984;Brady, Shores, McEvoy, Ellis, & Fox,1987; Goldstein & Wickstrom, 1986;Gunter, Fox, Brady, Shores, &Cavanaugh, 1988; Kohler & Fowler,1985, Odom & Strain, 1986; Sasso etal., 1986).
Odom and Strain (1986), for exam-ple, compared the relative effective-ness of peer-initiated and teacher-antecedent interventions with autisticchildren. In the peer-initiationcondition, confederates were taught toinitiate interaction with the autisticchildren, whereas in the teacher-antecedent condition teachersprompted the autistic children toinitiate with confederates who hadbeen taught to reciprocate. During theteacher-antecedent condition,children's social initiations andresponses increased, and longerchains of social interactions werenoticed. The peer-initiation proce-dure also reliably increased thesocial responses of autistic children.
Goldstein and Wickstrom (1986)demonstrated success with threebehaviorally disordered preschoolchildren using peer-mediatedintervention. The interventionresulted in higher rates of interactionthat stayed above baseline levelsduring the maintenance condition foreach of the children.
Peer-mediated interventions arebased on the assumption thatchildren develop social skills throughtheir interactions with peers (Hol-linger, 1987; Kohler & Fowler, 1985).Learning a particular prosocialbehavior in the presence of peersprovides a natural environment whichmay facilitate maintenance and
BEST COPY AVAILABLE
Peer-mediated interventions
are based on the assumption
that children develop social
skills through their interactions
with peers.
CCBD Retrospective Series / 5

Table 1
Qualitative Aspects of intervention Research Focusing on
Citations Subjects Setting Target BehaviorsAmish, Gesten, Smith, Clark,& Stark (1988)
25 severely emotionallydisturbed children
School Problem-solving skills, socialadjustment
Bierman (1986) 27 unpopular children withconversational problems
School Conversational skills positivepeer responses
Brady, Shores, Gunter, 1 autistic adolescent boy School Social interactionMcEvoy, Fox, & White (1984)
Brady, Shores, McEvoy, Ellis, 2 autistic children School Social interaction& Fox (1987)
Christoff, Scott, Kelly,Schlundt, Baer, & Kelly
6 shy preadolescents School Problem-solving skills,conversational skills
(1985)
Dubow, Huesmann, & Eron(1987)
104 aggressive boys School Promote prosocial behavior,decrease aggression
Fox, Shores, Lindeman, & 3 withdrawn preschool School Social initiations, peerStrain (1986) children responses
Goldstein & Wickstrom(1986)
3 behaviorally disordered,language-delayed preschoolchildren
School Communicative interaction
Gunter, Fox, Brady, Shores, &Cavanaugh (1988)
2 socially withdrawn autisticboys
School Social interaction initiation,soliciting response
Kohler & Fowler (1985) 3 young girls with behaviorproblems
School Prosocial responses
Odom & Strain (1986) 3 preschool autistic boys School Social initiation, responses
Sainato, Maheady, & Shook 3 socially withdrawn School Social interaction, sociometric(1986) kindergarten children stand ing
Sasso, Mitchell, & Struthers(1986)
4 autistic, 4 nonhandicappedchildren
School Cooperative interaction,instructional interaction
Serna, Schumaker, Hazel, & 12 behavior-problem County juvenile Youth skills, parent skills,Sheldon (1986) adolescents and 6 parents court office youth parent interaction skills
Tiffen & Spence (1986) 25 isolated and 25 rejectedchildren
School Social competence
Vaughn, Ridley, & Bullock 24 aggressive children School Problem-solving behavior(1984)
Yu, Harris, Solovitz, &Franklin (1986)
35 behaviorally disorderedboys
Clinic Social cognitive skills,behavioral adjustment
6 / CCBD Retrospective SeriesMIIIIIIIII1111611111111

Behaviorally Disoreivnd Children and Youth from 1984 to 1988
ProceduresInstruction, discussion, modeling, role-play, feedback
Social skill training, peer experience
Instructions, modeling, physical guidance,prompting
Multiple peer exemplar training
Problem-solving, conversation training,group training
Cognitive training, behavioral training,combined training, attention/play training
Prompting, praising, fading
Direct instruction, peer training, teacherprompting
Prompt, praise
Peer training, group contingency,modeling, rehearsal, feedback
Peer-initiated intervention, teacher-antecedent intervention
Role-play, environmental manipulation
Peer-tutoring, structured interactionactivities
Reciprocal social skill training
Instruction, discussion, modeling, role-play, feedback, social reinforcement
Role-play, practice, teaching languageconcepts, cue sensitivity, goal identification
Social problem-solving, role-play groupdiscussions, drawing projects, parentalinvolvement
Experimental Design
Group study
Group study
Multiple baseline acrosspeers
Multiple baseline acrosspeers
Multiple baseline acrossskills
Group study
Withdrawal, multiple baselineacross subjects
Multiple baseline acrosssubjects
Multiple baseline acrosspeers
Multiple baseline acrossbehavior and reversal
ResultSF'S trained subjects generated moresolutions
Increase in social skill performance
Increase in social interaction
Generalized behavior change in one subject
Improvement in target skills
Positive results in combined and attention/play training
Increase in social interaction of 2 children
Increase in target behavior
Increase in target behavior in one subject
Positive effects on interaction
Alternating treatment design Differential effects of interventions
Multiple baseline acrosssubjects
Inverted design
Multiple baseline acrossskills, control group design
Group study
Croup study
Group study
Positive results in both target behaviors
Structured interaction more effective thantutoring
Overall improvements in each of the trainedskills areas
Failed to produce the effectiveness of SST
Increase in target behavior
Increase in social cognitive skills
CCBD Retrospective Series / 7ammimmmN

An important consideration injudging the success of an
intervention relates to theextent of behavioralgeneralization.
111111111=11111101111111111111111111MINIIIIIIIIIIIM
8 / CCBD Retrospective Seriessimmumminuminmsiii
generalization of the newly learnedbehavior. Conducting social skillstraining in the peer group may be aneffective way of addressing the socialadjustment problems faced bymainstreamed behaviorally disor-dered children. Although there isevidence that various groups ofbehaviorally disordered childrenbenefit from these interventions, itappears that particularly withdrawnand autistic children, because oftheir often limited language skills,would benefit most from peer-mediated interventions (Brady et al.,1984; Brady et al., 1987; Goldstein& Wickstrom, 1986; Gunter et al.,1988).
GENERAUZATION
An important consideration injudging the success of an interventionrelates to the extent of behavioralgeneralization (e.g., Baer, Wolf, &Risley, 1968). Behavioral researchershave addressed the difficulties inachieving durable behavior change(Keeley, Shemberg, & Carbonell,1976; Stokes & Baer, 1977). Morerecently, Rutherford and Nelson(1988) found in their review ofliterature that less than 2% of theapproximately 5,300 articles pub-lished in the journals from 1977 to1988 contained studies that ad-dressed maintenance and generaliza-tion of educational treatment effects,and less than 1% contained studiesthat systematically programmed formaintenance and generalization ofthese effects across settings, re-sponses, trainers, or time.
Following the format developed bySchloss et al. (1986), the 17 articlesreviewed in the present study wereanalyzed with regard to the extent thatstimulus generalization, responsegeneralization, and generalizationover time were tested or programmedand whether these forms of generali-zation were found (Table 2).
ill
The findings of the present reviewthat relate to generalization effectsindicate that improvement is neededin achieving generalization of sociallycompetent behavior across time,stimuli, and responses. Of the 17intervention research studies reportedin Table 2, only 1 0 includedevidence of programming for stimulusgeneralization, with only 9 showingpositive results. Response generaliza-tion was reported to be measured in 8studies, of which 7 showed favorableresults. And 12 studies includedfollow-up data to indicate mainte-nance of results over time.
Generalization strategies included theuse of nontraining settings to transferand maintain performance (Gunter etal., 1988); nonintrusive use ofprompting to promote target behaviors(Goldstein & Wickstrom, 1986);response-dependent fading of stimuli(Fox et al., 1986); group-orientedcontingencies (Kohler & Fowler,1985); peer reciprocity and peerentrapment (Kohler & Fowler, 1985);overlearning of material (Amish etal., 1988); developing problem-solving skills (Yu et al., 1986); andsystematic inclusion of parentalinvolvement (Serna et al., 1986).Multiple peer exemplar training alsoappeared to be a viable component ofgeneralization programming (Brady etal., 1987; Gunter et al., 1988).
Despite the small number of studiesthat indicated generality and mainte-nance of effects, the literature revealsan overall development of generaliza-tion technology (Rutherford &Nelson, 1988).
CONCLUSION
There is strong evidence suggestingthe effectiveness of social skillsinterventions with behaviorallydisordered children and youth.However, there are several criticallimitations apparent in the literatureincluding a lack of comprehensive
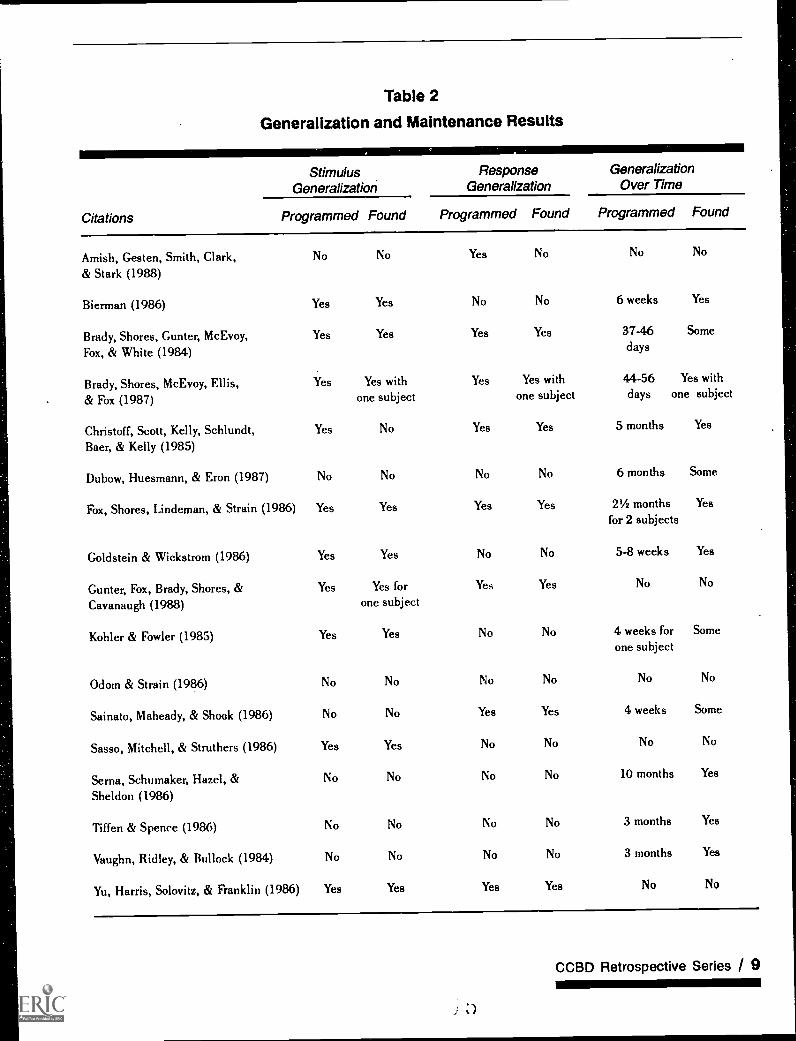
Table 2
Generalization and Maintenance Results
StimulusGeneralization
ResponseGeneralization
GeneralizationOver Time
Citations Programmed Found Programmed Found Programmed Found
Amish, Gesten, Smith, Clark, No No Yes No No No
& Stark (1988)
Bierman (1986) Yes Yes No No 6 weeks Yes
Brady, Shores, Gunter, McEvoy,Fox, & White (1984)
Yes Yes Yes Yes 37-46 Somedays
Brady, Shores, McEvoy, Ellis,& Fox (1987)
Yes Yes withone subject
Yes Yes withone subject
44-56 Yes withdays one subject
Christoff, Scott, Kelly, Schlundt, Yes No Yes Yes 5 months Yes
Baer, & Kelly (1985)
Dubow, Huesmann, & Eron (1987) No No No No 6 months Some
Fox, Shores, Lindeman, & Strain (1986) Yes Yes Yes Yes 21/2 months Yes
for 2 subjects
Goldstein & Wickstrom (1986) Yes Yes No No 5-8 weeks Yes
Gunter, Fox, Brady, Shores, &Cavanaugh (1988)
Yes Yes forone subject
Yes Yes No No
Kohler & Fowler (1985) Yes Yes No No 4 weeks for Some
one subject
Odom & Strain (1986) No No No No No No
Sainato, Maheady, & Shook (1986) No No Yes Yes 4 weeks Some
Sasso, Mitchell, & Struthers (1986) Yes Yes No No No No
Serna, Schumaker, Hazel, & No No No No 10 months Yes
Sheldon (1986)
Tiffen & Spence (1986) No No No No 3 months Yes
Vaughn, Ridley, & Bullock (1984) No No No No 3 months Yes
Yu, Harris, Solovitz, & Franklin (1986) Yes Yes Yes Yes No No
CCBD Retrospective Series / 9

Most of the research in thearea of social skills has
focused upon changes inspecific behaviors without
considering their social utility incontext.
110111111111111111111111111=11
10 / CCBD Retrospective SeriesINIMMONINNIMINMEMENN
conceptual framework of socialcompetence, a lack of social valida-tion of interventions, and insufficientgeneralization.
The results of the review by Schlosset al. (1986) indicate severallimitations existing in the literature toinclude: (a) a lack of comprehensiveconceptualization, (b) a lack of socialimportance of training effects, (c)poorly defined and inconsistentlyapplied training tactics whichdecreases the likelihood of replica-tion of research, and (d) failure todemonstrate generalization acrosssettings, responses, and time. Theresults of the present review are inagreement with the aforementionedfindings of Schloss et al. (1986).
The field remains limited in terms ofa general conceptual framework ofsocial competence. Researchers areusing their own idiosyncraticdefinitions to define almost anybehavior as a social skill (Gresham,1986). In the studies reviewed, targetbehaviors included eye contact,loudness of speech, giving andreceiving compliments, socialinitiation, conversational skills,social adjustment, listening toinstructions, and so forth. Thepurpose of response discrete defini-tion is to operationalize the behaviorwhich further enhances the possibili-ty of the replication of the study.However, the disadvantages offocusing on discrete responsedefinitions include: (a) an emphasison isolated responses in which globalconceptual systems are disregarded(Schloss et al., 1986), (b) limitedsocial validity of behavior, and (c)limited generalization of behavior. Weneed a conceptual system which isbroad enough to incorporate bothprecision in evaluation and widerange of behavior.
With some notable exceptions, mostof the research in the area of socialskills has focused upon changes in
b
specific behaviors without consider-ing their social utility in context.Future research should be directed atassessing those specific behaviorsthat are best predictors of an individ-ual's standing on important socialoutcomes (Gresham, 1986).
Simply teaching a specific prosocialbehavior or strategy of social behaviorto increase the quantity of behavior isgenerally not the goal of socialcompetence training. The goal is todemonstrate the long-term mainte-nance and generalization of thedesired social behavioral changes ofbehaviorally disordered children(Stokes & Baer, 1977).
Appropriate social behaviors mustcontinue after intervention ceasesand behavior must occur outsidethe training settings. Althoughmuch success has been noted withdeveloping social competence ofbehaviorally disordered children,the limited ability of social skillstraining to produce generalizablechanges in behavior raises thequestion of how training proce-dures can be improved.
REFERENCES
Amish, P L., Cesten, E. L., Smith, H. B.,Clark, H. B., & Stark, C. (1988).Social problem-solving training forseverely emotionally and behaviorallydisturbed children. BehavioralDisorders, 13, 175-186.
Asher, S. R., & Wheeler, V. A. (1985).Children's loneliness: A comparisonof rejected and neglected peer status.Journal of Consulting and ClinicalPsychology, 53, 500-505.
Baer, D. M., Wolf, M. M., & Risley, T.R. (1968). Some current dimen-sions of applied behavior analysis.Journal of Applied BehaviorAnalysis, I, 91-97.
Bierman, K. L. (1986). Process of changeduring social skills training withpreadolescents and its relation totreatment outcome. Child Develop-ment, 57, 230-24.0.

Brady, M. P., Shores, R. E., Gunter, R.,McEvoy, M. A., Fox, J. J., & White, C.(1984). Generalization of an adoles-cent's social interaction behavior viamultiple peers in a classroom. Journalof the Association for Persons withSevere Handicaps, 9, 278-286.
Brady, M. P., Shores, R. E., McEvoy, M.A., Ellis, D., & Fox, J.J. (1987).Increasing social interaction ofseverely handicapped autisticchildren. Journal of Autism andDevelopmental Disorders, 17, 375-
390.Christoff, K. A., Scott, W. N., Kelly, M.
L., Schlundt, D., Baer, G., & Kelly, J.A. (1985). Social skills and socialproblem-solving training for shy
young adolescents. Behavior Therapy,16, 468-477.
Cowen, E. L., Pederson, A., Babigian, H.,Izzo, L. D., & Trost, M. A. (1973).Long-term follow-up of early detectedvulnerable children. Journal ofConsulting and Clinical Psychology,41, 438-446.
Dubow, E. F., Huesmann, R., & Eron, L.D. (1987). Mitigating aggression andpromoting prosocial behavior inaggressive elementary schoolboypBehavior Research Therapy, 25, 527-
531.Fox, J. J., Shores, R. E., Lindeman, D., &
Strain, P S. (1986). Maintaining socialinitiations of withdrawn handicappedand nonhandicapped preschoolersthrough a response dependent fadingtactic. Journal of Abnormal ChildPsychology, 14, 387-396.
Gaylord-Ross, R., & Haring, T. (1987).Social interaction research foradolescents with severe handicaps.Behavioral Disorders, 12, 264-275.
Goldstein, H., & Wickstrom, S. (1986).Peer intervention effects on communi-cative interaction among handicappedand nonhandicapped preschoolers.Journal of Applied Behavior Analysis,19, 209-214.
Gresham, E M. (1982). Misguidedmainstreaming: The case for socialskills training with handicappedchildren. Exceptional Children, 48,422-433.
Gresham, E M. (1986). Conceptual anddefinitional issues in the assessmentof children's social skills: Implicationsfor classification and training. Jow nalof Clinical Child Psychology, 15, 3-
15.
Gresham, F M., & Elliott, S. N. (1987).The relationship between adaptivebehavior and social skills: Issues indefinition and assessment. Journal ofSpecial Education, 21, 167-181.
Gunter, P. Fox, J. J., Brady, M. P., Shores,R. E., & Cavanaugh, K. (1988).Nonhandicapped peers as multipleexemplars: A generalization tactic forpromoting autistic students' socialskills. Behavioral Disorders, 13, 116-
126.Hollinger, J. D. (1987). Social skills for
behaviorally disordered children aspreparation for mainstreaming:Theory, practice, and new directions.Remedial and Special Education, 8,17-27.
Keeley, S. M., Shemberg, K. M., &Carbonell, J. (1976). Operant clinicalintervention: Behavior management orbeyond? Where are the data?
Behavior Therapy, 7, 292-305.Kohler, F., & Fowler, S. A. (1985).
Training prosocial behaviors to youngchildren: An analysis of reciprocitywith untrained peers. Journal ofApplied Behavior Analysis, 18, 187-
200.LaNunziata, L. J., Hill, D. S., & Krause,
L. A. (1981). Teaching social skills inclassrooms for behaviorally disor-dered students. Behavioral Disorders,6, 238-246.
LeLand, H. (1978). Theoretical consider-ations of adaptive behavior. In A.Coulter & H. Morrow (Eds.), Adaptive
behavior: Concepts and measurements(pp. 21-44). New York: Gnme &Stratton.
McConnell, S. R. (1987). Entrapmenteffects and the generalization andmaintenance of social skills trainingfor elementary school students withbehavioral disorders. BehavioralDisorders, 12, 252-263.
McFall, R. M. (1982). A review andreformulation of the concept of social
skills. Behavioral Assessment, 4, 1-33.
Meichenbaum, D., Butler, L., & Gruson,L. (1981). Toward a conceptual modelof social competence. In J. D. Wine &M. D. Smye (Eds.), Social competence.New York: Guilford.
Odom, S.. L., & Strain, P S. (1986). Acomparison of peer-initiation andteacher antecedent interventions forpromoting reciprocal social interactionof autistic preschoolers. Journal ofApplied Behavior Analysis, 19, 59-71.
CCBD Retrospective Series / 11tioniNoimomoom
BEST COPY AVAILABLE

12 / CCBD Retrospective Series
Roff, M., Sells, B., & Golden, M. (1972).Social a4ustment and personalitydevelopment in children. Minneapolis:University of Minnesota Press.
Rutherford, R. B., Jr., & Nelson, C. M.(1988). Generalization and mainte-nance of treatment effects. In J. C.Witt, S. N. Elliott, & E M. Gresham(Eds.), Handbook of Behavior Therapyin Education. New York: Plenum.
Sainato, D. M., Maheady, L, & Shook, G.L. (1986). The effects of a classroommanager role on the aocial interactionpatterns and social status of with-drawn kindergarten students. Journalof Applied Behavior Analysis, 19, 187-195.
Is
Sasso, G. M., Mitchell, V. M., & Struth-ers, E. M. (1986). Peer tutoring versusstructured interaction activities:Effects on the frequency andtopography of peer initiations.Behavioral Disorders, 11, 249-259.
Schloss, P J., Schloss, C. N., Wood, C. E.,& Kiehl, W. S. (1986). A criticalreview of social skills research withbehaviorally disordered students.Behavioral Disorders, 12, 1-14.
Serna, L. A., Schumaker, J. B., Hazel, J.S., & Sheldon, J. B. (1986). Teachingreciprocal social skills to parents andtheir delinquent adolescents. Journalof Clinical Child Psychology, 15, 64-77.

A Validation of Social Skillsfor Students withBehavioral Disorders
Nancy MeadowsRichard S. NeelGerilyn ParkerKimberly Timo
ABSTRACT Secondary students with behavioral disorders, regular educationsecondary students, secondary teachers of students with behavioral disorders,regular education secondary teachers, and parents of both student populationsfrom the states of Washington, Iowa, and Colorado were asked to complete theAdolescent Social Skills Survey (Walker, Todis, Holmes, & Horton, 1988). Thesurvey consists of 48 items about how adolescents relate to themselves, to other
adolescents, and to adults. Overall, all groups thought all items on the surveywere important. As a group, students with serious behavioral disorders ratedinterpersonal skills higher than other skills on the survey. However, these samestudents consistently rated all items lower. These students also rated compli-ance and cooperation skills as less important than the two teacher groups.Discussion centers around the implications these results have on programmingfor seriously behaviorally disordered students, with future needs being directedtoward developing a functionally valid list of critical social skills.
Since the enactment of Public Law 94-142 and its mandate of "leastrestrictive environment," exceptional students have been mainstreamedinto regular classrooms in greater numbers than ever before. Unfortunate-ly, the physical placement of mildly handicapped children in the presenceof their nonhandicapped peers has not resulted in mutual social interac-tion and acceptance between the two groups (Gresham, 1982; Sabornie,1985). Research has shown that all handicapped students do not have theappropriate social skills to succeed in mainstream situations nor do theyacquire the necessary social skills by modeling their nonhandicappedpeers (Asher & Hymel, 1981; Cartledge, Frew, & Zaharias, 1985; Gre-sham, 1981, 1982). Moreover, studies have demonstrated that there aretypically low rates of social interaction between mainstreamed handi-capped children and their classmates (Bruininks, 1978; Gresham, 1981;Morgan, 1977).
For students with serious behavioral disorders, social skill deficienciesmay be the most critical deterrent to social acceptance (Schloss, Schloss,Wood, & Kiehl, 1986). By definition, these students are set apart by theirlack of social competence. Numerous studies have indicated that (a)
Reprinted from Behavioral
Disorders, VoL 16, Number 3,
May 1991, pp. 200-210
CCBD Retrospective Series / 13alm

Investigation of currentinstruction of 'social skills has
provided mixed results,indicating that new socialbehaviors may be learned butthey do not generalize across a
variety of social situations anddo not maintain afterintervention is terminated.
1111111111=1111M111=1111111111
14 / CCBD Retrospective Seriesimiimmoommmismoino
students with behavioral disorderslack appropriate social skills(Gresham, 1982, 1986; Kauffman,1989); (b) many students withbehavior problems are poorlyaccepted by their peers (Asher &Hymel, 1981; Asher & Taylor, 1983;Gresham, 1986; Michelson &Wood, 1980; Sabornie, 1985); and(c) many students with behavioraldisorders are rated by their teachersas having inadequate social skills(Gresham, 1982, 1986). Thesefindings indicate that, prior toplacing seriously behaviorallydisordered students in mainstreamclasses, educators need to lookmore closely at students' specificsncial skills deficits and theirlevels of social competency.
It has been well documented in theliterature that social skills have animportant relationship to all aspectsof students' lives: educational, social,and employment (Combs & Slaby,1977; Gronlund & Anderson, 1962;Michelson & Wood, 1980; Roff,Sells, & Golden, 1972; Ullman,1957). Furthermore, problems inthese areas have long lasting effects.Adults who have documented socialdeficits as children are reported tohave psychological problems (Gott-man, Gonso, & Schuler, 1976;Sheperd, 1980), unsuccessfulemployment histories (Knold, 1985;Neel, Meadows, Levine, & Edgar,1988), negative military servicerecords (Roff, 1970), and increasedincidences of suicide (Stengel,1973). Psychologists, employers, andeducators agree that early interven-tion should occur within the schoolsetting in an attempt to counteractthese problems (Gottman et al., 1976;Knold, 1985; Roff, 1970; Roff et al.,1972; Sheperd, 1980).
Investigatim of current instruction ofsocial skills has provided mixedresults, indicating that new socialbehaviors may be learned but they (innot generalize across a variety of
t
social situations and do not maintainafter intervention is terminated(Bellack, 1983; McConnell, 1987).Social skills training programs havenot produced behavioral changes thatmake handicapped children moresocially acceptable (Kauffman,1989).
One of the ..asons suggested for thelack of succcss of social skillsprograms is that the skills targeted forinstruction may not be those whichwill lead to positive social exchanges.As Kauffman (1989) states, "The goalof intervention must be to help thesocially isolated individual becomeenmeshed or entrapped in positive,reciprocal, self-perpetuating socialexchanges, which can be done onlyby carefully choosing the targetskills" (p. 336). Target skills mustrelate to peers or other importantpeople in the environment (teacher,parents, other adults) where they willencounter naturally occurringprompts and reinforcers (McConnell,1987). It is important to teach skillsthat are valued not only by theindividual student but also by othersin his or her environment.
The social skills currently targetedfor instruction may not be thosewhich are socially valid for students.Current social skills programs havefocused on those skills which adults,not students themselves, have judgedimportant (Kazdin & Matson, 1981;LeCroy, 1983). As a result, sociallyincompetent students may notincrease their levels of socialacceptance even if specific skills aremastered.
Kazdin and Matson (1981) havesuggested subjective evaluation asone method for establishing thevalidity of training targets. Thisinvolves obtaining feedback fromsignificant others to establish socialsignificance of target behaviors. If thesocial skill acquired is not valued byothers in the learner's environment,

social competence in those settingswill not be increased. The identifica-tion of functional social skillsskillswhich will increase a child's compe-tence in the classroom, with peers,with teachers, and with otheradultsis urgently needed.
The purpose of this study was to takea closer look at the social skillswhich have been targeted for inter-vention and to determine if theparticular needs of seriously behav-iorally disordered students have beenaddressed. Extending the work ofWilliams, Walker, Holmes, Todis, andFabre (1989) to validate the socialskills included in the ACCESSprogram for instructing social skills,this study identified the sets of socialskills valued by teachers, parents,peers, and the seriously behaviorallydisordered students in various schoolenvironments. The following researchquestions were posed:
1. Which skills identified by theSurvey of Adolescent Social Skills(Williams et al., 1989) were ratedas important by regular educationteachers, teachers of students withbehavioral disorders, regulareducation students, students withbehavioral disorders, regulareducation parents, and parents ofstudents with behavioral disor-ders?
2. Were there differences in the rankordering of these skills in terms oftheir importance to each group?
3. What were the specific differencesamong the groups with regard tohow they rated the specific socialskill?
METHOD
Subjects
Special education directors fromschool districts in Washington, Iowa,and Colorado solicited volunteersfrom among the upper elementary andjunior high (grades 4-9) teachers of
the seriously behaviorally disorderedin their districts. Subjects wererecruited from urban, suburban, andrural schools but were not randomlyselected and thus do not constitute anonvolunteer sample. Generalizationsregarding the results of this study arelimited to teachers who may choose tovolunteer for such tasks. The specialeducation teachers who agreed toparticipate were asked to nominate aregular education teacher. Theparticipating teachers then eachnominated a student, contacted theparents of their students for consent,and distributed the surveys to parentsand those students for whom they hadreceived consent. Students whoparticipated were from upperelementary and junior high schoolgrades (grades 4-9).
The subject pool was comprised of atotal of 383 subjects and included thefollowing six groups: 70 regulareducation students (RES), 69students with behavioral disorders(SES), 80 teachers of students withbehavioral disorders (SET), 76regular education teachers (RET), 54parents of regular education students(REP), and 33 parents of studentswith behavioral disorders (SEP).Students identified as having seriousbehavioral disorders were so classi-fied according to their individualstates' regulations and criteria.Because state regulations and criteriavary across states, generalizationsregarding the special educationstudent data may be limited.
Instrumentation
The Adolescent Social Skills Survey(Walker et al., 1988) containing 48items was used to collect the data. A5-point Likert scale was provided forthe subjects' use in rating theimportance of each skill. The skillslisted in the survey were designed toprovide information regarding threebehavioral domains considered to beimportant to adolescent adjustment.
The identification of functionalsocial skillsskills which willincrease a child's competence
in the classroom, with peers,with teachers, and with otheradultsis urgently needed.
Nowsomemmiummimmis
CCBD Retrospective Series / 15

Three behavioral domains
considered important toadolescent adjustmentare relating to others, adults,and self.
11111111110111111111111
16 / CCBD Retrospective Series
1 . Relating to othersThis domaininvolves skills which are neededto relate to peers, coworkers, and/or other students and to developfriendships and social supportnetworks.
2. Relating to adultsThis domainincludes skills needed to relate toteachers, employers, and/orparents and to behave in wayswhich meet adult expectations forcompliance and performance.
3. Relating to selfThis domainexamines those skills which allowthe individual to independentlyand effectively manage his or herlife.
There were 23 skills included insection 1 (relating to others), 9 skillsin section 2 (relating to adults), and16 skills in section 3 (relating tosell). The items under each sectionwere randomly distributed to controlfor item presentation or sequenceeffects. Three versions of the surveywere generated in this manner andrandomly distributed to subjects.Blank spaces were provided at theend of each section for respondents toinclude any additional skills they feltto be important.
Test-retest reliability had beenpreviously reported (Timo, 1988) andranged from .92 to .56 for all but onesection. The test-retest reliability waslow (.21) for special educationteachers in the relating-to-otherssection. Williams et al. (1989)reported estimates of internalconsistency (split-half reliability) forstudents and teachers at .96.
Procedures
Teachers, students, and parents fromWashington, Colorado, and Iowa wereasked to complete the survey ofadolescent social skills developed byWalker and his colleagues at theUniversity of Oregon. There werethree versions of the survey, allcontaining identical items but
arranged in differing order. Versions1, 2, and 3 were randomly distributedto subjects. All students were giventhe survey after verbal instructionsand asked to return them to theirteachers. Any student who neededassistance in reading or interpretingan item was given the necessary help.The surveys were distributed andcollected over two school years,1987-1988 and 1988-1989.
In order to assess the importance ofthe skills in this survey (ResearchQuestion 1), mean scores werecalculated for each group on eachitem (see Table 1). Spearman rankorder correlations were calculated inorder to assess the rank orderagreement within the three adjust-ment domains sampled by the survey(Research Question 2). Correlationswere computed using the mean scoresand item rankings by section.Spearman rank order correlationswere chosen because the data wereordinal and Spearman rank ordercorrelations provided the mostconservative representation of thedata. In an effort to determine thespecific differences among the groupsregarding their opinions on specificsocial skills (Research Question 3),chi-square analyses were computed.Chi-square analyses were chosenbecause the data were ordinal (and assuch did not fulfill the basic assump-tions of analysis of variance). Inaddition, chi-square analyses allowfor an examination of differencesamong sets of groups.
RESULTS
Question I: Are the social skills on thissurvey perceived as important byteachers, students, and parents?
As 4 was defined as Important and 5as Very Important, items with meanscores of 4.0 or above were deter-mined to be perceived by the groupsas important. Overall, teachers,students, and parents viewed the
skills on this survey as importantsocial skills. Both parent groups(REP and SEP) as well as the regulareducation teachers and students(RET and RES) rated at least 43 ofthe 48 skills (90%) as important(having a mean above 4.0) to adoles-cent social success.
Table 1 lists the frequency of items atvarious ranges of means by section.In section 1 (getting along withothers) the majority of items receiveda score of 4.0 or higher from all sixgroups. However, the percentage wasslightly lower for the special educa-tion students and teachers (SES andSET), each of whom rated 18 out of23 (78%) items as important.
In section 2 (getting along withadults), the same basic patternpersists. Five of the six groups (RES,RER SEP, RET, SET) rated all butone skill as important. All five groupsindicated that the same skillbeingof assistance to the teacher was theonly skill included on the list thatwas not critical. Students withbehavioral disorders (SES) indicatedthat three of the nine skills were notcritical to getting along with adults.
In section 3 (getting along withyourself) all of the skills were rated at4.0 or above by all of the groupsexcept special education teachers(SET) who rated 14 out of the 16skills (87%) as important.
Question 2: Were there differences inthe rank ordering of these skills interms of their importance to eachgroup?
Results are summarized in Table 2.Correlation coefficients indicated amoderate (p <.05) or high (p < .01)agreement between the parents andteachers of both special and regulareducation students (REP/RET, SEP/SET). The agreement level betweenthe two student groups (I1ES andSES) was moderate or high (section 1= .76, section 2 .78, section 3 =
.62). Scores from students withbehavioral disorders (SES) had onlymoderate agreement with the adultgroups (SES/RET, SES/SEP; SES/SET). Correlations for regulareducation students (RES) with theadult groups were somewhat higher.
Question 3: Taal are the specificdifferences among the groups regard-ing their opinions on specific socialskills?
Section 1. Results of the chi-squareanalyses are summarized in Table 3.The special education students (SES)differed from the special educationteachers (SET) on three items: BeResponsible, Express Anger theRight Way, and Handle Aggression.In each case, the teachers rated theskills higher. Special educationstudents differed from regulareducation teachers (RET) on sevenitems. In each case, teachers indi-cated that the skills were moreimportant. The only item in section 1on which a significant differenceoccurred between the two studentgroups (RES, SES) was Be Consider-ate. Regular education studentsplaced a higher value on this skill.
Section 2. Significant differences inthe rating of the item Be of Assis-tance to the Teacher were observed insix of the ten group analyses. Bothstudent groups and the parents ofstudents with behavioral disordersindicated that Being of Assistance tothe Teacher was more important thandid either teacher group or theregular education parent group. Theregular education teachers differedfrom both student groups in placing ahigher value on the development ofindependent study skills. Specialeducation students differed from bothregular and special educationteachers in placing a lesser value onFollowing Classroom Rules. Studentswith behavioral disorders also placeda lesser value on Disagreeing withAdults in an Acceptable Manner thandid their parents, teachers, their
Regular education teachers
place a high value on the
development of independent
study skills.
IN11111111111111111M11111111M=11111111111111
CCBD Retrospective Series / 17

The participants in this studyviewed a majority of the socialskills surveyed as important.
immommilmomisamommi
18 / CCBD Retrospective Series
TABLE 1
List of Means Above 4.0
SES RES SET RET SEP REP
Section 1Relating to others (23 items)
4.5 - 5.0 2 4 6 11 5
4.25 - 4.49 2 10 7 9 7 7
4.0 - 4.24 15 10 7 6 4 7
Less than 4.0 5 1 5 2 1 4
Section 2Relating to adults (9 items)
4.5 - 5.0 0 1 0 2 4 2
4.25 - 4.49 0 3 6 5 4 3
4.0 - 4.24 6 4 2 1 0 3
Less than 4.0 3 1 1 1 1 1
Section 3Relating to self (16 items)
4.5 - 5.0 0 4 6 8 7 6
4.25 - 4.49 4 7 6 6 8 5
4.0 - 4.24 12 5 2 2 1 5
Less than 4.0 0 0 2 0 0 0
regular education peers, and regulareducation teachers.
Section 3. In this section, studentswith behavioral disorders differedfrom both teacher groups on anumber of items. They (SES) differedfrom special education teachers onthe following skills: Be Honest,Accept Consequences, and LookGood. They (SES) differed fromregular education teachers on thosethree items and also on HaveStandards for Own Behavior, Do WhatYou Say You'll Do, and Self-Control.The special education studentsplaced a greater emphasis on LookGood and Feel Good About Self. Theteachers (SET, RET) placed greateremphasis on Have Standards for OwnBehavior, Be Honest, Accept Conse-quences, Do What You Say You'll Do,
and Self-Control. Special educationstudents differed from their parentsin that they placed a lower value onAccepting Consequences, BeingHonest, and Having Standards forOwn Behavior. The irm Look Goodwas consistently more important tostudents than to adults.
DISCUSSION
This study was designed to examinethe opinions of students, teachers,and parents regarding adolescentsocial skills and to understand what,if any, differences existed among thegroups. Overall, the participants inthis study viewed a majority of theskills surveyed as important, support-ing the conclusions made by Will-iams et al. (1989). There were,however, some differences between

TABLE 2
Spearman Rank Correlations
Groups REP REP RES RES RES RET RET SEP SET SEP
RES RET RET SES SET SES SET SES SES SET
Relating to others .52 .91 .48 .76 .39 .40 .90 .35 .33 .62
Section 1 ** ** * ** * ** **
Relating to adults .77 .77 .47 .78 .48 .36 .67 .32 .23 .73
Section 2
Relating to self .65 .88 .58 .62 .60 .29 .82 .36 .17 .71
Section 3 ** ** * ** ** **
*p < .05 **p < .01
groups which merit discussion,especially with regard to program-ming for seriously behaviorallydisordered students.
Students with behavioral disordersdid not feel that skills such as Beingof Assistance to the Teacher, AvoidingConfrontations and Problems withAdults, and Disagreeing with Adultsin an Acceptable Way were as criticalas other skills. This is a directcontradiction of the high value thatregular and special educationteachers have placed on behaviorsthat demonstrate compliance andcooperation, both in this study and inothers reported in the literature(Cartledge et al., 1985; Kerr &Zigmond, 1986).
Regular education students ratedadult-oriented skills such as BeingConsiderate more highly than didspecial education students. Thisdifference may be the result of actualdifferences between the values of thetwo student groups. It is quitepossible that the regular educationstudents, those in the mainstream,
have become proficient at fulfillingthe expectations of the school system.Cairns (1986) suggests that peopletend to perform their habitualresponses in reoccurring situations.In this way, social systems arereinforced and maintained. Studentswith behavioral disorders may notfeel such a part of the adult-orientedschool system. As a result, they mightbe less interested in performing thoseskills valued by adults.
It is important to note that studentswith behavior problems may findthemselves in trouble with adults forlacking the very skills that theyindicated are not a priority to them. Itseems quite significant that thisgroup, alone out of the six, placed alower value on getting along withadults. Why did the students withbehavioral disorders indicate they didnot place as high a value on theseskills as did the other five groups?Gresham (1986) providt's a conceptu-alization of social competency whichmay shed some light on this issue. Hemakes a distinction between skilldeficits and performance deficits.
Students with behavioraldisorders may not feel a part
of the adult-oriented school
system.
IIIIIM11=11111111N111111111111111111111111M11
CCBD Retrospective Series / 19

20 / CCBD Retrospective Seriesnowimimis
TABLE 3
Chi Square Analyses
Group Item x 2 Level of Rated
Significance Higher
Section 1-Relating to othersRES/RET Be responsible 20.96 .00001 RET
Aggression 13.30 .0013 RETRES/SES Be considerate 14.35 .0008 RESRES/SET Be responsible 13.35 .0013 SET
Aggression 19.18 .0001 SETRET/SES Be considerate 15.88 .0004 RET
Be responsible 30.97 .00001 RETPressure 29.87 .00001 RETAggression 21.85 .00001 RETRejection 17.90 .0001 RETAsk for assistance 16.66 .0002 RETListen 13.48 .0012 RET
SEP/SES Permission 14.56 .0007 SEPResponsible 14.40 .0007 SEPPressure 20.06 .00001 SEPAggression 15.15 .0005 SEP
SET/SES Responsible 23.81 .00001 SETExpress 13.99 .0009 SETAggression 27.54 .00001 SET
Section 2-Relating to adultsRES/RET Assist teacher 17.17 .0002 RES
Develop independent
study skills 14.18 .0008 RETRES/SET Assist teacher 24.49 .00001 RESRET/SES Assist teacher 29.47 .00001 SES
Develop independent
study skills 19.99 .00001 RETDisagree 16.96 .0002 RETFollow classroom rules 17.81 .0001 RET
Avoid confrontations 17.22 .0002 RETSEP/SES Develop independent
study skills 12.48 .0019 SEPSET/SES Assist teacher 29.16 .00001 SES
Disagree 22.48 .00001 SETFollow classroom rules 13.92 .0009 SET
SEP/SET Assist teacher 24.31 .00001 SEP
t )
Continued on next page.

TABLE 3, ContinuedNam.
Group Item x 2 Level of Rated
Significance Higher
Section 3-Relating to self
REP/RES Look good 15.50 .0004 RES
RES/RET Set goals 16.92 .0002 RET
Look good 25.15 .00001 RES
RES/SET Set goals 13.48 .0012 SET
Look good 21.48 .00001 RES
RET/SES Be honest 24.50 .00001 RET
Have standards 15.87 .0004 RET
Accept consequence 35.97 .00001 RET
Look good 27.53 .00001 SES
Do what you say 16.02 .0003 RET
Have self-control 16.57 .0003 RET
SEP/SES Be honest 18.26 .0001 SEP
Accept consequence 14.25 .0008 SEP
SET/SES Be honest 14.39 .0008 SET
Accept consequence 31.10 .00001 SET
Look good 24.07 .00001 SES
The basis of the distinction rests onwhether or not the student knows howto perform the skill in question.Gresham (1986) posits that a lack ofmotivation may be one underlyingcause for social skill performancedeficits. If this is true, students maynot be motivated to perform theseskills because the rewards are notgreat enough or because the skills donot meet their needs.
The issue of social significanceshould play a major part in the designand implementation of behavioralinterventions. The social significanceof a particular skill is usually basedon the subjective judgments ofrelevant others in the students'environment (Gresham, 1986;Kazdin, 1977). Responses fromteachers in this study have indicatedthat certain skills are necessary forsuccess, at least in the academicenvironment. It becomes imperative,
then, to understand why students withbehavioral disorders do not value andperform these skills. The answer tosuch fundamental questions mightdetermine how one approaches theseskills in a training program. Onecaution, however, must be raised.Since the reported reliability ofspecial education teachers was low,further investigations regarding theirperceptions should be conducted.
As expected, both teacher groupsplaced the greatest importance onthose skills that would aid in thesmooth running of the classroom.Both teacher groups focused oncompliance skills such as acceptingconsequences and following direc-tions as major requirements for theirstudents. Independent study skillsand following classroom rules withoutundue supervision were also valuedby both teacher groups. Theseresponses are consistent with other
The issue of social significanceshould play a major part in the
design and implementation ofbehavioral interventions.
11111=1111111111111111MIMIII=111111111
CCBD Retrospective Seiies / 21

It could be very important for
teachers of students withbehavioral disorders toencourage their students tostart to develop standards fortheir behavior that reflect thoseof general education students.
111=111111111111111111111111111111111111111
22 / CCBD Retrospective SeriesooimmEmomimm
research which has indicated thatteachers place the highest value onadaptive behaviors that ensure asmooth running classroom (Calkins etal., 1984; Cartledge et al., 1985;Walker, 1984; Walker & Rankin,1983).
There were, however, differencesbetween the two groups of teachers.For example, special educationteachers placed greater emphasis onExpressing Anger the Right Way andon Disagreeing with Adults in anAcceptable Way than did regulareducation teachers. This differencemay reflect the different populationsthat they serve.
Regular education teachers also felt itwas important for students to havestandards for their own behavior. Itcould be very important for teachersof students with behavioral disordersto encourage their students to start todevelop standards for their behaviorthat reflect those of general educationstudents. It also seems imperativethat they develop a set of independentbehaviors that will enable them toplan their activities and monitor theirprogress and behavior. The work ofLloyd and his colleagues (1989) inthe area of self-management offersseveral suggestions for planners ofsocial skills programs.
Another interesting finding of thisstudy is the lack of concordance ofthe values expressed by the childrenwith behavioral disorders and allother groups. With a data set that isso similar across groups, the lack ofcorrelation between the findings forthis group and the others is notewor-thy. A review of Table 2 shows that amajority of their ratings are discor-dant with the other groups studied.This is especially true in section 2,relating to adults. A functionalapproach to analyzing behaviorsuggests that chains of behaviorproduce an effect (Neel, 1984). Thesuccess or failure does not depend on
2
its acceptance by others, but itsability to produce a desired result.Using this framework, social skillsare viewed as a set of (or series of)behaviors required to achieve a socialgoal in a particular situation (Neel,Meadows, & Scott, 1990). If we wereto assume a functional approach toanalyzing social skills, it would seemthat a major component in thetraining of social skills would have tobe teaching children with behavioraldisorders to value interacting withadults. This may require a restructur-ing of the methods for deliveringservices that we now use (Neel &Cessna, 1990; Neel, Cessna, Swize,& Borock, 1988).
If one of the major goals of a socialskills training program is to preparestudents for reentry into the generaleducation classroom, then it seemscritical to examine the priorities ofthe teachers of those classrooms, whohave shown themselves to be highlyoppositional to the behavior of manymainstreamed children (Sarason &Doris, 1978). The perception ofgeneral education teachers is animportant one. When teachers designprograms to teach children withbehavioral disorders those skillsrequired to integrate effectively intogeneral education environments, theyshould be aware of the skills whichare highly valued by regular educa-tion teachers and students.
It is also not surprising that studentsprefer immediate social goals to thosewith more long-term indirect payoffs.In fact, the degree to which studentsand teachers agree might be consid-ered a measure of socializationtoward adult values. Again asexpected, the ratings of generaleducation students on social skillitems correspond more closely to theadults than did the ratings ofchildren with behavioral disorders.These findings, though not unexpect-ed, do accent the need for inclusionof training of skills required by youth

to become successful with their peersand adults.
The data in this study, however, alsoshow that there is another set of skillsthat are critical to the social successof children with behavioral disorders:those that effect short-term peeradjustment. In fact, these latter skillshave a greater value for students thanthose most valued by their teachers orparents. The need to develop effectivetraining programs to address theseskills can no longer be ignored. Ifschool programs are going to be ableto meet the needs of all their students,they will have to realign theirpriorities to include peer focusedsocial skills training (Neel, Cessna etal., 1988).
CONCLUSION
The results of this study indicate thatparents, students, and teachersviewed the 4.8 skills on this survey asimportant. However, it must beremembered that the participants inthis study were subjected to a forcedchoice condition. They were provideda prechosen list of skills and asked torate their importance. This limits thedegree to which the data may begeneralized. While it is true that thisstudy and others like it (Timo, 1988;Williams et al., 1989) have shownthese skills to be important, theyhave not proven them to be critical.Subjects in this study were onlyasked to react to a fixed set of skills.Having groups of people generatetheir own lists of skills may producedifferent skills. Further researchneeds to be done that will determinewhich of these skills are critical tosuccessful integration.
Despite the possibly limiting effectsmentioned above, understanding thedifferences among the groups in thisstudy will begin to increase under-standing of why social skills trainingprograms do not work as well asexpected. If it is true that many of the
social skills included in trainingprograms were chosen on the basis offace validity (Kazdin & Matson,1981), then this kind of empiricaltesting is one way to understandwhich skills will be valued andreinforced. Skills that are notconsidered valuable by students, andthose who work and live with them,have less chance of becoming afunctional part of the student'sbehavior (McConnell, 1987).
Because the goal of many social skillstraining programs is to have thestudents return to the mainstreamclassroom, the differences betweenregular education teachers andspecial education students should beconsidered carefully. More significantdifferences occurred between thesetwo groups than any other possiblecombinition. In order for students,especially students with behavioraldisorders, to benefit from social skillstraining programs, the skills theylearn must be important to them andto the many other people with whomthey interact. Students and adultsneed to be aware of their own and eachother's values. This study is just abeginning in the effort to understandwhich skills are critical and why.
Future research needs to be directedtowards developing a functionallyvalid list of critical social skills. Itseems quite possible that if this manydifferences exist under a forcedchoice condition, even more differ-ences in values and priorities mightbe revealed under different experi-mental conditions. It is essential thatfuture training programs includeskills that will make functionaldifferences in students' behavior andin the judgments of those who comein contact with them.
REFERENCES
Asher, S. R., & Hymel, S. (1981).Children's social competence in peerrelations: Sociometric and behavioral
rt "
BEST COPY AVAILABLE
Future research needs to be
directed toward developing afunctionally valid list of critical
social skills.
111111111111111=111MMIN11111111111111
CCBD Retrospective Series / 23alimmiemomommom

assessment. In J. D. Wine & M. D.Syme (Eds.), Social competence (pp.125-157). New York: Guilford Press.
Asher, S. R., & Taylor, A. R. (1983).Social skill training with children:Evaluating processes and outcomes.Studies in Educational Evaluation, 8,237-245.
Bel lack, A. S. (1983). Recurrentproblems in the behavioral assess-ment of social skill. BehavioralResearch Therapy, 21(1), 29-41.
Bruininks, V. L (1978). Actual andperceived peer status of learningdisabled students in mainstreamprograms. Journal of Special Educa-tion, 12, 51-58.
Cairns, R. B. (1986). A contemporaryperspective on social development. InP S. Strain, M. J. Curalnick, & H. M.Walker (Eds.), Children's socialbehavior: Development assessmeru andmodVication (pp. 3-47). Orlando, FL:Academic Press.
Calkins, C. F., Walker, H. M., Bacon-Prue, A., Gibson, B. A., Martinson,M., Offner, R., & Intagliata, J. (1984).The learning and adjustment process.Kansas City: University of Missouri,Institute for Human Development.
Cartledge, G., Frew, T, & Zaharias, J.(1985). Social skill needs of main-streamed students: Peer and teacherperceptions. Learning DisabilitiesQuarterly, 8, 132-139.
Combs, M. L., & Slaby, D. A. (1977).Social skills training with children. InB. B. Lahey & A. E. Kazdin (Eds.),Advances in child clinical psychology(Vol 1, pp. 39-60). New York: Plenum.
Gottman, J., Congo, J., & Schuler, P(1976). Teaching social skills toisolated children. Journal of AbnormalPsychology, 4, 179-197.
Gresham, F M. (19C1). Social skillstraining with handicapped children: Areview. Review of EducationalResearch, 51 (1),139- 176.
Gresham, F M. (1982). Misguidedmainstreaming: The case for socialskills training with handicappedchildren. Exceptional Children, 49,49-54.
Gresham, F. M. (1986). Conceptualism...8 in the assessment of socialcompetence in children. In PS. Strain,M. J. Guralnick, & H. M. Walker(Eds.), Children's so( rl behav;,or:Development, assessment, and
24 / CCBD Re'aospective Series
modification (pp. 143-179). Orlando,FL: Academic Press.
Gronlund, H., & Anderson, L. (1962).Personality characteristics of sociallyaccepted, socially neglected, andsocially rejected junior high schoolpupils. In J. Sedeman (Ed.), Educat-ing for mental health (pp. 162-173).New York: Cromwell.
Kauffman, J. M. (1989). Characteristics ofbehavior disorders of children andyouth (4th ed.).Columbus, OH:Merrill.
Kazdin, A. E. (1 977). Assessing theclinical or applied importance ofbehavior change through socialvalidation. Behavior Modification, I,427-452.
Kazdin, A. E., & Matson, J. L. (1981).Social validation in mental retarda-tion. Applied Research in MentalRetardation, 2, 39-53.
Kerr, M., & Zigmond, N. (1986). What dohigh school teachers want? A study ofexpectations and standards. Educa-tion and Reatment of Children, 9,239-249.
Knold, J. A. (Ed.). (1985). Employeetraining needs as expressed byemployers in Washington state.Olympia: Washington State Commis-sion for Vocational Education.
LeCroy, C. W. (1983). Social skillstraining with adolescents: A review.Child and Youth Services, 5, 91-116.
Lloyd, J. W., Landrum, T J., & Hallahan,D. P (1989). Self-monitoringapplications for classroom intervention(Virginia Behavior Disorders Project,Research Report No. 8). Charlottes-ville: University of Virginia.
McConnell, S. R. (1987). Entrapmenteffects and the generalization andmaintenance of social skills trainingfor elementary school students withbehavioral disordem. BehavioralDisorders, 12, 252-263.
Michelson, L., & Wood, R. (1980).Behavioral assessment and training ofchildren's social skills. Progress inBehavior Modification, 9, 241-291.
Morgan, S. R. (1977). A descriptiveanalysis of maladjusted behavior insocially rejected children. BehavioralDisorders, 3, 23-30.
Ned, R. S. (1984). Teaching socialroutines to behaviorally disorderedyouth. In C. R. Smith & E. McGinnis(Eds.), Educational instruments in

behavioral disorders (pp. 73-88). DesMoines: Iowa State Department ofEducation.
Neel, R. S., & Cessna, K. K. (1990). Do
these behaviors make sense? Menu-
script submitted for publication.Neel, R. S., Cessna, K., Swize, M., &
Borock, J. (1988). Position paper onserving S.LE.B.D. students. Unpub-lished manuscript, Colorado StateDepartment of Education, Denver.
Neel, R. S., Meadows, N. B., Levine, P,& Edgar, E. B. (1988). What happensafter special education: A statewidefollow-up study of secondary studentswho have behavioral disorders.Behavioral Disorders, 13, 209-216.
Neel, R. S., Meadows, N. B., & Scott, C.M. (1990). Determining social tasks: Apreliminary report. Manuscriptsubmitted for publication.
Roff, M. (1970). Childhood socialinteractions and young adult badconduct. Journal of Abnormal andSocial Psychology, 63, 333-337.
Roff, M., Sells, B., & Golden, M. (1972).Social adjustment and personalitydevelopment in children. Minneapolis:University of Minnesota Press.
Sabornie, E. J. (1985). Social main-streaming of handicapped students:Facing an unpleasant rea/ity.Remedial and Special Education,6(2),12-16.
Sarason, S., & Doris, J. (1978). Main-streaming: Dilemmas, opposition,oppori unities. In M. Reynolds (Ed.),Futures of education for exceptionalchildren: Emerging structures (pp. 3-39). Reston, VA: The Council forExceptional Children.
Schloss, P J., Schloss, C. N., Wood, C. E.,& Kiehl, W. S. (1986). A criticalreview of social skills research withbehaviorally disordered students.Behavioral Disorders, 12,1-14.
Sheperd, G. (1980). The treatment ofsocial difficulties in special environ-ments. In P Feldman & J. Orford(Eds.), Psychological problems: Thesocial context (pp. 312-359). NewYork: John Wiley & Sons.
Stengel, E. (r971). Suicide and attemptedsuicide. Middlesex, NJ: Penguin.
Timo, K. S. (1988). Adolescent socialskills validation by teachers andstudents. Unpublished master's thesis,University of Washington, Seattle.
Ullman, C. A. (1957). Teacher, peers, andtests as predictors of adjustment.Journal of Educational Psychology,48, 257-267.
Walker, H. M. (1984). The socialbehavior survival program (SBS): Asystematic approach to the integrationof handicapped children into lessrestrictive settings. Education andTreatment of Children, 6, 421-441.
Walker, H. M., & Rankin, R. (1983).Assessing the behavioral expectationsand demands of less restrictivesettings. School Psychology Review,12, 274-284.
Walker, H. M., Todis, B., Holmes, D., &Horton, G. (1988). The Walker socialskills curriculum. Austin, TX: Pro-Ed.
Williams, S. L., Walker, H. M., Holmes,D., Todis, B., & &bre, T. R. (1989).Social validation of adolescent socialskills by teacher and students.Remedial and Special Education,10(4), 18-27.
CCBD Retrospective ',eries / 25

Social Interaction Researchand Families of BehaviorallyDisordered Children:A Critical Review and Forward Look
James FoxSarah Save Ile
ABSTRACT: This article critically reviews research on the social interactionsof behaviorally disordered children with family members. Behaviorally disor-dered children are in part characterized by their difficulty in establishing ormaintaining positive social relationships. This includes conduct disordered,socially withdrawn, and autistic children. Most applied research on socialdevelopment has been conducted in educational settings. Yet, parents and sib-lings are typically acknowledged as the earliest and one of the most enduringinfluences on children's social development. Descriptive and intervention re-search that includes direct observational measures of social interaction be-tween behaviorally disordered children, their siblings, or parents are reviewed.Two principal questions are addressed: (a) to what degree have these researchstudies shown that behaviorally disordered children exhibit deficits in positiveinteraction with family members when compared to nonhandicapped childrenand their families; and (b) what interventions have been shown to be effectivein increasing positive interaction between behaviorally disordered children andtheir families? Issues and questions for future research in this area are dis-cussed.
Difficulty in establishing and maintaining social relationships is one ofthe defining characteristics of behaviorally disordered child:en and youth(Bower & Lambert, 1961; Kauffman, 1985). Such problems in socialdevelopment include conduct disorders in which the child typicallyengages in negative interactions with other children and adults, and socialwithdrawal in which the child either fails to engage in or actively avoidsinteraction with others (Michaelson & Mannario, 1986).
Over the past 50 years applied researchers have sought to (a) describemore precisely the nature, course, and implications of disorders in socialbehavior; and (b) develop and empirically evaluate intervention proce-dures with which to teach more adaptive social skills and increase positiveinteraction. In many respects our understanding of these problems and ourintervention technology have improved substantially (Hops, 1982; Strain,1983; Strain & Fox, 1981; Strain, Guralnick, & Walker, 1986; Van Has-selt, Hersen, Whitehill, & Bellack, 1979).
Reprinted from Behavioral
Disorders, Vol. 12, Number 4,
August 1987, pp. 276-291isommiu
CCBD Retrospective Series / 27wiemmummomm

The bulk of social interactionresearch has focused on peerrelations in educationalsettings.
28 / CCBD Retrospective Seriesimemoolommisimmem
However, the bulk of social interac-tion research has focused on peerrelations in educational settings (Day,Fox, Shores, Lindeman, & Stow-itschek, 1983; Foster & Ritchey,1979; Fox, Day, & McEvoy, in press;Powell, Sahberg, Rule, Levy, &Itzkowitz, 1983). With the exceptionof conduct disordered children (e.g.,Patterson, 1982), rarely have investi-gators subjected parent and siblinginteractions to direct analysis orevaluated their relationship to thedevelopment of peer-related socialskills and interaction. This seems aparticularly glaring omission for tworeasons. Parents and siblings havebeen conceptualized as the earliestand potentially one of the mostenduring socialization influences(Hartup, 1970, 1983; Maccoby &Martin, 1983). Secondly, naturalisticresearch with normally developingchildren indicates that nuclear familymembers can and do play an activerole in the shaping of a child's socialrepertoire (e.g., Abramovitch, Corter,Pep ler, & Stanhope, 1986; Dunn &Kendrick, 1982; Lamb, 1978); thefew existing studies with handi-capped children suggest a similarrole for those families (James & Egel,1986; Powell et al., 1983).
Our purpose in writing this article istwofold: (a) to critically review socialinteraction research with behaviorallydisordered children, their siblings,and parents; and (11) to suggest areasfor future research. In particular thisreview will address research inregard to two questions:
1. Do behaviorally disorderedchildren exhibit deficits in socialinteraction with parents and/orsiblings when contrasted withfamilies of nonhandicappedchildren?
2. How can positive interactionbetween behaviorally disorderedchildren and family members beincreased?
By social interaction we refer tobehaviors directed by one person toanother, the purpose or function ofwhich is to initiate and maintain theexchange of behaviors between thetwo interactants. We will not empha-size studies of social exchangesbetween a child and other familymembers which are primarilymanagerial (commands, compliance,etc.) or tutorialthose in which onefamily member attempts to teach theother certain academic, cognitive, orself-help skills. This is not to denythe importance of such behavioralexchanges or their possible relevanceto social interaction between behav-iorally disordered children and theirfamilies. Rather, it is primarily apractical distinction. Such studieshave not typically addressed socialinteraction as we have defined ithere. In addition, reviews of the useof behavior management procedures byparents with their emotionally dis-turbed children are available elsewhere(e.g., Gordon & Davidson, 1981).
Descriptive Analysis ofFamily InteractionHome-based, observational analysesof normally developing children'sinteractions with family membershave increased considerably in recentyears (e.g., Abramovitch et al., 1986;Brody, Stoneman, & MacKinnon,1982; Dunn & Kendrick, 1982;Lamb, 1978; Stoneman, Brody, &MacKinnon, 1984). Analyses of thefamily interactions of behaviorallydisordered children under naturalis-tic conditions have a somewhat moresporadic history.
Behavior problemIconduct disorderedchildren. Outcomes of family-basedobservational studies have beenvirtually unanimous in distinguishingconduct disordered and nonreferredchildren in terms of their inappropri-ate behaviors and have also found
""'IT COPY AVAILABLE

that their parents and siblings arecharacterized by greater levels ofnegative social behaviors than infamilies of nonreferred children(Arnold, Levine, & Patterson, 1975;Horne, 1980, as cited in Patterson,1982; Patterson, 1976, 1982; Snyder,1977; Tap lin & Reid, 1977). Howev-er, differences in positive interactionsbetween family members have beenless clearly established.
Two studies have reported differencesin positive social behaviors betweenconduct disordered and nonreferredchildren. Bernal and her colleagues(Bernal, Delfini, North, & Kreutzer,1976; De lfini, Bernal, & Rosen,1976) observed two groups of youngboysa discipline problem groupreferred for fighting, disobeying,arguing, and so forth, and a normal(nonreferred) group from regularkindergarten and first grade classes.Four 30-min observations wereconducted for each child. The homedata indicated that problem boysexhibited significantly more annoyingand deviant behavior and significant-ly fewer desirable (e.g., on-task,appropriate verbal and nonverbalinteraction) and compliant behaviorsthan nonproblem boys. However, theabsolute difference in rate of desir-able behavior was rather small, themost pronounced differences betweenthe two groups being in terms ofannoying and deviant behaviors.Also, it was not clear from the dataanalyses to whom, parent or sibling,these desirable social behaviors weredirected nor were specific responsesto these behaviors reported.
Later, Mash and Mercer (1979)compared deviant (clinically re-ferred) and nondeviant (nonreferred)boys under two conditions--playingalone and with their brothersin alaboratory playroom. Deviance wasdefined in terms of clinical referralstatus (aggression, noncompliance,and disturbed peer relations) andscores on the Walker Problem
Behavior Identification Checklist.Normal subjects were volunteers fromlocal community groups and schools.During the sibling condition, normalsubjects and their siblings engaged insignificantly more cooperative playwhereas deviant subjects engaged inmore negative verbal and physicalinteractions. Also, for normal siblingpairs both their interactive behaviorsappeared to be more reciprocal thanthose of deviant sibling pairs.However, the most frequent behaviorfor both groups during the siblingcondition was solitary play.
The findings from Patterson's (1976)study of clinically referred, aggres-sive boys and nonreferred boys standin contrast to those of the precedingstudies. In-home observations wereconducted using a multicategoryobservation system (Patterson, Ray,Shaw, & Cobb, 1969) designed toassess both positive and negativebehaviors. Although rates of eightdeviant behaviors (negative com-mands, disapproval, humiliate,ignore, noncomply, negativism, tease,and yell) were significantly higher foraggressive subjects, none of thecomparisons for prosocial behaviorrates were significantly different.However, these comparisons werebased on total rates and did notindicate to whom the person beingobserved directed these behaviors.
It does appear that the social ex-changes of conduct disorderedchildren and their family membersare less reciprocal. Analyses ofnaturally contingencies provided byfamily members of conduct disor-dered boys referred for treatmentwere reported by Tap lin and Reid(1977). Baseline data indicated thatparents were about as likely topositively consequate deviantbehavior as they were prosocialbehavior. Snyder (1977) examinedinteractional differences betweenproblem and nonproblem familieswith a male child between 5 and 10
Outcomes of family-based
.observational studies have
been virtually unanimous in
distinguishing conductdisordered and nonreferredchildren in terms of theirinappropriate behaviors and
have also found that theirparents and siblings arecharacterized by greater levels
of negative social behaviors
than in families of nonreferredchildren.
111111111111111111111111
CCBD Retrospective Series / 29NNNINNNN

Some studies have indicatedthat conduct disorderedchildren engage in fewerpositive social behaviors with
family members than donormal children while othershave not found any significantdifferences in the rate ofprosocial behaviors betweenconduct disordered andnonreferred children.
Ii11111111=1111111111M1M11111
30 / CCBD Retrospective Series
years old. Groups were defined by thechild's score on the Behavior ProblemChecklist and parents' reports ofmarital conflict on the Locke-WallaceMarital Adjustment Scale. Familieswere videotaped once for 45 minutesin a laboratory room arranged asliving room-play room combination.For data analyses, observationalcategories were reduced to one of twoclassespleasing and displeasingbehaviorusing families' averagedratings of each category. Responseswere reduced to one of three contin-genciespositive, negative, orneutral.
Although most behavior in both typesof families was pleasing, the rate ofdispleasing behavior in problemfamilies was approximately twice thatof nonproblem families. (Analyses ofdifferences in pleasing behavior rateswere not reported.) Further, problemfamily members provided significant-ly fewer positive and more neutral oraversive consequences for pleasingbehaviors; they also received feweraversive and more positive conse-quences for displeasing behavior.Finally, conditional probabilityanalyses indicated that problemfamily members were significantlyless likely than nonproblem familymembers to repeat pleasing behaviorsthat were followed by positiveconsequences and more likely tocontinue displeasing behaviorsfollowed by aversive consequences.
To summarize briefly, some studieshave indicated that conduct disor-dered children engage in fewerpositive social behaviors with familymembers than do normal children(De llfini et al., 1976; Mash &Mercer, 1979) while others have notfound any significant differences inthe rate of prosocial behaviors(Patterson. 1976) between conductdisordered and nonreferred children.The disparity in these findings mayresult from methodological differenc-es between the studies, including theselection criteria for conduct disor-
:3 o
dered subjects, differences inbehavior definitions, conditions ofobservation and observationalprocedures, and the units of analyses.For example, some investigators(Patterson, 1976, 1980; Tap lin &Reid, 1977) have selected conductdisordered subjects primarily on thebasis of their referral to a treatmentprogram due to problems characteriz-ing conduct disordered children(aggression, noncompliance, tan-trums, etc.) whereas other researchersused additional criteria such assubjects' scores on a standardizedbehavior checklist (Mass & Mercer,1979). Snyder (1977), in fact,selected problem families using acombination of child referral statusand behavior checklist scores, andparents' scores on a marital adjust-ment scale.
Then, too, some studies have usedinterval recording procedures (Bernalet al., 1976; Delfmi et al., 1976;Mash & Mercer, 1979) while otherstudies have used continuous,sequential recording (Patterson,1976, 1980; Snyder, 1977). Continu-ous sequential recording should bemore sensitive to differences in thefrequency/rate of behavior, yet studiesemploying less precise intervalrecording have reported differencesin conduct disordered and normalchildren's social interactions withfamily members. Studies have alsovaried in terms of the physicallocation and setting conditions (homebased vs. laboratory analog) in whichobservations have been conducted.Until these and other procedural/methodological variations betweenstudies are controlled or systematical-ly investigated, comparisons acrossstudies will remain tenuous.
Children exhibiting social withdraw-al. The term social withdrawal refersto a low rate or avoidance of socialinteraction (Strain & Fox, 1981).Used in this way, it refers to a generalbehavioral deficit that may beexhibited by a diverse array of

children, including those who areotherwise normally developing aswell as children with more pervasivehandicaps (e.g., autism, mentalretaniation). Hereafter, we will refer tothese otherwise normally-developingchildren as "withdrawn children."
In an earlier review of social with-drawal, Finch and Hops (1983)briefly described a study of 30 intactfamilies. Preliminary analyses weresaid to indicate that:
Parents of withdrawn childrenshowed somewhat reduced ratesof prosocial behavior comparedto parents of either the highaverage or highly sociablechildren. In addition, fathers ofthe low sociability childrenprovided more adverse and fewerprosocial consequences for childprosocial behavior than fathers ofthe other two groups.
To date, this is the only reference toan observational analysis comparingthe family interactions of withdrawnand nonwithdrawn children of whichwe are aware.
Social withdrawal has been one of thedefining characteristics of autismsince the disorder was first describedby Kanner (1943). Indeed, asSchopler and Mesibov (1986) havenoted, some consider social deficitsto be the basic problem of autism,and as De Myer (1979) noted in herinterview studies with parents, someof their most painful experiences anddifficult decisions center upon theautistic child's reactions to peopleand their social distance. Yet, home-based observational studies ofautistic children have been andcontinue to be extremely rare, thisdespite the fact that clinical andparent reports suggest some autisticindividuals make at least some socialadaptations and interact moreappropriately as they age (De Myer,1979; Kanner, 1971; Kanner,Rodriguez, & Ashenden, 1972).
Possibly the earliest home-basedobservation analysis of an autisticchild was reported by Lichstein andWahler (1976). A 5-year-old autisticboy was observed both at home withhis family (parents and nonhandi-capped older sister) and in twoclassroom settings. A total of 75 30-min observations were obtained in thehome and 42 in each school setting.The subject's behavior was scored interms of various social, nonsocial,and autistic behavior categories(Wahler, House, & Stambaugh,1976). Over the course of the studyboth social and nonsocial behaviorsvaried considerably. In the home, thesubject engaged in little interactionwith his sister, rarely initiatedinteractions with any family member,and on the average, interactedinfrequently with his parents(approximately 11% of the time). Themost frequent behaviors at home werenonsocial, autistic behaviors such asself-stimulation and noninteraction.Finally, the investigators also notedthat the boy rarely engaged in anysustained toy play either alone orwith others.
Martin and Graunke (1979) assessedthe home behavior of 15 autisticchildren and adolescems 5 to 13years old. Using Patterson, Ray,Shaw, and Cobb's (1969) observationsystem, subjects were observed for 45minutes on 5 different occasions-4weekdays and 1 weekend day.Individual helyv'ars were subsumedunder three general categoriesdeviant, nondeviant, and prosocial.As a group the autistic subjectsengaged in relatively iittle deviantbehavior (e.g., self-destructive, self-stimulation). Nondeviant behaviors(verbal neutral, physical contact,independent activity) were mostfrequent, accounting for approximate-ly 60% of the subjects' behavior.Prosocial behaviors (e.g., compliance,laugh, physical positive, play) wereintermediate in occurrence, account-ing for approximately 34% ofsubjects' behavior. However, consid-
Social withdrawal has been
one of the definingcharacteristics of autism.
CCBD Retrospective Series / 31

Compared to nondisabledchildren, children with mentalretardation appear deficientnot in the overall amount ofinteraction with familymembers but in certainaspects of interaction.
32 / CCBD Retrospective SerieswimsimmiwNomoo
erable intersubject variability wasnoted in all classes of behavior.Although all family members weremore likely to respond positively thannegatively to the autistic subjects,siblings were less likely to respondpositively to deviant behaviors thanwere parents.
Donne llan, Anderson, and Mesaros(1984) conducted observations of 7autistic boys ranging in age from 21/2to 11 years. Autistic child-familymember interactions were videotapedonce during each of three typicalhome activitiesmealtime, free time,and transition time (arriving homefrom school). These tapes were scoredusing a rating system designed toassess "family-member interactions,stereotypy, and environmentalvariables that might have influencedthem." However, length of theobservation sessions and the specificcodes were not described in thereport. Subject children interactedwith families during approximately56% of the intervals. Interactionswere more likely to occur duringintervals in which there was little orno stereotypy rather than duringlonger bouts of stereotypy. Stereotypicbehavior occurred 19% of the timeand was particularly prevalent duringunstructured activities.
Studies of the family interactions ofmentally retarded children have beenconducted somewhat more frequently.These studies suggest that we proceedwith conceptual and methodologicalcaution in attempting to descriptivelyanalyze family interactions. Studiesof both parent-child (Eheart, 1982;Stoneman, Brody, & Abbott, 1983;Terdal, Jackson, & Garner, 1976) andchild-sibling social interactions(Stoneman & Brody, in press;Stoneman, Brody, Davis, & Crapps,1986) indicate that the interactionaldifferences between mentallyretarded and normally developingchildren may not always be apparentas a deficit in the overall amount ofinteraction. Rather, differences
between handicapped and nonhandi-capped children's family interactionsappear to have more to do withparticular types of social encounters.
For example, compared with normallydeveloping children, mentallyretarded children are less responsiveto parents' (Eheart, 1982; Stonemanet al., 1983; Terdal et al., 1976) andsiblings' (Stoneman & Brody, inpress) social overtures. Their parentsand siblings are more likely to engagethem in directive/managerial/teachinginteractions. Also, Stoneman et al.(1986) found that nonhandicappedsiblings were more likely to engage insolitary play during several activitiesthan were sibling dyads with amentally retarded child. In a recenthome-based observational study, wetoo found that as a group not only didmentally retarded children engage inless solitary play (and more unoccu-pied behavior), they also receivedand emitted higher total rates ofpositive initiations and interactionswith both their siblings and mothers(Save Ile, Fox, & Phillips, 1987).Thus, compared to nonhandicappedchildren, mentally retarded chil-dren appear deficient not in theoverall amount of interaction withfamily members but in certainaspects of interaction (i.e., lessresponsive to others and fewerplayful interactions).
In summary, there have been very fewstudies of the in-home familyinteractions of either withdrawn(Finch & Hops, 1983) or of autisticchildren (Donne llan et al., 1984;Lichstein & Wahler, 1976; Martin &Graunke, 1979). Our knowledge ofwithdrawn children's interactionswith parents and siblings, thoughconsidered vital to socialization(Hartup, 1983; Maccoby & Martin,1983), is seriously lacking empirical-ly-based description. Social with-drawal has been considered aclinically significant problem at leastsince the turn of the century (Camp-bell, 1986) and is a ubiquitous factor

in the study of children's behavioraldisorders (Kauffman, 1985; Quay,1979). Yet even today we can saylittle about the quantity or quality ofwithdrawn children's interactions,positive or negative, with familymembers.
The situation is little better when weconsider autistic children. To date theseveral studies (Donne llan et al.,1984; Lichstein & Wahler, 1976;Martin & Graunke, 1979) haveproduced what would appear to beconsiderably different estimates ofpositive social interaction betweenautistic children and their families.In addition, these studies haveyielded disparate findings regardingstereotypic/other aberrant responses.Lichstein and Wahler (1976) foundthis to be the most predominantbehavior in their analyses, but Martinand Graunke (1979) and Donne Ilanet al. (1984) found stereotypy to becomparatively infrequent in theirgroup analyses. The implications ofdiffering rates of stereotypy wereindicated by the Donne llan studywhich found, not altogether surpris-ingly, that interactions were unlikelyto occur during periods of stereotypy.Lichstein and Wahler (1976), in anintensive single subject analysis,found a stable, inverse correlationbetween their categories of "self-stimulation" and "nonaversive adultsocial attention." These resultssuggest that it is important toconsider the occurrence and perhapsinfluence of aberrant behavior on thesocial relations of autistic childrenand their families. For example,stereotypic behavior may function topermit the autistic child to escape oravoid interaction with others.
As with studies of conduct disorderedchildren, attempts to synthesize ordraw conclusions from the fewanalyses of autistic children arefurther complicated by methodologi-cal and procedural differences (e.g.,behavior categories, observationalprocedures, length and frequency of
observations, setting conditions,individual vs. group analyses)between studies. To some degree, the"different" outcomes may be moreapparent than real. Clinical andanecdotal reports indicate that atleast some autistic persons becomemore aucial as they age (see De Myer,1979; Kanner, 1971; Kanner et al.,1972). Thus, one might expectdifferent results given the compara-tively young age of Lichstein andWahler's (1976) subject and thesubstantial age ranges of the childrenin the Martin and Graunke (1979)and the Donne Ilan et al. (1984)studies.
The differing results may also havebeen due to the differing analyticapproaches taken by the severalinvestigators, intensive single case(Lichstein & Wahler, 1976), andgroup statistical analysis (Donne Ilanet al., 1984; Martin & Graunke,1979). Given the substantial inter-subject and intrasubject variability insocial behaviors reported by Martinand Graunke (1979) and Lichsteinand Wahler (1976), respectively, it isnot at all surprising that three suchdiscrepant estimates of interactioncould result.
At the same time, however, it maybe thatlike mentally retardedchildrenbehaviorally disorderedchildren cannot be reliably distin-guished from their nonhandicappedcounterparts in terms of the overallamount of interaction with parentsor siblings. Autistic and mentallyretarded children sometimes exhibitsimilar behavior deficits andexcesses, and thus it may be thatthe bulk of autistic children'sinteractions with family membersare, as those of mentally retardedchildren, composed of directive,teaching, or manageriai socialexchanges. To address this possibil-ity, it will be necessary to employmore fine-grained behavior catego-ries and analyses than thosereported to date.
r."
It may be thatlike childrenwith mental retardationchildren with behavioraldisorders cannot be reliablydistinguished from theirnondisabled counterparts interms of the overall amount ofinteraction with parents orsiblings.
CCBD Retrospective Series / 33

There have been relatively fewobservational studies of the in-home, family interaction
patterns of children withbehavioral disorders.
34 / CCBD Retrospective Seriessiimsnommil
General summary and conclusionsdescriptive analysis of family interac-tion. In summary, there have beenrelatively few observational studies ofthe in-home, family interactionpatterns of behaviorally disorderedchildren. This lack of research isparticularly at ute for withdrawn andautistic children. Second, the extantresearch studies do not clearlydelineate the degree to which differenttypes of behaviorally disorderedchildren (conduct disordered, with-drawn, autistic) are characterized bydeficits in positive social interactionwith parents or siblings when comparedto normally developing children.Thirdand possibly related to thesecond pointin each of the popula-tions reviewed here, methodologicaland procedural differences betweenstudies further delimit the conclu-sions that can be drawn.
A number of issues, both substantiveand methodological, confront thoseinterested in pursuing descriptiveanalyses of behaviorally disorderedchildren's family interactions. In viewof the dearth of studies in this areaand the sometimes conflicting,variable results of existing studies,there is an obvious need for furtherresearch. However, we think itunlikely that simply increasing thenumber of descriptive studies will, byitself, advance our understanding ofthe nature and extent of familyinteractions.
Rather, future investigators would dowell to heed the advice offered 20years ago by Bijou, Peterson, and Ault(1968) regarding precise descriptionsif not direct control of settingconditions in a descriptive study.Many of the studies we reviewed haveattempted to provide an account ofthe "natural" amount of interaction,imposing a minimum of restrictions.Yet, these "natural conditions" ofobservation have varied both withinand between studies. We have arguedthat variations in physical and socialsetting factors may very well have
imposed variability in subjects'interactive behavior within andbetween studies.
For example, Patterson and hiscolleagues (Arnold et al., 1975;Patterson, 1976; Taplin & Reid,1977) required that all familymembers be present and that theyrestrict themselves to certain rooms ofthe hote-e during observation; Mashand Mer-er (1979) and Snyder(1977), however, restricted theirobservations to interactions betweensubjects and certain family members(siblings and parents, respectively)and conducted their observations incontrived settings. Research withnormally developing children hasshown that the type and frequency oftheir social interactions vary as afunction of changes in the socialcomposition of a setting (Brody,Stoneman, & MacKinnon, 1982;Corter, Abramovitch, & Pepler, 1983).What is needed, then, are studiesthat provide quantitative descriptionsof behaviorally disordered children'sfamily interactions in the context ofspecifically defined and measuredsetting conditions. Such a databasewould likely allow us to make moreinformed judgments about the needfor and nature of social behaviorinterventions.
A third issue is the conceptualizationand measurement of social behaviorsin family interaction research. Thecontinued use of global categoriessuch as positive, prosocial, or pleasinginteraction will not permit us toidentify the specific skills which arecritical to and facilitative of positivesocial exchanges between familymembers. Indeed, if we take aninteractionist reciprocal socialexchange perspective on children'ssocial development (see Shores'article in this issue), then it becomesimperative to more specificallyanalyze and describe the componentsof effective social interaction. Suchan approach has proven fruitful inschool-based studies (Strain, 1983;

Tremblay, Strain, Hendrickson, &Shores, 1981) and in home-basedstudies of nonhandicapped (Abramo-vitch et al., 1986), mentally retarded(Stoneman & Brady, in press), andconduct disordered children (Patter-son, 1982). Combined with thecontextual or setting factor analysesthis reciprocal perspective shouldpermit the development of a moreuseful descriptive database.
Family-basedIntervention ResearchConduct disordered children. In oneof the earliest reports of home-basedbehavioral treatment, llawkins,Peterson, Schweid, and Bijou (1966)described the parent-mediatedtreatment of a young boy exhibitingtantrums, disobedience, and aggres-sion to objects and people, especiallyhis younger sister. These "objection-able behaviors" were observed andthen treated by having the motherapply timeout contingent upon theiroccurrence and "occasionally" attendpositively to the subject's appropriateplay. Objectionable behaviorsdecreased during this intervention.Although never systematicallyrecorded, positive interactionsbetween mother and child reportedlyincreased also.
O'Leary, O'Leary, and Becker (1967)dealt more directly with increasingpositive interaction between a 6-year-old behaviorally disordered boy andhis younger brother. Cooperative,deviant, and isolate play were observedin the home. Prior to intervention, theboys' play interactions were character-ized by fighting, breaking toys andfurniture, tantrums, and noncomplianceto parents' instructions. Differentialreinforcement of cooperative play andtimeout for deviant behavior wereapplied first by the experimenters andlater by the parents. The interventionprocedures reliably increasedcooperative play between the siblings.Interestingly, isolate play alsoincreased during intervention.
Leitenberg, Burchard, Burchard,Fuller, and Lysaght (1977) contrastedthe effects of two differential attentionprocedures designed to reducesibling conflict between 6 behaviorproblem children and their siblings.Sibling conflict (verbal and physicalaggression) and appropriate interac-tion (playing games together, sharing,helping, conversation) were observedin the home. Following baseline,parents applied two different inter-ventions in alternating weeks.Differential reinforcement of otherbehavior (DRO) involved parentsdelivering contingent praise andpennies to both children for eachminute in which sibling conflict didnot occur. The second procedure,reinforcement of appropriate interac-tion (RAI), consisted of the samerewards delivered only after aninterval in which the siblings hadinteracted appropriately. Both DROand RAI reduced sibling conflictequivalently and both were associatedwith increases in appropriateinteraction. However, RAI resulted insubstantially more appropriatesibling.interaction.
Lavigueur (1976) evaluated a slightlydifferent approach to increasingsiblings' positive interactions inwhich siblings as well as parentsserved as intervention agents.Subjects were two disruptive childrenfrom two different families and theirsiblings, neither of whom werebehavior problems. Intcrval recordingsampled positive and negativeverbalizations, offering and givinghelp, aggression, noncompliance,playing, and positive affect. Followingbaseline, two procedures werecontrasted in sequential phases: (a)parent application of differentialattention and timeout contingent uponthe occurrence of target behaviors;and (b) application of differentialattention by both parents andsiblings. Initial targets were positiveand negative verbalizations. Later,"offering help" and "giving help"were added for families A and B,
BEST COPY AVAILABLE Ii
Family-based intervention
research is critical to the field.1111.1
CCBD Retrospective Series / 35smos

Differential reinforcement ofprosocial behavior and
reductive contingencies forinappropriate behavior havenot always increased positiveinteraction in families ofchildren with conductdisorders.
11111111111111111111111111111111111111101M1111011
36 / CCBD Retrospective Series
respectively. In family A, positiveverbalizations and offering helpincreased after the parent-onlyintervention but were not furtheraffected by the combined parent-sibling intervention. However,negative verbalizations did notdecrease until the combined inter-ventions were applied. In family B,all three behavior targets werechanged by the parent interventionalone. During the last two phases ofparent and parent-sibling interven-tion, play between the siblings (nevera direct treatment target) alsoincreased.
Thus, although increases wereobtained in several categories ofpositive interaction, the siblingintervention effects were minimal.
Differential reinforcement of proso-cial behavior and reductive contin-gencies for inappropriate behaviorhave not always increased positiveinteraction in families of conductdisordered children. In Tap lin andReid's (1977) study of aggressiveboys, parents applied a "socialreprogramming" interventionbehavior contracts, awarding ofpoints and rewards for prosocialbehaviors, and timeout for behaviorproblems. (However, it is unclear towhat extent positive social intcrac-tion as we have defined it here wastargeted.) Although maladaptiveparent-child interactions (positiveconsequences for deviant andaversive consequences for prosocialbehavior) were reduced, there was nochange in parents' positive conse-quences for children's prosocialbehavior.
Kelly, Embry, and Baer (1979) founda similar lack of effect of differentialattention and further demonstratedthat the problem child's positivesocial behavior to parents did notincrease until parents were taught tosupport each other's use of behaviormanagement techniques, and specific
A
positive interactions between parentsand child were arranged on a regularbasis.
Finally, Wahler and Fox (1979)investigated the relative effects ofsocial and independent toy playbehavior contracts on behaviorproblems and positive interactionsbetween several conduct disorderedboys and their mothers. Socialcontracts involved reinforcingsubjects for brief periods of appropri-ate play and interaction with theirmothers. Independent play contractscalled for reinforcing subjects forequivalent periods of appropriatesolitary play. Although parent-childinteraction increased under the socialcontract, there were concurrentincreases in the boys' oppositionalactions. The subsequent solitary playcontract condition returned interac-tion to baseline levels and decreasedoppositional behavior below baselinelevels.
Withdrawn, autistic, and mentallyretarded children. Published,empirical reports of home-basedinterventions designed to increasepositive interaction between sociallywithdrawn children and their parentsor siblings are virtually nonexistent.Studies with autistic children are alittle more frequent.
Miller and Cantwell (1976) reportedtwo case studies of sibling-mediatedintervention, one of which involved aboy who was "moderately retardedwith autistic features." Four oldersiblings were taught to use mildreprimands and timeout to eliminatethe subject's food stealing. Also, eachsibling was asked to spend 15minutes each day in a one-to-oneactivity (playing cars, going for awalk) with the subject, during whichtime they were to "encourage eyecontact, coherent speech, andappropriate social behaviors."Although quantitative measures ofinteraction and specifics of the
encouragement procedures were notreported, arguing was reportedlydecreased and positive interactionincreased.
Hems ley et al. (1978) describedlong-term outcomes of a behavioral,home-based training program forfamilies of autistic children. Al-though the specific interventions forteaching social interaction skills werenot described, increases were notedin certain classes of mother-childinteractive behaviorsocial languageof the child and language-facilitatingbehaviors of the mother such aspraise, corrections, prompting,questions, and expansions. However,other categories of interaction (playwith mother, overall positive interac-tion) did not increase.
Finally, in a recent study by Black-man (1986), mothers of two handi-capped girls were taught a set ofprocedures and target social initia-tions with which to increase positiveinteraction between their handi-capped and nonhandicapped chil-dren. One handicapped subject hadbeen identified as moderatelyretarded, socially withdrawn, andoppositional; the other had beendiagnosed as autistic and wasdescribed by her parents as severelywithdrawn and echolalic. Theprocedures (modeling, prompting,contingent praise) and target behav-iors (verbally organizing play,sharing, assisting) were those initiallydeveloped for classrooms (Day,Lindeman, Powell, Fox, Stowitschek,& Shores, 1984; Day, Powell, &Stowitschek, 1980) and later modi-fied for use with families (Powell,Salzberg, Rule, Levy, & Itzkowitz,1983). Parents applied the proce-dures'to both the handicapped andnonbandicapped siblings during a10-minute training session. Two 5-minute generalization sessions werealso conducted, one just before(delayed) and one just after (immedi-ate) the training session to assess
generalization of increased siblinginteraction to occasions whenintervention was not being applied.Previously, Powell et al. (1983)reported spontaneous transfer ofincreased sibling interaction todelayed, but not to immediate,generalization sessions. AlthoughBlackman (1986) found increasedinteractions during training for bothsibling dyads, there was littleevidence of transfer to either general-ization session.
In contrast to withdrawn and autisticchildren, mentally retarded childrenand their families have increasinglybeen the focus of applied socialinteraction research. Seitz and Terdal(1972) reported successful treatmentof interactional problems between amother and her young mentallyretarded son in a clinic setting.During pretest observations, mother-child interactions were characterizedby high rates of maternal instructionsand child noncompliance. Childcompliance and positive interactionincreased following therapist model-ing of how to praise, follow thechild's lead, and decrease instruc-tions. Similar increases in positiveinteraction were reported by Mashand Terdal (1973) who used grouptraining procedures to teach moreeffective play skills and behaviormodification techniques to severalgroups of mothers of handicappedchildren.
Christophersen and Sykes (1979)described a home-based program forthree families of developmentallydelayed children. Positive andnegative interactions were observed athome before and after parentsimplemented a reward system forappropriate behavior and timeout forinappropriate behavior. Positive andnegative interactions were verybroadly defined and the specificbehaviors for which these contingen-cies were arranged were not de-scribed. Subsequent to intervention,
In contrast to children who are
withdrawn and autistic, children
with mental retardation andtheir families have increasinglybeen the focus of appliedsocial interaction research.
ainimmimmummommis
CCBD Retrospective Series / 37

Parent training taught parentsto apply direct teaching tactics
to teach the target behaviorsand to increase siblinginteraction.
11110111=11111111111111
38 / CCBD Retrospective Series
positive interactions between all threesubjects and their parents increased;negative interactions decreased fortwo of the three.
McCollum (1984) used modeling,videotaped feedback, and discussionto increase specific socially-directed
iaternal behaviors (facial movementtoward the child, turn taking, vocalimitation of the child). Thesebehaviors were thought likely toincrease handicapped infants' andtoddlers' vocalizations and toy play.Increases in the mothers' targetbehaviors were associated withincreases in children's target behav-iors. However, these increases did nottransfer to generalization playsituations between the mothers andchildren.
Peer interaction research has spawnedseveral studies of sibling interactionsof mentally retarded children. Powellet al. (1983) experimentally investi-gated a parent-mediated intervention(see above description) to increasepositive interaction between theirhandicapped and nonhandicappedchildren. All handicapped subjectshad been previously diagnosed asmoderately mentally retarded and hadbeen referred to the investigators dueto deficits in sibling interaction.Target behaviors were sharing,verbally organizing play, assisting,rough and tumble, and affectionbehaviors that facilitated positiveresponses from peers in classroomreseatch (Tremblay et al., 1981).Reciprocal interactions were observedduring a 10-minute session involvingthe subject, sibling, and parent (thislater became the training time) andduring a subsequent 15-minutegeneralization session including onlythe two children. Three conditionswere implemented successively in amult;ple baseline across families;Baseline, Initial Attempts, and ParentTraining. In Initial Attempts, theexperimenters simply asked parents,without any training, to do their best
to get the children to play together.Parent Training taught parents toapply direct teaching tactics to teachthe target behaviors and to increasesibling interaction. During Baselineand Initial Attempts there was littleor no sibling interaction. ParentTraining increased the frequency andduration of sibling play interactionsmarkedly. Three of the four siblingdyads spontaneously increased theirinteractions during the generalizationsessions.
Since the Powell et al. (1983) study,there have been several replicationsand extensions. In the first of a seriesof studies, Save Ile, Fox, Spiegel-McGill, and Blackman (1986)attempted to identify the locus anddurability of change in siblinginteraction that might result from theinteraction training procedures.Because Powell et al. (1983) used asingle, broadly defined category ofreciprocal interaction, it could not bedetermined if changes in interactionresulted from increases in handi-capped children's, siblings', or bothchildren's initiations. Also, Powell etal. did not assess the durability ofthese gains.
In our first case study (A-B designwith follow-up), subjects were a 7-year-old moderately retarded girl, her5-year-old normally developing sister,and their parents. Target behaviors,parent training, and intervention werethe same as in the Powell et al.(1983) study. However, a continuous,sequential recording system noted thetopography of social behavior(positive/negative, initiations/response, extended interaction) andthe identity of the person (subject,sibling, parent) emitting the behavior.Second, parent intervention wasgradually faded out, and fellow-upobservation was conducted 3 monthsafter all intervention had ended. Boththe subject and her sister increasedtheir initiations and responses to oneanother as well as their extended

interactions, the subject's initiationsincreasing more than those of hernonhandicapped sibling. Althoughboth children's initiations decreasedas the parent intervention was fadedout, their extended interactionsincreased. At follow-up, initiationswere within intervention frequencies;and although extended interactionshad decreased, they remained abovebaseline levels.
In a later case study (Save Ile et al.,1986), the effects of the socialinteraction training procedures on amoderately retarded boy with ahistory of predominately negativeinteractions with family memberswere evaluated. Observation andintervention procedures remained thesame. When the mother beganintervention, the handicapped boy'spositive initiations to and interactionswith his older sister increased. Noconsistent change was noted in thesibling's initiations. Withdrawal ofintervention failed to completelyreverse these interactions, cloudingthe demonstration of experimentalcontrol. Such failure to completelyreverse increased social interactionsis not unknown in social interactionresearch (see Hecimovic, Fox, Shores,& Strain, 1985) and may indicate theoperation of any one of severalprocesses, for instance, "entrapment"of the siblings in mutually reinforc-ing interactions (see Baer & Wolf,1970; Kohler & Greenwood, 1986;McConnell, this issue) or reactivity tothe observer.
More recently, James and Egel (1986)analyzed effects of a package of socialinteraction training procedures, usingnonhandicapped siblings as theprimary intervention agents. Partici-pants were three socially withdrawn,handicapped children, their oldernonhandicapped siblings, and anonhandicapped friend of the sibling.The handicapped children were each4 years old and were mentallyretarded and/or physically handi-
capped. Siblings were 6 to 8 years ofage. During intervention, the experi-menters trained the nonhandicappedsiblings to initiate interactions,prompt responses, and reinforce bothinitiations and responses by thehandicapped child. Mothers learnedto use response priming (a verbalreminder to play together) duringgeneralization probes. Intervalrecording of initiations and reciprocalinteractions were conducted in thehome during (a) freeplay probes withthe sibling dyads and experimenter;(b) generalization probes involvingthe sibling dyads, nonhandicappedfriend, and parent (but excluding theexperimenter); and (c) 6-monthfollow-up probes similar to thegeneralization probes. A multiplebaseline across siblings analyzed theeffects of the sibling-mediatedintervention. Results showed that (a)the sibling-mediated interventionincreased initiations and interactionsbetween the siblings during freeplayprobes and these gains persisted atthe 6-month follow-up; (b) similarincreases in sibling initiations andinteractions occurred during generali-zation probes without interventionand response priming by the motherfurther magnified these generalizationeffects; (c) nonhandicapped friends'initiations to subjects increasedslightly during generalization probesbut handicapped subjects' initiationsto the friend did not; and (d) acrosssetting generalization of siblinginteraction was also noted.
Summary and conclusions. Tosummarize, there have been compara-tively few analyses of interventionsdesigned to increase behaviorallydisordered children's positiveinteractions with family members.This paucity of research is particular-ly evident for withdrawn and autisticchildren. Studies with conductdisordered children have producedmixed results, some showing thatpositive interactions with parents andsiblings can be increased through
BES1 copy AVAILABLE
There have beencomparatively few analyses of
interventions designed to
increase the positiveinteractions between children
with behavioral disorders and
other family members.
immiammummommo
CCBD Retrospective Series / 39

Child development theoristshave often linked internalizingdisorders such as socialwithdrawal to parent-child
interaction patterns.
1111=1=11111111111111111111111111
40 / CCBD Retrospective Seriesimsommimw
some form of differential reinforce-ment of appropriate interaction eitheralone or in combination with reduc-tive contingencies for negativebehaviors (Lavigueur, 1976; Leiten-berg et aL, 1977; O'Leary et al.,1967) while others have not (Kelly etaL, 1979; Tap lin & Reid, 1977). Atleast one study has shown thatincreasing positive interactionbetween some conduct disorderedchildren and their families hadunintended negative side effects onproblem behavior (Waller & Fox,1979).
The authors of this articl? wereunable to find any family-basedintervention studies of sociallywithdrawn children. Socially with-drawn children have been frequenttargets of intervention studies inclassroom settings (Odom & DeKly-an, in press; Strain & Fox, 1981).Also, child development theoristshave often linked internalizingdisorders such as social withdrawal toparent-child interaction patterns(e.g., Becker, 1964). Although thedata supporting this link are tenuous(Becker, 1964; Hetherington &Martin, 1979), recent researchsuggests that a child's scores onlaboratory measures of maternalattachment predict sociability withpeers. Consequently, the lack offamily-based intervention studieswith withdrawn children is surpris-ing. There remains a need to identifyand experimentally analyze parentand sibling behaviors which mayfacilitate the social behavior develop-ment of withdrawn children.
Equally surprising is the rarity ofstudies with autistic children,especially given the central role ofimpaired social responsiveness inautism. Social withdrawal is one ofthe primary defining characteristicsof the disorder (Kanner, 1943;Kauffman, 1985), a major concern ofparents (De Myer, 1979), and acritical factor in the integration of
4 3
severely handicapped persons intomore normalized environments(Brady, Gunte; McEvoy, Shores, &Fox, 1984). The outcomes of the fewfamily-based intervention studies ofautistic children are promising.Given training, parents (Blackman,1986; Hemsley et aL, 1978) orsiblings (Miller & Cantwell, 1976)can intervene to increase positiveinteractions with an autistic familymember. However, several cautionsare in order. With the exception of theBlackman study, interventionprocedures leading to improvedsocial interaction have not been wellspecified.
A somewhat similar problem exists interms of the locus of social behaviorchange. As Gaylord-Ross and Haringnote elsewhere in this issue, it isimportant that interventions not onlyincrease interaction between autisticand nonhandicapped persons, butthat they also teach the handicappedperson to initiate and reasonablysustain interactions.
Finally, the small number of childrenand families studied puts at issue thereplicability and generality of theseresults ft,, the larger population offamilies with autistic children. Again,there is an obvious need for furtherfamily-based intervention researchwith autistic children.
This is not to say that the need forfamily-based approaches to soci4development is going unheeded. Infact, over the past decade a numberof publications have discussed thenature and implications of autisticwithdrawal for the family and havedescribed clinical programs thataddress the social needs of autisticchildren and their families (see forexample, Rutter & Schopler, 1978;Schopler & Mesibov, 1984, 1986).However, it seems that what we dolack is an adequate empirical basefor family intervention that identifiestarget social skills, environmental

contexts, and efficient interventionprocedures for enhancing the socialdevelopment of autistic children andadolescents.
The slightly larger body of interven-tion research with mentally retardedchildren and their families is of somehelp in this respect. Generally, theseintervention procedures have beenmore specifically described and thestudies more controlled. Again, theresults are encouraging. Both parents(Christophersen & Sykes, 1979;Mash & Terdal, 1973; McCollum,1984; Powell et al., 1983; Save Ile etal., 1986; Seitz & Terdal, 1972) andsiblings (James & Egel, 1986) havesuccessfully applied learning theory-based interventions to increasepositive interactions with mentallyretarded children. Indeed, familyresearchers have already begun toapply and evaluate generalization and
maintenance programming tech-niques, such as response priming(James & Egel, 1986) and fading ofintervention tactics (Save Ile et al.,1986). There may, however, belimits to the applicability of thesestudies to families with autisticchildren. Potential limiting factorsinclude the degree and specificnature of social withdrawal (Strain& Fox, 1981) and the presence ofcompeting or aberrant responses(Donne Ilan et al., 1984; Lichstein& Wahler, 1976).
In the studies reviewed, few of thementally retarded subjects appearedunresponsive to parents' or siblings'social overtures when they occurrednor were many characterized aaengaging in high rates of stereotypicor other aberrant behavior. It remainsto be seen if and how existing socialintervention procedures will need tobe modified for children who exhibit
more extreme withdrawal (lessresponsiveness to or active avoidanceof social overtures) and/or who engagein high rates of stereotypic and other
aberrant behavior.
Finally, there are research issues andneeds that cut across categoricalboundaries. We briefly pose theGe as
a series of questions below.
1. What are the behavioral targetsthat if taught will facilitate andperhaps "entrap" behaviorallydisordered children and theirsiblings or parents into positiveinteraction? Will the socialinitiation targets which effect peerinteraction (Strain, 1983; Trem-blay et al., 1981) serve a similarfunction in sibling or parentinteraction? So far the outcomeshave been quite positive in thosefamily-based studies where thesesocial initiation skills have beentargeted (Blackman, 1986; Powellet al., 1983; Save Ile et al., 1986).On the other hand, recent descrip-tive analyses of normally developingchildren suggest that sibling andpeer interactions differ in terms of
social roles assumed by theinteractantsteacher, manage;playmate, initiator, responder(Abramovitch et al., 1986; Brody,Stoneman, MacKinnon, & Mac-Kinnon, 1985; Stoneman, Brody, &MacKinnon, 1984). What iscurrently needed are studies ofchildren that descriptively andexperimentally analyze the socialeffects of particular behaviorsmuch as Strain (1983) andTremblay et al., (1981) conductedin preschool settings.
2. What of the contexts in whichresearchers have sought toincrease family interaction? Withfew exceptions, researchers haveanalyzed and intervened uponbehaviorally disordered children'sinteractions in play situations. Canor should we reasonably expectchildren to engage in longer andlonger bouts of play interaction,especially when observational dataindicate that normally developingsibling pairs spend a considerableamount of time in solitary play
(e.g., Mash & Mercer, 1979;
Parents and siblings havesuccessfully applied learningtheory-based interventions to
increase positive interactions
with children with mental
retardation.
CCBD Retrospective Series / 41wommowalmrsol

The current gaps in our
empirical knowledge aboutfamily interaction are wide andcomplicated by the fact thatdirect, observation-based
studies of families are by nomeans easy to implement.
111111111111=1111111111111111111M1111
42 / CCBD Retrospective Seriesinomwilwi
Save Ile et al., 1986)? What are thevarious activities and situations inwhich sibling and parent interac-tions typically take place? Avariety of contexts other than playcan serve as occasions for interac-tions including television watching(Brody & Stoneman, 1983; Brody,Stoneman, & Sanders, 1980;Stoneman & Brody, 1983), goingfor walks (Miller & Cantwell,1976), and dinnertime conversa-tion. How, if at all, can thesesituations be used as opportunitiesfor improving family interactionsof behaviorally disorderedchildren and how may improve-ments in interaction in one ofthese home situations affectinteraction in another?
3. If interaction between behaviorallydisordered children and theirsiblings or parents increases, whatif any effects accrue to theirinteractions with other relatives,neighborhood children, or theirclassmates and teachers at school?James and Egel (1986) notedmodest generalization of increasesin retarded subjects' siblinginteraction to interactions with aneighborhood friend duringspecially arranged play sessionsand this is encouraging. However,other descriptive (Abramovitch etal., 1986; Bernal et al., 1976;Lichstein & Wahler, 1976) andintervention (Wahler, 1975)studies have found little acrosssetting or person generalization ofinteraction patterns.
4. It is now almost trite to say thatthere is a need for generalizationand maintenance research.However, it is true that socialinteraction interventions havebeen quite effective at producingsituational change and lessreliable in creating broader, moredurable impact on social develop-ment. Techniques for "program-ming" generalization and mainte-nance of social behavior gains are
available and have tentativeempirical support. These includemultiple exemplar training (e.g.,Brady, Shores et al., 1984; Fox etal., 1984; Gaylord-Ross, Haring,Breen, & Pitts-Conway, 1984) andresponse-dependent fading ofintervention tactics (e.g., Fox,Shores, Lindeman, & Strain,1986; Timm, Strain, & Eller,1979). Certain of these techniques(i.e., intervention fading tactics)and others such as responsepriming have also begun to beapplied in families of handi-capped withdrawn children (James& Egel, 1986; Save Ile et al.,1986). What is needed then areadditional systematic analyses ofthe generalization and mainte-nance effects of these and othersimilar tactics and of the settingsand persons of whom generaliza-tion can be achieved. In manyrespects, the James and Egel(1986) study provides futureresearchers with an exemplarymodel.
These and many other questionsconfront those who would attempt amore comprehensive understandingof the social development of behav-iorally disordered children. As wehave tried to point out, the currentgaps in our empirical knowledgeabout family interaction are wide.This is complicated by the fact thatdirect, observation-based studies offamilies are by no means easy toimplement. Yet, the studies reviewedillustrate that such research can bedone and give a foundation uponwhich to increase the database.Hopefully, the issues and questionsraised will serve as a point ofdeparture and debate if not somethingof a guide for future research.
REFERENCES
Abramovitch, R., Carter, C., Peppier, D.,tit Stanhope, L. (1986). Sibling andpeer interaction: A final follow-up and

a comparison. Child Development, 57,217-229.
Arnold, J., Levine, A., Patterson, G.(1975). Changes in sibling behaviorfollowing family intervention. Journalof Consulting and Clinical Psychology,43, 683-688.
Baer, D., & Wolf, M. (1970). The entryinto natural communities of reinforce-ment. In R. Ulrich, T. Stachnik, & J.Mabry (Eds.), Control of humanbehavior, from cure to prevention (Vol.2, pp. 319-324). Glenview, IL: Scott-Foresman.
Becker, W. (1964). Consequences ofdifferent kinds of parental discipline.In M. Hoffman & L Hoffman (Eds.),Review of child development research(Vol. 1, pp. 169-208). New York:Russell Sage Foundation.
Bernal, M., Delfini, L., North, J., &Kreutzer, S. (1976). Comparison ofboys' behaviors in homes andclassrooms. In E. Mash, L. Hamer-lynck, & L Handy (Eds.), Bthaviormodifwation and families (pp. 204-227). New York: Brunner-Mazel.
Bijou, S., Peterson, R., & Ault, M.(1968). A method to integratedescriptive and experimental fieldstudies at the level of data andempirical concepts. Journal of AppliedBehavior Analysis, I, 175-191.
Blackman, J. (1986). Parent-mediatedtreatment of exceptional children'ssocial withdrawal. Unpublisheddoctoral dissertation, George PeabodyCollege for Teachers of VanderbiltUniversity.
Bower, E., & Lambert, N. (1961). Aprocess for inschool screening ofchildren with emotional handicaps.Princeton, NJ: Educational TestingService.
Brady, M. P., Gunter, P., McEvoy, M. A.,Shores, R. E., & Fox, J. J. (1984).Considerations for socially integratedschool environments for severelyhandicapped students. Education andTraining of the Mentally Retarded, 19,246-253.
Brady, M. P, Shores, R. E., Gunter, P,McEvoy, M. A., Fox, J. J., White, C.(1984). Generalization of an adoles-cent's social interaction behavior viamultiple peers in a classroom setting.Journal of the Association for SevereHandicaps, 9, 278-286.
Brody, G., & Stoneman, Z. (1983). Theinfluence of television viewing on
family interactions. Journal of FamilyIssues, 4, 329-348.
Brody, G., Stoneman, Z., & MacKinnon,C. (1982). Role asymmetries ininteractions among school-agedchildren, their younger siblings, andtheir friends. Child Development, 53,1364-1370.
Brody, G., Stoneman, Z., MacKinnon, C.,& MacKinnon, R. (1985). Rolerelationships and behavior betweenpreschool-aged and school-agedsibling pairs. Developmental Psychol-ogy, 21, 124-129.
Brody, G., Stoneman, Z., & Sanders, A.(1980). Effects of television viewingon family interactions: An observa-tional study. Family Relations, 29,216-220.
Campbell, H. (1986). Morbid shyness.The British Medical Journal, 2, 805 -807.
Christophersen, E., & Stykes, B. (1979).An intensive, home-based familytraining program for developmentally-delayed children. In L. Hamerlynck(Ed.), Behavioral systems for thedevelopmentally delayed. Vol. 1.School and family environments (pp.89-101). New York: Brunner-Mazel.
Coder, C., Abramovitch, R., & Pepler, D.(1983). The role of the mother insibling interaction. Child Develop-ment, 54, 1599-1605.
Day, R., Fox, J. J., Shores, R. E.,Lindeman, D., & Stowitschek, J.(1983). The social competenceintervention project: Developingeducational procedures for teachingsocial interaction skills to handi-capped children. Behavioral Disor-ders, 8, 120-127.
Day, R., Lindeman, D., Powell, T., Fox, J.J., Stowitschek, J., & Shores, R. E.(1984). Empirically-derived teachingpackage for socially withdrawnhandicapped and nonhandicappedchildren. Teacher Education andSpecial Education, 7, 46-55.
Day, R., Powell, T., & Stowitschek, J.(1980). The social competenceintervention package for preschoolyoungsters. Nashville, TN: GeorgePeabody College for Teachers atVanderbilt University.
Delfini, L., Bernal, M., & Rosen, P(1976). Comparison of deviant andnormal boys in home settings. In E.Mash, L. Hamerlynck, & L. Handy(Eds.), Behavior nwdification and
BEST COPY AVAILABLE
CCBD Retrospective Series 43

families (pp. 228-24.8). New York:Brunner-Mazel.
De Myer, M. (1979). Parents and childrenin autism. New York: John Wiley &Sons.
Donne Ilan, A., Anderson, J., & Mesaros,R. (1984). An observational study ofstereotypic behavior and proximityrelated to the occurrence of autisticchild-family member interactions.Journal of Autism and DevelopmentalDisorders, 14, 205-210.
Dunn, J., & Kendrick, C. (1982).Siblings: Love, envy, and understand-ing. Cambridge, MA: HarvardUniversity Press.
Eheart, B. (1982). Mother-childinteractions with nonretarded andmentally retarded preschoolers.American Journal of Mental Defi-ciency, 87, 20-25.
Finch, M., & Hops, H. (1983). Reme-diation of social withdrawal in youngchildren: Considerations for thepractitioner. Child and Youth Services,5, 29-42.
Foster, S., & Ritchey, W. (1979). Issues inthe assessment of social competencein children. Journal of AppliedBehavior Analysis, 12, 625-638.
Fox, J. J., Day, R., & McEvoy, M. A. (inpress). An empirically-basededucational approach to developingsocial competence in young children:Outcomes and issues. ChildhoodEducation.
Fox, J. J., Gunter, P, Brady, M. P,Bambara, L., Spiegel-McGill, P, &Shores, R. E. (1984). Using multiplepeer exemplars to develop generalizedsocial responding of an autistic girl.In. R. B. Rutherford & C. M. Nelson(Eds.), Severe behavior disorders ofchildren and youth (Vol. 7, pp. 17-27). Reston, VA: Council for Childrenwith Behavioral Disorders.
Fox, J. J., Shores, R. E., Lindeman, D., &Strain, P (1986). The effects ofresponse dependent fading proceduresin developing and maintaining socialinitiations of withdrawn preschoolchildren. Journal of Abnormal ChildPsychology, 14, 387-396.
Gaylord-Ross, R., Haring, T., Breen, C.,& Pitts-Conway, V. (1984). Thetraining and generalizations of socialinteraction skills with autistic youth.Journal of Applied Behavior Analysis,17, 229-247.
Cordon, S., & Davidson, N. (1981).Behavioral parent training. In A.
44 / CCBD Retrospective Series
Gunnan & D. Kniskern (Eds.),Handbook of family therapy (pp. 515-575). New York: Brunner-Mazel.
Hartup, W. (1970). Peer interaction andsocial organization. In I! Mussen(Ed.), Carmichael's manual of childpsychology (Vol. 2, pp. 361-456). NewYork: John Wiley & Sons.
Hartup, W. (1983). Peer relations. In PMussen (Series Ed.), Handbook ofchild psychology (4th ed., pp. 167-172). New York: John Wiley & Sons.
Hawkins, R., Peterson, R., Schweid, E.,& Bijou, S. (1966). Behavior therapyin the home: Amelioration of problemparent-child relations with the parentin a therapeutic role. Journal ofExperimental Child Psychology, 4, 99-107.
Hecimovic, A., Fox, J. J., Shores, R. E.,& Strain, P (1985). An analysis ofdevelopmentally integrated andsegregated freeplay settings and thegeneralization of newly-acquiredsocial behaviors of socially withdrawnpreschoolers. Behavioral Assessment,7, 1367-388.
Hemsley, R., Nowlin, P. Berger, M.,Hersov, L, Holbrook, D., Rutter, M.,& Yule, W. (1978). Treating autisticchildren in a family context. In M.Rutter & E. Schopler (Eds.), Autism:A reappraisal of concepts andtreatment (pp. 379-411). New York:Plenum.
Hetherington, M., & Martin, B. (1979).Family interaction. In H. Quay & J.Weny (Eds.), Psychopathologicaldisord,ers of childhood (2nd ed., pp.247-302). New York: John Wiley &Sons.
Hops, H. (1982). Social skills training forsocially withdrawn/isolate children. In
Karoly & J. Steffen (Eds.),Improving children's competence:Advances in child behavior analysis(VoL 1, pp. 39-101). Lexington, MA:Heath.
James, S., & Egel, A. (1986). A directprompting strategy for increasingreciprocal interactions betweenhandicapped and nonhandicappedsiblings. Journal of Applied BehaviorAnalysis, 19, 173-186.
Kanner, L. (1943). Autistic disturbancesof affective contact. Nervous Child, 2,217-250.
Kanner, L. (1971). Follow-up study ofeleven children originally reported in1943. Journal of Autism and Child-hood Schizophrenia, 1, 119-145.

Kanner, L, Rodriguez, A., & Ashenden,B. (1972). How far can autisticchildren go in matters of socialadaptation? Journal of Autism andChildhood Schizophrenia, 2, 9-33.
Kauffman, J. (1985). Characteristics ofchildren's behavior disorders (3rd ed.,pp. 1-25, 66-81). Columbus, OH:Merrill.
Kelly, M., Embry, L, & Baer, D. (1979).Skills for child management andfamily support. Behavior Modification,3, 373-396,
Kohle; F., & Greenwood, C. (1986).Toward a technology of generalization:The identification of natural contin-gencies of reinforcement. BehaviorAnalyst, 9, 19-26.
Lamb, M. (1978). The development ofsibling relationships in infancy: Ashort-term longitudinal study. ChildDevelopment, 49, 1189-1196.
Lavigueur, H. (1976). The use of siblingsas an adjunct to the behavioraltreatment of children in the home withparents as therapists. BehaviorTherapy, 7, 607-613.
Leitenberg, H., Burchard, J., Burchard,S., Fuller, E., & Lysaght, T. (1977).Using positive reinforcement tosuppress behavior: Some experimentalcomparisons with sibling conflict.Behavior Therapy, 8, 168-172.
Lichstein, K., & Wahler, R. (1976). Theecological assessment of an autisticchild. Journal of Abnormal ChildPsychology, 4, 31-54.
Maccoby, E., & Martin, J. (1983).Socialization in the context of thefamily: Parent-child interaction. In EMussen (Series Ed.), Handbook ofchild psychology (4th ed., pp. 1-101).New York: John Wiley & Sons.
Martin, S., & Graunke, B. (1979). Abehavioral analysis of the homeenvironment of autistic children. In L.Hamerlynck (Ed.), Behavioral systemsfor the developmerually delayed: Vol.I. School and family environments(pp. 172-192). New York: Brunner-Mazel.
Mash, E., & Mercer, B. (1979). Acomparison of deviant and nondeviantboys while playing alone andinteracting with a sibling. Journal ofChild Psychology and Psychiatry andAllied Disciplines, 20, 197-207.
Mash, E., & Terdal, L. (1973). Modifica-tion of mother-child interactions:Playing with children. MentalRetardation, 11, 44-49.
McCollum, J. (1984). Social interactionbetween parents and babies:Validation of an intervention proce-dure. Child: Care, health, anddevelopment, 10, 301-315.
Michaelson, L, & Mannarino, A. (1986).Social skills training with children:Research and clinical application. InI? Strain, M. Guralnick, & H. Walker(Eds.), Children's social behavior.Development, assessment, andmodification (pp. 373-406). Orlando,FL: Academic Press.
Miller, N., & Cantwell, D. (1976). Siblingas therapist: A behavioral approach.American Journal of Psychiatry, 133,447-450.
Odom, S., & DeKlyen, M. (in press).Social withdrawal in childhood. In G.Adams (Ed.), Behavior disorders:Theory and characteristics. EnglewoodCliffs, NJ: Prentice-Hall.
O'Leary, K., O'Leary, S., & Becker, W.(1967). Modification of a deviantsibling interaction pattern in thehome. Behavior Research andTherapy, 5, 113-120.
Patterson, G. (1976). The aggressivechild: Victim and architect of acoercive system. In L. Hamerlynck, L.Handy, & E. Mash (Eds.), Behaviormodification and families: Theory andresearch (Vol. 1, pp. 267-316). NewYork: Brunner-Mazel.
Patterson, G. (1980). Mothers: Theunacknowledged victims. Mono-graphs of the Society for Research inChild Development, 44(5, Serial No.186).
Patterson, G. (1982). Coercive familyprocesses. Eugene, OR: Castalia.
Patterson, G., Ray, R., Shaw, D, & Cobb,J. (1969). Family observation code.Unpublished manuscript, Universityof Oregon, Eugene.
Powell, T., Salzberg, C., Rule, S., Levy,S., & Itzkowitz, J. (1983). Teachingmentally retarded children to playwith their siblings using parents astrainers. Education and Treatment ofChildren, 6, 343-362.
Quay, H. (1979). Classification. In H.Quay & Weny (Eds.), Psychopatho-logical disorders of childhood (2nded., pp. 1-42). New York: John Wiley& Sons.
Rutter, M., & Schopler, E. (1978).Autism: A reappraisal of concepts andtreatment. New York: Plenum..
Savelle, S., Fox, J. J., & Phillips, M.(1987, March). Handicapped and
CCBD Retrospective Series / 45

46 / CCBD Retrospective Series
nonhandicapped children's socialinteractions with their siblings: Apreliminary descriptive analysis. Paperpresented at the Gatlinburg Confer-ence on Research and Theory inMental Retardation and Developmen-tal Disabilities, Gatlinburg, TN.
Schopler, E., & Mesibov, G. (1984). Theeffects of autism on the family. NewYork: Plenum.
Schopler, E., & Mesibov, G. (1986).Introduction to social behavior inautism. In E. Schopler & G. Mesibov(Eds.), Social behavior in autism (pp.1-11). New York: Plenum.
Seitz, S., & Terdal, L (1972). A modelingto changing parent-child interactions.Mental Retardation, 10, 39-43.
Snyder, J. (1977). Reinforcement analysisof interaction in problem andnonproblem families. Journal ofAbnormal Psychology, 86, 528-535.
Stoneman, Z., & Brody, G. (1983). Familyinteractions during three programs.Journal of Family Issues, 4, 349-365.
Stoneman, Z., & Brody, G. (in press).Observational research on mentallyretarded children, three parents, andtheir siblings. In S. Lanesman &Vietze (Eds.), Living environmentsand mental retardation. Washington,DC: AAMD.
Stoneman, Z., Bnxly, G., & Abbott, D.(1983). In-home observations ofyoung Down's syndrome children withtheir mothers and fathers. AmericanJournal of Mental Deficiency, 87, 591-600.
Stoneman, Z., Brody, G., Davis, C., &Crapps, J. (1986, April). Mentallyretarded children and their oldersiblings: Role relationships andresponsibilities. Paper presented atthe Conference on Human Develop-ment, Vanderbilt University,Nashville, TN.
Stoneman, Z., Brody, G., & Mac-Kinnon, C. (1984). Naturalisticobservations of children's activitiesand roles while playing with theirsiblings and friends. Child Develop-ment, 55, 617-627.
Strain, P (1983). Identification of socialskill curriculum targets for severelyhandicapped children in mainstreampreschools. Applied Research inMental Retardation, 4, 369-382.
Strain, P, & Fox, J. (1981). Peers asbehavior change agents for withdrawnclassmates. In B. Lahey & A. Kazdin(Eds.), Advances in clinical childpsychology (Vol. 4, pp. 167-198). NewYork: Plenum.
Strain, P, Guralnick, M., & Walker, H.(1966). Children's social behavior anddevelopment: Assessment andmodification. Orlando: AcademicPress.
Taplin, P., & Reid, I (1977). Changes inparent consequation as a function offamily interaction. Journal ofConsulting and Clinical Psychology,4, 973-981.
Terdal, L, Jackson, R., & Game; A.(1976). Mother-child interactions: Acomparison between normal anddevelopmentally delayed groups. In E.Mash, L. Hamerlynck, & L. Handy(Eds.), Behavior modification andfamilies (pp. 249-264). New York:Brunner-Mazel.
Timm, M., Strain,P, & Eller, P (1979).Effects of systematic response-dependent fading and thinning on themaintenance of child-child interac-tion. Journal of Applied BehaviorAnalysis, 12, 308.
Tramblay, A., Strain, P, Hendrickson, J.,& Shores, R. E. (1981). Socialinteractions of normally developingpreschool children: Using normativedata for subject and target behaviorselection. Behavior Modification, 5,237-253.
Van Hasselt, V, Hersen, M., Whitehill,M., & Bellack, A. (1979). Social skillassessment and training for children:An evaluative review. BehaviorResearch and Therapy, 17, 413-437.
Wahler, R. (1975). Some structuralaspects of deviant child behavior.Journal of Applied Behavior Analysis,8, 27-42.
Wahler, R., & Fox, J. J. (1979). Solitarytoy play and timeout: A familytreatment package for children withaggressive and oppositional behavior.Journal of Applied Behavior Analysis,/3, 23-39.
Wahler, R., House, A., & Stambaugh, E.(1976). Ecological assessment of childproblem behavior: A clinical packagefor home, school, and institutional
settings. New York: Pergamon.
BEST COPY AVAILABLE5 1.

Structured Learning:A Psychoeducational Approach forTeaching Social Competencies
Arnold P. GoldsteinRobert P. SprafkinJane GershawPaul Klein
ABSTRACT: This article describes the use of Structured Learning, apsychoeducational approach for teaching social competencies to adolescentsand preadolescents. The youngsters who are likely to be trained through Struc-tured Learning are generally categorized as aggressive, withdrawn, imma-ture, or developmentally lagging. Research evidence evaluating the effective-
ness of this approach is also discussed.
Psychological education, or what many are coming to refer to as thepsychoeducational movement, has been gaining an undeniable footholdwithin teacher training for many years. Growing out of the personaldevelopment context which nurtured such earlier movements as progres-sive education (Dewey, 1938) and character education (Chapman, 1977), anumber of psychoeducational approaches have emerged. These approachesgenerally deal with teaching concepts and behaviors relevant to values,morality, and emotional development. Such programs as moral education(Kohlberg, 1973), values clarification (Simon, Howe, & Kirschenbaum,1972), effective education (Miller, 1976), and identity education (Wein-stein & Fantini, 1970) are contemporary examples of this educationaldirection. They share concerns with the facilitation of social effectiveness,personal development, and competence within educational curricula. MAuthier, Gustafson, Guerney, and Kastorf (1975) observed, many individu-als would prefer to restrict formal education to the traditional 3R's andleave such concerns as morality, coping skills, and other aspects of socialcompetence to others (e.g., parents, religious organizations). However, the
demand for teachers and schools to meet these needs in youngsters isevident and increasing.
One psychoeducational approach known as Structured Learning hasgained considerable attention in recent years (Cartledge & Milburn, 1980;Goldstein, Sprafkin, Gershaw & Klein, 1980; Larsen, in press; Rathjen &Foreyt, 1980). Structured Learning consists of four major components,
Reprinted from Behavioral
Disorders, Vol. 8, Number 3, May
1983, pp. 161-170seimiww
CCBD Retrospective Series / 47

Skill deficiencies are mostlikely to be manifested inproblems of aggressiveness,
withdrawal, immaturity, and
associated difficulties insurmounting developmentalhurdles.
IIMIIMI1111111111111=11111111111111111101
48 / CCBD Retrospective Seriessimmimismoismosomismo
each of which has a strong empiricalbasis in psychology. These compo-nents are: (a) modeling, (b) roleplaying, (c) performance feedback,and (d) transfer of training. InStructured Learning, youngsters'interpersonal, affective, coping, andplanning behaviors are viewed asskills in which they may be proficientor nonproficient. The task of Struc-tured Learning is to teach these skillswhen youngsters are deficient inthem. Skills taught via StructuredLearning are divided into six groups.
Group I- Beginning Social Skills1. Listening2. Starting a conversation3. Having a conversation4. Asking a question5. Saying thank you6. Introducing yourself7. Introducing other people8. Giving a compliment
Group II- Advanced Social Skills9. Asking for help
10. Joining in11. Giving instructions12. Following instructions13. Apologizing14. Convincing others
Group III-Skills for Dealingwith Feelings
15. Knowing your feelings16. Expressing your feelings17. thiderstanding the feelings
of others18. Dealing with someone else's
anger19. Expressing affection20. Dealing with fear21. Rewarding yourself
Group IV-Skill Alternatives toAggression
22. Asking permission23. Sharing something24. Helping others2:). Negotiating26. Using self-control
00
27. Standing up for your rights28. Responding to teasing29. Avoiding trouble with others30. Keeping out of fights
Group V-. Skills for Dealing withStress
31. Making a complaint32. Answering a complaint33. Sportsmanship after the
game
34. Dealing with embarrassment35. Dealing with being left out36. Standing up for a friend37. Responding to persuasion38. Responding to failure39. Dealing with confusing
messages40. Dealing with an accusation41. Getting ready for a difficult
conversation42. Dealing with group pressure
Group VI-Planning Skills
43. Deciding on something to do44. Deciding on what caused a
problem45. Setting a goal46. Deciding on your abilities47. Gathering information48. Arranging problems by
importance49. Making a decision50. Concentrating on a task
Skill deficiencies are most likely tobe manifested in problems ofaggressiveness, withdrawal, immatu-rity, and associated difficulties insurmounting developmental hurdles.
Structured Learning is a grouptechnique, generally involving five toeight youngsters plus one or twotrainers. Adaptations for usingStructured Learning in regular-sizedclasses have also been made. Theapproach has been used mostextensively in regular and specialeducation classes in junior and seniorhigh schools or upper-level grades inelementary schools. Structured
Learning trainers have usually beendrawn from the ranks of regular andspecial education teachers. Thislatter group has shown particularinterest in Structured Learningbecause of its compatibility with therequirements of Public Law 94-142.Skill acquisition is geared towardenabling handicapped youngsters tofunction better within the leastrestrictive, most normal environment.As Structured Learning is behavioral-ly oriented, its procedures are able tobe assessed in observable, concreteterms necessary for the developmentof Individual Education Plans (IEPs),and for measuring progress inyoungster's skill acquizition.
TRAINING PROCEDURES
Modeling
Teaching a skill begins by exposinggroups of youngsters to vivid ex-amples (live on video or audio tape,filmsor filmstrip) of the skill beingused well. This constitutes themodeling component. Modelingdisplays present scenes or vignettesin which the protagonist handlespotentially troublesome situationssuccessfully by employing the skillbeing taught. One skill is taught at atime, so that the modeling vignettesdepict several examples of a singleskill being used in different situa-tions. To make a skill presentation asconcrete as possible, the skill isbroken down into its componentbehavioral steps, each of which isillustrated in the modeling vignette.Youngsters' skill deficits are assessedvia self-reports, observer's reports,and for research purposes, situationalbehavioral tests.
Role Playing
Following the presentation of themodeling display, a group discussionensues. Youngsters are urged tocomment on what they have seen andheard, and to relate the modeling ofthe skill to times in their own lives
when use of the perticular skill hasbeen difficult. From the materialgenerated in these discussions, roleplays are developed. Each youngsteris given an opportunity to role play orpractice the skill as a rehearsal for asituation that might actually occur ina real-life circumstance. Thus roleplaying is presented as practice orrehearsal for future skill use. Eachyoungster in the main actor role getsan opportunity to choose as a co-actorsomeone who resembles the real-lifeprotagonist or antagonist in as manyways as possible, and to enact theskill following the behavioral stepswhich constitute the skill. Consider-able coaching and support is pro-vided by the trainers throughout therole play.
Performance Feedback
Following the enactment of the roleplay, the trainers elicit peiformancefeedback (approval, praise, construc-tive criticism) from the other groupmembers. In general in this phasr ,the main actor is given support aswell as helpful suggestions on howhis or her performance might bemade even more effective. At timesthe trainer may have the main actorreplay the scene immediately so thatthe feedback from the other young-sters (and/or the trainers) may beincorporated without delay.
Transfer of Training
Finally, in a forthright effort t effecttransfer of training, or transfer of theskill into the youngsters' real-lifebehavioral repertoire, a variety ofprocedures are implemented:
I. Provision of general principles.Transfer of training has been demon-strated to be facilitated by providingtrainees with general mediatingprinciples governing successful orcompetent performance on thetraining and criterion tasks. Thisprocedure has typically been opera-tionalized in laboratory contexts by
Social skills trainingprocedures indude modeling,
role-playing, performancefeedback, and transfer of
training.
IIIIMIN1111111111110111111M=111
CCBD Retrospective Series / 49111111111111111111111111111111

The greater the similarity ofphysical and interpersonalstimuli in the Structured
Learning setting and theschool, home, or other settingin which the skill is to beapplied, the greater thelikelihood of transfer.
111111111111111111111111111111111111111111111111111111111111111
50 / CCBD Retrospective SeriesImmommmiminmEmo
providing subjects with the organiz-ing concepts, principles, strategies,or rationales that explain or accountfor the stimulus-response relation-ships operative in both the trainingand application settings. Theprovision of general principles toStructured Learning trainees is beingoperationalized in our training by thepresentation in verbal, pictorial, andwritten forms of appropriate informa-tion governing skill instigation,selection, and implementationprinciples.
2. Over learning. Over learning is aprocedure whereby learning isextended over more trials than arenecessary merely to produce initialchanges in the subjects' behavior.The overlearning, or repetition ofsuccessful skill enactment, in thetypical Structured Learning session isquite substantial, with the given skilltaught and its behavioral steps (a)modeled several times, (b) roleplayed one or more times by thetrainee, (c) observed live by thetrainee as every other group memberrole plays it, (d) read by the traineefrom a blackboard and on the SkillCard, (e) written by the trainee in hisor her Trainee's Notebook, (f)practiced in vivo one or more timesby the trainee as part of the formalhomework assignment, (g) practicedin vivo one or more times by thetrainee in response to adult and/orpeer leader coaching, and (h)practiced in vivo one or more timesby the trainee in response to skill-oriented, intrinsically interestingstimuli introduced into his or herreal-life environment.
3. Identical elements. In perhaps thoearliest experimental concern withtransfer enhancement, Thorndike andWoodworth (1901) concluded :hatwhen there was a facilitative effect ofone habit on another, it was to theextent that and because they sharedidentical elements. Ellis (1965) andOsgood (1953) have more recently
emphasized the importance oftransfer of similarity betweenstimulus and response aspects of thetraining and application tasks. Thegreater the similarity of physical andinterpersonal stimuli in the Struc-tured Learning setting and the school,home, or other setting in which theskill is to be applied, the greater thelikelihood of transfer.
The "real-lifeness" of StructuredLearning is operationalized in anumber of ways. These operationalexpressions of identical elementsinclude (a) the relevant and realisticcontent and portrayal of the models,protagonists, andsituations in themodeling displays tapes, all designedto be highly similar to what traineesare likely to face in their daily lives;(b) the physical props used in andthe arrangement of the role-playingsetting to be similar to the real-lifesettings; (c) the choice, coaching, andenactment of the co-actors or protago-nists to be similar to real-life figures;(d) the manner in which the roleplays themselves are conducted to beas responsive as possible to the real-life interpersonal stimuli to which thetrainee will actually respond with thegiven skill, and to provide behavioralrehearsal of that skill as he/sheactually plans to employ it; (e) the invivo homeworkcoached andpracticed in the training group,completed in the real-world setting,and reported upon in the traininggroup in the immediately followingsession; and (0 the training of livingunits (all the members of a givenclass or cottage) as a unit.
4. Stimulus variability. Callantineand Warren (1955), Duncan (1959),and Shore and Sechrest (1961) haveeach demonstrated that positivetransfer is greater when a variety ofrelevant training stimuli are em-ployed. Stimulus variability isimplemented in our StructuredLearning studies by (a) rotation ofgroup leaders across groups, (b)

rotation of trainees across groups, (c)having trainees re-role play a givenskill with several co-actors, (d)having trainees re-role play a givenskill across several relevant settings,and (e) use of multiple homeworkassignments for each given skill.
5. Real-life reinforcement. Givensuccessful implementation of bothappropriate Structured Learningprocedures and the transfer enhance-ment procedures examined above,positive transfer may still fail tooccur. As Agras (1967), Gruber(1971), Patterson (1963), and Tharpand Wetzel (1969), and literallydozens of other investigators haveshown, stable and enduring perfor-mance in application settings ofnewly learned skills is very much atthe mercy of real-life reinforcementcontingencies.
We have found it useful to implementseveral supplemental programsoutside of the Structured Learningsetting to help provide the rewards ofreinforcements trainees need so thattheir new behaviors are maintained.These programs include provision forboth external social reward (providedby people in the trainee's real-lifeenvironment) and self-reward(provided by the trainee himself orherself).
In several schools, juvenile detentioncenters, and other agencies, we haveactively sought to identify anddevelop environmental or externalsupport by holding orientationmeetings for staff and for relativesand friends of trainees (i.e., the real-life reward and punishment givers).The purpose of these meetings was toacquaint significant others in thetrainees' life with Structured Learn-ing theory and procedures. Mostimportant in these sessions is thepresentation of procedures wherebystaff, relatives, and friends canencourage and reward trainees asthey practice their new skills. We
TABLE 1
Successful Transfer-Enhancing Procedures
1. Over learning (Lopez, 1977)
2. Helper role structuring (Litwack, 1977; Solomon, 1978)
3. Identical elements (Wood, 1977; Guzzetta, 1974)
4. Coping modeling (Fleming, 1976)
5. Stimulus variability (Hummel, 1977)
6. General principles (Lopez, 1977; Lack, 1975)
7. Programmed reinforcement (Gutride, Goldstein, & Hunter, 1973;Greenleaf, 1977)
8. In vivo feedback (Goldstein & Goedhart, 1973)
9. Teaching skills in tandem (reciprocal benefits) (Hummel, 1977)
10. Mastery induction (Solomon, 1977)
consider these orientation sessions forsuch persons to be a major value fortransfer of training.
Frequently, environmental support isinsufficient to maintain newlylearned skills. It is also the case thatmany real-life environments in whichtrainees work and live will activelyresist the trainees' efforts at behaviorchange. For this reason, we havefound it useful to include in ourtransfer efforts a program of self-reinforcement. Trainees can beinstructed in the nature of self-reinforcement and encouraged to "saysomething and do something nice foryourself" if they practice their newskill well.
The five transfer-enhancementprocedures we have briefly describedabove do not exhaust the actual rangeof techniques employed for suchpurposes that we have examined inour research program. A completelisting of these procedures, withcitation of our research program'sinvestigations) demonstrating theirtransfer-enhancing efficacy, are listedin Table 1 (Goldstein, 1981).
73EST COPY AVAILABLE
We have found it useful toimplement several
supplemental programs
outside of the StructuredLearning setting to helpprovide the rewards ofreinforcements trainees need
so that their new behaviors are
maintained.
111111111111111111111111111111111111=
CCBD Retrospective Series / 51ammilmommom

In Structured Learning groups,group members may activelyresist participation asprescribed, may participate butinappropriately, or may displayone or another form ofinactivity or hyperactivity.
52 / CCBD Retrospective Series
All of these demonstrated transfer-enhancing techniques, as well as asubstantial number of potentiallyfruitful techniques, are examined atlength in two recent texts devoted tothis all-important concern withgeneralization and endurance oftreatment effects (Goldstein &Kanfer, 1979; Karoly & Steffen,1980).
A thorough review of psychotherapyoutcome and follow-up researchconducted by us (Goldstein & Stein,1976) revealed that "though thenumber of studies reporting positivetherapeutic outcomes is high (85%),only 14% of the studies conductedreport maintenance or transfer oftherapeutic gains" (Goldstein &Kanfer, 1979, p. 2). This exceedinglylow level of persistence of effect hasalso been documented by many others(e.g., Kazdin, 1975; Keeley, Shem-berg & Carbonell, 1976; Margolin,Siegel, & Phillips, 1976). It is to benoted and underscored in thiscontext, however, that in our researchon Structured Learning we have beenable to attain a skill transfer effect inapproximately 45 to 50% of thetrainees involved. This skill transfereffect appears to occur in directproportion to the number of specifictransfer-enhancing procedures (seeTable 1) explicitly incorporated intothe Structured Learning format.
DEALING WITHMANAGEMENTPROBLEMS ANDRESISTIVE BEHAVIOR
In Structured Learning groups, as inall training or psychotherapy inter-ventions, group members mayactively resist participation asprescribed (e.g., cutting, lateness,refusal to role play, walking out), mayparticipate but inappropriately (e.g.,excessive restlessness, inattention,inability to remember procedures),display one or another form ofinactivity (e.g., apathy, minimal
participation, falling asleep), orhyperactivity (interrupting, monopo-lizing, digressing, jumping out ofrole). To deal effectively and rapidlywith this array of group or individualmanagement problems, we utilize oneor more of the following resistance-reducing techniques:
1. Empathic enccuragement. Thisintervention consists of: (a) offeringthe trainee the opportunity to explainin greater detail his/her difficulty inparticipating as instructed andlistening nondefensively; (b) clearlyexpressing your understanding of thetrainee's feelings; (c) if appropriate,responding that the trainee's view is aviable alternative; (d) presenting yourown view in greater detail with bothsupporting reasons and probableoutcomes; (e) expressing the appro-priateness of delaying a resolution ofthe trainee-trainer difference; and (f)urging the trainee to tentatively try toparticipate.
2. Reinstruct and simplify. Thisapproach may be implemented in oneor more of the following ways: (a)Have the trainee follow one behavior-al step, rather than a series of steps.(b) Have the trainee play a passive(co-actor or nonspeaking) role in therole play prior to playing the role ofthe main actor. (c) Cut the role playshort. (d) Instruct the trainee in whatto say in the role play (either prior tothe role play or in a coaching fashionduring the role play). (e) Reinforcethe trainee for improvement overprior performance rather than havinghim/her live up to standards set forother members.
3. Reduce threat. For trainees whofind some aspect of the StructuredLearning session threatening oranxiety-producing, we recommend aseries of procedures designed to helpthe trainee calm down sufficiently sothat he/she can attend to the task athand. Some threat reduction methodsinclude: (a) Have one of the trainers

model a particular task before askingthe threatened trainee to try the task.(b) Reassure the trainee with remarkssuch as "Take your time," "I knowit's hard," or "Give it a try and I'llhelp you through it." (c) Clarify anyaspects of the trainee's task which arestill unclear.
4. Elicit responses. This set ofmethods is called for in cases wherethe group is being unresponsive toefforts to get trainees involved. Someelicitation methods include: (a) Callfor volunteers. (b) Introduce topicsfor discussion. (c) Ask a specifictrainee to participate, preferablysomeone who has shown some signsof interest or attention (i.e., eyecontact, gesture).
5. Terminate responses. Finally, urgetrainers to take a direct stand insituations which divert the attentionof the group from the task at hand.Some termination methods include:(a) Interrupt ongoing behavior. (b)Extinguish through inattention totrainee behavior. (c) Cease interactionwith resistive trainee and ask othersto participate. (d) Urge trainees to getback on the correct topic.
RESEARCH EVALUATION
Starting in 1970, our research grouphas conducted a systematic researchprogram oriented toward evaluatingand improving the effectiveness ofStructured Learning. Approximately50 investigations have been con-ducted involving a wide variety oftrainee populations. These includechronic adult schizophrenics (Gold-stein, 1973; Goldstein, Sprafkin &Gershaw, 1976, 1979; Liberman,1970; Orenstein, 1969; Sutton-Simon, 1974), geriatric patients(Lopez, 1977; Lopez, Hoyer, Gold-stein, Gershaw, & Sprafkin, 1980),child abusing parents (Solomon,1977; Sturm, 1980), young children(Hummel, 1980; Swanstrom, 1974),such change-agent trainees as mental
hospital staff (Berlin, 1974; Gold-stein & Goodhart, 1973; Lack, 1975;Robinson, 1973; Schneiman, 1972),police (Goldstein, Monti, Sardino, &Green, 1979), persons employed inindustrial contexts (Goldstein &Sorcher, 1973, 1974), and in recentyears aggressive and other behavior-ally disordered adolescents (Gold-stein, Sprafkin, Gershaw, & Klein,1979,1980; Greenleaf, 1980;Litwack, 1976; Trief, 1976; Wood,1977).
With regard to adolescent trainees,Structured Learning has beensuccessful in enhancing suchprosocial skills as empathy, negotia-tion, assertiveness, following instruc-tions, self-control, and perspectivetaking. Beyond these initial demon-strations that Structured Learningworks with youngsters, these begin-ning studies have also highlightedother aspects of the teaching ofprosocial behaviors. Fleming (1976),in an effort to capitalize uponadolescent responsiveness to peerinfluence, demonstrated that gains innegotiating skill are as great when theStructured Learning group leader is arespected peer as when the leader isan adult. Litwack (1976), moreconcerned with the skill-enhancingeffects of an adolescent anticipatingthat he will later serve as a peerleader, showed that such helper roleexpectation increases the degree ofskill acquired. Apparently, when theadolescent expects to teach others askill, his own level of skill acquisi-tion benefits, a finding clearlyrelevant to Reissman's helper therapyprinciple (1965). Trief (1976)demonstrated that successful use ofStructured Learning to increase theperspective-taking skill (i.e., seeingmatters from other people's view-point) also leads to consequentincreases in cooperative behavior.The significant transfer effects bothin this study and in the Golden(1975), Litwack (1976), and Raleigh(1977) investigations have been
1./
Structured Learning has beensuccessful in enhancing
prosocial skills with adolescent
students.
11111111111111111111111111111
CCBD Retrospective Series / 53Immemonwammr

Aggression-prone adolescentsoften get into difficulty whenthey respond with overtaggression to authority figureswith whom they disagree.
11111111M11111111111111111111111
40'
54 / CCBD Retrospective Series
important signposts in planningfurther research on transfer enhance-ment in Structured Learning.
As in earlier efforts with adulttrainees, the value of teaching certainskill combinations has begun to beexamined. Aggression-prone adoles-cents often get into difficulty whenthey respond with overt aggression toauthority figures with whom theydisagree. Golden (1975), respondingto this type of event, successfullyused Structured Learning to teachsuch youngsters resistance-reducingbehavior, defined as a combination ofreflection of feeling (the authorityfigure's) and assertiveness (forthrightbut nonaggressive statement of one'sown position). Jennings (1975) wasable to use Structured Learningsuccessfully to train adolescents inseveral of the verbal skills necessaryfor satisfactory participation in moretraditional, insight-oriented psycho-therapy. And Guzzetta (1974) wassuccessful in providing means to helpclose the gap between adolescentsand their parents by using StructuredLearning to teach empathic skills toparents.
The overall conclusions which mayjustifiably be drawn from theseseveral empirical evaluations of ourwork with adolescent as well as othertrainees are threefold.
1. Skill acquisition Across diversetrainee populatio (clearly includingaggressive adolescents in urbansecondary schools and juveniledetention centers) and target skills,skill acquisition is a reliable trainingoutcome, occurring in well over 90%of Structured Learning trainees.While pleased with this outcome, weare acutely aware of the manner inwhich therapeutic gains demonstrablein the training context are rathereasily accomplishedgiven thepotency, support, encouragement, andlow-threat value of trainers andtherapists in that contextbut that
the more consequential outcomequestion by far pertains to traineeskill performance in real-worldcontexts (i.e., skill transfer).
2. Skill transfer. Across diversetrainee populations, target skills, andapplied (real-world) settings, skilltransfer occurs with approximately50% of Structured Learning trainees.Goldstein and Kanfer (1979) as wellas Karoly and Steffen (1980) haveindicated that across several dozentypes of psychotherapy involvingmany different types of psychopathol-ogy, the average transfer rate onfollow-up is between 15% and 20%of patients seen. The 50% rateconsequent to Structured Learning isa significant improvement upon thiscollective base rate, though it mustimmediately be underscored that thiscumulative average transfer findingalso means that the gains shown byhalf of our trainees were limited toinsession acquisition. Of specialconsequence, however, is the consis-tently cleat manner in which skilltransfer in our studies was a functionof the explicit implementation oflaboratory derived transfer-enhancingtechniques, such as those describedearlier in this article.
3. Prescriptiveness. A prescriptiveresearch strategy is, at heart, an effortto conceptualize, operationalize,andevaluate potentially optima: trainer xtrainee x training method matches.Prior to constituting such combina-tions, trainer, trainee, and trainingcharacteristics which may be activecontributors to such matches must beexamined singly and in combination.Stated otherwise, active and inertcontributors to skill acquisition andtransfer must be identified. A smalland continuing series of multipleregression investigations conductedby us have begun to point to state,trait, cognitive, demographic, andsociometric predictors of high levelsof skill acquisition and transfer(Anderson, 1981; Hoyer, Lopez, &

Goldstein, 1982). More such pre-scriptive ingredients research seemsworthy of pursuit.
REFERENCESAgras, W. S. (1967). Transfer during
systematic desensitization therapy.Behavior Research and Therapy, 5,193-199.
Anderson, L (1981). Role playing abilityand young children: The prescriptivequestion. Unpublished masters thesis,Syracuse University.
Authier, J., Gustafson, K., Guerney, B. G.,Jr., & Kasdorf, J. A. (1975). Thepsychological practitioner as teacher.The Counseling Psychologist, 5, 1-21.
Berlin, R. J. (1974). Training of hospitalstaff in accurate effective perceptionfear-anxiety from vocal cues in thecontext of varying facial cues.Unpublished masters thesis, SyracuseUniversity.
Callantine, M. E, & Warren, J. M. (1955).Learning sets in human conceptformation. Psychological Reports, 1,363-367.
Cartledge, G., & Milburn, J. (1978). Thecase for teaching social skills inclassroom: A review. Review ofEducational Research, 48(11), 133-156.
Cartledge, G., & Milburn, J. (1980).Teaching social skills to children. NewYork: Pergamon Press.
Chapman, W. E. (1977). Roots ofcharacter education. Schenectady, NY:Character Research Press.
Dewey, J. (1938). Experience andEducation. New York: Collier.
Dun..:an, C. E (1959). Recent research onhuman problem solving. PsychologicalBulletin, 56, 397-429.
Ellis, H. (1965). The transfer of learning.New York: Macmillan.
Fleming, D. (1976). Teaching negotiationskills to pre-adolescents. Unpublisheddoctoral dissertation, SyracuseUniversity.
Golden, R. (1975). Teaching resistance-reducing behavior to high schoolstudents. Unpublished doctoraldissertation, Syracuse University.
Goldstein, A. P (1973). Structuredlearning therapy. Toward a psycho-therapy for the poor New York:Academic Press.
Goldstein, A. P (1981). Psychological
skill training. New York: PergamonPress.
Goldstein, A. P. & Goedhart, A. (1973).The use of structured learning forempathy-enhancement in paraprofes-sional psychotherapist training.Journal of Community Psychology, 1,168-173.
Goldstein, A. P, and Kanfer, F. (Eds.).(1979). Maximizing treatment gains.New York: Academic Press.
Goldstein, A. P, Monti, P J., Sardino, T.J., & Green, D. J. (1979). Police crisisintervention. New York: PergamonPress.
Goldstein, A. P, & Sorcher, M. (1973,March). Changing managerialbehavior by applied learningtechniques. Training & DevelopmentJournal, 36-39.
Goldstein, A. P, & Sorcher, M. (1974).Changing supervisor behavior. NewYork: Pergamon Press.
Goldstein, A. P, Sprafkin, R. P, &Gershaw, N. J. (1976). Skill trainingfor community living. New York:Pergamon Press.
Goldstein, A. P. Sprafkin, R. P. &Gershaw, NJ. (1979). I know what'swrong, but I don't know what to doabout it. Englewood Cliffs, NJ:Spectrum.
Goldstein, A. P., Spralkin, R. P., Gershaw,N. J., & Klein, P (1979). Skillstreaming the adolescent. Urbana, IL:Research Press.
Goldstein, A. P, Sprafkin, R. P, Gershaw,N. J., & Klein, P (1980). Structuredlearning and the skill deficientadolescent. In G. Carteledge & J.Milburn (Eds.), Teaching social skills tochildren. New York: Pergamon Press.
Goldstein, A. P. & Stein, N. (1976).Prescriptive psychotherapies. NewYork: Pergamon Press.
Greenleaf, D. (1977). Peer reinforcementas transfer enhancement in structuredlearning therapy. Unpublishedmasters thesis, Syracuse University.
Gruber, R. P (1971). Behavior therapy:Problems in generalization. BehaviorTherapy, 2, 361-368.
Gutride, M. E., Goldstein, A. P, &Hunter, G. F. (1973), The use ofmodeling and role playing to increasesocial interaction among asocialpsychiatric patients. Journal ofConsulting and Clinical Ps)chology,40, 408-415.
Guzzetta, R. A. (1974). Acquisition and
CCBD Retrospective Series / 55

transfer of empathy by the parents ofearly adolescents through structuredlearning training. Unpublisheddoctoral dissertation, SyracuseUniversity.
Hoye; W. J., Lopez, M., & Goldstein, A.P (1982). Predicting social skillacquisition and transfer by psycho-geriatric inpatients. InternationalJournal of Behavioral Geriatrics, .1,43-46.
Hummel, J. W. (1980). An examination ofstructured learning therapy, self-control, negotiazions training, andvariations in stimulus conditions.Unpublished doctoral dissertation,Syracuse University.
Jennings, R. L. (1975). The use ofstructured learning techniques to teachattraction enhancing interviewee skillsto residentially hospitalized Inwersocioeconomic, emotionally disturbedchildren and adolescents: A psycho-therapy analogue investigation.Unpublished doctoral dissertation,University of Iowa.
Karoly, P, & Steffen, J. J. (Eds.). (1980).Improving the long-term effects ofpsychotherapy. New York: GardnerPress.
Kazdin, A. E. (1975). Behavior modifica-tion in applied settings. Homewood,IL: Dorsey Press.
Keeley, S. M., Shemberg, K. M., &Carbonell, J. (1976). Operant clinicalintervention: Behavior management orbeyond? Behavior Therapy, 7, 292-305.
Kohlherg, L. (1973). Collected papers onmoral development and moraleducation. Cambridge, MA: HarvardGraduate School of Education.
Lack, D. Z. (1975). Problem-solvingtraining, structared learning training,and didactic instruction in thepreparation of paraprofessional menialhealth personnel for the utilization ofconiingency managerneni techniques.Unpublished doctoral dissertation,Syracuse University.
Larsen, D. (in press). Giving psychologyaway. San Francisco: Brooks Cole.
Liberman, B. (1970). The effect ofmodeling procedures on attraction anddisclosure in a psychotherapyanalogue. Unpublished doctoraldissertation, Syracuse University.
Litwack, S. E. (1977). The use of thehelper therapy principle to increasetherapeutic effectiveness and reducetherapeutic resistance: Structured
56 / CCBD Retrospective Seriesminiiimommommommmi
learning therapy with resistantadolescents. Unpublished doctoraldissertation, Syracuse Universit.,.
Lopez, M. (1977). The effects of over-learning and prestructuring instructured learning therapy withgeriatric patients. Unpublisheddoctoral dissertation, SyracuseUniversity.
Lopez, M. A., Hoyer, W. J., Goldstein, A.P, Gershaw, N. J., & Sprafkin, R. P(1980). Effects of overleaming andincentive on the acquisition andtransfer of interpersonal skills withinstitutionalized elderly, Journal ofGerontology, 35(3), 403-408.
Marholin, D., Siegel, L. J., & Phillips, D.(1976). Treatment and transfer Asearch for empirical procedures. InM. Hersen, R. M. Eisler, & P M.Miller (Eds.), Progress in behaviormodification (Vol. 3). New York:Academic Press.
Miller, J. P (1976). Humanizing theclassroom. New York: Praeger.
Orenstein, R. (1969). The influence ofself-esteem on mokkling behavior in apsychotherapy analogue. Unpublishedmasters thesis, Syracuse University.
Osgood, C. E. (1953). Method and theoryin experimental psychology. New York:Oxford University Press.
Patterson, G. R., & Gullion, M. E.(1972). Living with children.Champaign, IL: Research Press.
Raleigh, R. (1977). Individual vs. group-structured learning therapy forassertiveness training with senior andjunior high school students. Unpub-lished doctoral dissertation, SyracuseUniversity.
Rathjen, D., & Foreyt, J. (1980). Socialcompetence: Intervention for childrenand adults. New York: PergamonPress.
Reissman, F. (1965). The culturallydeprived child. New York: Harper.
Robinson, R. (1973). Evaluation of astructured learning empathy trainingprogram for lower socioeconomicstatus hcme-aide trainees. Unpub-lished masters thesis, SyracuseUniversity.
Schneiman, R. (1972). An evaluation ofstructured learning and didacticlearning as methods of trainingbehaviormodification skills to lowerand middle socioeconomic levelteacher-aides. Unpublished doctoraldissertation, Syracuse University.
1

Shore, E., & Sechrest, L. (1961).Concept attainment as a function ofnumber of positive instancespresented. Journal of EducationalPsychology, 52, 303-307.
Simon, S. B., Howe, L W, & Kirschen-baum, H. (1972). Values clarification.New York: Hart.
Solomon, E. (1978). Structured learningtherapy with abusive parents:Training in self-control. Unpublisheddoctoral dissertation, SyracuseUniversity.
Swanstron, C. (1974). Training self-control in behavior problem children.Unpublished doctoral disserultion,Syracuse University.
Sturm, D. (1980). Therapist aggressiontolerance and dependency toleranceunder standardized client conditionsof hostility and dependency.Unpub-
lished masters thesis, SyracuseUniversity.
Tharp, R. G., & Wetzel, R. (1969).Behavior modification in the naturalenvironment. New York: Academic
Press.Thorndike, E. L., & Woodworth, R. S.
(1901). The influence of improvementin one mental function upon theefficiency of other functions. Psycho-
logical Review, 8, 247-261.
Trief, P (1976). The reduction ofegocentrism in acting-ow adolescentsby structured learning therapy.Unpublished doctoral dissertation,Syracuse University.
Weinstein, G., & Fantini, M. D. (1970).Toward humanizing education: A
curriculum of affect. New York:
Praeger.Wood, M. (1977). Adolescent acquisition
and transfer of assertiveness throughthe use of structured learning therapy.Unpublished doctoral dissertation,Syracuse University.
-
CCBD Retrospective Series / 57lisommmmmie

Use of Cognitive MediationStrategies for Social Skills Training:Theoretical and Conceptual Issues
John W. Maag
ABSTRACT Social skills training curricula have been used to teach appropri-ate social interaction to behaviorally disordered youth. Concomitantly, cogni-
tive interventions such as self-management training have been advocated forenhancing generalization and maintenance of treatment effects. The purposeof this article is to discuss the benefits of incorporating cognitive mediationstrategies into social skills training interventions. Cognitive mediation tech-niques are described and relevant literature reviewed. Issues related to treat-ment implementation of cognitive mediation strategies for social skills train-
ing are discussed.
Development of social skills training procedures have burgeoned duringthe past decade. Standardized empirically-based curricula and materialsare readily available to clinicians and educators (cf. McConnell, 1987).Despite advances in applied social skills technology, prospects for gener-alization and maintenance of trained social skills remain dismal (Schloss,Schloss, Wood, & Kiehl, 1986). While considerable information exists forprogramming generalization (e.g., Stokes & Baer, 1977), and while it isdiscussed by authors of social skills training curricula (e.g., Goldstein,Sprafkin, Gershaw, & Klein, 1980; Walker et al., 1983), seldom aregeneralization procedures systematically incorporated into social skillstreatment efficacy studies (Schloss et al., 1986).
Stokes and Osnes (1986, 1988) recently described 11 tactics for promot-ing the successful programming of generalization. These tactics may be
roughly classified into two general categories: environmental manipulationand cognitive mediation (Maag, in press). Environmental manipulationtechniques such as the use of multiple peer exemplars, structuringinteraction with significant others, integrating training into naturalenvironments (Shores, 1987), and in particular, promoting entrapmenteffects (McConnell, 1987) have been proffered as efficient generalizationenhancers. Unfortunately, several methodological problems limit theefficacy of solely relying on enVironmental manipulation techniques for
promoting generalization of social skills. The concept of entrapmentprovides an excellent example of two of these drawbacks.
Reprinted from Monograph in
Behavioral Disorders, Volume 12,
Summer 1989, pp. 87-100ENI
CCBD Retrospective Series / 59

In order for entrapment to
occur, the student's trainedsocial skill(s) must be
reinforced by their peers andvice-versa, therebyperpetuating positive reciprocalinteraction.
111111111111111111MINIIMINIIIIIIMINM111111111111
60 / CCBD Retrospective Series
Entrapment refers to a bidirectionalreciprocal process whereby newlyacquired behaviors are maintained bynaturally occurring communities ofsocial reinforcers (McConnell, 1987).It reflects a shift in stimulus controlfrom training to generalizationsettings. In order for entrapment tooccur, the student's trained socialskill(s) must be reinforced by theirpeers and vice-versa, therebyperpetuating positive reciprocalinteraction. Unfortunately, it isunlikely that appropriate socialresponses always can come under thecontrol of naturally occurringreinforcers. There are many instanceswhen appropriate behaviors are notreinforced by others. For example,employers often fail to praiseemployees for exemplary work, orstudents exhibiting appropriate groupentry skills frequently are shunnedby their peers. More problematic hasbeen indications that even whenrejected students engage in prosocialbehaviors, they continue to berejected by their peers (Bierman &Furman, 1984; Bierman, Miller, &Stabb, 1987). The elusive goal ofimproved peer acceptance followingsocial skills training threatens thetheoretical underpinnings of entrap-ment for promoting generalization. Itis unlikely that reciprocity ofreinforcement will occur if a stu-dent's peer group continues to dislikehim or her after demonstratingimproved social skills.
Despite the success of operantprocedures for teaching social skills,several researchers have advocatedthe use of cognitive mediationstrategies for promoting generaliza-tion because of their reduced relianceupon environmental contingencies tomaintain behaviors in nontreatmentsettings (e.g., Gross & Drabman,1982; Kanfer & Karoly, 1982;Kendall & Braswell, 1982). Cognitivemediation represents a fairly newarea of social skills training researchwhen compared to the attention
6 ,1
environmental manipulation strate-gies receive (Simpson, 1987). Current-ly, there is a need to systematicallyinvestigate the differential efficacy ofcognitive mediation strategies forsocial skills training interventions(Meador & 011endick. 1984).
The purpose of this article is todiscuss the benefits of cognitivemediation strategies for social skillstraining interventions. Severalcognitive mediation strategies will bedescribed and relevant researchdiscussed for (a) self-instructiontraining, (b) self-managementtraining, (c) problem-solving training,(d) attribution retraining, and (e)relaxation training. Issues related totreatment implementation arediscussed. This article is intended topresent a theoretical and conceptualframework for future research andapplication of cognitive mediationstrategies for social skills training.
COGNITIVE MEDIATIONSTRATEGIES
Cognitive mediation strategistsattempt to place the responsibility forchange or skill acquisition/produc-tion on the individual. The self-regulatory nature of cognitivemediation has resulted in mainte-nance and generalization of behaviorchange in some students exhibitingmaladaptive behavior (e.g., Kendall& Braswell, 1982; Lochman &Lampron, 1988). Although method-ological deficiencies using cognitivemediation strategies with childrenhave been noted on such variables assubject selection, adequacy ofoutcome measures, and experimentaland statistical methodology (Hobbs,Moguin, Tyroler, & Lahey, 1980), agrowing number of researchersreported promising results that meritfurther investigation. However, twotheoretical issues should be ad-dressed which have proceduralimplications for api)lication of thesetreatment techniques.

First, practitioners should take intoconsideration the similarity andoverlap among many cognitivemediation strategies. All cognitivemediation techniques involve self-instruction or private speech. Forexample, individuals engage in self-instruction or private speech whenself-monitoring, self-evaluating, andadministering self-reinforcement/punishment by deciding when andwhat behavior they should emit, if thebehavior is performed appropriately,and what type of self-reinforcement/punishment they deserve. Similarly,in order to employ relaxation train-ing, individuals must use self-instructions for determining situa-tions that require the relaxationresponse and for performing theresponse correctly. Problem-solvingtraining probably represents the mostinclusive and systematic use of self-instructions. Braswell and Kendall(1988) suggested that a problem-solving approach to behavioral orinterpersonal dilemmas representsthe general orientation of cognitive-behavioral interventions.
Second, it is important for practitio-ners to preserve an environmental/behavioral view of treatment. Socialinteraction requires individuals tofunction within the social context(Kendall, 1985). This view is reflectedby the importance given to structuringenvironmental conditions (e.g.,entrapment) to promote generalizedsocial interaction skills (Gaylord-Ross & Haring, 1987). As promisingas environmental manipulationtechniques appear, it is not possiblenor desirable to structure all socialcontexts to become conducive forsocial reciprocity occurring. However,individuals can be taught cognitivemediation strategies to use regardlessof the social context and environmen-tal demands of a given situation.
Self-Instruction Training
Verbal mediation, private speech, andself-instruction are synonymous terms
for a person making covert or overtmediated responses when presentedwith a learning task. Teachingstudents self-instruction tactics hasbeen effective in training (a) behav-iorally disordered children toincrease attending and on-taskbehaviors (Barkley, Copeland, &Sivage, 1980; Bornstein & Quevillon,1976; Kendali & Braswell, 1982;Kendall & Wilcox, 1980; Kendall &Zupan, 1981; Morrow & Morrow,1985); (b) increasing academic skills(Bryant & Budd, 1982; Graham,1983; Harris, 1986a; Leon & Pepe,1983); and (c) increasing appropriatesocial behaviors (Burron & Bucher,1978; Kneed ler, 1980).
Host studies investigating the use ofself-instruction have used adaptationsof a training sequence developed byMeichenbaum and Goodman (1971):(a) cognitive modelingan adultmodel performs a task while talkingto himself out loud; (b) overt,external guidancethe studentperforms the same task under thedirection of the model's instructions;(c) overt, self-guidancethe studentperforms the task while instructinghimself aloud; (d) faded, overt self-guidancethe student whispers theinstructions to himself while goingthrough the task; and (e) covert self-instructionthe student performs thetask while guiding his performancevia private speech (p. 32). Thismethod has been commonly referredto as the "faded rehearsal" method ofself-instruction training. A modifica-tion of this approach which hasbecome more popular in recent yearsis the "directed discovery" method.In the latter method, the trainer leadsthe student to discover specific sets ofself-guiding strategies through Socraticdialogue rather than providing thestudent with predetermined strategies(Braswell & Kendall, 1988).
Self-Management Training
Self-management training involvesthe personal application of tech-
t3
Cognitive mediation strategists
attempt to place theresponsibility for change or skillacquisition/production on the
individual.
CCBD Retrospective Series / 61

As an isolated procedure, self-evaluation has not been
particularly effective forreducing disruptive classroombehaviors nor for strengtheningappropriate behaviors.
imismommonommimmom
62 / CCBD Retrospective Serieslionormoommooloomiso
niques for individuals changing theirown behavior. Self-managementtraining usually involves self-monitoring, self-evaluation, self-determination of contingencies, andself-instruction (cf. O'Leary & Dubey,1979; Rosenbaum & Drabman,1979). The focus of this section willbe on the first three techniques asself-instruction was addressedpreviously. Although self-manage-ment training has been used forpromoting generalized behaviorchange (Baer, Holman, Stokes,Fowler, & Rowbury, 1981) andimproving academic skills (Harris &Graham, 1985), few researchers haveemployed simultaneously all fourtechniques in treatment efficacystudies. Rather, individual tech-niques have become major therapeu-tic interventions in their own right.
Se If-Monitoring. Self-monitoring hasbeen tiefined as an individual'ssystematic observation of her/his ownbehavior and recording a specifiedtarget response (Cooper, Heron, &Heward, 1987). Self-monitoring hasbeen used successfully to increasestudents' attention in the classroom(Broden, Hall, & Mitts, 1971;Kneed ler & Hallahan, 1981),decrease disruptive behaviors (Lovitt,1973; Stevenson & Fantuzzo, 1984;Sugai & Rowe, 1984), and improveacademic performance (Harris,1986b; Hundert & Bucher, 1978;James, Trap, & Cooper, 1977).
Self-monitoring can have a reactiveeffect on the target response beingself-observed, whereby the behaviorchanges as a function of the self-monitoring process (Rosenbaum &Drabman, 1979). Thus, the act ofengaging in self-observation can bean effective behavior change tech-nique. Self-monitoring has beensuggested to result in behaviorchange because it produces positiveor negative self-evaluative statementsthat serve to either reinforce desir-able behaviors or to punish undesir-
able behaviors (Cautela, 1971;Malott, 1981).
Self-Evaluation. The distinctionbetween self-monitoring and self-evaluation often is arbitrary. Forexample, if self-monitoring is toresult in behavior change, it must beaccompanied by self-evaluativestatements. However, O'Leary andO'Leary (1976) distinguishedbetween self-monitoring and self-evaluation. Although both proceduresentail self-observation, in self-monitoring behavior is monitored andrecorded with a minimum amount ofjudgment. In self-evaluation, the self-monitoring process is followed by acovert evaluation of the behavior,usually with an externally providedcriterion. Therefore, self-evaluation isa necessary component for self-monitoring to result in behaviorchange.
Several researchers attempted toisolate the effects of self-evaluationfrom self-monitoring. As an isolatedprocedure, self-evaluation has notbeen particularly effective forreducing disruptive classroombehaviors (Santogrossi, O'Leary,Romanczyk, & Kaufman, 1973;Turkewitz, O'Leary, & Ironsmith,1975) nor for strengthening appropri-ate behaviors (Layne, Rickard, Jones,& Lyman, 1976). Although somesuccess has been demonstrated withself-evaluation procedures (e.g.,Nelson, Lipinski, & Boykin, 1978;Sagotsky, Patterson, & Lepper, 1978),O'Leary and Dubey (1979) suggestedtheir effectiveness may be increasedwhen used in combination with self-monitoring and reinforcement.
Self-ReinforcementIPunishmeru. Self-reinforcement/punishment involvesarranging to have one's own behaviorreceive specified consequencesaccording to self-planned contingen-cies of reinforcement and/or punish-ment (Cooper et al., 1987). It isdifficult to evaluate effects of self-

reinforcement procedures because ofthe confounding of self-monitoring,which is a necessary prerequisite toself-reinforcement. However, Mastersand Santrock (1976) successfullyisolated self-administered reinforce-ment from both self-monitoring andself-evaluation. Children who aretaught to verbalize pride in their workdemonstrated significantly greatertask persistence than when they weretold to utter neutral statements.Similarly, Ballard and Glynn (1975)found that while self-monitoring hadno effect upon students' classroomwriting skills, the sequential additionof self-reinforcement increased theaccuracy and amount of writingskills.
Less research has been conducted onthe effect of self-administeredpunishment. Self-determinedresponse cost procedures have beenused effectively for increasingstudents' social behavior (Kaufman &O'Leary, 1972) and academic work(Humphrey, Karoly, & Kirschen-baum, 1978). Contingent self-determined snaps of a rubberband(Mastellone, 1974) and timeout(James, 1981) have been usedsuccessfully to treat problematicbehaviors. However, there is a cleartrend for researchers and practitio-ners preferring to instruct youngstersin the use of self-reinforcement.
Problem-Solving Training
Problem-solving training represents aform of self-instruction for systemati-cally approaching, evaluating, andsolving interpersonal dilemmas(Braswell & Kendall, 1988). Itdepicts the general orientation ofcognitive-behavioral methodology.Problem-solving interventions havebeen applied extensively withbehaviorally disordered youngsters,For instance, Robin, Schneider, andDolnick (1976) taught emotionallydisturbed students to generatealternative solutions and examinetheir consequences to inhibit
aggression and impulsivity in socialsituations. Amish, Gesten, Smith,Clark, and Stark (1988) trainedbehaviorally disordered children togenerate significantly more alterna-tive solutions to interpersonalproblems than those generated by acontrol group of children. Problem-solving training also has been usedsuccessfully with delinquent andpredelinquent adolescents (Sarason& Ganzer, 1973; Sarason & Sarason,1981).
Lochman and colleagues developedan interpersonal cognitive problem-solving intervention for use withaggressive boys (cf. Loahman,Nelson, & Sims, 1981). Lochman,Burch, Curry, and Lampron (1984)and Lochman and Curry (1986)found that this problem-solvingintervention plus a goal settingcondition resulted in reductions inoff-task passive behaviors, disrup-tion, and aggression in the boys'classroom. Parent ratings of theirchild's aggression indicated somegeneralization of treatment effects tothe home setting. Lochman andLampron (1988) found that improve..ments in classroom behavior foraggressive boys receiving problem-solving training were maintained at a7-month follow-up.
D'Zurilla (1988) suggested that socialskills training programs shouldinclude training in problem-solvingskills in order to enhance generaliza-tion of interpersonal skills. D'Zurilla(1986) described a five-componentmodel for solving problems: (a)problem orientation, (b) problemdefinition and formulation, (c)generation of alternative solutions, (d)decision making, and (e) solutionimplementation and verification. Interms of clinical applications withchildren, Fisch ler and Kendall(1988) suggested that trainingprograms should emphasize modelingand reinforcement of appropriateproblem-solving strategies.
Problem-solving training
represents a form of self-
instruction for systematicallyapproaching, evaluating, and
solving interpersonal dilemmasand has been appliedextensively with youngsters
with behavioral disorders.
CCBD Retrospective Series / 63

The role of strategy selection isgermane to the production ofsocial skills.
1111111111111111111111111111111111=1
64 / CCBD Retrospective Series
Attribution Retraining
Attribution retraining arose from theviewpoint that children's causalexplanations for why they are doingwell or poorly has implications fortheir behavioral persistence, expect-ancies for future performance, andaffective reactions to success andfailure (Braswell & Kendall, 1988).Attribution retraining attempts toincrease children's behavioralpersistence on a task through use ofeffort-oriented statements. Forexample, Dweck (1975) found thatwhen children who had difficultysolving math problems were in-structed to tell themselves that"failure means you should tryharder," they persisted longer on theproblems than children in a success-only condition in which mathproblems were presented that werewithin their ability and that wouldensure success.
Attributional beliefs also may affectstudents use of strategic behavior(Borkowski, Weyhing, & Turner,1986). The role of strategy selectionis germane to the production of socialskills. Social skill deficits often canbe traced to the inability of studentsto assemble and sequence subtasksinto task strategies for successfulperformance (Harris, 1988; Howell,1985). Kurtz and Borkowski (1984)found students who attributed successto effort were more likely to applystrategic behavior than students whoattributed success to external factors.It appears likely that many motiva-tional deficits in social skill knowl-edge and subsequent performance arelinked to negative attributional states.
Before implementing attributionalretraining for social skills training,two factors need to be considered.First, Pearl (1985) suggested that inorder to be effective, attributionalstatements should he accompaniedwith sperific behavioral efforts. ibrexample, Short and Ryan (1984)
found that attribution retraining wasineffective when students madeeffort-oriented statements prior toreading a passage rather than afterhaving had difficulty with thepassage. Second, Schunk (1983)suggested that attribution retrainingis likely to be most successful withchildren who are not using the skillsthey possess. This approach wouldnot be appropriate, for example, withchildren whose maladaptive behavioris due to specific skill deficits(Fincham, 1983).
Relaxation Training
Relaxation training techniques aredesigned to relieve distress and fosteremotion-regulation (Meichenbaum,1985). Emotion-regulation andcognitive mediation have beenconsidered interrelated and insepa-rable concepts (Kendall, 1985;Santostefano & Reider, 1984).Progressive muscle relaxation hasbeen the most widely used relaxationtraining technique with children.Muscle relaxation training has beenused successfully to decreasedisruptions and aggression andincrease social skills and academicperformance with behaviorallydisordered, learning disabled, andmentally retarded students (Carter &Russell, 1980; Fejes & Prieto,1987; Marholin, Steinman, Luise lli,Schwartz, & Townsend, 1979;Omizo, 1980; Robin et al., 1976;Walton, 1979).
Muscle relaxation generally involveshaving students tense and relaxmuscle parts of their bodies whilefocusing on how pleasant specificparts of the body feel when relaxed(cf. Jacobsen, 1938). This procedureis repeated with arms, legs, feet,hands, face, and stomach. Afterrelaxation responses are practicedseparately, they are incorporated intoone motion. The whole body is tensedfor a count of from one to 10 and thenquickly relaxed.
6 L-)
BEST COPY AVAILABLE

Maag (1988a) suggested that progres-sive muscle relaxation provides ameans for students to cope withsituation-induced stress that other-wise may interfere with production of'newly acquired social skills. In someinstances, acquisition of social skillsis mediated by the use of relaxation(Vallis, 1984). Practicing relaxationfor social skills training is particular-ly germane when stressful or aversivesituations can be neither altered noravoided (Meichenbaum, 1985).Amerikaner and Summer lin (1982)found that teacher ratings of theacting out and distractibility oflearning disabled students whoreceived relaxation training werelower than for students who receivedsocial skills training. While thisresult should not be interpreted assupport for the superiority of relax-ation training over social skillstraining, it does point out theimportance relaxation training playsin the amelioration of skill deficits.
THEORETICAL ANDCONCEPTUAL TRAININGISSUES
The rationale for incorporatingcognitive mediation strategies intosocial skills training interventionslargely evolvA from Bandura's sociallearning theory. In particular, hisresearch on modeling demonstratedthat behavior is acquired throughmediating influences of symboliccoding, cognitive organization,symbolic rehearsal, and motorrehearsal of information (Bandura,1977, 1978). According to Bandura'sconceptualization, environmentalinfluences are "mediated" bycognitive processes. That is, aperson's anticipation of reinforcingconsequences (antecedent control)has a greater impact upon behavioralperformance than the consequenceson any particular response (conse-(1uent control; Gresham & Lemanek,1983).
The strategies reviewed in this articlefocused upon the role of cognitivemediation in the acquisition andproduction of social skills. Althoughseveral researchers acknowledged therole of cognitive mediation forlearning social skills (e.g., Craig-head, 1982; Kazdin, 1982; Kendall& Braswell, 1982), few have system-atically evaluated the efficacy ofthese strategies on actual perfor-mance of social skills. In fact,Gresham (1985) noted that whileself-instruction and social problem-solving, for example, may representeffective social skills trainingstrategies, little research has beenconducted to demonstrate theireffectiveness. Part of the difficulty inassessing efficacy of these strategiesfor social skills training is theabsence of a comprehensive formatfor delivering training, inattention toconduct functional assessment, andinadequate implementation of tacticsfor promoting generalization. Each ofthese issues is discussed brieflywithin the context of cognitivemediation for social skills training.
Developing a ConceptualModel
The efficacy of cognitive mediationstrategies for social skills training isinterrelated to the conceptual modelused to deliver treatment. Althoughthere is an abundance of social skillstraining interventions (e.g., McConnell,1987), Schloss et al. (1986) lamentedthat lack of a conceptual model fordelivering training severely limits theability to assess treatment efficacy.Having a structured training model isespecially important for incorporatingcognitive mediation strategies intosocial skills training programs. There isoften an arbitrary distinction betweenbehavioral and cognitive orientations.For instance, many cognitively-basedstrategies share behavioral methodologysuch as modeling, rehearsal, roleplaying, and instruction (Gresham,1985; Maag, 1989).
Research on modeling hasdemonstrated that behavior is
acquired through mediatinginfluences of symbolic coding,
cognitive organization,symbolic rehearsal, and motorrehearsal of information.
CCBD Retrospective Series / 65ormio

The multiplicity of social skillstraining techniques confoundsthe prospects forsystematically delivering
intervention in the absence ofa structured conceptual model.
nommilmoloroo
66 / CCBD Retrospective Series111111111111111111111111111MIN
The multiplicity of social skillstraining techniques confounds theprospects for systematically deliver-ing intervention in the absence of astructured conceptual model. Thecomplexity and multifaceted nature ofcurrent social skills training pro-grams is exemplified by Goldstein's(1988) PREPARE social curriculum.PREPARE includes ten coursesencompassing a wide variety ofbehavioral and cognitive procedures:(a) interpersonal skills training; (b)anger control training; (c) moralreasoning training; (d) problem-solving training; (e) empathy train-ing; (f) social perception training; (g)anxiety management; (h) cooperationtraining; (i) building a prosocialsupport group; and (j) understandingand using group processes. The firstseven course offerings fall under therubric of "cognitive" or "cognitive-behavioral" interventions.
This PREPARE curriculum repre-sents diverse intervention strate-gieseach postulating slightlydifferent theoretical orientations.Determining which technique(s) toemploy first requires considerableskill conducting sophisticatedmulticomponent pretreatmentassessment (Maag, in press). Assum-ing assessment yielded informationregarding the reciprocal relationshipsamong behavior, cognitions, andenvironment, implementing all or acombination of training techniqueswould be cumbersome and potentiallyoverwhelming without having aconceptual training format fromwhich to work.
A comprehensive training formatwould provide a structured system foremploying various techniques thatfall under the cognitive-behavioralrubric. One such conceptual format isoffered in the stress inoculationtraining (SIT) paradigm. SIT hasbeen used with behaviorally disor-dered youngsters to treat depression(Maag, 1988b), for aggression and
anger management (Feindler &Fremouw, 1983; Maag, Parks, &Rutherford, 1989), and to teachinterpersonal coping responses (Maaget al., 1989). Briefly, SIT consists ofthree phases: (a) conceptualization,(b) skills acquisition and rehearsal,and (c) applkation and follow-through (see Maag, 1988b, andMeichenbaum, 1985, for detaileddescription of stress inoculationtraining). SIT provides a structuredformat for assessing student andenvironmental characteristics,tailoring specific techniques toaddress assessment information, andproviding in vitro and in vivo practiceunder conditions that arouse but donot overwhelm students' copingresponses.
Functional Assessment
As interest in cognitive mediationstrategies for social skills traininggrows, the need for assessing theirdifferential efficacy also increases.Unfortunately, assessment methodol-ogy used in social skills trainingprograms has been dismal. Criticismsinclude ignoring relationshipsbetween treatment techniques andspecific subject characteristics,nonempirical methods of selectingtarget behaviors, failure to specifysituational determinants of selectedskills, and lack of using sociallyvalid assessment measures (Gresham,1985; Hughes & Sullivan, 1988;Schloss et al., 1986). All too often,students are taught to maintain eyecontact, improve body posture, orincrease question-asking withoutresearchers or practitioners firstdetermining whether students areactually deficient in these skills orwhether intervention promotessocially important outcomes such asimproved peer acceptance (Maag, inpress).
The cavalier approach to social skillsassessment often results from theneed to operationalize behavior more

precisely (Kazdin, 1985). Unfortu-nately, this practice ignores the factthat students' observed performancedeficits may be due to (a) missingrequisite behavioral skills, (b)inability to assemble and sequencesubtasks into a task strategy forsuccessful performance, (c) theselection of behaviors automaticallyrather than consciously, and (d)environmental antecedents andconsequences militating againstcompetent performance (Harris,1985, 1988; Howell & Morehead,1987; Long & Sherer, 1984).
In addition to problems in assessingindividual-specific characteristicscontributing to performance deficitsand erroneous target behaviorselection, few researchers haveassessed the differential efficacy ofspecific training componentsespecially cognitive mediationstrategies (Gresham, 1985). In orderto determine their differentialefficacy, cognitive mediation strate-gies must be selected to matchspecific student deficits as deter-mined through pretraining assess-ment. It is clear that when trainingtechniques are applied irrespective ofassessment information, treatmentefficacy is decreased (McKnight,Nelson, Hayes, & Jarrett, 1984). Theultimate benefit of cognitive media-tion strategies for social skillstraining remains theoretically sound,but thus far requires considerableresearch.
Maintenance andGeneralization
Perhaps no area of social skillstraining has generated as muchattention as promoting generalizationof behavior change. This areaprobably represents the biggestpotential contribution cognitivemediation can offer for social skillstraining. In their seminal article,Stokes and Baer (1977) discussed theneed to incorporate self-mediated
stimuli into a program for promotinggeneralization. However, therecontinues to be a lack of program-ming for generalization in socialskills training (e.g., Maag et al.,1989).
Perhaps the failure of researchers toimplement effective generalizationstrategies in social skills trainingprograms is due to the sophisticatednature of the process. Programminggeneralization requires time andpractice and should be built into anyserious social skills training programfrom its inception. Stokes and Osnes(1988) suggested that programmingfor generalization requires conductingfunctional assessment, yet relevantuse of information gathered from thisprocess often is omitted or ignored. To
increase the understanding ofgeneralization, generalization itselfneeds to be a major dependentvariable, and generalization program-ming strategies need to be indepen-dent variables (Stokes & Osnes,1988). Clearly, studying cognitivemediation strategies for social skillstraining needs to proceed on severalfronts.
SUMMARY ANDCONCLUSION
Cognitive mediation strategies havebeen proffered as a method forenhancing efficacy of social skillstraining interventions. Several ofthese strategies were reviewedincluding self-instruction training,self-management training, problem-solving training, attribution retrain-ing, and relaxation training. Althoughthese procedures have strong theoreti-cal underpinnings, few researchershave assessed their differentialefficacy for enhancing social skillstraining. Part of the difficulty hasbeen the lack of a conceptual modelfrom which to deliver treatment,inadequate or completely absentpretreatment assessment, and thelack of programming for generaliza-
tAtJeT AVAILABLE
No area of social skills training
has generated as much
attention as promotinggeneralization of behavior
change.
CCBD Retrospective Series / 67

tion. These issues must be addressedin order to substantiate the theoreti-cal précis of cognitive mediationstrategies for social skills training.
REFERENCES
Amerikaner, M., & Summer lin, M. L.(1982). Group counseling withlearning disabled children: Effects ofsocial skills and relaxation training onself-concept and classroom behavior.Journal of Learning Disabilities, 15,340-343.
Amish, P L., Cesten, E. L., Smith, J. K.,Clark, H. B., & Stark, C. (1988).Social problem-solving training forseverely emotionally and behaviorallydisturbed children. Behavioral .
Disorders, 13, 175-186.Baer, D. M., Holman, J., Stokes, T. E,
Fowler, S. A., & Rowbury, T. G.(1981). Uses of self-control tech-niques in programming generalization.In S. W. Bijou & R. Ruiz (Eds.),Behavior modification: Contributionsto education 1J3p. 39-61). Hillsdale,NJ: Lawrence Erlbaum.
Ballard, K. D., & Glynn, E. L. (1975).Behavioral self-management in story-writing with elementary schoolchildren. Journal of Applied BehaviorAnalysis, 8, 387-398.
Bandura, A. (1977). Self-efficacy: Towarda unifying theory of behavior change.Psychological Review, 84, 191-215.
Bandura, A. (1978). The self system inreciprocal determinism. AmericanPsychologist, 33, 344-358.
Barkley, R., Copeland, A., & Sivage, C.(1980). A self-control classroom forhyperactive children. Journal ofAutism and Developmental Disorders,10, 75-89.
Bierman, K. L., & Furman, W. (1984).The effects of social skills trainingand peer involvement on the socialadjustment of preadolescents. ChildDevelopment, 55, 151-162.
Bierman, K. L., Miller, C. L., & Stabb, S.D. (1987). Improving the socialbehavior and peer acceptance ofrejected boys: Effects of social skilltraining with instructions andprohibitions. Journal of Consultingand Clinical Psychology, 55, 194-200.
Borkowski, J. G., Weyhing, R. S., &Turner, 1. A. (1986). Attributionalretraining and the teaching of
68 / CCBD Retrospective Series1111111=111111111111=11111111111=
strategies. Exceptional Children,53, 130-137.
Bornstein, P H., & Quevillon, R. P(1976). The effects of a self-instruc-tional package on overactive pre-school boys. Journal of AppliedBehavior Analysis, 9, 179-188.
Braswell, L., & Kendall, P C. (1988).Cognitive-behavioral methods withchildren. In K. S. Dobson (Ed.),Handbook of cognitive-behavioraltherapies (pp. 167-213). New York:Guilford.
Braden, M., Hall, R. V., & Mitts, B.(1971). The effect of self-recording onthe classroom behavior of two eighth-grade students. Journal of AppliedBehavior Analysis, 4, 191-199.
Bryant, L. E., & Budd, K. S. (1982).Self-instructional training toincrease independent workperformance in preschoolers.Journal of Applied BehaviorAnalysis, 15, 259-271.
Burron, D., & Bucher, B. (1978). Self-instructions as discriminative cues forrule-breaking or rule-following.Journal of Experimental ChildPsychology, 26, 46-57.
Carter, J. L., & Russell, H. L. (1980).Biofeedback and academic attainmentof LD children. Academic Therapy, 15,483-486.
Cautela, J. R. (1971). Covert condition-ing. In A. Jacobs & L. B. Sachs(Eds.), The psychology of privateevents: Perspective on covert responsesystems (pp. 109-130). New York:Academic Press.
Cooper, J. 0., Heron, T. E., & Heward, W.L (1987). Applied behavior analysis.Columbus, OH: Merrill.
Craighead, W. E. (1982). A brief clinicalhistory of cognitive-behavioral therapywith children. School PsychologyReview, 11, 5-13.
Dweck, D. S. (1975). The rule ofexpectations and attributions in thealteration of learned helplessness.Journal of Personality and SocialPsychology, 25, 109-116.
D'Zurilla, T. J.,(1986). Problem-solvingtherapy: A social competence approachto clinical inlerventions. New York:Springer.
D'Zurilla, T. J. (1988). Problem-solvingtherapies. In K. S. Dobson (Ed.),Handbook of cognitive-behavioraltherapies (pp. 85-135). New York:Guilford.

Feindler, E., & Fremouw, W. (1983).Stress inoculation training foradolescent anger problems. In D.Meichenbaum & M. Jarernko (Eds.),Stress reduction and prevention (pp.451-485). New York: Plenum.
Fejes, K. E., & Prieto, A. G. (1987). Thepotential of relaxation training for thehyperkinetic trainable mentallyretarded child. Child and FamilyBehavior Therapy, 9, 55-66.
Fincham, F. D. (1983). Clinical applica-tions of attribution theory: Problemsand prospects. In M. Hewstone (Ed.),Auribution theory: Social andfunctional extensions (pp. 187-203).Oxford: Blackwells.
Fisch ler, G. L., & Kendall, P C. (1988).Social cognitive problem solving andchildhood adjustment: Qualitative andtopological analyses. CognitiveTherapy and Research, 12, 133-153.
Gaylord-Ross, R., & Haring, T. (1987).Social interaction research foradolescents with severe handicaps.Behavioral Disorders, 12, 264-275.
Goldstein, A. P (1988). PREPARE: Aprosocial curriculum for aggressiveyouth. In R. B. Rutherford, Jr., C. M.Nelson, & S. R. Fontess (Eds.), Basesof severe behavior disorders in childrenand youth (pp. 119-142). San Diego,CA: College-Hill.
Goldstein, A. P, Sprafkin, R. P, Gershaw,N. J., & Klein, P (1980). Skillstreaming the adolescent: A structuredlearning approach to teachingprosocial skills. Champaign, IL:Research Press.
Graham, S. (1983). The effect of self-instructional procedures 'on LDstudents' handwriting performance.Learning Disability Quarterly, 6, 231-234.
Gresham, F. M. (1985). Utility ofcognitive-behavioral procedures forsocial skill straining with children: Acritical review. Journal of AbnormalChild Psychology, 13, 411-423.
Gresham, F. M., & Lemanek, K. L.(1983). Social skills: A review ofcognitive-behavioral trainingprocedures with children. Journal ofApplied Developmental Psychology, 4,239-261.
Gross, A. M., & Drabman, R. S. (1982).Teaching self-recording, self-evaluation, and self-reward tononclinic children and adolescents. InP Karoly & F. N. Kanfer (Eds.), Self-
management and behavior change;From theory to practice (pp. 285-314).New York: Pergamon.
Harris, K. R. (1985). Conceptual,methodological, and clinical issues incognitive-behavioral assessment.Journal of Abnormal Child Psychol-ogy, 13, 373-390.
Harris, K. R. (1986a). The effects ofcognitive-behavior modification onprivate speech and task performanceduring problem solving among learningdisabled and normally achievingchildren. Journal of Abnonnal ChildPsychology, 14, 63-67.
Harris, K. R. (19866). Self-monitoring ofattentional behavior versus self-monitoring of productivity: Effects onon-task behavior and academicresponse rate among learning disabledchildren. Journal of Applied BehaviorAnalysis, 19, 417-423.
Harris, K. R. (1988). Cognitive-behaviormodification: Application withexceptional students. In E. L. Meyen,G. A. Vergason, & R. J. Whelan(Eds.), Effective instructionalstrategies for exceptional children (pp.216-242). Denver: Love.
Harris, K. R., & Graham, S. (1985).Improving learning disabled students'composition skills: Self-controlstrategy training. Learning DisabilitiesQuarterly, 8, 27-36.
Hobbs, S. A., Moguin, L. E., Tyroler, M.,& Lahey, B. B. (1980). Cognitivebehavior therapy with children: Hasclinical utility been demonstrated?Psychological Bulletin, 87, 147-165.
Howell, K. W. (1985). A task-analyticapproach to social behavior. Remedialand Special Education, 6, 24-30.
Howell, K. W., & Morehead, M. K.(1987). Curriculum-based evaluationfor special and remedial education.Columbus, OH: Merrill.
Hughes, J. S., & Sullivan, K. A. (1988).Outcome assessment in social skillstraining with children. Journal ofSchool Psychology, 26, 167-183.
Humphrey, L. L., Karoly, P, & Kirschen-baum, D. S. (1978). Self-managementin the classroom: Self-imposedresponse cost versus self-reward.Behavior Therapy, 9, 592-601.
Huntlert, J. & Bucher, B. (1978). Pupils'self-scored arithmetic performance: Apractical procedure for maintainingaccuracy. Journal of Applied BehaviorAnalysis, 11, 304.
CCBD Retrospective Series / 69

Jacobsen, E. (1938). Progressiverelaxation. Chicago: University ofChicago Press.
James, J. C., Trap, J., & Cooper, J. 0.(1977). Students' self-recording ofmanuscript letter strokes. Journal ofApplied Behavior Analysis, 10, 509-514.
James, J. E. (1981). Behavioral self-control of stuttering using timeoutfrom speaking. Journal of AppliedBehavior Analysis, 14, 25-37.
Kanfer, F. N., & Karoly, P (1982). Thepsychology of self-management:Abiding issues and tentative direc-tions. In P. Karoly & F. N. Kanfer(Eds.), Self-management and behaviorchange: From theory to practice (pp.571-599). New York: Pergamon.
Kaufman, K. F., & O'Leary, K. D. (1972).Reward, cost, and self-evaluationprocedures for disruptive adolescentsin a psychiatric hospital school.Journal of Applied Behavior Analysis,5, 293-309.
Kazdin, A. E. (1982). Current develop-ments and research issues incognitive- behavioral interventions: Acommentary. School PsychologyReview, 11, 75-82.
Kazdin, A. E. (1985). Selection of targetbehaviors: The relationship of thetreatment focus to clinical dysfunc-tion. Behavioral Assessment, 7, 33-47.
Kendall, P C. (1985). Toward a cognitive-behavioral model of child psychopa-thology and a critique of relatedinterventions. Journal of AbnormalChild Psychology, 13, 357-372.
Kendall, P C., & Braswell, L. (1982).Cognitive-behavioral self-controltherapy for children: A componentsanalysis. Journal of Consulting andClinical Psychology, 50, 672-689.
Kendall, P C., & Wilcox, L. E. (1980). Acognitive-behavioral treatment forimpulsivity: Concrete versus concep-tual training in non-self-controlledproblem children. Behavior Therapy,12, 344-359.
Kneedler, R. D. (1980). The use ofcognitive training to change socialbehaviors. Exceptional EducationQuarterly, I, 65-73.
Kneedler, R. D., & Hallahan, D. P(1981). Self-monitoring of on-taskbehavior with learning disabledchildren: Current studies anddirection. Exceptional EducationQuarterly, 2(3), 73-82.
70 / CCBD Retrospective Series
Kurtz, B. E., & Borkowski, J. G. (1984).Children's metacognition: Exploringrelations among knowledge, process,and motivational variables. Journal ofExperimental Child Psychology, 37,335-354.
Layne, C. C., Rickard, H. C., Jones, M.T., & Lyman, R. D. (1976). Accuracyof self-monitoring on a variable ratioschedule of observer verification.Behavior Therapy, 7, 481-488.
Leon, J. A., & Pepe, H. J. (1983). Self-instructional training: Cognitivebehavior modification for remediatingarithmetic deficits. ExceptionalChildren, 50, 54-60.
Lochman, J. E., Burch, P R., Curry, J. F.,& Lampron, L B. (1984). Treatmentand generalization effects of cognitive-behavioral and goal-setting interven-tions with aggressive boys. Journal ofConsulting and Clinical Psychology,52, 915-916.
Lochman, J. E., & Curry, J. F. (1986).Effects of social problem-solvingtraining and self-instruction trainingwith aggressive boys. Journal ofClinical Child Psychology, 15, 159-164.
Lochman, J. E., & Lampron, L. B.(1988). Cognitive-behavioralinterventions for aggressive boys: 7-month follow-up effects. Journal cfChild and Adolescent Psychotherapy.5, 15-23.
Lochman, J. E., Nelson, W. M., III, &Sims, J. P (1981). A cognitivebehavioral program for use withaggressive children. Journal of ClinicalChild Psychology, 10, 146-148.
Long, S. J., & Shere4 M. (1984). Socialskills training with juvenile offenders.Child and Family Behavior Therapy,6, 1-11.
Lovitt, T. C. (1973). Self-managementprojects with children with behavioraldisabilities. Journal of LearningDisabilities, 6, 138-150.
Maag, J. W. (1988a). Palliative copingand social skills training: Guidelinesand recommendations. Perceptions,24, 32-33.
Maag, J. W. (19886). Treatment ofchildhood and adolescent depression:Review and recommendation. In R. B.Rutherford, Jr., & J. W Maag (Eds.),Severe behavior disorders of childrenarul youth (Vol. 11, pp. 49-63).Reston, VA: Council for Children withBehavioral Disorders.

Maag, J. W. (1989). Moral discussiongroup interventions: Promisingtechnique or wishful thinking?Behavioral Disorders, 14, 99-106.
Maag, J. W. (in press). Assessment insocial skills training: Methodologicaland conceptual issues for researchand practice. Remedial and SpecialEducation.
Maag, J. W., Parks, B. T., & Rutherford,R. B., Jr. (1989). Generalization andbehavior covariation of aggression inchildren receiving stress inoculationtherapy. Child and Family BehaviorTherapy, 10, 20-47.
Malott, R. W. (1981). Notes from aradical behaviorist. Kalamazoo, MI:
Author.Marholin, D., II, Steinman, W. M.,
Luiselli, J. K., Schwartz, C. S., &Townsend, N. M. (1979). The effectsof progressive muscle relaxation onthe behavior of autistic adolescents: Apreliminary analysis. Child BehaviorTherapy, 1, 75-84.
Mastellone, M. (1974). Aversion therapy:A new use of the old rubberband.Journal of Behavior Therapy andExperimented Psychiatry, 5, 311-312.
Masters, J. C., & Santroek, J. W. (1976).Studies in the self-regulation ofbehavior: Effects of contingentcognitive and affective events.Developmerual Psychology, 12, 334-
348.McConnell, S. R. (1987). Entrapment
effects and the generalization andmaintenance of social skills trainingfor elementary school students withbehavioral disorders. BehavioralDisorders, 12, 252-263.
McKnight, D. L., Nelson, R. 0., Hayes, S.C., & Jarrett, R. B. (1984). Impor-tance of treating individually assessedresponse classes in the amelioration of
depression. Behavior Therapy, 15,
315-335.Meador, A. E., & 011endick, T. H. (1984).
Cognitive behavior therapy withchildren: An evaluation of its efficacyand clinical utility. Child and FamilyBehavior Therapy, 6, 25-44.
Meichenbaum, D. (1985). Stress
inoculation training. New York:
Pergamon.Meichenbanin, D., & Goodman, J. (1971).
Training impulsive children to talk tothemselves: A means of developing
self-control. Journal of AbnormalPsyclwlogy, 77, 115-126.
Morrow, L W., & Morrow, S. A. (1985).Use of a verbal mediation procedureto reduce talking-out behaviors. In M.K. Zabel (Ed.), TEACHING: Behavior-
ally disordered youth (pp. 23-28).Reston, VA: Council for Children withBehavioral Disorders.
Nelson, R. 0., Lipinski, D. P, & Boykin,R. A. (1978). The effects of self-recorders' training and the obtrusive-ness of the self-recording of self-monitoring. Behavior Therapy, 9, 200-
208.O'Leary, S. G., & Dubey, D. R. (1979).
Applications of self-controi proce-dures by children: A review. Journalof Applied Behavior Analysis, 12, 449-
475.O'Leary, S. G., & O'Leary, K. D. (1976).
Behavior modification in the school.
In H. Leitenberg (Ed.), Handbook ofbehavior modification and behaviortherapy (pp. 475-515). EnglewoodCliffs, NJ: Prentice-Hall.
Omizo, M. M. (1980). The effects ofbiofeedback-induced relaxationtraining in hyperactive adolescentboys. Journal of Psychology, 105,131-138.
Pearl, R. (1985). Cognitive-behavioralinterventions for increasing motiva-
tion. Journal of Abnormal ChildPsychology, 13, 443-454.
Robin, A. L., Schneider, M., & Dolnick,M. (1976). The turtle technique: Anextended case of self-control in the
classrooms. Psychology in the Schools,
13, 449-453.Rosenbaum, M. S., & Drabman, R. S.
(1979). Self-control training in theclassroom: A review and critique.Journal of Applied Behavior Analysis,12, 467-485.
Sagotsky, G., Patterson, C. J., &Lepper, M. R. (1978). Trainingchildren's self-control: A fieldexperiment in self-monitoring andgoal-setting in the classroom.Journal of Experimental ChildPsychology, 25, 242-253.
Santogrossi, D. A., O'Leary, K. D.,Romanczyk, R. G., & Kaufman, K. F.(1973). Self-evaluation by adolescentsin a psychiatric hospital school tokenprogram. Journal of Applied BehaviorAnalysis, 6, 277-287.
Santostefano, S., & Reider, C. (1984).Cognitive controls and aggression in
children. Journal of Consulting arulClinical Psychology, .52, 46-56.
CCBD Retrospective Series / 71

72 / CCBD Retrospective SeriesImmommommonim
Sarason, 1. G., & Ganzer, V. J. (1973).Modeling and g oup discussion in therehabilitation of juvenile delinquents.Journal of Counseling Psychology, 20,442-449.
Sarason, I. G., & Sarason, B. R. (1981).Teaching cognitive and social skills tohigh school students. Journal ofConsulting and Clinical Psychology,49, 908-918.
Schloss, P J., Schloss, C. N., Wood, C. E.,& Kiehl, W. S. (1986). A criticalreview of social skills research withbehaviorally disordered students.Behavioral Disorders, 12, 1-14.
Schunk, P H. (1983). Ability versus effortattributional feedback: Differentialeffects on self-efficacy and achieve-ment. Journal of EducationalPsychology, 75, 848-856.
Shores, R. E. (1987). Overview ofresearch on socill interaction: Ahistorical and personal perspective.Behavioral Disorders, 12, 233-241.
Short, E. J., & Ryan, E. B. (1984).Metacognitive differences betweenskilled and less skilled readers:Remediating deficits through storygrammar and attribution training.Journal of Educational Psychology,76, 225-235.
Simpson, R. L. (1987). Social interac-tions of behaviorally disorderedchildren and youth: Where are we andwhere do we need to go? BehavioralDisorders, 12, 292-298.
Stevenson, H. C., & Fantuzzo, J. W.(1984). Application of the "generali-zation map" to a self-control interven-tion with schoolaged children. Journalof Applied Behavior Analysis, 17, 203-212.
Stokes, T. F., & Baer, D. M. (1977). Animplicit technology of generalization.
h
Journal of Applied Behavior Analysis,10, 349-367.
Stokes, T. F., & Osnes, P G. (1986).Programming the generalization ofchildren's social behaviot In P S.Strain, M. Guralnick, & H. Walker(Eds.), Children's social behavior:Development, assessment, andmodification (pp. 407-443). Orlando,FL: Academic Press.
Stokes, T. F., & Danes, P G. (1988). Thedeveloping applied technology ofgeneralization and maintenance. In R.H. Horne; G. Dunlap, & R. L Koegel(Eds.), Generalization and mainte-nance (pp. 5-19). Baltimore, MD: PaulH. Brookes.
Sugai, G., & Rowe, P (1984). The effectof self-recording on out-of-seatbehavior of an EMR student.Education and Training of theMentally Retarded, 19, 23-28.
Turkewitz, H. O'Leary, K. D., & Iron-smith, M. (1975). Generalization andmaintenance of appropriate behaviorthrough self-control. Journal ofConsulting and Clinical Psychology,43, 577-583.
Vallis, T. (1984). A complete componentanalysis of stress inoculation for paintolerance. Cognitive TheraPY ondResearch, 8, 313-330.
Walker, H. M., McConnell, S. R., Walker,J., Holmes, D., Todis, B., & Golden,N. (1983). ACCEPTS: A curriculum
for effect peer and teacher skills.Austin, TX: Pro-Ed.
Walton, W. T. (1979). The Use of arelaxation curriculum andbiofeedback training. in theclassroom to reduce inappropriatebehaviors of emotfoniillycapped children. Ae_kavioralDisorders, 5, 10-115.:`-'-
Air

Using a Peer Confrontation Systemin a Group Setting
Spencer J. SalendNancy Reid JantzenKaren Giek
ABSTRACT. The effectiveness of a peer confrontation system applied in a groupsetting was examined using a reversal design. Two groups of students withdisabilities educated in a self-contained classroom within a public school pro-gram served as subjects for the study. The results show that a peer confronta-tion system was effective in modifying the inappropriate behavior of the twogroups. Student satisfaction data indicate that the students had positive reac-
tions to the system.
There has been a growing recognition of the value of using a variety ofpeer-mediated interventions to modify a wide range of classroom behaviors(Nelson, 1981; Salend, 1987; Smith & Fowler, 1984; Solomon & Wahler,1973; Strain & Odom, 1986). One highly effective peer-mediated inter-vention is a peer confrontation system (Bellafiore & Salend, 1983; San-dler, Arnold, Gable, & Strain, 1987; Savicki, 1981). Peer confrontation isbased on Vorrath and Brendtro's Positive Peer Culture Model (1974) whichwas developed to teach students to challenge the deviant behavior of their
peers and to realize its effect on others. Peer confrontation employs athree-step model: (a) identifying the problem, (b) determining its effectson others, and (c) engaging in problem solving. Initially, peers identify theinappropriate behavior and challenge disruptive classmates to be aware oftheir behavior. Then, the peers discuss the consequences of the inappro-priate behavior on others. Finally, peers engage in problem-solving togenerate positive alternatives to the inappropriate behavior (Bellafiore &
Salend, 1983; Candler & Goodman, 1979). Through problem-solving,peers are directly involved in helping classmates learn new behaviorswhile they in turn are learning appropriate responses to the disruptivebehaviors of their classmates.
Peer confrontation also includes elements of mild punishment. Like averbal reprimand such as no, the peer confrontation system may functionas a conditioned aversive stimulus (Bellafiore & Salend, 1983; Greenwood& Hops, 1981). While research on the efficacy of verbal reprimands ismixed, several factors appear to contribute to the effectiveness of repri-mands in the classroom (Van Houten, Nau, Mackenzie-Keating, Sarneoto,& Calavecchia, 1982). These authors found that the effectiveness ofreprimands was enhanced when the reprimand was (a) combined withnonverbal behaviors associated with reprimands (e.g., eye contact, firm
Reprinted from Behavioral
Disorders, Vol. 17, Number 3,
May 1992, pp. 211-218
wilimmommoiimi
CCBD Retrospective Series / 73

While the value of a peerconfrontation system directedat individual students hasappeared in the literature,there have been no studies toassess its effectiveness whenapplied to a group of students.
1111111111111111111111111111111
74 / CCBD Retrospective Series
grasp), and (b) delivered in closeproximity to the student. Using twosame sex pairs of elementary levelchildren, they also explored theeffects of verbal reprimands directedat one member of the dyad duringindependent work time. In addition toreducing the inappropriate behaviorof the reprimanded student, theverbal reprimands had positivespillover effects on the student siftingnext to the reprimanded student.
Bellafiore and Salend (1983)illustrated that teacher-directed peerconfrontation was a highly effectivesystem for decreasing the inappropri-ate behavior of a targeted behavioral-ly disordered student. They alsonoted the intervention led to vicariouseffects on the behavior of twonontargeted peers. Sandler et al.(1987) replicated these findings bydemonstrating the effectiveness of thetechnique with middle schoolstudents with behavioral disorders.Lemlech (1979) and Savicki (1981)also reported using a peer confronta-tion system successfully.
While the value of a peer confronta-tion system directed at individualstudents has appeared in the litera-ture (Be llafiore & Sa lend, 1983;Sandler et al., 1987), there have beenno studies to assess its effectivenesswhen applied to a group of students.The present study was designed toinvestigate the efficacy of a peerconfrontation system employed in agroup setting. Additionally, data onthe students' reactions to the systemare presented.
METHOD
Subjects
Two groups of students with disabili-ties educated in a public schoolprogram served as subjects for thisstudy. Students in both groups hadbeen identified as having a disability
7
by the school district's multidisci-plinary team in accordance with NewYork state guidelines. The studentsreceived their academic program in aself-contained class and wereintegrated with their nonhandicappedpeers for music, art, and physicaleducation. Descriptive data on thestudents in this study are presentedin Table 1.
Group A consisted of 9 males whoseages ranged from 8 years 7 months to10 years 6 months. Of the students inGroup A, 2 were classified aslearning disabled, 4 were classifiedas emotionally disturbed, 2 wereclassified as mentally retarded, and 1was classified as speech impaired.Their IQ scores as tested by theWechsler Intelligence Scale forChildren Revised (WISC-R; Wechsler,1974) ranged from 61 to 106, with amean of 88.
Group B consisted of 4 males and 1female whose ages ranged from 8years 5 months to 9 years 11 months.In Group B, 3 of the students wereclassified as learning disabled and 2students were classified as emotional-ly disturbed. Their IQ scores astested by the WISCR ranged from 81to 105, with a mean of 93.
Setting
Data were collected during Group A'sand Group B's language arts period.Group A's language arts period wasconducted from 9:00 to 9:15 a.m.,while Group B's language arts periodoccurred from 10:00 to 10:30 a.m.The length of these sessions remainedconsistent throughout the study. Theinstructional activities for Group Aincluded oral reading and worksheetsfrom the Time Concept Series (Ded-rick & Lattyak, 1981), while Group Bworked on spelling and languageskills using the Working Words inSpelling: Level B (Woodruff & Moore,1984) and Language Skills: Level A(Woodruff & Moore, 1987) programs.

TABLE 1
Descriptive Data on Students Across Groups
Student Age Sex Disability*
Woodcock-JohnsonIQ Percentile Scores
(WISC-R) Reading Math
Group A
1 10-6 M MII
2 9-1 M MH
3 9-8 M ED
4 8-7 M ED
5 9-11 M ED
6 8-11 M SI
7 9-5 M ED
8 9-11 M LD
9 9-9 M LD
Group B
1 9-8 M ED
2 9-8 F LD
3 9-11 M LD
4 9-9 M LD
5 8-5 M ED
61 0 0
82 36 4
106 6 16
101 11 15
94 13 24
91 20 5
78 8 8
NA** 5 12
91 19 11
105 11 19
81 1 9
NA** 5 12
91 19 11
96 11 19
* MI-I = Mentally Handicapped, ED = Emotionally Disturbed, SI = Speech
Impaired, LD = Learning Disabled
**NA = Not Available
Each group's language arts periodtook place in a classroom comprisedof two standard-size classroomsseparated by a sliding center dividerthat remained open throughout thestudy. The students and the teachersat in chairs around the perimeter oftwo double-desks that were placedtogether. During this time period, thestudents were instructed by theirlanguage arts teacher who hadundergraduate and master's degrees
in special education and New Yorkstate certification in special educa-tion. At the time of this study, shehad been teaching students withspecial education needs for 7 years.
Target Behaviors
The teacher and teacher's aide wereasked to select the students' behav-iors that were most disruptive andhad the greatest negative impact on
;!
f1EST COPY AVAILABLE
The teacher and teacher's aide
selected the students'behaviors that were mostdisruptive and had the greatestnegative impact on the learning
environment.
CCBD Retrospective Series / 75

Data were collected by trained,
independent observers, andinterobserver agreementmeasures were obtained.
76 / CCBD Retrospective Series
the learning environment. Theseinappropriate behaviors were thenoperationally defined and recordedduring a pre-baseline period to assesstheir frequency. Those behaviors thatoccurred at high rates and wereexhibited by several group memberswere selected as the target behaviors.
Because Group A's low levels of on-task behavior were interfering withinstruction, the target behavior forGroup A was to increase on-taskbehavior. On-task behavior wasdefined as eyes and/or pencil on therequired book, workbook, paper, orassignment. It also included eyes onpeers discussing the Material andeyes on the teacher when instruc-tions, directions, and feedback weregiven. On-task behavior also consist-ed of comments related to thematerial being covered in class.
Because the behavior that wasconsidered most disruptive for GroupB was inappropriate verbalizations,the target behavior for Group B was todecrease inappropriate verbaliza-tions. Inappropriate verbalizationswere defined as any student commentwithout teacher permission. Teacherpermission could be granted by theteacher acknowledging a student'sraised hand or the teacher requestingthat a student respond verbally.
Data Recording Strategies
Data were collected by trained,independent observers. One observerwas a graduate student working onobtaining her master's degree inspecial education. She had completedan undergraduate training program inspecial education and taught studentswith severe behaviGral disorders for 2years. The second observe; wes acommunity volunteer who had noformal training in special education.
The observers were trained usingSalend's model (1983) for identifyingand recording target behaviors over a
3-day period. Observer trainingconsisted of reviewing, studying, anddiscussing the target behaviordefinitions and observation proce-dures. Next, observers viewedexamples and nonexamples of thetarget behaviors and identified thesalient features of the target behav-iors. Observers also were asked topresent examples of the targetbehavior. Finally, the observers role-played and practiced using theobservation procedures.
Data on Group A's on-task behaviorwere collected by using a wholeinterval recording system of 15-secintervals whereby students had tomaintain on-task behavior throughoutthe entire interval. A whole intervalrecording system was employedbecause on-task behavior should bemaintained for an extended period oftime to be meaningful.
Event recording was employed tocount the number of inappropriateverbalizations exhibited by Group Bthroughout the observation periodbecause this behavior had discretebeginnings and endings. DuringGroup B's language arts period, eachtime a student exhibited an inappro-priate verbalization, it was recordedby the observer. If two studentsengaged in an inappropriate verbal-ization at the same time, two inappro-priate verbalizations were recorded.
Interobserver Agreement
Interobserver agreement measureswere obtained by having two trainedobservers independently record thetarget behaviors. For Group A,interobserver agreement measures onoccurrence agreement were taken on30% of the sessions and weredistributed across all phases.Interobserver agreement was calcu-lated by dividing the number ofagreements by the number ofagreements and disagreements on aninterval by interval basis and

multiplying by 100. Interobserveragreement measures had a mean of84%. The Try.f.an interobserveragreement for Baseline 1, Interven-tion 1, Baseline 2, and Intervention 2were 79, 86, 87, and 84%, respec-tively.
For Group B, interobserver agreementmeasures on occurrence agreementwere taken on 28% of the sessionsand were distributed across allphases. Since event recording wasused to collect the data, interobserveragreement was calculated by dividingthe smaller number of recordedinappropriate verbalizations by thelarger for each observation andmultiplying by 100. Interobserveragreement measures had a mean of89%. The mean interobserveragreement for Baseline 1, Interven-tion 1, Baseline 2, and Intervention 2were 81, 94, 82, and 95%, respec-tively.
Experimental Design
The study employed a reversal design(Baer, Wolf, & Risley, 1968). To helpstudents discriminate baseline andtreatment conditions, prior to eachtreatment session the teacherinformed the students that "we willbe using the system today" and thenreviewed the system with them.Additionally, at the beginning of eachBaseline 2 session, the students weretold that "we are not going to use thesystem today." The procedures forevaluating the effectiveness of theintervention conditions are describedbelow.
Baseline 1
Prior to instituting the peer confronta-tion system, data were collected oneach group's target behavior. Theteacher responded to the students'behavior in her usual manner. Duringbaseline and throughout the study,the teacher implemented a classroomtoken system. Students earned tokensand received teacher praise at
variable intervals for appropriatebehaviors such as working quietly,staying in-seat, and completing theirwork. The number of tokens studentsearned during their language artsperiod depended upon each student'sbehavior. Typically, students earnedbetween 3 and 8 tokens daily. At theend of the week, these tokens wereexchanged for reinforcers such asmagic markers, stickers, free time,books, and posters. Baseline 1conditions were maintained for 7days for both groups.
Intervention 1
The intervention was a teacher-directed peer confrontation system inwhich all group members partici-pated. Each time a group memberexhibited an inappropriate behavior(i.e., off-task behavior for Group A,inappropriate verbalization for GroupB), the teacher initiated the interven-tion by asking the group to respond tothe following: (a) "(Subject) seems tobe having a problem. Who can tell(Subject) what the problem is?"; (b)"Can you tell (Subject) why that is aproblem?"; (c) "Who can tell(Subject) what s/he needs to do tosolve the problem?" If two studentsengaged in an inappropriate behaviorsimultaneously, the peer confronta-tion system was directed at bothstudents (e.g., Johnny and Mary seemto be having a problem).
Following each question, the teacherselected a volunteer from the group torespond to that qtiestion. The teacheremployed verbal praise to reinforceappropriate responses to the ques-tions and to encourage the students'participation in the process. Addi-tionally, the teacher used verbalpraise to reinforce the student whohad been confronted for acceptingand engaging in the positive alterna-tives suggested by the group mem-bers. Intervention 1 conditions lasted7 and 10 days for Group andGroup B, respectively.
The teacher employed verbalpraise to reinforce appropriate
responses and to encourage
student participation.
11111M1111111111111111111111E111111
CCBD Retrospective Series / 77

Students said they preferredthe peer confrontation system
to the system used prior to thestudy.
1111=111111116.
78 / CCBD Retrospective Series
Prior to instituting the peer confronta-tion system, the teacher receivedtraining in its implementation. Thetraining focused on dealing withstudent responses, reinforcingappropriate behavior, and implement-ing the system in a positive, non-threatening manner. Before beginningthe intervention, the teacher engagedin role-playing and practiced usingthe system with groups not includedin the study. The training wusconducted by the senior ate.hor of thisarticle and lasted for 3 days.
Baseline 2
This period replicated the conditionsdescribed in Baseline 1. Baseline 2conditions were maintained for 5 and6 days for Group A and Group B,respectively.
Intervention 2
This phase was characterized by areturn to the experimental conditionsdescribed in Intervention 1. Interven-tion 2 lasted 11 and 12 days forGroup A and Group B, respectively.
RESULTS
The results are presented in Figures1 and 2. The data indicate that theintervention led to a marked decreasein both groups' inappropriatebehavior.
For Group A, the percentage ofintervals of on-task behavior duringBaseline 1 ranged from 29 to 62%with a mean of 44.1%. DuringIntervention 1 the percentage ofintervals in which Group A exhibitedon-task behavior increased to a meanof 84% with a range of 45 to 100%.The percentage of intervals of on-taskbehavior during Baseline 2 rar.gedfrom 43 to 64% with a mean of57.4%. During Intervention 2 thepercentage of intervals of on-taskbehavior yiAded a mean of 87.5%with a range of 59 to 96%.
For Group B, the number of inappro-priate verbalizations per minuteduring Baseline 1 ranged from .76 to1.42 with a mean of 1.10. DuringIntervention 1 Group B's inappropri-ate verbalizations per minutedecreased to a mean of .22 with arange of .06 to .52. The mean numberof inappropriate verbalizations perminute during Baseline 2 was .52with a range of .14 to .91. Datacollected during Intervention 2yielded a mean of 33 inappropriateverbalizations per minute with arange of 0 to .31.
Student Satisfaction Data
Students in both groups wereinterviewed individually by theirteacher at the end of the study todetermine their perceptions of thetreatment conditions. Prior to theinterview, the teacher assured thestudents that their comments wouldbe used to help the teacher assiststudents in the class and would notbe shared with anyone else. In theinterview, students were asked torespond orally to the following:
1. Would you rather work the way weused to or under the peer confron-tation system?
2. What did you like about the peerconfrontation system?
3. What didn't you like about thepeer confrontation system? and
4. Would you like to continueworking using the peer confronta-tion system?
Of the 13 students, 11 said theypreferred the peer confrontationsystem to the system used prior to thestudy. Students liked several thingsabout the system in, luding theproblem-solving aspect and theirability to "work better and payattention." The aspects of the systemdisliked by the students were "it wasembarrassing (to be confronted)" and"sometimes it.slowed the group."When asked if they would like to

100
90
80
60,r)
50
40TD>(i) 30
a)a0
Baseline 1 InterventIon I Baseline 2 Intervention 2
5 10 15 20 25 30
Figure 1. Percentage of intervals of on-task behavior for Group A.
continue the peer confrontationsystem, 12 of the 13 studentsresponded in the affirmative.
DISCUSSION
The results of this study suggest thata peer confrontation system used inconjunction with a token economysystem may be an effective methodfor decreasing inappropriate behaviorof students in groups. This finding isconsistent with and adds to theprofessional literature on peerconfrontation (Bellafiore & Salend,1983; Sandler et al., 1987). Theteacher reported that when theintervention was in effect, she "wasable to accomplish more and spent
less time disciplining students." Shealso noted during the treatmentsessions, "students completed morework and worked at a faster pace."
The system has several advantages. Aunique aspect of the peer confronta-tion system is the problem-solvingcomponent. Through problem-solving, peers offer positive alterna-tives to the inappropriate behaviorand become actively involved in theclasses' behavior managementsystem. For example, throughout thisstudy peers told disruptive studentsto `.-9t be distracted by other kids,""wait until the class is over beforetalking .o someone," try to rememberto raise your hand," and "concentrate
BEST COPY AVAILABLE
CCBD Retrospective Series / 79

I1.4
1.3
1.2 -
1.1 -
1.0 -
.9
.81
.7 -
.6
.5 -
.4
.3
.2
.1
.0
Baseline I Intervention 1 Baseline 2 Intervention 2
DAYS 5 10 15 201 1
25 30 35
Figure 2. Inappropriate verbalizations per minute for Group B.
on listening to the teacher." Anotheradvantage of the system is thestudents' positive reactions. Studentswere observed actively engaging inthe process and occasionally initiatedthe procedure. Student satisfactiondata indicated students liked thesystem and would like to continueusing it. These findings are consis-tent with anecdotal reports thatstudents enjoy the procedure andapply it spontaneously (Bellafiore &Salend, 1983; Sandler et al., 1987).
The system has several benefits forteachers. First, it is easy to imple-ment and can be employed withouttaking a lot of teacher time orresources. Second, peer confrontation
80 / CCBD Retrospective Series
is a relatively natural consequence ofmisbehavior. Third, while containingelements of mild punishment, theintervention offers information tostudents about what to do and notmerely what not to do. Finally, thesystem can be employed across avariety of behaviors and classroomsettings.'
The system also can be modified forimplementation in mainstreamedsettings. For example, to avoid thepotential embarrassment that can beassociated with directing the systemtoward the student who engaged inthe inappropriate behavior (e.g., Daleseems to be having a problem. Whocan tell Dale what the problem is?),

the system can be adapted so thatwhen any class member engages inthe targeted inappropriate behavior,the class is viewed as having aproblem (e.g., The class seems to behaving a problem. Who can tell theclass what the problem is?). Addi-tionally, to minimize the teacher'sinvolvement in the system, studentscan be taught to initiate and tomanage the system.
Willems (1974) cautioned research-ers to consider "the indirect andunintended effects of the interven-tion" (p. 161). He suggests thatresearchers examine the side effectsof the intervention on behaviors,individuals, and settings as well asthe timing of the effects. Because thepeer confrontation system haselements of punishment and peerpressure (Bellafiore & Salend, 1983;Sandler et al., 1987), professionalsshould watch for the negative sideeffects associated with punishment(e.g., escape avoidance, withdrawn oraggressive behavior) and peerpressure based strategies (e.g., verbalthreats, physically threateninggestures, aggressive acts; Alberto &Troutman, 1986; Axelrod, 1973).
In this study, while initially there wassome grimacing and face hiding whenthe intervention was applied and onestudent felt it was embarrassing to beconfronted, the potential risks ofpunishment and peer pressure werenot evidenced. The potential deleteri-ous effects of the use of aversives maynot have been realized because thepeer confrontation system providedinstruction to students concerningwhat o do as well as what not to do.Additionally, the potential negativeside effects of punishment and peerpressure may have been minimizedbecause the intervention was appliedto each member of the group ratherthan to a single targeted student. Thefact that the teacher had previouslyestablished positive and acceptingrelationships with the students and
was trained in the implementation of
the system also served to lessenpotential negative outcomes.
The results of this study should beinterpreted with several reservations.While the teacher reported thatstudent performance improved whenthe intervention was in effect, no dataconcerning work completion werecollected. Future research shouldprovide data to assess the impact ofthe intervention on measures ofacademic achievement. Because oftime constraints associated with theend of the school year, the number ofobservations sessions were limitedand data to determine the mainte-nance effects of the treatment werenot provided. Subsequent studiesshould examine the efficacy of thetreatment over a longer period of timeand offer data to examine themaintenance of the treatment effects.While social validity data concerningthe student's perceptions werecollected, future studies also shouldaddress other social validity issues(e.g., selection of target behaviors). Inlight of the emphasis on educatingstudents with disabilities in main-streamed settings, research toexamine the efficacy of a peerconfrontation system in regularclassroom settings is needed.
REFERENCESAlberto, P A., & Troutman, A. C. (1986).
Applied behavior analysis for teachers.Columbus, OH: Merrill,
Axelrod, S. (1973). Comparison ofindividual and group contingencies intwo special classes. Behavior Therapy,4, 83-90.
Baer, D. M., Wolf, M. M., & Risky, T R.(1968). Some current dimensions ofapplied behavior analysis. Journal ofApplied Behavior Analysis, I, 91-97.
Bellafiore, L. A., & Salend, S. J. (1983).Modifying inappropriate behaviorthrough a peer confrontation system.Behavioral Disorders, 8, 274.279.
Candler, A., & Goodman, C. (1979).SPACE for students to managebehavior. Academic Therapy, 15, 87-90.
BEST COPY AVAILABLE C
Future research should (a)
provide data to assess theimpact of the intervention on
measures of academicachievement and (b) examine
the efficacy of a peerconfrontation system in regular
classroom settings.
CCBD Retrospective Series / 81womersNo

Dedrick, S., & Lattyak, J. (1981). Timeconcept series. Beaverton, OR:Dormac.
Greenwood, C., & Hops, H. (1981).Group-oriented contingencies andpeer behavior change. In P Strain(Ed.), Utilization of classroom peers asbehavior change agents (pp. 189-259). New York: Plenum.
Lemlech, J. K. (1979). Classroommanagement. New York: Harper &Row.
Nelson, C. M. (1981). Classroommanagement. In J. M. Kauffman & D.
Hallahan (Eds.), Handbook ofspecial education (pp. 663-687).Englewood Cliffs, NJ: Prentice-Hall.
Salend, S. J. (1983). Guidelines forexplaining target behaviors tostudents. Elementary School Guidanceand Counseling, 18, 88-93.
Salend, S. J. (1987). Group-orientedbehavioral strategies. TeachingExceptional Children, 20, 53-56.
Sandler, A. C., Arnold, L. B., Cable, R.A., & Strain, P S. (1987). Effects ofpeer pressure on disruptive behaviorof behaviorally disordered classmates.Behavioral Disorders, 12, 104-110.
Savicki, V. (1981). Working with troubledchildren. New York: Human Science.
Smith, L., & Fowle; S. (1984). Positivepeer pressure: The effects of peermonitoring on children's disruptive
82 / CCBD Retrospective Series
behavior. Journal of Applied BehaviorAnalysis, 17, 213-227.
Solomon, R. W., & Wahler, R. G. (1973).Peer reinforcement control ofclassroom problem behavior. Journalof Applied Behavior Analysis, 6, 49-56.
Strain, P S., & Odom, S. L. (1986). Peerst.cial initiations: Effective interven-tions for social skill development ofexceptional children. ExceptionalChildren, 52, 543-552.
Van Houten, R., Nau, P, Mackenzie-Keating, S., Sameoto, D., & Calavec-chia, B. (1982). An analysis of somevariables influencing the effectivenessof reprimands. Journal of AppliedBehavior Analysis, 15, 65-83.
Vorrath, H., & Brendtro, L. (1974).Positive peer culture. Chicago: Aldine.
Wechsler, D. (1974). Wechsler intelligencescale for children-revised. SanAntonio, TX: Psychological Corp.
Willems, E. P (1974). Behavioraltechnology and behavioral ecology.Journal of Applied Behavior Analysis,7, 151-165.
Woodruff, G. W, & Moore, G. N. (1984).Working with words in spelling (LevelB). North Billerica, MA: CurriculumAssociates.
Woodruff, G. W., & Moore, G. N. (1987).Language skills (Level A). NorthBillerica, MA: Curriculum Associates.

Social Interaction Trainingfor Preschool Childrenwith Behavioral Disorders
Mary A. McEvoySamuel L. Odom
ABSTRACT The importance of early peer interaction for the development ofpositive outcomes on adult life adjustment measures has been well documented.Children who do not engage in social interaction, or do so at a depressed rate,do not have access to this avenue for skill development. The purpose of thisarticle is to provide an illustrative review of the most recent advances in socialinteraction research for children who exhibit a wide range of behavioral disor-ders. Specifically, teacher-mediated, peer mediated, and interpersonal prob-lem-solving approaches to prompting social interaction are presented. In addi-tion, factors which affect social interaction training such as type of activities,presence of socially competent peers, and subject characteristics are discussed.
Finally, suggestions for further research are advanced.
Young children first begin to interact socially with their peers duringinfancy (Mueller & Vanden, 1979). These interactions grow in frequencyand complexity and reach a plateau in the third and fourth years of life(Ilartup, 1983). A convergence of research findings suggests that partici-pation in social interactions with peers contributes directly to the acquisi-tion of cognitive (Murray, 1972; Perret-Clermont, 1980; Piaget, 1926),social cognitive (Damon, 1984), language (Guralnick, 1981), and evenmore advanced social skills (Hartup & Sancilio, 1986). Children who do
not engage in social interaction with peers, or who do so at a depressedrate, do not have access to this rich avenue for skill development. Anumber of researchers have documented the relationship between.failureto establish positive peer relationships in childhood and negative out-
comes on such adult life adjustment measures as referral for psychiatrictreatment (Cowen, Peterson, Babigian, Izzo, & Trost, 1973), bad conductdischarges from the military (Roff, 1961), withdrawal from school prior tograduation (Ullmann, 1957), and juvenile delinquency (Roff, Sells, &Golden, 1972; West & Farrington, 1973).
Preparation of this article was supported by Grant No. G008630344 fromthe U. S. Department of Education, OSERS. The authors wish to thankWilma Davis for her technical assistance.
BEST COPY AVAILABLE
Reprinted from Behavioral
Disorders, Vol. 12, Number 4,
August 1987, pp. 242-251
sommimmow=m
CCBD Retrospective Series / 83

Researchers have developed
and evaluated procedures forsocial interaction training forchildren with autism andsocially withdrawn or isolatechildren.
111111110111111111111111111111111=111
84 / CCBD Retrospective Seriesiii
In recent years a growing number ofexperimental studies have examinedthe problem of social skill develop-ment for preschool children withbehavioral disorders. Specifically,researchers have developed andevaluated procedures for socialinteraction training for children withautism (Lord & Hopkins, 1986;McEvoy et al., 1987; Mc Hale, 1983;Odom, Hoyson, Jamieson, & Strain,1985; Odom & Strain, 1986) andsocially withdrawn or isolate children(Furman, Rahe, & Hartup, 1979;Hecimovic, Fox, Shores, & Strain,1985; Hendrickson, Strain, Tremblay,& Shores, 1982; Twardosz, Nor-dquist, Simon, & Botkin, 1983).Given the immediate and long-termsignificance of peer social interac-tions for preschool children withbehavioral disorders and the docu-mented delays that may occur in thedevelopment of their peer socialinteraction skills, an inclusion ofsocial interaction skills as legitimatetargets of instruction in preschoolprograms would seem appropriate.The purpose of this article is toprovide an illustrative review of themost recent advances in socialinteraction research with preschoolchildren who exhibit a range ofbehavioral disorders. Included withinthat group will be children who aresocially withdrawn and children whoare autistic. We will examine teacher-mediated, peer-mediated, andinterpersonal problem-solvingapproaches to promoting socialinteraction skills. Factors affectingoutcomes of social interactiontraining will be described and,finally, suggestions for futureresearch will be advanced.
Teacher-MediatedInterventionsIn a recent review of early interven-tion procedures for socially with-drawn preschool children, Mastro-pieri and Scruggs (1985) reportedthat teachers were major or minor
6 6
intervenors in over 80% of thestudies. The most typical form ofteacher mediation is the use ofprompting and positive reinforce-ment (e.g., praise) for appropriatesocial interaction. A number ofstudies have shown.that teacherscan increase the social interactionsof preschool children with behav-ioral disorders (e.g., Allen, Hart,Buell, Harris, & Wolf, 1964; Hart,Reynolds, Baer, Brawley, & Harris,1968; Strain, Shores, & Kerr, 1976;Strain & Timm, 1974; Strain &.Weigerink, 1975; Timm, Strain, &Eller, 1979). More recently, Bryantand Budd (1984) evaluated theeffectiveness of a teacher-mediatedpackage for training behaviorallyhandicapped children to share.Teachers used a program developedby Barton and Ascione (1979)which consisted of instructions,modeling, behavioral rehearsal, andteacher prompts and praise forinteraction. Substantial increases insharing were seen for 5 of the 6children who participated in thetraining. The authors also reportedconcomitant decreases in negativeinteractions.
Wolfe, Boyd, and Wolfe (1983)investigated the effects of verbalinstructions and a token economy onthe rate of cooperative play amongpreschool children with behaviorproblems. Three children who wereaggressive or socially withdrawn weregiven "happy faces" and praised bythe classroc,m teacher contingentupon cooperative play. In addition,children who received a predeter-mined number of "happy faces" wereallowed 10 min of outdoor freeplay.Increases in cooperative play wereseen for all 3 children when theintervention was implemented. Theauthors reported that the childrenmaintained cooperative behavior afterthe intervention procedures weresystematically fiuled, although theprocedures were never eliminatedcompletely.

While teacher-mediated procedureshave effectively produced changes inthe social interaction skills ofpreschoolers with behavioral disor-ders, researchers have identifiedseveral problems with this type ofintervention. First, Strain, Cooke, andApolloni (1976) reported thatteacher-mediated procedures thatincorporate a specific set of promptsand reinforcers have been evaluatedprimarily in highly structuredtraining settings using well-trainedpractitioners. In addition, Strain andFox (1981) reported that this tech-nique may disrupt ongoing interac-tions. Odom and Strain (1986)compared teacher prompting proce-dures with a peer-mediated approach.In discussing the limitations ofteacher-mediated procedures, theyreported that the children with autismdid not initiate interactions unlessprompted by the teacher to do so. Inaddition, Timm, Strain, and Eller(1979) have pointed out the lengthyfading and learning process that isnecessary when reducing teacherprompts. Clearly, more attention mustbe focused on designing teachermediated procedures that can beimplemented readily in the classroomsetting and that do not requirecontinuous use of teacher promptsand praise.
Recently, several researchersevaluated the use of teacher-mediatedgroup affection activities to promotesocial interaction. Affection activitieswere developed by Twardosz et al.(1983) in response to some of thecriticisms of teacher-mediatedinterventions discussed above. Thoseinvestigators were interested indesigning procedures that would berelatively easy to implement bypreschool teachers, would focus onfunctional social interaction behav-iors, would provide opportunities foracquisition of new skills, could beimplemented in the settings whereincreases in interaction were desired(thus addressing the generalization
problem), and would involve multiplepeers in training. In addition,Twardosz et al. (1983) were interestedin the expression of affection and itsrelationship to other types of socialinteraction. Tremblay, Strain,Hendrickson, and Shores (1981) hadfound that physical affection was oneof several social initiation categoriesthat was likely to be responded topositively by peers. Twardosz et al.(1983) developed and evaluatedprocedures that would encourage theexpression of affection and addressthe issues raised above.
A number of researchers (Brown,Ragland, & Fox, 1987; McEvoy et al.,1987; Twardosz et al., 1983) havenow used group affection activities toincrease the peer interactions ofpreschool children who were sociallywithdrawn or of autistic preschoolers.These activities occur during grouptime and are based upon typicalpreschool games, songs, and materi-als. At the start of the activity, thechildren greet each other by exchang-ing some form of physical affectionsuch as a hug, pat on the back, highfive, and so forth. The children thenparticipate in an activity such as"fanner in the dell" or singing "Ifyou're happy and you know it."However, these well-known preschoolgames and songs are modified toinclude an affection component. Forexample, insiead of singing "thefarmer takes a wife" or "the wifetakes a child", the teacher might havethe children "hug a wife" or "tickle achild." Not only has interaction beenincreased during the affectionactivities, but also during freeplayperiods in which training did not( arr. Twardosz et al. (1983) hypoth-esized that the procedures may beeffective for several reasons: thepairing of peers with pleasurableexperiences, desensitization to peerinteraction, and/or teaching thehandicapped children skills thatfacilitate freeplay interaction. Also,generalization may have been effected
,tAST COPY AVAILABLn
More attention must befocused on designing teachermediated procedures that can
be implemented readily in theclassroom setting and that do
not require continuous use ofteacher prompts and praise.
111111111101=1111111111111=1111111
CCBD Retrospective Series / 85

. t è-
Peer-mediated interventionsare based on the premise thatchildren develop social skillsthrough their interactions withpeers.
oimmmmomnom
86 / CCBD Retrospective Series
.::: o.-t ..'"ifit--j"..4 .
4i .. ..s... . ," %
',.1... P 4' ..by the use of.,rnkltrokl:rieriellitik-;,f.fee, ce strategies
more a4VaiedsoCidt4ialiolte,:":":, 7...:.rekativiite44d type of peer-results trorittroup af4thin Mir:diet '...::' ... mediatieCtiar:Olitions. In tKeseactivitresarencoptm.Hoykivge,...: - interventiirq, Ars are taught togiventhe'slcialidlyr,0 the 414414-* prompt; t}!e'. iksiiolUe that they wantmediated,:intreechke4 clikrissed ..' froniIIChiklviithlihavioral disor-aboye"0-nd14,relearcherd have ders, 44;44 yr, prIplyide.;reinforce-purd.the use of peer-mediated men't....for:e'rtgrnpe;:aW pdrt of hisprocedures as an alternative. # study.n#integrated,classroom,r .
1,. IsforihirriM,(!07-8)1ught preschoolers
Peer-Mediated .4 '-'. Or- (a)ookitgoiriautistic tlassmate to1.-
".' /- "-` *-%- ' Ifiei till h.....,...,...:-.norbitlk .t.-rnot e avior and thenIntervention ...:'..rdgirstrijdo-the. utistre.child with" '.-.---
Peer-itediatd i*ili, 4Ikliaill :.1m' :.
i' 74t'iPtrie dr.,...
4,4 . .....,based ni744te,ii,ertii. t chilei . .,- - ''''.''.develop social alifi rough their.interactions with peef;s. An added Peer!tlitiOtion strategfes represent
frAft: ::':,,
assumption'is that socially competent theftosarequently used peer-peers naturally interact with their nitdiaed intervention for promotingyoung peers in ways that facilitate socialtinteraction skills (Strain &social skill acquisition and that they Odrift; ):986). In this intervention,can be taught to use these interac- thetleit'eher or investigator teachestions systematically to enhance the soaailV.competent peers to directsocial skills of young children with soarraj initiations to the children withr-behavioral disorders. Such interven- behavioral dis6rders. These peertions are called peer-mediated inter*nnora*ekl t to persist inbecause the teacher does not directly their:social, a:because theprompt or reinforce the child with beaviniaN i orid Peers may bebehavioral disorders in the interven- unrestreful4f1 e initial : When neces-tion, but rather the intervention is striy.,11. tgcher malliovide verbal
. r 4delivered through the peer. Odom and prompt4 the peer Inervenor orStrain (1984a) idenYfied three types prov einforcement to the interve-of peer-mediated interventions. In n he end of thssession if he orproximity interventons, children with s ohed an established criterion.behavioral disorde'rs are simply
Al . fplaced with socially competent peers rly peer-Initiation study,and the effects due to this proximity ittrilt(f Shores, and Timm (1977)are measured. For example, Furman iti.Otift preschooLpeer to increaseet al. (1979) randomly assigned 4..1..Wstskial initratAnsto a sociallysocially withdrawn kpchool%, .,*(;,;:.Nvill;cliglivn peerVared Ated increaseschildren to a small iilaypoup,,1!7; 1,... -..:. in the14dr.a.ilorcidld's socialcontaining play partners'Of theArne.1::..;- .- interaetiOn.Vtdeco'nd study, Strainage, a small play group contd., (1977). erralized increases inplay partners 12 to 20 months ',. .... . sociaillyllit 71r4,,n preschoolers'younger, or in a no tre'atment cbrifroc '.. inttvc4iith peers across settingssituation. Withdrawn children Astiki.k.f....,. .whetr,,atpeeryeervenor beganto the cross-aged play group exhi'biteit . ';'.: diiittra so;ral initiations to thesignificantly higher levOs of tociak * ., 1v1. ttrafin chilk .
interaction than did children iii.th ':'-...f '.. v. ., .. ', v .
other groups. Proximity interviti.. 11.1.:(7.1`. ;-...,0, reeent.research on peer-with elementary-aged children with _ritY,;;;.....iir. dtion ihteiventions hus examined. .autism have revealed similar ine'rea 1: 4,1 e component features of the
..4 'in social interaction (Lord & H6pki " ',...i Intervention package. To investigate1986; McHale, 1983). r il...""the relativieffi.cdcy of the compo-
I. '
e,behavior was

nents of a peer-initiation interventionwith 3 preschoolers with autism orother behavioral disorders, Odom etal. (1985) systematically analyzed theimportance of reinforcement andteacher prompts for the peer interven-tors (i.e., children who delivered thetreatment). They found that the peerintervenors continued to directinitiations to the target children whenreinforcement was withdrawn, buttheir initiations decreased whenteacher prompts were removed andincreased when teacher prompts werereinstituted. The behaviorallydisordered children's level of socialinteraction covaried with peers'limitations.
To reduce the peer intervenors'reliance on teacher verbal prompts,Odom and Watts (1987) used acorrespondence training approach toteach the peer intervenor to continueinitiating to the 3 autistic children inthe absence of the teacher's verbalprompts. Peer intervenors werereinforced when they did what theysaid they were going to do. With thisapproach, peer intervenors' initia-tions continued when the teacherwithdrew her prompts and the autisticchildren continued to interact. Thenumber of peers included as interve-nors in peer-initiation interventionsis another variable that has beeninvestigated. In teacher-mediatedsocial interaction research withelementary-aged children andadolescents with autism, investigatorshave used multiple peer exemplars topromote peer and setting generaliza-tion of social interactions (Brady etal., 1984; Fox et al., 1984). Toexamine the use of multiple peerintervenors with preschool children,Odom, Strain, Karger, and Smith(1986) employed 3 peer intervenorsin one peer-initiation interventionand compared its effects with a peer-initiation intervention with a singlepeer. Although total social tateractionfor the 2 target children, 1 autisticand 1 electively mute child, did not
differ across interventions, theelectively mute preschool childengaged in more frequent socialinitiations in both conditions duringthe latter phases of the study.
To compare the relative effects of apeer-initiation strategy with a teacherprompting intervention, Odom andStrain (1986) used an alternatingtreatments design with 3 autisticpreschool children. During theteacher-mediated intervention, theteacher prompted the target child tointeract with a peer and taught peersto respond and extend the interaction.During the peer-initiation interven-tion, peers were taught to directsocial interactions to the target child,but not necessarily to respond.Autistic subjects' mean length ofinteraction was greater during theteacher prompting/peer responseintervention, although the peerinitiation intervention also producedsubstantial increases in the autisticchildren's social interaction. Al-though peer-mediated interventionsappear to produce substantialchanges in the social interactions ofautistic and socially withdrawnpreschoolers, researchers havepresented little evidence for mainte-nance of these changes after theintervention is removed or clearevidence for cross-setting generaliza-tion. Both of these topics need to beexamined in future research.
Interpersonal SocialProblem-SolvingInterventionsInterpersonal social problem-solvingis a process by which children solveproblems related to social interac-tions with peers. With preschoolchildren from low sociometric status(SES) families, Spivak and Shure(1974) created an interpersonalproblem-solving program containing46 lessons that taught children boththe linguistic prerequisites forproblem-solving skills and how to
BEST COPY AVAILABLE
Interpersonal social problem-
solving is a process by whichchildren solve problems related
to social interactions with
peers.
=111111=11111111=11111111110
CCBD Retrospective Series / 87wimmoIIm

Interpersonal social problem-solving appears to be a
promising technique forchildren without disabilities,and tentative evidence existsfor its effects upon the
problem-solving skills ofpreschoolers who arewithdrawn and aggressive.
11M1111111111111=11111=111111111111111111=11
88 / CCBD Retrospective Serieswisornommoomm
generate alternative solutions tointerpersonal problems. Whenimplemented with low SES preschoolchildren, these authors foundsubstantial increases in the chil-dren's ability to generate alternativesolutions to social problems in a testsituation and also found positivechanges on teacher ratings of socialadjustment, which maintained at aone year follow-up.
Other researchers have examined theSpivak and Shure (1974) techniquefor training problem-solving akills.Sharp (1981) implemented aninterpersonal problem-solvingprocedure with low SES children andfound positive changes in preschool-ers' verbal generation of problem-solving, but no changes in thechildren's behavior in the classroom.The absence of effect upon behaviorin the classroom was replicated byRickel, Eshelman, and Loigman(1983).
Extending Spivak and Shure's model,Ridley and Vaughn (1982) created asocial problem-solving programcomposed of 53 lessons that empha-sized language concepts, empathy,goal identification, generatingalternative solutions, cue sensitivity,and goal identification. Relative totheir control group, these authorsfound significant gains in socialproblem-solving as measured by abehavioral assessment in an analogsituation, as well as increases inpositive self-perception. In a replica-tion of ihis study, Vaughn and Ridley(1983) observed increases in positivesocial interaction with peers in theclassroom as a result of their inter-vention.
Social problem-solving researchershave most frequently conducted theirresearch with preschool children whowere normally developing, or whowere at some risk for behavioraldisorders through the socioeconomicstatus of their families. However, with
a group of aggressive preschoolchildren, Vaughn, Ridley, andBullock (1984) implemented a socialproblem-solving intervention andfound that children in their interven-tion group engapd in significantlymore solutions to problems, measuredby the Behav ioral InterpersonalProblem-Solving Test (Ridley &Vaughn, 1982), than did children ina control group with direct adultcontact. These differences maintainedat a 6-month follow-up. With a groupof preschool-aged children identifiedas emotionally disturbed (i.e., actingout or aggressive), Koenings andOppenheimer (1985) trained role-taking skills using a small groupformat across 20 lessons. They foundsignificant changes in the interven-tions group's ability to perceiveemotional consequences and to takethe perspective of others. However,neither of these studies trackedchanges in classroom behavior.
In summary, interpersonal socialproblem-solving appears to be apromising technique for childrenwithout handicaps, and tentativeevidence exists for its effects uponthe problem-solving skills of with-drawn and aggressive preschoolers.Future research should examine theeffects of these interventions upon theclassroom behavior with childrenwith behavioral disorders.
Contextual FactorsAffecting theSuccess ofinterventionsSocial interaction interventions forbehaviorally disordered preschoolchildren exist in a rich environmentalcontext. Within this context, a rangeof factors may affect the ultimateoutcomes of interventions (Strain &Kohler, in press). Although a fullreview is beyond the scope of thisarticle, two factors that appear to haveparticularly powerful effects on socialinteraction intervention are the

classroom activities in which thechildren with behavioral disordersparticipate and the characteristics ofthe peers with whom the childrenmay interact.
Activities. The type of activity inwhich children engage their peersdetermines to a large degree whetherchildren will interact with otherchildren or engage in solitary play.Although few studies have beenconducted with behaviorally disor-dered children, studies with pre-school children who exhibit otherhandicaps may be instructive.Stoneman, Cantrell, and Hoover-Dempsey (1983) observed the typesof activities around which preschoolhandicapped children in main-streamed zlasses interacted. Coopera-tive play occurred most frequentlyaround block activities, vehicles, andwater play. Solitary play occurredmost often around library, fine motor,and art aeivities.
In another observational studyoccurring in an integrated setting,DeKlyen and Odom (1987) classifieda large number of play activitiesaccording to the degree of structurethat each eontained. Structure wasdefined as the amount of definitioninherent in the activity (i.e., well-specified roles, clear behavioralrequirements) as well as the amountof definitinn that the teacher initiallyprovided. Frequency of socialinteraction was significantly relatedto the degree of structure in theactivities. Interestingly, negativecorrelations existed for the level ofteacher interactions in most activitiesand the level of social interactionwith peers, thus supporting thefindings of an earlier study byShores, Hester, and Strain (1976).
To explain the variability during thetreatment phase of an interventionstudy with behaviorally disorderedchildren, Odom and Strain (1984b)examined the relative effectiveness of
the intervention in different activi-ties. They found that the interventionwas much more effective in certaintypes of activities (e.g., sociodramaticplay) than in other types of interven-tions (e.g., fine motor activities). Insum, activities which are madeavailable and/or the activities whichchildren elect to engage affect thelevel of social interaction, thusmodifying the effectiveness of socialinteraction interventions.
Presence of socially competent peers.One can train children with behavior-al disorders to interact with theirpeers, but unless there are sociallyresponsive peers with whom tointeract, it would not seem reasonableto expect social interactions tocontinue in the absence of interven-tion or to generalize to other class-room settings. Strain (1983) exam-ined the cross-setting generalizationof a peer-mediated intervention withautistic preschool children, andfound that the autistic children didgeneralize treatment gains to a settingcontaining normally developingpeers, but not to one containing onlyhandicapped peers. In a secondstudy, Strain (1984) found that cross-setting generalization also occurredonly when the peer group had beencoached to respond to the interactionof the autistic child. However,Hecimovic et al. (1985) were unableto replicate this finding with a secondgroup of preschool children withbehavioral disorders. Similarly, in theOdom et al. (1985) examination ofcross-setting generalization of theeffects of a peer-mediated interven-tion, the presence of normallydeveloping peers did not facilitatecross-setting generalization. Fromthese it appears that the presence ofsocially responsive peers is adesirable condition for promotingsocial interaction, but not a sufficientcondition. Further research mustaddress the factors in addition to thepresence of normally developingpeers that mediate generalization.
One can train children withbehavioral disorders to interact
with their peers, but unless
there are socially responsivepeers with whom to interact, it
would not seem reasonable toexpect social interactions tocontinue in the absence ofintervention or to generalize to
other classroom settings.
10111111IINNINNIMINIMII
CCBD Retrospective Series / 89sommomm

Literature has established thatinterventions can be
implemented successfully toincrease the positive socialinteraction of children withbehavioral disorders.
90 / CCBD Retrospective Series
Subject CharacteristicsAs noted above, the broad classifica-tion of behavioral disorders includeschildren with a wide range ofcharacteristics. It seems reasonablethat children who are socially with-drawn might respond differently tocertain social interaction interventionsthan would children who are aggressiveor autistic. The characteristics of thechild will play a major role in deter-mining the success of the intervention,and should be considered closely whena teacher selects an interventionstrategy to use with a child.
Several of the interventions describedabove (e.g., Spivak and Shure, 1974)require that the child have someverbal skills (i.e., social problem-solving, social coaching). Althoughthere is some evidence that aggres-sive and socially withdrawn childrenmay benefit from those interventions(Vaughn & Ridley, 1983), it seemshighly likely that autistic children,because of their limited languageskills, would not benefit. Sociallywithdrawn and autistic preschoolersappear to benefit from peer-mediatedinterventions, yet it is unlikely thatsuch interventions would be aseffecti ve with aggressive children orethically amenable for peer interve-nors (i.e., the peer initiations couldelicit aggressive behaviors toward thepeer intervenor). In addition, groupaffection training activities appearmore effective with socially with-drawn preschool children than withautistic children (McEvoy et al., 1987).For an intervention to be successful, anappropriate match must occur betweenthe prerequisite skill requirements ofthe intervention and the characteristicsof the preschool child with behavioraldisorders.
Conclusions and FutureDirections for ResearchOver the past decade a growing bodyof literature has established thatinterventions can be implemented
successfully to increase the positivesocial interaction of children withbehavioral disorders. Earlier studiestested the effects of adult socialreinforcement on social behavior(Allen et al., 1964; Buell, Stoddard,Harris, & Baer, 1968; Hart et al.,1968). Recently, researchers havebegun to investigate the use ofteacher-mediated group affectionprocedures to increase the rate ofsocial interaction (Brown et al., 1987;McEvoy et al., 1987; Twardosz et al.,1983). However, due to the powerfulinfluence peers have on children'sbehavior, much of the recent researchhas employed a peer-mediatedapproach (e.g., Odom et al., 1985;Odom et al., 1986; Odom & Watts,1987). In addition, for youngchildren with verbal skills, socialproblem-solving interventions haveproven effective in increasing socialinteraction.
While researchers have beensuccessful in increasing the socialinteraction skills of children withbehavioral disorders, the currentresearch has several limitations.First, the issue of generalization andmaintenance must be addressed infuture research. Appropriate socialinteraction skills must occur ins:tuations outside of the trainingsetting and they must maintain acrosstime. While researchers haveproduced impressive treatmenteffects, there has been an inconsis-tent demonstration of cross-settinggeneralization and maintenance(Odom & Strain, 1984a). Stokes andOsnes (1987) ',-.ave pointed out anumber of procedures that could beincluded in training programs topromote generalization and mime-mince. These include taking advan-tage of natural communities ofreinforcement, training diversely, andincorporating functional mediators(e.g., use of common physical andsocial stimuli). Future researchshould be sensitive to the need todevelop procedures that are easily

implemented by classroom teachersand actively program for generaliza-tion and maintenance. In addition,much of the research to date hasinvestigated procedures to increasethe frequency of certain categories ofinteraction (e.g., initiations andresponse). Whether simple increasesin the quantity of these behaviors isappropriate is an empirical question.For example, data from the Hendrick-son et al. (1982) study suggested thatafter a certain point, increases inhandicapped children's rate ofinitiations did not necessarilyincrease rate of responses to thoseinitiations. The suggestion that "moreis better" is an area that deservesfuture empirical analysis.
A second limitation of the currentresearch is the use of global quantita-tive measures of social interaction asopposed to qualitativ2 measures. Inthe recent past, researchers haveassessed global measures of socialinteraction (e.g., positive socialinteraction, initiations, responses;Allen et al., 1964; Strain & Timm,1974). When researchers havedeveloped behavioral taxonomies thatare more descriptive than the often-used global measures of socialinteractions, the single criterion forselection of behaviors was theprobability that the behavior wouldelicit a positive social response froma peer (Nordquist, Twardosz, McEvoy,& Wilson, 1981; Strain, Odom, &McConnell, 1984; Tremblay et al.,1981).
A broader view of children's socialinteraction is needed. When childreninteract with their peers, they have apurpose which they intend to achieve(i.e., an intended function). They mayuse different behaviors to achieve thefunction, and these behaviors willhave differential probabilities ofsuccess (i.e., actually achieving thefunction). Children with behavioralproblems may encounter difficultiesin peer interactions either because
they do not choose the correctfunctions to pursue in a givencontext, they use less successfulbehaviors to achieve the desiredfunctions, or they simply do notengage in any functional interactions.Odom, McEvoy, Ostrosky, and Bishop(1987) are currently field testing anobservational procedure for measur-ing the functional characteristics ofchildren's social interactions andspecific behaviors that make up thoseinteractions. Future research in thisarea could have relevance for theselection of target behaviors ininterventions for children withbehavioral disorders.
Finally, Strain and Koh ller (in press)have called on researchers to assessthe social validity of their interven-tion procedures. They urge thatattention be given to the socialacceptability of the procedures, thesocial significance of the targetbehaviors, and the social importanceof the behavior change to the consum-ers; that is, do increases in socialinteractions achieve the ultimate goalof increases in friendships or socialsupport relationships betweenindividuals? Future research isneeded on the development andevaluation of procedures that addressthese broader outcome variables.
REFERENCES
Allen, K. E., Hart, B., Buell, J. S., Harris,E R., & Wolf, M. M. (1964). Effects ofsocial reinforcement on isolatebehavior of a nursery school child.Child Development, 35, 511-518.
Barton, E. J., & Ascione, F. R. (1979).Sharing in preschool children:Facilitation, stimulus generalization,response generalization, andmaintenance. Journal of AppliedBehavior Analysis, 12, 417-430.
Brady, M. P, Shores, R. E., Gunter, P,McEvoy, M. A., Fbx, & White, C.(1984). Generalization of a severelyhandicapped tyloleseent's socialinteraction responses via multiplepeers in a classroom setting. Journal
9 o
When children interact with
their peers, they have apurpose which they intend to
achieve.
CCBD Retrospective Series / 91

of the Association for Persons withSevere Handicaps, 9, 278-286.
Brown, W. H., Ragland, E. V, & Fox, J. J.(1987). Effects of group socializationprocedures on the social iraeractions ofpreschool children. Manuscriptsubmitted for publication.
Bryant, L. E, & Budd, K. S. (1984).Teaching behaviorally handicappedpreschool children to share. Journalof Applied Behavior Analysis, 17(1),45-56.
Buell, J. S., Stoddard, T., Harris, E R., &Baer, D. M. (1968). Collateral socialdevelopment accompanying reinforce-ment of outdoor play in a preschoolchild. Journal of Applied BehaviorAnalysis, 1, 167-173.
Cowen, E. L., Peterson, A., Babigian, H.,Izzo, L. D., & Trost, M. A. (1973).Long tem( follow-up of early detectedvulnerable children. Journal ofConsulting and Clinical Psychology,41, 438-446.
Damon, W. (1984). Peer education: Theuntapped potential. Journal of AppliedDevelopmental Psychology, 5, 331-334.
DeKlyen, M., & Odom, S. L. (1987).Structure and preschool peer interac-tions: Beyond the mainstream.Manuscript submitted for publication.
Fox, J. J., Gunter, P, Brady, M. P,Bambara, L. M., Speigel-McGill, P.Shores, R. E. (1984). Using multiplepeer exemplars to develop generalizedsocial responding of an autistic girl. InR. B. Rutherford, Jr. & C. MichaelNelson (Eds.), Severe BehaviorDisorders of Children and Youth (Vol.7, pp. 17-26). Reston, VA: Council forChildren with Behavioral Disorders.
Furman, W., Rahe, D., & Hartup, W.(1979). Rehabilitation of sociallywithdrawn preschool children throughmixed-age and same-age socialization.Child Development, 50(4), 915-922.
Guralnick, M. J. (1981). Peer influenceson development of communicativecompetence. In P Strain (Ed,), Theutilization of peers as behavior changeagents (pp. 31-68). New York:Plenum.
Hart, B. M., Reynolds, N. J., Baer, I). M.,Brawley, E. R., & Harris, E R.(1968). Effect of contingent andnoncontingent social reinforcement mithe cooperative play of a presclnadrhil(l . Journal of Applied BehaviorAnalysis, I, 73-76.
92 / CCBD Retrospective Series
Hartup, W. W. (1983). Peer relations. InM. Heatherington (Ed.), Handbook ofChild Psychology (Vol. 4, pp. 103-196). New York: John Wiley & Sons.
Hartup, W. W., & Sancilio, M. E (1986).Children's friendships. In E. Schopler& G. Mesibov (Eds.), Social behaviorin autism (pp. 61-80). New York:Plenum.
Hecimovic, A., Fox, J. J., Shores, R. E.,& Strain, P S. (1985). An analysis ofdevelopmentally integrated andsegregated freeplay setting and thegeneralization of newly-acquiredsocial behaviors of socially withdrawnpreschoolers. Behavioral Assessment,7, 367-388.
Hendrickson, J. M., Strain, P S.,Tremblay, A., & Shores, R. E. (1982).Interactions of behaviorally handi-capped preschoolers: Functionaleffects of peer social initiations.Behavior Modification, 6, 323-353.
Koenings, A., & Oppenheimer, L. (1985).Development and training of role-taking abilities with emotionallydisturbed preschoolers: A pilot study.Journal of Applied DevelopmentalPsychology, 6, 313-320.
Lord, C., & Hopkins, J. M. (1986). Thesocial behavior of autistic childrenwith younger and same-agednonhandicapped peers. Journal ofAtaism and Developmental Disorders,16, 249-262.
Mastropieri, M. A., & Scruggs, T. E.(1985). Early intervention for sociallywithdrawn children. Journal of SpecialEducation, 19(4), 427-441.
McEvoy, M. A., Nordquist, V. M.,Twardosz, S., Heckaman, K. A.,Wehby, J. H., & Denny, R. K. (1987).Promoting autistic children's peerinteraction in integrated earlychildhood settings using affectionactivities and incidental teaching.Manuscript sulnnitted for publication.
PacHale, S. (1983). Social intervention ofautistic and nonhandicapped childrenduring freeplay. American Jourtud ofOrthopsychiatry, 53(1), 81-91.
Mueller, E., & Vandell, D. (1979). Infant-infant interaction. In J. Osofsky (Ed.).Handbook qf infant development (pp.714-756). New York: John Wiley &Suns.
Murray, E (1972). The acquisition ofmiservation throug!I social interac-tion. Developmental Psycholop; 6. 1-
6.

Nordquist, V. M. (1978). A behavioralapproach to the analysis of peerinteractions. In M. Guralnick (Ed.),Early intervention and the integrationof handicapped and nonhandicappedchildren (pp. 53-84). Baltimore:University Park Press.
'4nrdquist, V. M., Twardosz, S., McEvoy,M. A., & Wilson, S. (1981). ProjectSEARCH: Observer training manual.Unpublished manuscript, Universityof Tennessee, Knoxville.
Odom, S. L., Hoyson, M., Jamieson, B.,& Strain, P S. (1985). Increasinghandicapped preschoolers peer socialinteractions: Cross setting andcomponent analysis. Journal ofApplied Behavior Analysis, 18, 3-16.
Odom, S. L, McEvoy, M. A., Ostrosky,M., & Bishop, L (1987, May).Measuring the functional socialinteraction of preschool children.Paper presented at the meeting of theAssociation of Behavior Analysis,Nashville, TN.
Odom, S. L & Strain, P S. (1984a).Peer-mediated approaches toincreasing children's social interac-tions: A review. American Journal ofOrthopsychiatry, 54, 544-557.
Odom, S. L., & Strain, P S. (19846).Classroom-based social skillsinstruction for severely handicappedpreschool children. Topic.s in EarlyChildhood Special Education, 4, 97-116.
Odom, S. L., & Strain, P S. (1986). Acomparison of peer-initiation andteacher-antecedent interventions forpromoting reciprocal social interactionof autistic preschoolers. Journal ofApplied Behavior Analysis, 190), 59-71.
Odom, S. L., Strain, P S., Karger, M. A.,& Smith, J. D. (1986). Using singleand multiple peers to promote socialinteraction of preschool children withhandicaps. Journal of the Division ofEarly Childhood, 10, 53-64.
Odom, S. L., & Watts, E. (1987). Crosssetting generalisation of autisticpreschool children's social interactionin peer-initiation intervention.Manuscript to be submitted forpublication.
Perret-Clermont, A. N. (1980). Socialinteraction and cognitive developmentin children. European Monographs inSocial Psychology. London: AcademicPress.
Piaget, J. (1926). The language andthought of the child. London:Routledge & Kegen Paul.
Rickel, A. V., Eshelman, A. K., &Loigman, G. A. (1983). Socialproblem-solving training: A follow-upstudy of cognitive and behavioraleffects. Journal of Abnormal ChildPsychology, 11, 15-28.
Ridley, C. A., & Vaughn, S. R. (1982).The effects of a preschool problem-solving program on interpersonalbehavior. Journal of Applied Develop-mental Psychology, 3, 177-180.
Rolf, M. (1961). Childhood socialinteractions and young adult badconduct. Journal of Abnonnal SocialPsychology, 63, 333-337.
Roff, M., Sells, B., & Golden, M. M.(1972). 5SST2 Social adjustment andpersonality in children. Minneapolis:University of Minnesota Press.
Sharp, K. C. (1981). Impact of interper-sonal problem-solving training onpreschoolers' social competency.Journal of Applied DevelopmentalPsychology, 2, 129-143.
Shores, R. E., Hester, P, & Strain, P S.(1976). The effects of amount andtype of teacher-child interaction onchild-child interaction duringfreeplay. Psychology in the Schools,13, 171-175.
Spivak, C., & Shure, M. B. (1974). Socialadjustment of young children: Acognitive approach to solving real-lifeproblem.s. San Francisco: Jossey-Bass.
Stokes, T. F., & Osnes, E' G. (1987).Programming generalization ofchildren's social behavior. In I? Strain,M. Guralnick, & H. Walker (Eds.),Children's social behavior: Develop-ment, assessment, and intervention(pp. 408-443). New York: AcademicPress.
Stoneman, Z.. Cantrell, M. L., & Hoover-Dempsey, K. (1983). The associationbetween play materials and socialbehavior in a mainstreamed pre-school: A naturalistic investigation.Journal of Applied DevelopmentalPsychology, 4, 163-174.
Strain, P S. (1977). An experimentalanalysis of peer social initiations onthe behavior of withdrawn preschoolchildren: Some training and generali-zation effects. Journal of AbnormalPsychology, 5, 445-455.
Strain, P S. (1983). Generalization ofautistic children's social behavior
CCBD Retrospective Series / 93

94 / CCBD Retrospective Seriesmolimisomnrimmloom
change: Effects of developmentallyintegrated and segregated settings.Analysis and Intervention in Develop-mental Disabilities, 3, 23-34.
Strain, P S. (1984). Social interaction ofhandicapped preschoolers indevelopmentally integrated andsegregated settings: A study ofgeneralization effects. In T. Field(Ed.), Friendship between normallydeveloping and handicapped children(pp. 187-208). Chicago: Society forResearch in Child Development.
Strain, P S., Cooke, T. P. & Apolloni, T.A. (1976). Teaching exceptionalchildren: Assessing and modifyingsocial behavior. New York: AcademicPress.
Strain, P S., & Fox, J. J. (1981). Peersocial initiations and the modificationof social withdrawal: A review andfuture perspective. Journal ofPediatric Psychology, 6, 417-433.
Strain, P S., & Kohler, E W. (in press).Social skill intervention with younghandicapped children. In S. Odom &M. Karnes (Eds.), Research in earlychildhood special education. PaulBrookes Publishing.
Strain, P S., & Odom, S. L. (1986). Peersocial initiations: Effective interven-tion for social skill development ofexceptional children. ExceptionalChildren, 52, 543-552.
Strain, P S., Odom, S. L., & McConnell,S. R. (1984). Promoting socialreciprocity of exceptional children:Identification, target behaviorselection, and intervention. Remedialand Special Education, 5, 526-531.
Strain, P S., Shores, R. E., & Kerr, M. M.(1976). An experimental analysis of"spillover" effects on the socialinteraction of behaviorally handi-capped preschool children, Journal ofApplied Behavior Analysis, 9, 31-40.
Strain. P S., Shores, R. E., & Timm, M.(1977). Effects of peer social initiationson the behavior of withdrawn preschoolchildren. Journal of Applied BehaviorAnalysis, 10, 289-298.
Strain, P S. & 'limm, M. (1974). Anexperimental analysis of socialinteraction between a behaviorallydisordered preschool child and herclassroom peers. Journal of AppliedBehavior Analysis, 7(4), 583-590.
Strain, P S., & Weigerink, R. (1976). Theeffects of sociodramatic activities onsocial interaction among behaviorallydisordered preschool children.Journal of Special Education, 10, 71-75.
Timm, M., Strain, P S., & Eller, P (1979).Effects of systematic responsedependent fading and thinningprocedures on the maintenance ofchild-child interaction. Journal ofApplied Behavior Analysis, 12(2), 308.
Tremblay, A., Strain, P S., Hendrickson,J. M., & Shores, R. E. (1981). Socialinteractions of normal preschoolchildren. Behavior Modification, 5,237-253.
Twardosz, S., Nordquist, V. M., Simon, R.,& Botkin, D. (1983). The effect ofgroup affection activities on theinteraction of socially isolate children.Analysis and Intervention in Develop-mental Disabilities, 13, 311-338.
Ullman, C. A. (1957). Teachers, peers,and tests as predictors of adjustment.Journal of Educational Psychology,48, 257-267.
Vaughn, S. R., & Ridley, C. A. (1983). Apreschool interpersonal problem-solving program: Does it affectbehavior in the classroom? ChildStudy Journal, 13, 1-12.
Vaughn, S. R., Ridley, C. A., & Bullock,D. D. (1984). Interpersonal problem-solving kills training with aggressiveyoung cAdren. Journal of AppliedDevelopmental Psychology, 5, 213-223
West, D. J., & Farrington, D. P (1973).Who becomes delinquent? London:Heineman Press.
Wolfe, V. V., Boyd, L. A., & Wolfe, D. A.(1983). Teaching cooperative play tobehavior problem preschool children.Education and Treatment of Children,6(1), 1-9.
BEST COPY AVAILABLE0

Entrapment Effects and theGeneralization and Maintenancec#: Social Skills Trainingfor Elementary School Studentswith Behavioral Disorders
Scott R. McConnell
Effective social interaction is a desired goal for all children. Socialinteraction provides opportunities for learning and practice of language,motor, and other skills (Hartup, 1983; Hops, Finch, & McConnell, 1985),and provides children with opportunities to play and work with others.Further, skills for social interaction are associated with and thoughtnecessary for adjustment and achievement in schools (Grectn, Vosk,
Forehand, Beck, & Vosk, 1980; McConnell et al., 1984), families (Patter-son, 1982), and work settings (Warrenfeltz et al., 1981).
Because of these relationships, attention to social interaction skills isespecially important for children with behavioral disorders. By definition,these children experience difficulties interacting with others (Kauffman,1985). Such interactive difficulties lead to rejection by peers, socialisolation, and reduced access to opportunities to benefit from socialinteraction with nonhandicapped peers (Strain, Odom, & McConnell,1984; Walker, McConnell, & Clarke, 1985). Together, characteristics thatlead to initial identification of behavioral disorders, as well as the primarytreatment of these disorders in restricted educational settings, put identi-fied children at risk for continued and future difficulties interacting withpeers.
For these reasons, and a host of others (Hops et al., 1985), social skillstraining has recently become a major focus of research and treatmentefforts for young children with behavioral disorders. This surge of interestand concern has led to a proliferation of assessment procedures for identi-fying social skills deficits among children, and treatment procedures forremediating these identified deficits.
These assessment and treatment procedures have been reviewed exten-sively, both in this journal (Schloss, Schloss, Wood, & Kiehl, 1986) andother sources (e.g., Cartledge & Milburn, 1980; Gresham, 1986; Hops etal., 1985; Hops & Greenwood, 1981, in press; Van Hasse lt, Hersen,Whitehall, & Bel lack, 1979). Typically, these reviews have focused onspecific child characteristics and their implications for assessment and
Reprinted from Behavioral
Disorders, Vol. 12, Number 4,
August 1987, pp. 252-263
111111111111111111111111111111MINE
CCBD Retrospective Series / 95

Entrapment is a behavioralprocess by which .newly
acquired social responsescome under the control ofnaturally occurring reinforcers.
111=11111111111=11111=1111111111111
96 / CCBD Retrospective SerieswommoriogimmiNi
treatment; relatively less attentionhas been paid to interaction variablesthat influence the development ofsocial competence by handicappedand high-risk youngsters.
Attention to interaction variables maybe one way of increasing our under-standing of generalization andmaintenance effects in socialinteraction skills training. Behavioralresearchers, including those interest-ed in social skills, have increasedtheir efforts to identify proceduresthat will enhance generalization andmaintenance of treatment (Stokes &Baer, 1977; Stokes & Osnes, 1986).In their recent review, Stokes andOsnes identify one class of generali-zation enhancement strategies asthose that "take advantage of naturalcommunities of reinforcement" (p.418). Within this class of strategies,these authors place particularemphasis on the importance of socialinteractive relationships that willproduce durable changes in targetbehaviors.
Rather than review assessment andtreatment issues generally, thepurpose of this article is to discussrecent research trends that focus oninteraction variables that contributeto generalization and maintenance insocial skills interventions forbehaviorally disordered elementaryschool children. In particular, thisarticle will outline one interactivephenomenonentrapmentandargue that this conceptualization ofsocial behavior offers special promisefor developing and evaluating socialskill interventions. Based on thisdiscussion, the author will reviewseveral factors to be considered inselection of target behaviors forintervention. Finally, recentlydeveloped treatment packages (andadaptations of existing packages) thatappear to target those variablesrelated to the entrapment of adaptivesocial behavior by behaviorally
I Li
handicapped elementary schoolstudents will be examined.
Entrapment:A Conceptual Frameworkfor Social InteractionSkills TrainingEntrapment is a behavioral processby which newly acquired socialresponses come under the control ofnaturally occurring reinforcers; thesereinforcers are, by and large, thesocial behaviors of peers. [The authornotes the potentially negativeconnotation of the term entrapmentthat is used here to identify agenerally desirable phenomenon.However, it has been elected to usethe term to preserve continuity withearlier work in this area (cf., Baer &Wolf, 1970; Kohler & Greenwood,1986).] Entrapment describes onemechanism by which all childrenmay develop and elaborate thosebehaviors termed social skills. Forexample, early in the school experi-ence a child may offer a toy to a peer.This share offer is very likely to setthe occasion for a positive peerresponse (Tremblay, Strain, Hen-drickson, & Shores, 1981) and to bereciprocated by peers offering toys tothe child in the future (cf., Charles-worth & Hartup, 1967; Kohler &Fowler, 1985). If positive interactionand reciprocated sharing serve asreinforcers for the child, sharing islikely to become entrapped: Thelikelihood of future share offers bythe child is thus increased byexposure to naturally occurring socialbehaviors of others.
Social interaction is bidirectional andreciprocal (Strain & Shores, 1977),requiring the interrelated behavior oftwo or more individuals to occur.Hops and Greenwood (in press)compare social interaction to a tennismatch; each interaction begins whenone person's "serve" (or socialinitiation) is followed by another's

"return" (or social response). Afterthe initial exchange, interactionscontinue as a series of "volleys" witheach person's behavior serving asboth response and antecedent to thesocial behavior of the other. In thisway, interaction unfolds with itsoverall content mutually determinedby the ongoing, interdependentbehavior of the interactants.
It is in this reciprocal, bidirectionalprocess that newly acquired behav-iors come into contact with naturallyoccurring reinforcing responses andthat entrapment Jccurs. Entrapmentmay thus represent an essentialfeature of social skill interventionsfor behaviorally disordered children.To guarantee generalized and durablebehavior change, we must teachchildren to exhibit those behaviorsthat will be naturally reinforced bypeers. Further, at times we mustrestructure existing reinforcementcontingencies in peer play groups,such that these new contingencieswill maintain newly acquiredadaptive social behaviors exhibitedby children receiving our training.
Simply put, this conceptualization ofentrapment as a primary process inthe acquisition, maintenance, andgeneralization of social behaviorsleads to an increased emphasis oninteraction variables in social skillsassessment and treatment for behav-iorally disordered children. Attentionto entrapment expands our assess-ment focus to include not only thesocial behavior of an individualchild, but also the behavior of othersin the child's environment; inparticular, assessment must describepeer or teacher behavior that serves toreinforce and maintain adaptive ormaladaptive social responding by thetarget child. Similarly, emphasis onthe process of entrapment leads tochanges in intervention proceduresincluding (a) increased attention totraining and coaching that teachesidentified children to produce critical
social interaction skills, and (b) moredirect focus on peer behaviors thatare likely to contribute to mutuallydependent "entrapped" relationshipsthat will maintain target behaviorslong after intervention is ended.Thus, attention to interactive vari-ables in social skills training mayenhance the identification of essentialtarget behaviors and the developmentof effective treatment procedures thatlead to entrapment of adaptive socialresponses for children with behavior-al disorders. We now turn to these twoissues.
Selecting TargetBehaviors for SocialInteraction Skills TrainingThis analysis of entrapment wouldsuggest that careful selection of targetbehaviors is critical to success insocial skills training for children withbehavioral disorders. In particular,intervention programs should includetraining for those skills and behaviorsthat (a) are adaptive or desirable andcontribute to development of socialcompetence for the handicappedchild, and (b) prompt peer responsesthat are likely to serve as reinforcers,thus ontributing to the entrapment ofthe targeted behavior.
To guarantee these outcomes, skillsincluded in any training programshould be selected empirically, basedon these two criteria (Hops et al.,1985). To date, however, this empiri-cal basis has not been consideredroutinely in target behavior selectionfor social skill interventions. Rather,skills are often drawn from logicalanalyses of social interaction or peeracceptance, or from extrapolations ofempirical work completed withadults. Both practices have beencriticized (Foster & Ritchey, 1979;Hops & Greenwood, 1981; Strain etal., 1984).
Recently, however, several reviewersin this area have offered conceptual
Attention to interactivevariables in social skills training
may enhance the identificationof essential target behaviorsand the development ofeffective treatment proceduresthat lead to entrapment ofadaptive social responses for
children with behavioral
disorders.
1111111Mill1111111=11
CCBD Retrospective Series / 97

The history of social skillstraining with children withbehavioral disorders is repletewith studies in which childrendemonstrate significant gainsduring treatment but fail tomaintain these gains afterintervention ends.
98 / CCBD Retrospective Series
guidelines for the empirical selectionof social skills. In one of the mostcomplete works on entrapment ofsocial behavior in children availableto date, Kohler and Greenwood(1986) describe five necessary formsof evidence for the identification ofbehavioral entrapment; three of theserules have direct bearing on theselection of target behaviors for socialskills interventions. To maximize thelikelihood of entrapment for socialskills included in our interventions,we must:
1. Select behaviors that will bemaintained after intervention isterminated. Social skills training istypically designed to increase (or insome cases decrease) specific socialbehaviors to criterion or therapeuticlevels of occurrence. To guaranteeeffectiveness and efficiency of theseinterventions, target skills must beselected that are most likely to bemaintained at higher or more desiredrates of occurrence by exposure tonaturally occurring reinforcers afterthe period of intervention ends.
This point may seem obvious and notworth mentioning. However, thehistory of social skills training withbehaviorally disordered children isreplete with studies in whichchildren demonstrate significantgains during treatment, but fail tomaintain these gains after interven-tion ends (Hops, 1982). For example,Bornstein, Bel lack, and Hersen(1980) trained four aggressivechildren between the ages of 8 and12 to improve three specific aspectsof positive assertiveness: increasedeye contact, decreased use of hostilevoice tone, and increased requests fornew behavior. Although improvementwas noted during treatment for allsubjects across all three targetbehaviors, only one of the individual-ly targeted behaviors (reduced use ofhostile tone) continued at a similarlevel 4 to 26 weeks after trainingended; for two subjects, decreasing
1,)
trends were noted in requests for newbehavior, and one child declined topretreatment levels on the measure ofeye contact. Thus, children main-tained only one of three targetbehaviors, reduced use of hostilevoice tone.
Given these findings, we can hypoth-esize that only reduced use of hostilevoice tone came under the control ofnaturally occurring reinforcementfrom peers. It should be noted thatmultiple reasons may exist formaintenance and generalization ofsocial skills, and that data presentedby Bornstein and his colleagues(1980) is but one piece of a morecomprehensive proof for the existenceof behavioral entrapment (Kohler &Greenwood, 1986). However, toguarantee the efficiency and overalleffectiveness of social skills training,particular attention must be given toidentifying those skills that are mostlikely to be maintained long aftertraining is completed.
2. Select skills that will generalize across settings or other behaviors.Social skills training typically occursin one particular setting (e.g., aclassroom), or in a restricted set ofsettings (e.g., classrooms andplayground of one school). Further,training is generally provided for alimited range of a particular re-sponse. However, in all but a fewcases, the purpose of this training isto produce elaborated performancefor a class of behaviors across a rangeof social settings. For instance, let usassume that "sharing" is 'Included ina social skill intervention for 2nd-grade students. During intervention,students may be given opportunitiesto share balls, trucks, and blocks inan indoor play area. The intent of thistraining is to produce more general-ized sharingit would be desirableto observe participating studentssharing academic materials, othertoys, play equipment, or othermaterials in the classroom, lunch-

room, library, playground, or outsideof school.
Thus, the efficiency and overalleffectiveness of social interactionskills training will be increased byselecting target skills that representmore general response classes thatoccasion positive peer responsesacross a variety of social situations.In this way, slight variations of anindividual skill can be more closelymatched to the behavioral demands ofa given situation, thus increasing thelikelihood that a child's performancewill produce reinforcing responsesfrom peers.
3. Select target behaviors that covarywith specific social behaviors of peers.Finally, we must select targetbehaviors that reliably follow specificpeer initiations or precede positivepeer responses. One major assump-tion of the entrapment model is thatspecific aspects of peers' socialbehavior can serve to prompt orreinforce the occurrence of desiredsocial skills by children receivingtraining. In selecting target behav-iors, then, we must give priority tothose skills that are most likely tobecome "embedded" in socialinteractions with peers. To the extentthat targeted social skills producepositive responses from peers, or tothe extent that these behaviors arereliably prompted by peer behavior,the likelihood of entrapinent isenhanced.
Thus, Kohler and Greenwood (1986)have offered conceptual guidelines forthe selection of target behaviors insocial interaction skills training.While we have not yet conductedmuch systematic research thatexplicitly follows these guidelines, asmall collection of recent investiga-tions does offer some further empiri-cal guidance for planning interven-tions. Several of these investigationshave been descriptive, using observa-tional measures to compare and
contrast the interactions of behavior-ally handicapped and nonhandi-capped children in naturalisticsettings. Additionally, severalexperimental investigations havedemonstrated differential effects forthe entrapment of various targetbehaviors among young children.These investigations can serve as asolid empirical foundation for furtherresearch into the selection of targetbehaviors in social interaction skillstraining, and are briefly reviewedbelow.
Descriptive investigations. Descriptivestudies based on observationalassessment of children's socialbehavior offer one method foridentifying specific skills that meetthe multiple criteria for entrapmentoutlined above. Several investigationsof this type have been completed withpreschool children (e.g., Greenwood,Todd, Hops & Walker, 1982; Strain,1983; Tremblay et al., 1981).Additionally, several investigationshave examined relationships betweenobserved social behaviors andsociometric status for nonhandi-capped (e.g., Dodge, 1983) andhandicapped (e.g., Bryan, 1974)elementary school children. To date,however, only a few studies havespecifically examined social behav-ioral relationships between behavior-ally handi( apped children and theirpers. Although these studies do notspecifically address entrapment ofsocial behavior, each has somerelevance for the selection of targetbehaviors for intervention.
McConnell (1982) compared freeplaysocial behaviors of 43 handicappedand nonhandicapped boys in grades 1through 4. Each handicapped subjectreceived at least some educationalservices in regular education settings,and had been identified by hisspecial education teacher as havingdifficulty making friends, playingappropriately, or being accepted bypeers in mainstream settings.
The efficiency and overalleffectiveness of socialinteraction skills training will be
increased by selecting target
skills that represent moregeneral response classes that
occasion positive peerresponses across a variety of
social situations.
111111=111111111111111111
CCBD Retrospective Series / 99

Participation in structured playactivities must be assessed,
and the frequency and type ofsocial initiations made bychildren with disabilities, aswell as peer responses to
these initiations, must beexamined more carefully.
IINNINIIIIIMIIM111111111MININI11
100 / CCBD Retrospective SeriesInimmo
Nonhandicapped participants wereselected at random from regulareducation classrooms of the handi-capped subjects.
McConnell found little difference inbroad measures of social interactionfor the two groups; handicapped andnonhandicapped boys spent similaramounts of time participating in sometype of social play and talking withpeers. Similarly, peers spoke tosubjects in the two groups at equiva-lent rates.
However, several important differenc-es emerged when more fine-grainedmeasures were examined. First,handicapped children spent signifi-cantly less time than nonhandicappedpeers in structured play (i.e.,organized games). Second, handi-capped children initiated to peerssignificantly more often than didnonhandicapped subjects. However,peers were less likely to respond toindividual social initiations fromhandicapped subjects.
These findings suggest severalgeneral guidelines for the selection oftarget behaviors. First, participationin structured play activities must beassessed t;nd, where necessary,brought to normative levels. Struc-tured playground games appear to bea primary site for freeplay interactionamong elementary school boys, andaccess to interaction during thesegames may facilitate entrapment ofmore specifically targeted socialbehaviors. Second, the frequency andtype of social initiations made byhandicapped children, as well aspeer responses to these initiations,must be examined more carefully.Findings from McConnell's (1982)study indicated that handicappedsubjects made more initiations thandid nonhandicapped subjects, butengaged in equivalent overall rates ofsocial interaction. Given that peersresponded to a smaller pmportion ofinitiations front handicapped
I
subjects, one can wonder whether thespecific social bids exhibited bythese children differed in quality ortype from the initiations of thenonhandicapped comparison group.Methods like those used by Tremblayet al. (1981), where peer responses todifferent types of social initiationswere specifically evaluated, may aidin the further understanding of thiseffect.
In a second study, Foster and Ritchey(1985) observed children in grades 4to 6 during two classroom activities.Observed children were assigned toone of three groups, based on positiveand negative peer nominationsociometric assessment: acceptedsubjects (high number of positivenominations), rejected children (highnumber of negative nominations), andignored children (few negative orpositive nominations). Like McCon-nell's (1982) study, Foster andRitchey found no differences inoverall interaction rates for childrenin the three groups. However,observational assessment indicatedthat accepted children received morepositive initiations from peers, andhad a higher proportion of their totalinteractions initiated by peers (ameasure of sociability from Green-wood et al., 1982) than subjects ineither the rejected or neglectedgroups.
Across these two descriptive studies,several common findings emerge.Measures of discrete, child-specificbehavior (e.g., subject initiations)may not discriminate behaviorallyhandicapped children from nonhand-icapped peers.
Such differences do emerge, however,when one examines relationshipsbetween the social behavior of two ormore children: handicapped studentsare more likely to be ignored follow-ing initiations to peers (McConnell,1982), and are less likely to receivepositive initiations from peers (Foster

& Ritchey, 1985). Thus, descriptivestudies corroborate the notion thatinteractim variables may be relativelymore important than discrete behav-ioral variables in the assessment,description, and treatment of socialinteraction deficits among elementaryschoolaged children.
Experimental investigations. Inaddition to these correlationalstudies, two experimental investiga-tions contribute to the identificationof target behaviors that are likely tobecome entrapped. In the first,Walker, Greenwood, Hops, and Todd(1979) demonstrated that overallrates of social interaction for sociallywhhdrawn elementary studentschanged as a function of specificcomponents of interaction beingreinforced by the teacher. Highestobserved rates of social interactionoccurred when children in a playgroup received praise for continuedinteraction with peers (i.e., a socialinitiation, followed by a positiveresponse, followed by ongoingexchange of social behavior betweentwo or more children). When childrenwere praised for only initiations orresponses, overall levels of socialinteraction declined. During thesephases, subjects often engaged inwhat Walker and his colleaguestermed "cocktail party" interac-tionseither a solitary initiation, oran initiation and response, followedby termination of the interaction.Thus, children produced andmaintained high rates of socialinteraction only when reinforcementwas contingent on the behavior ofboth interactants (i.e., continuedinteraction).
In a second experimental investiga-tion, Kohler and Fowler (1985)demonstrated at least partial entrap-ment of one social skill among threeelementary-aged girls. Subjects weretrained to produce four specific typesof swial invitations (i.e., offer toshare, offer assistance, inviting peers
to play, requesting permission to playwith peers); two subjects alsoreceived training in the use of socialamenities (i.e., please, thank you,you're welcome, I'm sorry, or excuseme). Coaching procedures wereintroduced to increase rates of thesetarget behaviors during freeplayactivities with classmates, and ratesof social invitations and amenitiesemitted by subjects and peers wererecorded. These investigators focusedon two particular types of peerresponses: social reciprocity (i.e., thenumber of invitations or amenitiesdirected to subject by peers) andsocial responsiveness (i.e., immediateacceptance or refusal of subjectinvitations).
For two of the children, Betty andSarah, increased rates of socialinvitations to peers were associatedwith similar increases in rates ofsocial invitations from peers.Although the third subject, Amanda,also increased her rate of invitationsto peers, similar increases were notseen for peer invitations directed toher. Interestingly, both Betty andSarah maintained their rates of socialinvitations to and from peers aftertermination of the initial interventionphase; sustained rates of socialinvitations were not noted forAmanda. Such maintenance wasdemonstrated only after the investi-gators introduced a group contin-gency to increase Amanda's peers'invitations to higher, more recipro-cal rates.
Quite different effects were noted,however, for social amenities. BothSarah and Betty increased their useof amenities during intervention.However, reciprocal increases werenot obtained for peer social amenitiesdirected to these subjects. Further,Betty's and Sarah's use of socialamenities declined to baseline levelsimmediately following the withdrawalof interventionno maintenanceoccurred.
1 {
REST COPY AVAILABLE
Descriptive studies corroborate
the notion that interactivevariables may be relatively
mcre important than discretebehavioral variables in the
assessment, description, andtreatment of social interactiondeficits among elementaryschool-aged children.
MIIIIIIIIIMMIIII1111111111111=1111111111111
CCBD Retrospective Series / 101oimummilmmi

Descriptive and *experimental
studies suggest the importanceof a bidirectional perspective inassessment of social behaviorfor elementary students withbehavioral disorders.
1=111111111111111111111111011111111.11
102 / CCBD Retrospective Seriesammismii
Kohler and Fowler (1985) thusconclude that peer reciprocity maycontribute to the entrapment of socialskills, and that such reciprocity maybe relatively more important thansocial responsiveness, or moretemporally related peer responses(e.g., positive response to socialinvitation). Further, these findingssuggest that specifi.; invitations toplay are more likely to becomeentrapped, or maintained by naturallyoccurring peer behavior, than areverbal compliments and amenities.
Summary. Taken together, thesedescriptive and experimental studiessuggest the importance of a bidirec-tional perspective in assessment ofsocial behavior for elementarystudents with behavioral disorders.Interaction variables (e.g., responsesfrom peers, ratios of initiations givento initiations received) more reliablydiscriminate behaviorally handi-capped children from nonhandi-capped classmates, and socialbehaviors associated with entrapmentor changes in social interaction aremore likely to be maintained or togeneralize to nontreatment settings.
At this time, we know relatively littleabout interactional variables andpossible entrapment effects in thesocial interactions of elementaryschoolaged children; we know moreabout the social behavior of preschoolchildren (Hops & Greenwood, inpress; Kohler & Greenwood, 1986;Strain et al., 1984). However, severalgroups of investigators have recentlybegun to examine possible entrap-ment effects within academicinteractions between elementaryschoolaged children and their peers(Kohler, Greenwood, & Baer, 1985) orteachers (McConnell, Lenkner,Szumowski, & Strain, 1985). In bothcases, researchers were able toproduce new interaction patternsassociated with increased rates ofacademic engagement. These recentanalyses offer important parallels to
work in child-child social interac-tion, and may possibly serve asprompts for continued work in thisarea.
Designing InterventionProcedures to PromoteEntrapmentIn addition to careful considerationin the selection of target behaviors,we may be able to promote theentrapment of social interaction skillsthrough the use of specific interven-tion procedures. Generally, theseprocedures must be designed toinitially increase rates of specifictarget behaviors through teacher-provided antecedents and/or conse-quences, and then remove these"artificial" elements of interventionin such a way that control overtargeted skills is transferred toreinforcing elements of interactionwith peers.
These treatment procedures mustfocus, to a large extent, on the peergroup as the target for intervention.Rather than assuming that interactivedifficulties are individual-specificand require change in some discretetarget behavior, this analysis ofentrapment suggests that treatmentprocedures directly target changes ininteractions between the target childand his or her peers. Assume, forexample, that observational measuresindicate a 4th-grade child exhibitsfew positive initiations to peers andfrequently responds negatively oraggressively to initiations from peers.Treatment based on a simple,individual-specific skill deficitmodel might include teacher praiseand/or tokens to increase positiveinitiations to peers, and a response-cost program to decrease negative oraggressive responses; both elementsof treatment would focus solely on thebehavior of the referred child. Anintervention to enhance entrapmentmay go further, however, to includedirect reinforcement of peer behaviors

associated with these targeted skills.For instance, a p,mup contingencycould be implemented whereby theentire play group is given access toadditimad freetime contingent onappropriate interaction rates of thereferred child. In this way, both thetarget child anti peers initiallyrecei,e direct, teacher-providedreinfmeement for increased rates t.fpositive initiations (i.e., the chili;initiates, peer responds) and de-.creased rates of negative respe;nses
from the child; after initial imple-mentation, this group contingencycan be faded and control transferredto new, more positive interactiverelationships between the. behavior ofthe target ehild and peers. Thus,treatment effectiveness is enhancedby attention to change', in both targetchild and peer behavior.
Recently, increased attention hasbeen devoted to group reinforcementcontingencies (Greenwood & Hops,1981) and other treatment procedures(Strain, 1981; Odom & Strain, 1984)that include peers in direct treatmentof social behavioral excesses ordeficits. These procedures holdparticular promise for enhancingentrapment of adaptive socialinteraction for at least three reasons.First, group-oriented contingenciescan be applied more effectively tointeractive aspects of children's socialbehavior'. In the example above, agroup-oriented contingency wasapplied to increase rate of positiveinteractions initiated by the targetchild; thus, a single reinforcementprogram increased both the targetchild's rate of positive initiations topeers and the likelihood of peers'
affirmative responses to theseinitat ions. Second, group-orientedcontingencies and other peer-mediated interventions provide aframework for creating interactionsthat will ultimately lead to entrap-ment of targeted social responses.Finally, t ;ing group-orientedcontinge cies and other peer-
mediated interventions enhancesentrapment through the directinvolvement of peers in the therapeu-tic process. Peers are expected tomaintain entrapped social behaviorsafter treatment is terminated. As aresult, the efficiency of interventionmay be increased by including thesepeers as early as possible in the
change program.
Group-oriented procedures that canbe expected to enhance entrapmentamong elementary school studentswith behavioral disorders arecurrently available in three standard-ized, empirically validated socialinteraction skills interventionprograms: RECESS (ReprogramingEnvironmental Contingencies forEffective Social Skills; Walker et al.,1978), PEERS (Procedures forEstablishing Effective RelationshipSkills; Hops et al., 1978), andACCEPIS (A Curriculum forEffective Peer and Teacher Skills;Walker et al., 1983). Each of theseintervenCon packages includes, orhas been adapted to include, treat-ment procedures that produce orenhance entrapment of adaptivesocial responding for behaviorallyhandicapped elementary schoolchildren. Each of these interventionpackages and their respectiveentrapment procedures is described
below.
RECESS. RECESS (Walker et al.,
1978) is a comprehensive behaviormanagement package designed to
decrease negative/aggressive behaviorand simultaneously increase positive,cooperative interaction of youngelementary schoolaged children.RECESS is designed to be imple-mented primarily in playgroundsettings, although the authors includeprocedures for extending programcomponents to classroom or othersituations. The intervention packageincludes four major components: (a)discrimination training, in whichreferred children are taught to
BEST COPY AVAILABLE
Treatment effectiveness isenhanced by attention to
changes in both target child
and peer behavior.
IMINI11111111111=11111111111=11NIIII
CCBD Retrospective Series / 103Immum=1
The original developers ofRECESS have carefully
evaluated the effectiveness ofindividual treatmentcomponents and the overalltreatment package.
104 / CCBD Retrospective S,3riesimommemmormiam
identify appropriate versus inappro-priate social behaviors: (b) a re-sponse-cost point system, implement-ed during daily freeplay activities toprovide direct decelerative conse-quences for negative or aggressivebehavior: (c) adult praise for positiveand/or cooperative interaction duringfreeplay periods; and (d) concurrentgroup and individual reinforcementcontingencies for child behaviorduring freeplay. As in many behaviorchange programs, this last reinforce-ment contingency provides points tothe child contingent on daily perfor-mance; these points can be ex-changed at home for one of severalindividual rewards. Additionally, thegroup-oriented contingency of thiscomponent provides the entireclassroom with freetime activitiescontingent on the daily performanceof the target child; in this way, peersreceive direct reinforcement forparticipating in interactions wherrythe child acquires, elaborates, orgeneralizes positive social behaviors.
The original developers of RECESShave carefully evaluated the effec-tiveness of individual treatmentcomponents and the overall treatmentpackage (Walker et al., 1978; Walker,Hops, & Greenwood, 1984). Twoparticular findings are of relevance tothe discussion here. First, Walkerand his colleagues found that adultattention, particularly praise, was inand of itself insufficient to produceimmediate or durable change in thebehavior of sovially negative oraggressive children; rather, theRECESS developers concluded thatcoercive interactions with peers, andultimately the social behavior of thesepeers, was an important component inthe maintenance of negative behaviorby referred children. Second, fieldtrails of RECESS suggested thatgroup-oriented contingencies, inwhich classroom peers "shared" inthe reinforcement of improvedperformance, increased the efficiency
of the entire intervention package(Walker et al., 1978).
In a more recent investigation,RECESS intervention procedureswere modified to increase peerinvolvement in ongoing treatment; asa result, we now have further evi-dence of possible entrapment effectswith RECESS. Dougherty, Fowler, andPaine (1985) modified stone ardRECESS procedures by appointingand training peer monitors for recessintervention periods. These peermonitors observed the target child'sbehavior throughout recess, awardingpoints for positive or exemplarybehavior and withdrawing points fornegative behavior or violations ofplayground rules. These points werethen exchanged, according to aprearranged criterion, for small groupactivities immediately followingrecess and for large group activitiesprovided once each week. Duringpeer monitoring treatment phases forDennis, the first child treated,classmates served as peer monitors.Subsequently, Dennis served as peermonitor for Ed, the second childtreated.
Peer monitors effectively maintainedinitial treatment effects obtainedwhen a consultant operated the recesspoint system, and produced generali-zation to previously untreated periodsfor both Dennis and Ed. In allinstances, negative interaction ratesdeclined to near-zero levels followingthe introduction of treatment. Inaddition, Dougherty and her col-leagues noted three other effectsparticularly relevant to the currentdiscussion. First, Dennis' negativeinteractive behavior in an untreatedrecess period declined significantlyto near-zero levelsfollowing hisappointment as Ed's peer monitor.Second, although Ed initiallyreceived treatment in only one ofthree daily recess periods, generaliza-tion occurred across two untreated

periods. Finally, reductions innegative peer initiations to Dennisand Ed were observed ',vial ill. Onsetof intervention. Th,.,se reductionswere similar to reductions to overallnegative behavior for nontreatedchildren following irtroduction of thepeer monitoring condition.
Together, data offered by Walker et al.(1978) and Dougherty et al. (1083)demonstrate that RECESS produceschanges in negative/social interactionthat are likely to be entrappedthrough reinforcement duringnaturally occurring interactions withpeers. Reduced levels of negativeinteraction and increased rates ofpositive interaction were maintained,at least to some extent, for severalchildren in original field tests(Walker et al., 1978), and for bothDennis and Ed (Dougherty et al.,1983). Additionally, Dougherty andher colleagues noted generalization ofintervention effects across untreatedconditions, behaviors, and childrenin their investigation. Finally, itappears that RECESS implementors,particularly in the Doughertyinvestigation, successfully targetbehaviors for both acceleration anddeceleration that are positivelyassociated with social behaviors ofpeers. While the evidence for thisfinal point is somewhat indirect,Dougherty and her colleaguesdocurremt two important, concurrentchanges: reduction in observednegative interaction rates for Dennisand Ed, accompanied by (a) applica-tion of simple peer monitoringprocedures in which childrenmonitored and provided feedback forthe behavior of their classmates, and(b) reductions in negative peerinitiations to the subjects as well asoverall negative peer behavior duringrecess periods.
PEERS. PEERS (Hops et al., 1978)was developed by the same teamresponsible for RECESS, and was
BEST COPY AVAILABLE
designed as a similarly comprehen-sive intervention package to increasethe social interaction rates of sociallywithdrawn children in kindergartenthrough 3rd grade. PEERS containsfour major program components: (a)social skills training, in which thereferred child is taught and givenopportunities to rehearse socialinitiations, responses to initiations,and strategies for continuing orextending interactions; (b) joint-taskactivities, in which the referred childand nonwithdrawn peers are givenopportunities to interact duringstructured activities; (c) a reinforce-ment point system for social interac-tion during recess, where pointsearned by the child are exchanged forclasswide activities; and (d) acorrespondence training procedure,in which the child is taught to .
describe accurately social behavioroccurring during preceding recessperiods, so that classroom teacherscan provide additional reinforcement.As with RECESS, the PEERSreinforcement point system includesan interdependent group contingen-cyreinforcement for the peer groupis provided contingent on thebehavior of one child (i.e., the childreceiving treatment), with peers"contributing" to points earned byinteracting with the child. In thisway, PEERS explicitly establishesand then systematically fades anartificial reinforcement contingencythat is designed to promote entrap-ment of social interaction.
Paine and his colleagues (1982)evaluated the effects of brief,repeated "booster sessions" ofPEERS intervention pmcedures onsubsequent maintenance of increasedrates of social interaction. Earlierwork (reported by Baer and Wolf,1970) had suggested that repeatedexposure to brief (e.g., 3 to 5 (lay)periods of intervention leads tomaintenance of higher rates of socialinteraction. Paine's group sought to
PEERS was developed by the
same team responsible forRECESS, and was designed
as a similarly comprehensive
intervention package toincrease the social interaction
rates of socially withdrawn
children in kindergarten
through 3rd grade.
CCBD Retrospective Series / 105

ACCEPTS was designed toteach critical social skills tochildren with mild andmoderate disabilities prior totheir full-time integration intoregular education settings.
111111111111111111111111111111111111111
106 / CCBD Retrospective Series
replicate and extend this earlierwork, evaluating the relative effects ofrepeated intervention for subjectswho had either completed interven-tion earlier or were being exposed tointervention for the first time.
Participating in this study were 9elementary-aged, socially withdrawnchildren; 5 of the children hadcompleted PEERS treatment 1 to 6months prior to this investigation,and had returned to low levels ofinteraction with peers. The remaining4 subjects had not received anytreatment for social withdrawal priorto their participation in this project.All participants received three 5-daysessions of intervention, interspersedwith baseline periods in which nointervention was provided. Interven-tion included the recess-based pointsystem, social skills training, jointtasks, and correspondence training asoriginally outlined in PEERS (Hopset al., 1978).
All subjects immediately andsignificantly increased their rates ofsocial interaction during eachintervention period. Addittonally, 5 ofthe 9 children (4 of whom hadpreviously received treatment)showed increased maintenance overthe courses of the study. Whilereversals were noted for interactionrates following each withdrawal oftreatment, the extent of these rever-sals declined across booster sessions.By the end of the third interventionperiod, all 5 children were interact-ing at normative rates in the absence
of explicit, teacher mediated rein-forcement. For these children, socialinteraction had come under thecontrol of naturally occurringreinforcers.
ACCEPTS. ACCEPTS (Walker et al.,1983) was designed to teach criticalsocial skills to mildly and moderatelyhandicapped children prior to theirfull-time integration into regulareducation settings. Three major
components make up ACCEPTS: (a)social skills training, a small-groupinstructional arrangement in whichchildren are taught to produce 24different skills for interacting withpeers in freeplay settings, and 4skills for interacting with teachers inacademic settings; (b) recess coach-ing, which combines adult-mediatedprompts and praise with a group-oriented contingency managementsystem to increase the use of criticalsocial skills during child-childinteraction; and (c) a classroom-based, individual specific contingen-cy management program to increase achild's appropriate interactions withteachers and overall adjustment to thedetnands of the classroom setting.
ACCEPTS draws heavily on proce-dures thought to facilitate entrap-ment. To the maximum extentpossible, target behaviors for thesocial skills training sequence wereselected that were empiricallyassociated with (a) positive responsesfrom peers, (b) appropriate interac-tion, or (c) more general measures ofpeer preference and social compe-tence. Further, social skills traininglessons were designed to leadchildren to mastery in the perfor-mance of specific skills prior toexposing these skills to reinforcementcontingencies in freeplay activities;in this way, children are more likelyto produce social responses ofsufficient quality that peers are morelikely to respond. Finally, nonhandi-capped peers from the target child'sregular education class are includedin social skills training lessons andrecess coaching. In this way, peerscan both provide positive models forthe target child, and can begin todevelop new skills for interactingwith that child in a wide variety ofsettings.
In one of the initial evaluations of theACCEPTS program (McConnell &Walker, 1983; Walker et al., 1983),the effects of social skills training

and recess coaching on a small set of"critical skills" was evaluated. Theseskills included positive initiations topeers, positive responses to peerinitiations, compliments, smiles, andtouches, and were selected on an apriori basis as being essentialcomponents for a more generalmeasure of social interaction.
Randomly assigned to treatment orcontrol groups were 20 mildlyhandicapped second to fifth gradestudents, identified by their teachersas lacking essential social skills.Children in the treatment groupreceived the total ACCEPT'S interven-tion package, including small groupsocial skills training, recess coach-ing, and classroom contingencymanagement in regular educationclassrooms: children in the controlgroup received only those servicesalready available in their resourcerooms. Observations were conductedfor all subjects prior to, during, andafter a 6-week intervention period.Results indicated that childrenreceiving treatment significantlyincreased their rates of positive"entrapment skills" during interven-tion, and that this increased rate wasmaintained at slightly lower levelsfollowing the termination of treat-ment. Unfortunately, these datarepresent group means, and are basedon observations completed severalweeks apart. As a result, it is difficultto describe specific changes in theinteractions of these children over thecourse of intervention or to offer moredetailed information on the mecha-nisms by which this maintenance wasobtained.
Summary.. RECESS, PEERS, andACCEPTS each appear to incorporateintervention procedures associatedwith entrapment of social interactionskills for elementary school studentswith behavioral hamlicaps. Each ofthese intervention programs wasoriginally designed, and in one casehas been further adapted, to specifi-
cally include peers in the ongoingtreatment of social behavior excessesor deficits. Inclusion of peers leadsdirectly to changes in child-childinteraction that are likely to supportmore adaptive interaction long afterintervention is ended.
To some extent, maintenance effectsassociated with each of these inter-vention programs offers tentativeevidence that new, more adaptiveresponses of behaviorally handi-capped children are coming underthe control of naturally occurring,peer-mediated reinforcers. However,as Kohler and Greenwood (1986)have shown, maintenance of behaviorchange is but one part of a morecomplete proof for the existence ofentrapment. Future research, particu-larly more detailed analyses ofchanges in child-child interactionsduring any or all of these interven-tions, can be expected to more clearlydescribe the processes of entrapment,as well as to increase the efficiencyand effectiveness of social behavioralinterventions with children.
CONCLUSION
Children are referred for social skillstraining because, at least in pan, theyfail to demonstrate competence intheir interactions with peers. Histori-cally, these problems have beenconceptualized as social skilldeficits: The child does not exhibitspecific skills (e.g., social initia-tions), or does not exhibit these skillsat appropriate frequencies. However,social interaction is a reciprocal,bidire( Ilona] process. As a result,changes in the social behavior of onechild may often require changes inthe associated social behavior ofothers, such as peers in a child'sclass.
Entrapment is a process throughwhich the social lwhavior of onechild comes wider the control ofnaturally occurring reinforcers. In
1 I
UST COPY AVAILABLE
Changes in the social behavior
of one child may often requirechanges in the associatedsocial behavior of others, such
as peers in a child's class.
CCBD Retrospective Series / 107

Emphasis on entrapment leads
to a reconceptualization for ourdefiraion of social skillstraining.
1111111111111111111111111111=1111111111
108 / CCBD Retrospective Series
particular, entrapment can occurwhen changes in the social behaviorof one child are reinforced by thesocial behavior of others duringinteractions in naturalistic settings.When this type of entrapment occurs,we expect newly-acquired socialbehaviors to continue at high ratesand to generalize to new settings orbehaviors long after intervention isterminated.
To produce this entrapment of moreadaptive social skills, we must payparticular attention to both theselection of target behaviors and theuse of intervention tactics that reflectthe interactive nature of child-childsocial behavior; in particular, wemust work to create social interac-tions that naturally provide reinforce-ment for the continued use andelaboration of recently acquiredskills. As such, emphasis on entrap-ment leads to a reconceptualizationfor our definition of social skillstraining.
Research on entrapment effects insocial skills assessment and trainingwith behaviorally handicappedelementary school students is clearlyin its infancy. At this point, we havesome evidence that entrapmentoccurs (e.g., Baer & Wolf, 1970;Dougherty et al., 1985; Kohler &Greenwood, 1986). However, contin-ued systematic inquiry is still neededto more fully describe the process ofentrapment, and to more carefullyinclude procedures that foster thisprocess in our social behaviorinterventions. The results of thisresearch can 1-ye expected to dramati-cally increase the power and efficien-cy of interventions for children withbehavioral handicaps.
REFERENCES
Baer, D. M., & Wolf, M. M. (1970). Theentry into natural communities ofreinforcement. In R. Ulrich, TStachnik, & J. Mabry (Eds.), Control
1 4
of human behavior. Glenview, IL:Scott-Foresman.
Bornstein, M., Bellack, A. S., & Hersen,M. (1980). Social skills training forhighly aggressiVe children: Treatmentin an inpatient psychiatric setting.Behavior Modification, 4, 173-186.
Bryan, T. H. (1974). An observationalanalysis of classroom behavior ofchildren with learning disabilities.Journal of Learning Disabilities,7(10), 26-34.
Cartledge, G., & Milburn, J. (1980).Teaching social skills to children:Innovative approaches. New York:Pergamon.
Charlesworth, R., & Hartup, W. W.(1967). Positive social reinforcementin the nursery school play group.Child Development, 38, 993-1002.
Dodge, K. A. (1 983). Behavioralantecedents of peer social status.Child Development, 51, 162-170.
Dougherty, B. S., Fowler, S. A., & Paine,S. C. (1985). The use of peer monitorsto reduce negative interaction duringrecess. Journal of Applied BehaviorAnalysis, 18, 141-153.
Foster, S. L., & Ritchey, W, L. (1979).Issues in the assessment of socialcompetence in children. Journal ofApplied Behavior AnalysLs, 12, 625-638.
Foster, S. L., & Ritchey, W. L. (1985).Behavioral correlates of sociometricstatus of fourth-, fifth-, and sixth-grade children in two classroomsettings. Behavioral Assessment, 7, 79-93.
Green, K. D., Vosk, B., Forehand, R.,Beck, S. J., & Vosk. B. (1980). Anassessment of the relationshipbetween measures of children's socialcompetence and children's academicachievement. Child Development, 51,1149-1156.
Greenwood, C. R., & Hops, H. (1981).Croup-oriented contingencies andpeer behavior change. In P S. Strain(Ed.), The utilization of classroompeers as behavior change agents (pp.189-259). New York: Plenum.
Greenwood, C. H., Todd, N. M., Hops, H.,& Walker, H. M. (1982). Behaviorchange targets in the assessment andmodification of socially withdrawnpreschool children. BehavioralAssessment, 4, 273-297.
Greslmin, F. M. (1986). Concejaual anddefinitiona! issues in the assessment

of children's social skills: Implicationsfor classification and treatment.Journal of Clinical Child Psychology,15, 3-15.
Hartup, W. W. (1983). The peer system.In P H. Mussen (Series Ed.) and E.M. Hetherington (Vol. Ed.), Handbookof child psychology (4th ed.): Tbl. 4.
Socialization, personality, aml socialdevelopment (pp. 103-196). New York:Wiley.
Hops, H. (1982). Social skills training forsocially isolated children. In P Karoly& J. Steffen (Eds.), Enhancingchildren's social competencies.lxxington, MA: Lexington Books.
Hops, H., Finch, M., & McConnell, S.(1985). Social skills deficits. In P H.Bornstein & A. F,. Kazdin (Eds.),Handbook of clinical behavior therapywith children (pp. 543-598). Home-wood, IL: Dorsey.
Hops, H., & Greenwood, C. R. (1981).Social skills deficits. In E. J. Mash &L. C. Terdal (Eds.), Behavioralassessment of childhood disorders.New York: Guilford.
Hops, H., & Greenwood, C. R. (in press).Social skills deficits. In E. J. Mash &f., C. Terdal (Eds.), Behavioralassessment of childhood disorders 2nded.). New York: Guilford.
Hops, H., Guild. J. J., Fleischman, D. H.,Rune, S. C., Street, A., Walker; H. M.,& Greenwood, C. R. (1978). PEERS(Procedures fir Establishing EffectiveRelationship Skills): Manual forconsultants. Unpublished manuscript,University of Oregon, Center atOregon for Behavioral Education ofthe Handicapped, Eugene.
Kauffman, J. M. (1985). Characteristics ofchildren's behavior disorders (3rd ed.).Columbus, Oli: Merrill.
Kohler; F. W.. & Fowler, S. A. (1985).Training prosocial behaviors to youngchildren: An analysis of reciprocitywith untrained peers. Journal ofApplied Behavior .4nalysis, 18, 187-
200.Kohlei; F. W. & Greenwood, C. R.
(1986). Toward a technology ofgeneralization: The identification ofnatural contingencies of reinforce-ment. The Behavior Analyst, 9. 19-26.
)(Alm E W., Greenwood, C. R., & Baer,D, M. (1985, May). Assessing the peertutoring process: The identification ofnatural communities of socialreinforcement. Palwr presented at the
annual meeting of the Association ofBehavior Analysis, Columbus, OH.
McConnell, S. R. (1982). lderuilicauon ofsocial skills for handicapped boys:Evaluation of teacher rating, peersociometric, and direct observationmeasures. Unpublished doctoraldissertation, University of Oregon.
McConnell. S. R., Lenkner, D.A.,Szumowski, E.,& Strain, P S. (1985,May). Effects of child academicbehavior on rates of contingent teacherattention: Entry into a complexcommunity of reinforcement. Paper
presented at the annual meeting of theAssociation for Behavior Analysis,Columbus, OH.
McConnell, S. R., Strain, P S., Kerr, M.M.. Stagg, V, Lenkner, D. A., &Lambert, D. L (1984). An empiricaldefinition of school adjustment:Selection of target behaviors for acomprehensive treatment program.Behavior Modifwation, 8, 451-473.
McConnell, S. R., & Walker, H. M.(1983, May). Peer-mediated behaviorchange within a standardized socialskills curriculum. Paper presented atthe annual meeting of the Associationfor Behavior Analysis, Milwaukee,WI.
Odom, S. L., & Strain, P S. (1984). Peer-mediated approaches to increasingchildren's social interactions: Areview. American Journal qf Ortho-psychiatry; $4. 544-557.
Paine, S. C., Hops, H., Walker, H. M.,Greenwood, C. R., Fleischman, D. H.,& Guild, J. J. (1982). Repeatedtreatment effects: A study of maintain-ing behavior change in sociallywithdrawn children. BehaviorModyication, 6, 171-199.
Patterson, G. R. (1 982). Coercive family
processes. Eugene, OR: Castalia.Schloss, P J., Sehloss, C. N., Wood, C. E.,
& Kiehl, W. S. (1986). A criticalreview of social skills research withbehaviorally disordered students.Behavioral Disorders. 12, 1-14.
Stokes, T. E, & Baer, D. M. (1977). Animplicit technology of generalization.Journal of Applied Behavior Analysis.9, 349-367.
Stokes, T. F, & Osnes, P C. (1986).Programming for the generalization ofchildren's social behavior. hi P S.
Strain, M. J. Curalnirk, & H. M.Walker (FAls.), Childre0 wrialbehavior: Development, assessment,
I
BEST COPY AVAILABLE
CCBD Retrospective Series / 109smoms

110 / CCBD Retrospective SeriesoniimmisnimiONMEMM
and modification. Orlando, FL:Academic Press.
Strain, P S. (Ed.). (1981). The utilizationof classroom peers as behavior changeagents. New York: Plenum.
Strain, P S. (1983). Identification ofsocial skill curriculum targets forseverely handicapped children inmainstream preschools. AppliedResearch in Mental Retardation, 4,369-382.
Strain, P S., Odom, S. L., & McConnell,S. R. (1984). Promoting socialreciprocity of exceptional children:Identification, target behaviorselection, and intervention. Remedialand Special Education, 5, 21-28.
Strain, P S., & Shores, R. E. (1977).Social reciprocity: Review of researchand educational implications.Exceptional Children, 43, 526-531.
Tremblay, A., Strain, P S., Hendrickson,J. M., & Shores, R. E. (1981). Socialinteractions of normally developingpreschool children: Using nonnativedata for subject and target behaviorselection. Behavior Modification, 5,237-253.
Van Hasselt, V. B., Hersen, M., White-hall, M. B., & Bellack, A. S. (1979).Social skills assessment and trainingwith children: An evaluative review.Behavior Research and Therapy, 17,413-437.
Walker, H. M., Greenwood, C. R., Hops,H., & Todd, N. M. (1979). Differentialeffects of reinforcing topographiccomponents of social interaction:Analysis and systematic replication.Behavior Modifwation, 3, 291-321.
1
Walker, H. M., Hops, H., & Greenwood,C. R. (1984). The CORBEH researchand development model: Program-matic issues and strategies. In S. C.Paine, G. T. Bellamy, & B. Wilcox(Eds.), Human services that work:From innovation to standard practice(pp. 57-77). Baltimore, MD: Brookes.
Walker, H. M., McConnell, S. Ft., &Clarke, J. Y. (1985). Social skillstraining in school settings: A modelfor the social integration ofhandicapped children in lessrestrictive settings. In R. J.McMahon & R. DeV. Peters (Eds.),Childhood disorders: Behavioral-developmental approaches. NewYork: Bruner-Mazel.
Walker, H. M., McConnell, S. R., Walker,J., Holmes, D., Todis, B., & Golden,N. (1983). ACCEPTS: A Curriculumfor Effective Peer and Teacher Skills.Austin, TX: Pro-Ed.
Walker, H. M., Street, A., Garrett, B.,Crossen, J., Hops, H., & Greenwood,C. Ft. (1978). RECESS (ReprogramingEnvironmental Contingencies forEffective Social Skills): Manual forconsultants. Unpublished manuscript,University of Oregon, Center atOregon for Behavioral Education ofthe Handicapped, Eugene.
Warreafeltz, R. B., Kelly, W. J., Salzberg,C. L., Beegle, C. P. Levy, S. M.,Adams, T. A., & Crouse, T. R. (1981).Social skills training of behaviordisordered adolescents with self-monitoring to promote generalizationto a vocational setting. BehavioralDisorders, 7, 18-27.

Structured Learning UsingSelf-Monitoring to PromoteMaintenance and Generalization ofSocial Skills Across Settings for aBehaviorally Disordered Adolescent
Cheryl Strobel KiburzSidney R. MillerLonny W. Morrow
ABSTRACT: Recent literature has highlighted the importance of teaching so-cial skills to behaviorally disordered adolescents. Although it has been demon-strated that social skills can be taught to this population, skills maintenanceand generalization have remained problematic. Using a rnultiple baseline-
across-behaviors design, the present investigation incorporated techniques de-signed to facilitate maintenance and generalization of skills. This study in-volved an 18-year-old youth placed in a residential state mental health facil-ity because of social skills deficits that included greetings, initiating conversa-tion, and thanking behavior. The treatment occurred over a 48-dayperiod in
which the student was observed in four distinct settings. Results suggest that
the skills trainedgreetings and thanking behaviorwere maintained andgeneralized to three natural settings: (a) the route the student walked to theclassroom, (b) the student lounge located near the classroom, and (c) a voca-tional setting located within walking distance of the classroom. Training also
produced an incidental increase in the skill initiating conversation.
With the increased emphasis on vocational training and communityplacement, the need to teach appropriate social skills to behaviorallydisordered adolescents is becoming essential. As Adams, Strain, Salzberg,
and Levy (1979) observed, social skills are nec3ssary in those settings in
which individuals are required to interact with others (e.g., school, work,
and community). Failure in job placement is often linked to poor social-
interpersonal skills rather than inadequate specific job skills (Kochany &
Keller, 1980). In all, a growing body of literature substantiates the fact
that social skills are imperative for successful employment of behaviorally
disordered adolescents (Foss & Peterson, 1981).
There have been a variety of approaches used to teach social skills tononhandicapped and handicapped populations. Studies have tested theeffects of manipulating antecedents (Ballard, Gorman, Gottlieb, & Kauf-
man, 1978; Shores, Hester, & Strain, 1976; Strain & Timm, 1974),consequences (Buell, Stoddard, Harris, & Baer, 1968; Mayhew, Enyart, &
Reprinted from Behavioral
Disorders, Vol. 10, Number 1,
November 1984, pp. 47-55.
imiiimmommis
CCBD Retrospective Series / 111IMMIIIM111=111i

One method to promotemaintenance and
generalization is the use ofself-monitoring.
1111111111MNIM111111=11111=111111111111111111111
112 / CCBD Retrospective SeriesImilimi=1
Anderson, 1978; Walker, Greenwood,Hops, & Todd, 1979), the use ofmodeling (Marburg, Houston, &Holmes, 1976; O'Connor, 1969,1972), and cognitive behavioraltechniques (Gresham & Nagle, 1980;Meichenbaum, 1977; Zahavi &Asher, 1978). Further, Goldstein,Sprafkin, Gershaw, and Klein (1983)reported a structured learningstrategy as effective in training socialskills with a wide variety of popula-tions including those dencribed asaggressive, withdrawn, immature, ordevelopmentally delayed. However, inspite of the effectiveness of theseprocedures for promoting skillsacquisition, few studies havedemonstrated maintenance andgeneralization of the skills trained(Gresham, 1981).
One method being investigated topromote maintenance and generaliza-tion is the use of self-monitoring(O'Leary & Dubey, 1979) in which anindividual is responsible for system-atically monitoring and recording his/her own performance of certainbehaviors (Workman, 1982). Forexample, self-monitoring procedureswere incorporated in treatmentsdesigned to increase both academicand social behavior (Turkewitz,O'Leary, & lronsmith, 1975) and insocial skills training programs(Warrenfeltz, Kelly, Salzberg, Beegle,Levy, Adams, & Crouse, 1981).Turkewitz et al. (1975) combined amodified token program with self-monitoring to increase academic andsocial behavior of eight disruptiveyouth. The skills were not generalizedto a new setting and maintenance wasobserved only in the regular class-room across subject areas. In theWarrenfehz et al. (1931) study, fourbehaviorally disordered adolescentsparticipated in a vocationally orientedsocial skills training program. Thefirst procedure consisted of didacticinstruction and resulted in noconcomitant change in most of thestudent's interpersonal behavior in
1
the generalization setting (i.e.,vocational training room). A subse-quent intervention, role-playing andself-monitoring, was implementedand the targeted social skills general-ized to the vocational training site.However, since the role-play and theself-monitoring procedure wereimplemented simultaneously, theirseparate effect could not be isolatedand measured. These findingssuggest that self-monitoring facili-tates maintenance and generalizationof social skills trained followingtermination of the intervention.Further research is needed toreplicate these results and extricatethe individual contributions of eachtreatment component.
The present study investigated theseparate effects of structy.red learning(using modeling, role-playing, andperformance feedback) and self-monitoring procedurei on promotingmaintenance and generalization ofsocial skills across settings with aseverely behaviorally disorderedadolescent.
METHODOLOGY
Subject
The subject was an 18-year-oldCaucasian male resident of a mentalhealth and development centerlocated in southern Illinois. He wasadmitted to the center at the age of15. His behavior at admissionconsisted of aggressive acts (e.g.,striking others and damagingproperty), chronic bizarre behaviors(e.g., eating soap, drinking shampoo),yelling and cursing for no apparentreason, and poor peer and staffinteractions. A 3-year-old psychologi-cal evaluation reported him as mildlyretarded based on an IQ of 60(WAIS-11). A recent psychologicalreported identified the student as tooemotionally disturbed to submit tostandardized testing. He receiveddaily instruction in reading, math-
ematics, spelling, writing, domestic,and vocational skills in classroomand vocational settings.
Settings
The study was conducted in fourdifferent settings. Social skillsinstruction occurred in a classroomthat served five other seriouslybehaviorally disordered adolescents.Small group instruction was providedby a female, certified specialeducation teacher. Generalizationprobes took place in three settings:(a) the route the student walked to theclassroom, (b) the student loungelocated near the classroom, and (c) avocational setting located withinwalking distance of the classroom.
Behavioral Definitions
Behaviors selected for interventionwere based on the results of subjec-tive evaluation, a procedure withestablished precedent in naturalisticsettings (Kazdin, 1982). This processconsisted of obtaining opinions ofpersons knowledgeable about thebehavior patterns of behaviorallydisordered persons and/or who werefamiliar with the student. Specifi-cally, the classroom teacher, programmanager, supervisor, and classroomaide were asked to evaluate thestudent's social skills and to priori-tize those in need of immediateremediation. Following identification
.of those social skills to be trained(e.g., greetings, thankings, andinitiating conversation), criteria toscore each appropriate social behaviorwere defined (see Appendix).
Assessment
Before training was initiated,baseline data were gathered todetermine the number of behaviorsthe student (a) was able to verbalizefor cach targeted response, and (b)could perform for each targetedresponse. To determine the student'sexisting repertoire of social behavior,
BEST COPY AVAILABLE
he was asked to discuss the steps toperform the targeted skills. Second,his ability to perform the targetedskills was assessed by presentingsituations similar to real life thatrequired him to perform the targetedskills. Training continued until hehad achieved 100% mastery andperformance was stable in bothassessment areas. No feedback orreinforcement for correct answers orperformance was provided.
Assessment data were gatheredcontinuously at the three generaliza-tion sites (i.e., the route the studentwalked to the classroom, the studentlounge, and the vocational setting) for20 min daily. Trained observersrecorded the appropriate or inappro-priate performance of each targetedskill. Since the data gathered at thegeneralization sites were collected insettings not subject to examinercontrol, the frequency of opportuni-ties to exhibit the behavior variedaccording to the social situation. Toreflect the proportion of appropriateresponses to the number of opportu-nities to respond over time, percent-age measures were obtained bycounting both the number of opportu-nities for the behavior to occur andthe number of appropriate responses,and then dividing that count by thetotal opportunities (Gentry & Haring,1976). A percentage scale wasutilized to equalize the data (Repp,1979).
Training
Training took place in the classroomduring 30-min sessions of structuredlearning consisting of four majorcomponents: (a) modeling, (b) role-playing, (c) performance feedback,and (d) transfer of training; these aredescribed as follows:
Modeling. Teaching the social skillbegan by exposing the subject, withina small group, to controlled appropri-ate examples of the skill being
"
Social skills instructionoccurred in a classroom that
served five other adolescents
with serious behavioraldisorders.
111111111119111111111111
CCBD Retrospective Series / 113slommommilmmomm

A multiple baseline design
across skills combined with
withdrawal features wasemployed to evaluate
intervention effectiveness andresponse maintenance.
MIIIIIIMINI1111111111111111
114 / CCBD Retrospective Series
exhibited by the teacher. Each skillwas taught separately and themodeling process depicted severalexamples of the skill used in differ-ent situations. To make the presenta-tions as concrete as possible, the skillwas broken down into componentbehavioral steps and illustrated in themodeling.
Role-playing. Following the presenta-tion of modeling, a group discussionensued. The group was urged tocomment on what they saw and heardand to relate the behaviors to theirown lives. From the informationgenerated in the discussions, role-plays were developed. Each studentwas given the opportunity to role-playor practice the skills taught as arehearsal for situations similar to reallife. The student then had theopportunity to be the principle modeland re-enact the modeled skill.During the role-play, support andcoaching were provided.
Performance feedback. Following therole-play, the teacher elicitedperformance feedback (i.e., praise,compliments, approval, constructivecriticism) from the group members.In this component, the s!'..lent wasgiven support as well as constructivesuggestions for improving hisperformance.
Transfer of training. In the classroomsetting, structured social learningincluded modeling, role-playing, andperformance feedback instruction.Self-monitoring was implemented ina later phase to determine theseparate effects of this instructionaltechnique on maintenance ahdgeneralization across settings. Thestudent was taught the skill of self-monitoring in the same fashion as thetargeted social skills. The trainerbegan by modeling self-monitoring,followed by role-playing and perfor-mance feedback. The student was
then provided a self-monitoring form.The trainer asked the student to takethe self-monitoring form with him atthe beginning of each day and torecord, by circling a number, eachtime he performed the targeted skillappropriately. The student used self-monitoring at each generalizationsite. Staff members were informedthat the student would be monitoringhis own behavior at these specifiedsites. He was asked to bring hismonitoring form to the subsequentclassroom where it was discussed. Hereceived social reinforcement forreturning and completing the form.
o
Next, a reinforcement contingencywas added to the self-monitoringprocedure based on a reinforcementsurvey that revealed tangible rein-forcers and social activities, such asgoing to a local restaurant, were themost reinforcing events. In thisphase, the student continued thesame self-monitoring procedure, butthis time the forms were discussed inan evaluative manner with pointsassigned according to the number oftimes he performed the skill appro-priately. A changing criterion for thenumber of points to be accumulatedduring each period of time wasimposed according to his previousperformance.
Evaluation Design
A multiple baseline design acrossskills combined with withdrawalfeatures was employed to evaluateintervention effectiveness andresponse maintenance (Rusch &Kazdin, 1981). Intervention beganwith the first three components of thestructured learning approach,followed by the fourth component,transfer of training, which in thisstudy was self-monitoring. Next, self-monitoring with reinforcement wasimplemented, followed again by self-monitoring and then a return tobaseline conditions.

Reliability
Two college students served asobservers and were trained simulta-neously and independently to observetargeted social skills in role-playsituations similar to real life.Interobserver agreement was calcu-lated by dividing the larger numberof appropriate responses by thesmaller and multiplying by 100 toprovide a percentage score. Thismethod has been labeled the WholeSession Method (Repp, 1979).
RESULTS
Reliability in the generalizationsettings was assessed at least once aweek throughout the study (12 days),and was based on a mark-by-markcomparison of data collected by thetwo observers. The mean inter-observer agreement for the skillgreeting was 87% (range 83-100%);for thanking, 90% (range 75-100%);while for conversation it was 97%(range 80-100%).
During the baseline condition, thestudent's behavior was characterizedby low mean percentages of appropri-ate social skills at the generalizationsettings. The mean percentage rangedfrom 13-41% for greetings, 8-24%for thankings, and 40-57% forinitiating conversation, respectively.
Training began by employing threecomponents of the structured learningprocess (modeling, role-playing, andperformance feedback) for each skill.The student received training on eachtargeted skill until he was able toverbalize the steps with 100%accuracy and performance was stableHe was also required to role-play theappropriate use of the skill indifferent situations with 100%accuracy. The student required eightsessions to reach criterion for eachskill, for both knowing the behavioralcomponents and performing the skillin role-play situations. During this
phase, the student's mean percentageof appropriate skills also increasedwhen compared to baseline condition;ranging between 49-61% for greeting,32-57% for thanking, and 53-67%for initiating conversation, respec-tively.
Following the training phase a self-monitoring phase, in which thestudent was taught self-monitoringutilizing the same procedure used toteach the targeted social skills, wasimplemented. Training continueduntil 90% criterion was met andstable. He reached criterion in fourself-monitoring sessions involvinggreeting and in two self-monitoringsessions involving thanking. Asbefore, during this phase the studentperformed the skills appropriatelywith mean percentages ranging from51-63% for greeting, 48-70% forthanking, and 62-70% for initiatingconversation.
The next phase included a reinforce-ment contingency added to the self-monitoring procedure. The range ofmean percentages for performance forgreetings were 71-89%; for thanking,58-100%; while for initiatingconversation, they were 69-97%across settings.
Following self-monitoring withreinforcement, a return to self-monitoring was implemented. Thestudent maintained a higher meanpercentage of appropriate skillperformance than the training phasebut the mean pt reentages of appro-priate performance did decrease fromthe self-monitoring with reinforce-ment phase (see Figures 1 and 2).The mean percentages of this phaseranged from 71-77% for greeting, 64-79% for thanking, and 77-84% forinitiating conversation.
The final phase included a return tobaseline in which a higher meanpercentage of appropriate social
L ;1
The student received training
on each targeted skill until he
was able to verbalize the steps
with 100% accuracy andperformance was stable.
CCBD Retrospective Series / 115

The effects of structuredlearning and self-monitoring
were isolated and measured todetermine their impact on themaintenance andgeneralization of social skillstrained.
11=1111111111111111=111111111MIIIIMMINIIIIIMIIM
116 / CCBD Retrospective Series
skills compared to preceding phasesof the study was evidenced. Datawere available for greeting onlybecause of changes in the student'sdaily schedule. The mean percentageof appropriate performance ofgreeting ranged from 91-95%.
Generalization data are presented onthe route the student walked to theeducational center (Figure 1), thestudent lounge (Figure 2), and thevocational center (Figure 3), respec-tively. (The figures display thepercentage of appropriate perfor-mance of each skill according to thenumber of opportunities provided inthe natural setting.) The figures showthat the student's generalizationperformance was greatest when self-monitoring was paired with reinforce-ment. When reinforcement waswithdrawn and only self-monitoringwas utilized, the student's generaliza-tion performance maintained at ahigher mean percentage compared tothe baseline condition.
DISCUSSION
This study sought to expand on theearlier studies of Turkewitz et al.(1975) and Warrenfletz et al. (1981).Unlike these investigations whichutilized a combination of proceduresto increase appropriate socialbehavior, in this study the effects ofstructured learning and self-monitor-ing were isolated and measured todetermine their impact on themaintenance and generalization ofsocial skills trained. In addition, theeffectiveness of self-monitoringprocedures combined with reinforce-ment was explored.
The structured learning process(modeling, role-playing, and perfor-mance feedback) resulted in a rapidacquisition of new social skills.Although generalization of socialskills to other settings occurred, itwas at a lesser extent than occurredwhen self-monitoring was implement-
ed. The greatest level of appropriateperformance was reached when self-monitoring with reinforcement wasutilized. Withdrawal of treatmentresulted in the maintenance of socialskills taught at a higher level thanwas attained prior to training, but alesser level than reached during thereinforcement and self-monitoringphases.
The similarity of data points betweenthe two skills of greeting and initiat-ing conversation is noteworthy.Although no interventions wereimplemented for the skill initiatingconversation, the interventionsimplemented for greeting apparentlyhad an effect on this skill. Thissimilarity may have been, in part, theresult of the overlap of these twosocial behaviors.
Before implementing the self-monitoring phase of the study,researchers had briefly informedstaff members at the three generali-zation settings about the socialskills being taught and alsoexplained the self-monitoringprocess. Although cooperative, infuture studies it would be benefi-cial to provide training to staffmembers at these sites. The trainingshould consist of the followingcomponents: (a) instruction on thebehavioral steps of the skillstrained, (b) training of how tomodel the skill appropriately, and(c) instruction in how to provide.social reinforcetnent to the studentfor appropriate performance of theskill. Training of personnel wouldprovide continuity of expectationsacross generalization settings andmight facilitate the generalization ofappropriate performance of theskill.
In applied research, ideal opportu-nities lot data collection are notalways available due to the variabil-ity of conditions in naturalisticsettings. This study was limited in

75
so
25
25 311 35 45 45 55
5 IS 15 20 25 30 35 40 45 50Osys
PERCENTAGE OF APPROPRIATESOCIAL SKILLS WALKING TO THE EDUCATIONAL CENTER
Figure 1. Percentage of greeting, thanking, and conversational skillsdisplayed while walking to the educational center.
terms of an ability to controlantecedent conditions during datacollection phases of the project. Forthis reason, data were converted topercentages based upon studentresponse in relationship to opportu-nity to respond, allowing for a moreaccurate assessment of studentperformance, facilitating monitoringof student progress, and interpreta-tion of final results. Still, Cooper(1981) has cautioned that percentage
data should be interpreted judicious-ly to avoid overrepresentation.
Future studies are necessary todetermine the consistency of effectsacross different subjects and acrossa broader range of targeted socialskills. Finally, it would be benefi-cial to measure the generalizationand maintenance of the targetedsocial behaviors in a wider array ofenvironmental settin rs.
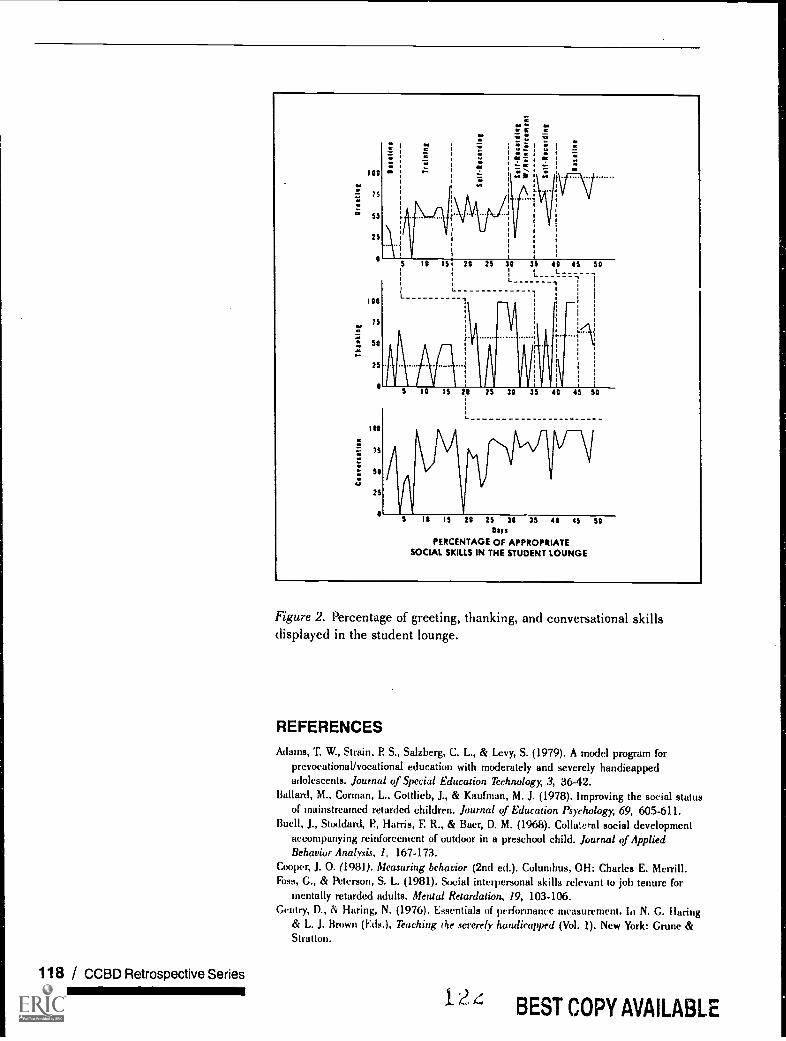
118 / CCBD Retrospective SeriesminimimilmmoNE
100
7 5
50
25
100
75
50
25
100
75
50
25
\\
29 25 3,0 35 40 45 50L
t.
1
10 tS 20 25 30 35 40 45 50
10 15 20 25 30 35 40 45 50Rays
PERCENTAGE OF APPROPRIATESOCIAL SKILLS IN THE STUDENT LOUNGE
Figure 2. Percentage of greeting, thanking, and conversational skillsdisplayed in the student lounge.
REFERENCES
Adams, T. W., Strain, P S., Salzberg, C. L., & Levy, S. (1979). A model program forprevocationallvocational education with moderately and severely handicappedadolescents. Journal of Special Education Techrwlogy, 3, 36-42.
Ballani, M.. Corman, L, Gottlieb, J., & Kaufman, M. J. (1978). Improving the social statusof mainstreamed retarded children. Journal of Education Psychology, 69, 605-611.
Buell, J., Stoddard, P, Harris, F. R., & Baer, D. M. (1968). Collateral social developmentaccompanying reinforcement of outdoor in a preschool child. Journal of AppliedBehavior Analysis. 1, 167-173.
Cooper, J. 0. (198)). Measuring behavior (2nd ed.). Columbus, OH: Charles E. Merrill.Foss, G., & Peterson, S. L. (1981). Social interpersonal skills relevant to job tenure for
mentally retarded adults. Menuil Retardation, 19, 103-106.Gentry, D., & Haring, N. (1976). Essentials of performance measurement. hi N. G. Haring
& L. J. Brown (Eds.), Teaching the severely handicapped (Vol. 1). New York: Crune &Stratton.
12BEST COPY AVAILABLE
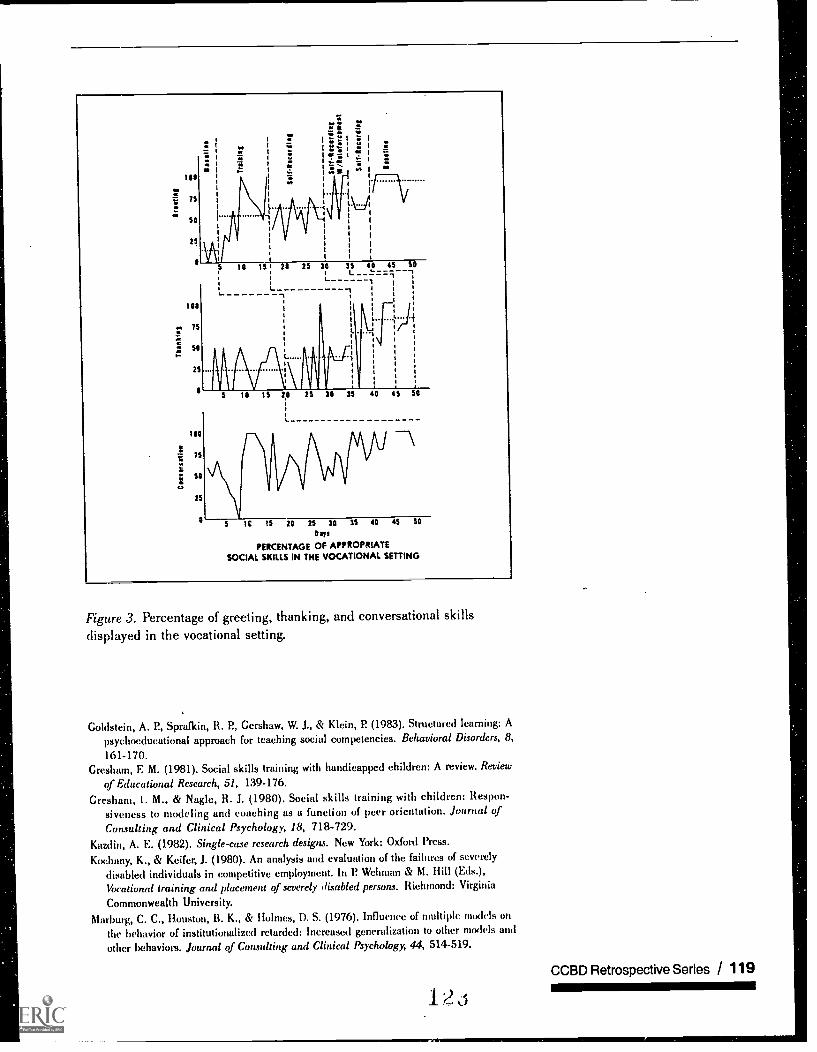
25
75
/It
50
25
L.
"
t\:.}
20 25 30 35 40 45 50L
1
-t
5 10 15 20 25 30 35 40 45 50
25
5 IC 15 20 25 30 35 40 45
ays
PERCENTAGE OF APPROPRIATESOCIAL SKILLS IN THE VOCATIONAL SETTING
50
Figure 3. Percentage of greeting, thanking, and conversational skillsdisplayed in the vocational setting.
Goldstein, A. P, Sprafkin, R. P, Gershaw, W. J., & Klein, P (1983). Structured learning: A
psychocducational approach for teaching social competencies. Behavioral Disorders, 8,161-170.
Gresham, F. M. (1981). Social skills training with handicapped children: A review. Review
of Educational Research, 51, 159-176.Gresham, 1. M., & Nagle, R. J. (1980). Social skills training with children: Respon-
siveness to modeling and coaching as a function of peer orientation. burnal ofConsulting and Clinical Psychology, 18, 718-729.
Kazdin, A. E. (1982). Single-case research designs. New York: Oxford Press.Koehany, K., & Keifer, J. (1980). An analysis and evaluation of the failures of severely
disabled individuals in competitive employment. In P Wehman & M. Hill (Eds.),
Vocatiorml training and placement of severely disabled persons. Richmond: Virginia
Commonwealth University.Marburg, C. C., Houston, B. K., & Holmes, D. S. (1976). Influence of multiple models on
the behavior of institutionalized retarded: Increased generalization to other models and
other behaviors. Journal of Consulting and Clinical Psychology, 44, 514-519.
CCBD Retrospective Series / 119
i2 i

Mayhew, G. L, Enyart, P, & Anderson, J.(1978). Social reinforcement and thenaturally occurring social responses ofseverely and profoundly retardedadolescents. American Journal ofMental Deficiency, 83, 164-170.
Meichenbaum, 0. H. (1977). Cognitive-behavior 1710dification: An integrativeapproack New York: Plenum Press.
O'Connor, R. D. (1969). Modification ofsocial withdrawal through systematicmodeling. Journal of Applied BehaviorAnalysis, 2, 15-22.
O'Connor, R. D. (1972). Relative efficacyof modeling, shaping, and thecombined procedures for modificationof social withdrawal. Journal ofAbnormal Psychology, 79, 327-334.
O'Leary, S. G., & Dubey, D. R. (1979).Applications of self-control proce-dures by children: A review. Journalof Applied Behavior Analysis, 12, 449-466.
Repp, A. C. (1979). Describing andmonitoring behavior. In D. A. Sabatino& T. L Miller (Eds.), Describinglearning characteristics of handi-capped children and youth. New York:Grune & Stratton.
Rusch, ER., & Kazdin, A. E. (1981).Toward a methodology of withdrawaldesigns for the assessment of responsemaintenance. Journal of AppliedBehavior Analysis, 14, 131-140.
Shores, R. E., Hester, P., & Strain, P. S.(1976). Effects of amount and type ofteacher-child interaction on child-
1120 / CCBD Retrospective Series
child interaction during free-play.Psychology in the Schools, 13, 171-175.
Strain, IR S., & Timm, M. A. (1974). Anexperimental analysis of socialinteraction between a behaviorallydisordered preschool child and herclassroom peers. Journal of AppliedBehavior Analysis, 7, 583-590.
Turkewitz, H. K., O'Leary, D., &Ironsmith, M. (1975). Generalizationand maintenance of appropriatebehavior through self-control. Journalof Consulting and Clinical Psychology,43, 577-583.
Walker, H., Greenwood, C., Hops, H., &Todd, N. (1979). Differential effects ofreinforcing topographic components ofsocial interaction: Analysis andsystematic replication. BehaviorModification, 3, 291-321.
Warrenfeltz, R. B., Kelly, W. J., Salzberg,C. L., Beegle, C. I?, Levy, S. M.,Adams, T. A., & Crouse, T. R. (1981).Social skills training of behaviorallydisordered adolescents with self-monitoring to promote generalizationto a vocational setting. BehavioralDisorders, 7, 18-27.
Workman, E. A. (1982). Teachingbehavioral self-control to students.Austin, TX: Pro-Ed.
Zahavi, S. L., & Asher, S. R. (1978). Theeffect of verbal instructions onpreschool children's aggressivebehavior. Journal of School Psychol-ogy, 16, 146-153.

APPENDIX
Behavioral Definitions of the Targeted Social Skills
Greeting
1. The student responded to or initiated a greeting (i.e., hi, hello) 5 sec afteran opportunity. (An opportunity was defined as when a person passed himin the hallway or while he walked to the educational center, or when adifferent person entered his environment within a distance of approxi-mately 3 feet while no other persons were between him and the person newto the environment.)
2. He made eye contact with the person he was greeting.
3. The student greeted the individual with a smile.
4. He used a moderate tone of voice.
5. He offered a greeting when the person was not already engaged in aconversation.
6. The student said the greeting only once.
7. He offered to shake the other person's hand.
Thanking
1. The student said "thank you" 5 sec after an opportunity. (An opportunity wasdefined as after being complimented or praised, after a request or favor wasgranted, or after a gift had been given to the student.)
2. The student said "thank you" in a friendly way.
3. He used a moderate tone of voice.
4. The student made eye contact with the individual he was thanking.
5. The subject thanked the person only once.
Initiating Conversation
1. The student initiated conversation (i.e., "It's a nice day today," "What did youdo this weekend?"), and "Did you see the movie this weekend?" 10 sec afteran opportunity. (An opportunity was defined as when a person was within 3feet of the student with no other persons between him and the person. To beconsidered an opportunity the other person must not already be engaged in aconversation [i.e., the person might be sitting by the student or walking by thestudent].)
2. The student made eye contact.
3. He used a moderate tone of voice.
4. The student made content-appropriate statements.
S. He made the initiation statement only once.
BEST COPY AVAILABLECCBD Retrospective Series / 121immimei
Council forChildren withBehavioralDisorders
Other Professional Development Products from
The Council for Children with Behavioral Disorders
WThe Mini-Library Series on Emotional/Behavioral Disorders
Edited by Lyndal M. Bullock and Robert A. Gable
Best Practices for Managing the Behavior of Adolescents with EmotionallBehavioralDisorders Within the School EnvironmentBeverley H. Johns, Eleanor C. Guetzloe, Mitchell Yell, Brenda Scheuermann, Jo Webber,Valerie G. Carr, and Carl R. SmithStock No. D5130, ISBN 0-86586-265-6, 1996, 48 pp.
Developing a System of Care: Interagency Collaboration for Students with Emotional!Behavioral DisordersRussell Skiba, Lewis Polsgrove, and Karen NasstromStock No. D5131, ISBN 0-86586-266-4, 1996, 56 pp.
Early Intervention for Young Children At Risk for EmotionallBehavioral Disorders:Implications for Policy and PracticeWesley Brown, Maureen A. Conroy, James J. Fox, Joseph Wehby, Carol Davis, and MaryMcEvoyStock No. D5132, ISBN 0-86586-267-2, 1996, 40 pp.
Effective Strategies for Teaching Appropriate Behaviors to Children With Emotional/Behavioral DisordersRobert B. Rutherford, Jr., Mary M. Quinn, and Sarup R. MathurStock No. D5133, ISBN 0-86586-268-0, 1996, 48 pp.
Planning and Implementing Effective Programs for School-Aged Children and Youth withEmotionallBehavioral Disorders Within Inclusive SchoolsHoward S. Muscott, Daniel P Morgan, and Nancy B. MeadowsStock No. D5134, ISBN 0-86586-269-9, 1996, 56 pp.
Teacher-Mediated Behavior Managemera Strategies for Children With EmotionallBehav-ioral DisordersSarup R. Mathur, Mary M. Quinn, Robert B. Rutherford, Jr.Stock No. D5135, ISBN 0-86586-270-2, 1996, 48 pp.
Types of Youth Aggression and Violence and Implicationsfor Prevention and TreatmentRichard Van AckerStock No. D5136, ISBN 0-86586-271-0, 1996, 48 pp.
Save 10% by ordeeng the entire library, Stock No. D5137, 1996. For themost current price information or to order
Call 1-800-CEC-READ (232-7323) or FA X 703-264-1637
The Council for Exceptional Children1920 Association Drive Reston, VA 22091-1589
1 o