dmdr maria hdhernandez-fuentes - sefh · p-value q-value genes with highest enrichment scores...
TRANSCRIPT

Bi dBiomarcadoresde utilidadde utilidadclínica enclínica en TrasplanteTrasplante
D M H d FDr Maria Hernandez-Fuentes
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
The Translational ‘fever’The Translational feverScientificScientific discovery
Useful ClinicalClinical Event
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
Insuficiencia funcional de un órgano www.getbetterhealth.comórgano ....
Transplante
=> inmunosupresión de por vida
Biomarcadores pueden indicar como utilizarmantener los pacientes en las mejoresmantener los pacientes en las mejorescondiciones posibles
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
Necesitamos biomarcadores en transplante?p
• predecir la evolución natural del trasplante. Supervivencia del paciente y el injertoinjerto• predecir el riesgo de cada individuo de sufrir eventos de importancia
• Acute rejection (AR)j ( )• Chronic rejection (CR)• Developing donor-specific tolerance
• evaluar el grado de actividad/deterioro de la función del injerto• evaluar el grado de actividad/deterioro de la función del injerto• high-performance techniques:
• genómicaó• microarrais expresión mRNA
• microarrais microRNA• metabolómica
t ó i• proteómica• cytómica
gran capacidad de detectar biomarcadores múltiples
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
gran capacidad de detectar biomarcadores múltiples

Rejection vs ToleranceRejection vs Tolerance
Regulation
RejectionTissue damage:
eGFR eGFRCRT
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
Transas

Consequence for patientsConsequence for patients
Cardio-Vascular events Rejection:
Acute
Cancer
AcuteChronic
Infections CellularAb mediatedAb-mediated
Nephrotoxicity Alive!
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
Alive!
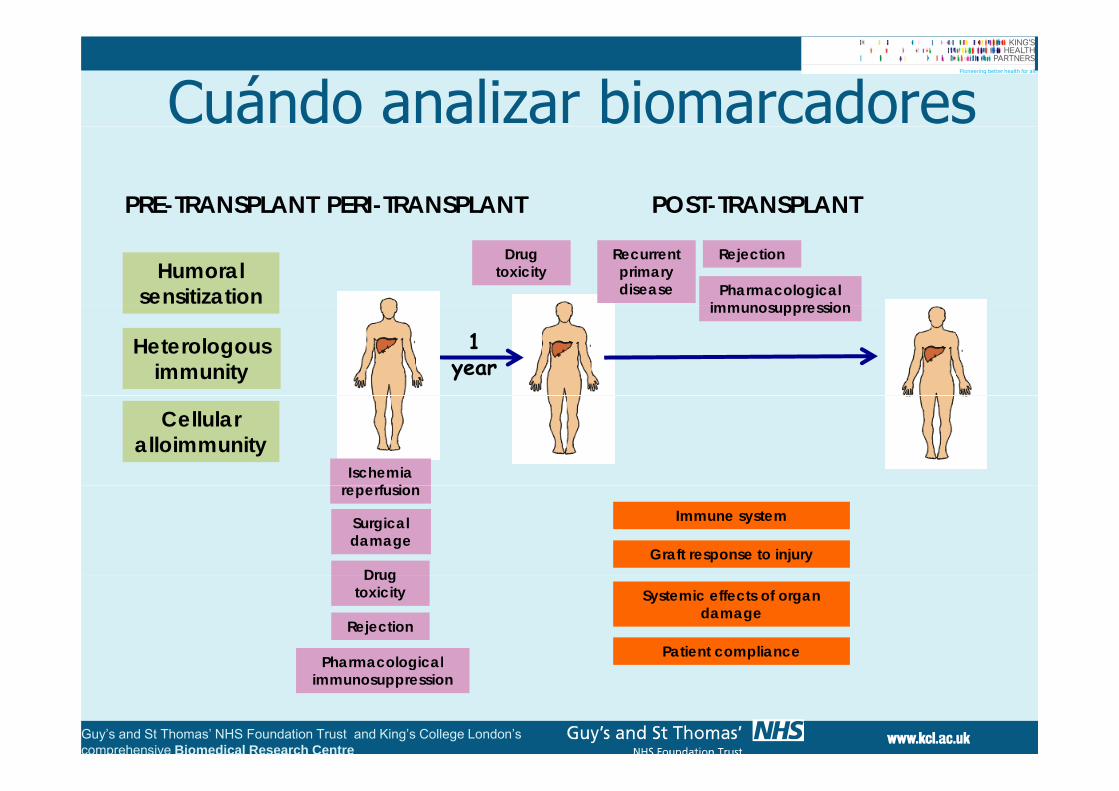
Cuándo analizar biomarcadoresPERI-TRANSPLANTPRE-TRANSPLANT POST-TRANSPLANT
Humoral sensitization
Drug toxicity
RejectionRecurrentprimarydisease Pharmacological
immunosuppression
1 year
Heterologousimmunity
immunosuppression
Ischemiaf i
Cellularalloimmunity
reperfusion
Surgicaldamage
Drug
Immune system
Graft response to injuryDrug
toxicity
Rejection
Pharmacological
Systemic effects of organdamage
Patient compliance
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
Pharmacologicalimmunosuppression
Biomarcadores de utilidad clínicaBiomarcadores de utilidad clínica
Bi d d R h A d• Biomarcadores de Rechazo Agudo en trasplante renaltrasplante renal
• Biomarcadores de rechazo agudo en trasplante cardiaco
Bi d d t l i t l t•Biomarcadores de tolerancia en trasplantesde hígado y riñóng y
• Perspectivas para el futuro
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre

M l lMolecular
Cellular / HistologicalCellular / Histological
Clinical
Time
Tx Rationale: earlyTx Rationale: early intervention
GWAS microRNAmRNA
proteins
Molecular and cellular surveillance t t iproteins strategies
anticipate histological and
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
histological and clinical rejection.

Rúbricas moleculares en biopsiasRúbricas moleculares en biopsiasCriterios Histopatológicos BANFF
ion
of r
ejec
tob
abili
tyig
ned
pro
Anglicheau D, et al Proc Natl Acad Sci U S A. 2009 Mar 31;106(13):5330-5.PA
M a
ssi
Famulski KS, et al American Journal of Transplantation 2010; 10: 810–820.
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
A Molecular classifier for predicting future graft lossEinecke G, et al J of Clinical Investigation 2010; 120 (6): doi:10.1172/JCI41789

Biomarcadores en Orina / SangreBiomarcadores en Orina / Sangre
Muthukumar et al
CD154 ICOS CTLA4 PD1
Muthukumar, et al Alakulppi et al, Transplantation 2007;83: 791–798
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre

Kidney ALograft Immune Biomarkers of REjection& Immune Monitoring for AR (KALIBRE & IMAR)& Immune Monitoring for AR (KALIBRE & IMAR)
Study cohort: 200 consecutive kidney transplant patients y y p p
(adults) performed at Guy’s Hospital
1 2 3 4 5 6 7 8 9 10 11 12 Time(months)
Frequency
W kl Fortnightly Monthly + any ARWeekly Fortnightly Monthly
4ml peripheral blood EDTA 3 3 l bl d U iRecruitment 4ml peripheral blood EDTA 3x3 ml blood
Cryopreserved PBMCs mRNA
Urin
e
Recruitment
Biobank
Flow cytometry RT-PCRBRC facilities
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre

Preliminary Results 1Preliminary HTqPCR data:
10 i
y
10 muestras por pacientecada 2 semanas en 13 estables and 8 con ARestables and 8 con AR diagnosticado con BiopsiaIP−10
Semana 2 post-Tx
C f
Granzyme B
Results completos en TGF−b
C6orf25
p2012
PF4
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
Sta
ble
Sta
ble
Sta
ble
Sta
ble
Sta
ble
Sta
ble
Sta
ble
Sta
ble
Sta
ble
Rej
ecto
r
Sta
ble
Rej
ecto
r
Sta
ble
Rej
ecto
r
Sta
ble
Rej
ecto
r
Sta
ble
Sta
ble
Rej
ecto
r
Rej
ecto
r
Rej
ecto
r
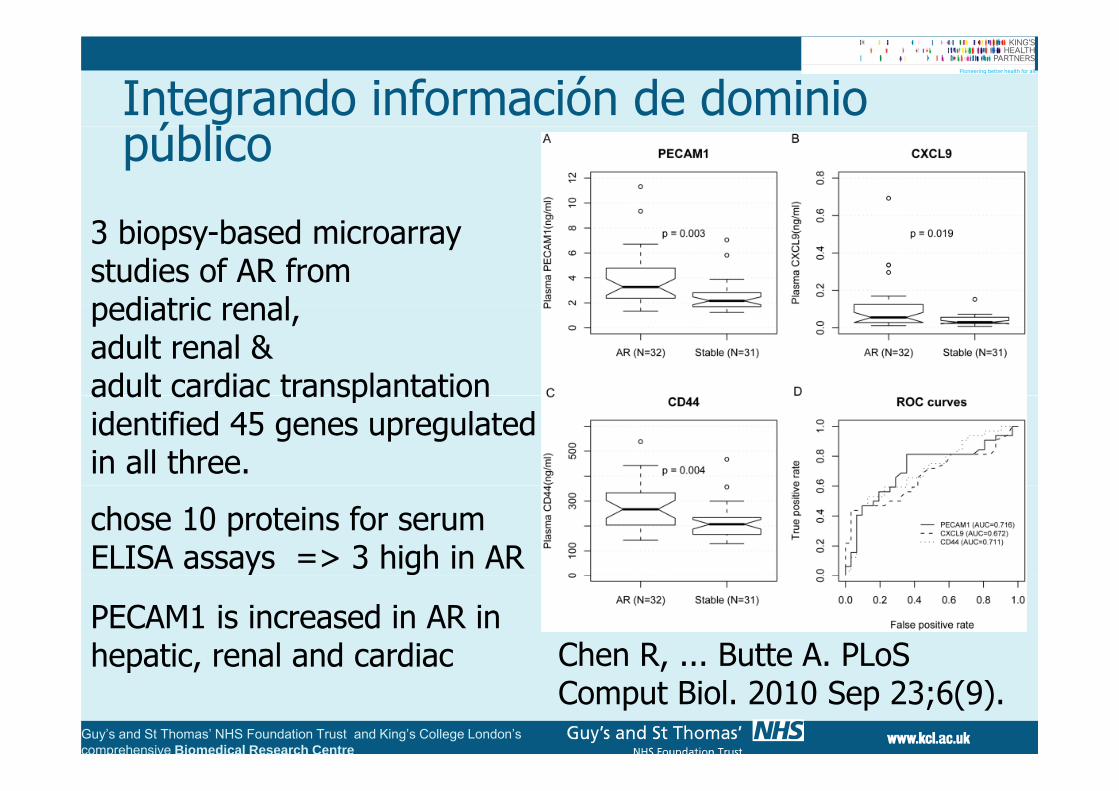
Integrando información de dominio úblipúblico
3 biopsy-based microarray studies of AR frompediatric renalpediatric renal, adult renal &adult cardiac transplantationadult cardiac transplantation identified 45 genes upregulatedin all three.
chose 10 proteins for serum ELISA assays => 3 high in AR
PECAM1 is increased in AR in hepatic, renal and cardiac Chen R, ... Butte A. PLoS
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
hepatic, renal and cardiac Chen R, ... Butte A. PLoSComput Biol. 2010 Sep 23;6(9).

Biomarcadores de utilidad clínicaBiomarcadores de utilidad clínica
Bi d d R h A d• Biomarcadores de Rechazo Agudo en transplante renaltransplante renal
• Biomarcadores de rechazo agudo en trasplante cardiaco
Bi d d t l i t l t•Biomarcadores de tolerancia en trasplantesde hígado y riñóng y
• Perspectivas para el futuro
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
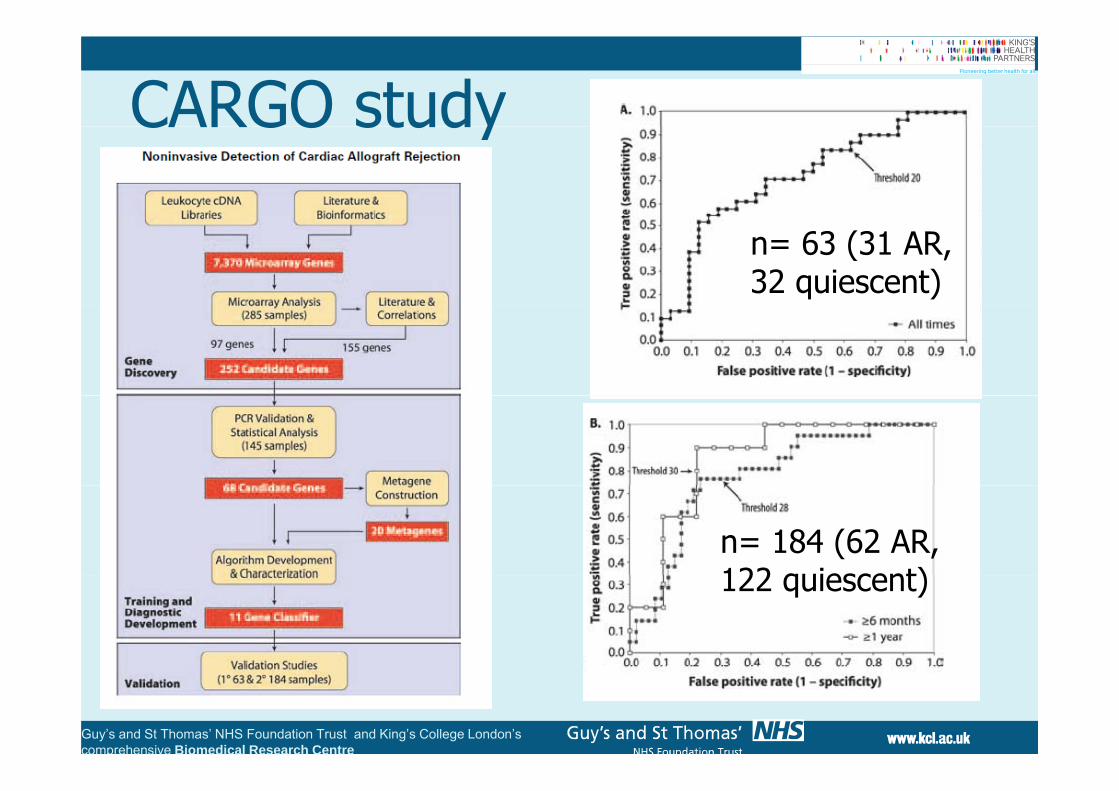
CARGO studyCARGO study
n= 63 (31 AR, 32 quiescent)
n= 184 (62 AR, 122 quiescent)122 quiescent)
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre

Biomarcadores de utilidad clínicaBiomarcadores de utilidad clínica
Bi d d R h A d• Biomarcadores de Rechazo Agudo
• Biomarcadores de rechazo agudo en• Biomarcadores de rechazo agudo en trasplante cardiaco
• Biomarcadores de tolerancia en trasplantesd hí d iñóde hígado y riñón
• Perspectivas para el futuroPerspectivas para el futuro
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre

Transplantation tolerance would addressTransplantation tolerance would address major problems that limit transplants half-life:
transplants would last longer; less patients would transplants would last longer; less patients would return to waiting list
chronic rejection would be reducedj
i i ld b i i i d/ ithd immunosuppression could be minimised/withdrawn
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
... “bespoke immunosuppression”

ObjetivosObjetivos Definir “Rúbrica molecular” asociada tolerancia Definir Rúbrica molecular asociada toleranciaoperativa
Desarrollo de tests in vitro específicos, reproducibles y fiables asociados a toleranciareproducibles y fiables asociados a toleranciaoperativa
Transferencia a la clínica: desarrollo de herramientas que permitan predecir a quéherramientas que permitan predecir a quépacientes se les puede disminuir la inmunosupresión
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
inmunosupresión.
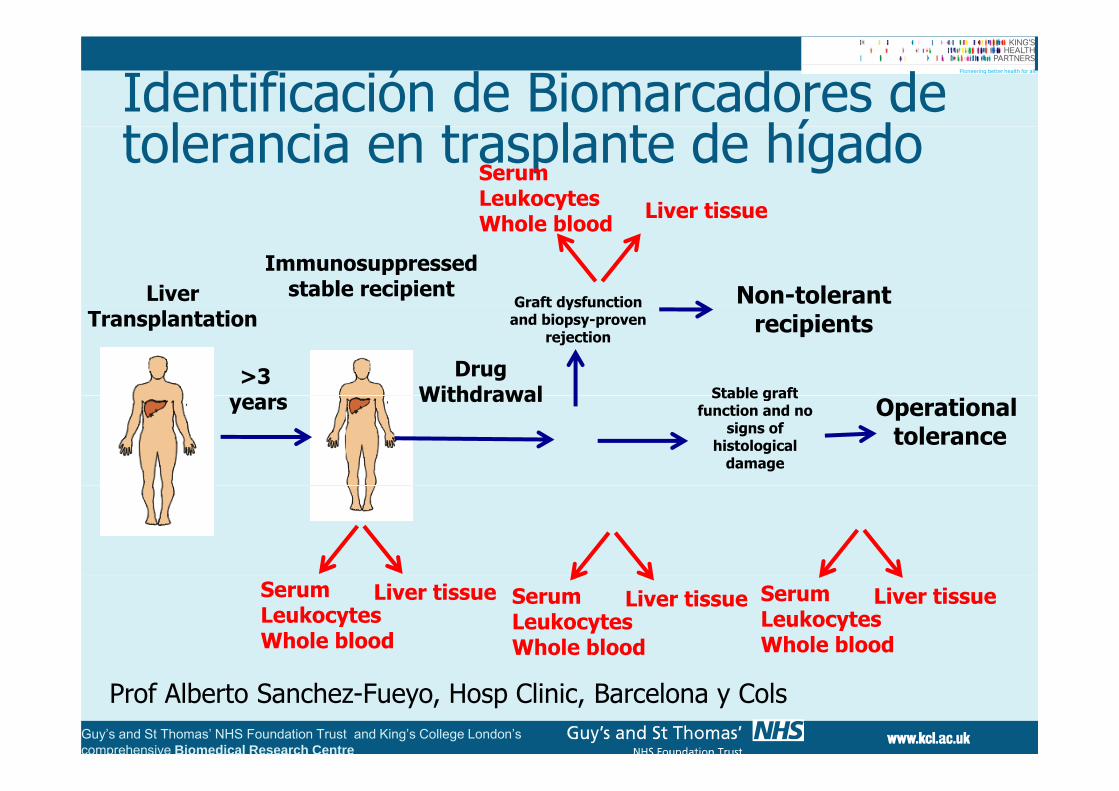
Identificación de Biomarcadores de t l i t l t d hí dtolerancia en trasplante de hígado
SerumLeukocytesWh l bl d Liver tissue
Immunosuppressedstable recipient
Graft dysfunction Non-tolerantLiver
Whole blood Liver tissue
Drug Withdrawal Stable graft
Graft dysfunctionand biopsy-proven
rejectionrecipients
>3
Transplantation
Withdrawal Operationaltolerance
Stable graftfunction and no
signs ofhistological
damage
years
SerumLeukocytesWhole blood
Liver tissue SerumLeukocytesWhole blood
Liver tissue SerumLeukocytesWhole blood
Liver tissue
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
Prof Alberto Sanchez-Fueyo, Hosp Clinic, Barcelona y Cols

497 Patients were screened
395 Patients were excluded
497 Patients were screened
160 had been transplanted for < 3 years58 had medical disorders incompatible with the safe conduct of the study
and/or interpretation of the results. 35 declined to participate30 were included in another clinical trial29 had history of autoimmune liver disease19 h d b l li f ti t t di ifi d it i19 had abnormal liver function tests exceeding pre‐specified criteria19 exhibited abnormalities in basal liver biopsy exceeding pre‐specified criteria18 could not be closely followed‐up14 had history of rejection in the previous 12 months9 had no side effects of IS drugs4 were already receiving no immunosuppressive drugs
102 Patients were enrolled
4 P ti t ithd f t d d i d d ti4 Patients withdrawn from study during dose reduction classified as Non‐TOLERANT in the ITT analysis
41 Patients were TOLERANT 57 Patients REJECTED
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre

Peripheral blood transcriptional and cellular markers of operational tolerance
Enriched in tolerant recipients p-value q-value Genes with highest enrichment scores Geneset
database
Natural Killer (CD56) cell lineage
0.000 0.000 KLRC3, NCAM1, CD160, BNC2, KIR3DL2, LAIR2, SH2D1B, KIR3DL1,KLRF1, CLIC3, AKR1C3, FEZ1, PDGFRB, GZMB, IL2RB
Haematlas
Graft versus host disease
0.000 0.000 KIR3DL1, KIR3DL2, KIR3DL3, KIR2DL1, GZMB, KIR2DL5A, KLRD1 KEGG
disease
Antigen processing and presentation
0.000 0.000 KLRC4, KLRC3, KIR3DL2, KIR3DL1, KIR2DS3, KIR2DS4, KIR2DL5A,KIR2DL1, KIR2DS1, KLRD1
KEGG
N t l Kill ll0.000 0.001 KLRC3, KIR3DL2, SH2D1B, KIR3DL1, KIR2DL2, GZMB, KIR2DL1, TNF,
KLRD1 KIR2DL3Biocarta
Natural Killer cell mediated cytotoxicity
KLRD1, KIR2DL3
VIP pathway0.000 0.001 EGR3, EGR2, PRKAR1B, NFKBIA, PRKAR2B, NFATC2, PPP3CC KEGG
DARPP32 events0.000 0.006 PDE4D, PRKAR2B, PRKAR2B, PPP3R1, PDE4B, PPP3C. Biocarta
Immunoregulatory 0.000 0.013 CD160, KIR3DL2, KIR3DL1, KIR2DL2, KIR2DS2, KIR2DL3, CD226,KIR2DL1, ICAM4
Reactome
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
interactions
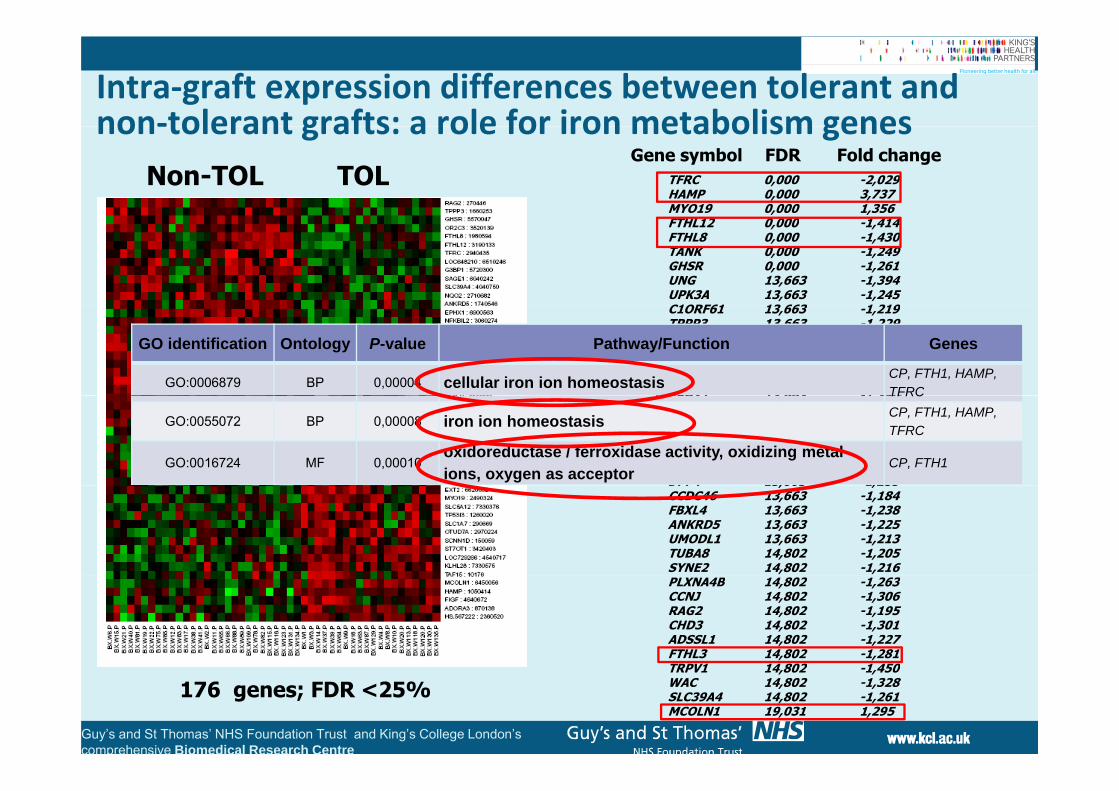
Intra‐graft expression differences between tolerant and non‐tolerant grafts: a role for iron metabolism genesnon‐tolerant grafts: a role for iron metabolism genes
Non-TOL TOL TFRC 0,000 -2,029HAMP 0,000 3,737MYO19 0,000 1,356
FDR Fold changeGene symbol
FTHL12 0,000 -1,414FTHL8 0,000 -1,430TANK 0,000 -1,249GHSR 0,000 -1,261UNG 13,663 -1,394UPK3A 13,663 -1,245C1ORF61 13 663 1 219C1ORF61 13,663 -1,219TPPP3 13,663 -1,229MUTED 13,663 -1,258TSPAN2 13,663 -1,256FDXR 13,663 -1,451RTP2 13,663 -1,222EPHX1 13 663 -1 380
GO identification Ontology P-value Pathway/Function Genes
GO:0006879 BP 0,00004 cellular iron ion homeostasis CP, FTH1, HAMP, TFRCEPHX1 13,663 -1,380
G3BP1 13,663 -1,220TAS2R50 13,663 -1,283HSD17B11 13,663 -1,297FAM162A 13,663 -1,295RNASE13 13,663 -1,215DPP4 13,663 -1,285
TFRC
GO:0055072 BP 0,00008 iron ion homeostasis CP, FTH1, HAMP, TFRC
GO:0016724 MF 0,00010oxidoreductase / ferroxidase activity, oxidizing metal ions, oxygen as acceptor
CP, FTH1DPP4 13,663 1,285CCDC46 13,663 -1,184FBXL4 13,663 -1,238ANKRD5 13,663 -1,225UMODL1 13,663 -1,213TUBA8 14,802 -1,205SYNE2 14,802 -1,216PLXNA4B 14,802 -1,263CCNJ 14,802 -1,306RAG2 14,802 -1,195CHD3 14,802 -1,301ADSSL1 14,802 -1,227FTHL3 14,802 -1,281TRPV1 14 802 1 450
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
176 genes; FDR <25%TRPV1 14,802 -1,450WAC 14,802 -1,328SLC39A4 14,802 -1,261MCOLN1 19,031 1,295

Kidney: Indices of Tolerance, y ,King’s College London, UK
Robert LechlerMaria Hernandez Fuentes
Oxford University, UKKathryn WoodStephanie ChapmanPiotr Trzonkowski
BerlinCologne
BerlinCologne
Miltenyi Memorec, GermanyUwe JanssenBettina PetersStefan TomiukMaria Hernandez Fuentes
Pervinder Sagoo Esperanza Perucha Elvira JimenezFlavia RovisSaskia Stevenson
Gregor WarneckeIan RobertsLondon
OxfordLondonOxford
Imperial College London, UK
Charité University Medicine, Germany
Hans Dieter Volk
Stefan Tomiuk
Saskia StevensonSharon Hughes
London, UKAnthony WarrensAmany BallowRuhena SergeantJan WatersJackie and Katie
Hans-Dieter VolkBirgit Sawitzki
Guy’s Hospital, UK
Rachel Hilton
Immune Tolerance Network
Irene Rebollo Mesa
Jackie and KatieRachel HiltonRobert VaughnFred ComptonLiz, Ola and Diane
McGill University Montreal, CanadaDavid Stephens
Network
Institute for Medical Immunology, ULB, Belgium Michel Goldman
Ligia Cracium
Brussels
NantesNantes
ITERT - INSERM, FranceJean-Paul Soulillou
Sophie Brouard
Vicki SeyfertLarry Turka
Kenneth NewellKasia BourcierLigia Cracium
Alain Le MoineMyriam Libin
NantesNantesSophie BrouardCecile BraudeauMagali Giral Patrick Miqueu
Kasia BourcierIgnacio Sanz
Wei ChungwenJames Roger
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
Participating PhysiciansParticipating PhysiciansUKPoland
Dr Magdalena KrajewskaIreland
Dr Richard BakerSt. James's University Hospital
Dr Sue CarrLeicester General Hospital
Dr Rachel HiltonFrance
Dr Herve Le Monies de S.
Dr Magdalena KrajewskaMedical University of Wroclaw, Wrocław
Dr Alan WatsonSt Vincent’s
Hospital, Dublin
Dr Rachel Hilton Guy’s &St. Thomas’ NHS Trust London
Dr Phillip MasonJohn Radcliffe Hospital, Oxford
Dr Will McKaneSheffield Kidney Institute
Hôpital Victor Provo, Roubaix
Dr Legendre& Sophie Lechaton
Hôpital Necker-Enfants
SwitzerlandDr Markus Mohaupt
Inselspital, Universitätsspital Bern
Sheffield Kidney InstituteDr Jo TaylorDorset County Hospital
Dr Sui Phin KonGuy’s &St. Thomas’ NHS Trust London
D Ad Sh if
pMalades, Paris
Dr Magali Giral& Dr Jean Paul Soulillou
CHU-HôtelDieu, NantesDr Evangeline Pillebout Dr Adnan Sharif
Univesity Hospital Wales, Cardiff
Spain
BelgiumDr Alain Lemoine
Dr Evangeline PilleboutHôpital Saint Louis, Paris
Czech RepublicD O d j Vikli kýSpain
Dr Josep Campistol& Dr Fritz Dickman
Hospital Clínic de Barcelona Dr Juan Bravo
& Dr Martin WissingCUB Hôpital Erasme
Bruxelles
Italy
Dr Ondrej ViklickýKlinika Nefrologie TC IKEM
Prague
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
Hospital Universitario Virgen de las Nieves, Granada
yDr Giuseppe Orlando
Ospedale S. Eugenio, Rome

Patient sets to search for biomarkers of Tolerance:
EU cohort• Tolerants
USA cohort• Tolerants
• n=11• Stable function
L P d
• Tolerants• n=24
• Stable function• Low Pred• CNI-free• Triple therapy
Stable function• Monotherapy• Triple therapy
• Triple therapy• Chronic rejection
• CAN
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
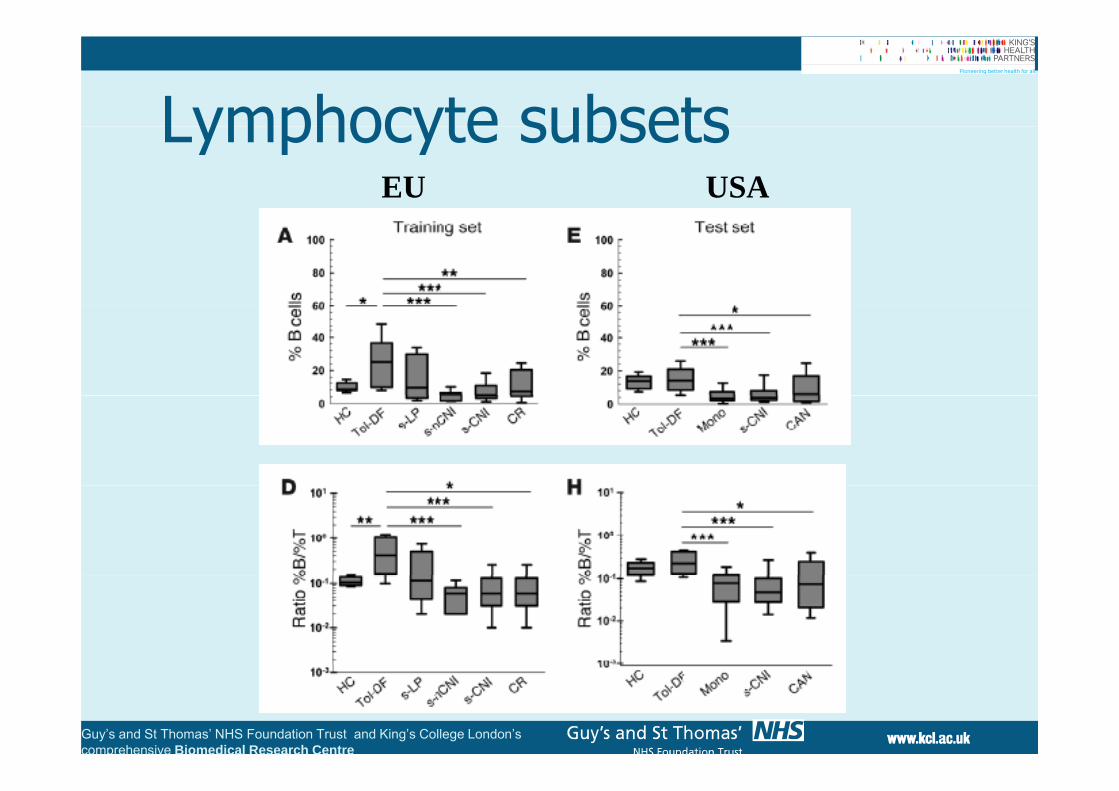
Lymphocyte subsetsLymphocyte subsetsEU USA
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
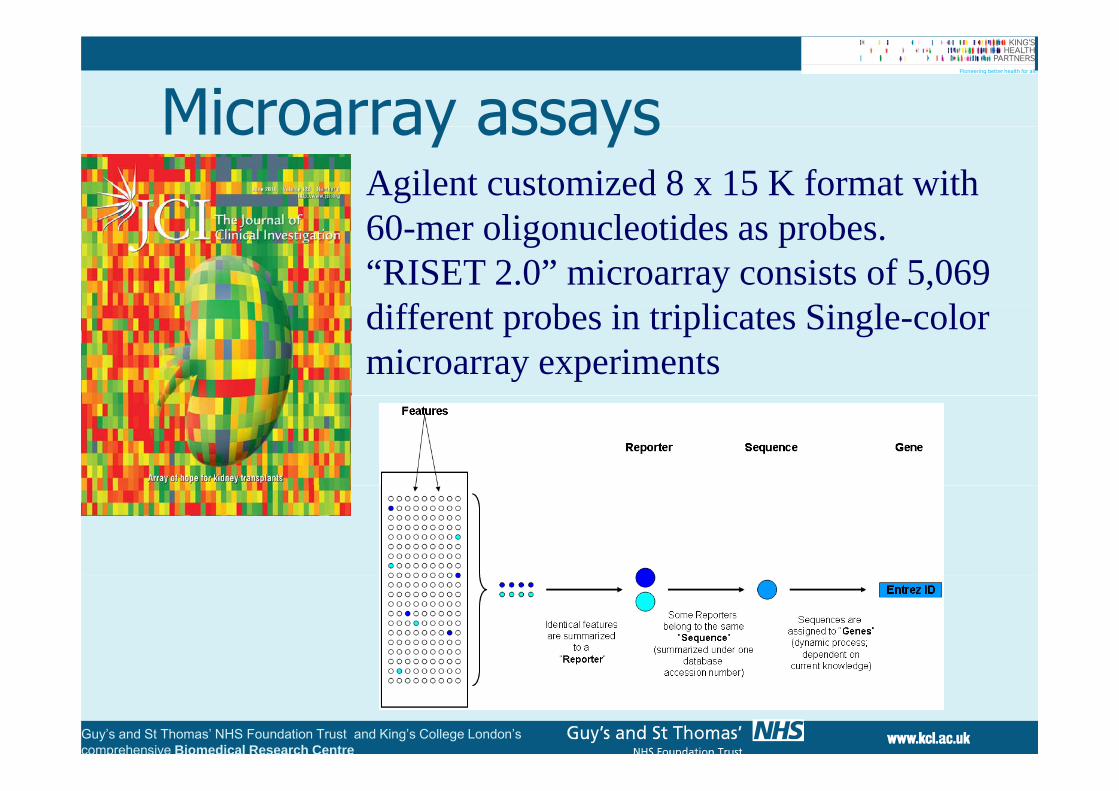
Microarray assaysMicroarray assaysAgilent customized 8 x 15 K format with 60 li l id b60-mer oligonucleotides as probes. “RISET 2.0” microarray consists of 5,069 diff b i i li Si l ldifferent probes in triplicates Single-color microarray experiments
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre

MicroarrayTraining set T t t
Custom microarray analysis (5069 probes, 4607 genes)
Microarray analysis
Training set Test set
CNI
Tol-DF Tol-DF
s-CNIs-nCNI s-LP
CR CANs-CNIMono
Four-class analysisusing a Kruskal-Wallis nonparametric test.
CD79BTCLA1HC HC
pProbes were rankedwithin the training set based on their P values with adjustment
HS3ST1SH2D1BMS4A186
174
1204for 1% FDR. Top 10 ranked probes that overlapped with genes
MS4A1 TLR5FCLR14identified
in the test set were subsequently used for ROC
l i
PNOCSLC8A1FCRL2
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
Top 10 ranked probes/genes selected for ROC analysisanalysis. FCRL2

Set of Biomarkers 1Set of Biomarkers 1
Lower percentage of recently activated T cells Lower percentage of recently activated T cells
Expansion of peripheral blood B cells. High p p p gB/T cell ratio.
Absence of anti-donor Ab
Lower direct pathway anti donor responses Lower direct pathway anti-donor responses
High Foxp3/a1,2-mannosidase High Foxp3/a1,2 mannosidase
Differential expression of a set of 10 genes
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre

Cross-platform biomarkerCross platform biomarker ROC curve
EU USAEU USA
Sensibility = 1 Sensibility = 0.903Specificity = 0 923Specificity = 1 Specificity = 0.923
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre

Probability of beingProbability of being tolerant
Training set Test setEU USA
oler
ant
3
10-2
10-1
100
oler
ant
1
100
of B
ein
g To
10-11
10-10
10-9
10-8
10-3
f B
eing
To
10-2
10-1
obab
ility
o
10 16
10-15
10-14
10-13
10-12
10
babi
lity
of10 710-610-510-410-3
Patient groups
Pro
10-17
10-16
Tol-DF s-LP s-CNI/-nCNI CR
Patient groups
Pro
10-1010-910-810-7
Tol-DF Mono s-CNI CAN
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
Patient groups Patient groups

Validación extensiva:Validación extensiva: GAMBIT
• Prevalencia del fenotipo de tolerancia: Recipientescon función estable > 3 5 yrs post Tx econ función estable, > 3-5 yrs post-Tx, e inmunosupresión standard, BioM of Tol is ~ 5 - 15%. n = 200
• Repetitividad: > 80% de pacientes tolerantesRepetitividad: > 80% de pacientes tolerantesidentificados de novo expresan los BioM of Tol. n = 20
t l+ controls
• Estabilidad: BoM of Tol permanecen estables
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
pdespues de disminución de inmunosupresión

ConclusionesConclusiones Se estan desarrollando bioensayos y biomarcadoresy yque ayudan determinar si lo pacientes tienen un riesgo mas alto de sufrir rechazo si lo pacientes tienen un riesgo mas alto de sufrir rechazo agudo => oportunidad de incrementar el tratamiento si los pacientes estan desarrolando características de si los pacientes estan desarrolando características de tolerancia => oportunidad de disminuir el tratamiento
El futuro del tratamiento del post transplante se El futuro del tratamiento del post-transplante se basará en regímenes terapeúticos basados en
dBiomarcadores Medicina personalizada
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
p

The GAMBIT ConsortiumKing’s College London, UKMaria Hernandez Fuentes
Sonia NorrisEstefania No a Lampe ti
Cardiff and Vale University Health Board
Hull Royal InfirmaryDr Sunil BhandariKaren James
Tracy Cathcart
St Jame’s HospitalLeedsDr Richard Baker
Estefania Nova-LampertiPaula MobilloYogesh KamraMano Runglall
Tom LewisFlorence Delany
Health BoardDr Sian Griffin
Tracy Cathcart
Royal Free HospitalDr Alan Salama
Leicester General HospitalDr Sue CarrRachel Westacott
Dr Aravind Cherukuri
St Geo ge’s HospFlorence DelanyIrene Rebollo-Mesa
Rosalynn MillerDarlene Catalan
Jude GreenRobert Lechler
Roy Marshall King’s College HospitalDr Sui Phin KonBeatriz Tucker
Nicolene Atkinson
Queen Alexandra Hospital,Postmouth
Dr Judith Stevens Manchester Royal
St George’s HospDr Iain McPhee
Dr Joyce PopoolaRaj Ramkhelawon
Robert LechlerGraham Lord
Guy’s Hospital, UKRachel HiltonRobert Vaughn Transplantační laboratoř
Kent and CanterburyDr Chris FarmerGillian Eaglestone
Hazel Broad
Dr Judith StevensLynn Watkins
Frances Williams
Manchester Royal InfirmaryDr Hany Riad
Dr Nick Simon Clare Griffing
Hospital Universitari Valld'Hebrón, Barcelona
Dr Daniel SeronMaria Sarria
Transplantační laboratořIKEM, Prague
Dr Ondrej VicklikyPetra Hribova
INSELSPITAL, Universitätsspital BernDr Markus Mohaupt
Petra Hribova
Evelina Children’s HospDr Manish Sinha
Liz Reus, Joy & Paula
Hospital de las Cruces, Bilbao
Dra Sofia Zarraga
Petra Hribova
G t O d St t
Salford RoyalDr Phillip KalraLesley Haydock
Northern General Hospital,SheffieldDr William McKane
Faith OkuhoyaGlasgow General HospitalDr Patrick Mark
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre
Great Ormond StreetDr Stephen Marks
Dr Patrick MarkDonna Kelly
Lorraine McGregor

Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’sComprehensive BiomedicalComprehensive Biomedical Research Centre
Dr Paramit Chowdhury
D Rachel HiltonDr Rachel Hilton
Prof Steve Sacks
Prof Robert LechlerProf Alberto Sanchez-
Prof Robert Lechler
Prof Graham LordFueyo
Hospital Clinic Barcelona
Guy’s and St Thomas’ NHS Foundation Trust and King’s College London’scomprehensive Biomedical Research Centre