disseminated intravascular coagulation
DESCRIPTION
it is complete ppt of DICTRANSCRIPT
DISSEMINATEDINTRAVASCULAR COAGULATION
P.GIRISH KUMAR ROLL NO.89

Other names :
1.Consumption coagulopathy2.Defibrination syndrome
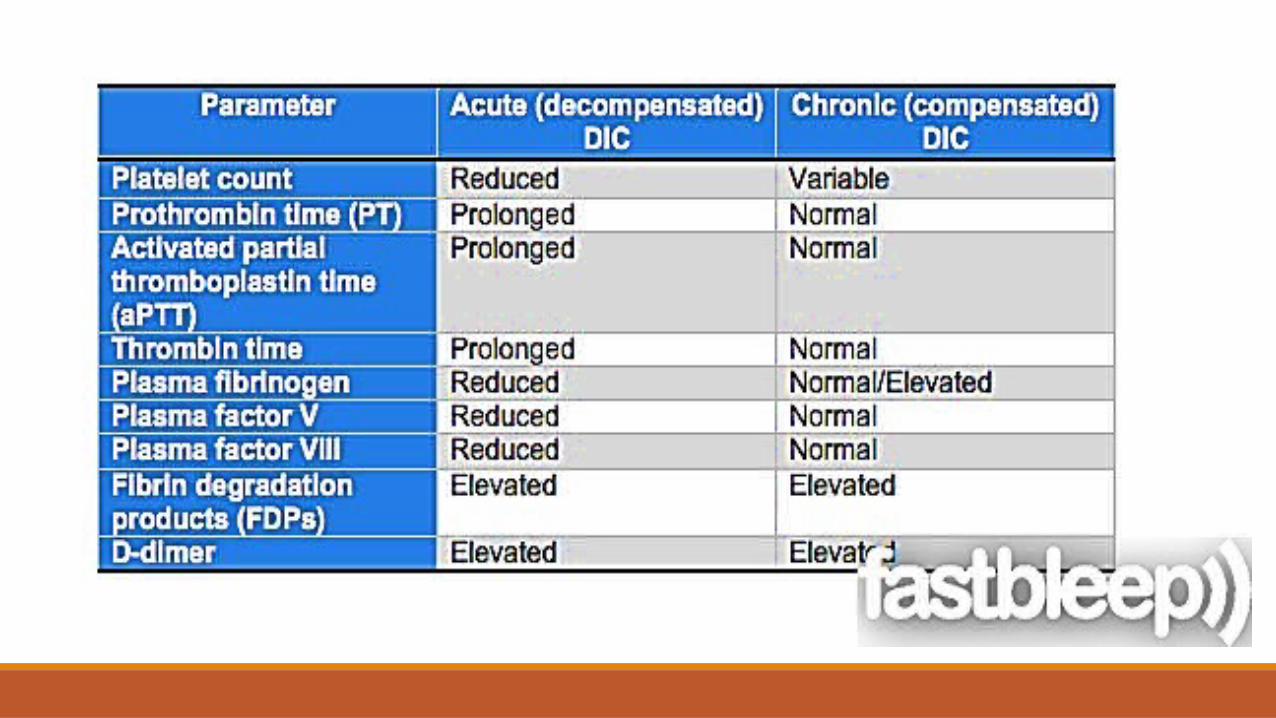
Types :1) Acute DIC2) CHRONIC DIC

NORMAL HEMOSTASIS

What is dic ?

PATHOGENESIS :1. Generation of a hyperthrombinemic state.2. Alteration of the physiological anticoagulants levels.3. Impaired fibrinolysis at the onset of DIC.4. Activation and liberation of inflammatory cytokines in the
pathogenesis of DIC.

Generation of hyperethrombinemic state 1. The exposing of the tissue factors thromboplastins and
factor3 during injury causes a cascade activation of a factor pathway that has a dominant role in the hyperthrombinemic state in DIC.
2. Cytokines and the bacterial endotoxins are all triggers to the formation of endothelial cell tissue factor.
3. In severe trauma also tissue phospholipids initiates the clotting cascade.

The cascade goes as follows :

Thrombin in turn activates :

Alteration of the physiological anticoagulant levels:
There are 3 most common Anticoagulants in the body :1. Antithrombin2. Active protein C3. Tissue factor pathway inhibitor (TFPI) In DIC :1. Anti thrombin2. Active protein C
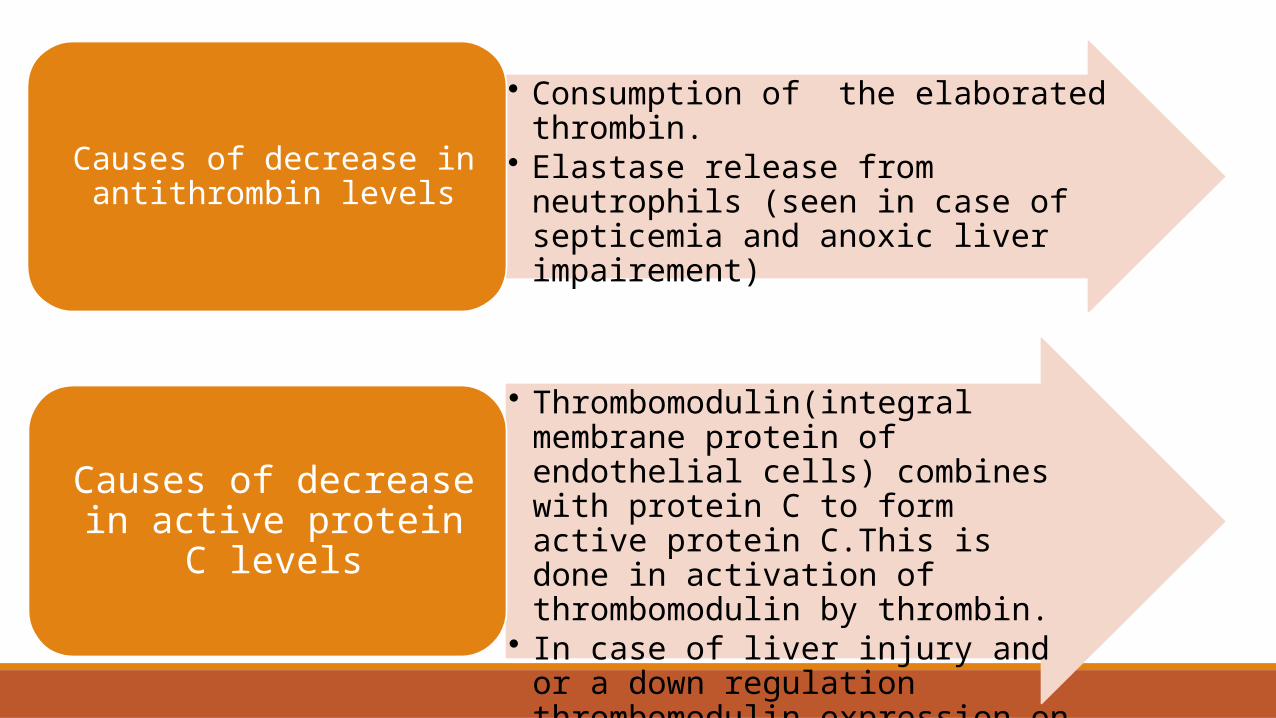
• Consumption of the elaborated thrombin.• Elastase release from neutrophils (seen in
case of septicemia and anoxic liver impairement)
Causes of decrease in antithrombin levels
• Thrombomodulin(integral membrane protein of endothelial cells) combines with protein C to form active protein C.This is done in activation of thrombomodulin by thrombin.
• In case of liver injury and or a down regulation thrombomodulin expression on the vascular surface.
Causes of decrease in active protein C levels



Impaired fibrinolysis at the onset of DIC:
1. PAI-1 a neurohumoral compound released from endothelial cells.
2. It suppresses fibrinolysis normally
3. In some DIC individuals , PAI -1gene mutation shown leading to
increased PAI-1 levels

Activation and liberation of inflammatory cytokines in DIC :

Clinical features :•Microangiopathic hemolytic anemia
•Dyspnea
•Cyanosis and respiratory failure
•Convulsions and coma
•Oliguria and acute renal failure
•Sudden or progressive circulatory failure and shock
•Petechiae
•Bleeding , possibly from multiple sites of body
SITES OF THROMBOSIS IN DECREASING ORDER OF FREQUENCY•Brain
•Heart
•Kidney
•Adrenals
•Spleen
•Lungs
•Liver



DIFFERENTIAL DIAGNOSIS :
1. Severe liver disease :lab parameters won’t change rapidly and presence of portal hypertension.
2. Microangiopathic disorders(TTP) :no consumption of clotting factors or hyperfibrinolysis.

Lab investigations of DIC :
CBC and blood smearClotting timesFibrin related markersCoagulation factors
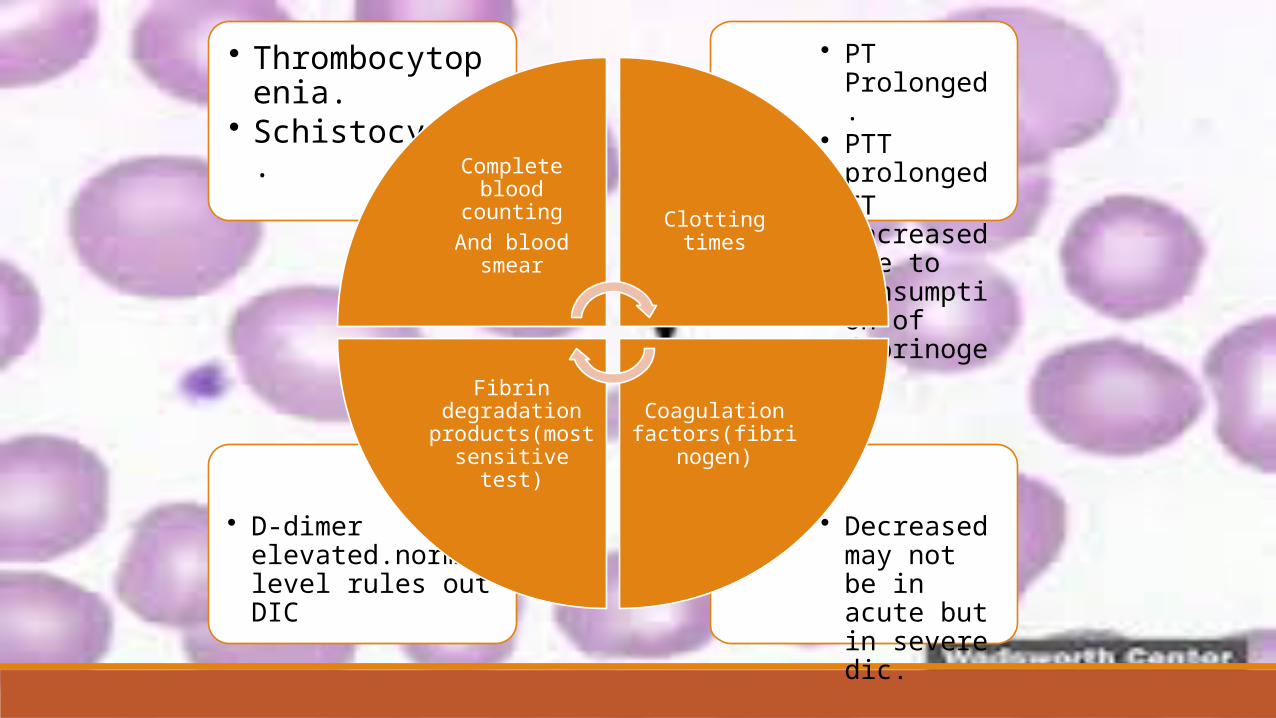
• Decreased may not be in acute but in severe dic.
• D-dimer elevated.normal level rules out DIC
• PT Prolonged.• PTT prolonged• TT increased
due to consumption of fibrinogen
• Thrombocytopenia.
• Schistocytes.
Complete blood counting
And blood smear Clotting times
Coagulation factors(fibrinogen)
Fibrin degradation products(most sensitive test)
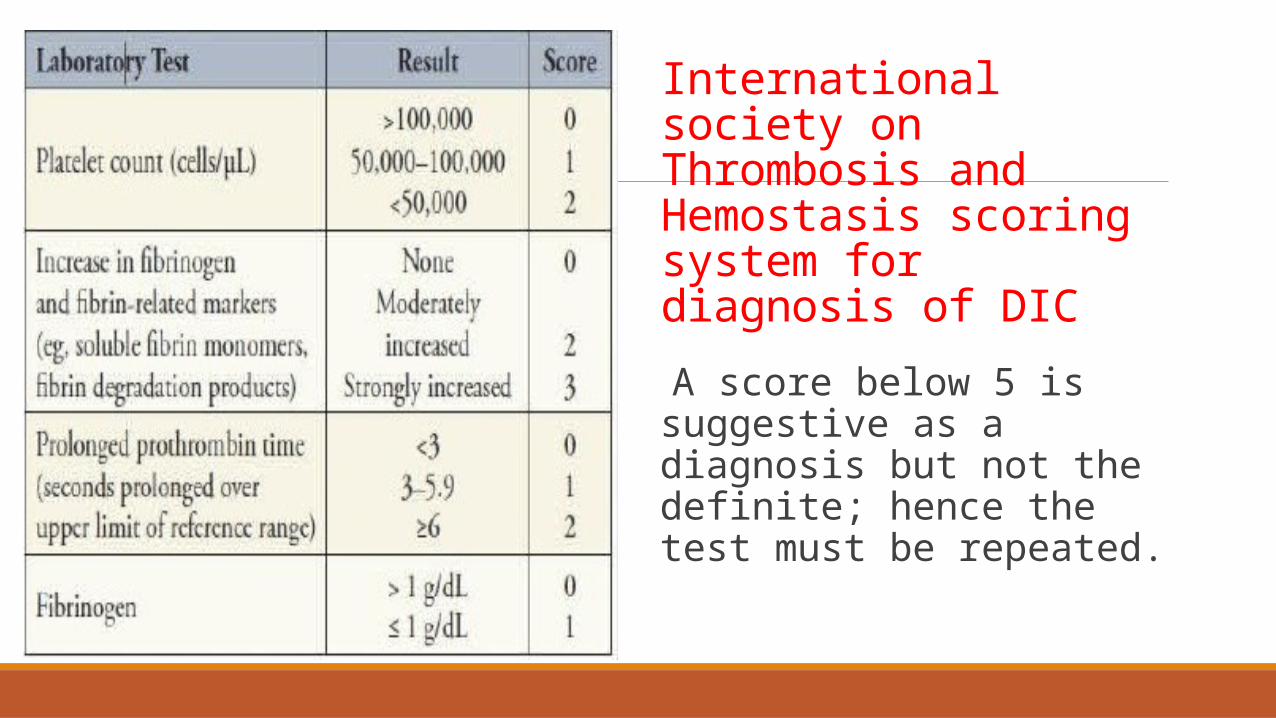
International society on Thrombosis and Hemostasis scoring system for diagnosis of DIC
A score below 5 is suggestive as a diagnosis but not the definite; hence the test must be repeated.

