differences between countries - nsf berit guttormsen... · bronkospasme luftveisødem ingen...
TRANSCRIPT
AnaphylaxisDifferences between countries
Anne Berit GuttormsenDepartment of Anaesthesia and Intensive Care,
Haukeland University Hospital and Section for Anaesthesiology and Intensive Care,
Department of Surgical Sciences, Medical Faculty, University of Bergen
Aetiology
• Allergy is common, but progression of an allergic
reaction to a severe life-threatening condition is
rare.
• Most common causes of the life-threatening
reactions are drugs, stinging insects and food.
European Resuscitation council Guidelines for Resuscitation 2005
Early signs
• Urticaria
• Rhinitis
• Conjunctivitis
• Abdominal pain
• Vomiting and diarrhoea
• Flushing or pallor
European Resuscitation council Guidelines for Resuscitation 2005
Diagnosis is difficult
• Due to
– Lack of consistent clinical information
– A wide range of presentations
• Always exclude anaphylaxis as the cause
of the reaction.
– Misinterpretation might be fatal!

Anaphylaxis
• An acute general
hypersensitivity reaction– That takes place seconds/minutes
after exposure with the
drug/specimen in question
– The reaction involves one or more
organ systems
– The symptoms vary
• Often dramatic, potentially
lifethreatening
– Several mechanisms
• IgE/Non IgE
• Non allergic
Classification
• Grade 1: Symptoms from the skin, only
• Grade 2: Systemic, not lifethreatening
• Grade 3: Systemic, lifethreatening
• Grade 4: Asystoli/or respiratory arrest
• Grade 5: Death
Ring J, Messmer K. Lancet 1977
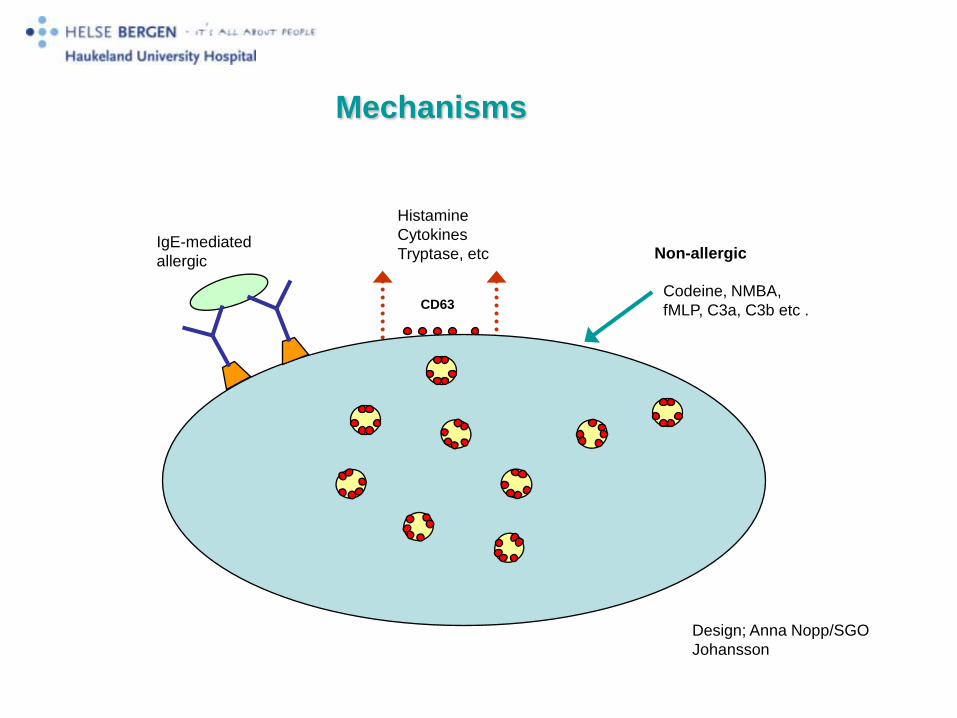
IgE-mediated
allergicNon-allergic
Codeine, NMBA,
fMLP, C3a, C3b etc .
Histamine
Cytokines
Tryptase, etc
CD63
Design; Anna Nopp/SGO
Johansson
Mechanisms
Patients

Patient 1 Male born 1972 (2006)
• He developed an itchy head, dizziness, facial oedema and
hypotension 10-20 minutes after taking cough-syrup containing ethyl
morphine.
• His wife suspected anaphylaxis and took him to hospital.
• On admission; BP was 84/58 mmHg, declining to 68/40 mmHg, and
he still had the facial oedema.
• He was treated with adrenaline, i.v. fluids, steroids and
antihistamines. He stabilized.
• Observed at the hospital for one night.
• (2005) Spinal anaesthesia, Bupivacaine with
fentanyl. After 50 minutes; Urticaria, face,
thorax lower part of abdomen and groins, itching
sensation on his palms. A small decrease in
blood pressure.
• Treatment
Ephedrine 10 mg, antihistamine and steroids
Patient 2 Male born 1935 (2005)

• (2001) Had Corsodyl mouth rinse – after surgery in the
mouth performed by the dentist. Five minutes after
exposure his body felt “itchy and strange”
• He left the dentist office, went to his car, turned the
switch, and 30 minutes later he woke up in the
Emergency Department, at the local hospital
• He lost his drivers licence for 3 months because doctors
thought he had a heart problem
• Although the patient was convinced that the reaction was
due to the mouth rinse
Patient 3 Pregnant female born 1962 (2006)
1987
• Forceps delivery – performed without general
anaesthesia. She was stable during the procedure
• Cervical laceration – suture in general anaesthesia
• Induction of general anaesthesia
– Fentanyl, Thiopenthone, Suxamethonium

• After induction she became cyanotic and
hypotensive
• Treatment: Rapid infusion of dextran, iv
ephedrine. Still low BP
• Reasons: Embolus to the lungs, amniotic fluid
embolus, sepsis or allergy.
1990
• Planned caesarean in general anaesthesia. She believes
that she will die during the procedure!
• Induction: Fentanyl, Thiopentone and suxamethonium.
• Reaction: BP dropped to 48 mm/Hg systolic.
Vasoconstriction, bronchospasm, cyanosis, oedema in
the face and the tongue.
• Treatment: Adrenaline 0,1 mg/ml in increments,
Ephedrine in increments and steroids
No follow-up – no warning card!

Patient 4 Female born 1942 Breast cancer surgery (2005)
• Daycare surgery
• Premedication; paracetamol and a NSAID
• Induction; remifentanil and propofol, circulation stable.
• Subcutaneous injection of Patent Blue (sentinal node)
• 20 minutes after induction;
– BP cannot be measured,
– Sinus rhythm on ECG
– Read skin, but no urticaria,
– No bronchospasm
– Saturation 68-78% on FiO2 1.0.
– 10 minutes with BP < 65 mmHg systolic
• The Emergency team was alarmed
• Treatment
• Chest compressions
• Intubation
• Extra iv lines
• Arterial line
• Ephedrine and phenylephrine
• Increments i.v with adrenaline, total 4 mg,
• Adrenaline infusion 0,1 µg/kg/min - 0,02 µg/kg/min
• Fluids
Follow-up
• Patient 1 Patient drinking cough syrup
– He refused re-challenge - but the most probable cause to the
reaction was ethyl-morphine –no other exposure
– He had antibodies towards morphine and pholcodine in serum
– Incremental challenge up to 5 mg showed tolerance to morphine.
• Patient 2 Patient with mouth rinse and spinal anaesthesia
– IgE mediated reaction towards Chlorhexidine – specific IgE and
positive skin test.
– Chlorhexidine in the mouth rinse and in the disinfectant used to
wash the operation field
• Patient 3 Pregnant female
– Suxamethonuim – identified 19 years after the
first reaction – the GP referred her
• Patient 4 Patient with breast cancer
– Patent blue

Urticaria in a patient with a suspected reaction on
patent blue
Photo: ABGuttormsen

There was a complete match between the
suspected cause and the result of
follow-up in only 7% of the cases
Challenges
• Early diagnosis
• Early and adequate treatment– Adrenaline and fluids are the cornerstones in treatment
Diagnosis and treatment are difficult!
91doctors from different specialties answered questionnaire about treatment of anaphylaxis:
92 % would give adrenaline as first line treatment
20% knew correct dose and route of administration
43% would give iv, 20% of these in doses of 1mg or greater!
Thain S, Rubython. N. Z. Med. J. April 2007
42 anaesthetists in anaphylaxis simulation:
0 made the diagnosis within 10 minutes
6 teams considered anaphylaxis after 15 minutes and heavy hints from
instructor
0 teams had a plan for treating anaphylaxis
Jacobsen Jet al. AAS 2001 45: 315-319

Study of fatal anaphylaxis
124 fatal reactions in Great Britain 1992-1998
• 47 in hospital, 31 of these in operating theatre
• Incidence 1:10.000.000 population
• Most reactions to drugs happen within 5 minutes of administration, mainly circulatory symptoms
Reasons for death:
• 48 cases no administration of adrenaline
•
• 60 cases late administration of adrenaline
• 1 case lack of clinical response to adrenaline
• 3 cases too high doses of adrenaline for mild reactions
RSH Pumphrey, Clin exp allergy 2000; 30: 1144-1150
• Identify risk patients
– Patients who have suffered severe
anaphylaxis
• A standardized follow-up to identify the
cause of anaphylaxis in risk patients
Key to success
”Anaphylaxis kit”

Reporting
Hud
Ventrikkeltachycardi
Ventrikkelfl immer
Asystoli
Annet.......................
Ingen endring
Endring av rytme
Bronkospasme
Luftveisødem
Ingen reaksjon
Ventilasjon
Kramper
Annet .............................
Ingen reaksjon
CNS
Brekning
Annet ............................
Ingen reaksjon
GI
Andre manifestasjoner
AnnetTekstReaksjonsbilde
Reaksjonsbilde
Høyeste målte
luftveistrykk
Laveste målte BT
Tid hypotensiv -
SAP<80 mmHg
Hjertefrekvens
Laveste
målte
metning
Rubor
Urticaria
Angioødem
Ingen reaksjon
/ mmHg
minutter
/min
cmH2O
%
Design Torkel Harboe

Differences between countries
• Prevalence of anaphylaxis caused by
NMBAs
– High in Norway, France, New Zealand
– Low in Denmark, Sweden, USA
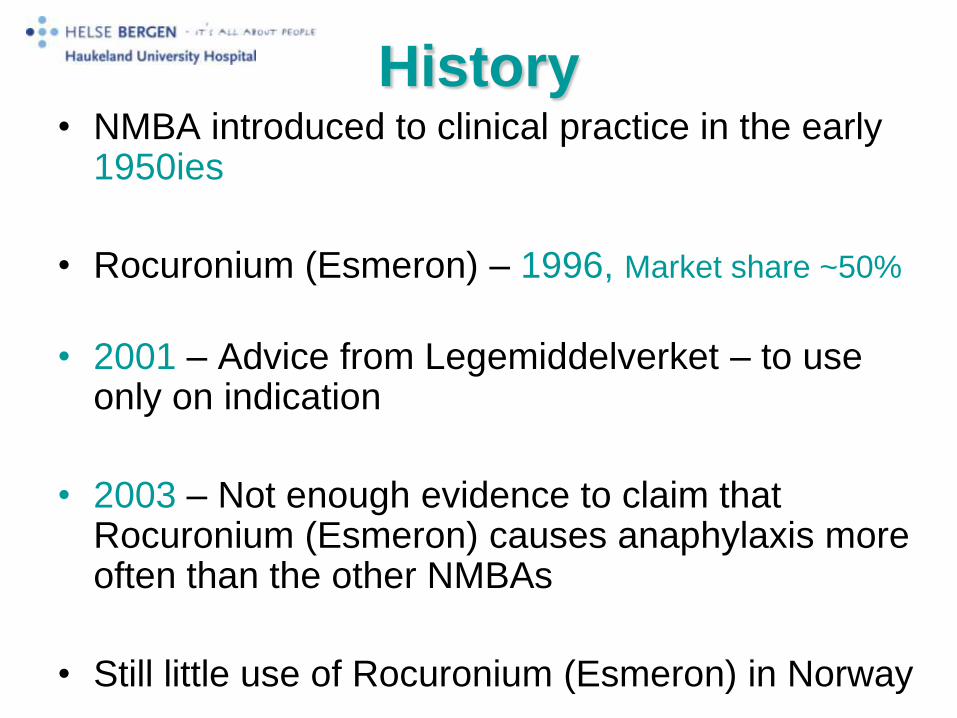
History• NMBA introduced to clinical practice in the early
1950ies
• Rocuronium (Esmeron) – 1996, Market share ~50%
• 2001 – Advice from Legemiddelverket – to use only on indication
• 2003 – Not enough evidence to claim that Rocuronium (Esmeron) causes anaphylaxis more often than the other NMBAs
• Still little use of Rocuronium (Esmeron) in Norway
HO
H
O
HO
N
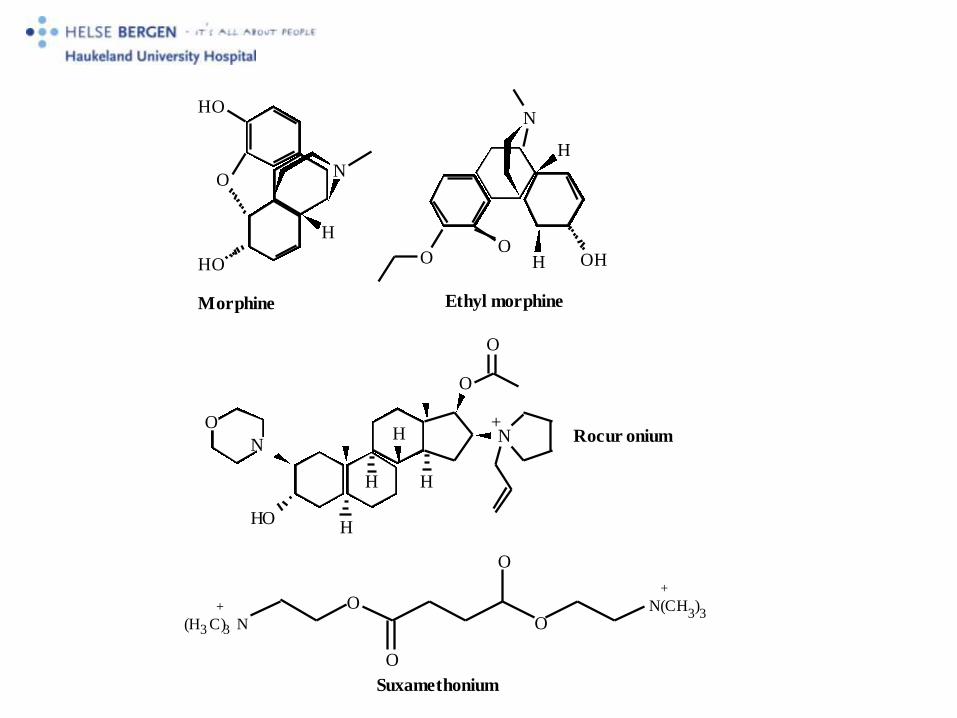
Morphine
OO
H OH
H
N
Ethyl morphine
O
HO
N
H
H
H
N
O
O
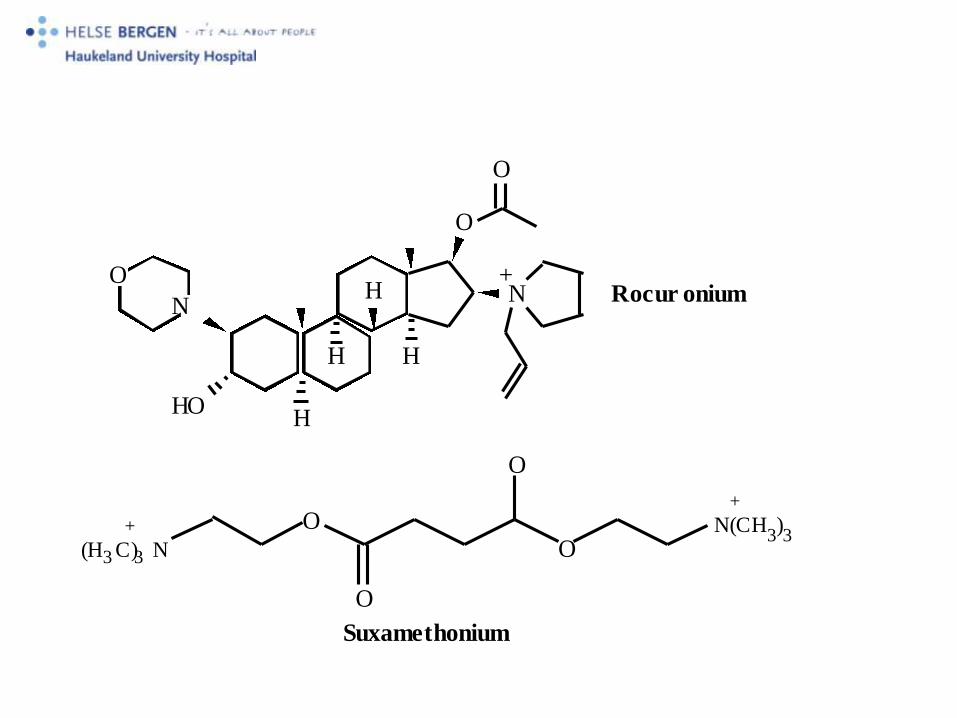
+Rocur onium
H
(H3 C)3 N
+
Suxamethonium
O
O
O
ON(CH
3)3
+
O
NCH3
H
HO
HO
Morphine
O
NCH3
H
O
HO
N
O
Pholcodine

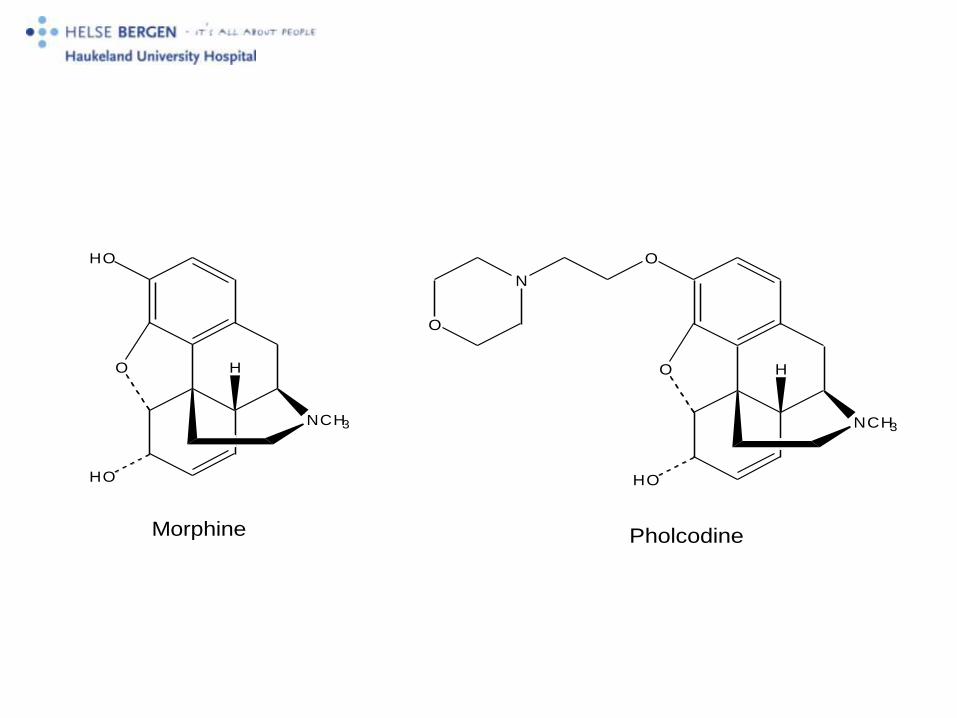
Morphine and pholcodine (PHO) are monovalent for two,
noncross reacting allergenic epitopes
QAI MOR/PHO Mo+
SGO Johansson

HO
H
O
HO
N
Morphine
OO
H OH
H
N
Ethyl morphine
O
HO
N
H
H
H
N
O
O
+Rocur onium
H
(H3 C)3 N
+
Suxamethonium
O
O
O
ON(CH
3)3
+
O
NCH3
H
HO
HO
Morphine
O
NCH3
H
O
HO
N
O
Pholcodine

IgE-mediated
allergicNon-allergic
Codeine, NMBA,
fMLP, C3a, C3b etc .
Histamine
Cytokines
Tryptase, etc
CD63
Design; Anna Nopp/SGO
Johansson
Mechanisms
“Morphine RIA is the most appropriate in vitro test for the
detection of IgE antibodies that cross-react with substituted
ammonium ions and hence for the in vitro diagnosis of NMBD-
induced anaphylaxis”.
M.Rose and M. Fisher, Brit J Anaest 2001;86:678-82
IgE antibodies to suxamethonium, morphine and
pholcodine in serum of Norwegian “nonallergics” (blood donors)
• Suxamethonium
2/500 (0.4 %)
• Morphine
25/500 (5.0 %)
• Pholcodine
30/500 (6.0 %)

Sales figures for pholcodine
• DDD per million inhabitants (1994-1998)
– Norway: 2773
– France: 2936
– United kingdom: 1522
– Ireland 3837
– New Zealand: 1458
– Finland: 944
– Denmark: 2
– Sweden 0
– USA 0

Pholcodine stimulates a dramatic increase of
IgE in IgE-sensitized individuals. A pilot study.
E. Florvaag, S.G.O. Johansson, H. Öman,
T. Harboe, A. Nopp
Haukeland University Hospital, Bergen, Norway,
Karolinska University Hospital, Stockholm, Sweden
Allergy 2006, 61:49-55

Cough syrup exposure test
Two PHO-sensitized and two non-sensitized,
healthy individuals were taking codeine alt.
noscapine (negative control) for one week
followed by one week of an OTC cough syrup
containing pholcodine.
Serum levels of IgE and IgE antibodies to
PHO, MOR and SUX were followed before
and after exposure.
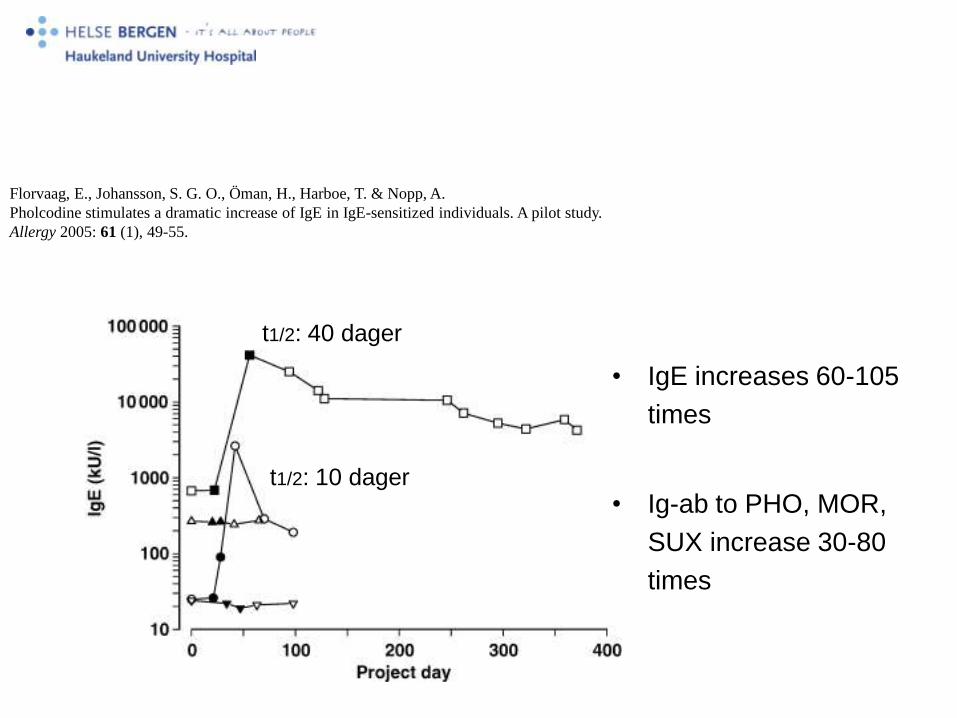
Close this WindowFlorvaag, E., Johansson, S. G. O., Öman, H., Harboe, T. & Nopp, A.
Pholcodine stimulates a dramatic increase of IgE in IgE-sensitized individuals. A pilot study.
Allergy 2005: 61 (1), 49-55.
• IgE increases 60-105
times
• Ig-ab to PHO, MOR,
SUX increase 30-80
times
t1/2: 40 dager
t1/2: 10 dager

Further studies
• The ISPHO study; International study of
pholcodine
• Animal experiments to elucidate how
pholcodine triggers IgE synthesis
How do we become better?• To train
– Patients
– Relatives
– Paramedics
– Nurses
– Doctors
• Anaphylaxis drill among hospital employees
• Focus on– How to recognize anaphylaxis?
– How to treat – appropriate doses and correct administration of adrenaline
– How to prevent new anaphylactic episodes – to perform follow-up
Guideline
Limited knowledge

Adrenaline - adults
Moderate reaction 10 - 50 µg i.v
Circulatory collapse 0,1 -1 mg i.v.
Titrate
Fluids
Crystalloid 20 ml/kg
In conclusion• Be Alert
• Be Aggressive in your approach
• To give Adrenaline and Fluids
Strategy for secondary follow-up• All patients surviving an anaphylactic shock must have a
follow-up
• Testing all drugs/substances encountered beforereaction
• Risk assessment• Which drugs/specimens should be avoided?
• Patients with in-hospital anaphylaxis are tested with latex and chlorhexidine
Garvey LH et al Acta Anaesthesiol Scand 2001
Harboe T et al, Anaesthesiology 2005
HO
H
O
HO
N
Morphine
OO
H OH
H
N
Ethyl morphine
O
HO
N
H
H
H
N
O
O
+Rocur onium
H
(H3 C)3 N
+
Suxamethonium
O
O
O
ON(CH
3)3
+