diastolic dysfunction
TRANSCRIPT
Assessment of diastolic dysfunction and anesthetic considerations in diastolic
dysfunction
By: Dr.Gopan. G Date: 19-01-2015
Moderator: Dr. Satyen Parida

Definition Inability of ventricle to fill at low atrial pressures.
Impaired relaxation impaired compliance
( Active process) ( passive process)
(Lusitrophy)

Duration of diastole
Mechanical point of view starts with closure of aortic valve
ends with closure of mitral valve
Molecular level
Dissociation of actin-myosin cross bridges
Ref: Gillebert TC, Leite-Moreira AF, De Hert SG. Relaxation-systolic pressure relation. A load-independent assessment of left ventricular contractility. Circulation 1997; 95: 745–52
Early phase of LV Ejection

Diastole – an active process

4 phases of Diastole Isovolumetric relaxation from closure of semi-lunar valves
till opening of AV valves
Rapid filling Trans valvular pressure gradient
Diastasis Low flow
Late rapid filling Atrial kick


Diastolic dysfunction- mechanisms
Slow/ incomplete myocardial relaxation- MI, LVH
Impaired peak LV filling rate
Altered elasticity- fibrosis
Pericardial constriction
LVEDP LVEDV

Clinical manifestations
Diagnosis
Gold standard Direct measurement of LV pressure & volume.
Micromanometer & conduction catheters.
Echocardiography

ECHO Trans-mitral flow velocity
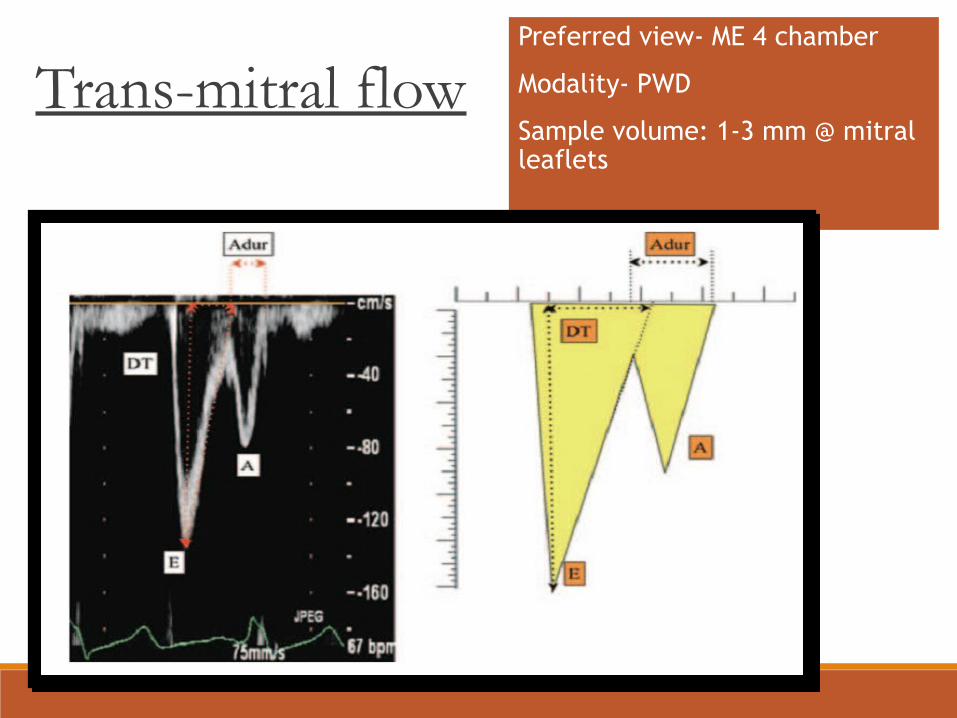
Trans-mitral flow Preferred view- ME 4 chamber
Modality- PWD
Sample volume: 1-3 mm @ mitral leaflets

Trans-mitral flow
Peak E wave velocity: 70 – 100 cm/sec.
Peak A wave velocity: 45 – 70 cm/sec.
E deceleration time (DT): 160 – 240 msec.
Iso- Vol. Relaxation Time- 65± 20 ms.
The deceleration time (DT) shows the pressure decay of early
filling. The shorter the DT, the higher the filling pressure.

1) Impaired relaxation pattern
E/A <1 DT ↑ ( >240 ms) IVRT > 90 ms.

2) Pseudo- normal pattern

3) Restrictive pattern
E/A > 1.5
DT ↓ (<160 ms)
IVRT < 70 ms.

Trans-mitral flow
Limitations
Affected by age, rate, rhythm, loading conditions, LV systolic function,
Atrial function & mitral valve disease.
Cannot be used in isolation to predict Diastolic dysfunction
Limitations
Affected by age, rate, rhythm, loading conditions, LV systolic function,
Atrial function & mitral valve disease.
Cannot be used in isolation to predict Diastolic dysfunction

Pulmonary venous inflow
Preferred view- ME 4C view
for LUPV
Modality- PWD
Sample volume 2-3mm, 1-2
cm into PV
Pulsatile PVF pattern is generated by the ‘x’ and ‘y’ descents of the LAP tracing

Normal pulmonary venous flow
Peak S wave velocity: 60 ± 15 cm/sec.
Peak D wave velocity: 40 ± 15 cm/sec.
Peak S / Peak D ratio: 1.3 – 1.5 ( ± 0.3).
Peak Ar wave velocity: -32 cm/sec.
Ar duration: 137 + 31 msec.

Pulmonary venous flow
Limiting factors
Technical difficulties in
getting arterial waveforms
Load dependence
LA wall artifacts
Effects of arrhythmias
Ar velocity > 35 cm/s and (Ar- Adur) > 30 msec is highly predictive of LVEDP > 15 mm Hg.Ref: Rossvol et al JACC; 1999 21: 1687
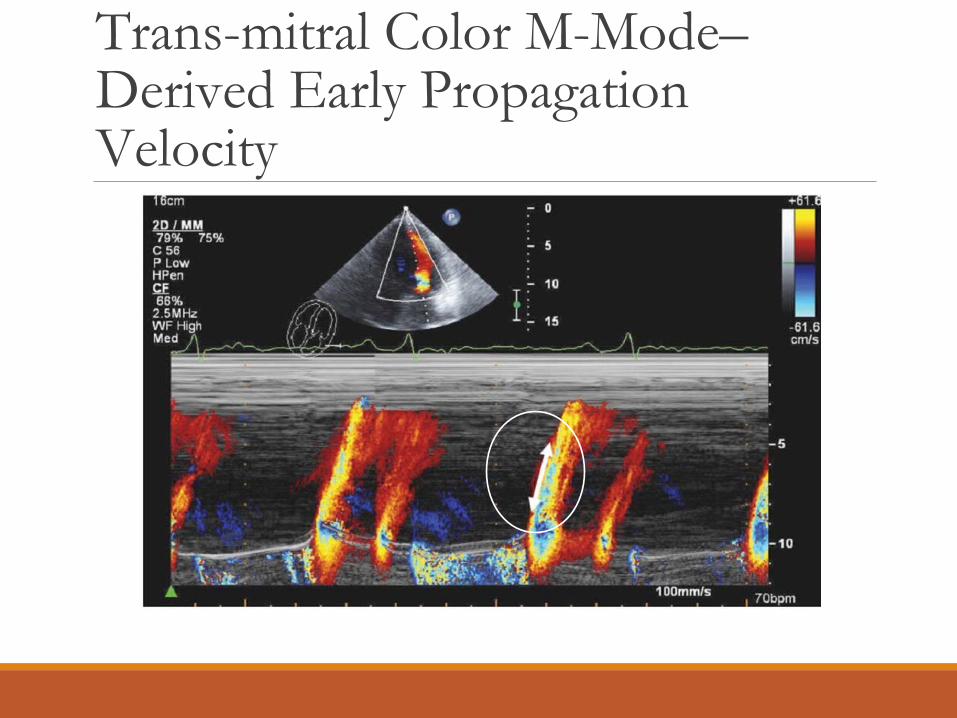
Trans-mitral Color M-Mode–Derived Early Propagation Velocity
Early diastolic LV filling
Wave front of propagation from LV base to apex
Preferred view- ME 4C view
Modality- CFD and M mode
Colour flow sector- on LV cavity with parallel M-mode alignment
Trans- mitral velocity profile (Vp) ≈ LV suction in early diastole
Less affected by preload than TMF and PVF.
Trans-mitral Color M-Mode–Derived Early Propagation Velocity

Trans-mitral Color M-Mode–Derived Early Propagation Velocity
Method described by Garcia et al., in which the slope of the first aliasing
velocity (the outermost velocity) is measured, is considered the most
reliable and reproducible method.
A Vp value of <0.50 m/s is consistent with impaired relaxation.

Trans-mitral Color M-Mode–Derived Early Propagation Velocity
Limitations
may not be possible to measure Vp because the slope of flow
propagation is sometimes curvilinear and does not “travel” a
sufficient distance (<4 cm) into the LV cavity or is difficult to
appreciate.
merely diagnoses the presence of abnormal relaxation, and not
necessarily its severity.

Doppler Tissue Imaging Measures tissue velocities and motion.
Preferred view- ME 4C
Modality- PWD optimized for tissue motion
Sample volume- 5- 10 mm within 1 cm of mitral leaflet insertion

Doppler Tissue Imaging
Reduced E’ velocity for age
is considered diagnostic of
abnormal LV relaxation.
E’- Early diastolic waveA’ – Late diastolic waveS’ – Systolic wave

Doppler Tissue Imaging
E/ E’ ratio < 8 identifies patients with normal LVEDP
E/ E’ ratio > 15 identifies patients with LVEDP > 12 mm Hg
Ref: Nagueh et al. JACC 1997. 30: 1527
Doppler Tissue Imaging
Average E’ velocity may not accurately represent global LV
diastolic function in the presence of basal lateral and septal
wall motion abnormalities.
E’ wave represents only the relaxation (early) phase of
diastole and does not provide any information about LV
compliance.

Prognosis
Diastolic dysfunction develops early in most cardiac diseases.
Clinical studies have shown the association of short mitral DT with heart-failure and death.
Pulmonary venous velocities was less frequently examined but were still predictive of clinical events.
Several studies have shown that E/E´ is highly predictive of adverse events. It is the most reproducible echocardiographic parameters to estimate PCWP and is the preferredprognostic parameter in many cardiac conditions.
Anesthetic considerations in diastolic dysfunction
Effect of inhalational anaesthetics on diastolic function
Halothane and sevoflurane do not cause prolongation of the IVRT.
In preexisting diastolic dysfunction, sevoflurane causes a slight improvement in early LV relaxation assessed with E’ velocity.
Isoflurane did not exacerbate preexistent diastolic dysfunction and had no lusitropic effects.

Effect of IV anaesthetics on diastolic function
Propofol prolongs the IVRT in patients with no history of cardiac disease, but does not cause worsening of preexisting diastolic dysfunction.
Barbiturates and ketamine exert similar effects by inhibition of sarcolemmal transport of calcium ions.
The impact of etomidate on LV diastolic function has not been studied

Anaesthetic considerations
Detailed Pre-operative evaluation
Assessment of functional status & exercise tolerance
Optimizing the patient

Perioperative drugs
Diuretics
Beta blockers, calcium channel blockers
ACEI & ARBs
Statins
Antiplatlets
Monitoring - Major surgeries
Standard monitoring tools
Invasive arterial pressures
Monitoring volume status is important
Central venous pressures or Pulmonary artery catheter or TEE

GA or Regional
No definite recommendation either way
Epidural vs. spinal ?
Epidural wins

General anesthesia
Good induction practices
Consideration for age
Titrate to effect
Hpoxia, hypercarbia worsens PHT

General anesthesia
IV induction & maintained with volatile agents ,
opioids & muscle relaxants.
Greater hemodynamic instability

Drug combination for hemodynamics Low dose nitroglycerin and titrated phenylephrine
Either agent alone can worsen the hemodynamics

Nitroglycerine + Titrated phenylephrine
1. Preserves vascular distensibility
2. Avoids reduction in preload
3. Maintains coronary perfusion pressure
4. Maintains stroke volume with minimal cardiac work

Management of hypertensive crisis
Sound anesthetic practices
Plan for post-op analgesia
Intravenous calcium channel blocker
IV nitroglycerin
Post-op diastolic heart failure
Optimise preload
Diuretics
Use of nitrates
CPAP
As contractile function is preserved, the role of sympathomimetic
inotropes is limited.

Specific drugs for diastole Milrinone
o Phosphodiesterase III inhibitor
o Inotropic, vasodilatory with minimal chronotropy
o Increases calcium ion uptake to SR
o Lusitropic effect more evident in heart failure
o Bolus dose of 50µgm/Kg over 60 minutes
o Infusion of 0.375 to 0.75µgm/Kg/min

Specific drugs for diastole Levosimendan
o Sensitizes the contractile elements to calcium and a has
positive inotropic effect, by modulating the interaction
between troponin and calcium.
o combines a vasodilator effect, by opening ATP-sensitive
potassium channels.
o Improves both systolic and diastolic function
Conclusion
The prognostic significance of diastolic dysfunction in
cardiac patients cannot be understated.
A simplified approach will allow assessment of severity of
diastolic function in nearly all cases and allow tailoring of
management.

Practical approach to diastolic dysfunction
Ref: Nagueh et al European Journal of Echocardiography (2009) 10, 165–193

Thank you