diagnostic intervention in breast...
TRANSCRIPT
Document down
Radiología. 2011;53(6):531---543
www.elsevier.es/rx
UPDATE IN RADIOLOGY
Diagnostic intervention in breast disease�
A. Vega Bolívar
Sección de diagnóstico por imagen mamaria, Hospital Universitario Marqués de Valdecilla, Santander, Spain
Received 26 January 2011; accepted 1 June 2011
KEYWORDSCore biopsy;Vacuum-assistedbreast biopsy;Galactography
Abstract Imaging-guided percutaneous biopsy techniques have been developed to diagnosethe lesions detected in breast cancer screening programs based on mammography.
Although traditional fine-needle aspiration cytology continues to be indicated in some cases,in many others it has been supplanted by more modern techniques such as core biopsy orvacuum-assisted biopsy guided by ultrasonography, stereotaxy, or magnetic resonance imaging.These highly reliable techniques have minimized the need for surgical biopsy.
Radiologists play a key role in the histological diagnosis of breast cancer in the early stages ofdisease and in the evaluation of its local and regional extensions through magnetic resonanceimaging and sentinel node biopsy.© 2011 SERAM. Published by Elsevier España, S.L. All rights reserved.
PALABRAS CLAVEBiopsia mama;Estereotaxia;Galactografía
Intervencionismo diagnóstico en patología de mama
Resumen Con el desarrollo de los programas de detección precoz de cáncer de mama basadosen la mamografía se han ido desarrollando de forma paralela técnicas de biopsia percutáneaguiadas por la imagen para el diagnóstico de las lesiones detectadas sospechosas de cáncer demama.
Aunque la técnica tradicional de punción con aguja fina sigue teniendo indicaciones, se ha idosustituyendo por las mas modernas técnicas de biopsia con aguja gruesa o sistemas de biopsiaasistidos por vacío, con guía ecográfica, estereotáxica o por resonancia magnética (RM). Losresultados de esta técnica son de una alta fiabilidad, por lo que se ha reducido al mínimo la
loaded from http://http://zl.elsevier.es, day 22/10/2013. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
biopsia quirúrgica.El papel del radiólogo es determinante para el diagnóstico histológico del cáncer de mama
en sus fases iniciales, la valoración de su extensión local y regional mediante la utilización dela RM y realización de la técnica del ganglio centinela.
or El
© 2011 SERAM. Publicado p� Please cite this article as: Vega Bolívar A. Intervencionismo diagnóstiE-mail address: [email protected]
2173-5107/$ – see front matter © 2011 SERAM. Published by Elsevier Esp
sevier España, S.L. Todos los derechos reservados.
co en patología de mama. Radiología. 2011;53:531---43.
aña, S.L. All rights reserved.
5
idbm
aobas
dwstapod
Pl
Pt
ntio
T
Aptub
WWtmpv
f
Fac
Document downloaded from http://http://zl.elsevier.es, day 22/10/2013. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
32
Mammography, ultrasonography, and magnetic resonancemaging (MRI) have proved to be very effective in the earlyetection, diagnosis, and evaluation of the extension ofreast cancer, which have played a decisive role in reducingortality caused by this disease.1
Radiologists specialising in this field have recentlyssumed new responsabilities, including early detectionf breast cancer, accurate diagnosis through percutaneousiopsy techniques, assessment of local extension using MRI,nd use of radiotracers for a correct performance of theentinel node technique.
Until recently, excisional surgical biopsy was the tra-itional technique for diagnostic confirmation. However,ith the widespread implementation of population-based
creening programs for early breast cancer detection andhe definitive consolidation of ultrasonography and MRIs complementary imaging techniques, new interventionalrocedures guided by these techniques have been devel-ped with the aim of achieving an accurate histologiciagnosis without the need of surgery.2
reoperative localization of non-palpable
esionsreoperative localization is the traditional technique andhe most commonly used technique. Operative excision of
msue
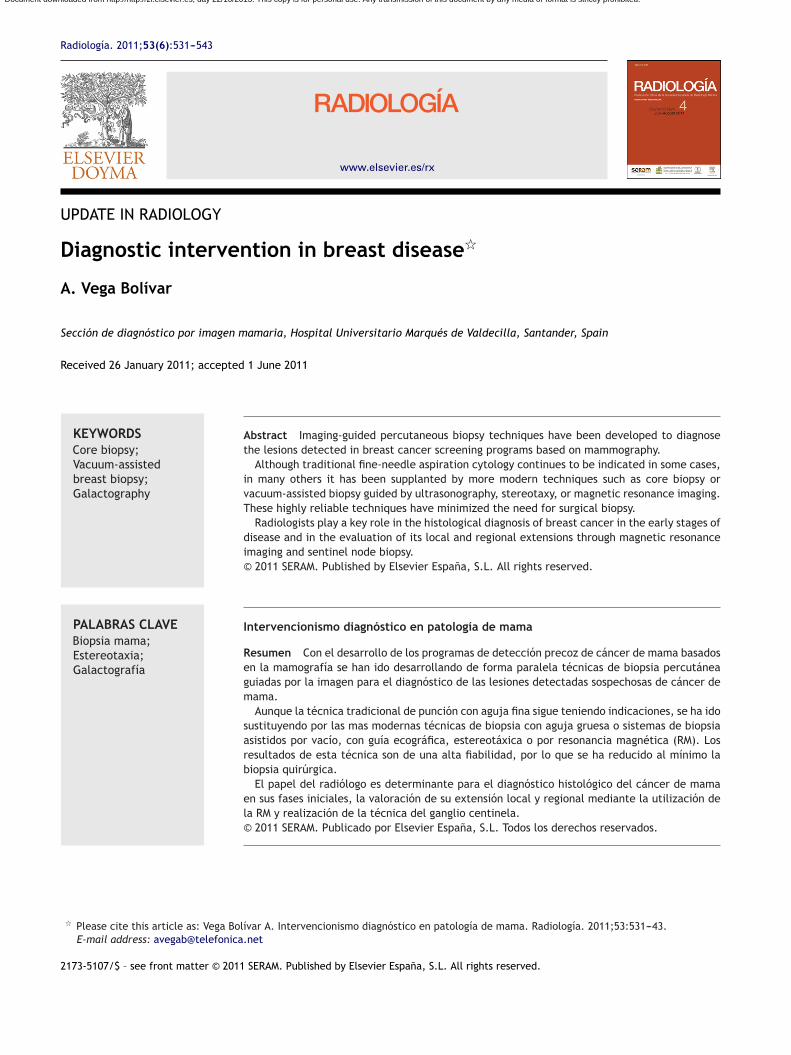
igure 1 Preoperative localization for biopsy of a non-palpablelphanumeric grid. (B) Types of needles with localizing guide wiompression plate.
A. Vega Bolívar
on-palpable lesions requires prior localization of lesionshat usually involves the placement of guide wires or mark-ng the site of the biopsy by injecting a stable carbon solutionr a radiotracer.3
echnique and results
lthough the localization technique originally involved thelacement of needles into the lesion site, guided by localiza-ion coordinates provided by mammography, overtime these of needles has been replaced by wires as they allow foretter anchorage into the breast.
ires (hookwires)ires are radiopaque and their tips have been designed
o avoid displacement once placed into the breast. Mam-ographic or ultrasonographic guidance can be used forlacement, depending on which technique provides the bestisualisation of the lesion.
Mammographic guidance is commonly performed withenestrated compression plates with a radiopaque alphanu-
eric grid (Fig. 1). Some radiologists prefer to use thetereotactic device, but we need to keep in mind thatnwanted displacement may occur due to the ‘‘accordionffect’’ that appears when the breast is decompressed.
lesion. (A) Fenestrated compression plate with radiopaqueres (‘‘hook wires’’). (C) Harpoon insertion with fenestrated
Diagnostic intervention in breast disease 533
ue.
l plan
es
RTtapupAou
mtgsp
of
Document downloaded from http://http://zl.elsevier.es, day 22/10/2013. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
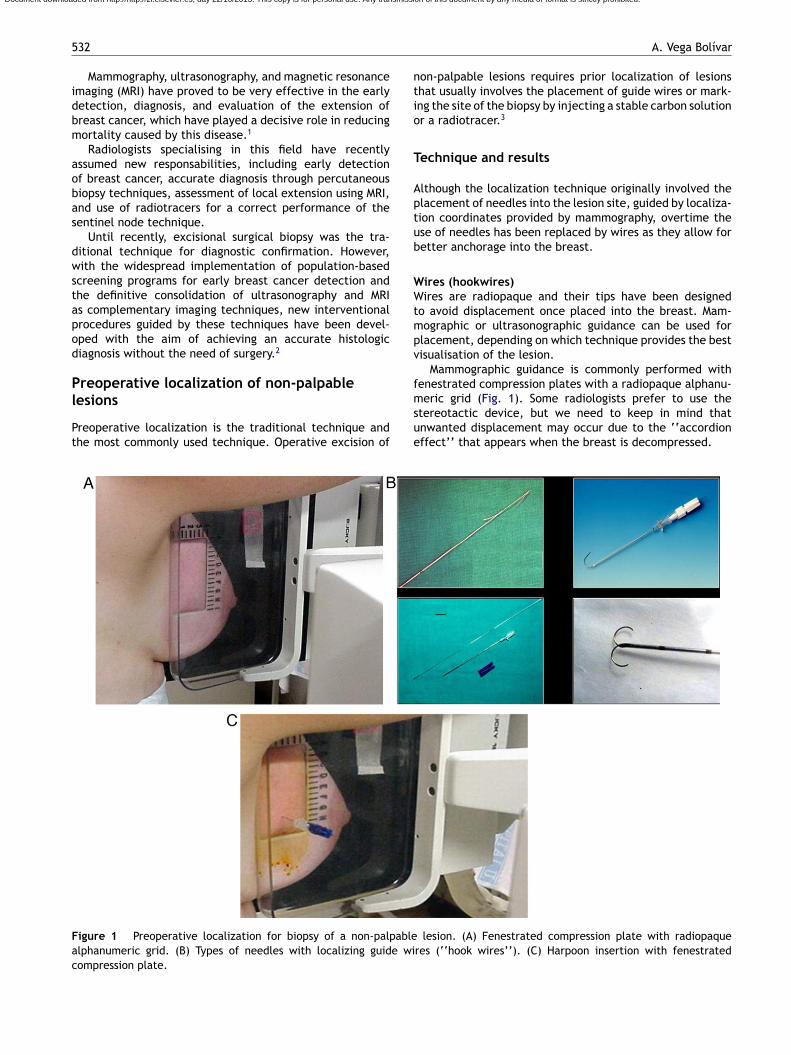
Figure 2 Fine needle aspiration (FNA). (A) Free-hands techniqit back in a number of times, while maintaining aspiration in al
Whenever possible, ultrasonographic guidance shouldbe used because the patient may lie down, the techniquedoes not require breast compression and does not exposethe patient to ionising radiation. Moreover, the mammog-raphy room is free and the procedure is monitored in realtime.
Obviously, ultrasonographic guidance is not possible inthose cases in which the lesion can only be visualised on MRI.In such cases, a non-ferromagnetic marker can be placed inthe lesion site to facilitate subsequent mammographic orultrasonographic localization.
Regardless of the guidance technique used, the accessthat provides the surgeon the shortest path to the lesionshould always be chosen. In all cases, the localization ofthe hookewire must be confirmed using two views, lateraland craniocaudal that must be shown to the surgeon priorto operation so that he become aware of the spatial rela-tionship between the wire and the lesion, the depth andthe most appropriate surgical approach. Large lesions mayrequire the placement of two or more hookwires.
Injection carbon solutionAlthough less common, those who use this method argue that
it is very accurate. It involves ‘‘tattooing’’ the biopsy site byinjecting a stable carbon solution. Although this technique issafe, less costly than wire localization and can be performedseveral days before the intervention, it is not free of adverse5bpr
Aspiration is performed by withdrawing the needle and pushinges. (B) Material spreading.
ffects, such as potential histologic changes at the biopsyite.4
OLL (radio-guided occult lesion localization) techniquehis method involves imaging-guided injection of a radio-racer into the biopsy site. The aim is the preoperativend postoperative localization of the lesion using a gammarobe. A main advantage of this technique is that, whensed for localization in therapeutic procedures, it can beerformed in conjunction with the sentinel node technique.dditionally, there seem to be evidence that the likelihoodf obtaining tumor-free margins in the surgical specimensing ROLL.5
Regardless of the technique and the imaging guidanceodality used, the surgical specimen should be X-rayed
o confirm lesion resection. On some occasions, ultrasono-raphic examination of the specimen is required to mark theite of the lesion by placing one or more needles to help theathologist in the localization of the lesion.
The accuracy of these techniques for the localizationf non-palpable lesions is variable. The failure rates rangerom 2% to 18%, but desirable values should be lower than
%. Failure to resect the lesion is most frequently causedy incorrect placement of the localization device, dis-lacement of the device, or poor communication betweenadiologist and surgeon.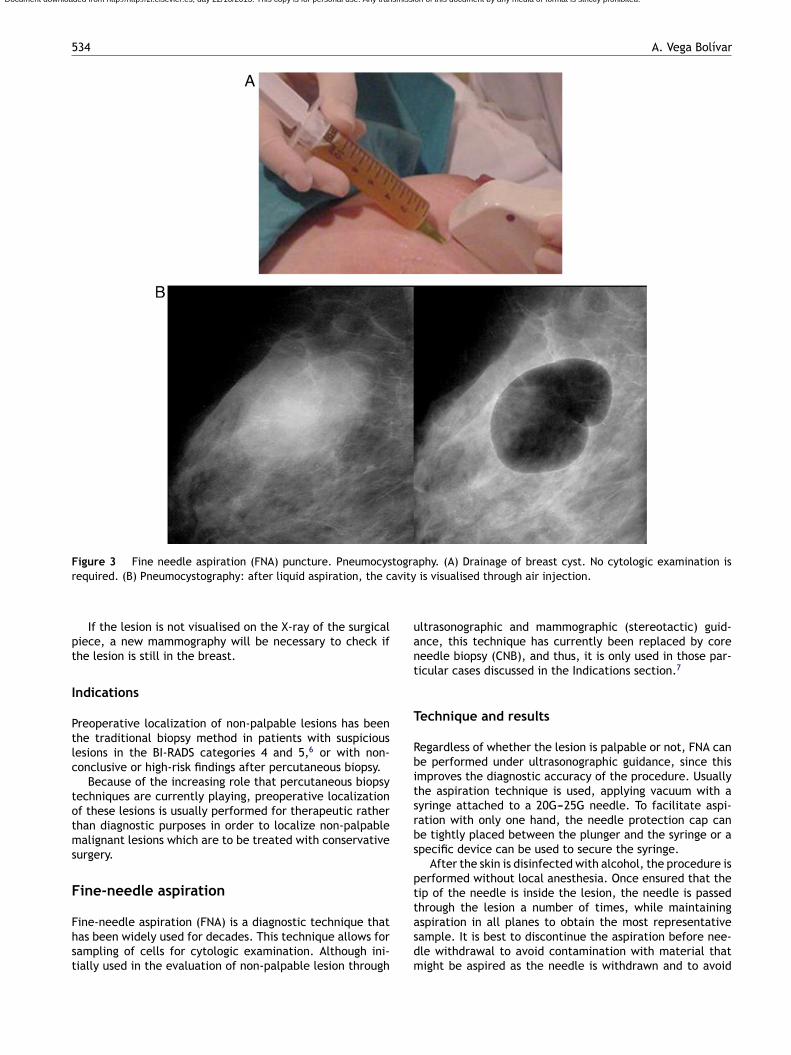
534 A. Vega Bolívar
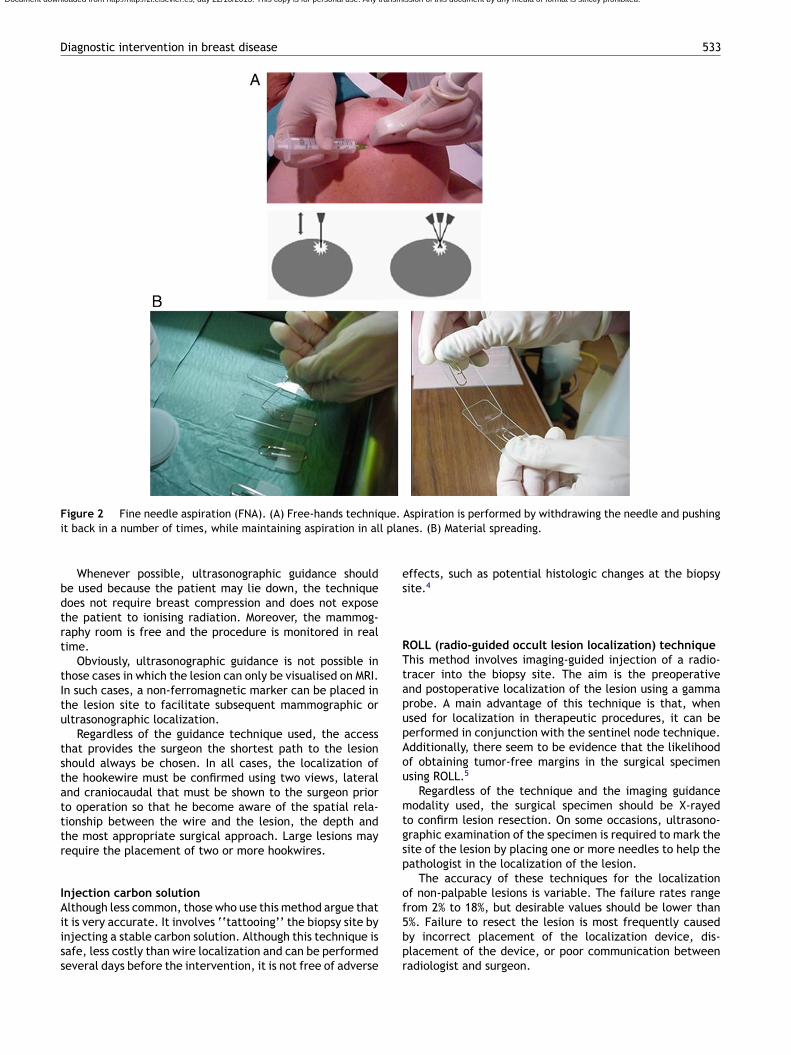
Figure 3 Fine needle aspiration (FNA) puncture. Pneumocystography. (A) Drainage of breast cyst. No cytologic examination isr avity
pt
I
Ptlc
totms
F
Fhst
uant
T
Rbitsrbs
ptt
Document downloaded from http://http://zl.elsevier.es, day 22/10/2013. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
equired. (B) Pneumocystography: after liquid aspiration, the c
If the lesion is not visualised on the X-ray of the surgicaliece, a new mammography will be necessary to check ifhe lesion is still in the breast.
ndications
reoperative localization of non-palpable lesions has beenhe traditional biopsy method in patients with suspiciousesions in the BI-RADS categories 4 and 5,6 or with non-onclusive or high-risk findings after percutaneous biopsy.
Because of the increasing role that percutaneous biopsyechniques are currently playing, preoperative localizationf these lesions is usually performed for therapeutic ratherhan diagnostic purposes in order to localize non-palpablealignant lesions which are to be treated with conservative
urgery.
ine-needle aspiration
ine-needle aspiration (FNA) is a diagnostic technique thatas been widely used for decades. This technique allows forampling of cells for cytologic examination. Although ini-ially used in the evaluation of non-palpable lesion through
asdm
is visualised through air injection.
ltrasonographic and mammographic (stereotactic) guid-nce, this technique has currently been replaced by coreeedle biopsy (CNB), and thus, it is only used in those par-icular cases discussed in the Indications section.7
echnique and results
egardless of whether the lesion is palpable or not, FNA cane performed under ultrasonographic guidance, since thismproves the diagnostic accuracy of the procedure. Usuallyhe aspiration technique is used, applying vacuum with ayringe attached to a 20G---25G needle. To facilitate aspi-ation with only one hand, the needle protection cap cane tightly placed between the plunger and the syringe or apecific device can be used to secure the syringe.
After the skin is disinfected with alcohol, the procedure iserformed without local anesthesia. Once ensured that theip of the needle is inside the lesion, the needle is passedhrough the lesion a number of times, while maintaining
spiration in all planes to obtain the most representativeample. It is best to discontinue the aspiration before nee-le withdrawal to avoid contamination with material thatight be aspired as the needle is withdrawn and to avoid
535
Figure 4 Ultrasound-guided core needle biopsy (CNB).(A) Free-hands technique using an automated device with 14Gta
bw
FTwBtaAp
Document downloaded from http://http://zl.elsevier.es, day 22/10/2013. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Diagnostic intervention in breast disease
aspiration of this material into the syringe. Once the needleis withdrawn, the material is transferred and smeared ontoa slide and fixed according to the recommendations of thePathologic Anatomy Laboratory (Fig. 2).
Although this technique has practically no complications,slight pressure on the site of puncture should be appliedfor some minutes to avoid hematomas. Significantly largehematomas rarely occur. The risk of more serious conditions,such as pneumothorax, is almost inexistent if an adequatepuncture technique is performed with controlled needleadvancement.
An expert cytopathologist is necessary to obtain conclu-sive findings. The cytopathologist report is based on thefollowing categories: normal, benign, atypical, suspicious,malignant, and insufficient.
The sensitivity of FNA varies significantly (70---90%)because false negatives sometimes occur. Atypical or suspi-ciously malignant lesions always require histologic diagnosisby percutaneous or surgical biopsy.8 In spite of its high speci-ficity, this technique also yields false positives (1---2%). Forthis reason, in case of malignant findings, most surgeons andgynecologists only take a surgical decision after performingan intraoperative biopsy. In addition, FNA does not discrim-inate between in situ and infiltrating carcinomas. A benignfinding is only reliable in patients with BI-RADS category3 lesions.
Indications
FNA is used both for palpable and non-palpable lesions.Below are the most common indications.
Drainage of palpable cystsThis is a very common clinical situation leading patients toa state of anxiety, although the use of FNA is very effective.Drainage is performed under ultrasonographic guidance,sometimes followed by a mammography after injection ofa volume of air equal to two thirds of the extracted fluid(pneumocystography). This procedure is no longer diag-nostically useful because of the high quality of currentultrasonographic imaging, and its therapeutic role in redu-cing the recurrence of cysts is being questioned (Fig. 3).Pneumocystography should not be performed on cysts withintracystic solid lesions given the possibility of failing toidentify the solid lesions for subsequent biopsy. Although acytologic analysis of the drained liquid is not necesssary, itcan be useful if a palpable lesion is still appreciable in thebreast after drainage.
Differentiation between solid and cystic lesionsThere may be nonconclusive diagnoses, as sometimes occurin complex cysts. These cysts are echogenic because theycontain inflammatory fluid that can mimic a solid lesion onultrasonography.
Cytologic examination of palpable areas
This analysis is particularly common when dealing withbenign-looking lesions (BI-RADS category 3), which typicallyoccur in young women, and are usually suggestive of afibroadenoma.oBd
rucut needle. (B) Devices for CNB: automated and semi-utomated devices.
It can also be useful in patients with undefined palpa-le areas, having no clear radiologic correlation, or patientsith dense breasts.
NA of axillary lymph nodeshis is a common procedure that is performed in patientsith breast cancer to assess the state of their axillas.ecause of positivity of the FNA puncture, the sentinel nodeechnique is not necessary. Puncture of supraclavicular, infr-clavicular and laterocervical adenopathies is usual as well.ll of these conditions are readily imaged by ultrasonogra-hy.
Further indications of the FNA technique are puncturef nodes of probable inflammatory or infectious nature,I-RADS category 3 multiple nodes and other particular con-itions.

536 A. Vega Bolívar
F ighert
C
Ctotgc
dh
Fb
Document downloaded from http://http://zl.elsevier.es, day 22/10/2013. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
igure 5 Core needle biopsy (CNB): types of samples. The hissue (less diagnostic value).
ore needle biopsy
ore needle biopsy (CNB) puncture has gained wide accep-ance as the technique of choice in the histologic diagnosis
f palpable and non-palpable breast lesions, especially inhose cases in which the lesion is visualised on ultrasono-raphic images. Being a safe, fast, complication-free andost-efficient technique,9 CNB has been shown to have a highT
Ca
igure 6 Vacuum-assisted biopsy (VAB): sequence featuring excisielow the lesion. Contiguous samples up to five times as big as thos
flotability of the specimens means more concentration of fat
iagnostic accuracy to evaluate any breast lesions requiringistologic diagnosis.
echnique and results
NB is performed with automated or semiautomated devicesnd 14G (2.1 mm in diameter) trucut needles used to
on of a probably benign nodular lesion. Notice the 11G cannulae obtained with 14G needles.

Diagnostic intervention in breast disease 537
Figure 7 Stereotactic technique involving vacuum-assisted biopsy (VAB). (A) Patient on prone-table. For easier access to thethe otion,
ti
aiwdii
Document downloaded from http://http://zl.elsevier.es, day 22/10/2013. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
breast tail, it is advisable to introduce the patient’s arm into
breast calcifications performed with a 11G cannula. After resec
remove a tissue sample from the lesion (Fig. 4). CNB isdone with local anesthetic, normally taking three to fivecores----although more cores are recommended in cases ofbiopsy of clustered calcifications.
The imaging techniques that are commonly used as guid-ance are stereotaxis, and particularly, ultrasonography.
Stereotactic guidanceThis technique relies on the calculation of the localization
coordinates of the lesion, based on evaluation of the appar-ent lesion displacements on two mammographic imagesobtained at a ±15---20◦ angulation on the lesion. Digitalprone-table stereotactic units allow for shorter examinationUTa
pening. (B) VAB with 11G cannula (lateral access). (C) VAB of a clip is placed to mark the biopsy site.
imes and minimize the chance of the patient moving thatmproves the results.
Stereotactic biopsy provides highly reliable results,lthough false negatives may occur. Moreover, when deal-ng with calcifications, the lesion can be underestimatedhen biopsy findings reveal atypical hyperplasia or intra-uctal carcinoma (approximately 50% of the former arentraductal carcinomas, and 30% of the latter are found to benfiltrating carcinomas at surgery).10
ltrasonographic guidancehis is the best technique for lesions that can be visu-lised on ultrasonography. The technique is similar to that

538 A. Vega Bolívar
Figure 8 Ultrasound-guided VAB with a 11G cannula. Freehands technique as used in the rest of ultrasound-guided tech-n
dt
srinc
vica
idi
n
A
Tlsd9
emcas
D
Bg
Figure 9 MRI-guided VAB. (A) Device used for MRI-guidedb
SClIaamitc
tt
HAcatam
mbb
Document downloaded from http://http://zl.elsevier.es, day 22/10/2013. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
iques.
escribed for FNA, although the larger needle gauge requireshe use of local anesthesia.
Ultrasonographic guidance is a better approach thantereotactic guidance because it does not rely on ionisingadiation, is more effective in multidirectional lesion local-zation, enables real-time visualisation and control of theeedle, and offers greater patient comfort. Moreover, itosts less.
As with FNA, CNB under ultrasonographic guidance hasirtually no complications. In fact, it can be performedn patients on anticoagulant therapy. The most commonomplications are hematomas, which are generally small,nd do not require any treatment.
Needle-track seeding after is not unique to CNB sincet can also occur in any other interventionional proce-ure, such as surgical biopsy, and is considered virtuallyrrelevant.11
Pneumothorax occurs very rarely if an appropriate tech-ique is performed.
dvantages
he main advantage of CNB is that it provides a histo-ogic diagnosis of all lesion types, with a rate of insufficientpecimens significantly lower than that of cytology. Theiagnostic value of ultrasound-guided CNB is very high (over5%).12,13
Another advantage of this technique is that it can differ-ntiate between intraductal and infiltrating carcinoma inost cases. This reduces the surgical decision-making pro-
ess to one single stage. The costs of the biopsy process arelso reduced because of the decreased need of diagnosticurgery.
rawbacks
elow are the major drawbacks of this technique, which areenerally associated with the biopsy of calcifications.
wbn
iopsy. (B) Placement of the VAB device for biopsy.
ampling errorsNB involves the removal of small tissue samples from the
esion, which may not be representative of the entire lesion.n highly suspicious lesions, a malignant finding is regardeds correct. However, if benign, it might prompt questionsbout the validity of the sample (particularly in cases oficrocalcifications), thus, additional CNB or surgical biopsy
s indicated. The sample is considered appropriate whenhe histologic findings are consistent with the imaging andlinical examination.
A good indication is the evaluation of the floatability ofhe cores in formalin (cores that sink in formalin are likelyo be diagnostic) (Fig. 5).
istologic underestimation CNB finding revealing atypical hyperplasia or intraductalarcinoma may significantly underestimate the presence ofn intraductal or infiltrating carcinoma, respectively. Thisypically occurs with microcalcifications and requires andditional CNB or surgical biopsy in order to reach a confir-ation of the diagnosis.14
In addition, there is a specific set of high-risk lesions thatay also be misdiagnosed or underestimated at CNB: wheniopsy reveals a benign papillary tumour, a radial scar, aenign phyllodes tumour or a lobular carcinoma in situ, itill be necessary to rely on surgery or on vacuum-assisted
iopsy (VAB) (see next section) for a fully conclusive diag-osis.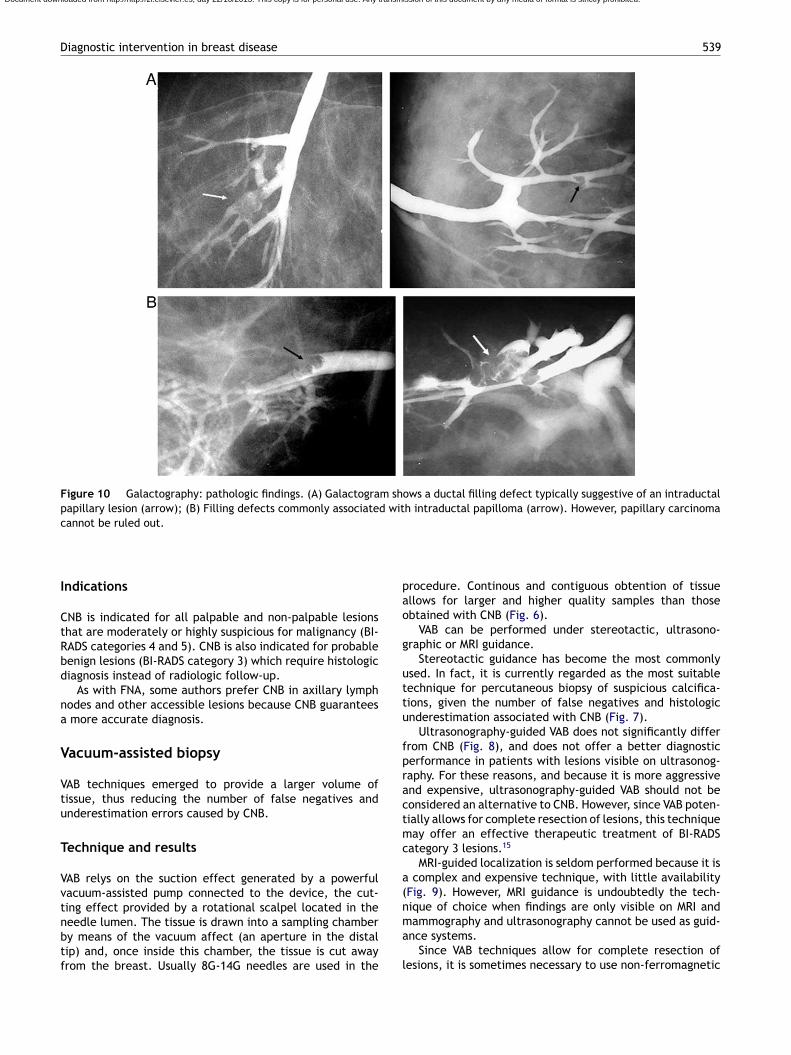
Diagnostic intervention in breast disease 539
Figure 10 Galactography: pathologic findings. (A) Galactogram shows a ductal filling defect typically suggestive of an intraductalpapillary lesion (arrow); (B) Filling defects commonly associated with intraductal papilloma (arrow). However, papillary carcinomacannot be ruled out.
pao
g
uttu
fpractmc
a(n
Document downloaded from http://http://zl.elsevier.es, day 22/10/2013. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Indications
CNB is indicated for all palpable and non-palpable lesionsthat are moderately or highly suspicious for malignancy (BI-RADS categories 4 and 5). CNB is also indicated for probablebenign lesions (BI-RADS category 3) which require histologicdiagnosis instead of radiologic follow-up.
As with FNA, some authors prefer CNB in axillary lymphnodes and other accessible lesions because CNB guaranteesa more accurate diagnosis.
Vacuum-assisted biopsy
VAB techniques emerged to provide a larger volume oftissue, thus reducing the number of false negatives andunderestimation errors caused by CNB.
Technique and results
VAB relys on the suction effect generated by a powerfulvacuum-assisted pump connected to the device, the cut-ting effect provided by a rotational scalpel located in the
needle lumen. The tissue is drawn into a sampling chamberby means of the vacuum affect (an aperture in the distaltip) and, once inside this chamber, the tissue is cut awayfrom the breast. Usually 8G-14G needles are used in thema
l
rocedure. Continous and contiguous obtention of tissuellows for larger and higher quality samples than thosebtained with CNB (Fig. 6).
VAB can be performed under stereotactic, ultrasono-raphic or MRI guidance.
Stereotactic guidance has become the most commonlysed. In fact, it is currently regarded as the most suitableechnique for percutaneous biopsy of suspicious calcifica-ions, given the number of false negatives and histologicnderestimation associated with CNB (Fig. 7).
Ultrasonography-guided VAB does not significantly differrom CNB (Fig. 8), and does not offer a better diagnosticerformance in patients with lesions visible on ultrasonog-aphy. For these reasons, and because it is more aggressivend expensive, ultrasonography-guided VAB should not beonsidered an alternative to CNB. However, since VAB poten-ially allows for complete resection of lesions, this techniqueay offer an effective therapeutic treatment of BI-RADS
ategory 3 lesions.15
MRI-guided localization is seldom performed because it is complex and expensive technique, with little availabilityFig. 9). However, MRI guidance is undoubtedly the tech-ique of choice when findings are only visible on MRI and
ammography and ultrasonography cannot be used as guid-nce systems.Since VAB techniques allow for complete resection of
esions, it is sometimes necessary to use non-ferromagnetic
540 A. Vega Bolívar
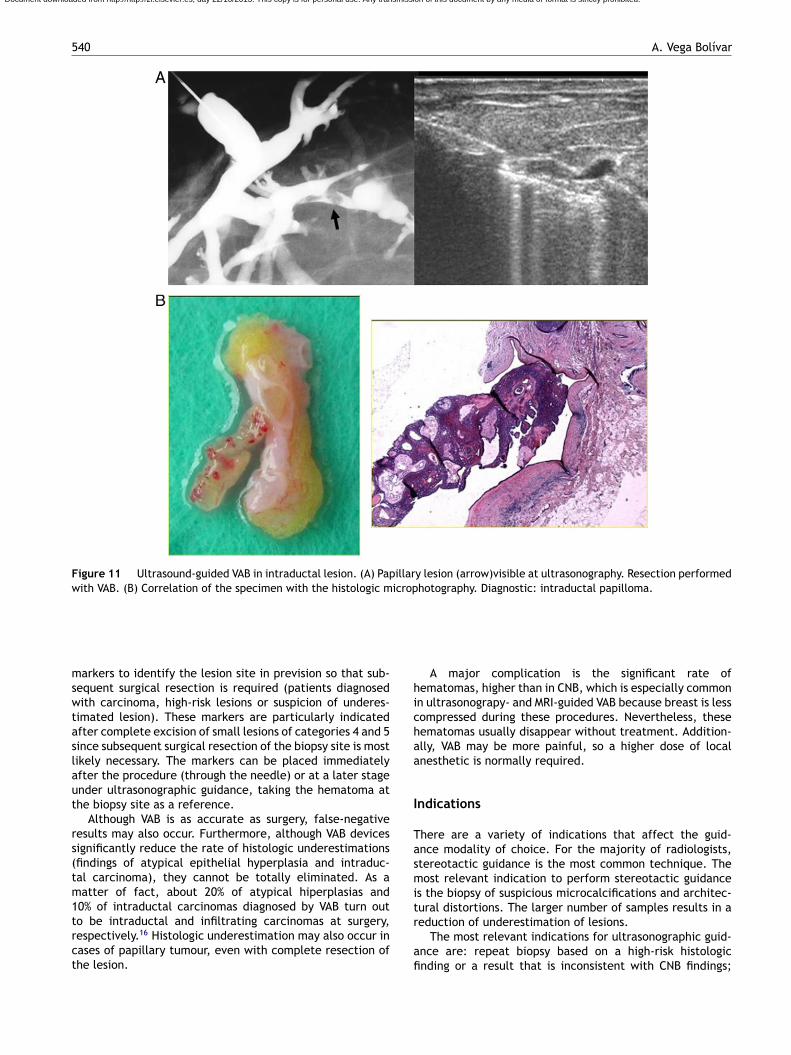
Figure 11 Ultrasound-guided VAB in intraductal lesion. (A) Papillary lesion (arrow)visible at ultrasonography. Resection performedwith VAB. (B) Correlation of the specimen with the histologic microphotography. Diagnostic: intraductal papilloma.
mswtaslaut
rs(tm1trct
hichaa
I
Tasmit
Document downloaded from http://http://zl.elsevier.es, day 22/10/2013. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
arkers to identify the lesion site in prevision so that sub-equent surgical resection is required (patients diagnosedith carcinoma, high-risk lesions or suspicion of underes-
imated lesion). These markers are particularly indicatedfter complete excision of small lesions of categories 4 and 5ince subsequent surgical resection of the biopsy site is mostikely necessary. The markers can be placed immediatelyfter the procedure (through the needle) or at a later stagender ultrasonographic guidance, taking the hematoma athe biopsy site as a reference.
Although VAB is as accurate as surgery, false-negativeesults may also occur. Furthermore, although VAB devicesignificantly reduce the rate of histologic underestimationsfindings of atypical epithelial hyperplasia and intraduc-al carcinoma), they cannot be totally eliminated. As aatter of fact, about 20% of atypical hiperplasias and
0% of intraductal carcinomas diagnosed by VAB turn out
o be intraductal and infiltrating carcinomas at surgery,espectively.16 Histologic underestimation may also occur inases of papillary tumour, even with complete resection ofhe lesion.r
afi
A major complication is the significant rate ofematomas, higher than in CNB, which is especially commonn ultrasonograpy- and MRI-guided VAB because breast is lessompressed during these procedures. Nevertheless, theseematomas usually disappear without treatment. Addition-lly, VAB may be more painful, so a higher dose of localnesthetic is normally required.
ndications
here are a variety of indications that affect the guid-nce modality of choice. For the majority of radiologists,tereotactic guidance is the most common technique. Theost relevant indication to perform stereotactic guidance
s the biopsy of suspicious microcalcifications and architec-ural distortions. The larger number of samples results in a
eduction of underestimation of lesions.The most relevant indications for ultrasonographic guid-nce are: repeat biopsy based on a high-risk histologicnding or a result that is inconsistent with CNB findings;
Diagnostic intervention in breast disease 541
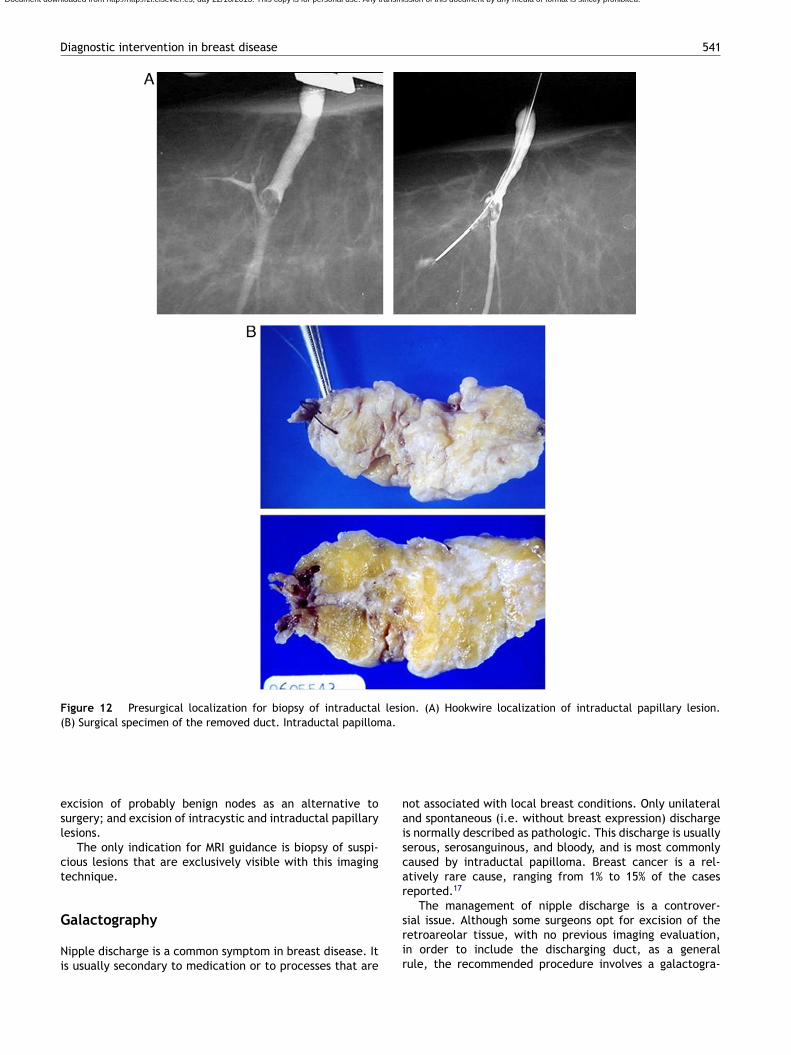
Figure 12 Presurgical localization for biopsy of intraductal lesion. (A) Hookwire localization of intraductal papillary lesion.(B) Surgical specimen of the removed duct. Intraductal papilloma.
naiscar
Document downloaded from http://http://zl.elsevier.es, day 22/10/2013. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
excision of probably benign nodes as an alternative tosurgery; and excision of intracystic and intraductal papillarylesions.
The only indication for MRI guidance is biopsy of suspi-cious lesions that are exclusively visible with this imagingtechnique.
Galactography
Nipple discharge is a common symptom in breast disease. Itis usually secondary to medication or to processes that are
srir
ot associated with local breast conditions. Only unilateralnd spontaneous (i.e. without breast expression) discharges normally described as pathologic. This discharge is usuallyerous, serosanguinous, and bloody, and is most commonlyaused by intraductal papilloma. Breast cancer is a rel-tively rare cause, ranging from 1% to 15% of the caseseported.17
The management of nipple discharge is a controver-
ial issue. Although some surgeons opt for excision of theetroareolar tissue, with no previous imaging evaluation,n order to include the discharging duct, as a generalule, the recommended procedure involves a galactogra-
5
pidd
T
Gstor
tidiAoS(a
ti
tut
m(aitrs
I
Gcl
os
C
T
A
TVi
R
1
1
1
1
1
1
1
Document downloaded from http://http://zl.elsevier.es, day 22/10/2013. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
42
hy before surgical decision-making since this techniques accurate in indicating absence or presence of an intra-uctal lesion and its localization within the abnormaluct.18
echnique and findings
alactography is commonly performed with the patient lyingupine. The breast is first tenderly expressed for identifica-ion of the discharging galactophorous duct and cannulationf the duct is then done with dedicated cannulas or sialog-aphy catheters.
Disinfecting the nipple and removing any air bubbles fromhe catheter are initial steps of the procedure. The catheters then introduced about 5 to 10 mm into the duct. A smallose of water-soluble iodinated contrast (0.5---1 ml) is nextnjected until the patient has a stinging feeling or pain.fter injecting the contrast, the catheter can be extractedr left in placed in case further injections are required.ubsequently, two orthogonal mammographic projectionscraniocaudal and mediolateral) are performed, and prefer-bly magnified.
Intraductal lesions manifest as filling defects or stop inhe contrast column (Fig. 10). The majority of lesions caus-ng discharge are benign, mostly papillomas.
Resection of the intraductual lesion identified at galac-ography can be performed by percutaneous VAB, generallynder ultrasonographic guidance,19 in institution where thisechnique is available (Fig. 11).
Localization of these lesions for surgical biopsy com-only relies on the coordinates provided by the galactogram
‘‘galacto-hook’’). Other techniques for localization of theffected duct involve injecting methylene blue or insert-ng metal guides (Fig. 12). Preoperative localization ofhe discharging duct is essential and failure to do so mayesult in missed identification of the lesion in the surgicalpecimen.20
ndications
alactography is indicated in cases of abnormal nipple dis-harge because it is commonly associated with intraductalesion, mostly papillomas.
Galactography is not indicated for bilateral or multi-rifice discharge because this type of discharge is notuggestive of breast disease, except for ductal ectasia.
onflict of interests
he authors declare not having any conflict of interests.
cknowledgments
he authors would like to thank Dr. Vicente Martinez deega and Dr. Mercedes Torres Tabanera for contributing themages in Figs. 9 and 11, respectively.
1
A. Vega Bolívar
eferences
1. Lee CH. Screening mammography: proven benefit, continuedcontroversy. Radiol Clin N Am. 2002;40:395---407.
2. Liberman L. Percutaneous image-guided core breast biopsy.Radiol Clin N Am. 2002;40:483---500.
3. Meyer JE, Smith DN, Lester SC, Kaelin C, DiPiro PJ, Denison CM,et al. Large-core needle biopsy of nonpalpable breast lesions.JAMA. 1999;281:1638---41.
4. Ruiz-Delgado MA, López-Ruiz JA, Sáiz-López A. Abnormalmammography and sonography associated with foreign-body giant-cell reaction after stereotactic vacuum-assistedbreast biopsy with carbon marking. Acta Radiol. 2008;49:1112---8.
5. Mariscal A, Balliu E, Solà M, Pérez de Tudela A, Fraile M,Julián JF. Comparación entre la inyección intratumoral y per-itumoral del radiotrazador para la localización y biopsia delganglio centinela en cáncer de mama no palpable. Radiologia.2008;50:309---16.
6. American College of Radiology. BI-RADS®. Sistema de informesy registro de datos de imagen de mama. Reston VA: ACR; 2003(Ed. esp.) Madrid: SERAM; 2006.
7. López Ruiz JA, Saralegui I, de Iturraspe CG, Echevarría JJ,Zabalza I, Alavarez J. Punción Aspirativa con Aguja Fina (PAAF)de lesiones no palpables: aspectos técnicos, indicaciones y valordiagnóstico (revisión de 1.000 casos). Rev Senologia Patol Mam.1997;10:161---73.
8. Tran PV, Lui PC, Yu AM, Vinh PT, Chau HH, Ma TK, et al.Atypia in fine needle aspirates of breast lesions. J Clin Pathol.2010;63:585---91.
9. Liberman L. Clinical management issues in percuta-neous core breast biopsy. Radiol Clin North Am. 2000;38:791---807.
0. Liberman L. Percutaneous imaging-guided core breast biopsy:state of the art at the millennium. AJR Am J Roentgenol.2000;174:1191---9.
1. Fitzal F, Sporn EP, Draxler W, Mittlböck M, Taucher S, Rudas M,et al. Preoperative core needle biopsy does not increase localrecurrence rate in breast cancer patients. Breast Cancer ResTreat. 2006;97:9---15.
2. Vega Bolivar A, Alonso Bartolomé P, Ortega García E, Gar-ijo F. Ultrasound-guided core needle biopsy of non-palpablebreast lesions: a prospective analysis in 204 cases. Acta Radiol.2005;46:690---5.
3. Youk JH, Kim EK, Kim MJ, Oh KK. Sonographically guided14-gauge core needle biopsy of breast masses: a review of2,420 cases with long-term follow-up. AJR Am J Roentgenol.2008;190:202---7.
4. Youk JH, Kim EK, Kim MJ. Atypical ductal hyperplasiadiagnosed at sonographically guided 14-gauge core nee-dle biopsy of breast mass. Am J Roentgenol. 2009;192:1135---41.
5. Alonso Bartolomé P, Vega Bolivar A, Torres Tabanera M, OrtegaGarcía E, Acebal Blanco M, Garijo Ayensa F, et al. Sono-graphically guided 11G directional vacuum-assisted breastbiopsy as an alternative to surgical excision: utility andcost study in probably benign lesions. Acta Radiol. 2004;45:390---6.
6. Apesteguía L, Mellado M, Sáenz J, Cordero JL, Repáraz B, deMiguel C. Vacuum-assisted breast biopsy on digital stereotaxictable of nonpalpable lesions non-recognisable by ultrasonogra-
phy. Eur Radiol. 2002;12:638---45.7. Richards T, Hunt A, Courtney S, Umeh H. Nipple discharge:a sign of breast cancer? Ann R Coll Surg Engl. 2007;89:124---6.

Document downloaded from http://http://zl.elsevier.es, day 22/10/2013. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Diagnostic intervention in breast disease
18. Slawson SH, Johnson BA. Ductography: how to and what If?Radiographics. 2001;21:133---50.
19. Torres-Tabanera M, Alonso-Bartolome P, Vega-Bolivar A,Sánchez-Gómez SM, Lag-Asturiano E, Sáinz-Miranda M, et al.Percutaneous microductectomy with a directional vacuum-assisted system guided by ultrasonography for the treatment
2
543
of breast discharge: experience in 63 cases. Acta Radiol.2008;49:271---6.
0. Vega Bolivar A, Landeras R, Ortega E. Intraductal placementof a Kopans spring-hookwire guide to localize nonpalpablebreast lesions detected by galactography. Acta Radiol. 1997;38:240---2.