detection of human papillomavirus type-16 dna utilising microtitre-plate based amplification...
TRANSCRIPT
ELSEVIER Journal of Virological Methods 58 (1996) 59-69
Journal of Virological Methods
Detection of human papillomavirus type- 16 DNA utilising microtitre-plate based amplification reactions and a solid-phase
enzyme-immunoassay detection system
Saban Cavuslua’b, William G. Starkey”, Jeremy N. Kaye”, Chandrima Biswa9, Christine Manta, Barbara Kell”, Philip Rice”, Jennifer M. Besta, John Casona,*
“The Richard Dimbleby Laboratory of Cancer Virology, Department of Virology, The Rayne Institute, United Medical and Dental Schools oj Guys and St Thomas’, St Thomas’ Hospital, Lambeth Palace Road, London SE1 7EH, UK
bThe Department of Irzfectious Diseases, Gulhane Military Medical Academy, Haydarpasa Teaching Hospital, 81327 Haydarpasa Istanbul, Turkey
Accepted 29 October 1995
Abstract
The development of a nested polymerase chain reaction (PCR) assay to detect low concentrations of human papillomavirus type-16 (HPV-16) DNA for epidemiological studies is described. The PCR utilises primers located in the E5 open reading frame, has an analytical sensitivity of 4 HPV-16 genomes and does not produce amplicons from other common genital HPVs (types-6, -11, -18, -31 and 33). This assay was carried out in 96-well plates utilising internal primers labelled with dinitrophenol (DNP) and biotin so that amplicons can be captured onto streptavidin- coated plates and detected using an alkaline phosphatase-labelled monoclonal antibody to DNP. The assay was effective for detecting HPV-16 DNA in plasmids, cell-lines and, both freshly collected or archival (formalin-fixed/ paraffin embedded) clinical specimens. This system is therefore suitable for epidemiological studies to identify individuals infected with HPV-16 DNA in episomal form who may be at increased risk of developing anogenital carcinomas.
Keywords: Human papillomavirus type 16; Nested PCR; Enzyme-immunoassay
1. Introduction -33, -35 and -54 are strongly associated with
More than 70 human papillomaviruses (HPV) have been identified, of which, about 30 exhibit tropism for the mucosa (de Villiers, 1992). Amongst these mucosal HPVs, types -16, -18, -31,
anogenital carcinomas and considered to be high cancer risk (zur Hausen, 1989, 1994; Syrjanen, 1989). HPV types -6 and -11 are commonly found in benign genital warts and are of low cancer risk, whilst infection with any of the remaining mu- cosal HPVs is believed to confer an intermediate
* Corresponding author. risk of cancer (de Villiers, 1992).
0166-0934/96/$15.00 0 1996 Elsevler Science B.V. All rights reserved SSDI 0166-0934(95)01988-X

60 S. Cavuslu et al. /Journal of Virological Methods 58 (1996,) 59-69
Cytological, histological and electron mi- croscopy studies can provide indirect evidence of HPV infection, but do not permit the identifica- tion of specific HPV types. Detection of particular HPVs relies currently upon the use of type-specific HPV probes in conjunction with methods such as in situ hybridization, dot-blotting, Southern blot- ting, filter in situ hybridization, the polymerase chain reaction (PCR) and, hybrid (DNA-RNA) capture (O’Banion et al., 1987; Caussy et al., 1988; Munoz et al., 1988; Manos et al., 1989; van den Brule et al., 1990). These techniques are labour intensive, often require specialised equip- ment and/or involve the use of radio-isotopes or toxic chemicals.
We are currently studying HPV-16 infections amongst infants delivered of HPV-16 DNA posi- tive women (Pakarian et al., 1994; Kaye et al., 1994; Cason et al., 1995). As in such cases viral DNA is presumably present in an episomal form and may often be present at low copy number, we required a sensitive assay for HPV-16. Ideal qual- ities for the assay were considered to be that it should be: (i) sensitive and specific for HPV-16 DNA; (ii) performed in a 96-well plate format, so that a high sample throughput could be achieved; (iii) based upon a colourimetric detection system, for use in diagnostic laboratories accustomed to enzyme-immunoassays (EIA) and automation; (iv) safe, i.e. utilise non-hazardous substances; (v) capable of detecting viral DNA in small quantities of clinical samples (and thus require use of smaller quantities of Thermophilus aquaticus DNA polymerase [Tag polymerase]); and (vi), able to detect viral DNA in both fresh and archival material.
We compared sensitivities and specificities of three HPV-16 PCRs which used primers based upon the E5, E6 or E7 open reading frames (ORFs). The most sensitive of these PCRs (using E5 primers) was developed into a nested assay, to increase specificity, and reduced to a 96-well for- mat for amplification and EIA detection stages. Performance of PCR-EIA was evaluated by com- paring results obtained by this method with those produced by the PCR for E7 DNA using samples from patients likely to be infected with HPV-16 (biopsies from cervical carcinomas and cervical
swabs of cervical intraepithelial neoplasia lesions
(GIN)).
2. Materials and methods
2.1. Biological samples
Ten-pm sections were cut (using disposable blades for each section) from archival samples (formalin-fixed paraffin-embedded blocks) of 9 cervical carcinomas and 10 lymph node metas- tases (provided by Dr J. Goodlad, Department of Histopathology, St Thomas’ Hospital, London, U.K.). Sections (one per sample) were dewaxed by extracting twice with octane followed by two ethanol washes (Wright and Manos, 1990). Eigh- teen cervical scrapes from women with CIN I/II attending clinics at St. Thomas’ Hospital were collected (by C.B.) and 32 buccal swabs were collected from children (by P.R.) and a selected population of known HPV-16 positive and nega- tive samples used. Permission for collection of these samples was provided by the Research Ethics Committee of St Thomas’ Hospital. Five biopsy samples from patients with anogenital and laryngeal warts were also studied. Cell-lines A431, CaSki, HeLa and SiHa were purchased from the American Type Culture Collection (Rockville MA, USA), XH-1 was provided by collaborators (Han et al., 1991). A plasmid containing HPV-16 DNA cloned at the BamHl site (pAt-HPV-16) was provided by Dr E-M. de Villiers (Deutsches Krebsforschungszentrum, Heidelberg, Germany). Freshly collected, or dewaxed (Wright and Manos, 1990), cells were pelleted by centrifuga- tion and digested with proteinase K (Kaye et al., 1994) in a final volume of 200 ~1, 10 ~1 of which was made up to 100 ,ul with PCR reaction mix.
2.2. Polymerase chain reactions (PCR)
Primers based on HPV-16 E5 (Straight et al., 1993), E6 and E7 ORFs and MY09/11 primers (Manos et al., 1989) were purchased (Table 1). PCR reactions were performed in 0.5 ml Eppen- dorf tubes or in 96-well plates with covers (Hy- baid Ltd., UK) in a thermal cycler (Omnigene:
S. Cavuslu et al. /Journal of Virological Methods 58 (1996) 59-69 61
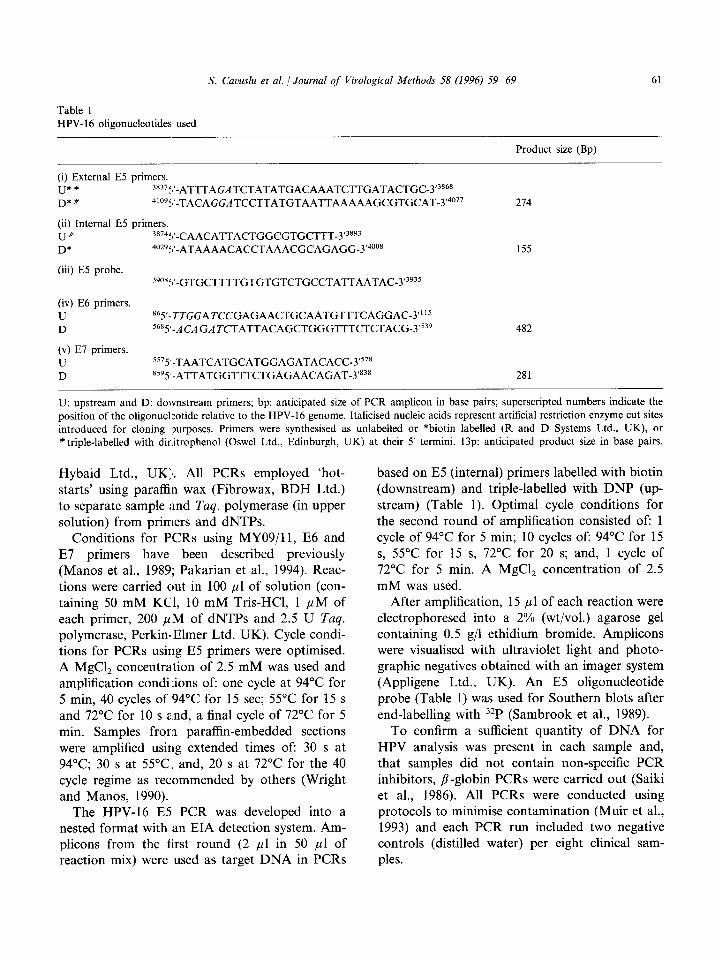
Table 1
HPV- 16 oligonucleotides used
Product size (Bp)
(i) External E5 primers.
U*# 38375’-ATTTAGATCTATATGACAAATCTTGATACTGC-3’3868
D*# 4’095’-TACAGGATCCTTATGTAATTAAAAAGCGTGCAT-3’4077
(ii) Internal E5 primers.
U” 38745’-CAACATTACTGGCGTGCTTT-3’3893
D* 4029f,‘-ATAAAACACCTAAACGCAGAGG-3’4008
(iii) E5 probe.
39”85’-GTGCTTTTGTGTGTCTGCCTATTAATAC-3’3935
214
155
(iv) E6 primers.
U 865’-TTGGATCCGAGAACTGCAATGTTTCAGGAC-3”’s
D 5685’-ACAGATCTATTACAGCTGGGTTTCTCTACG-3’539 482
(v) E7 primers.
U 5575’-TAATCATGCATGGAGATACACC-3’578
D 8595’-ATTATGGTTTCTGAGAACAGAT-3’838 281
U: upstream and D: downstream primers; bp: anticipated size of PCR amplicon in base pairs; superscripted numbers indicate the
position of the oligonucleotide relative to the HPV-16 genome. Italicised nucleic acids represent artificial restriction enzyme cut sites
introduced for cloning purposes. Primers were synthesised as unlabelled or *biotin labelled (R and D Systems Ltd., UK), or
# triple-labelled with dinitrophenol (Oswel Ltd., Edinburgh, UK) at their 5’ termini. 13~: anticipated product size in base pairs.
Hybaid Ltd., UK). All PCRs employed ‘hot- starts’ using paraffin wax (Fibrowax, BDH Ltd.) to separate sample and Taq. polymerase (in upper solution) from primers and dNTPs.
Conditions for PCRs using MY09/11, E6 and E7 primers have been described previously (Manos et al., 1989; Pakarian et al., 1994). Reac- tions were carried out in 100 ~1 of solution (con- taining 50 mM KCl, 10 mM Tris-HCl, 1 PM of each primer, 200 ,uM of dNTPs and 2.5 U Tuq.
polymerase, PerkinElmer Ltd. UK). Cycle condi- tions for PCRs using E5 primers were optimised. A MgCl, concentration of 2.5 mM was used and amplification conditions of: one cycle at 94°C for 5 min, 40 cycles of 94°C for 15 set; 55°C for 15 s and 72°C for 10 s and, a final cycle of 72°C for 5 min. Samples from paraffin-embedded sections were amplified using extended times of: 30 s at 94’C; 30 s at 55°C; and, 20 s at 72°C for the 40 cycle regime as recommended by others (Wright and Manos, 1990).
The HPV-16 E5 PCR was developed into a nested format with an EIA detection system. Am- plicons from the first round (2 ~1 in 50 ~1 of reaction mix) were used as target DNA in PCRs
based on E5 (internal) primers labelled with biotin (downstream) and triple-labelled with DNP (up- stream) (Table 1). Optimal cycle conditions for the second round of amplification consisted of: 1 cycle of 94°C for 5 min; 10 cycles of: 94°C for 15 s, 55°C for 15 s, 72°C for 20 s; and, 1 cycle of 72°C for 5 min. A MgCl, concentration of 2.5 mM was used.
After amplification, 15 ~1 of each reaction were electrophoresed into a 2% (wt/vol.) agarose gel containing 0.5 g/l ethidium bromide. Amplicons were visualised with ultraviolet light and photo- graphic negatives obtained with an imager system (Appligene Ltd., UK). An E5 oligonucleotide probe (Table 1) was used for Southern blots after end-labelling with 32P (Sambrook et al., 1989).
To confirm a sufficient quantity of DNA for HPV analysis was present in each sample and, that samples did not contain non-specific PCR inhibitors, P-globin PCRs were carried out (Saiki et al., 1986). All PCRs were conducted using protocols to minimise contamination (Muir et al., 1993) and each PCR run included two negative controls (distilled water) per eight clinical sam- ples.

62 S. Cavuslu et al. /Journal of Virological Methods 58 (1996) 59-69
2.3. Enzyme immunoassays (EIAs) to detect labelled amplicons
Three methods were investigated: (1) Capture of biotin/DNP labelled amplicons
onto 96-well plates coated with rat mono- clonal antibody (mAb) to DNP (Zymed Ltd., CA., USA) and detection with streptavidin-al- kaline-phosphatase (AP) conjugate (Sigma Ltd. U.K.).
(2) Capture of amplicons onto streptavidin- coated plates and detection with mAb to DNP conjugated via gluteraldehyde (Harlow and Lane, 1988) to horseradish-peroxidase (HRP: Sigma Ltd. U.K.).
(3) Capture of amplicons onto streptavidin- coated plates and detection with mAb to DNP labelled with AP (conjugated via gluter- aldehyde).
Coating of plates with streptavidin (3), rather than with antibodies to DNP (l), produced highest absorbance values and low background readings: high background absorbance values were also obtained when the HRP-mAb conju- gate (2) was used (data not shown). Hence, the last of these procedures (3) was selected for fur- ther development.
EIAs using streptavidin-coated plates and AP- labelled anti-DNP mAb were optimised using amplified pAt-HPV- 16 DNA (Results Section 3.2). 96-well plates (Maxisorp F96, Nunc Ltd. Denmark) were coated with 100 PI/well of 0.05 M carbonate/bicarbonate buffer (pH 9.6: Sigma Ltd., U.K.) containing 10 mg/l affinity-purified streptavidin (Sigma Ltd. U.K.) for 2 h at 37°C. Wells were washed 4 times with Dulbecco’s phosphate buffered saline (PBS) containing 0.05% (v/v) Tween-20 (PBS-Tween: BDH Ltd., U.K.) in a plate washer (MRW, Dynatech Ltd., U.K.) and wells were blocked with 200 ~1 of PBS-Tween containing 1% (w/v) bovine serum albumin (Sigma Ltd., U.K.) for 2 h at 37°C. Wells were washed 4 times with PBS-Tween and then either used immediately or stored at - 20°C.
Five ,ul of PCR product were added to dupli- cate wells of EIA plates which each contained
95 pi/well of PBS for 30 min at 37°C. Wells were washed 4 times with PBS-Tween and 50 PI/well of AP-labelled mAb were added for 30 min at 37°C. Plates were washed 4 times with PBS-Tween and rinsed twice with glycine buffer (aqueous 0.1 M glycine, 1 mM MgCl,, 1 mM ZnCl,, pH 10.4).
200 PI/well of substrate (1 g p-nitrophenyl phosphate/l glycine buffer: Sigma Ltd., U.K.) were added for 30 min and absorbances of wells at 405 nm (A,,,) were determined after the ma- chine (Labsystems Multiskan Multisoft, U.K.) had been zeroed against wells containing sub- strate. Negative controls for EIA were wells which contained PCR product plus substrate (but no mAb), mAb plus substrate (but no PCR product) and, reactions which contained primers (but no target DNA).
2.4. Statistical methods
Students t-tests were used to assist interpreta- tion of EIA data.
3. Results
3.1. Comparison of HPV-16 E-5, Ed and E7 primer based PCRs
HPV-16 PCRs (E5, E6 and E7 primers) pro- duced amplicons of the anticipated size from cell-lines containing HPV 16 (SiHa, CaSki and XH-1: Table 2). HPV-16 PCRs did not amplify DNA from clinical samples containing HPV-6, -11, -31, -33 or, from HPV-16 negative cell-lines HeLa (HPV-18) and A43 1 cells. MY09/11 based PCRs produced amplicons from all HPV-con- taining clinical samples (Table 2). PCRs using E5 or E7 primers allowed detection of 8 copies of HPV-16 DNA using an end point determined by visualisation in agarose gels: dilutions of pAt-HPV-16 produced comparable results (data not shown). Since it was planned to use EIA detection, a stage to ensure specificity of product was necessary and a nested ES-PCR was developed. This had a slightly greater sensi- tivity than the original E5 PCR (4 versus 8 HPV-16 copies, Fig. 1).

S. Cavuslu et al. /Journal of Virological Methods 58 (1996) 59-69 63
Table 2 Specificity and sensitivity of HPV-16 PCRs
Sample B-G ES # E6 El MY911 1 Present*
CaSki SiHa XH-1 HeLa A431 pAt-16 AL CM AB BL IW Sensitivity**
+ + + + + 16 + + + + + 16 + + + + i- 16 + - _ + 18 + - _ - _ - + + + + 16 + _ - - + 6 + _ - - + 6 + - _ - + 31 + - _ - + 33 + - - - + 11
8 16 8 32
+, amplicon of predicmd size detected or - , not detected in PCRs using HPV-16 E5 (external), E6 and El primer sets. Samples tested included cell lines (CaSki, SiHa, XH-1, HeLa and A431), genomic HPV-16 (pAt-16), and clinical samples derived from 5 patients (AL, CM, AB, BL and IW) whose HPV status had been determined using primer sets described previously (van den Brule et al., 1990)*. B-G, beta-globin PCR; E5 #, PCR using HPV-16 E5 (external) primers; **, sensitivity HPV-16 in genome copy numbers determined using SiHa cells (which contain 1 copy of HPV-16 DNA/cell: Yee et al., 1985)
3.2. Development ojc the enzyme immunoassay
(EIA)
3.2.1. Concentration of streptavidin for coating EIA plates
10 mg streptavidin/l for 2 h at 37°C produced greatest A,,, values (Fig. 2A) and incubation temperature had little effect upon streptavidin binding (Fig. 2B). Extending streptavidin coating time to 12 h at 4”‘C had no marked effect upon Aao5 values (Fig. 2.B: 4 C*). Streptavidin coated plates were stable for 1 month when stored at - 20°C.
3.2.2. Monoclonal antibody For each batch of AP-labelled mAb prepared,
standard curves were prepared to ensure the con- centration of mAb used in the detection stage was not limiting, typically, mAb concentrations within the range l-5 mg/l were used (e.g. Fig. 2C).
3.2.3. PCR produci’ concentration and colour development
5 ~1 of nested PCR product were added to 95 ,~l of PBS in assay plates. Increase in volume of amplicon solution ‘was necessary to ensure a max- imum area of streptavidin-coated EIA wells was
exposed. Tests using 50, 20, 10, 5 and 1 ~1 of PCR product from pAt-HPV-16 (in 100 ~1) revealed that only the use of 1 ,~l of PCR product resulted in a significant decrease in A,,, nm values (data not shown). Incubation time for samples with substrate was taken to be 30 min at 37°C since no advantage was noted in prolonging this (Fig. 2D). Aaos values obtained from PCR-EIAs indicated that this system had an equivalent sensitivity to the nested E5 PCR when amplicons were visu- alised in agarose gels and a high Ados value (0.59) was detected for 4 genome copies of HPV-16 (Fig. 1). Differentiation between positive and negative samples in PCR-EIA was usually possible on visual inspection of EIA plates (e.g. Fig. 3).
3.3. EIA Assay variation
Variation was assessed using 8 paraffin-embed- ded samples from patients with cervical cancer. Coefficients of variation (CV%) for within-assay variation of EIA did not exceed lOoh for HPV-16 agarose gel positive samples (n = 5, mean 7.8%, range 4.9-9.3%), whereas CV%s for gel negative samples were higher (n = 3, mean 16.7%, range 11.X-24.8%). Gel positive samples had signifi- cantly greater A,,, values than gel negative sam-

64 S. Cavuslu et al. /Journal of Virological Methods 58 (1996) 59-69
000 500
250 125
62.5
32 16 a 4
2 +
2.71
2.58
2.67 2.36
2.01
2.08 1.69 1.73
0.59 0.05
Fig. 1. Comparison of E5 (external) PCR, E5 (nested) PCR and Southern blots with PCR-EIA for the detection HPV-16 DNA. A: negative image of an ethidium bromide stained agarose gel containing E5 PCR products at a molecular weight of 274 bp. B: Southern blot corresponding to A. C: agarose gel of products from nested E5 PCR (molecular weight 155 bp). D: Southern blot of the same samples as C. On the right hand side EIA results as A,,, values are indicated. In all cases, samples were electrophoresed from right to left. Gels were loaded with 15 ~1 of product/well, nested E5 PCRs were produced from a l/25 dilution of the first round PCR and, in EIAs, only 5 ~1 of nested E5 PCR product was used.
ples (P < 0.01). Gel positive samples had A,,, values which exceeded the mean plus 3 SD of controls (Ado5 = 0.056) whilst all gel negative samples had values below this. A cut-off value of the mean Aa5 value for negative control wells plus 3 SD was therefore taken to define EIA positivity. Inter-assay variation for the EIA was low (mean CV% for gel positive samples was 10.9%, range 2.1- 19.5%). The difference in mean A 405 values between gel positive and negative samples was significant (P < 0.01).
3.4. Evaluation of the PCR-EIA for screening clinical samples
PCR-EIA was compared to PCRs which uti- lized E7, E5 and E5 (nested) primers, for the analyses of 19 archival samples. Nine samples (numbers 41, 49, 54, 59, 60, 61, 65, 66 and 68) were EIA positive (range of Aaos values: 0.8- 2.055) and ten negative (Ado5 range: 0.002-0.125: Table 3). Overall, 6 of 9 (66.6%) cervical car- cinomas and 3 of 10 (30%) lymph-node metas- tases were HPV-16 DNA positive by PCR-EIA.
Duplicate variation was low (e.g. for 9 PCR-EIA positive samples, mean + SD: 2.37% f 1.87%) with the greatest variation being 5.7%.
Fourteen of 19 (73.6%) samples produced con- sistent results in all assays and 2 samples (10.5%: 66 and 68) were positive in only the nested E5 PCR and PCR-EIA (Table 3). Six of 19 (31.5%: 41, 49, 54, 60, 61 and 65) samples were positive in all PCRs and PCR-EIA and, 8 of 19 (42.1%: 39, 42, 50, 53, 55, 63, 71 and 73) were negative in all assays. One sample (6.4%: number 59) was posi- tive in all three E5 based assays. Two samples (10.5%: 72 and 67), both from the same patient (case 18), were positive in just the E7 PCR. All samples were sufhcient for analysis since /?-globin amplicons were obtained (Table 3).
These data are representative of other experi- ments using non-fixed tissues such as cervical scrapes (which had been stored at -20°C). In- deed, for 18 samples from women with CIN I/II, 11 (61.1%) were positive in E5 PCR, nested PCR and PCR-EIA. Six of 18 (33.3%) were positive in just the latter two assays and 1 (5.5%) was nega- tive in all tests (data not shown). Similarly, when

A
1.5 IOSn se 2.5 qn
1 1-M
0.S
0 200 ‘loo 20 10 5
C
5
2.5
2
S. Cavuslu et al. /Journal of Virological Methods 58 (1996) 59-69
B
2 4C' 2OC
1.5 37c 4c
1
a5
0 200 100 20 10 5
D
25 60 min
3 30 mln
2,s
.2
1.5 2om*
1 0.6 lOlni!l
snin 0 -200 100 20 10 5
Reciprocal dilution of amplicons
Fig. 2. Optimisation of the EIA. A: Effect of differing streptavidin coating concentrations (coated for 2 h at 37°C) upon the detection of dilutions of HPV-16 amplicons. B: Effect of streptavidin (at 10 mg/l for 2 h at 37°C; or overnight at 4°C [4 C*]) coating temperature upon the ability to detect HPV-16 amplicons. C: Example of the selection of an appropriate antibody concentration to detect HPV-16 amplicons (plates coated with 10 mg/l streptavidin for 2 h at 37°C). D: Variation of substrate development time upon the ability to detect HPV-16 positive amplicons (plates coated with 10 mg/l streptavidin for 2 h at 37°C.
these assays were used to investigate HPV-16 DNA in buccal swabs from a selected population of children who h(ad previously been tested for HPV-16 DNA by PCR, 12 of 32 (37.5%) were positive by E5 PCR, nested PCR and PCR-EIA.
4. Discussion
A DNA amplification method is described for the detection of HPV-16 E5 DNA which can be performed in 96-well plates and utilises an im- muno-enzyme detection system. The assay has an analytical sensitivity of 4 HPV-16 genomes and did not produce amplicons from samples which contained DNA from 5 of the most common other genital HPVs (types -6, -11, -18, -31 and 33). It is unlikely that E5 nested PCR or PCR-EIA detects HPV-35 DNA, which is phylogenetically
most similar to HPV-16. Since, there is only a 61% nucleic acid homology between the amplified segment of HPV-16 and the equivalent region of HPV-35 DNA and, the four HPV-16 E5 primers used have low homologies (40, 45, 45 and 75%) with HPV-35.
The assay is rapid since results can be obtained in as little as 9 h from sample preparation when precoated plates are used. Furthermore, com- pared to other agents used to detect PCR prod- ucts (e.g. ethidium bromide and radioisotopes) p-nitrophenyl phosphate is non-hazardous and, positive EIA results can be discerned by visual inspection. Sensitivities of the E5 PCR and the nested PCR were not compromised by performing amplifications in 96-well plates using either 100 ~1 or 50 ,uI reaction volumes.
Since all products of the nested PCR will bear a DNP and a biotin label and produce positive

66
A
B
C
D
E
F
G
H
S. Cavuslu et al. /Journal of Virological Methods 58 (1996) 59-69
Fig. 3. Example of PCR-EIA results: Results (as duplicates) Al/BI, A2/B2 and C7/D7 are negative controls (distilled water added as ‘template’ in first round PCR); G9/H9 and GlO/HlO are positive controls (pAt-HPV-16 DNA in PCRs). Gl l/H1 1: AP-mAb plus substrate but no PCR product; G12/H12: substrate alone. E12/F12: positive controls but no AP-mAb. Samples A4/B4, A5/B5, A6/B6, AlO/BlO, A12/Bl2, Cl/Dl, C2/D2, C3/D3, C4/D4, E2/F2, E4/F4, E5/F5, E6/F6, E9/F9, ElO/FlO, El l/F1 1, G4/H4, G5/H5 and G7/H7 were scored positive both by visual inspection and A4a5 values; All/B11 was scored a weak positive by eye, but on absorbance values was not considered positive.
signals in EIAs, it is a fundamental prerequisite that primer-dimers do not occur. Initial studies using just the labelled E5 (external) primers indi- cated that dimers occurred intermittently. This problems was eliminated by the use of nested PCR based on the use of unlabelled external primers and labelled internal primers.
Others have developed solid-phase colourimet- ric/immuno-enzyme based detection systems for the nucleic acids of human immunodeficiency virus (Mallet et al., 1993), plant viruses (Hataya et al., 1994), Chlamydia trachomatis (Bobo et al., 1990), varicella zoster virus (Inouye and Hondo, 1990), hepatitis B virus (Mantero et al., 1991) hepatitis C virus (Whitby and Garson, 1995) and also human papillomaviruses (Baccard-Longere et al., 1994). Most of these methods include either a hybridization step (DNA/DNA or DNA/RNA) or, like the present report, nested PCRs to ensure specificity of amplification.
In assays based upon the same principle as that described here, another group has detected
HPV-16 E6 DNA (Sauvaigo et al. (1990); Bac- card-Longere et al. (1994)). However, our PCR- EIA method incorporates several significant improvements. First, we determined the most sensitive of three HPV-16 primer pairs for use in PCR and compared these assays with a well es- tablished PCR (based on HPV consensus primers MY09/11). Secondly, the nested primer used in the present report was labelled with three - rather than one - DNP moeity, and thus contains more antibody binding sites. Thirdly, we used a mAb that had been conju- gated to AP, rather than to HRP, since our initial results indicated that use of HRP pro- duced high background readings. Fourthly, PCR amplifications and EIA detections were per- formed in microwell plates rather than tubes, which permit rapid dispensing of reagents with multichannel pipetting equipment and the possi- bility of using automation using robotic arms, as has recently been described (Terry et al., 1994). Finally, whereas Baccard-Longere et al. (1994)

S. Cavuslu et al. /Journal of Virological Methods 58 (1996) 59-69 61
Table 3 HPV-16 DNA detection in clinical samples using PCR-EIA and PCRs using E7 or E5 (external) and E5 (nested) primers
Case # Source Sample # Agarose gel results PCR-EIA
/3-G E7 E5s E5 nest A 405
16 C 39 + _ _ _ _ 0.009 16 LN 66 + _ _ + + 0.801 17 LN 68 + _ _ + + 0.817 18 C 72 + + - _ _ 0.043 18 LN 67 + + _ _ - 0.023 19 C 65 + + + + + 2.107 20 C 63 + _ _ - - 0.125 20 LN 71 + _ _ - - 0.062 21 LN 55 + _ - - _ 0.010 22 C 59 + _ + weak + + 1.238 22 LN 73 + _ _ - _ 0.022 25 C 41 + + + + + 2.055 25 LN 42 + _ - - _ 0.038 25 LN 50 + - - _ _ 0.032 26 LN 54 + + + + + 1.955 27 C 49 + + + + + 1.905 29 C 60 + + + + + 0.875 29 LN 53 + _ _ _ _ 0.029 30 C 61 + + + + + 1.396 Water (n = 16) _ _ _ _ - 0.023 (0.016) Controls (n = 16) _ _ - _ _ 0.054 (0.042) Cutoff: 0.180
Samples derived from paraffin-embedded sections of lymph node (LN) or cervical carcinoma (C); 8-G: beta-globin PCR; E5s: using external primers; E5 nest: nested E5 PCR; A,, values are mean of duplicate readings (see text for details of duplicate variation). EIA: nested E5 PCR-EIA. Data for water and control wells (containing all reagents except target DNA) in the PCR-EIA are expressed as mean values and in parentheses, the standard deviation (SD); the cut off A,, value was calculated as the mean +3 SD.
simultaneously added labelled amplicons and an- tibody to streptavidin coated tubes, we used se- quential stages to permit maximal binding of labelled amplicons and then antibody.
It was anticipateld that it would be possible to use the PCR-EIA to estimate the quantity of DNA present in the original sample, for example by including a series of internal positive controls (containing a known quantity of HPV-16 genomes) processed concordantly with test sam- ples. However, using optimised protocols, no lin- ear dose-response relationship was observed. It is our opinion that in order to obtain a quantitative assay, amplifications would have to be performed at a sub-optimal cycle number (i.e. to be within the linear region Iof the cycle number/amplicon quantity relationship: Kaye et al., 1994), this
would have inevitably resulted in loss of sensitiv- ity.
Use of 96-well plates for the amplification stages increases the possibility of cross-contami- nation between samples. However, when paraffin wax, plate lids, duplicate samples and careful technique were used, contamination was rarely detected. Nevertheless, it may be prudent to em- ploy re-amplification and Southern blotting as a confirmatory assay for positive samples.
We were primarily interested in producing a sensitive assay to investigate samples from infants born to HPV-16 DNA positive mothers. How- ever, since in such cases the amount of viral DNA may be extremely low, we validated the PCR-EIA using clinical samples from a small population who were likely to be infected with HPV-16

68 S. Cavuslu et al. /Journal of Virologlcal Methods 58 (1996) 59-69
DNA, namely patients with cervical carcinomas and lymph node metastases. When PCR-EIAs were used to investigate these samples there was a high concordance (73.6%) between results ob- tained with E7, E5 and ES-nested PCRs and the PCR-EIA. Two samples were only positive by the nested E5 PCR and by PCR-EIA and this proba- bly reflects the greater sensitivities of these assays.
However, the results for two samples, both from the same patient with cervical carcinoma revealed a potential limitation of E5 primer based PCRs and PCR-EIAs in terms of the diagnostic sensitivity of the assay. These samples were posi- tive in PCRs which used HPV-16 E7 primers, but negative in assays which utilized E5 primers. These data are most readily explained by distur- bance of the E5 ORF in this patient. Whilst E5 is intact and transcribed in low grade cervical in- traepithelial neoplasias (Stoler et al., 1992) in some cervical cancer cell-lines HPV-DNA is inte- grated into host DNA with loss of the E5 ORF (Schwartz et al., 1985; Baker et al., 1987). How- ever, the frequency of HPV-16 E5 loss amongst patients with cervical cancers is as yet undeter- mined.
Consequently, ES-based assays may be of lim- ited value for the detection of HPV-16 DNA in some carcinomas. Despite this caveat, PCR-EIA is useful for detecting HPV-16 DNA, which oc- curs in subclinical infections and in low grade CIN (in both cases integration of viral DNA is believed not to occur) and may be particularly useful as: (i) an adjunct to cervical smear testing (in combination with assays for other high risk HPVs) and (ii), an epidemiological tool for studies of populations amongst whom HPV-16 DNA is present at low copy number.
Acknowledgements
We wish to thank the Special Trustees of St Thomas’ Hospital, The Richard Dimbleby Cancer Fund and the Wellcome Trust for financial assis- tance. Dr Cavuslu is grateful for the award of a training Fellowship from the Turkish Navy and for the continued advice and support of Dr O.S. Yenen (Department of Infectious Diseases, Gul-
hane Military Medical Academy, Haydarpasa Teaching Hospital, Istanbul, Turkey).
References
Baccard-Longere, M., Alpha-Bazin, B., Chypre, C., Sauvaigo, S., Teoule, R., Bernard, P. and Seigneurin, J.M. (1994) Fast solid support detection of human papillomavirus in in vitro amplified DNA using a DNP-anti-DNP monoclonal antibody couple. J. Virol. Methods 46, 29-38.
Baker, C.L., Phelps, W.C., Lindgren, V. et al. (1987) Struc- tural and transcriptional analysis of human papillomavirus type 16 sequences in cervicalk carcinoma cell lines. J. Virol. 61, 926-971.
Bobo, L., Coutlee, F., Yolken, R.H., Quinn, T. and Visctdt, R.P. (1990) Diagnosis of Chlamydia trachomatis cervical infection by detection of amplified DNA with an enzyme immunoassay. J. Clin. Microbial. 28, 1968-1973.
Cason, J., Kaye, J.N., Jewers, R.J., Kambo, P.K., Bible, J.M., Kell, B., Shergill, B., Pakarian, F., Raju, K.S. and Best, J.M. (1995) Perinatal infection by, and persistence of, human papillomavirus types 16 and 18 in infants. J. Med. Virol. 47, 209-218.
Caussy, D., Orr, W., Dean Daya, A., Roth, P., Reeves, W. and Rawls, W. (1988) Evaluation of methods for detecting human papillomavirus deoxyribonucleic sequences in clini- cal specimens. J. Clin. Microbial. 26, 2366243.
de Villiers, E.-M. (1992) Laboratory techniques in the investi- gation of human papillomavirus infection. Genitourin. Med. 68, 50-54
Han, X., Lyle, R., Eustace, D.L.S., Jewers, R.J., Parrington, J.M., Das, A., Chana, T., Money, S., Dagg, B., Bates, T.D., Kenney, A. and Heyderman, E. (1991) XH-1: a new cervical carcinoma cell line and xenograft model for tu- mour invasion, ‘metastasis’ and regression. Br. J. Cancer 64, 645-654.
Harlow, E. and Lane, D. (1988) Antibodies: A laboratory manual. Cold Spring Harbor Laboratory Press, Cold Spring Harbor, NY. 1988, pp. 349
Hataya, T., Inoue, A.K. and Shikata, E. (1994) A PCR microplate hybridization method for plant virus detection. J. Virol. Methods 46, 223-236.
Inouye, S. and Hondo, R. (1990) Microplate hybridization of amplified viral DNA segment. J. Clin. Microbial. 26, 1469- 1472.
Kaye, J.N., Cason, J., Pakarian, F.B., Jewers, R.J., Kell, B., Bible, J.M., Raju, K.S. and Best, J.M. (1994) Viral load as a determinant for transmission of human papillomavirus type 16 from mother to child. J. Med. Virol. 44, 4155421.
Mallet, F., Hebrard, C., Brand, D., Chapuis, E., Cros, P., Allibert, P., Besnier, J.M., Barin, F. and Mandrand, B. (1993) Enzyme-linked oligosorbent assay for detection of polymerase chain reaction amplified human immunodefi- ciency virus type 1. J. Clin. Microbial. 31, 14441449.

S. Cavuslu et al. /Journal of Virological Methods 58 (1996) 59-69 69
Manos, M., Ting, Y., Wright, D.K., Lewis, A.J., Broker, T.R. and Wolinsky S.M. (1989) Use of polymerase chain reac- tion amplification far the detection of genital human papil- lomaviruses. Cancer Cells 7, 209-214.
Mantero, G., Zonaro, A., Albertini, A., Bertolo, P. and Primi, D. (1991) DNA enzyme immunoassay: General method for detecting products of poiymerase chain reaction. Clin. Chem. 37, 4222429
Muir, P., Nicholson, F., Jhetam., N., Neogt, S. and Banatvala, J.E. (1993) Rapid (diagnosis of enterovirus infections by magnetic bead extmction and polymerase chain reaction detection of enterovirus RNA m clinical specimens. J. Clin. Microbial. 31, 31-?8
Munoz, N., Bosch, X. and Kaldor, J.M. (1988) Does human papillomavirus caus’e cervical cancer? The state of epidemi- ological evidence. Br. J. Cancer 57, 1-5.
O’Banion, M.K., Sunclberg, J.M., Rezka, A.A. and Reich- mann, M.E. (1987) Cross-hybridization and relationships of various papillomavirus DNAs at different degrees of stringency. Intervirology 28, 114- 121.
Pakarian, F.B., Kaye .J.M. Cason, J., Kell, B., Jewers R.J., Raju, K.S. and Best J.M. (1994) Cancer associated human papillomaviruses: perinatal transmission and persistence. Br. J. Obstet. Gynaecol. 101, 5144517
Sambrook, J., Fritsch, E.F. and Maniatis, T. (1989) Molecular cloning: a laboratory manual. Cold Spring Harbour Labo- ratory Press, Cold !$pring Harbour, NY, pp. 10.59-10.60.
Sauvaigo, S., Fouque, B., Roget, A., Livache, T., Bazin, H., Chypre, C. and Teoule, R. (1990) Fast solid support detection of PCR amplified viral DNA sequences using radioiodinated or hapten labelled primers. Nut. Acids Res. 18, 317553183.
Saikr, R.A., Bugawan, T.L., Horn, C.I.T., Mullis, K.B. and Erlich, H.A. (1986) Analysis of enzymatically amplified B-globin and HLA DQ alpha DNA with allele specific oligonucleotide pro oes. Nature 324, 163- 166
Schwartz, E., Freese, IJ.K., Gissmann, L. et al. (1985) Struc- ture and transcription of human papillomaviruse sequences in cancer cells. Nature 3 14, Ill - 114.
Straight, S.W., Hinkle, P.M., Jewers, R.J. and McCance D.J. (1993) The E5 oncoprotein of human papillomavirus type 16 transforms fibroblasts and effects the downregulation of the epidermal growth factor receptor in keratinocytes. J. Virol. 67, 4521-4532.
Staler, M.H., Rhodes, C.R., Whitbeck, A., Wolinsky, S.M., Chow, L.T. and Broker, T.R. (1992) Human papillo- mavirus type 16 and 18 gene expression in cervical neo- plasias. Human Pathol. 23, 117-127.
Syrjanen, K.L.J. (1989) Epidemiology of human papillo- mavirus infections and their associations with genital squamous cell cancer. APMIS 97, 957-970
Terry, G., Ho, L., Szarewski, A. and Cuzick, J. (1994) Semiau- tomated detection of human papillomavirus DNA of high and low oncvogenic potential in cervical smears. Clin. Chem. 40, 1890- 1892.
van den Brule, A.J.C., Meijer, C.J.L.M., Bakels, V., Kene- mans, P. and Walboomers, J.M.M. (1990) Rapid detection of human papillomavirus in cervical scrapes by combined general primer mediated and type specific polymerase chain reaction. J. Clin. Microbial. 28, 2739-2743.
Whttby, K. and Garson, J.A. (1995) Optimisation and evalua- tion of a quantitative chemiluminescent assay for Hepatitis C virus RNA. J. Virol. Methods 51, 75-88.
Wright, D.K. and Manos, M.M. (1990) Sample preparation from paraffin-embedded tissues. In: M.A. lnnis, D.H. Gelfand, J.J. Sninsky and T.J. White (Eds), PCR proto- cols: A guide to methods and applications. Ed: Pub: Aca- demic Press, SanDiego, CA, USA, pp. 153-158
Yee, C., Krishnan-Hewlett, I., Baker, C.C., Baker, C.C., Schlegel, R. and Howley, P. (1985) Presence and expres- sion of human papillomavirus sequences in human cervical carcinoma cell lines. Am. J. Pathol. 119, 361-366.
zur Hausen, H. (1989) Papillomavirus in anogenital cancer as a model to understand the role of viruses in human cancer. Cancer Res. 49, 4677-4681.
zur Hausen, H. (1994) Molecular pathogenesis of cancer of the cervix and its causation by specific human papillomavirus types. Curr. Top. Microbial. Immunol. 186, 131-156.