derango 2010 handout function 3 - nzimidnzimid.org/resources/3. derango 2010 handout function.pdfto...
TRANSCRIPT

3/14/2010
1
Dysfunction
Functional Treatment:Based on Disease Status and Risk
k
MODE
HIGH
Low Moderate Severe
Ris
k ERATE
Low
Disease Status
Treatment needs increase in intensity and aggressiveness as disease is more advanced and risk is higher. These two factors, risk and disease, need to be considered together when determining treatment.
Functional Risk Recognition
• Joint Health questionnaire /exam• Muscle Tenderness• Wear, Fremitus, Shifting of teeth• Type of diet
Existing bite relationship / Deep • Existing bite relationship / Deep overbites/Anterior open bites
• Position of teeth in face• Large masseters / Brachycephalics• Cause of existing tooth loss/ History• 9 Questions Interview
FOR DISCUSSION TODAY T.M.J. STANDS FOR:
TEETHMUSCLES JOINTS
• THESE ARE THE COMPONENTS OF OUR CHEWING SYSTEM .
• THIS ENTIRE SYSTEM MUST BE IN HARMONY AND FUNCTION TOGETHERAND FUNCTION TOGETHER
• Teeth that are stable : not wearing ,moving breaking
• Muscles that are healthy ,stable and work in harmony with the dental envelope
• Joints that have a proper codyle/disc/bone assemby , can accept load and are stable Smiles by design
Low Risk
At Risk
LOW MODERATE HIGH
Low Risk
At Risk
LOW MODERATE HIGHLow Risk
At RiskERO/ABR RISK ASSESSMENTLOW MODERATE HIGH
Erosive / Arbasion LesionsRecession
tooth brush hardness
Attrition (see function)
Mobility
Bleeding on probing (prognostic)
Pocket DepthsRecession(if yes check erosion)
DNA Pathogen TestingGenotypeShort Roots (Not a "risk factor" but, prognostic indicators)
Oral Hygiene
Furcation Involvement
PERIODONTAL RISK ASSESSMENTPast History of Periodontal Disease PERIODONTAL PROGNOSIS GOOD FAIR POOR
Medical Conditions (Diabetic Pts: Risk Increases with >7% H1AC Levels)Family HistoryPregnancy
Smoker
Exposed Root SurfacesFamily Members/Significant Other with DecayDeep Pits/Fissures, Developmental DefectsNon Fluoridated Water
Interproximal Enamel LesionsVisible PlaqueFrequent Sugary/Starchy SnacksOrtho Appliances of Partial DenturesXerostomia
Abrasivity of toothpaste
CARIES RISK ASSESSMENT
Rough White Spot LesionsActive Decay
Caries Restored in the Past 3 Years
Salivary Characteristics/xerostomiaMedical Conditions/gerd i.e.Medications / Supplements
Diet: Frequent Intake of Acidic Food/Beverages
Bone Loss (AAP > II)
Low Risk
At Risk
LOW MODERATE HIGH
Low Risk
At Risk
LOW MODERATE HIGH
Low Risk
At Risk
LOW MODERATE HIGH
\\Server\central form fi les\sec 9 Risk Forms
CariScreen Test Results
FUNCTIONAL RISK ASSESSMENT
Isthmus Width of RestorationTooth Location in Mouth
DietHabitsRoot Canal Treated Teeth, Full Coverage / Large Direct RestorationsOpposing TeethFunctional Risk Diagnosis
Masseter Muscle SizePast History of Tooth Fractures (Reason for existing crowns)Sensitivity to Bite/ craze lines
STRUCTURAL RISK ASSESSMENT
Tooth Shape
Bite Relationship (OPEN CONSTRICTED OTHER)
ESTHETIC RISK ASSESSMENTSmile LineBone CrestBiotype
Trouble with sleepPopping, clicking, joint soundsJaw pain, soreness, exhaustion, tension headachesGrinding, own/wear a occlusal guard BRUXING DYSFUNCTION NOT DETERMINEDExisting Wear(if yes check erosion) ACTIVE NON‐ACTIVE NOT DETERMINED YET
Trouble chewing a small piece of gumTrouble chewing bagels or dry chewy foodsTeeth changing in the last 5 years (wear, shorter/thinner, mobility, new spaces)More than 1 bite, clenching
15 years old
Low Risk
At Risk
LOW MODERATE HIGH
L At
Bite Relationship (OPEN CONSTRICTED OTHER)
Trouble with sleepPopping, clicking, joint soundsJaw pain, soreness, exhaustion, tension headachesGrinding, own/wear a occlusal guard BRUXING DYSFUNCTION NOT DETERMINEDExisting Wear(if yes check erosion) ACTIVE NON‐ACTIVE NOT DETERMINED YET
Trouble chewing a small piece of gumTrouble chewing bagels or dry chewy foodsTeeth changing in the last 5 years (wear, shorter/thinner, mobility, new spaces)More than 1 bite, clenching
FUNCTIONAL RISK ASSESSMENTg
7-10-08

3/14/2010
2
15 years old
Low Risk
At Risk
LOW MODERATE HIGH
L At
Bite Relationship (OPEN CONSTRICTED OTHER)
Trouble with sleepPopping, clicking, joint soundsJaw pain, soreness, exhaustion, tension headachesGrinding, own/wear a occlusal guard BRUXING DYSFUNCTION NOT DETERMINEDExisting Wear(if yes check erosion) ACTIVE NON‐ACTIVE NOT DETERMINED YET
Trouble chewing a small piece of gumTrouble chewing bagels or dry chewy foodsTeeth changing in the last 5 years (wear, shorter/thinner, mobility, new spaces)More than 1 bite, clenching
FUNCTIONAL RISK ASSESSMENTg
"Declare the past, diagnose the present, foretell the future; practice these acts. As to diseases, make a habit of two things — to help, or atof two things to help, or at least to do no harm.“
Hippocrates Epidemics, Bk. I, Sect. XI.
F ti Ri k A tFunction Risk Assessment □ □ □□ □ Trouble chewing a small piece of gum □ □ Trouble chewing bagels or dry chewing foods □ □ Teeth changing in last 5 years (wear, teeth appear shorter, thinner, loose or mobile, new spaces between teeth)□ □ More than 1 bite □ □ Trouble with sleep
□ □ Popping, clicking, joint sounds □ □ Jaw pain, soreness, exhaustion □ □ Clenching, grinding □ □ Existing wear □ □ Bite Relationship
UNDERSTANDING OCCLUSION IS CRITICAL TO THE LONG TERM SUCCESS OF OUR
DENTISTRY.HOW DO WE LOWER OUR PATIENT’S RISK TO HOW DO WE LOWER OUR PATIENT S RISK TO
OCCLUSAL DISEASE? WE HAVE TO DIAGNOSE IT FIRST!
Functional Diagnostic Categories
•Acceptable Function•Constricted Chewing Pattern•Occlusal DysfunctionOcclusal Dysfunction•Parafunction•Neurologic Disorders
Based on the work of John Kois, DMD
Terminology of OcclusionDental Envelope
dictated by anatomy of teeth
“Inside out”
Border MovementsPenwalt’s Envelope
Envelope of Function
orNeuromuscular
Envelope
“OUTSIDE IN” and Includes:AcceptableRestrictedDysfunctional

3/14/2010
3
Significant Concepts About the Envelope of Function
• Border movements are wider than functional zone.• Clinical evaluation of the functional zone is related to
postural position.• Dysfunction is characterized by a larger envelope of
functionfunction.• As the “home” position becomes more precise and
refined the functional zone narrows. • Other than true parafunction refining the home
position may help a patient clench less. Bilateral simultaneous and equal intensity contact is the goal.
Envelope of Destruction
– (Occasionally(Occasionally Dysfunction)
– Parafunction– Neurologic
TOOTH WEARWHAT DOES IT MEAN?
• TOOTH WEAR CAN BE AGE AND DIET APPROPRIATE AND PART OF A “NORMAL” OCCLUSION
• TOOTH WEAR IS NOT LINEAR THE WEAR YOU SEE TOOTH WEAR IS NOT LINEAR THE WEAR YOU SEE TODAY MAY HAVE OCCURRED YEARS EARLIER AND THE PATIENT HAS ADAPTED
• TOOTH WEAR CAN ALSO DEMOSTRATE THAT THE CHEWING SYSTEM IS OUT OF BALANCE AND THE STRESS IS BEING SEEN IN ABNORMAL WEAR
TOOTH WEARWHAT DOES IT MEAN?
• CAN BE CAUSED OR MODIFIED BY CHEMICAL PROCESSES
• CAN BE CAUSED BY MECHANICAL FORCES SUCH AS TOOTHPASTE OR TOOTHBRUSH ABRASION
• OUR JOB IS TO DETERMINE IF THE WEAR IS • OUR JOB IS TO DETERMINE IF THE WEAR IS ABNORMAL FOR THE AGE OF THE PATIENT AND IS IT DAMAGE AS A RESULT OF THE PATIENT’S OCCLUSION AND CHEWING (MASTICATORY) SYSTEM OR A CENTRAL NERVOUS SYSTEM PROBLEM( NEUROLOGIC OR TRUE PARAFUNCTION)
OCCLUSAL TOOTH TRAUMATISM(mobility) WHAT DOES IT MEAN?
DEFINED AS THE MOBILTIY OF THE TEETH RELATIVE TO THE ADJACENT TEETH.
OUR TEETH ARE HELD IN PLACE IF THE PERIODONTIUM HAS NOT BEEN COMPROMISED BY OCCLUSAL FORCES OR PERIODONTAL DISEASE.
PRIMARY OCCUSAL TRAUMATISM IS DEFINED AS LOOSENESS CAUSED BY EXCESSIVE FORCES ON A NORMAL PERIODONTIUM
SECONDARY OCCLUSAL TRAUMATISM IS DEFINED AS LOOSENESS CAUSED BY NORMAL FORCES ON A REDUCED PERIODONTIUM (BONE LOSS).
WHAT ARE SOME OF MY “TAKE HOME” MESSAGES FOR TODAY
• RECOGNIZE THAT WEAR ON TEETH IS NOT ALWAYS BRUXISM.
• RECOGNIZE THAT HOW YOU CHEW CAN CREATE TOOTH WEAR AND DESTROY YOUR DENTISTRY.
• UNDERSTAND THAT IF OUR CHEWING SYSTEM IS OUT OF BALANCE IN EITHER THE TEETH, THE MUSCLES, OR THE JOINTS, THE RESULT IS INCREASED RISK FOR OCCLUSAL DISEASE IN ONE OR MORE OF THE COMPONENTS
WHAT ARE SOME OF MY “TAKE HOME” MESSAGES FOR TODAY
• UNDERSTAND WHAT IS A PHYSIOLOGIC ACCEPTABLE OCCLUSION AND HOW UNDERSTANDING THIS AFFECTS THE DENTAL TREATMENT YOU WILL PROVIDETREATMENT YOU WILL PROVIDE
Functional Diagnostic Categories
•Acceptable Function•Constricted Chewing Pattern•Occlusal DysfunctionOcclusal Dysfunction•Parafunction•Neurologic Disorders
Based on the work of John Kois, DMD
Acceptable Function
• Physiological Wear• Efficient Use of Masticatory Muscles• Healthy or Stable Joints• Envelope of Function is WNL, HOWEVER
h l d f– Pathologic conditions exist if•Extrinsic localized (i.e. dietary factors)
create premature tooth structure loss.• Intrinsic localized (i.e. developmental
disturbances, GERD) create premature tooth structure loss.
• Iatrogenic

3/14/2010
4
ACCEPTABLE FUNCTION Chemical Erosion ? Is This Acceptable Function?
MalocclusionOcclusal InterferenceOcclusal DiscrepancyExcessive SlideLack Of GuidanceSteep GuidanceEtc, Etc
Diagnostic Opinion
10/99
99.10.8
Diagnosis of Acceptable Function Influences
• Material Choice And Prep Design• Post Op Expectations And Need For
Night Guards• Decrease Need For Posterior
Restorative Dentistry• Predictability of the restorations
8 Year Follow-up
10/2007
10 year follow-upWhat are the requirements of
an acceptable function ?
• FOR AN OCCLUSION TO BE STABLE, WE MUST BE ABLE TO BUILD OR MAINTAIN A MAXIMUM INTERCUSPATION THAT THE BRAIN CAN FIND AND IS COMFORTABLE. IF WE DO, THE PATIENT WILL BE ABLE TO CHEW COMFORTABLY AND NOT DESTROY YOUR DENTISTRY.
• .

3/14/2010
5
So If we do not have a stable occlusion, HOW DO WE START TO BUILD A BITE (MAXIMUM INTERCUSPATION) THAT THE BRAIN CAN
FIND AND IS COMFORTABLE?
WE START WITH THE THREE P’S OF OCCLUSION
The most Important things That I have learned at the Kois Center that have changed the way I approach clinical practice and patient care:
The Diagnostic Opinion / Risk AssessmentThe 10 Step Management Principles3 P’s of Occlusion
Keep This In Mind
“When evaluating different concepts, their similarities may be more
important than their differences.”
John C. Kois
THE THREE P’S OF OCCLUSION
• P1 POSITION : Orthopedic position of the mandible must be acceptable or must be established first
• P2 PLACE : Home position, the Maximum p ,intercuspation of the teeth(MIP) or how the teeth fit together at closing.
• P3 Pathway : Driveway into the Home, the working anterior guidance (outside /in) or guidance into maximum intercuspation.
Position PathwayTMJ Guidance
P1 P3
PlaceHome
P2
Functional OcclusionPosition (Orthopedic Position of mandible)
• M.I.PP1 • CR / Adapted Centric Posture • MyocentricObjective
• Reference / Starting PointTechnique
• FlawedConcerns
• M.I.P - Remaining Dentition • CR - Manipulation Techniques• NM - Muscles, Head Posture, Neurologic system
Place (Home)• Bilateral Equal Intensity Simultaneous ContactP2 • OVD? (Step 2 and 4)Obj ti OVD? (Step 2 and 4)Objective• Vertical Support / Posterior Teeth or Anterior PlatformTechnique
• Articulation Paper • Shim Stock• T - Scan • Digital Palpation
Concerns
• Mandibular Flexure • Worn Teeth• Periodontal Ligament • Pulpal Status
Pathway (Driveway)P • Steepness vs. Flatness3 Objective• Minimize Friction• Avoid Chewing Interferences
7
By J. Derango DDS
P1 = Position
© 2006 Kois Center, LLC
P2 = Place (home MIP)

3/14/2010
6
P3 = Pathway (driveway anterior guidance) P1 Position
• MIP The P1 position of the Existing bite: .
WHAT DO WE USE????
Teeth are KING
• Centric Relation /Adapted CR or Deprogrammed position:
• Neuromuscular Position myomonitorguided position:
Joint is KING
Muscles are KING
P1 Position
When can we use the P1 position dictated by MIP (the existing bite) ?
When we have a diagnosis of acceptable function are not at risk foracceptable function, are not at risk for developing occlusal problems and are not changing the vertical dimension of
occlusion(OVD)KEY: The P2 position is dictating the P1 position
With an effective and safe P3P1P2The P1 position may not be the most important of the
3 P’s
Smiles by design
P3P3
KEY: When the Home/Place(P2) is correct and you have an effective and safe Driveway/Pathway (P3) then the
Location/Position(P1) is not always the most important of the 3P’s.
This is why many dentist can do ok by h l hjust treating to MIP .This is also why
many orthodontist are successful with the teeth set up with good posterior contact P2 and correct overjet and
overbite P3
P1 PositionWhen do we use Centric Relation, the
deprogrammed position ?When our diagnosis is not acceptable
function, when we are changing the vertical di i f l i (OVD) hdimension of occlusion(OVD) or when we have the at risk patient needing extensive
single tooth dentistry(many teeth to be done one or two at a time)
KEY: The P1 position is dictating the P2 position
P1 Established from the Deprogrammed position

3/14/2010
7
WHEN DO YOU NEED CENTRIC RELATION AS YOUR P 1?
• ANYTIME YOUR TREATMENT WILL AFFECT OR REMOVE YOUR PATIENT’S EXISTING HOME OR PATHWAY.
• ANYTIME YOUR PATIENT HAS DIFFICULTY IN FINDING HOME P2 AND YOU ARE PLANNING TREATMENT THEN REMOVAL OF ONE TREATMENT. THEN REMOVAL OF ONE CONTACT CAN CAUSE THE PATIENT NOT TO BE ABLE TO FIND HIS “BITE”
• ANYTIME YOU CHANGE A PATIENT’S VERTICAL DIMENSION BY OPENING OR CLOSING HIS OVD.
P1 Position
When do we use Myocentric Position?
I use rarely
I
I use rarely
• This is not just how the teeth fit together. But fit together in harmony with the envelope of chewing
• Our goal is equal intensity, bilateral,
P2 Place
g q y, ,simultaneous contact of the posterior teeth. GOAL OF ALL OCCLUSAL CAMPS
• P2 sets the VDO The VDO is based on esthetics, functional, periodontal and biomechanical requirements
• Our guidance or pathway to where the teeth fit together. How do we get to home(P2) THE DRIVEWAY
• We have to look at the steepness vs flatness
P3 Pathway
pof the pathway. “Goldilocks Principle” too steep chance of CCP, to shallow chance of Occlusal Dysfunction . “Must be just right”
• Training tool to find P2 ?
• We normally check anterior guidance from the inside out but the chewing pathway occurs from the outside in. We need to re-evaluate our methods of checking guidance
P3 Pathway
If Occlusal problems are present then one or more of the three P’s is not in balanceP2 simultaneous , equal intensity, bilateral
contacts are common to all occlusal philosophies
3P’s Summary
philosophiesP1 may not be an exact point but an area
maintained by a healthy joint disc assemblyP3 is an outside-in guidance not inside-outP1 and P3 may serve as training wheels to
help find a newly established bite
FUNCTIONAL OCCLUSION
NOW LET’S LOOK AT HOW WE DIAGNOSE OCCLUSION
NOW LET’S LOOK AT HOW WE DIAGNOSE OCCLUSION
© 2006 Kois Center, LLC
DIAGNOSE OCCLUSIONDIAGNOSE OCCLUSION
CONCEPTS OF FUNCTIONAL OCCLUSION
WHAT ARE THE DIFFERENT POSSIBLE DIAGNOSIS?
Let’s look at each of these individually so we can learn to identify these clinically
Let’s look at each of these individually so we can learn to identify these clinically
© 2006 Kois Center, LLC
y yand use them in our treatment planning,
risk assessment, development of our prognosis
y yand use them in our treatment planning,
risk assessment, development of our prognosis
BASED ON THE WORK OF JOHN KOIS, D.M.D.
Diagnosis Decision ProcessFunctional Concerns
ACCEPTABLE FUNCTION (all 3 p’s acceptable)VS
CONSTRICTED CHEWING PATTERNVS
ACCEPTABLE FUNCTION (all 3 p’s acceptable)VS
CONSTRICTED CHEWING PATTERNVS
Prognosis Decreases
© 2006 Kois Center, LLC
OCCLUSAL DYSFUNCTIONVS
PARAFUNCTIONVS
NEUROLOGIC DISORDERS
OCCLUSAL DYSFUNCTIONVS
PARAFUNCTIONVS
NEUROLOGIC DISORDERS
Smiles by design
Based on the work of Dr John Kois Kois Center Seattle Wa

3/14/2010
8
Functional Diagnostic Categories
•Acceptable Function•Constricted Chewing Pattern•Occlusal DysfunctionOcclusal Dysfunction•Parafunction•Neurologic Disorders
Based on the work of John Kois, DMD
• Anterior tooth position is constricting the functional envelope
Constricted Chewing Pattern
• You may have wear and mobility of the anterior teeth.
• TMD – May contribute to the problem or be the result.
Constricted Chewing Pattern
• Can be broken down into two types:• First type is NON DISTALIZING. The
problem is demonstrated in the h f i hteeth…wear, fremitus, sore teeth.
• Second type is DISTALIZING. The problem is the constriction forces the condyle back and results in TMD issues.
Smiles by design
Constricted Path of Closure
Slides courtesy Of Dr Don Jayne
?
Constricted Path of Closure
Smiles by design
Slides courtesy Of Dr Don Jayne
Possible Signs Of Constricted Chewing Pattern
• Typical Wear Patten– Lingual Maxillary Anterior Teeth And
Facial Mandibular Anterior TeethM bilit Of A t i T th• Mobility Of Anterior Teeth
• No Posterior Mobility• Anterior Open Spaces• Fast Chewing – Fewer Cycles
Possible Signs Of Constricted Chewing Pattern
• Tender Joints / TMD• Tired Muscles When Speaking A Lot• Absence Of Wear On Posterior
T th*Teeth*• NOTE: Anterior Initial Contact
Following Deprogramming • Appearance And Position Of Teeth
In Face
*Depends On Timing Of Problem
What Can A Restricted E l L k Lik Cli i ll ?Envelope Look Like Clinically?

3/14/2010
9
Post-Ortho Mandibular Growth ?
Smiles by design
Restricted Envelope Of Function
What If The Dental Envelope Constricted The Functional Envelope
•Distalization Of The Condyle? p
??•Wear On The Linguals Of Max Incisors/Lower Buccals?
•Fremitus Or Flaring Of Anteriors?

3/14/2010
10
Ortho Literature
This paper looks at Chewing Envelope issues and how Anterior Guidance affects wear
d TMDand TMD
• It is this clinician's opinion that the concept of anterior interferences has not received adequate attention in our clinical management of orthodontic patients. Much has been written on the subject of Occlusal interferences in the posterior teeth during Occlusal function. This article will deal with the impact that anterior interferences have in the possible causation of specific Temporomandibular disorders and the impact of this information on how orthodontic cases should be finished. The effect of anterior i t f O l l d f ti i di d
Smiles by design
interferences on Occlusal dysfunctions is discussed. Finally, we will review the possible control of anterior interferences during fixed appliance mechanics. Five specific clinical sequela are identified, and their clinical implications in orthodontic treatment are reviewed. (Semin Orthod 2003;9:204-215.) © 2003 Elsevier Inc. All rights reserved.
The Five Known Consequences of Anterior Interferences
It is this clinician's observation and experience, having studied the clinical implications of anterior interferences, that five distinct clinical sequela can be identified. They are listed here in no particular order, and will be discussed separately in detail.
1. Anterior spacing and diastemas 1. Anterior spacing and diastemas 2. Fremitus3. Areas of excessive incisal wear4. Periodontal damage- gingival recession5. Intracapsular derangements of the
Temporomandibular joints
Figure 10. The initial contact between the maxillary and mandibular dentitions during the closing
movement of the mandible (A). Poster superior distraction of the mandible to establish posterior
intercuspation (B).
Figure 12. Corrected axis tomogram, demonstrating concentric position of the right
condyle at the point of initial contact (A). Corrected axis tomogram, demonstrating poster superior displacement of the right condyle as the patient
establishes maximum intercuspation (B).
SMILEImmediate post ortho age 13
2005 Age 18
Immediate post ortho Age 13
2005 Age 18 – Continued Mandible Growth
Class III Tendency: RISK
May be acceptable function now but at risk for CCP(P3 problem) and / or
Dysfunction(P2 problem)
Pre-Ortho Post-Ortho

3/14/2010
11
Can we achieve her esthetic desires , longer 4 incisors (correct reverse smile) and stay within her envelope of function?
Move Maxillary Anteriors ForwardMove Lower Anteriors BackProcline Maxillary AnteriorsRetrocline Lower AnteriorsSurgical corectionOpen Vertical Dimension of OcclusionUse Centric Relation P1 position
Can we achieve her esthetic desires and stay within her envelope of function?
Adjusting the envelope of function
Zone of high riskZone of high risk
•Chipped incisal edges bonded
• rebonded NC
• rebonded NC and nite guard
• new bonding agent rebond NC
• New Diagnosis
New Diagnosis
Reverse smile created by wear from constricted envelope
Full Composite Mock Up
Mock up for Dr. -Patient communication of desired results
Preparation/Temporization System
preservation of existing Incisal edge and contour

3/14/2010
12
Alginate of choice
Use of flexi-model technique to create functional temps
Duloid impression and mach 2 silicone. 3 minutes from start of impression to model
Flexi-Model System Multiple uses of flexi-models
Original contours used to guide new lingual contours , facial contours and
length
Original dental envelope….
Restored dental envelope….
Restoratively moving incisal 1/3 of tooth facially to unrestrict envelope
NOTE: ANGLE FROM PREP TO INCREASEROOM FOR ENVELOPE
Provisionals to confirm esthetics, function and a laboratory guide for final
restorations

3/14/2010
13
M t h t thi t
Laboratory Communication
Match to this contour M t h t thi t
Laboratory Communication
Match to this contour
Laboratory Verification
7&8 final veneers in relation to temps 9-10 note facial contour match
Temps day 3
Pre-op 2003Post-op 2009
Constricted Chewing Pattern Summary
o Anterior tooth position is constricting the functional envelope
o You may have wear and mobility of the anterior teeth or have spaces developing
o Typical Wear Pattern : Lingual Maxillary Anterior Teeth And Facial Mandibular Anterior Teeth
Smiles by design
Facial Mandibular Anterior Teeth o TMD– May contribute to the problem or be the result.o Absence Of Wear On Posterior Teeth, No posterior Mobilityo Previous ortho: Bicuspid extractions or early (before growth
completed) and Class III tendencyo Anterior Initial Contact Following Deprogramming o Appearance And Position Of Teeth In Face
Constricted Chewing Pattern Summary : How to Treat
•Orthodontics
Usually a problem of P3
•Surgical•Restorative: Open Vertical Dimension of Occlusion•Centric Relation P1 position
Functional Diagnostic Categories
•Acceptable Function•Constricted Chewing Pattern•Occlusal DysfunctionOcclusal Dysfunction•Parafunction•Neurologic Disorders
Based on the work of John Kois, DMD

3/14/2010
14
Occlusal DysfunctionA Posterior tooth position, that can cause an interference or avoidance pattern in the functional envelope to MIP(P2)MIP(P2)
Possible Signs of Dysfunction
• Muscle Fatigue or Soreness• More generalized wear facets can
appear or confuse with bruxismC h TMD• Can have TMD
• Usually posterior contact after deprogramming
• Can see anterior wear and mobility if avoidance pattern
Is this Acceptable Function? Dysfunction??
• Trouble chewing a small piece of gum• Trouble chewing bagels or dry chewy
foods • Teeth changing in last 5 years (active vs
adapted (wear, teeth appear shorter, thinner, loose or mobile, new spaces between teeth)
• More than 1 bite• Trouble with sleep
MUSCLE ENGRAMS ARE LEARNED MUSCLE PATTERNS THAT YOUR BRAIN DEVELOPS TO FIND P2(Place)
Risk and Disease Your risk in doing restorative dentistry in these types of patients are removing their “home” position
and putting your dentistry in a path that creates dysfunction.
How to find your bite
• Posterior Teeth / MIP• Anterior teeth /
Place P2Pathway P3
3P’s by Dr Kois
Anterior Guidance• Joint / CR /
Neuromuscular
Pathway P3
Position P1
What do we use to help develop the engrams
P2
P1
P3
How to find your bite
• Posterior Teeth / MIP• Anterior teeth /
Place P2Pathway P3
3P’s by Dr Kois
Anterior Guidance• Joint / CR /
Neuromuscular
y
Position P1
Kois Deprogrammer•Deprogram Muscle Engrams
•Aid in Diagnosis
•Establish a P1
•Aid in Equilibration establishing P2
“LUCIA JIG on a retainer”

3/14/2010
15
Risk and Disease Risk to RestorativeName: Referred by:
Married - Single - Divorced - Widowed DATE EMPLOYMENT/SCHOOL FAMILY
Risk Risk to Restorative Discussion L M H Biomechanical L M H Structural
L M H Carries
L M H Functional High risk to restorative Any tx to the bicuspids back face the risk of dysfunction a And not finding his bite. Check with shimstock Inform patient that he may need a deprogrammer And equilibration prior to any restorative tx or After treatment if problem with bite L M H Dentofacial
,tooth# Preliminary Treatment Definitive Treatment
Dysfunction acceptable constriction
Anterior open bite flat anatomy
Deep overbiteClass I
RISK TENDENCIES
SCI and erosion/attrition
Dysfunction/parafunction?
Gummy smile

3/14/2010
16
Goals of OrthoIntrude upper and lower anteriors to create room for restorative materials without additional tooth loss from preparation
Level posterior occlusal planes and align anterior gingival levels
Create a stable posterior occlusion P2 i d d P1 itiP2 in a deprogrammed P1 position, reduce dysfunction
Allow anterior room for an equilibration at end of ortho to create stable P2 position
Position anteriors, uppers and lowers , to allow a proper P3 ,anterior pathway, to be developed restoratively
Question: Where do you want the orthodontist
to position these teeth?
Use transitional bonding during orthodontic treatment to help get the ideal position
First layer is a very thin layer of bluish translucency to serve as a matrix for build-up and to allow for a natural translucency to the final restoration
KEY: do every other tooth to complete finish and polish then build the other teeth
right to the finished teeth
First layer is a very thin layer of bluish translucency to serve as a matrix for build-up and to allow for a natural translucency to the final restoration
Second layer is a dentin color to create lobes and preserve translucency between the lobes and at the incisal edge. Third layer is an incisal color to final contour
3/14/2010
17
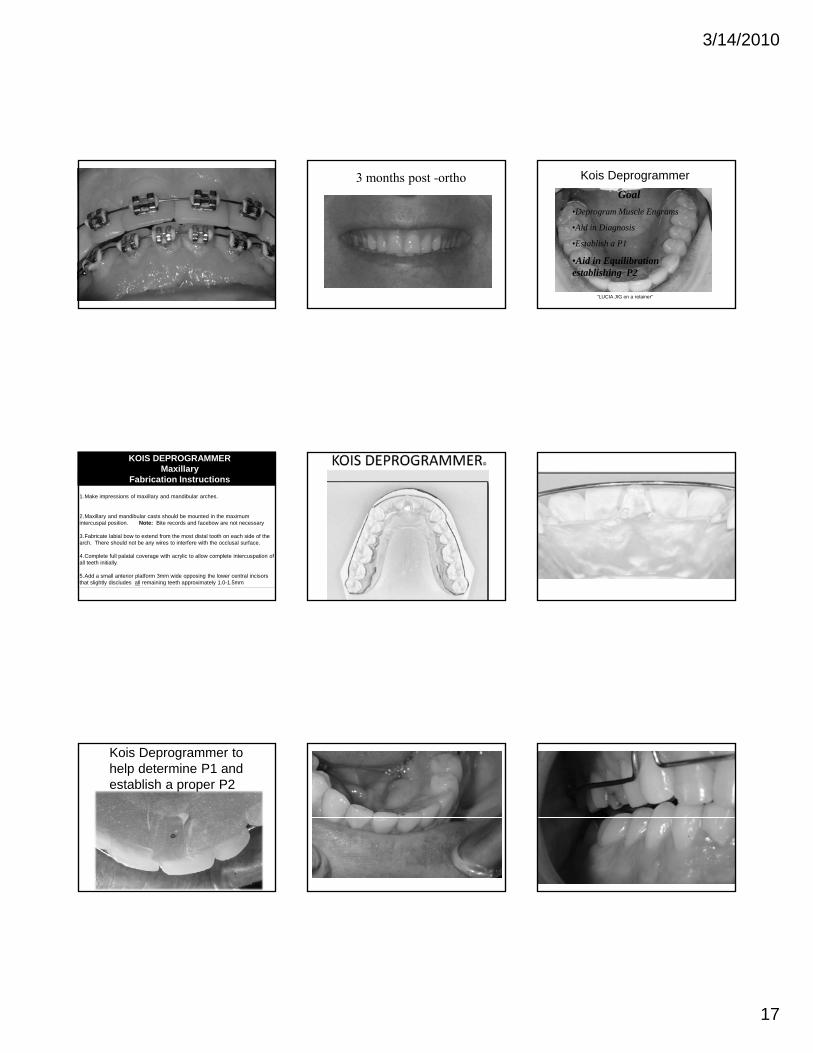
3 months post -ortho Kois DeprogrammerGoal
•Deprogram Muscle Engrams
•Aid in Diagnosis
•Establish a P1
•Aid in Equilibration establishing P2
“LUCIA JIG on a retainer”
1.Make impressions of maxillary and mandibular arches.
2.Maxillary and mandibular casts should be mounted in the maximum intercuspal position. Note: Bite records and facebow are not necessary
KOIS DEPROGRAMMERMaxillary
Fabrication Instructions
3.Fabricate labial bow to extend from the most distal tooth on each side of the arch. There should not be any wires to interfere with the occlusal surface.
4.Complete full palatal coverage with acrylic to allow complete intercuspation of all teeth initially.
5.Add a small anterior platform 3mm wide opposing the lower central incisors that slightly discludes all remaining teeth approximately 1.0-1.5mm
Kois Deprogrammer to help determine P1 and establish a proper P2

3/14/2010
18
First step is to adjust the anterior platform until the patient feels the first point of contact on the posterior teeth
Maximum intercuspation –simultaneous and equal bilateral contacts
GOAL
First point of contact after adjusting platform
Keep adjusting the anterior platform and the posterior teeth as you continue to refine the bite
Tooth contacts holding shim stock on all of the posterior teeth

3/14/2010
19
Refining the Envelope
ENVELOPE OF FUNCTION-- that creates harmony with muscle ,joints and tooth loading and an ANTERIOR GUIDANCE that correctly guides (Goldilocks) into maximum intercuspation
Envelope of Function has a Postural Component
Not This
Smiles by design
Correct patient position
Not This
Adjusted Lingual Contours And Retest
Final restorative dentistry can now be done as single tooth dentistry , Quadrant dentistry or Full arches
9 months post ortho

3/14/2010
20
Occlusal Dysfunction Summary
•Posterior tooth position that can cause an interference or avoidance pattern to MIP within the functional envelope resulting in wear and or TMD symptoms•Muscle Fatigue or SorenessMuscle Fatigue or Soreness•More generalized wear facets can appear or confuse with bruxism •Most likely a problem of P2
Functional Diagnostic Categories
•Acceptable Function•Constricted Chewing Pattern•Occlusal DysfunctionOcclusal Dysfunction•Parafunction•Neurologic Disorders
Based on the work of John Kois, DMD
Effect of a full-Arch Maxillary Occlusal Splint on Parafunctional activity during sleep in patients with
nocturnal bruxism and signs and symptoms of craniomandibular disorders
Holmgren K J Prosth.dent. 1993; 69:293-297
• The results revealed that the Occlusal splint does not stop the habit of
• The wear facets reappeared in the same location with the samenot stop the habit of nocturnal bruxismlocation with the same pattern
• During eccentric bruxismthe mandible moves far beyond the edge to edge contact relationship of the cuspids
Parafunction / Envelope of Destruction Treatment Goals
• Concept of mutual protection – The damage of horizontal excessive forces (bruxism) can be minimized – not eliminated
• Eliminate interferences within the functional envelopefunctional envelope
• Flatten anterior guidance• Minimize lateral contacts• Shallow the cuspid guidance pathway for
lateral destructive patterns• Shallow the anterior guidance pathway for
front to back destructive patterns
Parafunction
• Excessive vertical forces (clenching) cannot be reducedIntercuspal Position / Stable
Envelope of Destruction
• Intercuspal Position / Stable Vertical Contact Relationships
• simultaneous equal bilateral contact
• Deflecting incline contacts must be eliminated
Parafunction Parafunction Diagnosis
• High Risk Red Sticker• Patient Education And Communication Of
THEIR Risk NO GUARANTEE• Altered Preparation Design p g• Restorative Materials To Match Prep
Design• Flatten Guidance at expense of esthetics• Continued Use Of Night Guard Forever
Envelope of Destruction:Treatment Goals
• Concept of Mutual Protection– The damage of horizontal excessive
forces (bruxism) can be minimized – not eliminated
Eliminate interferences within the functional envelope
Fl tt t i id– Flatten anterior guidance– Minimize lateral contacts– Shallow the cuspid guidance pathway
for lateral destructive patterns– Shallow the anterior guidance pathway
for front to back destructive patterns

3/14/2010
21
Force Management
Niteguard like occlusionBuilt With Force Management in Mind. Flattened Anterior Guidance and Equal Bilateral Posterior Contacts.
Parafunctional Summary
• High Risk RED DOT
• Failure probable • Force Management Principles• Night Guards a must
BREAK TIME