delivery of maternal and newborn care services in africa: what are the facilities telling us? koye...
TRANSCRIPT
Delivery of Maternal and Newborn Care Services in Africa: What are the facilities telling us?
Koye Oyerinde MD, MPH, FAAPSymposium on Maternal Mortality, Dakar
The Averting Maternal Death and Disability Program - AMDD• Mailman School of Public Health, Columbia
University, New York City. • Help to strengthen heath systems to provide
emergency care for all women experiencing life-threatening obstetric complications.
• Conduct research and policy analysis, provide technical expertise, and advocate for solutions
• Collaborate with global, regional, and local institutions – including NGOs & academic centers

The Alliance• Memorandum of Understanding signed June
2008 between UNICEF, UNFPA, AMDD
• Alliance supports country plans for the strengthening of EmONC service delivery as a strategy for attaining MDGs 4 and 5.
• WHO collaborates on alliance activities at country and regional level.

Needs Assessment Overview• The EmONC Needs Assessments are facility
based cross-sectional studies of the capacity of a health system to provide health services to mothers and newborns
• Main focus – health system.▫ Accessibility/Coverage/Equity▫ 24 hour services▫ Human Resources▫ Equipment and Supplies▫ Infrastructure▫ Aspects of quality of care
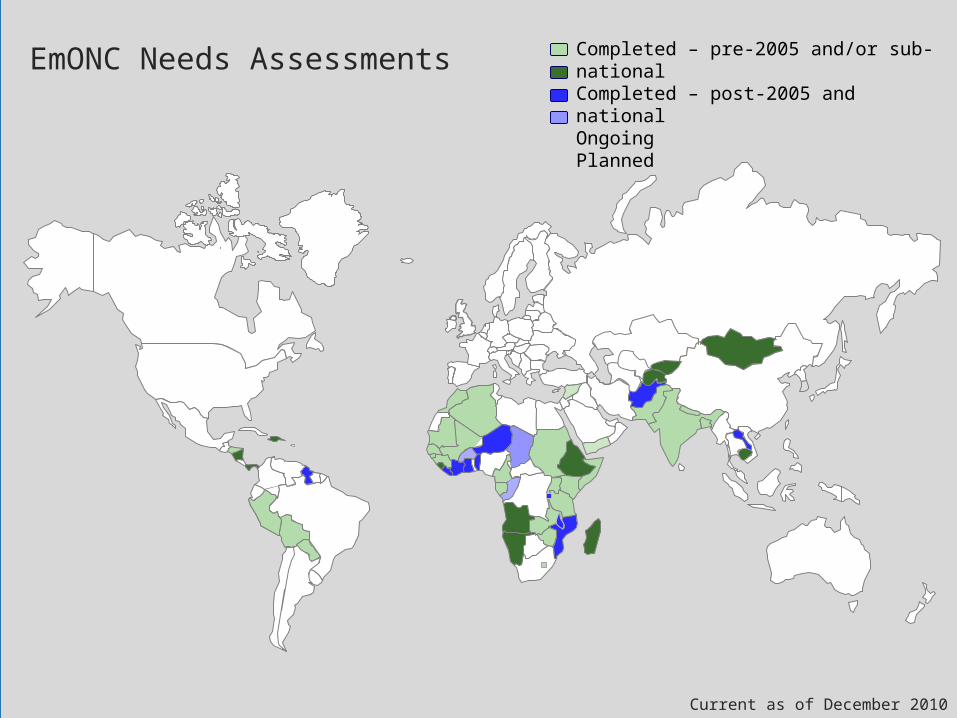
EmONC Needs Assessments Completed – pre-2005 and/or sub-nationalCompleted – post-2005 and nationalOngoingPlanned
Current as of December 2010

The Needs Assessment Process
• Conducting the Needs Assessment
Phase I: Advocacy and
Planning
Phase II: Conducting the
Needs Assessment
Phase III: From Data to Action
The AMDD team:
• provides customized technical support and training through these phases
• works remotely and in-country to support the MOH to conduct the assessments.

Some trends from the recent EmONC Needs Assessments in
Africa

Low no. of facilities offering EmONC signal functions
Coverage is defined as available EmONC facilities as a percentage of recommended EmONC facilities. There may be further disparities between urban and rural areas.
The recommended number of EmONC facilities is 5 per 500,000, at least one of which is Comprehensive (CEmONC).

Low no. of EmONC facilities Better CEmOC coverage than BEmOC
coverage But CEmOC requires BEmOC to function
properly BEmOC – 4 per 500,000 CEmOC – 1 per 500,000
Actual Recomm. Coverage Actual Recomm. Coverage
Ethiopia 25 591 4% 58 148 39%
Madagascar 3 155 2% 19 39 49%
Sierra Leone 0 48 0% 14 12 120%
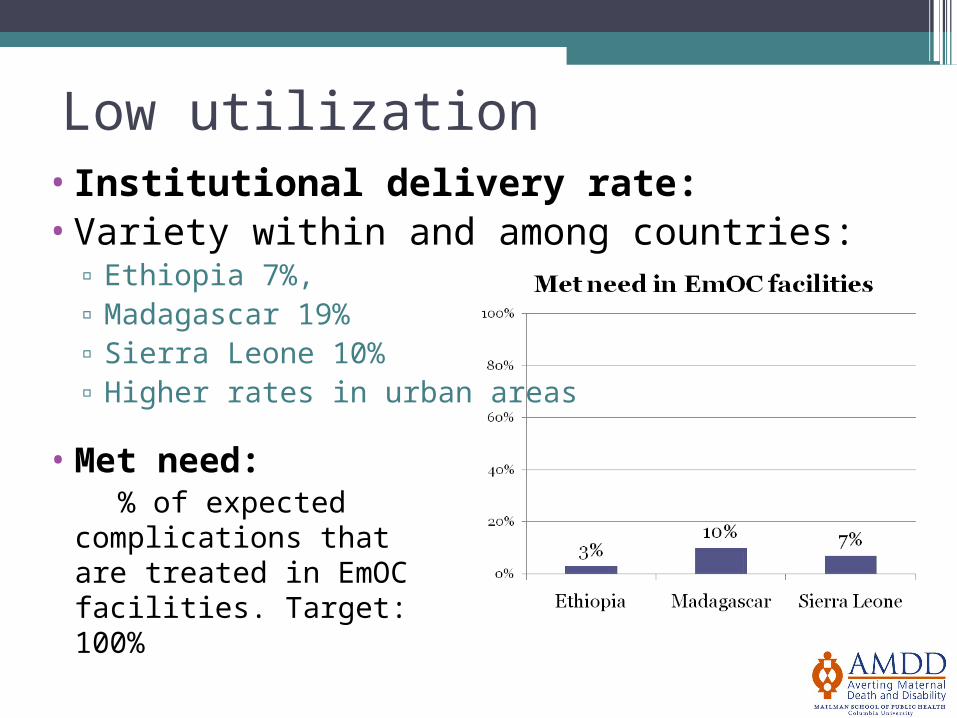
Low utilization•Institutional delivery rate: •Variety within and among countries:
▫ Ethiopia 7%, ▫ Madagascar 19%▫ Sierra Leone 10%▫ Higher rates in urban areas
• Met need: % of expected
complications that are treated in EmOC facilities. Target: 100%

Missing signal functions• MVA and AVD are most commonly missing SFs,
especially at the health center level.
Sierra Leone, 2008: Proportion of hospitals and CHCs by signal functions performed in last 3 months
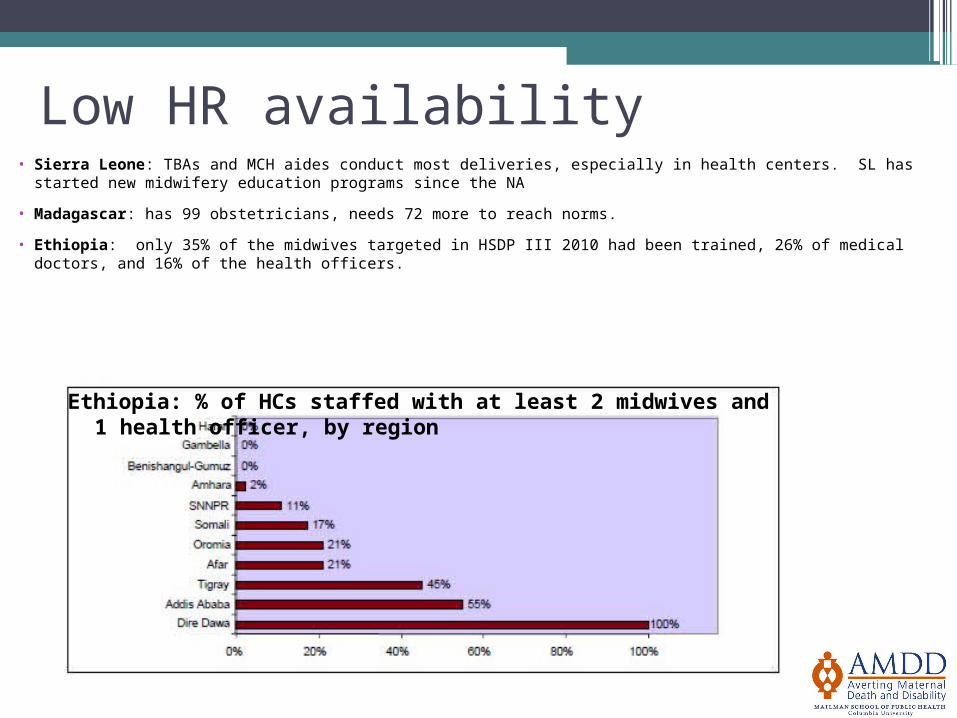
Low HR availability• Sierra Leone: TBAs and MCH aides conduct most deliveries, especially in health centers. SL has started new
midwifery education programs since the NA
• Madagascar: has 99 obstetricians, needs 72 more to reach norms.
• Ethiopia: only 35% of the midwives targeted in HSDP III 2010 had been trained, 26% of medical doctors, and 16% of the health officers.
Ethiopia: % of HCs staffed with at least 2 midwives and 1 health officer, by region

Inadequate commodities and supplies
Percentages of facilities with:
Misoprostol Mag Sulph Contraceptives
Ethiopia7% use for obstetric
indications
3% use as parenteral
anticonvulsant
90% have at least 3 methods
Madagascar11% (but 0% use for MVA)
0.68% use as parenteral
anticonvulsant
95% have oral contraceptives
Sierra Leone 21% 64% No info

Stock outsEthiopia: causes of delay of supplies in
hospitals
‘stock out atcentral store’ (41%)
‘financial problems’ (26%)
‘administrative difficulties’ (15%)
Madagascar: 73% of hospitals and 65% of health centers had not had a stock out of oxytocin, ergometrine, or atropine in the 12 months before the study.

Limited data collection•HMIS indicators
▫Often important indicators are not collected▫When collected the data are unused for
planning▫HMIS data often considered unreliable
A common outcome of the Needs Assessment is HMIS revision.
•Data collection at front-lines▫Facility registers often unclear and
incomplete ▫51% of health centers in Ethiopia had drug
and inventory registers

Fee for Service• Fees are often considered a barrier, especially for the
poorest.
• “Some women when told to go to the hospital would not because they do not have money; so they have problems during delivery” - Sierra Leone Needs Assessment, qualitative data:
• Sierra Leone made health services for pregnant and lactating mothers and children under 5 free in spring 2010▫ Initial reports suggest a phenomenal increase in
utilization; thus raising concerns for potential fall in quality of care

Socio-cultural barriers
•NA results are made more meaningful when combined with social science research
•Socio-cultural barriers – including abusive / disrespectful care - have been shown to delay utilization and limit benefits derived from the health system

An anthropologic question
Conclusion
•Needs Assessments have potential to surface gaps and indicate ways forward
•A systems science/health systems perspective is critical – we need strong health systems to support women during labor.

Conclusion
•Health facilities in Africa are saying:
▫Not enough, not the right type and not in the right place
▫Not adequately staffed, not with the right skills
▫Not adequately stocked, not with the right tools, drugs, and supplies

Many thanks!Merci beaucoup!
Further resources available from the AMDD website:
www.amddprogram .org