dallas, tx november 2–4, 2012 sepsis recognition and treatment of severe sepsis in the pediatric...
TRANSCRIPT

Dallas, TX • November 2–4, 2012
Sepsis
Recognition and Treatment of Severe Sepsis in the Pediatric and
Adult Populations
Dallas, TX • November 2–4, 2012
Can your staff recognize sepsis?
Sepsis can be subtle until it is so obvious you can’t miss it

Dallas, TX • November 2–4, 2012
62 year old admitted to hospital with hip infection
• On admission– T – 38.5– RR – 24– P – 104– WBC – 19,000
• Where should he be admitted?
Dallas, TX • November 2–4, 2012
36 hours post admission
Urine output drops – What should be done?
Dallas, TX • November 2–4, 2012
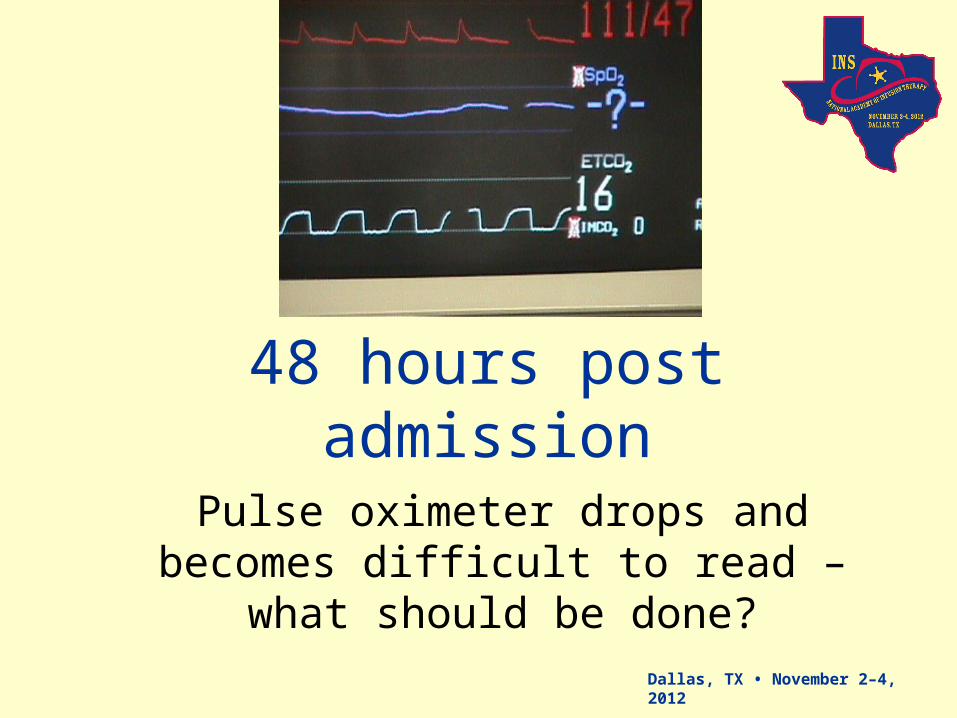
48 hours post admission
Pulse oximeter drops and becomes difficult to read – what should be
done?

Dallas, TX • November 2–4, 2012
Modified from criteria published in: Balk RA. Crit Care Clin. 2000;16:337-352. Kleinpell RM. Crit Care Nurs Clin N Am 2003;15:27-34.
CardiovascularTachycardiaHypotension
Altered CVP and PAOP
Renal OliguriaAnuria
Creatinine
Hematologic platelets,
PT/INR/ aPTT protein C D-dimer
Hepatic Jaundice
Liver enzymes Albumin
CNSAltered consciousness
Confusion
MetabolicMetabolic acidosis
Lactate level Lactate clearance
Respiratory Tachypnea
PaO2
PaO2/FiO2 ratio
IDENTIFYING ACUTE ORGAN DYSFUNCTION AS A MARKER OF SEVERE SEPSIS

Dallas, TX • November 2–4, 2012
Difference between Sepsis States
Sepsis / ICD 995.91 Severe Sepsis/ ICD 995.92 Septic Shock/ ICD 785.52
Pulse ≥ than 90 beats per minute
Respiratory rate ≥ than 20 breaths
per minute
Temperature > 38.0 oC or < 36.0 oC
WBC < 4,000 or > 12,000; or bands
> 10%
Pulse ≥ than 90 beats per minute
Respiratory rate ≥ than 20 breaths
per minute
Temperature > 38.0 oC or < 36.0 oC
WBC < 4,000 or > 12,000; or bands
> 10%
Pulse ≥ than 90 beats per minute
Respiratory rate ≥ than 20 breaths
per minute
Temperature > 38.0 oC or < 36.0 oC
WBC < 4,000 or > 12,000; or bands
> 10%
Real or suspected infection: Real or suspected infection: Real or suspected infection:
Organ dysfunction: Organ Dysfunction
Hypotension
SIRS- Patient’s labs/vitals reflect any two of the following with an infectious or noninfectious etiology: Temp= < 96.8 or > 100.4 RR= > 20/min or PaCO2 < 32 mmHG HR= > 90 bpm WBC= <4000 or > 12,000; or > 10% bands
Sepsis- Systemic Inflammatory Response Syndrome (SIRS) with an identified source or suspected source of infection.
Severe Sepsis- Sepsis associated with organ dysfunction, hypoperfusion or hypotension. Manifestations may include lactic acidosis, oliguria, and an acute alteration in mental status.
Septic Shock- Acute circulatory failure unexplained by other causes: SBP <90 or MAP < 60, Reduction in 40 mmHg from baseline despite adequate volume resuscitation or Patients who require inotropic or vasopressor support despite adequate fluid replacement.
Definitions
Dallas, TX • November 2–4, 2012
“Our arsenals for fighting off bacteria are so powerful, and involve so many different defense mechanisms, that we are more in danger from them than from the invaders.
“We live in the midst of explosive devices; we are mined!”
Lewis Thomas - 1972Germs, New England Journal Of Medicine
DR 32708 3000093662 1204.5 Copyright © 2004, Eli Lilly and Company. All rights reserved.Xigris is a registered trademark of Eli Lilly and Company.

Dallas, TX • November 2–4, 2012
“Except on few occasions, the patient appears to die from the body's response to infection rather than from it.”
Sir William Osler – 1904The Evolution of Modern Medicine

Dallas, TX • November 2–4, 2012
History of Treating Severe Sepsis
Antibiotics, fluids, vasopressors - Have they been successful?
Have we searched for better treatments?

Dallas, TX • November 2–4, 2012
Key to Success Rapid Identification
• Nursing’s role in identifying and helping in the treatment of sepsis is more important than ever before
• Implementing protocols on the floor, ED and ICU
• Physician and coder’s working together to improve documentation

Dallas, TX • November 2–4, 2012
12
Hemodynamics of Sepsis
• Concept of early resuscitation– Establishing urgency – use of
Lactate– Normal 1-2 mmol– > 4 mmol with metabolic acidosis
suggests tissue hypoxia
• Fluids with a goal– The role of mixed venous
oxyhemoglobin (ScvO2)
Dallas, TX • November 2–4, 2012
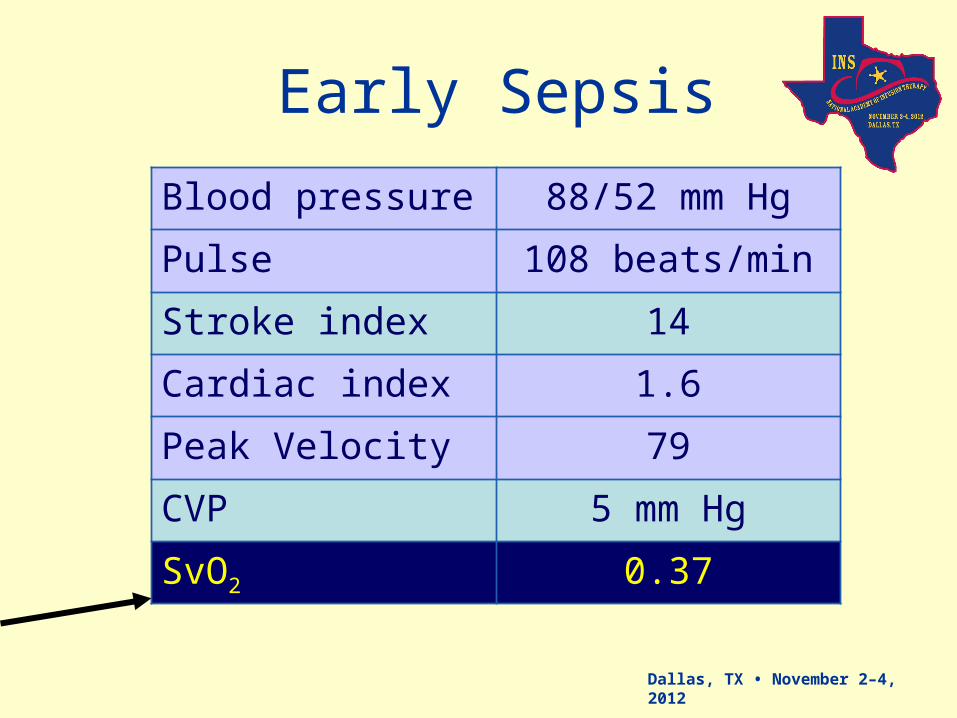
Early Sepsis
Blood pressure 88/52 mm Hg
Pulse 108 beats/min
Stroke index 14
Cardiac index 1.6
Peak Velocity 79
CVP 5 mm Hg
SvO2 0.37
Dallas, TX • November 2–4, 2012
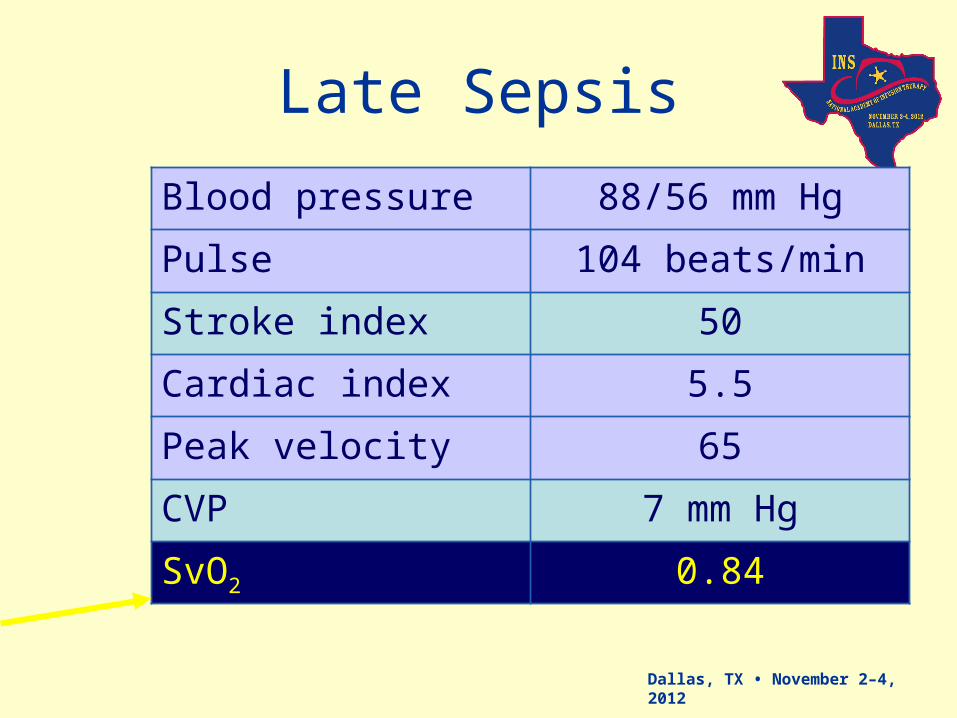
Late Sepsis
Blood pressure 88/56 mm Hg
Pulse 104 beats/min
Stroke index 50
Cardiac index 5.5
Peak velocity 65
CVP 7 mm Hg
SvO2 0.84
Dallas, TX • November 2–4, 2012
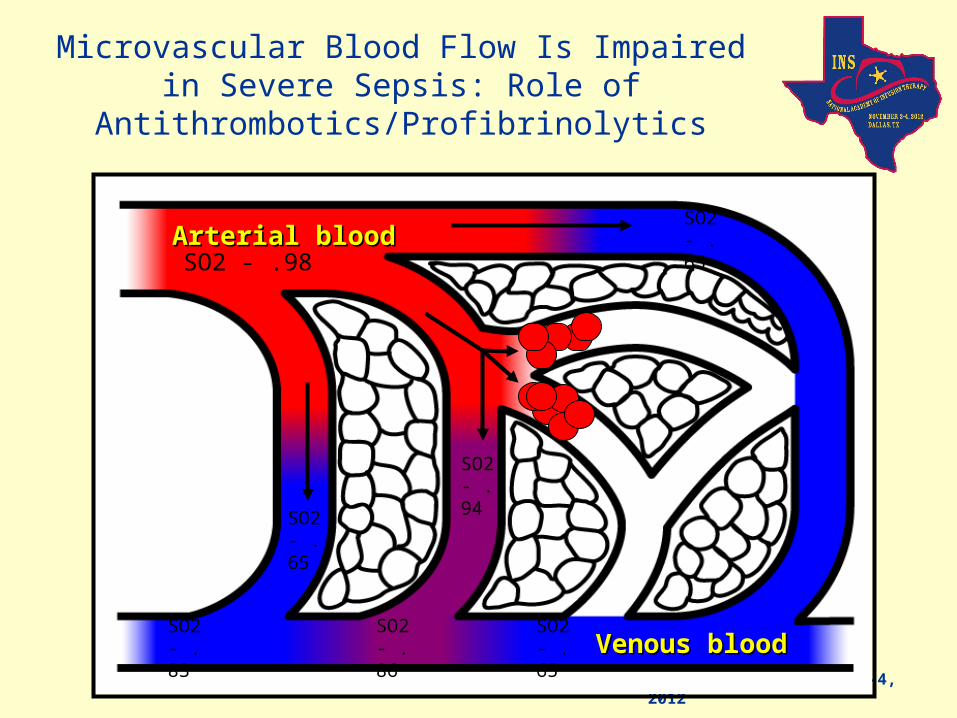
Microvascular Blood Flow Is Impaired in Severe Sepsis: Role of
Antithrombotics/Profibrinolytics
Venous bloodVenous blood
Arterial bloodArterial bloodSO2 - .98
SO2 - .94
SO2 - .65
SO2 - .86
SO2 - .65
SO2 - .83
SO2 - .65
Dallas, TX • November 2–4, 2012
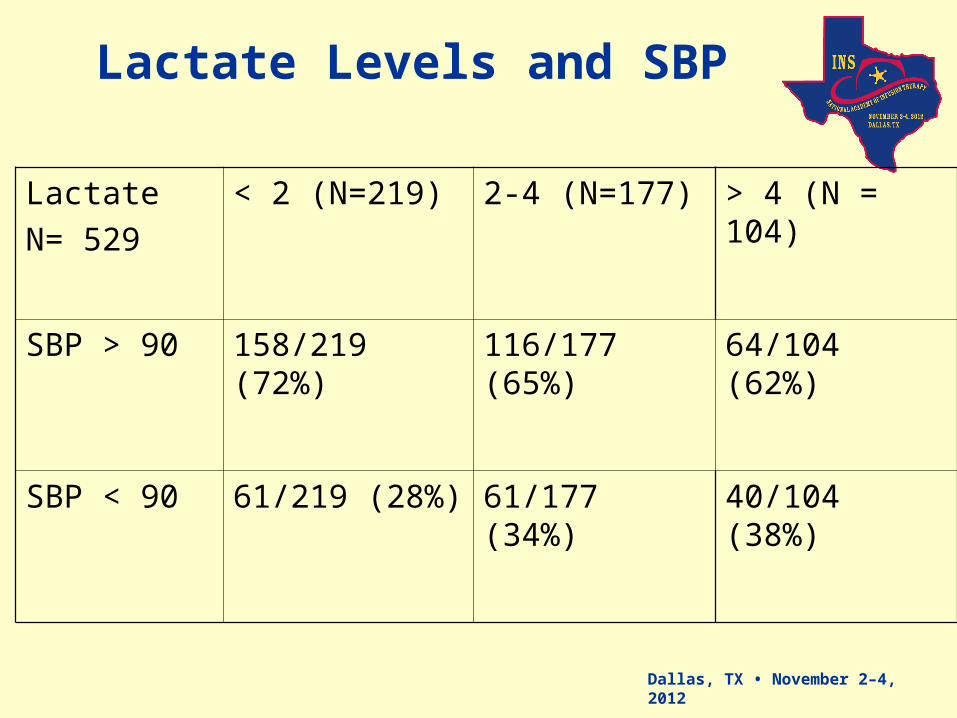
Lactate Levels and SBP
Lactate
N= 529
< 2 (N=219) 2-4 (N=177) > 4 (N = 104)
SBP > 90 158/219 (72%) 116/177 (65%) 64/104 (62%)
SBP < 90 61/219 (28%) 61/177 (34%) 40/104 (38%)
Dallas, TX • November 2–4, 2012
Case Example – Is Action Needed?
• 29 year old male with history of Crohn’s disease is admitted from ED with perirectal abscess.
• Lactate 5.9• SI – 20 ml/m2• StO2 - .51• SpO2 - .94• BP – 92/50• HR – 81• RR – 20• T – 38.1• UO – 1 ml/kg/hr (55
ml/hr)
Dallas, TX • November 2–4, 2012
Sepsis often progresses when the host cannot contain the
primary infection
• a problem most often related to– characteristics of the microorganism,
• such as a high burden of infection • the presence of superantigens and other virulence
factors, • resistance to opsonization and phagocytosis, • antibiotic resistance.
Dallas, TX • November 2–4, 2012
Cell dysoxia
• Epithelial cells have diminished oxygen consumption– due to a depletion of nicotinamide adenine
dinucleotide (NAD)
• Concept of cell stunning or hibernation

Dallas, TX • November 2–4, 2012
Pathophysiology of Sepsis
What do we need to know

Dallas, TX • November 2–4, 2012

Dallas, TX • November 2–4, 2012
Immune Response Immune Response

Dallas, TX • November 2–4, 2012
Coagulation and Impaired Fibrinolysis In
Severe Sepsis
Reprinted with permission from the National Initiative in Sepsis Education (NISE).
Endothelium
Neutrophil
Monocyte
IL-6IL-1TNF-
IL-6
Inflammatory Responseto Infection
Thrombotic Responseto Infection
Fibrinolytic Responseto Infection
TAFI
PAI-1
Suppressedfibrinolysis
Factor VIIIaTissue Factor
COAGULATION CASCADE
Factor Va
THROMBIN
Fibrin
Fibrin clotTissue Factor

Dallas, TX • November 2–4, 2012
Hotchkiss, R. S. et al. N Engl J Med 2003;348:138-150
The Response to Pathogens, Involving "Cross-Talk" among Many Immune Cells, Including Macrophages, Dendritic Cells, and CD4 T Cells

Dallas, TX • November 2–4, 2012
How do We Identify Sepsis Now?
In absence of biomarkers, must rely on crude physical indicators

Dallas, TX • November 2–4, 2012
SIRS AND SEPSISSepsis is defined as an infection
plus 2 SIRS criteria
• Temperature >38°C or <36°C
• HR >90 beats/min
• Respirations >20/min
• WBC count >12,000/mm3 or <4,000/mm3 or >10% immature neutrophils
SIRSSeveresepsis
MODSSeptic shock
SIRSSeveresepsis SepsisInfection
Other
Pancreatitis
Trauma
Burns
Sepsis
Levy MM, et al. Crit Care Med. 2003;31:1250-1256.

Dallas, TX • November 2–4, 2012
Case Study 1
Dallas, TX • November 2–4, 2012
Case Study 1
• 63 year old male in MICU with CAP, pneumothorax
• Progressing well but on day 3 – Develops spontaneous pneumothorax– RLL infiltrate
• Temp increases to 39.1– P – 122– BP – 92/58 (following EGDT)
• WBC 16,500• Is SOB, requires intubation, 50% FIO2,
AMV 12/14, Vt – 500 ccs, PEEP +10• Day 4
– SpO2 - .92, PaO2 64 (P/F ratio > 100), pH 7.28, PaCO2 32, HCO3 - 17
• Sepsis is suspected with treatment rapidly started
– Has received EGDT• 4 L NS• norepinephrine (Levophed) 30 mcg• ScvO2 < 60
• Is on hydrocortisone 50 mg Q 6 hrs• Insulin to keep glucose < 150 • Platelets – 110,000

Dallas, TX • November 2–4, 2012

Dallas, TX • November 2–4, 2012
Day 5

Dallas, TX • November 2–4, 2012
Case Study 2: Should Drotrecogin Alfa
(Activated) Have Been Started? • 62-year-old, 150 kg female with history of
ovarian cancer– Undergoes debulking surgery
for tumor– 4 days post-op develops
wound infection– Norepinephrine at
10 µg/min– PEEP 12 cm H2O, FiO2 90%– Sedated (Ramsey – 6)
• Drotrecogin alfa (activated) (24 µg/kg/hr) started on day 5– Day 6: norepinephrine off– Day 10: off ventilator
• Respiratory failure recurs on day 15• Dies on day 24

Dallas, TX • November 2–4, 2012
ICU Admission Characteristics
40% are low risk
Likely to recover without ICU admission
50% are mid risk
Will benefit and usually recover due to ICU care
10% are high risk
High mortality even with ICU care
Dallas, TX • November 2–4, 2012
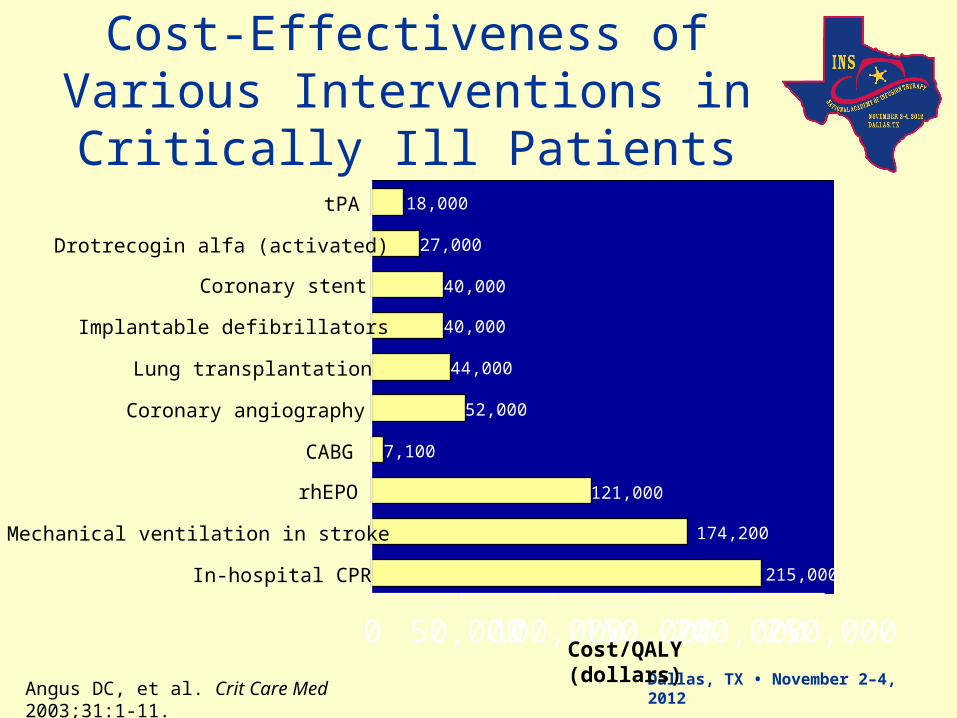
121,000
7,100
52,000
44,000
40,000
40,000
27,000
18,000
174,200
215,000
0 50,000100,000150,000200,000250,000
In-hospital CPR
Mechanical ventilation in stroke
rhEPO
CABG
Coronary angiography
Lung transplantation
Implantable defibrillators
Coronary stent
Drotrecogin alfa (activated)
tPA
Cost/QALY (dollars)
Cost-Effectiveness of Various Interventions in Critically Ill
Patients
Angus DC, et al. Crit Care Med 2003;31:1-11.

Dallas, TX • November 2–4, 2012
Erin K. Flatley/ Dr. Carl FlatleyIn 2002, sepsis claimed the life of Erin K. Flatley. Erin was a healthy, vibrant 23-year old graduate student in Florida. She went into the
hospital for a "routine" surgery but a post-operative infection occurred and because of the lack of recognition and prompt
treatment, it continued to advance. She died five days later. The killer was sepsis.
Stop the dying www.remembererin.com
Dallas, TX • November 2–4, 2012
Summary
• The bedside clinician, i.e. nurse or physician, is often the first to identify organ dysfunction as a marker of severe sepsis
• Treatments must be started rapidly to achieve benefit
• Cost issues are minimized by implementation of evidenced based practice