current status of evidence appraisal in appropriateness criteria development aha qcor conference...
TRANSCRIPT

Current Status of Evidence Appraisal in Current Status of Evidence Appraisal in Appropriateness Criteria Development Appropriateness Criteria Development
AHAAHAQCOR ConferenceQCOR Conference
Washington, DCWashington, DCMay 20,2010May 20,2010
Ralph Brindis, MD MPH FACCRalph Brindis, MD MPH FACCPresident, American College of CardiologyPresident, American College of Cardiology
Senior Advisor for CV Disease, Senior Advisor for CV Disease, Northern California Kaiser PermanenteNorthern California Kaiser PermanenteClinical Professor of Medicine, UCSFClinical Professor of Medicine, UCSF
Current Status of Evidence Appraisal in Current Status of Evidence Appraisal in Appropriateness Criteria Development Appropriateness Criteria Development
AHAAHAQCOR ConferenceQCOR Conference
Washington, DCWashington, DCMay 20,2010May 20,2010
Ralph Brindis, MD MPH FACCRalph Brindis, MD MPH FACCPresident, American College of CardiologyPresident, American College of Cardiology
Senior Advisor for CV Disease, Senior Advisor for CV Disease, Northern California Kaiser PermanenteNorthern California Kaiser PermanenteClinical Professor of Medicine, UCSFClinical Professor of Medicine, UCSF

Presenter Disclosure InformationPresenter Disclosure Information
• Ralph Brindis, MD MPH FACC FSCAIRalph Brindis, MD MPH FACC FSCAI• ““Current Status of Evidence Appraisal in Appropriateness Criteria Development”Current Status of Evidence Appraisal in Appropriateness Criteria Development”•
FINANCIAL DISCLOSURE:FINANCIAL DISCLOSURE:
NONENONE
UNLABELED/UNAPPROVED USES DISCLOSURE:UNLABELED/UNAPPROVED USES DISCLOSURE:
NONENONE

Institute of Medicine Priorities for AmericaInstitute of Medicine Priorities for America
• We must overhaul the system to create We must overhaul the system to create care to ensure it is:care to ensure it is:
Safe, Timely, Equitable, Efficient, Safe, Timely, Equitable, Efficient, Evidence-based and Patient-centeredEvidence-based and Patient-centered
• Care should…Care should…• Be customized to patients’ needs and valuesBe customized to patients’ needs and values
• Have the patient be the source of controlHave the patient be the source of control
• Enable knowledge to be shared freelyEnable knowledge to be shared freely
Adams, K & Corrigan,JM. Priority Areas for National Action:
Transforming Health Care Quality, IOM 2003 Institute of Medicine, Crossing the Quality Chasm:
A New Health System for the Twenty-first Century
Appropriate !!!Appropriate !!!Appropriate !!!Appropriate !!!

Variation in the Use of PCI vs. CABGVariation in the Use of PCI vs. CABG
February 4, 2009
US average is 2.6 PCIs for each CABG
http://www.dartmouthatlas.org/

Variation in PCI Higher than Other Procedures Variation in PCI Higher than Other Procedures Variation in PCI Higher than Other Procedures Variation in PCI Higher than Other Procedures
1.01.0
0.30.3
3.03.0
ColectomyColectomyfor CAfor CA
TURPTURPCABGCABG HipHipReplace-Replace-
mentment
Back Back SurgerySurgery
PCIPCI
Variation in procedures per 1000 MedicareVariation in procedures per 1000 Medicare patients in 306 hospital referral regions patients in 306 hospital referral regions Variation in procedures per 1000 MedicareVariation in procedures per 1000 Medicare patients in 306 hospital referral regions patients in 306 hospital referral regions
Source: Dartmouth AtlasSource: Dartmouth Atlas

Potential Impact of Inappropriate PCI
Potential Impact of Inappropriate PCI
• 900,000 PCI/yr in US
• 6% inappropriate and 38% uncertain (NY/Rand)
• 0-25% of uncertain PCI are actually inappropriate
• 900,000 PCI/yr in US
• 6% inappropriate and 38% uncertain (NY/Rand)
• 0-25% of uncertain PCI are actually inappropriate
~700 - 1700 deaths avoidable by eliminating Inappropriate PCI~700 - 1700 deaths avoidable by eliminating Inappropriate PCI
Inappropriate PCI

What are What are Appropriateness Criteria?Appropriateness Criteria?
• Define “what to do”, “when to do”, and “how often to do” in the Define “what to do”, “when to do”, and “how often to do” in the context of local care environments combined with patient and context of local care environments combined with patient and family preferences and valuesfamily preferences and values
• Address misuse, overuse and underuseAddress misuse, overuse and underuse• Connected to guideline content Connected to guideline content • Imply a level of detail and complexity that extends beyond the Imply a level of detail and complexity that extends beyond the
current recommendationscurrent recommendations

Guidelines and AUCGuidelines and AUC• Clinical Practice Guidelines (State of Science)
• Exhaustive review of literature• Virtually all-inclusive• Best practice • “Should do, should not do”
Class I, Class III, Class IIa, IIb
• Appropriate Use Criteria - AUC • Selective indications• Largely guideline based• Clinical scenarios/frequency • “Reasonable to do”
• Used to evaluate practice patterns
• Clinical Practice Guidelines (State of Science)• Exhaustive review of literature• Virtually all-inclusive• Best practice • “Should do, should not do”
Class I, Class III, Class IIa, IIb
• Appropriate Use Criteria - AUC • Selective indications• Largely guideline based• Clinical scenarios/frequency • “Reasonable to do”
• Used to evaluate practice patterns

Development of CPG’s, Performance Measures, and Development of CPG’s, Performance Measures, and Appropriate Use DocumentsAppropriate Use Documents
Antman, Circulation 2009:119:1180-1185.Antman & Peterson, Antman & Peterson, CirculationCirculation 2009:119:1180-1185. 2009:119:1180-1185.

APPROPRIATE USE CRITERIAThe ACC Queue
√ Nuclear cardiology (SPECT)October, 2005
√ Cardiac CT/CMR September, 2006
√ Echocardiography (TTE, TEE)
July, 2007
√ Echocardiography (Stress)December, 2007
Coronary revascularizationDecember, 2008
Revised radionuclide imagingMay, 2009
• Multi-modality criteria (with ACR)–Heart failure–Acute chest pain
• Revised CT criteria (completed)
• Revised echocardiography criteria
• Peripheral vascular disease
• Diagnostic catheterization
COMPLETED IN PROGRESS

Appropriateness Use Criteria Developed Using a Appropriateness Use Criteria Developed Using a Modified Rand/Delphi MethodologyModified Rand/Delphi Methodology
Appropriateness Use Criteria Developed Using a Appropriateness Use Criteria Developed Using a Modified Rand/Delphi MethodologyModified Rand/Delphi Methodology
The WritingThe WritingCommitteeCommittee
Define “Appropriateness” Define “Appropriateness” for Coronary Revascularizationfor Coronary Revascularization
Extensive CPG & literature Extensive CPG & literature review and synthesisreview and synthesis
of the evidence (usually after of the evidence (usually after clinical scenarios created)clinical scenarios created)
What are the known indicationsWhat are the known indicationsfor coronary revascularization?for coronary revascularization?
- Major randomized trials- Major randomized trials - Guidelines- Guidelines - Other sources- Other sources

Developing the Appropriateness Use CriteriaDeveloping the Appropriateness Use CriteriaDeveloping the Appropriateness Use CriteriaDeveloping the Appropriateness Use Criteria
The WritingThe WritingCommitteeCommittee
Define “Appropriateness” Define “Appropriateness” for Coronary Revascularizationfor Coronary Revascularization
CPG and literature review and synthesis CPG and literature review and synthesis of the evidence (pre and/or post clinical of the evidence (pre and/or post clinical
scenario creation)scenario creation)
Assumptions and Assumptions and DefinitionsDefinitions
What are the known indicationsWhat are the known indicationsfor coronary revascularization?for coronary revascularization?
- Major randomized trials- Major randomized trials - Guidelines- Guidelines - Other sources- Other sources 70% stenosis significant (>50% for LM)70% stenosis significant (>50% for LM)
Maximum medical therapyMaximum medical therapy (use of (use of 2 drug classes) 2 drug classes)High, Intermediate, low-risk stress testsHigh, Intermediate, low-risk stress testsHigh-risk clinical featuresHigh-risk clinical features (ECG, biomarkers, exam findings) (ECG, biomarkers, exam findings)

SY
MP
TO
MS
YM
PT
OM
SSST
AB
ILIT
ST
AB
ILIT
YY
ISC
HE
MIA
IS
CH
EM
IA
TE
ST
ING
TE
ST
ING
ME
DIC
AL
M
ED
ICA
L
Rx
Rx AN
AT
OM
AN
AT
OM
YY
Stable Stable anginaangina
STEMISTEMI
Class IClass IASxASx
Class IVClass IV
NoneNoneLow riskLow risk
HighHighriskrisk
NoneNone
MaxMax
No sig.No sig.CADCAD
LM +LM +3v CAD3v CAD
180180Clinical Clinical
ScenariosScenarios
Domains for Clinical Decision MakingDomains for Clinical Decision Making Five Core VariablesFive Core Variables
Domains for Clinical Decision MakingDomains for Clinical Decision Making Five Core VariablesFive Core Variables
OverOver40004000
PossiblePossibleClinical Clinical
ScenariosScenarios

Developing the Appropriateness Use CriteriaDeveloping the Appropriateness Use CriteriaDeveloping the Appropriateness Use CriteriaDeveloping the Appropriateness Use Criteria
The WritingThe WritingCommitteeCommittee
Define “appropriateness” Define “appropriateness” Preliminary CPG & literature searchPreliminary CPG & literature searchAssumptions & definitionsAssumptions & definitionsDeveloped 180 clinical scenariosDeveloped 180 clinical scenarios
• The Technical PanelThe Technical Panel– Nominated by professional societiesNominated by professional societies
– Selected for balance by the writing Selected for balance by the writing committee and Task Forcecommittee and Task Force
• 4 interventional cardiologists4 interventional cardiologists• 4 CT surgeons4 CT surgeons• 8 cardiologists8 cardiologists• 1 Health plan officer1 Health plan officer
Scenarios critiqued byScenarios critiqued byall organizationsall organizations
Scenarios modified and improvedScenarios modified and improved & In-depth literature, CPG search& In-depth literature, CPG search
Most examine the Most examine the “appropriateness” of“appropriateness” of
revascularizationrevascularization

Appropriateness ScoreAppropriateness Score
(7-9) Appropriate(7-9) Appropriate
(4-6) Possibly Appropriate/Uncertain (4-6) Possibly Appropriate/Uncertain
(1-3) Inappropriate(1-3) Inappropriate
Scored by a Technical PanelScored by a Technical Panel4 interventional cardiologists; 4 CT surgeons; 8 cardiologists; 1 Health plan officer4 interventional cardiologists; 4 CT surgeons; 8 cardiologists; 1 Health plan officer
Scored by a Technical PanelScored by a Technical Panel4 interventional cardiologists; 4 CT surgeons; 8 cardiologists; 1 Health plan officer4 interventional cardiologists; 4 CT surgeons; 8 cardiologists; 1 Health plan officer
The Technical PanelThe Technical Panel
MODIFIED RAND DELPHI METHODOLOGYMODIFIED RAND DELPHI METHODOLOGY
Independent 1Independent 1stst round ratings round ratings
Ratings tabulated – agreement determinedRatings tabulated – agreement determined
Face-to-face meeting – ratings discussedFace-to-face meeting – ratings discussed
Independent 2Independent 2ndnd and final round ratings and final round ratings
CCS Angina ClassCCS Angina Class
ASxASx I or I or IIII
III or III or IVIV
Number 17Number 17 Stable patients without prior CABGStable patients without prior CABG
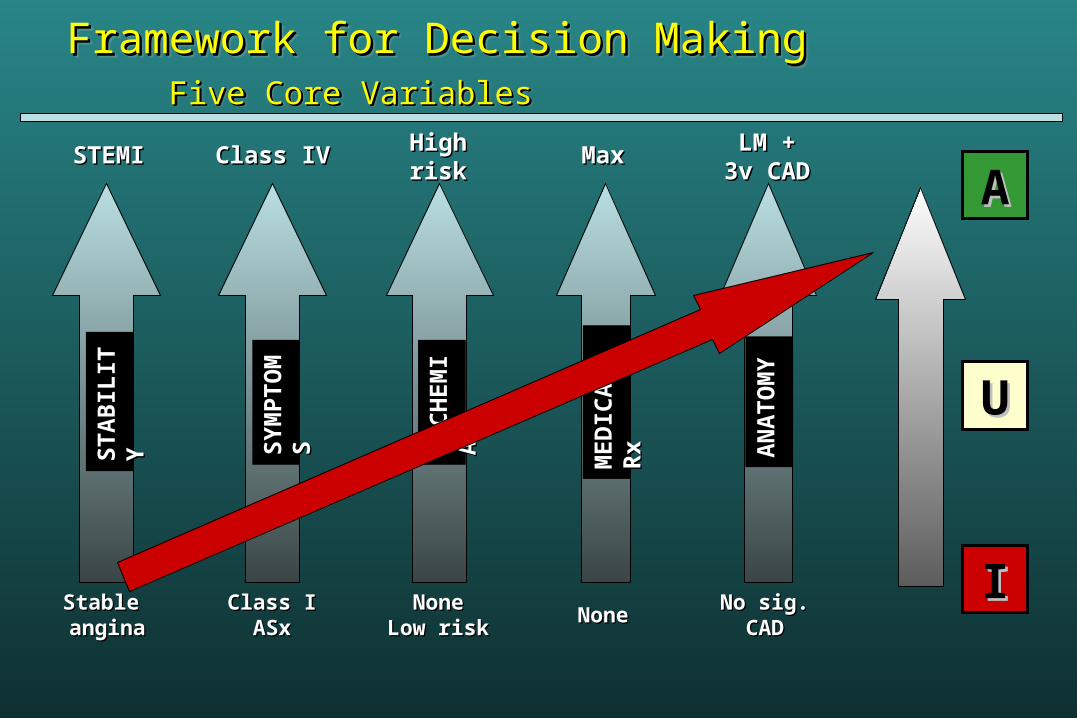
Framework for Decision MakingFramework for Decision Making Five Core VariablesFive Core Variables
Framework for Decision MakingFramework for Decision Making Five Core VariablesFive Core Variables
SY
MP
TO
MS
YM
PT
OM
SSST
AB
ILIT
ST
AB
ILIT
YY ISC
HE
MI
ISC
HE
MI
AA
ME
DIC
AL
M
ED
ICA
L
Rx
Rx AN
AT
OM
AN
AT
OM
YY
Stable Stable anginaangina
STEMISTEMI
Class IClass IASxASx
Class IVClass IV
NoneNoneLow riskLow risk
HighHighriskrisk
NoneNone
MaxMax
No sig.No sig.CADCAD
LM +LM +3v CAD3v CAD
AA
UU
II

Low-Risk Findings on Non-invasive Imaging Study Low-Risk Findings on Non-invasive Imaging Study
And Asymptomatic And Asymptomatic
(Patients Without Prior Bypass Surgery)(Patients Without Prior Bypass Surgery)Non-invasive testingNon-invasive testing
Symptoms/RxSymptoms/Rx
Burden of diseaseBurden of disease

AUC Methods are Robust, Thoughtful & Evidence Based
AUC Methods are Robust, Thoughtful & Evidence Based
• Unprecedented Transparency: AppendicesUnprecedented Transparency: Appendices• AUC Scores; Evidence tables & Maps to CPGs AUC Scores; Evidence tables & Maps to CPGs • AUC Coronary Revascularization: AUC Coronary Revascularization:
• 100% Congruence100% Congruence for CPG’s Class I & III Recs for CPG’s Class I & III Recs
• Cost is implicitly consideredCost is implicitly considered• Successfully Identifies new areas for researchSuccessfully Identifies new areas for research

Mapping of AUC with CPGsMapping of AUC with CPGs6.A(8)
STEMI with presumed successful treatment with fibrinolysis Asymptomatic; no HF, no recurrent ischemic symptoms, or no unstable
ventricular arrhythmias at time of presentation Depressed LVEF Three vessel coronary artery disease Elective/semi-elective revascularization
STEMI (p. e65) Percutaneous Coronary Intervention After FibrinolysisClass IIaIt is reasonable to perform routine PCI in patients with LVEF less than or equal to 0.40, CHF, or serious ventricular arrhythmias. (Level of Evidence: C)
PCI (p. e53)PCI After Successful Fibrinolysis or for Patients Not Undergoing Primary Reperfusion Class IIaIt is reasonable to perform routine PCI in patients with LV ejection fraction less than or equal to 0.40, HF, or serious
ventricular arrhythmias. (Level of Evidence: C)
CABG (p. e281)ST-Segment Elevation MI (STEMI)Class IIaIn patients who have had an STEMI or NSTEMI, CABG mortality is elevated for the first 3 to 7 days after infarction, and the benefit of revascularization must be balanced against this increased risk. Beyond 7 days after infarction, the criteria for revascularization described in previous sections are applicable. (Level of Evidence: B)

Mapping of AUC with CPGsMapping of AUC with CPGs13.Asymptomatic:
I2I or II: U5 III or IV: A7
One or two vessel coronary artery disease without involvement of proximal LAD
Low-risk findings on non-invasive testing Receiving a course of maximal anti-ischemic medical Rx
Chronic Stable Angina (p. 77-78)Recommendations for Revascularization With PCI (or Other Catheter-Based Techniques) and CABG in Patients With Stable AnginaClass ICoronary artery bypass grafting for patients with one- or two-vessel CAD without significant proximal LAD CAD who have survived sudden cardiac death or sustained ventricular tachycardia. (Level of Evidence: C)Class IIIUse of PCI or CABG for patients with one- or two vessel CAD without significant proximal LAD CAD, who have mild symptoms that are unlikely due to myocardial ischemia, or who have not received an adequate trial of medical therapy and
a. have only a small area of viable myocardium orb. have no demonstrable ischemia on noninvasive testing. (Level of Evidence: C)
Chronic Stable Angina (p. 90-91)Recommendations for Revascularization with PCI and CABG in Asymptomatic PatientsClass III Use of PCI or CABG for patients with one- or two-vessel CAD without significant proximal LAD CAD anda.only a small area of viable myocardium orb.no demonstrable ischemia on noninvasive testing. (Level of Evidence: C)Use of PCI or CABG for patients with borderline coronary stenoses (50% to 60% diameter in locations other than the left main coronary artery) and no demonstrable ischemia on noninvasive testing. (Level of Evidence: C)

Continued: Asymptomatic: I2; I or II: U5; III or IV: A7One or two vessel coronary artery disease without involvement of proximal LAD
Low-risk findings on non-invasive testingReceiving a course of maximal anti-ischemic medical Rx
Continued: Asymptomatic: I2; I or II: U5; III or IV: A7One or two vessel coronary artery disease without involvement of proximal LAD
Low-risk findings on non-invasive testingReceiving a course of maximal anti-ischemic medical Rx
• CABG (p. e 279)• Asymptomatic or Mild Angina• Class IIb• CABG may be considered for patients with asymptomatic or mild angina who have 1- or 2-vessel disease not
involving the proximal LAD (If a large area of viable myocardium and high-risk criteria are met on noninvasive testing, this recommendation becomes (Class I)Evidence:B
• CABG (p. e280)• Stable Angina• Class I• CABG is beneficial for patients with stable angina who have developed disabling angina despite maximal
noninvasive therapy, when surgery can be performed with acceptable risk. If angina is not typical, objective evidence of ischemia should be obtained. (Level of Evidence: B)
• Class III• CABG is not recommended for patients with stable angina who have 1- or 2-vessel disease not involving
significant proximal LAD stenosis, patients who have mild symptoms that are unlikely due to myocardial ischemia, or patients who have not received an adequate trial of medical therapy and
a. have only a small area of viable myocardium or (Level of Evidence: B) b. have no demonstrable ischemia on noninvasive testing. (Level of Evidence: B)

Continued: Asymptomatic: I2; I or II: U5; III or IV: A7One or two vessel coronary artery disease without involvement of proximal LAD
Low-risk findings on non-invasive testingReceiving a course of maximal anti-ischemic medical Rx
Continued: Asymptomatic: I2; I or II: U5; III or IV: A7One or two vessel coronary artery disease without involvement of proximal LAD
Low-risk findings on non-invasive testingReceiving a course of maximal anti-ischemic medical Rx
• PCI (p. e40)• Patients With Asymptomatic Ischemia or CCS Class I or II Angina• Class III• PCI is not recommended in patients with asymptomatic ischemia or CCS class I or II angina who do not meet the criteria as listed
under the class II recommendations or who have 1 or more of the following:• a. Only a small area of viable myocardium at risk• b. No objective evidence of ischemia.• c. Lesions that have a low likelihood of successful dilatation. • d. Mild symptoms that are unlikely to be due to myocardial ischemia.• e. Factors associated with increased risk of morbidity or mortality.• f. Left main disease and eligibility for CABG. • g. Insignificant disease (less than 50% coronary stenosis). (Level of Evidence: C)
• Stable Ischemic Heart Disease• Recommendations for Revascularization with CABG to Improve Survival in Patients with Stable Ischemic
Heart Disease
• Class IIa
Embargoed• Class III
Embargoed

Continued: Asymptomatic: I2; I or II: U5; III or IV: A7One or two vessel coronary artery disease without involvement of proximal LAD
Low-risk findings on non-invasive testingReceiving a course of maximal anti-ischemic medical Rx
Continued: Asymptomatic: I2; I or II: U5; III or IV: A7One or two vessel coronary artery disease without involvement of proximal LAD
Low-risk findings on non-invasive testingReceiving a course of maximal anti-ischemic medical Rx
• Recommendations for Revascularization with PCI to Improve Survival in Patients with Stable Ischemic Heart Disease
• Class IIa
Embargoed
• Class III
Embargoed
• Recommendations for Revascularization with CABG or PCI to Improve Symptoms in Patients with Stable Ischemic Heart Disease
• Class IIa
Embargoed
• Class Ib
Embargoed

Lessons with AUC-CPG MappingLessons with AUC-CPG Mapping
• Identification of “Holes” in Evidence Base possibly not Identification of “Holes” in Evidence Base possibly not acknowledged in CPGs WGsacknowledged in CPGs WGs
• Highlights opportunities of potential focus forHighlights opportunities of potential focus for
future studies or clinical trials to fill Evidence Gapsfuture studies or clinical trials to fill Evidence Gaps
• Opportunities for “cross-talk” with WGs of AUCs, CPGs, Opportunities for “cross-talk” with WGs of AUCs, CPGs, Consensus Documents, Scientific Advisories, Consensus Documents, Scientific Advisories, Performance Measures, and NCDR already occurring!Performance Measures, and NCDR already occurring!

What Do We Do When There is No Evidence? What Do We Do When There is No Evidence? Research!! Research!!
What Do We Do When There is No Evidence? What Do We Do When There is No Evidence? Research!! Research!!
• SPECT AUC: New Onset Atrial FibrillationSPECT AUC: New Onset Atrial Fibrillation• Low CAD risk: ULow CAD risk: U• High CAD: A High CAD: A
• SPECT CPG: No comment !!SPECT CPG: No comment !!
JACC 2007 50:1080JACC 2007 50:1080
Percentage of High-RiskPercentage of High-RiskSSS by Clinical Risk GroupsSSS by Clinical Risk Groups
Summed Stress Score ResultsSummed Stress Score Resultsin Patients W and Wo Atrial Fibrillationin Patients W and Wo Atrial Fibrillation

What Does Evidence-Based Mean? What Does Evidence-Based Mean? What Does Evidence-Based Mean? What Does Evidence-Based Mean?
• Methodology Manual for ACCF/AHA Guideline WritingMethodology Manual for ACCF/AHA Guideline Writing• Level of Evidence C: Level of Evidence C: Consensus opinion of experts, case studies, or Consensus opinion of experts, case studies, or
standard of care.standard of care.• ‘‘Despite all the evidence that may be available for writing the guideline, Despite all the evidence that may be available for writing the guideline,
expert interpretation is always necessary. Unfortunatelyexpert interpretation is always necessary. Unfortunately, much of the , much of the evidence falls into the “gray zone” of uncertainty.’evidence falls into the “gray zone” of uncertainty.’
• IOM 2001: Evidence based practice is the integration of best IOM 2001: Evidence based practice is the integration of best research evidence with clinical expertise and patient valuesresearch evidence with clinical expertise and patient values
• Even so, must guard against over-reaching:Even so, must guard against over-reaching:• Echo GL Class III: Echo GL Class III: Routine screening echo for participation in Routine screening echo for participation in
competitive sports in pts with a normal cardiovascular examcompetitive sports in pts with a normal cardiovascular exam• Echo AUC: Echo AUC: No commentNo comment

AMA Physician Consortium for AMA Physician Consortium for Performance Improvement (PCPI)Performance Improvement (PCPI)
Evidence Required for Measures DevelopmentEvidence Required for Measures Development
AMA Physician Consortium for AMA Physician Consortium for Performance Improvement (PCPI)Performance Improvement (PCPI)
Evidence Required for Measures DevelopmentEvidence Required for Measures Development
• PCPI considers all types of evidence reviewed in PCPI considers all types of evidence reviewed in guidelines, including expert opinion. guidelines, including expert opinion.
• Additional conditions must be met for acceptance of Additional conditions must be met for acceptance of guidelines with recommendations based on expert guidelines with recommendations based on expert opinion (e.g., opinion (e.g., use of a formal consensus use of a formal consensus development processdevelopment process). ).

PCPI Conditions for Acceptance of Recommendations Based on Consensus Opinion
PCPI Conditions for Acceptance of Recommendations Based on Consensus Opinion
Recommendation StatementsRecommendation Statements• Strength of Recommendation rated – HIGH PRIORITY (H.P.)Strength of Recommendation rated – HIGH PRIORITY (H.P.)• Methods used for grading strength of Rec. described - H.P.Methods used for grading strength of Rec. described - H.P.
Consensus Development ProcessConsensus Development Process• Consensus Development Process Described- REQUIREDConsensus Development Process Described- REQUIRED• Formal Consensus Method Used – REQUIREDFormal Consensus Method Used – REQUIRED• Informal Consensus Method Used – NOT ACCEPTABLEInformal Consensus Method Used – NOT ACCEPTABLE
Potential Benefits and HarmsPotential Benefits and Harms• Anticipated benefits and potential risks associated with recommendations Anticipated benefits and potential risks associated with recommendations
described. Benefits must > risk – H.P.described. Benefits must > risk – H.P.
Reproducibility of Appropriateness Reproducibility of Appropriateness Ratings in Cardiovascular ImagingRatings in Cardiovascular Imaging
Reproducibility of Appropriateness Reproducibility of Appropriateness Ratings in Cardiovascular ImagingRatings in Cardiovascular Imaging
• 2 Independent Panels (15 multi-speciality physicians)2 Independent Panels (15 multi-speciality physicians)• Stress Echo Panel and TTE/TEE panel Stress Echo Panel and TTE/TEE panel
• Rated the same 19 clinical indicationsRated the same 19 clinical indications• (Mixture of Stress and TTE/TEE)(Mixture of Stress and TTE/TEE)• 8 8 (42%) Inappropriate(42%) Inappropriate, 9 , 9 (47%) Appropriate(47%) Appropriate, ,
2 2 (11%) Uncertain(11%) Uncertain
• Agreement between panels for overall appropriateness Agreement between panels for overall appropriateness group (A,I,U) was 100%group (A,I,U) was 100%
Patel QCOR 2008Patel QCOR 2008

GL and AUC Have LimitationsGL and AUC Have Limitations
• Shared by GL and AUC Shared by GL and AUC (Antman Circ 2009 119:1180)(Antman Circ 2009 119:1180)• Insufficient evidence base; Not yet ‘living’ documentsInsufficient evidence base; Not yet ‘living’ documents• Incomplete translation to practiceIncomplete translation to practice• Untapped potential to improve careUntapped potential to improve care• Weak methods to measure consistent useWeak methods to measure consistent use• Neither can cover all clinical scenariosNeither can cover all clinical scenarios
• Practice Guidelines have additional limitationsPractice Guidelines have additional limitations• Explicitly exclude costs, cost effectivenessExplicitly exclude costs, cost effectiveness• Real risk of ‘academic vacuum’- Unrealistic, unmanageable in our Real risk of ‘academic vacuum’- Unrealistic, unmanageable in our
current health care environmentcurrent health care environment

AUC and CPG Interplay AUC and CPG Interplay• Imaging AUC Writing Groups has led to increased interest in the Imaging AUC Writing Groups has led to increased interest in the
role & value of Framingham Risk Score and also the new CV Risk role & value of Framingham Risk Score and also the new CV Risk Guidelines publication for AUC ratings of imaging testing. Guidelines publication for AUC ratings of imaging testing.
• Leape describes Guideline adherence poorer when changing Leape describes Guideline adherence poorer when changing practice patterns “ahead” of the CPG revisions. True also with AUC.practice patterns “ahead” of the CPG revisions. True also with AUC.
• To remain useful and credible, Guidelines and AUC documents To remain useful and credible, Guidelines and AUC documents need frequent revision when practice is advancing. Annual need frequent revision when practice is advancing. Annual revisions may be needed.revisions may be needed.

AUC Implementation and Evaluation :AUC Implementation and Evaluation :What Have We Learned So FarWhat Have We Learned So Far
AUC Implementation and Evaluation :AUC Implementation and Evaluation :What Have We Learned So FarWhat Have We Learned So Far
• Retrospective and prospective reviews Retrospective and prospective reviews
• >20 abstracts published; 2 peer-reviewed publications >20 abstracts published; 2 peer-reviewed publications
• Average inappropriate rates prior to intervention 10% - Average inappropriate rates prior to intervention 10% - 20%20%
• Preliminary studies of tools and education reduce by Preliminary studies of tools and education reduce by 50% or more inappropriate use50% or more inappropriate use
• Refinement of process; validation of ratingsRefinement of process; validation of ratings

Challenges with Challenges with Appropriateness Use RatingsAppropriateness Use Ratings
Challenges with Challenges with Appropriateness Use RatingsAppropriateness Use Ratings
• Rely on collection of currently unavailable clinical data to map patients Rely on collection of currently unavailable clinical data to map patients to appropriateness ratingsto appropriateness ratings
• Can the data always be collected?Can the data always be collected?
• Can patients be mapped to the prototypical scenarios?Can patients be mapped to the prototypical scenarios?
• SPECT MPI pilot project suggests yes with ideas to make data SPECT MPI pilot project suggests yes with ideas to make data collection easier and quicker!!collection easier and quicker!!
• Still being validated - AUC implementation will provide pragmatic, Still being validated - AUC implementation will provide pragmatic, observational research opportunities to study outcomes in specific observational research opportunities to study outcomes in specific populationspopulations
• No data yet demonstrating equal, improved, or worse outcomes with No data yet demonstrating equal, improved, or worse outcomes with AUC implementationAUC implementation
• Potential of CER (PCORI) for increasing evidence basePotential of CER (PCORI) for increasing evidence base

Stress or Imaging Studies Performed5100 : O No O Yes →If Yes, Specify Test Performed:
Test Performed
NoYes Result
Risk/Extent Of Ischemia
Standard Exercise Stress Test: (w/o imaging)
O O →If Yes,O Negative O Positive O Indeterminant O Unavailable
→If Positive,
O Low O Intermediate O High O Unavailable
Stress Echocardiogram
O O→ If Yes,
O Negative O Positive O Indeterminant O Unavailable
→ If Positive,
O Low O Intermediate O High O Unavailable
Stress Testing w/SPECT MPI
O O →If Yes,O Negative O Positive O Indeterminant O Unavailable
→If Positive,
O Low O Intermediate O High O Unavailable
Stress Testing w/CMR
O O →If Yes,O Negative O Positive O Indeterminant O Unavailable
→ If Positive,
O Low O Intermediate O High O Unavailable
Cardiac CTA O O →If Yes,O No disease O 1VD O 2VD O 3VD O Indeterminant O Unavailable
Coronary CalciumScore
O O→ If Yes,
Calcium Score:5251____________
Noninvasive Testing Noninvasive Testing

AUC: Implementation & EvaluationAUC: Implementation & EvaluationNew TechnologyNew Technology
ACC Cardiovascular Imaging Solution
• Migration towards point-of-orderMigration towards point-of-order
• Embedded clinical decision supportEmbedded clinical decision support
• Tracking/data registryTracking/data registry
• Reporting/feedbackReporting/feedback

““The right objective for health The right objective for health care is to increase value for care is to increase value for
patients, which is the quality of patients, which is the quality of patient outcomes relative to the patient outcomes relative to the
dollars expended.”dollars expended.”
- Michael Porter- Michael Porter
““The right objective for health The right objective for health care is to increase value for care is to increase value for
patients, which is the quality of patients, which is the quality of patient outcomes relative to the patient outcomes relative to the
dollars expended.”dollars expended.”
- Michael Porter- Michael Porter
