cryotherapy and leep
DESCRIPTION
Cryotherapy and LEEP, Dr. dr. Dwiana Ocviyanti, Sp. OG(K), JNPK - Department of Obstetrics and Gynecology Faculty of Medicine University of IndonesiaTRANSCRIPT

Cryotherapy and LEEP
Dwiana Ocviyanti• Department of Obstetrics and Gynecology Faculty of
Medicine University of Indonesia• National Clinical Training Network of Reproductive
Health/NCTN-RH

Back Ground• Some procedures being used to manage precancerous
lesions (dysplasia or CIN) are hysterectomy and cone biopsy
• Available scientific evidence supports the use of several outpatient procedures (e.g., cryotherapy and LEEP/Loop Electrosurgical Excision Procedures) as being highly effective
• The use of inpatient methods such as cone biopsy and hysterectomy are more costly and potentially more risky to women
• Cervical cancer screening in developing countries is offered at low resource healthcare system where outpatient treatment would be more proper if available.

Treatment for precancerous lesions
• In order for cervical cancer prevention programs to be truly effective and of public health value, testing should be linked to appropriate treatment for any precancerous lesions detected.

What lession need to be treated?
• High-grade (CIN II–III) lesions should be treated because they are more likely than low-grade lesions (CIN I) to progress to cancer
• Published studies indicate that most low-grade lesions will regress spontaneously and thus do not require treatment
• When close follow up or histological confirmation is not feasible or possible, treatment of acetowhitelesions (that could be low-grade or high-grade lesions, or a false positive) may be advisable, particularly if the treatment is not highly invasive or associated with serious side effects, complications or long-term sequellae.

Selection criteria
• The transformation zone must be fully visible
• There should be no suspicion of microinvasive disease or adenocarnoma in situ
• ATZ not extend into endocervical canal
• CIN biopsy proven
• Assesment by skilled colposcopist

The advantages of cryotherapy
• effective with small- and moderate- sized lesions (85–95% cure rate)
• inexpensive
• can be performed by non physician
• no local anesthesia required
• no electricity required
• associated with few complications/ side effects

The disadvantages of Cryotherapy
• variable success rate with large lesions (75–85% cure rate)
• destructive (leaves no tissue sample for confirmatory diagnosis)
• difficult to determine exact amount of tissue destroyed
• associated with profuse watery discharge for up to 6 weeks following treatment
• requires access to and resupply of coolant (CO2 or N2O).

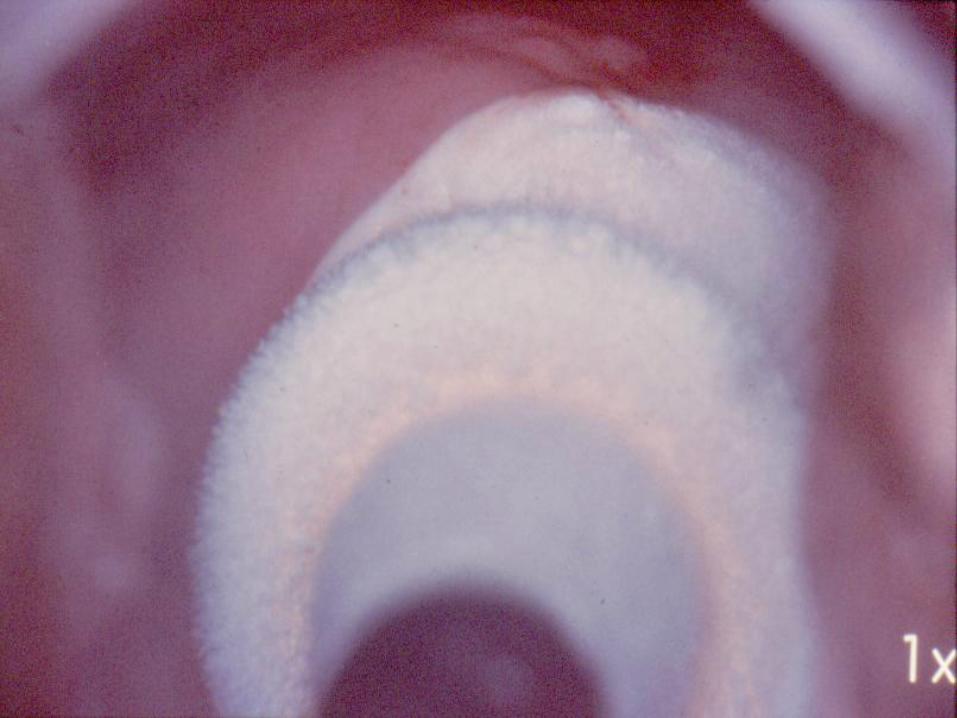
Cryotherapy
• The refrigerant gas N2O (-90 C), CO2 (-60 C).
• A single-freeze ( 3 minutes)
• A double freeze ( 3 min freze, 5 min thaw and 3 min refreeze)

The advantages of LEEP
• Effective (80–96% cure rate for all lesions), enables tissue sampling for diagnosis and associated with few complications/ side effects

The disadvantages of LEEP
• The equipment is more expensive than cryotherapy
• primary side effect is peri- and postoperative bleeding (about 3–8%)
• requires physician to perform it
• requires local anesthesia
• requires electricity (but could be battery powered)
• requires resupply of loops.

Some differences in effectiveness rates between cryotherapy and LEEP
• Especially when lesion size is large a recent randomized clinical trial,showed that, overall, the differences were not statistically significant (Mitchell et al. 1998)
• This study also demonstrated that LEEP had a higher rate of complication (8%) than cryotherapy(2%)
• Although these differences were not statistically significant, the main difference in complications among the procedures was the higher risk of postoperative bleeding with LEEP (3%) versus cryotherapy (0%)











Conclusion
• Compared to other methods of treatment, it is relatively easy to train different cadres of healthcare providers to use cryotherapy (Blumenthal et al.)
• This advantage, combined with its low cost and high efficacy rate, make it appropriate for low-resource settings where only nurses or nurse-midwives are posted.

Cryotherapy treatment and referral
• Women who are VIA test-positive are eligible for cryotherapy treatment if the lesion is not suspicious for cancer, occupies less than 75% of the cervix, does not extend onto the vaginal wall or into the cervical canal beyond the reach of the cryoprobe, and extends less than 2 mm beyond the diameter of the cryotherapyprobe including the tip of the probe
• If any of the above conditions are not met, refer the woman to an appropriate facility where additional diagnostic and treatment methods are possible and medical backup is available.