cronkhite canada syndrome: case report with some features not previously described
TRANSCRIPT

Cronkhite Canada syndrome: case reportwith some features not previouslydescribed
G. Nardone, MDF. D'Armiento, MD
P. Carlomagno, MDG. Budillon, MD
In 1955 Cronkhite and Canada l described a diseasecharacterized by gastrointestinal polyposis, hyperpigmentation of the skin, alopecia, and atrophy of thefingernails and toenails. The clinical picture is commonly characterized by diarrhea, malabsorption withprotein-losing enteropathy, and vomiting. We reporta case of this syndrome that showed several previouslyundescribed features.
CASE REPORT
A 69-year-old woman was admitted to our unit with ahistory of diarrhea and weight loss lasting 1 year. Diarrheaconsisted of 10 to 15 bowel movements per day withouteither blood or mucus. No abdominal pain was present. Herweight had fallen from 100 kg to 70 kg the year prior toexamination. She also noted gradual loss of hair and increasing thinness and brittleness of fingernails and toenails. Onexamination, the patient appeared to be overweight anddehydrated. She presented irregular alopecia and hair fellout upon being touched. There was brown pigmentation onthe back of her hands and in the periorbital region, whilethe fingernails and toenails were atrophied with onychodystrophy. The remainder of the physical examination wasunremarkable.
Serum laboratory values were: white blood count 3100,hemoglobin 11 g, hematocrit 29%, and iron 49 /lgjdl. Electrolytes were: sodium 136 mmol/liter, and potassium 2.4mmol/liter. Total proteins were 6 gjdl and albumin was 2.7gjdl. Gastrin was 1000 pgjml (NV, 20 to 80) and there wasno gastric acid production (MAO, 0); anti-gastric parietalcell antibody test was positive. Fecal microscopy and culturewere negative for pathogens. Liver and kidney function testswere normal. Evaluation of endocrine function was normal.Secretion test of pancreatic function showed normal volumeand bicarbonate output. Double-contrast barium enema andx-rays of the upper gastrointestinal tract revealed multiplefilling defects of the colon and stomach. A small bowelenema did not show any polypoid lesions.
The upper gastrointestinal endoscopy showed about 10(0.5 to 3 cm) sessile polyps in the stomach (Fig. 1); theesophagus and the duodenum were free ofpolyps. The gastricmucosa between polyps was thin and pale, without erosionsor ulcers. Colonoscopy revealed multiple (about 20) sessileand pedunculated polyps distributed throughout the colon.
Histologic analysis of the gastric polyps showed the surface epithelium to be mostly flattened without ulceration
From the Gastroenterology Department, Institute of Pathology, Second School of Medicine, Naples, Italy. Reprint requests: G. Budillon,MD, Universita degli Studi di Napoli, II Facolta di Medicina eChirurgia, Cattedra di Gastroenterologia 2, Via Pansini 5 1-80131,Napoli, Italy.
150
Figure 1. Gastric inflammatory sessile polyp.
Figure 2. Hyperplastic polyp. Note the serrated arrangementof the glandular lining and the predominance of irregular gobletcells and inflammatory infiltration (hematoxylin-eosin; originalmagnification x40).
(Fig. 2). Mucosal glands were tortuous, sometimes cysticallydilated and mucous filled. The vascular channels were engorged. Edema and inflammatory infiltration (lymphocytes,plasmocytes, polymorphonuclear cells) were observed in thelamina propria. Examination of the mucosa between pol~s
showed a picture typical of chronic atrophic gastritis. Microscopic examination revealed numerous gram-negative bacteria in glandular tubules with cytolytic areas (Fig. 3). WithGiemsa stain, the bacterial organisms presented the characteristic undulated appearance of Campylobacter pylori(Fig. 4).
Colon polyps showed irregular glands with columnar epithelial cells and marked inflammatory infiltration. One ofthe polyps contained adenomatous areas. The patient wastreated with intravenous fluid and electrolyte solutions andbroad spectrum antibiotics with improvement. After 3 yearsshe is apparently well, with recurrent bouts of diarrhea wellcontrolled by periodic cycles of non-systemic antibiotics,such as paramomycin or metronidazole. Recently, the endoscopic picture was unchanged despite 3 months of oralglucocorticoids and 10 days of parenteral nutrition.
GASTROINTESTINAL ENDOSCOPY
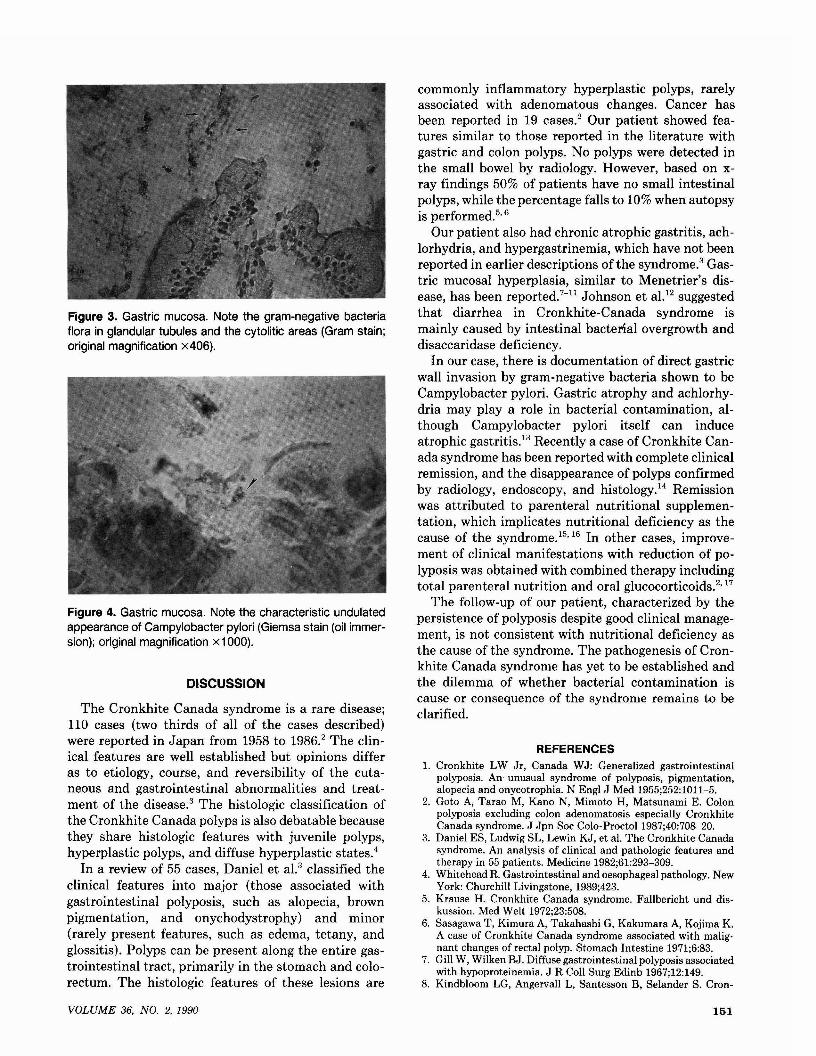
Figure 3. Gastric mucosa. Note the gram-negative bacteriaflora in glandular tubules and the cytolitic areas (Gram stain;original magnification x406).
Figure 4. Gastric mucosa. Note the characteristic undulatedappearance of Campylobacter pylori (Giemsa stain (oil immersion); original magnification x1 000).
DISCUSSION
The Cronkhite Canada syndrome is a rare disease;110 cases (two thirds of all of the cases described)were reported in Japan from 1958 to 1986.2 The clinical features are well established but opinions differas to etiology, course, and reversibility of the cutaneous and gastrointestinal abnormalities and treatment of the disease.3 The histologic classification ofthe Cronkhite Canada polyps is also debatable becausethey share histologic features with juvenile polyps,hyperplastic polyps, and diffuse hyperplastic states.4
In a review of 55 cases, Daniel et al.3 classified theclinical features into major (those associated withgastrointestinal polyposis, such as alopecia, brownpigmentation, and onychodystrophy) and minor(rarely present features, such as edema, tetany, andglossitis). Polyps can be present along the entire gastrointestinal tract, primarily in the stomach and colorectum. The histologic features of these lesions are
VOLUME 36, NO.2, 1990
commonly inflammatory hyperplastic polyps, rarelyassociated with adenomatous changes. Cancer hasbeen reported in 19 cases.2 Our patient showed features similar to those reported in the literature withgastric and colon polyps. No polyps were detected inthe small bowel by radiology. However, based on xray findings 50% of patients have no small intestinalpolyps, while the percentage falls to 10% when autopsyis performed.50 6
Our patient also had chronic atrophic gastritis, achlorhydria, and hypergastrinemia, which have not beenreported in earlier descriptions ofthe syndrome.3Gastric mucosal hyperplasia, similar to Menetrier's disease, has been reported.7-11 Johnson et aI,12 suggestedthat diarrhea in Cronkhite-Canada syndrome ismainly caused by intestinal bacterial overgrowth anddisaccaridase deficiency.
In our case, there is documentation of direct gastricwall invasion by gram-negative bacteria shown to beCampylobacter pylori. Gastric atrophy and achlorhydria may playa role in bacterial contamination, although Campylobacter pylori itself can induceatrophic gastritis.13 Recently a case of Cronkhite Canada syndrome has been reported with complete clinicalremission, and the disappearance of polyps confirmedby radiology, endoscopy, and histology.14 Remissionwas attributed to parenteral nutritional supplementation, which implicates nutritional deficiency as thecause of the syndrome.150 16 In other cases, improvement of clinical manifestations with reduction of polyposis was obtained with combined therapy includingtotal parenteral nutrition and oral glucocorticoids.2017
The follow-up of our patient, characterized by thepersistence of polyposis despite good clinical management, is not consistent with nutritional deficiency asthe cause of the syndrome. The pathogenesis of Cronkhite Canada syndrome has yet to be established andthe dilemma of whether bacterial contamination iscause or consequence of the syndrome remains to beclarified.
REFERENCES1. Cronkhite LW Jr, Canada WJ: Generalized gastrointestinal
polyposis. An unusual syndrome of polyposis, pigmentation,alopecia and onycotrophia. N Engl J Med 1955;252:1011-5.
2. Goto A, Tarao M, Kano N, Mimoto H, Matsunami E. Colonpolyposis excluding colon adenomatosis especially CronkhiteCanada syndrome. J Jpn Soc Colo-ProctoI1987;40:708-20.
3. Daniel ES, Ludwig SL, Lewin KJ, et al. The Cronkhite Canadasyndrome. An analysis of clinical and pathologic features andtherapy in 55 patients. Medicine 1982;61:293-309.
4. Whitehead R. Gastrointestinal and oesophageal pathology. NewYork: Churchill Livingstone, 1989;423.
5. Krause H. Cronkhite Canada syndrome. Fallbericht und diskussion. Med Welt 1972;23:508.
6. Sasagawa T, Kimura A, Takahashi G, Kakumara A, Kojima K.A case of Cronkhite Canada syndrome associated with malignant changes of rectal polyp. Stomach Intestine 1971;6:83.
7. Gill W, Wilken BJ. Diffuse gastrointestinal polyposis associatedwith hypoproteinemia. J R Coll Surg Edinb 1967;12:149.
8. Kindbloom LG, Angervall L, Santesson B, Selander S. Cron-
151

khite Canada syndrome. Cancer 1977;39:2651.9. Martini GA, Dolle W. Menetrier-Syndrom. Polyadenomatosis
des Margens mit Eiweissverlust in den Magen-Darm-Kanal.Dtsch Med Wochenschr 1961;86:2524.
10. Rubin M, Tuthill RJ, Rosato EF, Chen S. Cronkhite Canadasyndrome: report of unusual case. Gastroenterology1980;79:737.
11. Yokoi I, Haschimoto K. An autopsy case of Cronkhite Canadasyndrome with scleroderma. Trans Soc Pathol Jap 1974;63:263.
12. Johnson GK, Soergel K, Hensley GT, Dodds WJ, Hogan WJ.Cronkhite Canada syndrome: gastrointestinal pathophysiologyand morphology. Gastroenterology 1972;63:140.
13. Borody I, Noonan S, Cole P, et al. Triple therapy of C. pylori
Successful endoscopic retrieval of acocaine packet from the stomach
Alex Sherman, MDBarry M. Zingler, MD
The smuggling of cocaine into the United States byingestion of wrapped cocaine packets and gastrointestinal concealment is a common and well-recognizedpractice.I
-5 Three different categories of cocaine pack
ets are recognized.3 Early (type I) cocaine packets wereloosely and haphazardly wrapped, often leading topacket leakage and rupture in the gastrointestinaltract, acute cocaine toxicity, and death. Newer methods of cocaine packet wrapping have been developed,leading to the construction of tighter, multilayeredpackets (types II and II!), relatively resistant to breakage or leaching.
The amount of cocaine in each packet usually exceeds the recognized lethal dose of cocaine; thus,breakage of even one packet can lead to death.6 Controversy regarding the appropriate management of the"body-packer" syndrome exists. Some groups favorimmediate surgical intervention,? whereas others emphasize the relative safety of conservative management.4
To our knowledge, only one case of attempted endoscopic removal of a cocaine packet has been described.8 We report the first successful endoscopicremoval of a cocaine packet from the gastrointestinaltract.
CASE REPORTA 39-year-old Colombian man was brought to the Bellevue
Hospital Center Emergency Room by the New York CityPolice Department after being arrested in a hotel room forcocaine possession.
The patient stated that 2 days prior to admission he waspaid an undisclosed sum of money to transport 80 packets
From the Department of Medicine, New York University School ofMedicine, New York, New York. Reprint requests: Alex Sherman,MD, 614 Second Avenue, Suite B, New York, New York 10016.
152
can reverse hypochlorhydria. AGA 1989;1:589.14. Russel D, Bhathal PS, James D. Complete remission in Cron
khite Canada syndrome. Gastroenterology 1983;85:180-5.15. Takamata J, Okubo K, Komeda T, et al. Generalized gastroin
testinal polyposis associated with ectodermal changes and protein-losing enteropathy with a dramatic response to prednisolone. Digestion 1972;5:153-61.
16. Miyoshi M, Fujii H, Iwasa N, et al. Two autopsy cases of diffusegastrointestinal polyposis with ectodermal changes: CronkhiteCanada syndrome. Am J Gastroenterol 1975;4:357-64.
17. Saitoh 0, Masaki K, Tatsumi A, et al. Cronkhite Canadasyndrome. Report of two cases. Gastroenterol Endosc1986;28:595-605.
of cocaine from Bogota, Colombia to New York City. Thepatient claimed to have ingested the 80 packets and wasdiscovered in a hotel room after having passed 61 packetsper rectum (Fig. 1). Each packet was tightly wrapped, asshown in Figure 2, and contained approximately 4 g ofcocaine. The innermost lining was one "finger-end" of asurgical latex glove. The next layer was a wrapping of clearcellophane. Three additional finger-end layers were the outermost coverings. Each layer was tied very tightly withdental floss on alternating sides of the packet. The packetshad the characteristics of a type II packet.3 The patientdenied personal use of cocaine. He also denied significantmedical or gastrointestinal illnesses, any previous surgicalhistory, or allergies.
Physical examination revealed a regular tachycardia.Blood pressure was normal. Abdominal examination revealed normal bowel sounds and a soft abdomen withouttenderness or masses. Two packets of cocaine could be felton digital rectal examination. Stool was without evidence ofoccult blood.
Laboratory evaluation revealed normal blood counts,serum electrolytes, and coagulation studies. Urine toxicology
Figure 1. A photograph showing the 61 packets of cocainepassed spontaneously per rectum by the patient.
GASTROINTESTINAL ENDOSCOPY