critical updates in the management of chronic heart failure - critical updates in... ·...
TRANSCRIPT

Critical Updates in the Management of Chronic Heart Failure
Antoine T. Jenkins, PharmD., BCPS
Clinical Associate Professor
Chicago State University---College of Pharmacy
Internal Medicine Clinical Pharmacist
Norwegian American Hospital

Learning Objectives
• Differentiate between heart failure with reduced ejection fraction (HFrEF) and heart failure with preserved ejection fraction (HFpEF).
• Compare and contrast therapeutic recommendations from nationally published guidelines on chronic heart failure (HF) management.
• Discuss newer therapies specifically indicated for chronic heart failure treatment and their potential role in practice.
• Illustrate the role of the pharmacist in providing appropriate care in the outpatient setting.
At the conclusion of this program, the pharmacist will be able to:

Meet Mr. Johnson
Mr. Johnson is a 65 year old African-American male who presents to family medicine clinic for follow-up from hospitalization about 7 days ago; he was recently diagnosed with new onset heart failure.
PMH: HTN X 30 yrs, DM X 5 yrs, GERD, mild osteoarthritis, NSTEMI with 2 everolimus stents in the LAD artery about 3 years ago.
Meds: Lisinopril 5 mg daily, famotidine 20 mg daily, metformin 1000mg BID, saxagliptin 2.5 mg daily, naproxen 220mg BID, diltiazem CD 120 mg daily, and atenolol 25 mg daily, furosemide 20 mg daily, aspirin 81 mg daily.
Allergies: NKDA

Mr. Johnson…The Interview
• Vitals
• BP 150/100 mm Hg (repeat: 152/95 mg), HR 85 bpm (repeat: the same), RR 15 bpm, Tmax WNL
• Height
• 75 inches
• Weight
• 130 kg
Pertinent Labs (Fasting)
Glucose 155 mg/dL
BUN 35 mg/dL
SCr 1.0 mg/dL
CrCL > 100 mL/min
Sodium 140 mEq/L
Potassium 4.0 mEq/L
Chloride 99 mg/dL
BNP 280 ng/mL
You are tasked with (1) educating Mr. Johnson on his new diagnosis, and (2) making any evidence-based recommendations regarding his heart failure.

CHF: Quick Facts and Stats
• CHF: The “C” is not what you may think.
• Diagnosis is largely clinical in nature.
• Key statistics:
• By the age of 40 yrs, the lifetime risk of developing HF is 1 in 5.
• Disparities are certainly present.
• There are about 650,000 new cases reported annually.
• Total costs in the US > $40 billion!!!
JAMA. 2009;302:394-400.Arch Intern Med. 2008;168:2138-45.
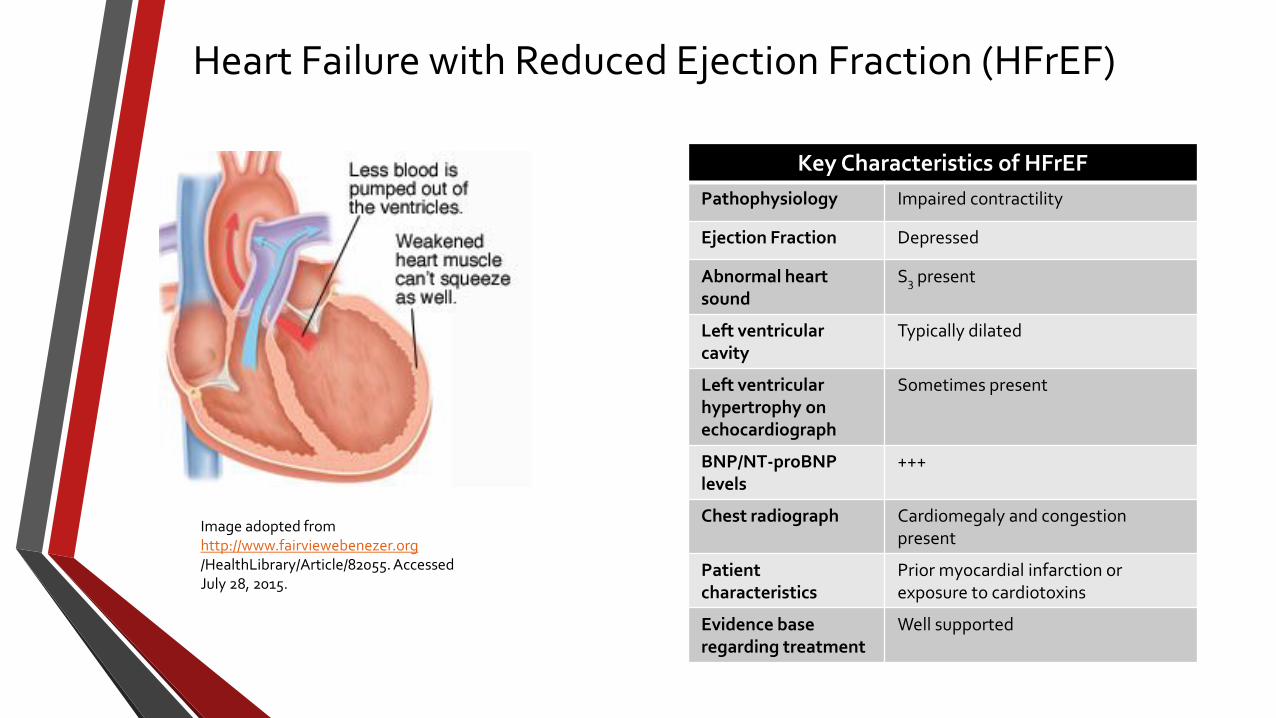
Heart Failure with Reduced Ejection Fraction (HFrEF)
Key Characteristics of HFrEF
Pathophysiology Impaired contractility
Ejection Fraction Depressed
Abnormal heart sound
S3 present
Left ventricularcavity
Typically dilated
Left ventricular hypertrophy onechocardiograph
Sometimes present
BNP/NT-proBNP levels
+++
Chest radiograph Cardiomegaly and congestion present
Patient characteristics
Prior myocardial infarction or exposure to cardiotoxins
Evidence base regarding treatment
Well supported
Image adopted fromhttp://www.fairviewebenezer.org/HealthLibrary/Article/82055. AccessedJuly 28, 2015.

Heart Failure with Preserved Ejection Fraction (HFpEF)
Key Characteristics of HFpEF
Pathophysiology Impaired lusitrophy
Ejection Fraction Normal or near-normal
Abnormal heart sound S4 present
Left ventricular cavity Normal, but left ventricle undergoes hypertrophy
Left ventricular hypertrophy onechocardiograph
Yes
BNP/NT-proBNP levels ++
Chest radiograph Congestion with or without cardiomegaly
Patient characteristics Individuals are typically obese. May have long-standing history of diabetes, hypertension, atrial fibrillation, or coronary artery disease
Evidence base regarding treatment
Poorly supported
Image adopted fromhttp://www.fairviewebenezer.org/HealthLibrary/Article/82055. AccessedJuly 28, 2015.

Mr. Johnson…The Interview
• We know that he was recently diagnosed with chronic HF, but what other key piece of information is needed?

Categories of Chronic HF
Categories of Chronic Heart Failure
Category Ejection Fraction
Determined
Comments
Heart Failure with reduced ejection fraction (HFrEF)
≤ 40% Previously known as “systolic heart failure”. Most studied groups of patients. Therapies known to improve both morbidity and mortality.
Heart Failure with preserved ejection fraction (HFpEF)
≥ 50% Previously known as “diastolic heart failure”. Common form of HF, but no known therapies to improve mortality.
HFpEF borderline 41-49% Considered an intermediate category. These patients are managed the same as those with HFpEF.
HFpEF improved >40% Patients who previously had HFrEF, but have had an improvement in EF. More research necessary on how to best manage these individuals.
Circulation 2013;128:e240-e327.

Mr. Johnson…The Interview
• Before hospitalization: He reported that he would experience SOB from doing regular chores around his home. He likes to garden but hasn’t been able to do so for several weeks. He noticed swelling in his legs that progressively worsened over time. In order for him to sleep, he had to sleep in his recliner chair. Whenever he would lie flat, he mentioned that it felt as if he was drowning.
• In the clinic: He reports that is SOB has improved. While he does experience some limitations in movement when performing chores, it is not as bad as it was prior to hospitalization. He reports that he has started to take walks around the neighborhood, but at this point, he can go a few blocks before feeling winded. Some edema is present in his lower legs…likely 1+. He is concerned that “none of the medications are working.”

Classification of Chronic Heart Failure
New York Functional Class System
Class Description
I No limitations in physical activity
II Mild impairment in activity. Able to comfortably rest.
III Moderate limitation in movements. Symptoms relieved with rest, but less than ordinary activities can provoke symptoms.
IV Inability to perform any activity without marked symptoms. Symptoms occur even during rest
The Criteria Committee for the New York Heart Association.

Classification of Chronic Heart Failure
ACC/AHA Staging System
Stage Description
A Presence of HF risk factors but no structural heart disease or HF symptoms
B Development of structural heart disease, but no HF symptoms
C Structural heart disease in addition to current or prior HF history
D Refractory HF symptoms requiring specialized interventions
Circulation. 2009; 119: e391-479.

Classification of Chronic Heart Failure
ACC/AHA Staging System New York Functional Class System
Stage Description Class Description
A Presence of HF risk factors but no structural heart disease or HF symptoms
None
B Development of structural heart disease, but no HF symptoms I No limitations in physical activity
C Structural heart disease in addition to current orprior HF history
II Mild impairment in activity. Able to comfortably rest.
III Moderate limitation in movements. Symptoms relieved with rest, but less than ordinary activities can provoke symptoms.
IV Inability to perform any activity without marked
symptoms. Symptoms occur even during rest.D Refractory HF symptoms requiring specialized
interventions
The Criteria Committee for the New York Heart Association.Circulation. 2009; 119: e391-479.

Mr. Johnson…The Interview
• Shx—Divorced. Former smoker, quit immediately after his MI. No illicit drug use. Drinks a glass of red wine with dinner 4-5x/week. Meals typically consists of TV dinners and he loves canned foods because “they are easy.” Once per week, he drinks about 1L of “pop” over the course of several days.

General Recommendations
• Patient education
• Sodium restriction
• Fluid restriction
• Exercise/Wellness
• Avoidance of specific drugs

General Recommendations: Patient Education
Recommendations Regarding Patient Education
Publication Commentary
2009 ACC/AHA HF Management Guideline--Focused Update of 2005 guideline
Brief mention of patient education.
2010 HFSA Comprehensive HF Practice Guideline
Dedicated section which details the importance of patient education and self-care. Outlines techniques to best accomplish goals. Encourages team-based approaches.
2013 ACCF/AHA HF Management Guideline
Expanded details regarding the importance of patient education and self care. Explicit recommendation developed--Patients with HF should receive specific education to facilitate HF self-care (Class I, LOE: B).
HOSPITAL CLINICS/COMMUNITY PHARMACIES
Spectrum of Patient Education
Circulation 2009;119;1977-2016.J Card Fail 2010;16:e475-539.Circulation 2013;128:e240-e327.
LOE=Level of Evidence

General Recommendations: Sodium Restriction
Recommendations Regarding Sodium Restriction
Publication Commentary
2009 ACC/AHA HF Management Guideline--Focused Update of 2005 guideline
Moderate restriction is recommended (3-4 gms daily).
2010 HFSA Comprehensive HF Practice Guideline
Dietary sodium restriction (2-3 g daily) is recommended. Further restriction (<2 g daily) may be considered in moderate to severe HF. (SOE=C).
2013 ACCF/AHA HF Management Guideline Sodium restriction is reasonable for patients with symptomatic HF to reduce congestive symptoms. (Class IIa, LOE: C). Clinicians should recommend some degree of restriction (< 3 gms) in stage C or D HF patients.
Circulation 2009;119;1977-2016.J Card Fail 2010;16:e475-539.Circulation 2013;128:e240-e327.
LOE= Level of Evidence, SOE=Strength of Evidence

General Recommendations: Fluid Restriction
Recommendations Regarding Fluid Restriction
Publication Commentary
2009 ACC/AHA HF Management Guideline--Focused Update of 2005 guideline
None
2010 HFSA Comprehensive HF Practice Guideline
Fluid restriction (<2 L/day) is recommended in patients with moderate hyponatremia (serum sodium <130 mEq/L) and should be considered to assist in treatment of fluid overload in other patients.(SOE=C)In patients with severe (serum sodium <125 mEq/L) or worsening hyponatremia, stricter fluid restriction may be considered. (SOE=C).
2013 ACCF/AHA HF Management Guideline Fluid restriction (1.5-2 L/daily) is reasonable in stage D, especially in patients with hyponatremia, to reduce congestive symptoms. (Class IIa, LOE: C).
Circulation 2009;119;1977-2016.J Card Fail 2010;16:e475-539.Circulation. 2013;128:e240-e327.
LOE= Level of Evidence, SOE=Strength of Evidence

General Recommendations: Exercise
Recommendations Regarding Exercising
Publication Commentary
2009 ACC/AHA HF Management Guideline--Focused Update of 2005 guideline
Exercise training is beneficial as an adjunctive approach to improve clinical status in ambulatory patients with current or prior symptoms of HF and reduced LVEF (Class I, LOE: B).
2010 HFSA Comprehensive HF Practice Guideline
Patients with HF undergo exercise testing to determine suitability for exercise training. If deemed safe, exercise training should be considered (while in a supervised setting). If tolerated, patients should increase duration and intensity with a goal of 30 minutes of moderate activity/exercise, 5 days per week with warm up and cool down exercises (SOE: B).
2013 ACCF/AHA HF Management Guideline Exercise training (or regular physical activity) is recommended as safe and effective who are able to participate to improve functional status (Class I, LOE:A).
Circulation 2009;119;1977-2016.J Card Fail 2010;16:e475-539.Circulation. 2013;128:e240-e327.
LOE= Level of Evidence, SOE=Strength of Evidence

General Recommendations: Avoiding Certain Drugs
Recommendations Regarding Drug Induced Heart Failure
Publication Commentary
2009 ACC/AHA HF Management Guideline--Focused Update of 2005 guideline
Drugs known to adversely affect the clinical status ofpatients with current or prior symptoms of HF should be avoided or withdrawn whenever possible (NSAIDs, most antiarrhythmic drugs, and most calcium channel blocking drugs). (Class I, LOE: B).
2010 HFSA Comprehensive HF Practice Guideline
NSAIDs, including cyclooxygenase-2 inhibitors, are not recommended in patients with chronic HF. (SOE:B)
2013 ACCF/AHA HF Management Guideline Drugs known to adversely affect the clinical status of patients with current or prior symptoms of HFrEF are potentially harmful and should be avoided or withdrawn whenever possible (e.g., most antiarrhythmic drugs, most calcium channel blocking drugs (except amlodipine), NSAIDs, or thiazolidinediones) (Class III, LOE: B)
Circulation 2009;119;1977-2016.J Card Fail 2010;16:e475-539.Circulation. 2013;128:e240-e327.
LOE= Level of Evidence, SOE=Strength of Evidence

General Recommendations: Avoiding Certain Drugs
Specific Agents Known to Exacerbate/Cause New-Onset HF
Mechanism Drugs
Retention of Sodium and Water NSAIDsCox II InhibitorsCorticosteroidsThiazolidinediones
Negative Inotropic Effects Calcium channel blockers (verapamil, diltiazem)ItraconazoleMost antiarrhymthic agents (except amiodarone and dofetilide)
Cardiotoxicity AnthracyclinesSunitinibTrastuzumabPaclitaxelIfosfamideExcessive amounts of ethanol
Miscellaneous Biologic response modifiers (infliximab, etanercept)ClozapineIllicit drugs (cocaine, amphetamines)Decongestants (pseudoephedrine, phenylephrine)Saxagliptin
Am J Health-Syst Pharm. 2011; 68:1791-804.
Role of Device Therapies
• Cardiac resynchronization therapy
• AICDs
• Specialized interventions
• LVADs
• Cardiac Transplantation
Circulation 2009;119;1977-2016.J Card Fail 2010;16:e475-539.Circulation. 2013;128:e240-e327.

Knowing what we know that this point…
• What would you recommend for Mr. Johnson regarding the following:
• Patient education?
• Sodium restriction?
• Fluid restriction?
• Exercise/Wellness?
• Avoidance of specific drugs?

Management of Heart Failure with Reduced Ejection Fraction
StageA
Treat per nationally published guidelines:
HypertensionDiabetes
DyslipidemiaIschemic Heart Disease
Obstructive Sleep Apena
Manage conditions that could incite HF exacerbation
Evaluate drug regimen if potential agents are present that can induce
HF
Circulation 2009;119;1977-2016.J Card Fail 2010;16:e475-539.
Circulation 2013;128:e240-e327.

Management of Heart Failure with Reduced Ejection FractionMaintain all stage A recommendations
Acute Coronary SyndromeSecondary Prevention Measures:
If reduced EF—ACEI or ARB + appropriateBB indefinitely
If preserved EF—ACEI or ARB indefinitely, BB X 3 yrs, then reevaulate
Left Ventricular Hypertrophy:Manage blood pressure per nationally
published guidelines
Circulation 2009;119;1977-2016.J Card Fail 2010;16:e475-539.Circulation 2013;128:e240-e327.Circulation 2011;124(22):2458-2473.JAMA 1997;278(3):212-216.Pharmacotherapy 2011;31(1):76-91.
Stage B
Valvular Malfunction:Repair or replacement may be warranted
ACEI=Angiotensin Converting Enzyme InhibitorARB=Angiotensin Receptor BlockerBB= Beta Blocker

Management of Heart Failure with Reduced Ejection Fraction
Stage C*Ensure routine use of Guideline-Directed Medical Therapy
(GDMT)Maintain Stage A and B recommendations
*ACEI or ARBs(Any agent is acceptable)
*BBs(Either metoprolol
succinate, carvedilol bisoprolol)Symptomatic relief from hypervolemia:
Loop Diuretics
Circulation 2009;119;1977-2016. J Card Fail 2010;16:e475-539. Circulation 2013;128:e240-e327.
Other Considerations/Thoughts*Goal should be to attain same target doses of ACEI (or ARBs) or BB used in trials.
*Think about your individual patient when considering GDMT.*Carvedilol CR listed as an option in 2013 guidelines, not the others.

Management of Heart Failure with Reduced Ejection Fraction
StageD
Continue all recommendations from stage A,B, and C
IV inotropic agentscan be administered as a
temporary measure
Cardiac transplantationPlacement of LVAD
Long term IV inotropic administration as a palliative
measure
Circulation 2009;119;1977-2016.J Card Fail 2010;16:e475-539.Circulation 2013;128:e240-e327.
Knowing what we know that this point…
• What would you recommend for Mr. Johnson regarding his HF regimen?

Mr. Johnson Returns…
After about 9 months, Mr. Johnson RTC. He reports that he has been adhering to all recommendations regarding exercising and sodium intake. He even keeps an organized log of physical activities. He no longer uses the naproxen for his mild OA. Additionally, he reports no missed doses of any meds. All of his HF meds currently are at target doses. Despite this news, he still experiences mild SOB and is not able to exercise for a full session without getting winded. He can perform most chores around his home.

Management of Heart Failure with Reduced Ejection Fraction—Stage C
Stage C with persistent symptoms
African-American patients, can consider hydralazine/
isosorbide dinitrate
Dual RAAS blockade
Digoxin
Circulation 2009;119;1977-2016.J Card Fail 2010;16:e475-539.Circulation 2013;128:e240-e327.
RAAS=Renin-Angiotensin-Aldosterone System

Management of Heart Failure with Reduced Ejection Fraction—Stage C
Story Behind Hydralazine/Nitrate Combination
V-HeFT I(Hydr/Nitrate vs. Placebo)
V-HeFT II(Hydr/Nitrate vs. Enalapril)
A-HeFT(Hydr/Nitrate vs. Placebo) N Engl J Med 1986;314:1547-52.
N Engl J Med1991;325:303-10.N Engl J Med 2004;351:2049-57.Hydr=Hydralazine

Management of Heart Failure with Reduced Ejection Fraction—Stage C
A-HeFT Trial1050 self identified black patients with NYHA III-IV and reduced EF
(Mean age 56 yrs, Mean EF 23%)
Hydr/ISDN (2 tabs TID)
+SOC
Placebo +SOC
Primary Endpoint: Composite of all cause death, change in quality of life, and first HF hospital admission
N Engl J Med 2004;351:2049-57.
ISDN=Isosorbide DinitrateSOC=Standard of care
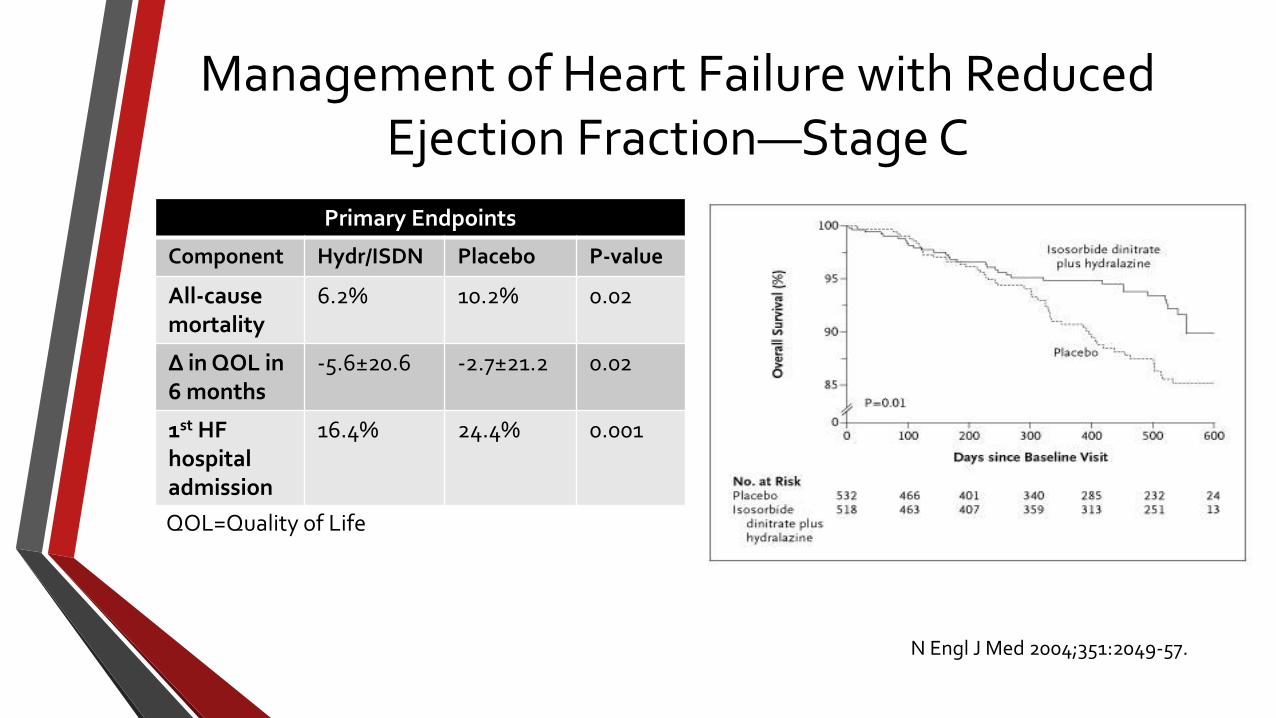
Management of Heart Failure with Reduced Ejection Fraction—Stage C
Primary Endpoints
Component Hydr/ISDN Placebo P-value
All-causemortality
6.2% 10.2% 0.02
∆ in QOL in6 months
-5.6±20.6 -2.7±21.2 0.02
1st HFhospitaladmission
16.4% 24.4% 0.001
N Engl J Med 2004;351:2049-57.
QOL=Quality of Life

Management of Heart Failure with Reduced Ejection Fraction—Stage C
• Considerations for Hydralazine/Isosorbide Dinitrate
• In African-American patients, the combination does not take precedence over ACEI (or ARB)/BB.
• Other ethnic groups
• Pill burden
• Cost

Management of Heart Failure with Reduced Ejection Fraction—Stage C
Dual RAAS Blockade
Standard Therapy +AldosteroneAntagonist
Standard Therapy +ARB

Management of Heart Failure with Reduced Ejection Fraction—Stage C
Landmark Studies Involving Aldosterone Antagonists
Trial Patients Inclusion Criteria Results
RALES(N=1663)
Active Group: Standard therapy + spironolactone 25-50mg/day
Control Group: Standard therapy + placebo
NYHA Class III and IV HF with EF ≤ 35%
All cause mortality: RR 0.70 (95% CI 0.60-0.82); p<0.01. Cardiac death: RR 0.69 (95% CI 0.58-0.82); p<0.001.Hospitalization: RR 0.70 (95% CI 0.59-0.82; p<0.001
EPHESUS(N=6632)
Active Group: Standard therapy + eplerenone 25-50mg/day
Control Group: Standard therapy + placebo
Prior acute MI and EF ≤ 40%
All cause mortality: RR 0.85 (95% CI 0.75-0.96); p<0.008. Cardiac death or hospitalization: RR 0.87 (95% CI 0.79-0.95); p<0.002
N Engl J Med 1999; 341:709-717.N Engl J Med 2003; 348:1309-1321.

Management of Heart Failure with Reduced Ejection Fraction—Stage C
EMPHASIS-HF StudyEplerenone in Mild Patients Hospitalization and Survival
Study in Heart Failure
(Pts ≥ 55 yrs old, EF ≤ 30-35%, NYHA II)
1364 patients received standard treatment
plus eplerenone 25-50 mg/day
1373 patients received standard treatment plus
placebo
Primary Endpoint: Death from CV causes or hospitalization
Secondary Endpoint: Many including hospitalizationfor HF or death from any cause, etc.
N Engl J Med 2011;364:11-21.

Management of Heart Failure with Reduced Ejection Fraction—Stage C
• Primary Outcomes
• CV causes or hospitalization for HF: HR 0.63 (95% CI 0.54-0.74); p<0.001
• All cause mortality: HR 0.76 (95% CI 0.62-0.93); p<0.008
• Secondary Outcomes
• Death from any cause or hospitalization for HF: HR 0.65 (95% CI 0.55–0.76); p<0.001
N Engl J Med 2011;364: 11-21.

Management of Heart Failure with Reduced Ejection Fraction—Stage C
Recommendations Regarding Aldosterone Antagonists
Publication Commentary
2009 ACC/AHA HF Management Guideline--Focused Update of 2005 guidelines
Addition of an aldosterone antagonist is recommended in selected patients with moderately severe to severe symptoms of HF and reduced LVEF who can be carefully monitored for preserved renal function and normal potassium concentration. Required labs: SCr ≤ 2.5 mg/dL in men or ≤ 2.0 mg/dL in women and potassium <5.0 mEq/L. Under circumstances where monitoring for hyperkalemia or renal dysfunction is not anticipated to be feasible, the risks of therapy may outweigh the benefits (Class I, LOE: B).
2010 HFSA ComprehensiveHF Practice Guideline
Administration of an aldosterone antagonist is recommended for patients with NYHA class IV (or class III, previously class IV) HF from reduced LVEF (<35%) while receiving standard therapy, including diuretics. (SOE=A).
2013 ACCF/AHA HF Management Guideline
Aldosterone antagonists are recommended in patients with NYHA class II-IV and who have EF of 35% ≤, unless contraindicated, to reduce morbidity and mortality. Patients with NYHA class II should have a history of prior cardiovascular hospitalization or elevated plasma natriuretic peptide levels to be considered for aldosterone antagonists. (Class I, LOE:A).
Circulation 2009;119;1977-2016.J Card Fail 2010;16:e475-539.Circulation 2013;128:e240-e327.
LOE=Level of Evidence SOE=Strength of Evidence

Management of Heart Failure with Reduced Ejection Fraction—Stage C
Recommendations Regarding the Addition of ARBs
Publication Commentary
2009 ACC/AHA HF Management Guideline--Focused Update of 2005 guidelines
The addition of an ARB may be considered inpersistently symptomatic patients with reduced LVEFwho are already being treated with conventionaltherapy. (Class IIB, LOE: B)
2010 HFSA ComprehensiveHF Practice Guideline
The addition of an ARB should be considered in patientswith HF due to reduced LVEF who have persistentsymptoms or progressive worsening despite optimized therapy with an ACE inhibitor and beta blocker. (SOE=A).
2013 ACCF/AHA HF Management Guideline
Addition of an ARB may be considered in persistently symptomatic patients with HFrEF who are already being treated with an ACE inhibitor and a beta blocker in whom an aldosterone antagonist is not indicated or tolerated (Class IIB, LOE:A).
Circulation 2009;119;1977-2016.J Card Fail 2010;16:e475-539.Circulation 2013;128:e240-e327.
LOE=Level of Evidence SOE=Strength of Evidence

Management of Heart Failure with Reduced Ejection Fraction—Stage C
• Digoxin
• Recommendations remain consistent across guidelines.
• Does not improve mortality, but can reduce hospitalization rates.
• Other considerations:
• Can be added to symptomatic patients with GDMT or its addition can be delayed.
• Useful for patients with concomitant atrial fibrillation.
• Doses should not exceed 250 mcg daily.
• Be cognizant of drug-drug interactions.
Circulation 2009;119;1977-2016.J Card Fail 2010;16:e475-539.Circulation 2013;128:e240-e327.

Management of Heart Failure with Reduced Ejection Fraction—Stage C
Recommendations Regarding Adjunctive Use of Dyslipidemic Agents
Publication Statins Omega 3 Fatty Acids (O3FAs)
2009 ACC/AHA HF Management Guideline--Focused Update of 2005 guidelines
None None
2010 HFSA Comprehensive HF Practice Guideline
There is no indication to use statins specifically for the treatment of HF, but statins are indicated to treat hyperlipidemia in HF patients.
None
2013 ACCF/AHA HF Management Guideline
Not beneficial as adjunctive therapy when prescribed solely for the diagnosis of HF in the absence of other indications for their use (Class III, LOE: A)
Reasonable to use as adjunctivetherapy in patients with NYHA class II-IV symptoms and HFrEF or HFpEF, unless contraindicated, to reduce mortality and cardiovascular hospitalizations (Class IIa, LOE: B)
Circulation 2009;119;1977-2016. J Card Fail 2010;16:e475-539. Circulation 2013;128:e240-e327.

Management of Heart Failure with Reduced Ejection Fraction—Stage C
GISSI Prevenzione trial--Patients s/p MI
21% reduction in death in those taking 1 gm O3FA (850-882 mg EPA/DHA) vs. placebo
GISSI Prevenzione trial---2,000 patients in treatment group had
reduced EF
Post hoc analysis
GISSI HF trial--6,975 Patients NYHA Class II-IV HF
Reductions in all cause death, CV death and hospitalizations in those taking 1 gm O3FA (850-882 mg EPA/DHA) vs. placebo
Eur J Heart Fail. 2005;7:904-9.Lancet. 2008;372:1223-30.J Am Coll Cardiol. 2009;54:585-94.Lancet. 1999;354:447-55.

Knowing what we know that this point…
• What would you recommend for Mr. Johnson regarding his HF regimen:
• Add digoxin?
• Add hydralazine/isosobide dinitrate?
• Add spironolactone?
• Add candesartan?

Management of Heart Failure with Preserved Ejection Fraction
• Overall treatment principles
• Maintain adequate blood pressure
• Reduce tachycardia
• Maintain euvolemia
• Treat and prevent myocardial ischemia
Circulation 2009;119;1977-2016.J Card Fail 2010;16:e475-539.Circulation 2013;128:e240-e327.

Management of Heart Failure with Preserved Ejection Fraction
• Key caveats to consider with managing blood pressure in these patients:
• No restrictions on which BB to use.
• Broader array of calcium channel blockers can be used.
• While ACEIs/ARBs may be used to manage blood pressure, data have demonstrated a small reduction in HF hospitalizations with the use of ARBs in a population of patients with HFpEF.
• Loop diuretics should be used carefully.
Circulation 2009;119;1977-2016.J Card Fail 2010;16:e475-539.Circulation 2013;128:e240-e327.

Newer Agents for Managing Chronic Heart Failure
• Ivabradine (Corlanor®)
• Hyperpolarization-activated cyclic nucleotide-gated channel blocker.
• Slows down heart rate by inhibition of the If current.
• Indicated for persistently symptomatic HF patients with resting pulse ≥ 70 bpm.
• Patient-specific criteria for use include:
• Reduced EF (≤ 35%)
• Stable disease with continued symptoms
• Sinus rhythm
• Max tolerated dose of BBs/contraindication for BB therapy.
http://hyperphysics.phy-astr.gsu.edu/hbase/biology/sanode.html. AccessedAug 3, 2015.

Newer Agents for Managing Chronic Heart Failure (Ivabradine)
• 6,000 patients with EF ≤ 35%, initial HR > 70 bpm, prior HF admission.
• All received standard therapies.
• Ivabradine groups had 2% reduction in all-cause readmissions (1,231 readmissions), compared to placebo (1,356 hospitalizations); p=0.003.
SHIFT(Systolic heart failure treatment with the
If inhibitor ivabradineTrial)
• 10,917 stable CAD patients with EF ≤40%, initial HR ≥ 60 bpm, with a prior HF hospital admission.
• All received standard therapies.
• HR ↓ in the ivabradine group compared to placebo, there was no difference in the primary outcomes (composite of CV death, hospitalization for MI or HF).
• Patients with HR > 70 bpm demonstrated no difference in primary outcomes, but differences were detected in secondary endpoints (admission due to MI or revascularization).
BEAUTIFUL(morBidity-mortality EvAlUaTion of the If inhibitor ivabradine in patients with coronary disease and left-ventricULar dysfunction)
Lancet 2010; 376: 875–85.Lancet 2008; 372: 807–16.

Newer Agents for Managing Chronic Heart Failure (Ivabradine)
Ivabradine (Corlanor®) Indication Reduce the risk of hospitalization of HF in patients with stable, persistently
symptomatic chronic disease.
Patient-specific criteria for usage
See prior slide
Dose 5 mg PO BID, then titrate to 7.5 mg PO BID if HR still > 60 bpm, or down titrate to 2.5 mg PO BID if HR < 50 bpm.
Contraindications Initial HR < 60 bpm prior to treatment, ADHF, BP < 90/50 mm Hg, patients who are dependent on a pacemaker (HR maintained exclusively by pacemaker), significant bradyarrhythmias, concomitant use of strong CPY 3A4 inhibitors.
Disease State considerations
Atrial fibrillation, ventricular dyssynchrony, 1st or 2nd degree heart block
Drug-drug interactions Strong CPY 3A4 inhibitors---AVOID
Adverse Effects Atrial fibrillation, development of phosphenes
https://www.corlanor.com/?WT.srch=1. Accessed Aug 4, 2015.
ADHF=Acute decompensated heart failure

Newer Agents for Managing Chronic Heart Failure
RAAS
Natriuretic Peptide System
Angiotensinogen Angiotensin I Angiotensin II
Aldosterone
Bradykinin
Adrenomedullin
Vasoconstriction
Natriuretic Peptides(B-type natriuretic peptide)
Inactive Fragments
Vasodilation
Neprilysin
Angiotensin-Neprilysin Inhibition

Newer Agents for Managing Chronic Heart Failure (Sacubitril/Valsartan)
PARADIGM-HF8442 patients with NYHA class II-IV disease with an EF ≤ 40%, either a BNP > 150 pg/mL
or prior HF hospitalization within past yr(Mean age 64 yrs, 71% of patients had NYHA II HF)
Sacubitril/Valsartan 200 mg BID + SOC
Enalapril 20 mg BID + SOC
Primary endpoints—Composite of death for CV causes or HF hospital admissionSecondary endpoints—Change in QOL scores from baseline to 8 months, time to reduction in renal
function, and time to new onset atrial fibrillation.
N Engl J Med 2014; 371:993-1004.SOC=Standard of careQOL=Quality of life

Newer Agents for Managing Chronic Heart Failure (Sacubitril/Valsartan)
N Engl J Med 2014; 371:993-1004.

Newer Agents for Managing Chronic Heart Failure(Sacubitril/Valsartan)
Sacubitril/Valsartan (Entresto™)Indication Reduce the risk of CV death and HF hospitalization in patients with heart failure
with reduced ejection fraction.
Patient-specific criteria for usage
If on an ACEI, it must be discontinued 36 hours prior to the initiation.
Dose 49/51 mg PO BID. Titrate after 7-14 days to target dose of 97/103 mg PO BID. Dose adjust in both renal/hepatic impairment.
Contraindications Concomitant use of ACEI, history of angioedema with ACEI or ARB, concomitant use with aliskiren in diabetic patients.
Drug-drug interactions Potassium-sparing diuretics, potassium supplements
Adverse Effects Cough, hypotension, angioedema
.
https://quo.novartis.com/entresto/index?site=SC016639, Accessed Aug 4, 2015.

Something to Think About
• Could Mr. Johnson be a candidate for…
• Ivabradine?
• Sacubitril/Valsartan?

Role of The Outpatient Pharmacist
• VITAL!!!!!!
• Remember the essential non-pharmacological measures.
• Patient education!!
• Dietary needs
• Daily weights
• Ensure mortality-saving agents are on board.
• Remain cognizant of drug-induced causes.
• Recommend other key therapies to manage other HF associated disease states (if necessary).
• Provide immunizations.

Other Recommendations for Mr. Johnson
• Any other needed interventions for Mr. Johnson?

Conclusions
• Chronic HF continues to be a common medical issue suffered by many.
• Nonpharmacological and pharmacotherapy are both key in improving QOL and extending life!
• Our role is instrumental in ensuring reduction in hospitalizations and improving mortality.

Critical Updates in the Management of Chronic Heart Failure
Antoine T. Jenkins, PharmD., BCPS
Clinical Associate Professor
Chicago State University---College of Pharmacy
Internal Medicine Clinical Pharmacist
Norwegian American Hospital