creating adoptable & sustainable...
TRANSCRIPT
Creating Adoptable & Sustainable ImprovementChris Hayes, MD, Chief Medical Information Officer, St. Joseph’s Healthcare Hamilton
Frank Federico, Vice President, Senior Expert, Patient Safety, IHI
December 4, 2016
IHI National Forum
Presenters have nothing to disclose
Objectives
Analyze why some QI strategies lead to more sustained
improvement
Utilize tools to develop more sustainably adoptable improvement
strategies
Use exercises learned in this session to engage others in their
organization in initiatives to create sustainable improvement
Agenda
1:00-1:10 Session introduction
1:10-1:25 Why do some improvement initiatives fail?
1:25-2:05 Exercise #1 – To Fail or Not to Fail
2:05-2:30 Highly Adoptable Improvement
2:30-3:00 Break
3:00-3:30 Exercise #2 – Assessing adoptability
3:30-4:15 Exercise #3 – Assessing and addressing workload
4:15-4:30 Open discussion and closing remarks
Why Do Some Improvement Efforts Fail
Poor implementation planning and overly aggressive timelines
Failing to create buy-in/ownership of the initiative
Ineffective leadership and lack of trust in upper management
Failing to create a realistic plan or improvement process
Ineffective and top-down communications
A weak case for change, unclear focus, and unclear desired outcomes
Little or no teamwork or cooperation
Failing to provide ongoing measurement, feedback, and accountability
Unclear roles, goals, and performance expectations
Lack of time, resources, and upper-management support
http://au621leadershipvsmanagement.weebly.com/uploads/5/4/6/9/54693805/why_hospital_improvement_efforts_fail.pdf

Why Do Some Improvement Efforts Fail
We do not get to the root of the problem
We fail to engage those that do the work
We do not understand human factors and engineer systems to
deal with the human condition
We do not simplify
– We add steps to the processes that result in increased complexity
We do not consider a system approach
Change Concepts
Simplification
– Are there Steps in your processes that can be eliminated?
Standardization
– Best known process to achieve desired results
– But known today-may change with new knowledge or new context
8

9

Bonacum, KP
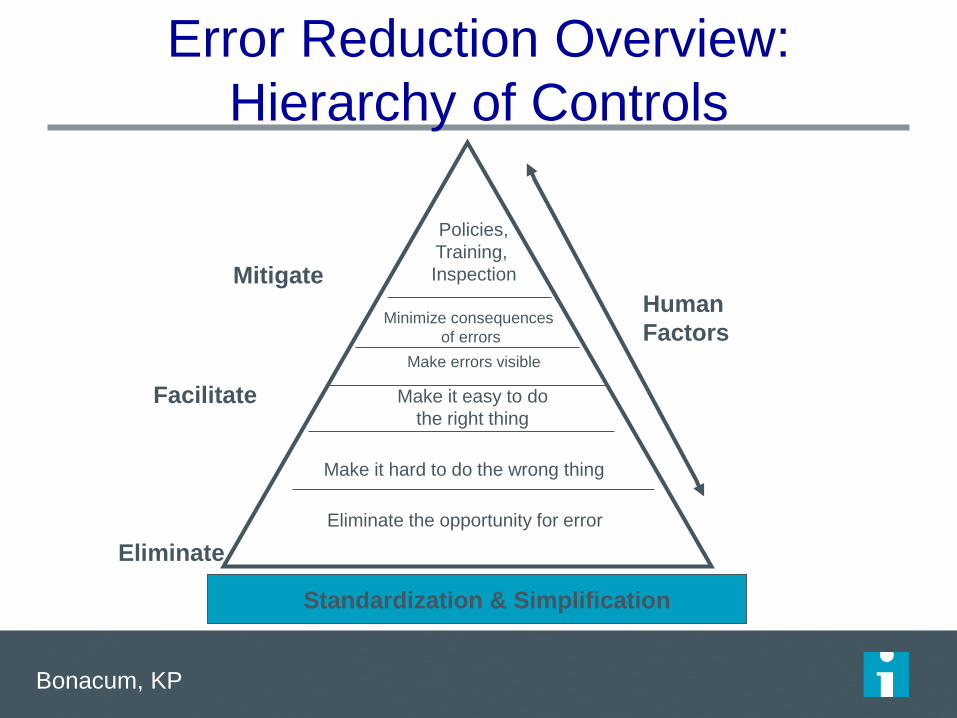
Error Reduction Overview:
Hierarchy of Controls
Standardization & Simplification
Policies,
Training,
Inspection
Minimize consequences
of errors
Make it easy to do
the right thing
Make it hard to do the wrong thing
Eliminate the opportunity for error
Human
Factors
Mitigate
Facilitate
Eliminate
Make errors visible
Five Main Factors That Influence Adoption of
an Innovation
Relative Advantage - The degree to which an innovation is
seen as better than the idea, program, or product it
replaces.
Compatibility - How consistent the innovation is with the
values, experiences, and needs of the potential adopters.
Complexity - How difficult the innovation is to understand
and/or use.
Triability - The extent to which the innovation can be tested
or experimented with before a commitment to adopt is
made.
Observability - The extent to which the innovation provides
tangible results.
To Fail or Not to Fail…that is your task
Exercise #1
– Work with the people at your table to design a QI project
– Groups A – you will work to design for high adoptability and success of
the QI intervention
– Groups B – you will work to design for low adoptability and failure of the
QI intervention
– Your QI task is – design falls prevention intervention(s) to reduce the falls
rate of admitted patients/ residents over age of 65. List attributes of the
design on flipchart paper
To Fail or Not to Fail…that is your task
For each group – underline the strategies that are similar to your
existing falls prevention strategy (be honest)
Report back
– What are the main features of your design plan?
– What are the key differences between the groups plans?

HIGHLY
ADOPTABLE
IMPROVEMENT
A model and tool to address workload-
capacity balance and perceived value
amongst quality improvement projects
15
Have you ever experienced this?
• We don’t have time for this
• Too much change happening
• We don't understand why we have to do this
• This doesn’t make sense
• This doesn’t match our workflow
OR
• Works for a while but not sustained
• Need to implement reminders
• Provide compliance data on unit’s/ areas performance
16

In an effort to Improve healthcare
are we making it Harder to provide care
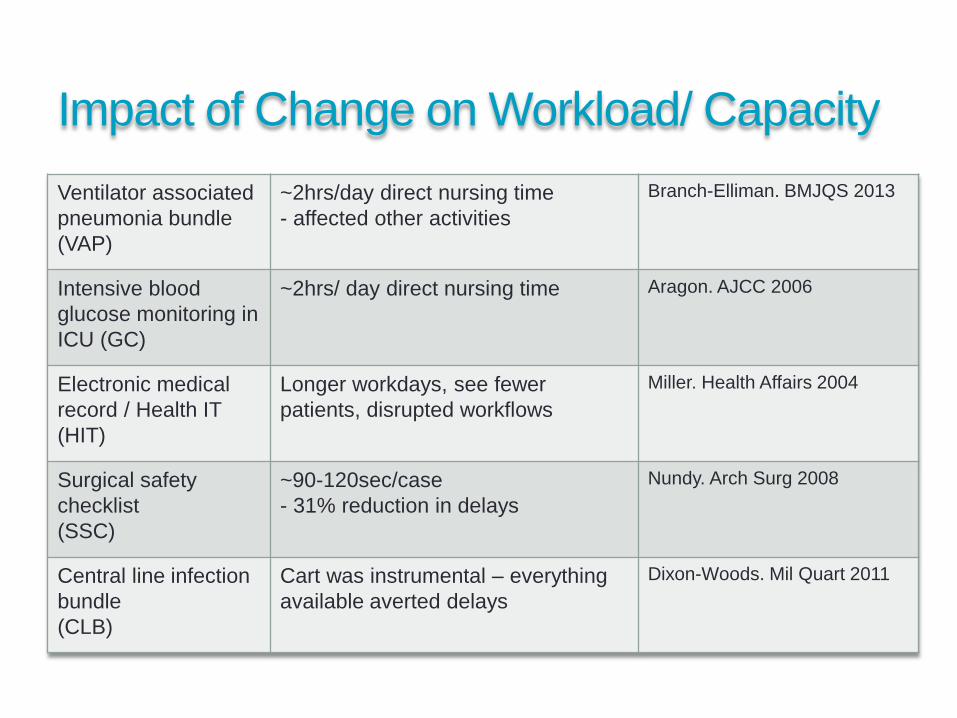
Impact of Change on Workload/ Capacity
Ventilator associated
pneumonia bundle
(VAP)
~2hrs/day direct nursing time
- affected other activities
Branch-Elliman. BMJQS 2013
Intensive blood
glucose monitoring in
ICU (GC)
~2hrs/ day direct nursing time Aragon. AJCC 2006
Electronic medical
record / Health IT
(HIT)
Longer workdays, see fewer
patients, disrupted workflows
Miller. Health Affairs 2004
Surgical safety
checklist
(SSC)
~90-120sec/case
- 31% reduction in delays
Nundy. Arch Surg 2008
Central line infection
bundle
(CLB)
Cart was instrumental – everything
available averted delays
Dixon-Woods. Mil Quart 2011
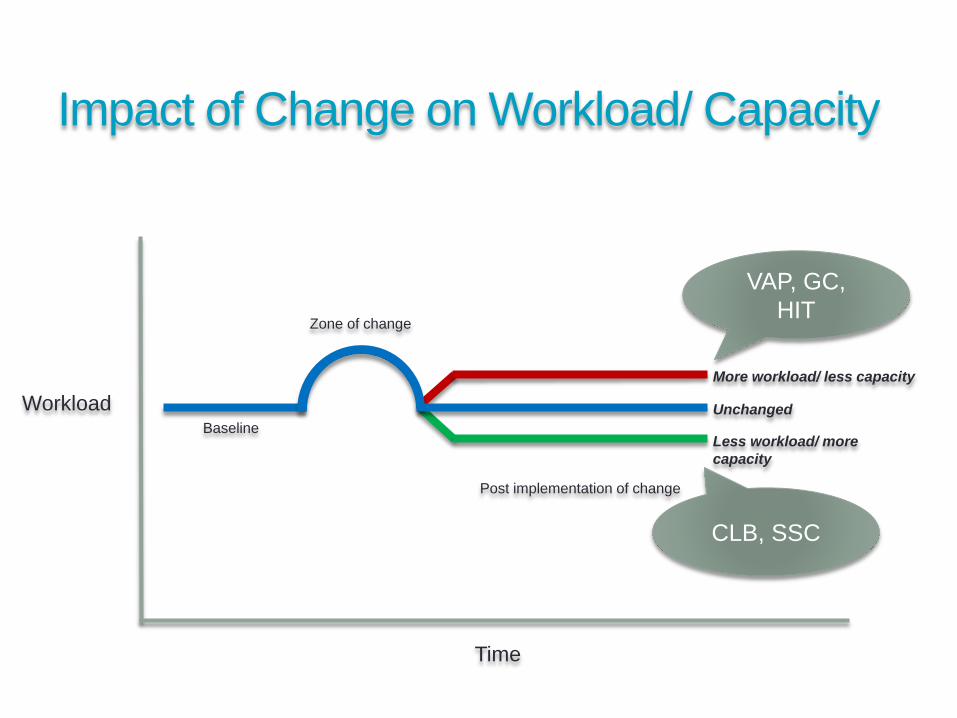
Impact of Change on Workload/ Capacity
Workload
Time
Baseline
Zone of change
Post implementation of change
Unchanged
More workload/ less capacity
Less workload/ more
capacity
VAP, GC,
HIT
CLB, SSC
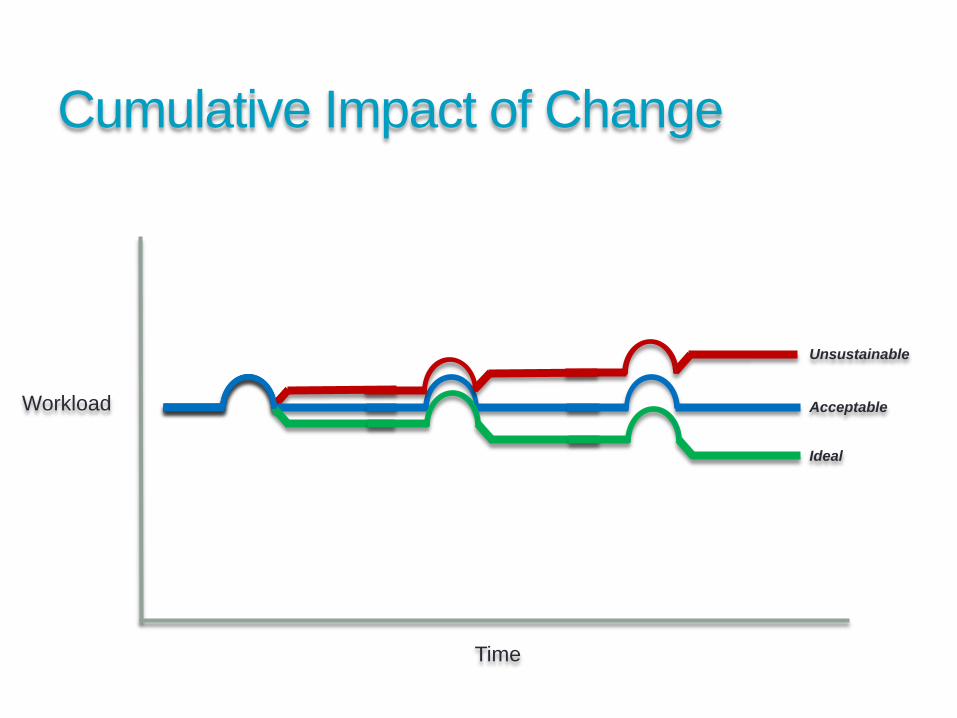
Cumulative Impact of Change
Time
Workload
Unsustainable
Acceptable
Ideal
Impact of Change on Perceived Value
• People are not passive recipients of change; they evaluate,
seek meaning and develop feeling towards change
• Perceived Valuethe willingness or readiness of individuals to adopt change when they believe
the outcome of the change will be of value to them (or things of importance to
them.)
• Emotional = That will save lives!
• Practical = I can see myself doing that new practice
• Logical = That new process makes sense
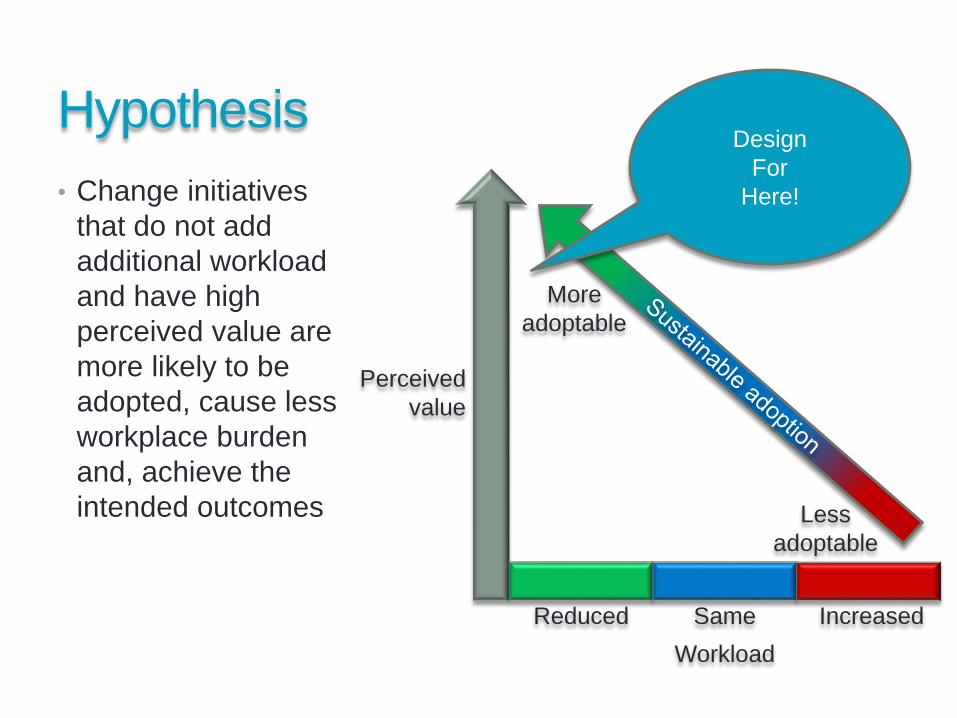
Hypothesis
• Change initiatives
that do not add
additional workload
and have high
perceived value are
more likely to be
adopted, cause less
workplace burden
and, achieve the
intended outcomes
More
adoptable
Less
adoptable
Perceived
value
Workload
SameReduced Increased
24
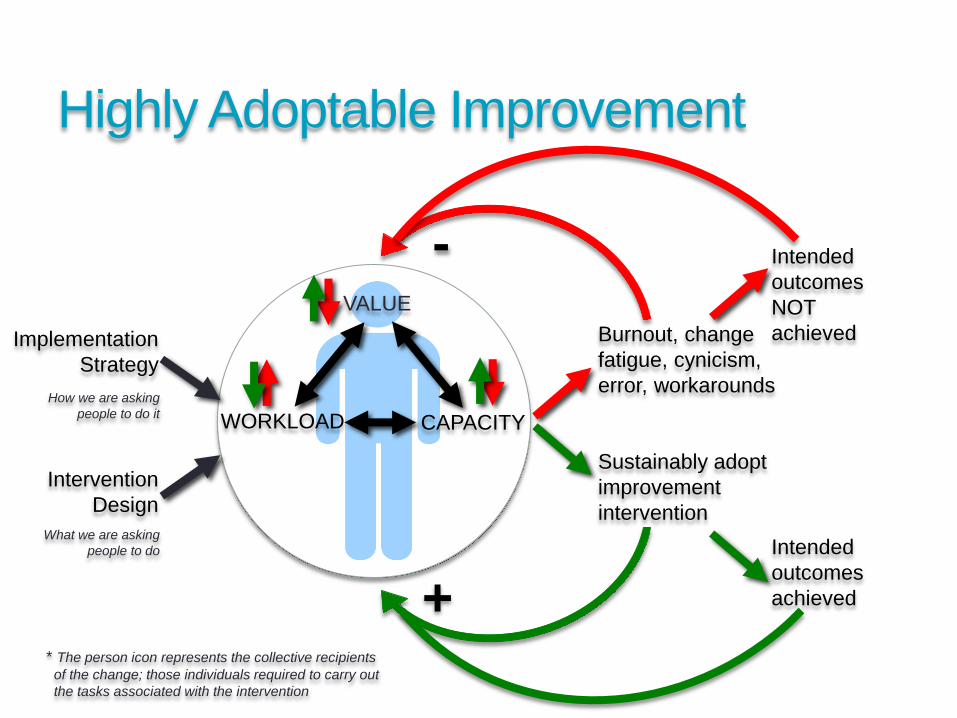
Design
For
Here!
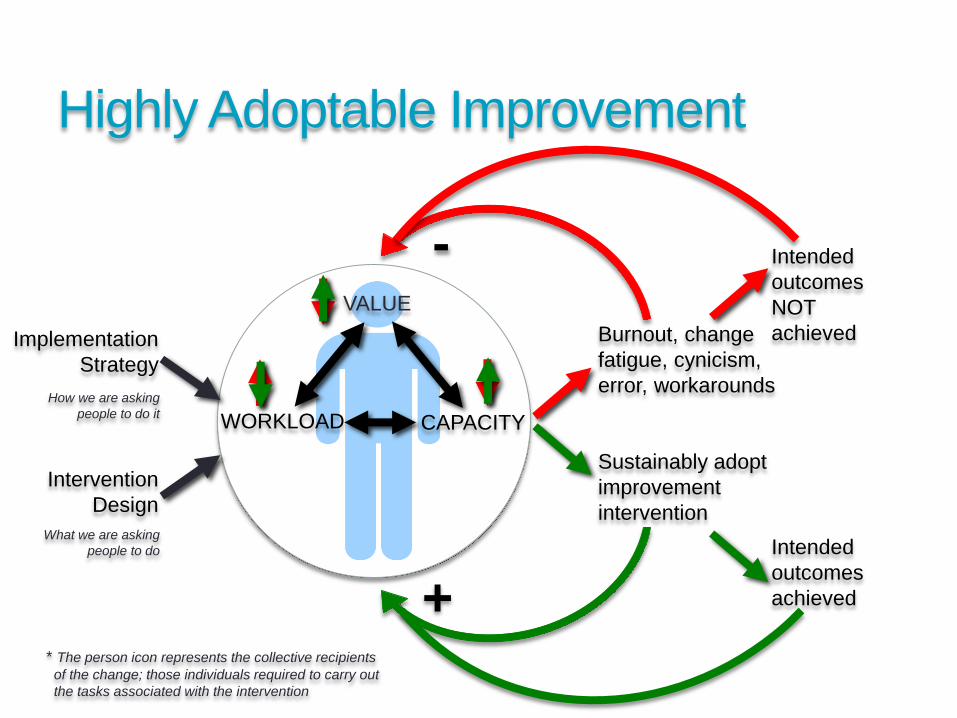
Intervention
Design
Burnout, change
fatigue, cynicism,
error, workarounds
Implementation
Strategy
Sustainably adopt
improvement
intervention
-
+
WORKLOAD
VALUE
CAPACITY
Intended
outcomes
NOT
achieved
Intended
outcomes
achieved
Highly Adoptable Improvement
* The person icon represents the collective recipients
of the change; those individuals required to carry out
the tasks associated with the intervention
How we are asking
people to do it
What we are asking
people to do
Now for a Highly Needed Break!
Please be back for 3:00!!
Intervention
Design
Burnout, change
fatigue, cynicism,
error, workarounds
Implementation
Strategy
Sustainably adopt
improvement
intervention
-
+
WORKLOAD
VALUE
CAPACITY
Intended
outcomes
NOT
achieved
Intended
outcomes
achieved
Highly Adoptable Improvement
* The person icon represents the collective recipients
of the change; those individuals required to carry out
the tasks associated with the intervention
How we are asking
people to do it
What we are asking
people to do
How do you assess adoptability?
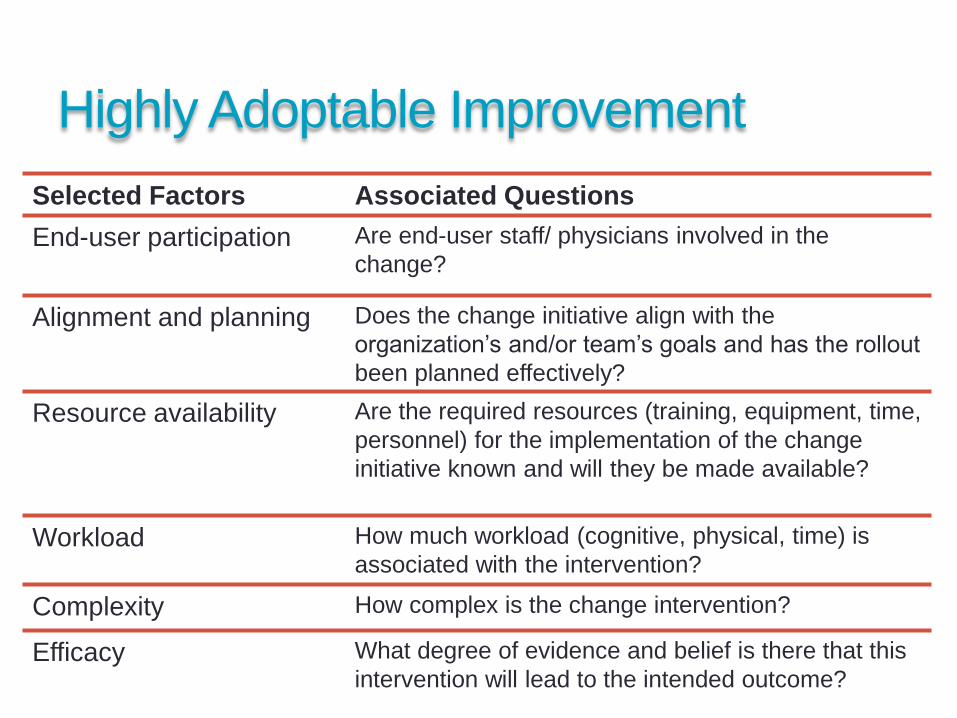
Highly Adoptable Improvement
29
Selected Factors Associated Questions
End-user participation Are end-user staff/ physicians involved in the
change?
Alignment and planning Does the change initiative align with the
organization’s and/or team’s goals and has the rollout
been planned effectively?
Resource availability Are the required resources (training, equipment, time,
personnel) for the implementation of the change
initiative known and will they be made available?
Workload How much workload (cognitive, physical, time) is
associated with the intervention?
Complexity How complex is the change intervention?
Efficacy What degree of evidence and belief is there that this
intervention will lead to the intended outcome?
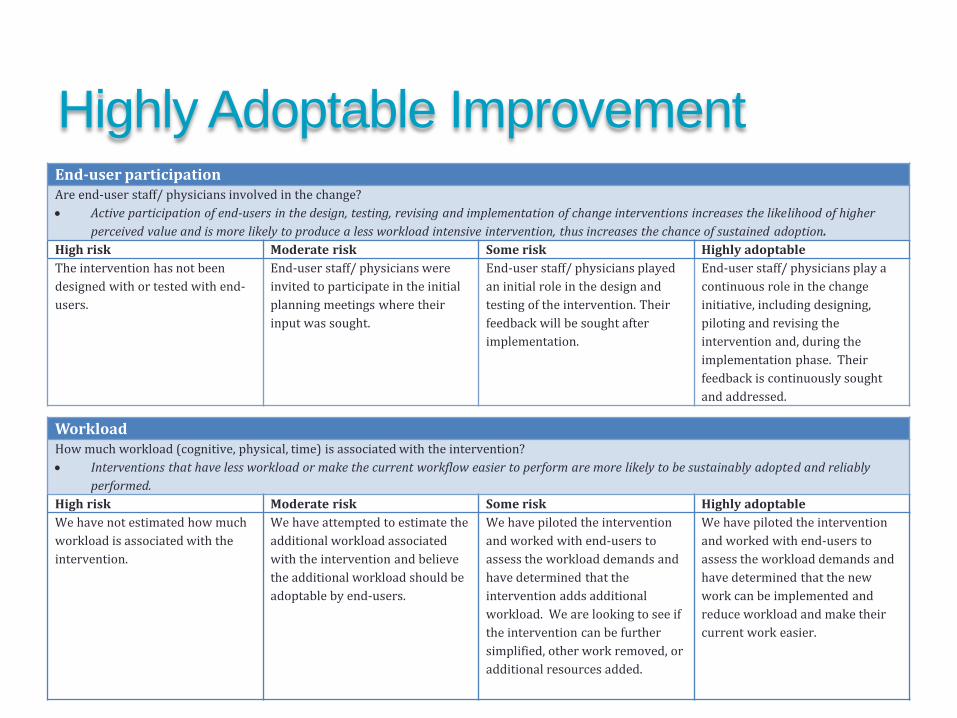
End-user participationAre end-user staff/ physicians involved in the change?
Active participation of end-users in the design, testing, revising and implementation of change interventions increases the likelihood of higher
perceived value and is more likely to produce a less workload intensive intervention, thus increases the chance of sustained adoption.
High risk Moderate risk Some risk Highly adoptable
The intervention has not been
designed with or tested with end-
users.
End-user staff/ physicians were
invited to participate in the initial
planning meetings where their
input was sought.
End-user staff/ physicians played
an initial role in the design and
testing of the intervention. Their
feedback will be sought after
implementation.
End-user staff/ physicians play a
continuous role in the change
initiative, including designing,
piloting and revising the
intervention and, during the
implementation phase. Their
feedback is continuously sought
and addressed.
30
WorkloadHow much workload (cognitive, physical, time) is associated with the intervention?
Interventions that have less workload or make the current workflow easier to perform are more likely to be sustainably adopted and reliably
performed.
High risk Moderate risk Some risk Highly adoptable
We have not estimated how much
workload is associated with the
intervention.
We have attempted to estimate the
additional workload associated
with the intervention and believe
the additional workload should be
adoptable by end-users.
We have piloted the intervention
and worked with end-users to
assess the workload demands and
have determined that the
intervention adds additional
workload. We are looking to see if
the intervention can be further
simplified, other work removed, or
additional resources added.
We have piloted the intervention
and worked with end-users to
assess the workload demands and
have determined that the new
work can be implemented and
reduce workload and make their
current work easier.
Highly Adoptable Improvement
How did your strategies fair?
• Exercise 2
• Look back at your fall prevention strategies.
• Using the Highly Adoptable Improvement Assessment Guide review
each set of statements
• Mark an X in the column that best matches to the strategy you used
in your falls prevention plan.
How does this relate to your work?
• Discuss with members of your table current or past QI
projects/ initiatives.
• For those that were a success discuss some of the
strategies you felt led to success
• Discuss the same for projects that were less successful or
weren’t sustained
• Would the Assessment Guide have helped at the onset and
during the project/ initiative?
How do you
Assess & Addressworkload?
Highly Adoptable Improvement34
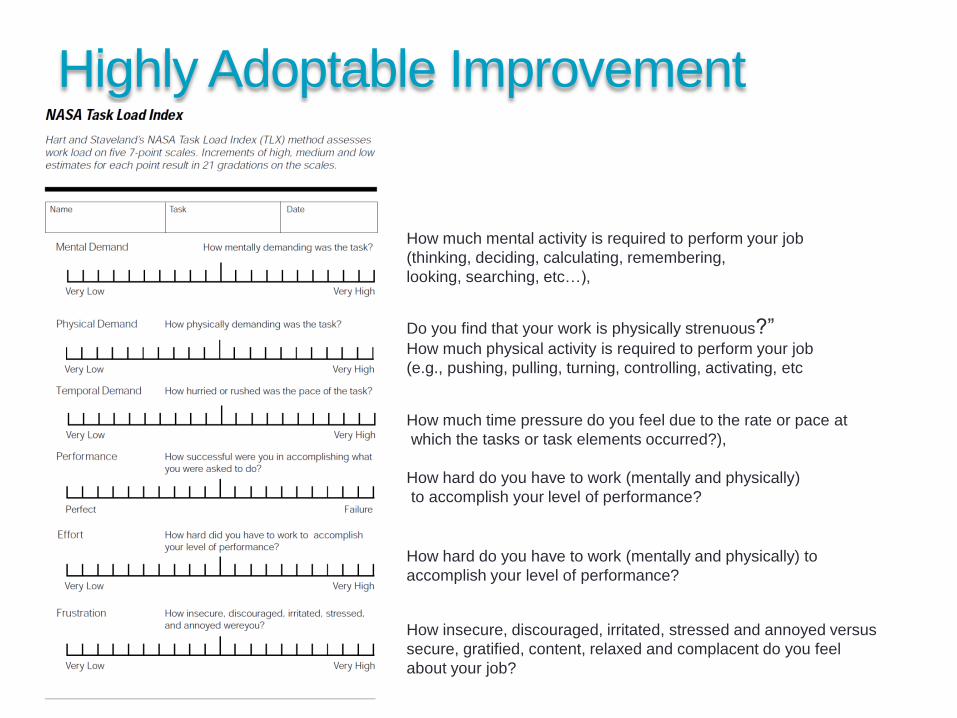
Do you find that your work is physically strenuous?” How much physical activity is required to perform your job
(e.g., pushing, pulling, turning, controlling, activating, etc
How much mental activity is required to perform your job
(thinking, deciding, calculating, remembering,
looking, searching, etc…),
How much time pressure do you feel due to the rate or pace at
which the tasks or task elements occurred?),
How hard do you have to work (mentally and physically) to
accomplish your level of performance?
How insecure, discouraged, irritated, stressed and annoyed versus
secure, gratified, content, relaxed and complacent do you feel
about your job?
How hard do you have to work (mentally and physically)
to accomplish your level of performance?
Assessing and addressing workload?
• Exercise 3
• Your organization is having an upcoming accreditation survey visit
• You will be introducing a new process aimed at meeting a gap in an
accreditation requirement
• The new process has not been assessed from a workload
perspective
• Your table will simulate the new process and then assess workload
using the NASA TLX score
• Groups A – two volunteers from each table go with Frank
• Groups B – two volunteers from each table go with Chris
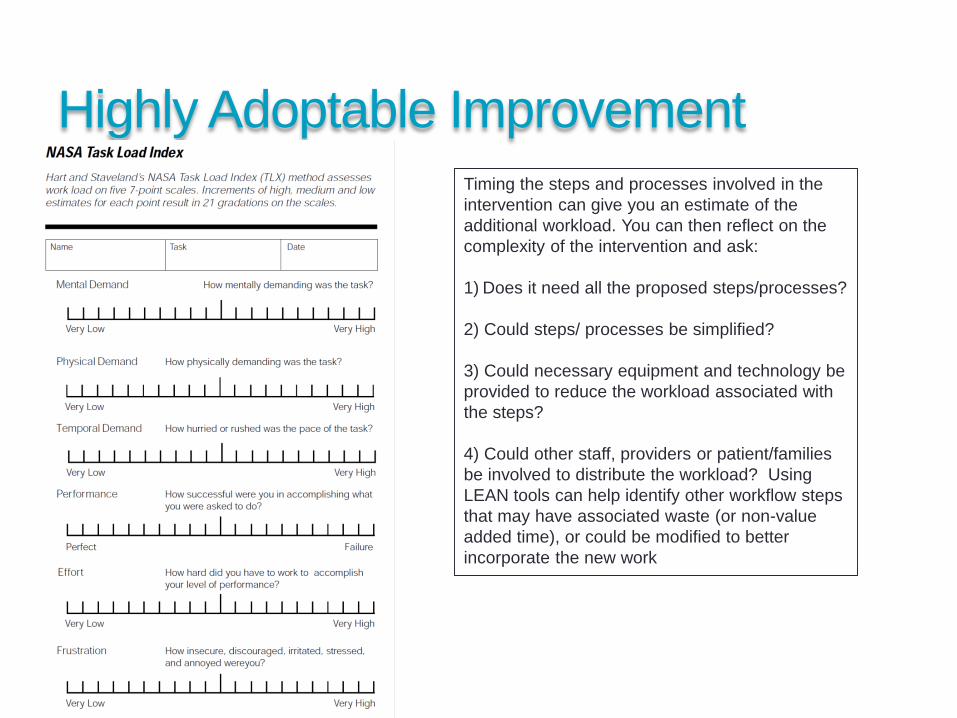
Highly Adoptable Improvement
Timing the steps and processes involved in the
intervention can give you an estimate of the
additional workload. You can then reflect on the
complexity of the intervention and ask:
1) Does it need all the proposed steps/processes?
2) Could steps/ processes be simplified?
3) Could necessary equipment and technology be
provided to reduce the workload associated with
the steps?
4) Could other staff, providers or patient/families
be involved to distribute the workload? Using
LEAN tools can help identify other workflow steps
that may have associated waste (or non-value
added time), or could be modified to better
incorporate the new work
36
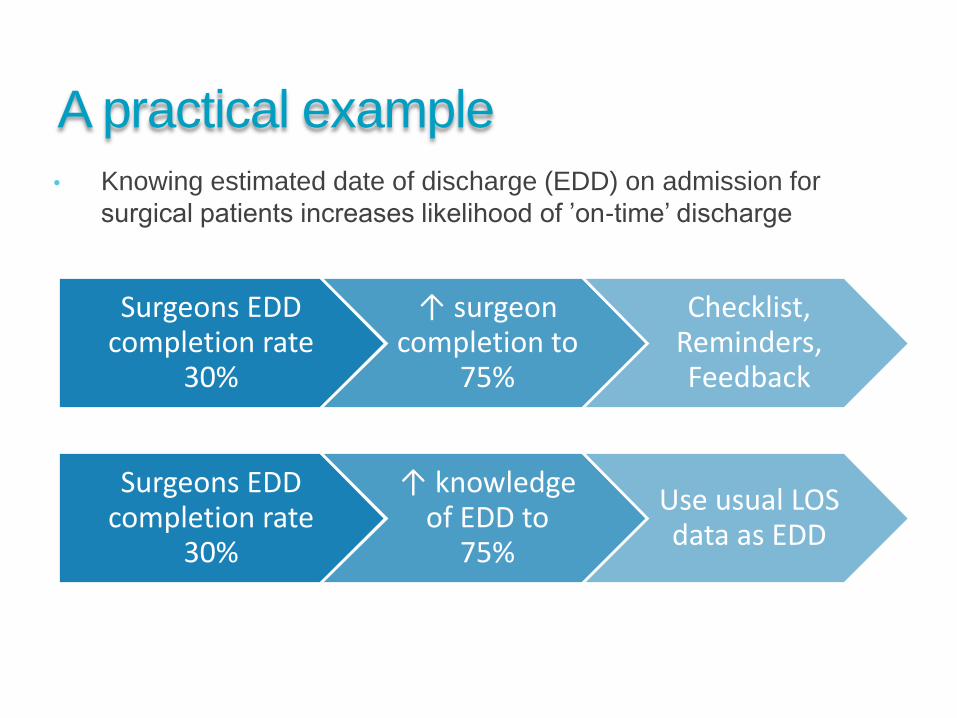
A practical example
37
Surgeons EDD completion rate
30%
↑ surgeon completion to
75%
Checklist, Reminders,Feedback
Surgeons EDD completion rate
30%
↑ knowledge of EDD to
75%
Use usual LOS data as EDD
• Knowing estimated date of discharge (EDD) on admission for
surgical patients increases likelihood of ’on-time’ discharge
Take home messages
Efforts to improve healthcare can increase workload and often fail
Choosing the right change interventions is essential
The Highly Adoptable Improvement model and guide supports focusing on the impact of change on care providers and staff and seems useful and usable
Ongoing work in this area will continue to provide guidance on effectively implementing improvement initiatives and programs
Change is hard….let’s avoid making it harder!!
