course leader: [email protected]@kcl.ac.uk ext: 0207848 3285
TRANSCRIPT

Course leader: [email protected]: 0207848 3285

Session 1Session 1 Concepts theories and models Concepts theories and models underpinning CBT practiceunderpinning CBT practice
Process of therapy Process of therapy
Session 2 Session 2 Assessment, formulation and Assessment, formulation and measurement. measurement.
Overview of cognitive behavioral Overview of cognitive behavioral techniquestechniques
Socratic techniqueSocratic technique
Session 3 Session 3 Cognitive behaviour approach to Cognitive behaviour approach to understanding and treating anxiety understanding and treating anxiety problems problems
Session4Session4 Cognitive behaviour approach to Cognitive behaviour approach to understanding and treating understanding and treating depressiondepression
Session 5 Session 5
Session 6 Session 6
CBT approaches to understanding CBT approaches to understanding and treating psychosisand treating psychosis
Third wave of CBTThird wave of CBT

To complete the course and receive the award students must successfully complete a 2500 word essay based on a case study which will be provided. The essay will focus on the student’s ability to present a cognitive behavioural formulation of the information presented in the case study, identifying maintaining factors and suitable targets for CBT work. The student will be asked to identify treatment strategies based on this formulation with reference to the evidence base for supporting these potential interventions.
The assignment should include the following: A brief explanation of CBT and its main principles. Discuss the role of formulation within CBT work and its strengths/weaknesses. Provide a description of your formulation of the case study (provided) with clear
identification and explanation of maintaining factors. Identify from the formulation possible targets for CBT work. Provide a rationale for and description of possible treatment strategies for these
identified targets with reference to the theory and evidence base underpinning these selected strategies.
Brief consideration of potential obstacles or limitations to the success of these strategies.

► ►What is your current understanding of CBT
and its core characteristics?

Cheryl Jordan

“Man is not affected by events but by the views he takes of them” ( Epictetus)
“There is nothing good or bad but thinking makes it so” ( Hamlet, Shakespeare)

Cognitive principleEmotional reactions are strongly
influenced by cognitions

Behavioural principleWhat we do is crucial in maintaining or in changing psychological states

The continuum principleEmotional problems arise from exaggerated versions of Normal process

Here and nowFocus on what’s happening in the present and what processes are maintaining it.

Interacting systems

Characteristic cognitions in different problems
Depression: negatively biased views themes of loss and failure
Anxiety: Overestimation of threat
Anger ?
Collaborative Structured and active engagement Time limited Empirical in approach Problem orientated Guided discovery Behavioural methods In vivo work Summaries and feedback

Albert Ellis 1913-2007 considered as the second most influential psychotherapist in history ( USA,Canada)Carl Rogers ranked first Sigmund Freud was ranked third
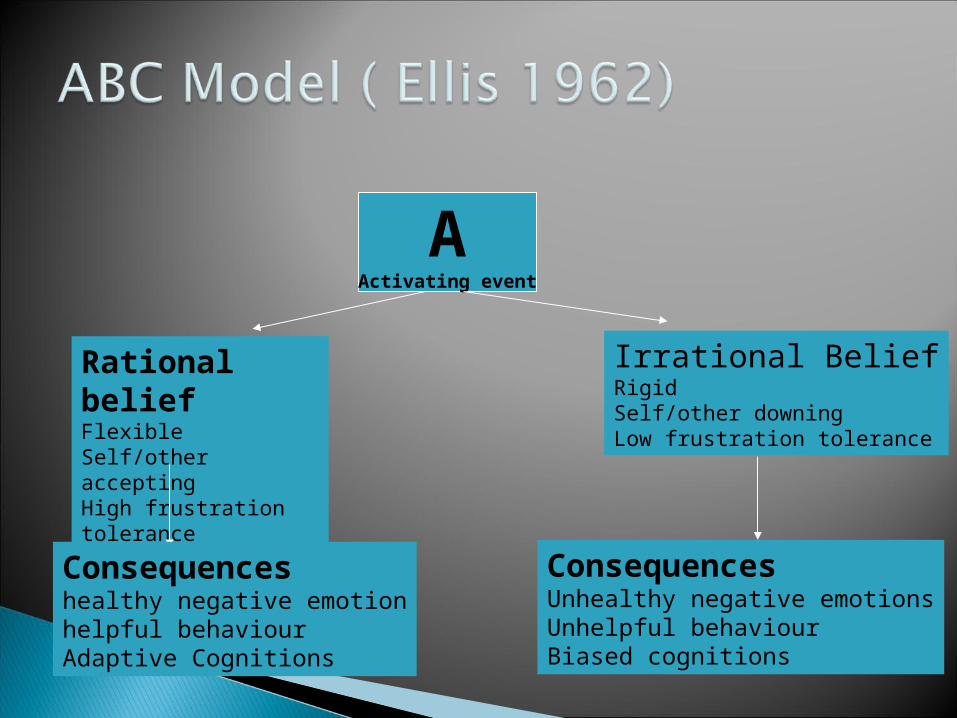
AActivating event
Rational beliefFlexible Self/other acceptingHigh frustration tolerance
Irrational BeliefRigidSelf/other downingLow frustration tolerance
Consequenceshealthy negative emotionhelpful behaviourAdaptive Cognitions
ConsequencesUnhealthy negative emotionsUnhelpful behaviourBiased cognitions

A
Rational beliefI prefer to pass but it is possible I may not, if I do it proves I am a fallible Human and I can tolerate it
Irrational BeliefI want to pass therefore this must happen, If i don’t it’s Proof I am a total failureI can’t stand it
Consequencesconcerned Focus on task at handGiving it my best
ConsequencesanxietyProcrastinate I going to fail, I’ ll never cope
Completing assignment

Please read the chapter Fit the information given into the ABC
model

ANo current partner
Rational beliefI would prefer to be in a relationship, I can accept myself if i am not.
Irrational BeliefI want to be in a relationship, therefore I absolutely should be. The fact I am not is proof I am defective.
ConsequencesSadSeek out reinforcements
ConsequencesDepression no one wants me There is something wrong with me Think about past failed relationshipswithdraw

Watch the clip Keep the ABC model in mind, see if you can
identify the problem......
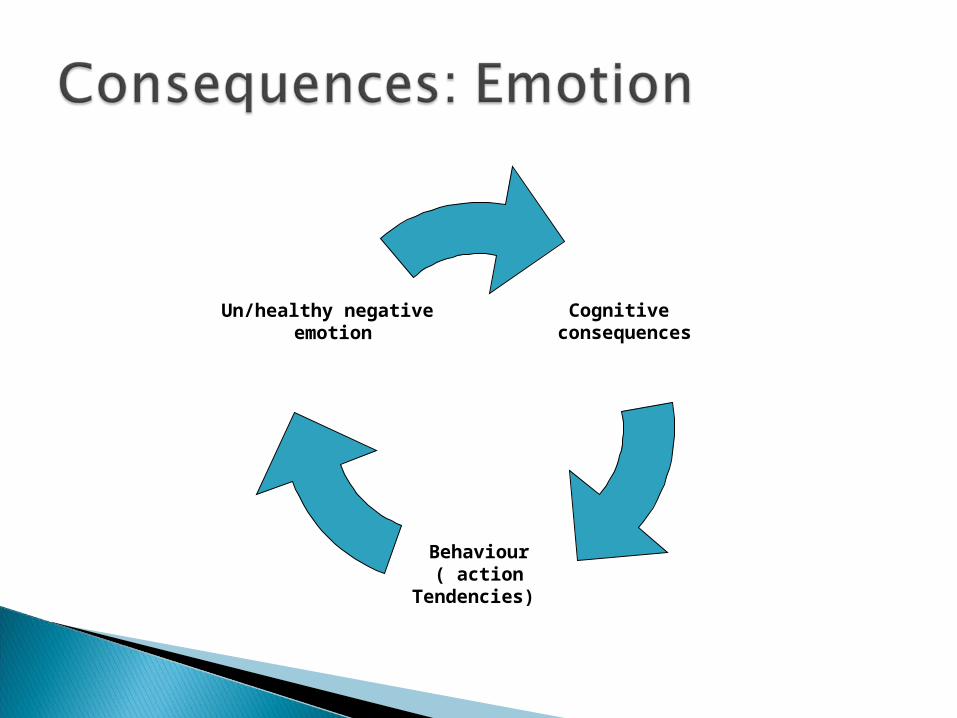
Cognitive consequences
Behaviour( action
Tendencies)
Un/healthy negative emotion

Think of the last time you felt angry about something.
Can you remember what you felt most angry about? went through your mind?
What did you do or feel like doing?

Cognitive consequences
Behaviour( action
Tendencies)
Un/healthy negative emotion
OverestimatesExtent to which other person acted Deliberately.See’s malicious intent in action of otherSelf right other wrongUnable to see others point of viewPlots to exact revenge
Hit, shout, sulk, kick the cat,Recruits allies against others

Trained as a psychoanalytic analyst at the Philadelphia Psychoanalytic Institute.
(1921-….)

EarlyExperience
Core Beliefs
Rules andAssumptions
CriticalIncident
Emotion
thinking
Behaviour
physiology
Self, world, others
If ……. Then……..I must………

EarlyExperience
Core Beliefs
Rules andAssumptions
CriticalIncident
Emotion
thinking
Behaviour
Somatics
I am not as lovable as other people
I should be in a relationship if not then …………
Relationship not working outSeeing others in relationships
depression
What am I doing wrongThink about past Relationships , no one wants me.
Withdrawruminates
Low energy

Core Schema
Assumptions
Negative automatic thoughts


Trigger: critical incident
Thoughts
Mood
Behaviour
Physical

Have a look at the film clip and map the information to the model.
What event triggered her reaction? What negative automatic thoughts is this
lady experiencing? How is this effecting her mood?
Behaviour?

Survey by Wright and Davis(1994), found that clients wanted their therapists to:
Offer physically safe, private, confidential setting free from distractions
Be respectful Treat concerns seriously Prioritise client interests over own Be competent Share information Permit client to make own choices Be flexible not assume the client fits a theory Review progress Pace , not rush or keep changing appointments
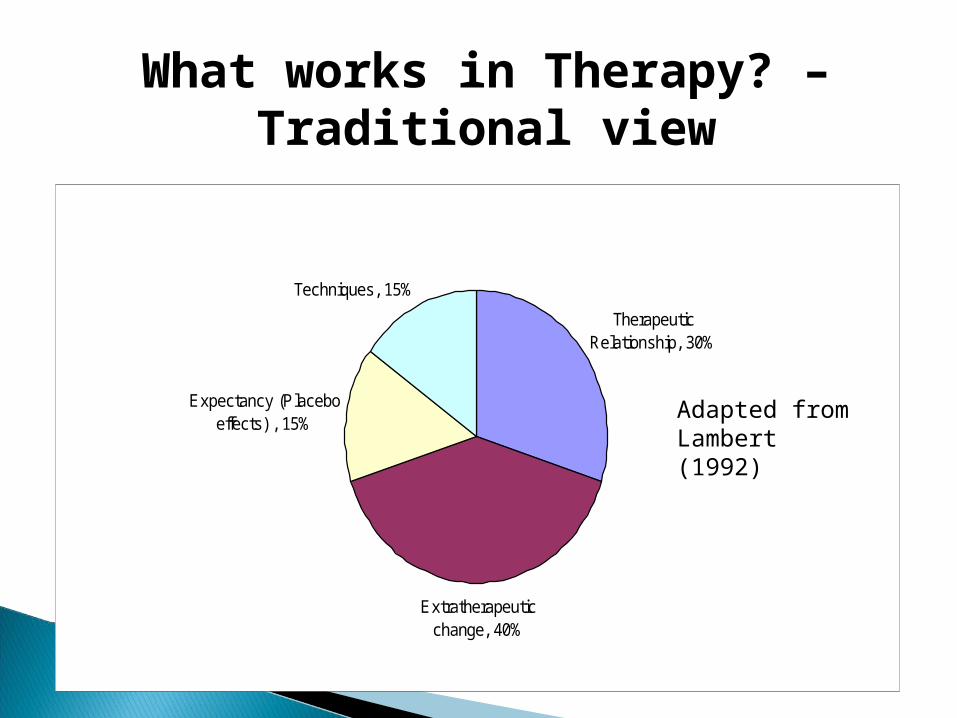
Therapeutic Relationship, 30%
Extratherapeutic change, 40%
Expectancy (Placebo effects) , 15%
Techniques, 15%
What works in Therapy? – Traditional view
Adapted from Lambert (1992)
How would you define each of these?

Consider what you think about the basic principles of CBT. Do they make sense to you?
What do you think of the theory underpinning CBT? does it make sense ? Does it fit with your experience?

1) Therapeutic relationship: engage and facilitate collaborative working process
2) Comprehensive assessment: Detailed picture of problem within context of person’s life experiences and history
3) Problems & Goals: agree on a ‘CB’ definition of problem set goals
4)Clinical Ratings: baseline ratings symptoms distress disability progress evaluated set time frame and target
5) Formulation; Develop shared understanding of problem and it’s maintenance.
6) Treatment rationale: explanations of how and why CBT could work with the problem
7) Interventions: aims reduce symptoms, increase coping
8) Evaluation: Of interventions for effectiveness
9) Relapse prevention: Maintain gains prevent relapse
10) Discharge.
11) Follow-up: further reflection on practice learnt . Set new long term goals

Phobic disorders Anxiety disorders (GAD panic disorder) Obsessive compulsive disorder Mild-moderate depression Post-traumatic stress disorder Eating disorder Substance abuse (alcohol, cocaine) Sexual dysfunction Habit & impulse control disorders Psychosis

Bipolar disorders Delusional disorders Personality disorders Severe depression Depression and anxiety associated with
long term chronic health problems

Observe your own experience and/or those of the clients you work. If you or they are upset about something See if you can identify what they/you are upset about, what patterns of thinking, feeling and behaving are occurring?
Branch R, Dryden W 2008, The cognitive behaviour counselling Primer. Athenoeum Press, UK.
Dryden W, 2001 10 steps to positive living. Sage. London Hawton K, Salkovskis P, Kirk J, Clark D,
1993, Cognitive behaviour therapy for psychiatric Problems. Oxford University Press.Oxford.
Beck A T, The current state of Cognitive Behaviour Therapy.Archive of Gen Psy 2005;629-539