corporate overview june 2016 - jefferies · corporate overview. june 2016. thomas f. miller, phd,...
TRANSCRIPT

Corporate OverviewJune 2016
Thomas F. Miller, PhD, MBAPresident & Chief Executive Officer
Overview• Clinical Stage Company with Lead Program in Ph2
• Prevention of Chronic Respiratory Morbidities in Preterm Infants -- enrollment complete May 2016
• Significant Unmet Need Without Therapeutic Options Today
• Large Market Opportunity Exceeding $500 M for Lead Indication
• Ph2 Trial Funded by FDA’s Office of Orphan Products• FDA Rare Pediatric Disease Designation
• FDA Fast Track Designation
• Orphan Designations (US/EU)
• Management team with significant experience including respiratory drug development through commercialization
• Strategic goal is to treat a wide range of pulmonary diseases with a novel, proprietary therapeutic class: Recombinant Secretoglobin Proteins
2

Management Team
3
Thomas F. Miller, PhD, MBA
President and Chief Executive Officer
Linda L. Chang Senior Vice President, Chief Financial Officer
Alan Cohen, MD Senior Vice President, Chief Medical Officer
Aprile Pilon, PhD Executive Vice President, Chief Scientific OfficerFounder
Scientific Advisory Board
• Mario Castro, MD, MPH, FCCP• Professor of Pulmonary and Critical Care Medicine, and Professor, Medicine and Pediatrics, Division of
Pulmonary and Critical Care Medicine
• Gerard J. Criner, MD• Chair and Professor of Thoracic Medicine and Surgery
• Steven M. Donn, MD• Professor of Pediatrics, Division of Neonatology
• Martin R. Zamora, MD• Professor of Medicine and Medical Director Lung Transplant Program, Pulmonary Sciences and Critical Care
Medicine
4
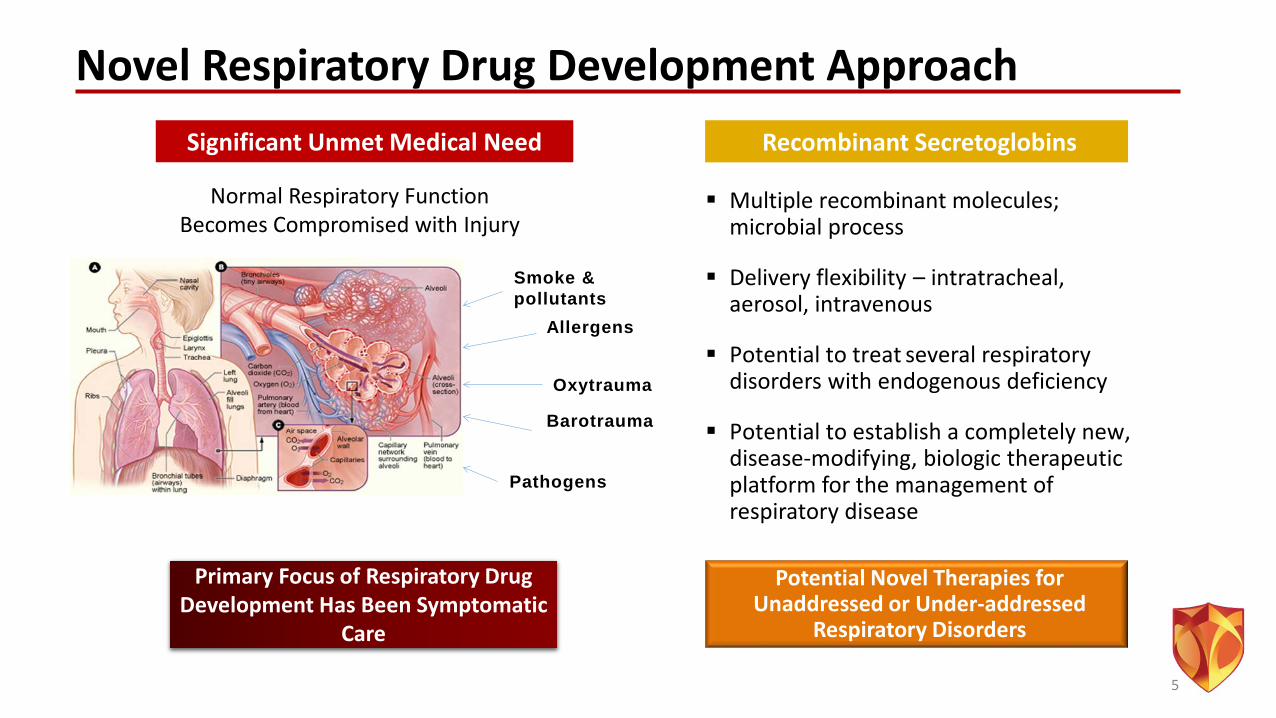
Novel Respiratory Drug Development Approach
Multiple recombinant molecules; microbial process
Delivery flexibility – intratracheal, aerosol, intravenous
Potential to treat several respiratory disorders with endogenous deficiency
Potential to establish a completely new, disease-modifying, biologic therapeutic platform for the management of respiratory disease
Recombinant SecretoglobinsSignificant Unmet Medical Need
Primary Focus of Respiratory Drug Development Has Been Symptomatic
Care
Potential Novel Therapies for Unaddressed or Under-addressed
Respiratory Disorders
Normal Respiratory Function Becomes Compromised with Injury
Barotrauma
Smoke & pollutants
Oxytrauma
Allergens
Pathogens
5
6
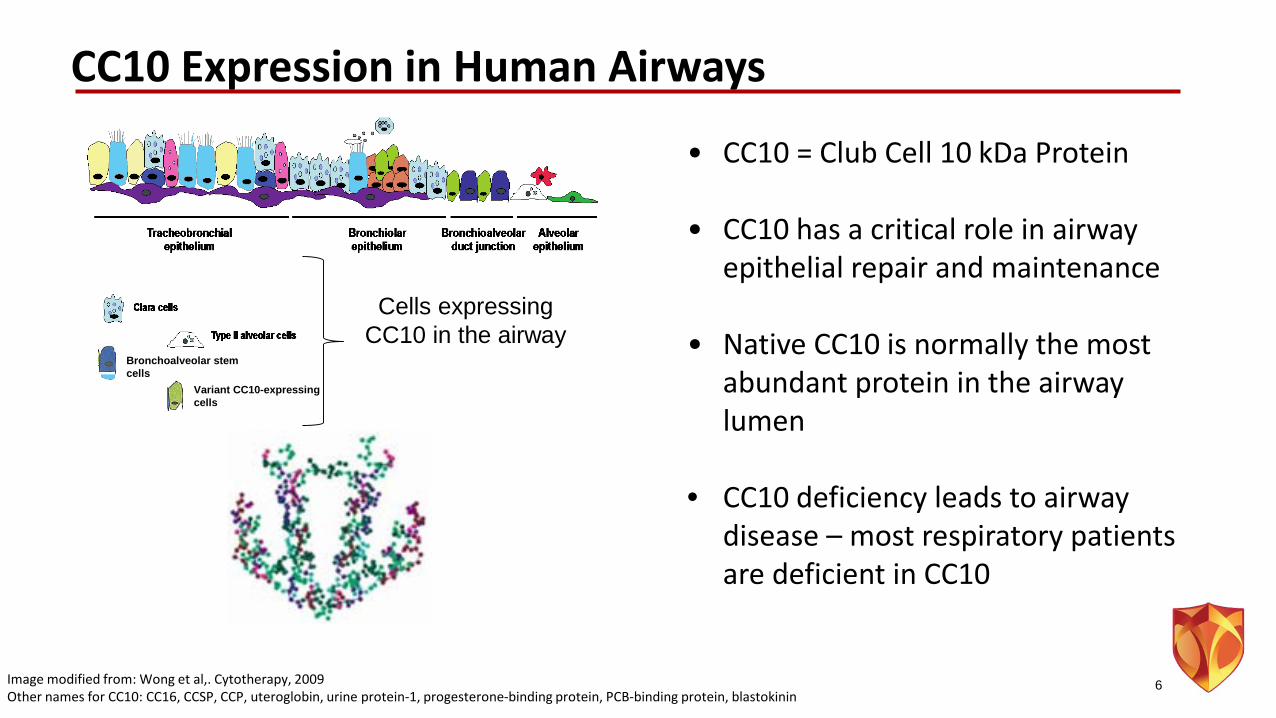
Cells expressing CC10 in the airway
Image modified from: Wong et al,. Cytotherapy, 2009Other names for CC10: CC16, CCSP, CCP, uteroglobin, urine protein-1, progesterone-binding protein, PCB-binding protein, blastokinin
• CC10 = Club Cell 10 kDa Protein
• CC10 has a critical role in airway epithelial repair and maintenance
• Native CC10 is normally the most abundant protein in the airway lumen
• CC10 deficiency leads to airway disease – most respiratory patients are deficient in CC10
CC10 Expression in Human Airways
Variant CC10-expressing cells
Bronchoalveolar stem cells
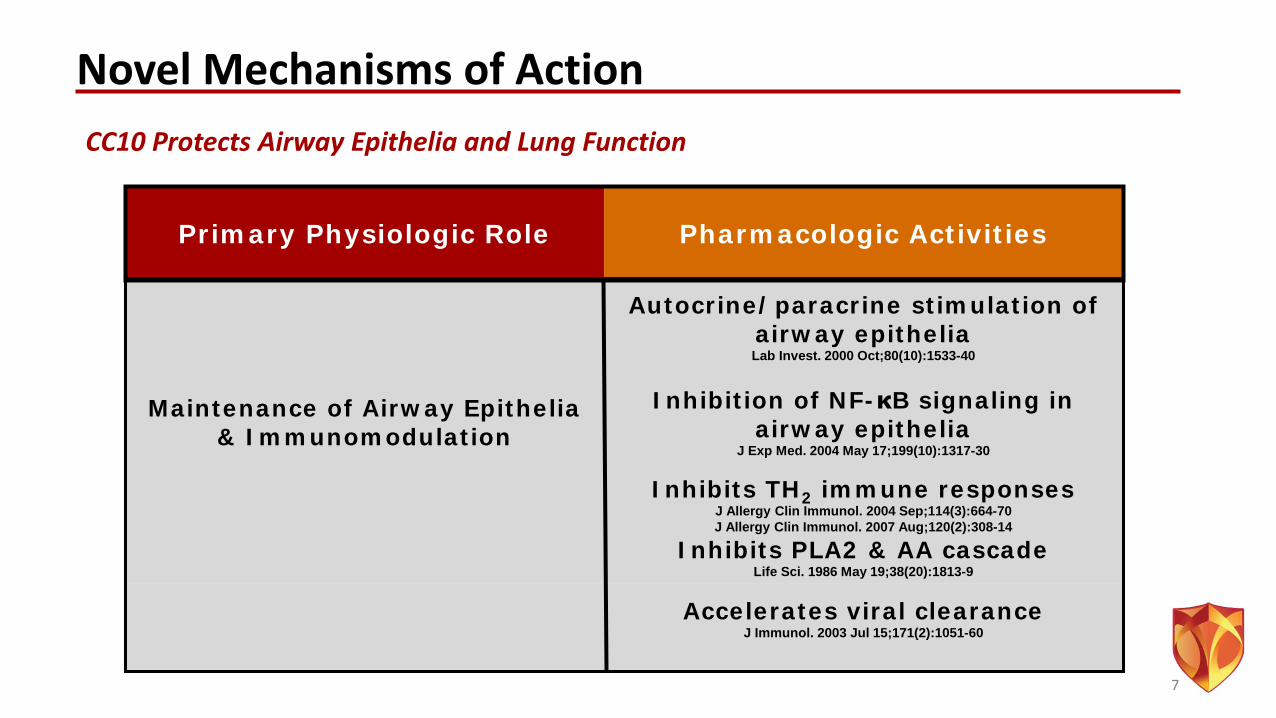
Novel Mechanisms of Action
Primary Physiologic Role Pharmacologic Activities
Autocrine/paracrine stimulation of airway epitheliaLab Invest. 2000 Oct;80(10):1533-40
Maintenance of Airway Epithelia & Immunomodulation
Inhibition of NF-κB signaling in airway epithelia
J Exp Med. 2004 May 17;199(10):1317-30
Inhibits TH2 immune responsesJ Allergy Clin Immunol. 2004 Sep;114(3):664-70J Allergy Clin Immunol. 2007 Aug;120(2):308-14
Inhibits PLA2 & AA cascadeLife Sci. 1986 May 19;38(20):1813-9
Accelerates viral clearanceJ Immunol. 2003 Jul 15;171(2):1051-60
7
CC10 Protects Airway Epithelia and Lung Function
Recombinant Secretoglobin Protein Technology Platform
• Phase 2 study for lead program in progress – evaluating rhCC10 for the prevention of chronic respiratory morbidities (CRM) in preterm infants
- FDA Rare Pediatric Disease Designation
- FDA Fast Track Designation
- Recipient of FDA’s Office of Orphan Products Development Grant
• Extensive pre-clinical PoC – therapeutic targets include:- Chronic Obstructive Pulmonary Disease (COPD)- Asthma- Recurrent / Chronic Sinusitis- Treatment Pediatric Acute Respiratory Failure (ARF)- Treatment of Traumatic Smoke Inhalation- Acute Lung Injury (ALI)- Bronchiolitis Obliterans Syndrome (BOS)
8
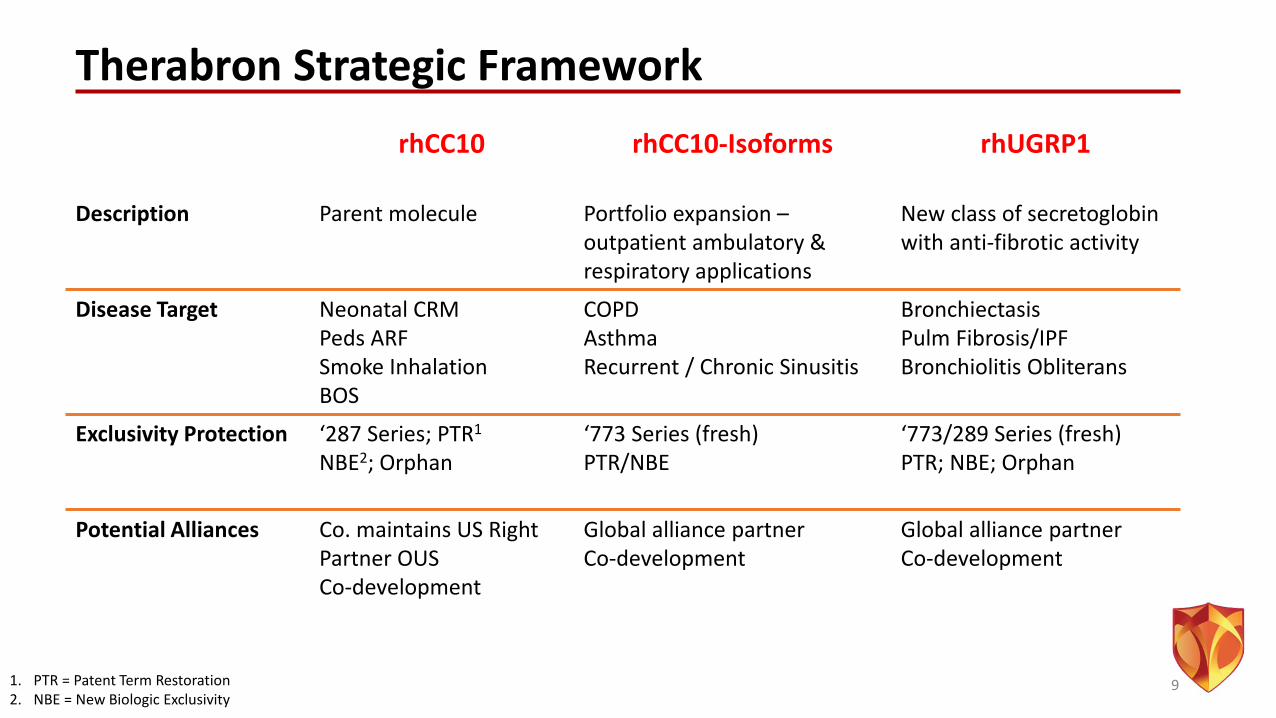
Therabron Strategic Framework
91. PTR = Patent Term Restoration2. NBE = New Biologic Exclusivity
rhCC10 rhCC10-Isoforms rhUGRP1
Description Parent molecule Portfolio expansion –outpatient ambulatory & respiratory applications
New class of secretoglobinwith anti-fibrotic activity
Disease Target Neonatal CRMPeds ARFSmoke InhalationBOS
COPDAsthmaRecurrent / Chronic Sinusitis
BronchiectasisPulm Fibrosis/IPFBronchiolitis Obliterans
Exclusivity Protection ‘287 Series; PTR1
NBE2; Orphan‘773 Series (fresh)PTR/NBE
‘773/289 Series (fresh)PTR; NBE; Orphan
Potential Alliances Co. maintains US RightPartner OUSCo-development
Global alliance partnerCo-development
Global alliance partnerCo-development
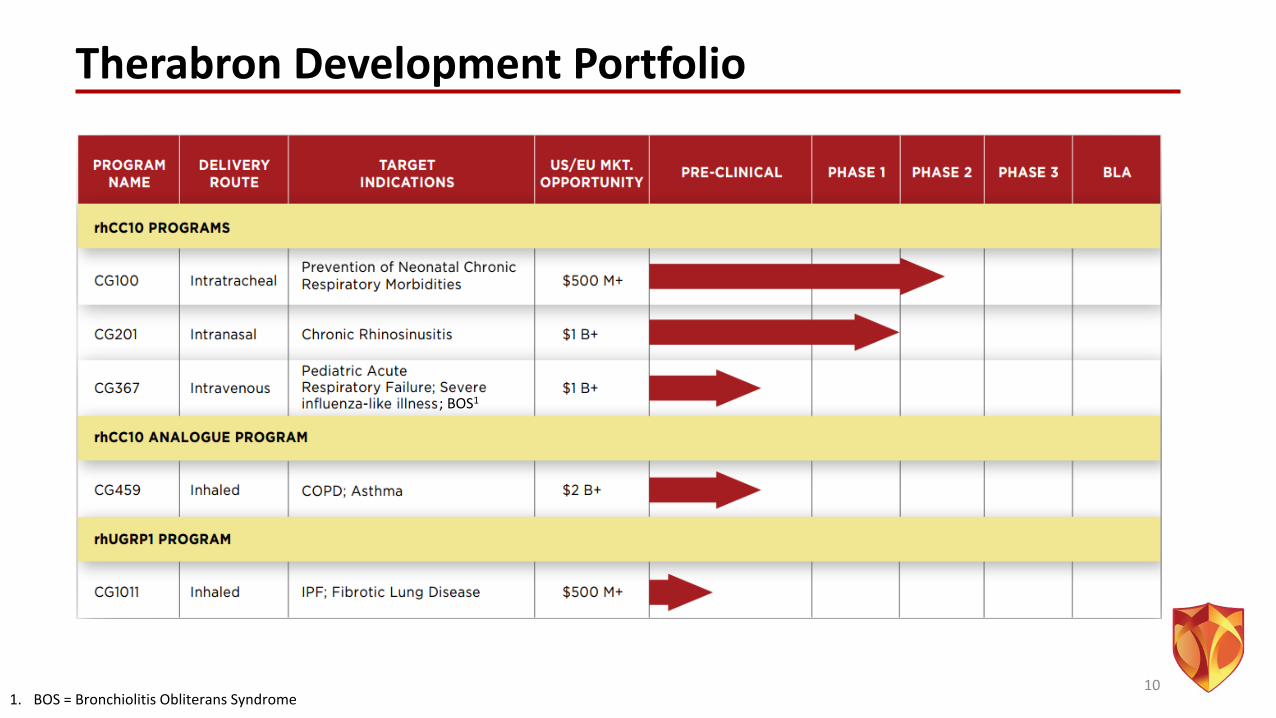
Therabron Development Portfolio
10
; BOS1
1. BOS = Bronchiolitis Obliterans Syndrome
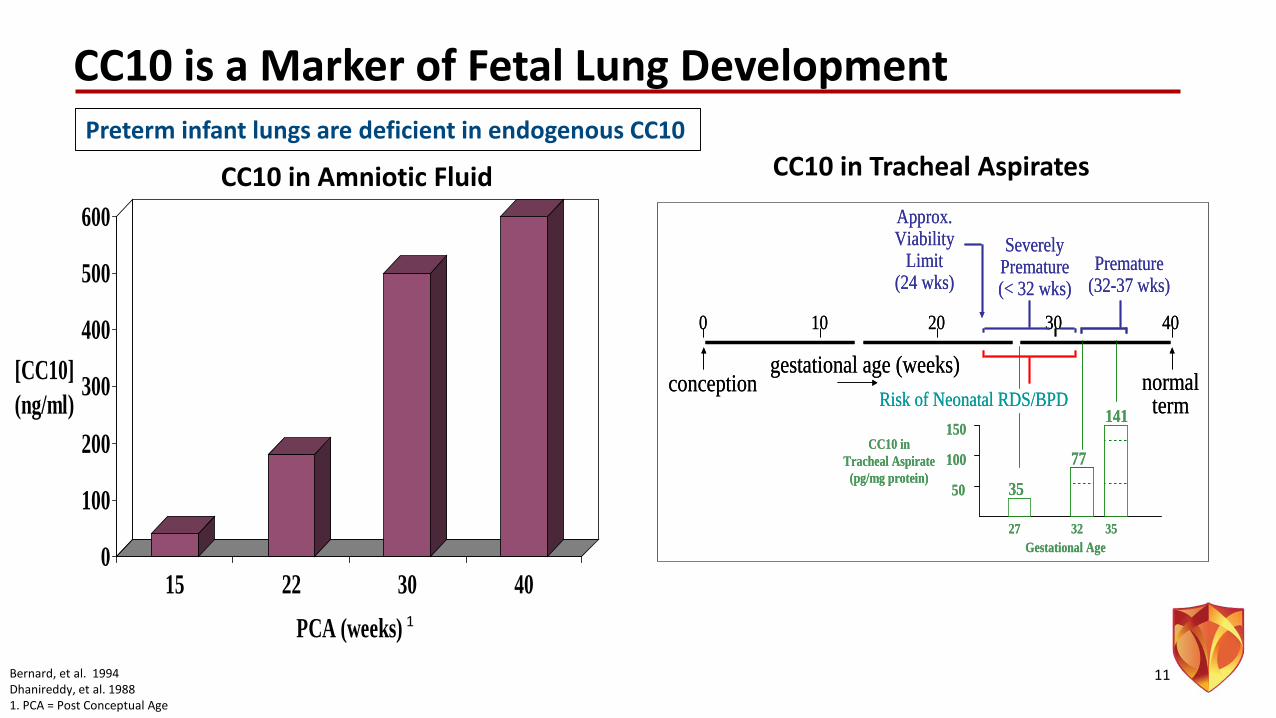
CC10 is a Marker of Fetal Lung Development
Bernard, et al. 1994Dhanireddy, et al. 19881. PCA = Post Conceptual Age
0
100
200
300
400
500
600
[CC10] (ng/ml)
15 22 30 40PCA (weeks)
10 20 30 400
gestational age (weeks)conception normal
term
Approx.Viability
Limit(24 wks)
SeverelyPremature(< 32 wks)
Premature(32-37 wks)
Risk of Neonatal RDS/BPD
27 32 35
50
100
150
35
77
141CC10 in
Tracheal Aspirate(pg/mg protein)
Gestational Age
10 20 30 400
gestational age (weeks)conception normal
term
Approx.Viability
Limit(24 wks)
SeverelyPremature(< 32 wks)
Premature(32-37 wks)
Risk of Neonatal RDS/BPD
27 32 35
50
100
150
35
77
141CC10 in
Tracheal Aspirate(pg/mg protein)
Gestational Age
CC10 in Amniotic Fluid CC10 in Tracheal Aspirates
11
Preterm infant lungs are deficient in endogenous CC10
1

Pre-clinical PoC: Preterm Infant Application
• rhCC10 exposure significantly improves lung function –multiple mammalian species
• rhCC10 significantly increases surfactant protein expression
• rhCC10 significantly decreases:- IL-8, other cytokines - Neutrophils in airway- Total protein in airway - MMP2, MMP9 in lung tissue
Wolfson et al., 2008Shashikant, et al., J Appl Physiol. 2005 Dec;99(6):2204-11
rHCC10 Significantly Improved Ventilation Efficiency Index
0102030405060708090
0 10 20 30 40Lu
ng V
olum
e (m
L)
Pressure (cm H2O)
NormalNo CC10Claragen (5 mg/kg)
p < 0.05
CC10
Chandra S et.al., Safety and Efficacy of Intratracheal Recombinant Human Clara Cell Protein in a Newborn Piglet Model of Acute Lung Injury. Pediatr Res. 54:509-515, 2003.1. SF = Surfactant; 0.5/1.5/5.0 = mg/kg rhCC10 exposure
12
1
FIM Trial Overview• Study Design
- n = 22 pre-term infants randomized, double-blind, placebo controlled- 1.5 mg/kg: 5mg/kg: PBO (1:1:1), single intra-tracheal administration- Primary goal: Assessment of safety and tolerability of two exposed doses of rhCC10
vs. PBO- Establish Proof of Pharmacology- 6/12 month follow up
• Safety & Tolerability Assessment- No reactions to instillation of rhCC10 or placebo observed - method identical to
surfactant instillation with small volumetric dose- No atypical AEs or SAEs;
- Placebo-153; 1.5 mg/kg-156; 5 mg/kg-165- No evidence of anti-CC10 antibodies in 28 day sera
13Levine, et al 200513
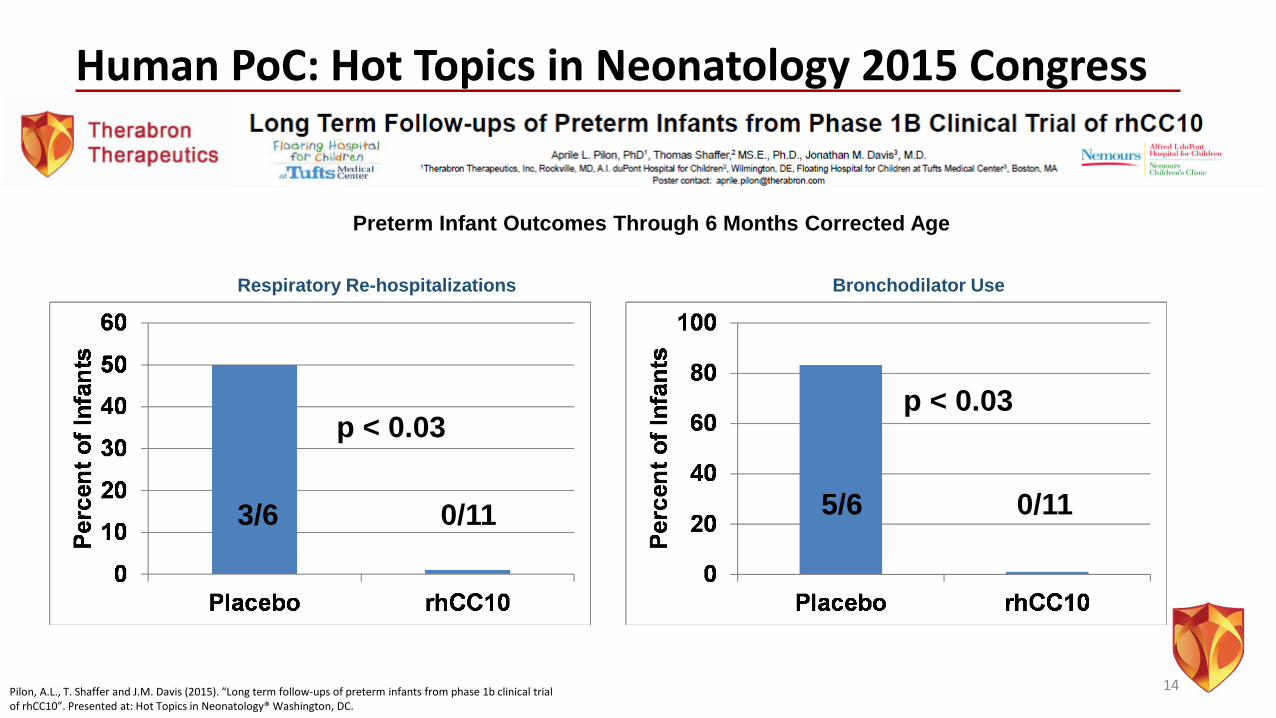
Human PoC: Hot Topics in Neonatology 2015 Congress
14
Preterm Infant Outcomes Through 6 Months Corrected Age
Respiratory Re-hospitalizations Bronchodilator Use
p < 0.03
3/6 0/11
p < 0.03
5/6 0/11
Pilon, A.L., T. Shaffer and J.M. Davis (2015). “Long term follow-ups of preterm infants from phase 1b clinical trial of rhCC10”. Presented at: Hot Topics in Neonatology® Washington, DC.
Ongoing Phase 2 Trial: Study Design• Similar design as Phase 1b – single CG100 IT dose within 4 hrs. of first dose of
surfactant• Randomized, placebo-controlled, double-blinded• n = 88 preterm infants (24-29 wk. CGA); 3 dose groups – placebo, low (1.5 mg/kg),
high (5 mg/kg)• Clinical protocol reviewed by FDA; Endpoints deemed “appropriate for patient
population”• Primary endpoint of interest:
- Survival without chronic respiratory morbidity (CRM) through 12 mo corrected age- CRM = composite endpoint comprised of respiratory symptoms, use of respiratory medications,
unscheduled doctor visits and re-hospitalizations
• Other exploratory endpoints: - Prevention of re-hospitalization from respiratory causes at 6 corrected age - Oxygen withdrawal challenge at 36 wks cga (physiologic BPD)
• Enrollment completed May 2016
www.clinicaltrials.gov15
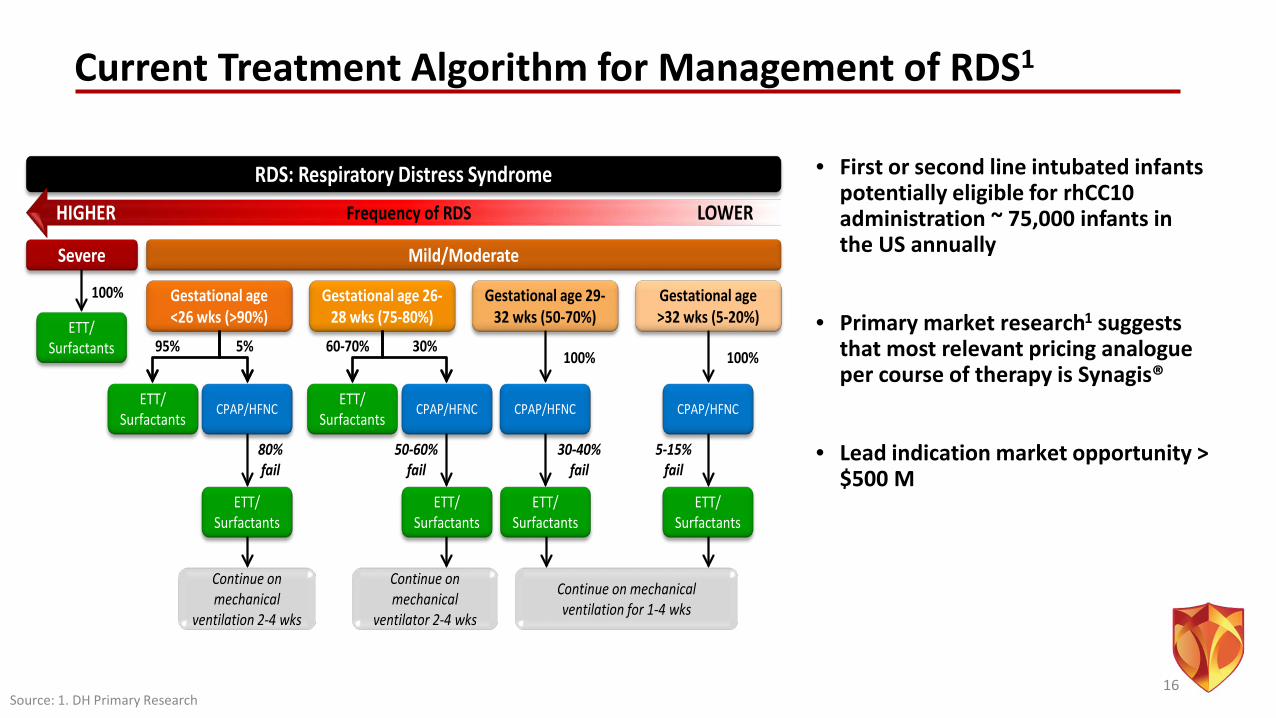
Current Treatment Algorithm for Management of RDS1
RDS: Respiratory Distress Syndrome
Severe
Frequency of RDSHIGHER LOWER
Mild/Moderate
ETT/ Surfactants
100% Gestational age <26 wks (>90%)
Gestational age 26-28 wks (75-80%)
Gestational age 29-32 wks (50-70%)
Gestational age >32 wks (5-20%)
5% 30%100%
CPAP/HFNC
100%
CPAP/HFNCETT/ Surfactants
CPAP/HFNC ETT/ Surfactants
CPAP/HFNC
60-70%95%
ETT/ Surfactants
ETT/ Surfactants
ETT/ Surfactants
ETT/ Surfactants
80% fail
50-60% fail
30-40% fail
5-15% fail
Continue on mechanical
ventilation 2-4 wks
Continue on mechanical
ventilator 2-4 wks
Continue on mechanical ventilation for 1-4 wks
• First or second line intubated infants potentially eligible for rhCC10 administration ~ 75,000 infants in the US annually
• Primary market research1 suggests that most relevant pricing analogue per course of therapy is Synagis®
• Lead indication market opportunity > $500 M
Source: 1. DH Primary Research16
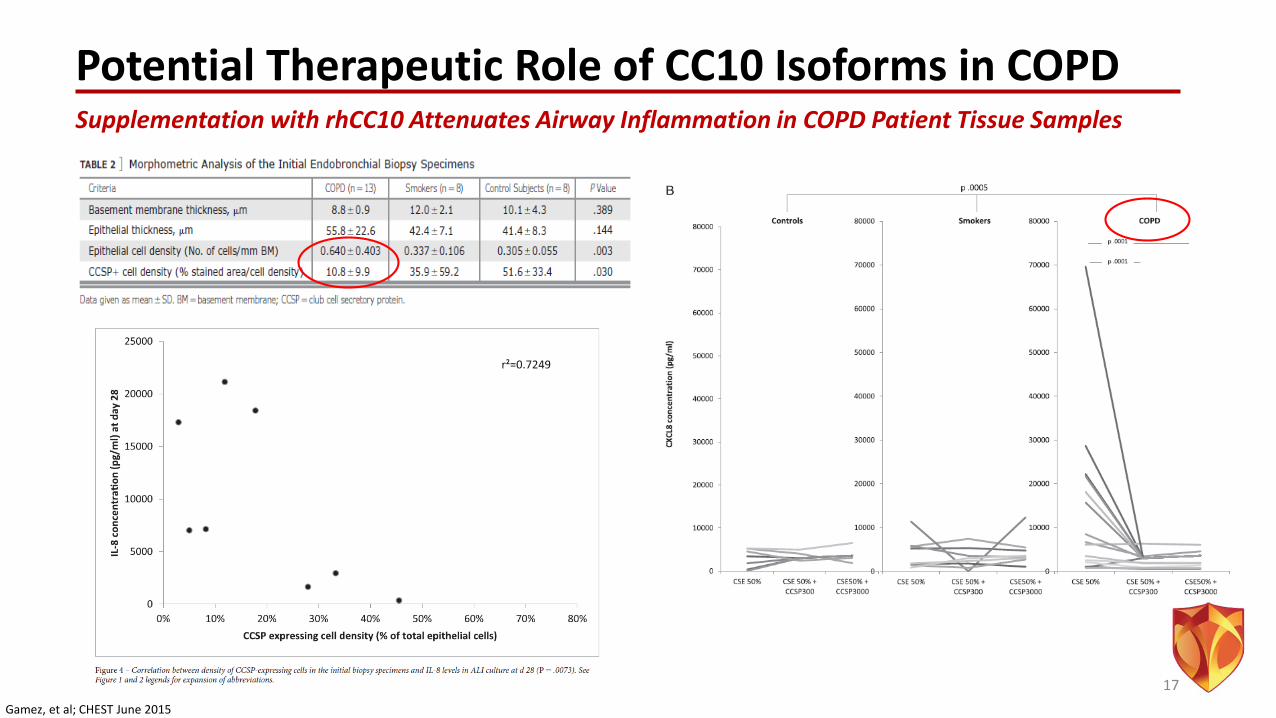
Potential Therapeutic Role of CC10 Isoforms in COPDSupplementation with rhCC10 Attenuates Airway Inflammation in COPD Patient Tissue Samples
17Gamez, et al; CHEST June 2015
Milestones: 2016 - 2017• Lead program (CG100)
- Enrollment complete May 2016- 12 mo patient follow up complete mid-17- EoP2 Meeting Target: 2H17- Initiate P3: 2H17
• Initiation of second program in 2016 (CG367 – IV dosage form of rhCC10)- Data available 2H17
• Recent / Potential Milestones:- Rare Pediatric Disease Designation for rhCC10 in preterm infants- Fast Track designation for rhCC10 for the prevention of chronic lung disease related to premature birth- New portfolio exclusivities (Notice of Allowance for patent “Modification and Compositions of Human
Secretoglobin Proteins received April 2016)- Multiple new data read outs / scientific presentations (WODC, PAS, ATS, Others)- Strategic partnerships
18
Financials• Capital Efficient Model -- $14 MM capital raised to date advanced Company
through completion of enrollment of Ph2 for lead program• Led by Brace Pharma Capital
• US Federal Government financial support• FDA – Office of Orphan Product Development
- 4 yrs.; Phase 2 clinical trial of CG100 (rhCC10) to prevent neonatal CRM in premature infants with respiratory distress syndrome
• US Army- 2 yrs.; evaluate rhCC10 in smoke inhalation lung injury and
dermal burn animal models
• Active pursuit of strategic alliance(s)
• Pursuing up to $30 M Series C Round – Use of Proceeds: • Data read and through EoP2 FDA meeting for CG100• Open 2nd IND with IV dosage form of rhCC10 (CG367)• Complete tech transfer through ‘commercial ready’ manufacturing and QC prior to Ph3
19
Summary• Clinical Stage Company with Lead Program in Ph2
• Prevention of Chronic Respiratory Morbidities in Preterm Infants -- enrollment complete May 2016
• Significant Unmet Need Without Therapeutic Options Today
• Large Market Opportunity Exceeding $500 M for Lead Indication
• Ph2 Trial Funded by FDA’s Office of Orphan Products• FDA Rare Pediatric Disease Designation
• FDA Fast Track Designation
• Orphan Designations (US/EU)
• Management team with significant experience including respiratory drug development through commercialization
• Strategic goal is to treat a wide range of pulmonary diseases with a novel, proprietary therapeutic class: Recombinant Secretoglobin Proteins
20
Corporate OverviewJune 2016
Thomas F. Miller, PhD, MBAPresident & Chief Executive Officer