corel ventura - ph-06 - semantic scholar. asha chitnis, m.p.t., ndt (ped), dr. ashok johari, m.s....
TRANSCRIPT

438C>A
Mr. N. VENKATESH
438C>A80; 1>0A3
Mr. V.C. JACOB, MUMBAI
Mr. S.S. RAO, CALCUTTA
Mr. KOSHY K MATHAI, DELHI
Mr. ADAM VINNAARASAN,CHENNAI
Letters, enquiries etc., addressedto the Editor may be sent to thefollowing address
Plot No.112, Shruthilaya, Ashok Brindavan, Off Village Road, Iyyapanthangal, Chennai - 600 056.
Printed by
AKSHARA , CHENNAI
?WhbX^cWTaP_h(FOR PRIVATE CIRCULATION ONLY)
C74 9>DA=0; >5 8=380= 0BB>280C8>= >5
?7HB8>C74A0?8BCB
0dVdbc !��!
CONTENTS
Pg.No.
1. Editorial 2
2. Botulinum Toxin Injection for Cerebral Palsy in the SecondDecade of LifeDr. Asha Chitnis, Dr. Ashok Johar, Dr. Laxit Doshi
3. Extracranical causes for Head Pain: Clinical Implications for thePhysical TherapistDr. Deepak Sebastian
9
4. A comparative Study of the Efficacy of lontophoresis andPhonophoresis in the treatment of Shin SplintAmarjeet Singh, G.B. Sethy, J.S. Sandhu, A.G.K Sinha
17
5. Wound ARea Measurement in Experimental Animals:Conventional Graph Paper Methods versus Autocad RLComputer AnalysisMaiya Arun G. Kumar Praod, Nayak Shivanand
21
6. Role of Cerebellum in Motor Learning - Relevance toPhysiotherapy (Literature Review)Uday Kiran Reddy Emani
25
Statements and information contained in this publication are believed tobe reliable. The opinions advanced in these articles are expressions of theauthors and not necessarily those of the Editor and members of the EditorialBoard.
1
EDITORIAL“POST GRADUATE PHYSIOTHERAPY EDUCATION IN INDIA”
“NATIONAL BOARD EXAMINATIONS FOR PHYSIOTHERAPISTS”
It was between 1980 - 2000, many undergraduate colleges started and have come to a saturationlevel now. Now it is turn for the postgraduate colleges. already a number of colleges are there inSouth India that offer P.G.Courses in Physiotherapy. There are few P.G. Colleges without properinfrastructure, teaching faculty and guides. We don’t know why universities allow such colleges tofunction. The Post Graduate Colleges should made it clear that the knowledge, skills and learningmethods are distinctly different from Under Graduate programmes. Any how relevant basic acumenshould link both under and post graduate courses. IAP is also in its way of defining set curriculumsfor both under and post graduate physiotherapy courses. Now there is a strong feeling that amongunder graduates that post graduate physiotherapy education is essential to upgrade their position,knowledge and skill.
But there are so many physiotherapists after graduation, who are unable to proceed further instudies because of non availability of seats in post graduate Govt Institutions, that offer Physiotherapy(M.Sc. or M.PT). Affordability makes it difficult for them to get into private colleges. Our IndianAssociation of physiotherapists is seriously thinking of starting National Board Examinations. Butthere are a few obstacles, namely we don’t have a council and the other is that the National BoardExaminations are conducted by Ministry of Health & Social Welfare. Hence we are not in a goodto start of our own; IAP is trying to get some universities to help in this matter.
On achieving and being able to run N.B.E.P we will be more strong and can show solidarityin achieving a mile stone in our Profession. Henceforth we shall do the needful help in this regardto IAP.
This issue consists of articles from our respected members of IAP. One article is from an IAPmember, who is a Doctorate in Physiotherapy, working in Wyne’s University, U.S.A. The editorialboard is keen on responses from its members and welcomes many more articles.
N. VENKATESH, M.P.T, M.Sc Fern MIAP,Editor, IAP Journal.Plot No 112, H/No 2/204, Shruthi LayaAshok Brindavan, Iyyapanthangal, Chennai - 600 056. IndiaPhone No: 044 627 4867Email - [email protected]
2

BOTULINUM TOXIN INJECTION FOR CEREBRAL PALSY INTHE SECOND DECADE OF LIFE
Dr. Asha Chitnis, M.P.T., NDT (Ped), Dr. Ashok Johari, M.S. (Ortho),Dr. Laxit Doshi, B.P.T., Dr. Tushar Agrawal, M.S. (Ortho)
INTRODUCTION
Cerebral Palsy is the most common motor disorderin infants and children and the prevalence is 2 of every1000 live births (Paneth & Kiely, 1984). The mostcommon form of cerebral palsy (C.P.) is spastic C.P.,which is 88% (Hagberg & Hagberg 1996).
We have a stepped care approach availablebeginning with more conservative options like motortraining, splinting, intramuscular injections andorthopaedic and neurosurgery for older children.
Efficacy of Botulinum Toxin type A in themanagement of Cerebral Palsy has been supported by 3randomized controlled trials in the lower limb (Komanet al; 1994, Corry et al; 1998, Sutherland et al; 1999).
In the limbs, spasticity causes a chain of eventswhich progress through reduced muscle excursion,increased muscle stiffness and fixed musculotendinouscontracture, to bony torsional abnormalities and jointinstability. These changes are timedependent, so thatyounger children have a much more complex problemwith spasticity, contractures and secondary bonydeformities.
Mechanism Of Action
Hyperactive muscle contraction, regardless ofunderlying cause, is characterized by excessive releaseof acetylcholine at the neuromuscular junction.Botulinum Toxin A blocks neuromuscular transmissionof acetylcholine through a 3-step process:
° Binding
° Internalization
° Blocking
This is followed by sprouting of new axonterminals, which result in reestablishment ofneuromuscular transmission (Alderson K. et al, 1991)
MATERIAL AND METHOD
We studied 17 patients treated with BotulinumToxin type A injection in the age group of 10 to 15years between the period of Jan 1999 to Dec 2001.Following is the patient distribution:
Hemiplegics-3
Diplegics-11
Quadriplegics-3.
Botulinum toxin was injected in the dose of 6-8units/Kg of body weight. The most common indicationwere:
1 Pre surgical assessment.
2 Delaying surgery and developing antigravitymuscles and postural control.
3 To treat post-surgical relapses and identfyingnewer target areas post surgery.
Patients were assessed pre-botox, immediatelypost-botox, post-botox 1 month, 3 months, 6 months, 9months and 12 months. All the patients were assessedusing following scales.
1. Modified Ashworth Scale
0 No increase in muscle tone
1 Slight increase in muscle tone, manifested by acatch and release or by minimal resistance atthe end of the range of motion when theaffected part is moved in flexion or extension.
2 Slight increase in muscle tone manifested by acatch, followed by minimal resistancethroughout the remainder (less than half) of therange of movement.
3 More marked increase in muscle tone throughmost of ROM, but affected part easily moved.
4 Considerable increase in muscle tone, passivemovement difficult.
5 Affected part rigid in flexion or extension.
2. % of function scale
Using the rating scale below, we estimated theamount of function the patient had at that point of time.Rate as if 0% represents fully disabled or no functionalactivity and 100% represents normal functional activity.
No Function Normal Function
0% 20% 40% 60% 80% 100%
At Ankle:
0% No function.
20% Can initiate dorsiflexion with knee flexion.
40% Can do full range of dorsiflexion with knee flexion.
3

60% Can initiate dorsiflexion with knee extension.
80% Can do dorsiflexion with knee extension, but noheel strike in gait.
100% Can do dorsiflexion with knee extension and heelstrike in gait.
At Knee
0% No function
20% Can do hip knee flexion, in prone can not do kneeflexion.
40% In prone can do knee flexion, but with hipreinforcement, can initiate knee extension with hipflexion.
60% Can do knee extension with hip flexion withposterior pelvic tilt. In prone can do knee flexion withoutreinforcement.
80% Assisted SLR with no reinforcement at hip. Goodeccentric control at knee.
100% Can do SLR till 80 degrees.
At Hip
0% No function.
20% Can initiate hip knee flexion, but in lordosis.
40% Can do hip knee flexion; but beyond 90 degressof hip knee flexion, the trunk goes into lordosis.
60% Can do hip knee flexion, with no lordosis, but SLRnot possible.
80% Can do SLR with reinforcement.
100% Can do good SLR in initial 30 degrees.
3. SELECTIVE MOTOR CONTROL
This rating scale is similar to % of function scale,whereby
0 is same as 0%1 is same as 20%2 is same as 40%3 is same as 60%4 is same as 80%5 is same as 100%
4. SENSORY EVALUATION:
Routine Sensory Evaluation was performed in all thepatients.
DISCUSSION:
We studied 17 patients diagnosed as Cerebral Palsyand Spasticity treated with Botulinum toxin type Ainjections between the period of Jan 1999 to Dec 2001.Their ages ranged from 10 to 15 years. Of these 3 wereHemiplegics, 11 were Diplegics and 3 wereQuadriplegics.
Botulinum toxin was injected in the dose of 6-8units/kg body weight. The most commonly injectedmuscles were: Hamstrings, Gastrosoleus, Hip Adductorsand Hip Flexors.
Although, Cerebral palsy is often described asSensori-motor disorder, the motor deficit has traditionallybeen the focus of attention in assessment and treatment.These motor problems are extensively described inliterature (Bobath 1975, Bly 1983, Wilson 1984).
During the last decade, the sensory processingproblems in Cerebral Palsy have been emphasized(Shunway, Cook. Horark 1986, Burke and Blanche1991). The sensory deficits in the child with CerebralPalsy are described as primary and secondary deficits(Moore 1984). Primary sensory processing disorders arethose deficits that occur concurrently with a movementdisorder. The insult that result in the movementdysfunction also results in a sensory processing disorder.Secondary sensory processing deficits occur as a resultof movement limitation (Moore 1984).
In this group, who were in 2nd decade of life andwhose treatment had plateaued, the problem areas were:
1. Motor Presence of primitive reflexes,
Positive Supporting reaction,
Startle Reflex
2. Sensory Poor balance in sitting and standing,
Postural Insecurity
Visual and Vestibular Problems.
3. Contractures
4. Obesity and
5. Psychologicalproblems.
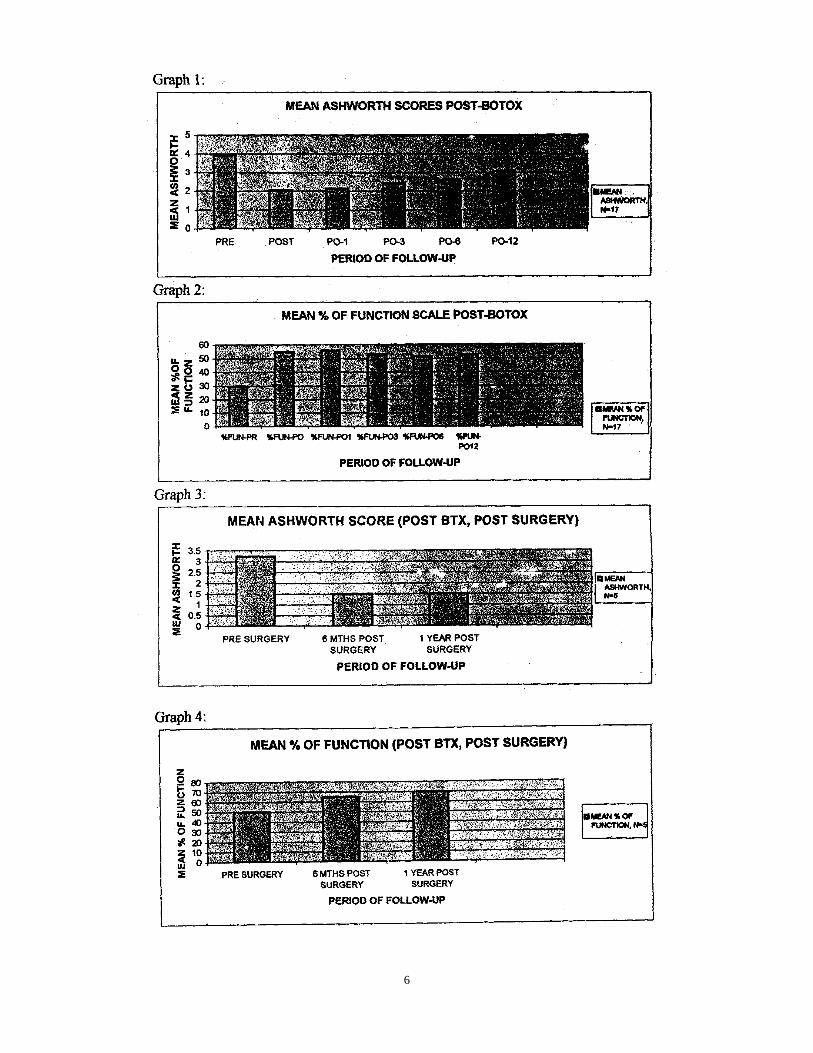
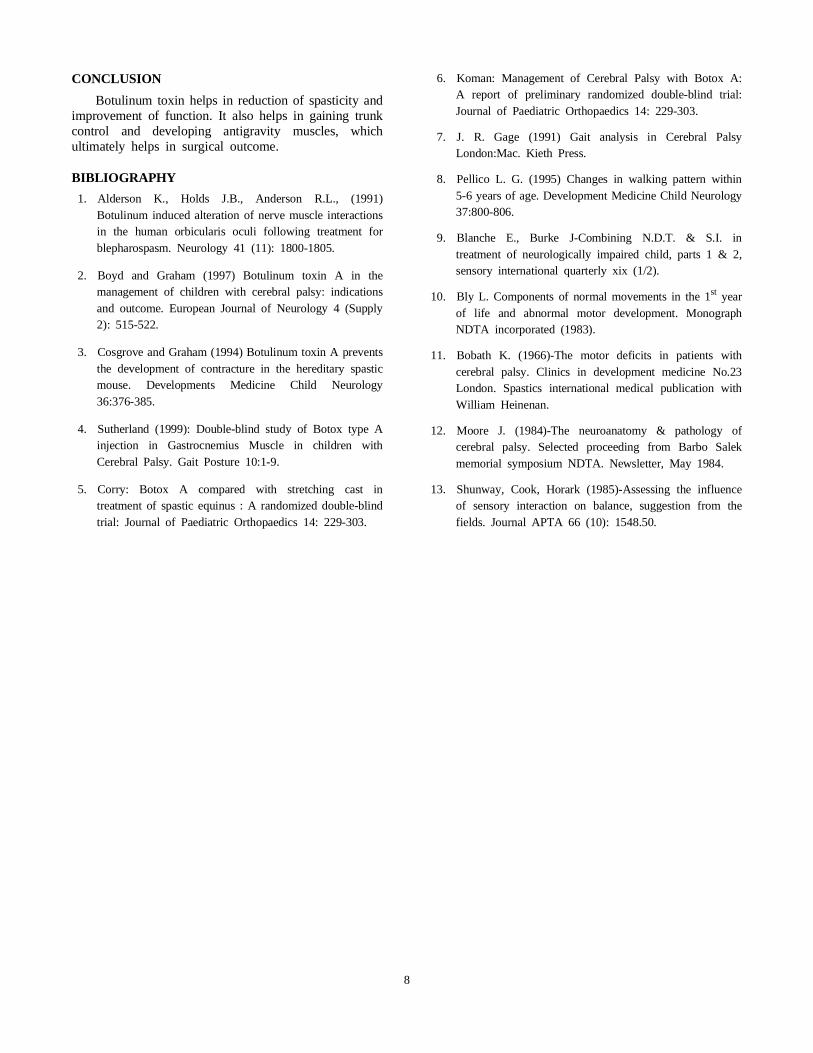
Most of our sample had never attained verticalpostures e.g., standing. Out of 17 patients, 12 wereinjected in the Hamstrings bilaterally, 8 in Gastrosoleusbilaterally, 5 in Hip flexors bilaterally, 2 in Adductorsbilaterally and 2 in gracillis bilaterally. Prebotox, thesepatients had a mean ashworth of 3.9 and post-botox 12months, the mean ashworth score was maintained at 3.07(Graph 1), trying to show that this sample did show avery early mixed picture of a dynamic and a staticcomponent. % of function improved from 29.9% to52.6% (Graph 2), trying to show that some amount ofantigravity control has improved.
Gage, 1991 advised that whenever possible, surgicalintervention should be postponed until the gait ismatured. From research (Pellico et al, 1995), it has beenconcluded that matured adult gait is achieved after theage of 6 years in normal children. Hence, for a largeproportion of our disabled children, who develop gait at
4

a very advanced age, it is advised that patients shouldreceive conservative treatment until the age of 10 years.When this conservative therapy is limited toPhysiotheraphy and Bracing, the mixed contracturesusually progress to fixed contractures and skeletaldeformation, causing severe biomechanical dysfunction.Hence in our sample, Single event multi-level surgerieswere performed after achieving some % of functionpostbotox, as shown in Graph 2. This also enable usselective training of more proximal muscle groups,which contributed to enhanced function post surgery asshown in Graph 4, which shows that % of functionimproved from 50% pre-surgery to 70% at 1 year postsurgery.
Cosgrove, 1994, stated that earlier the botox treatmentstarted, the functional and clinical outcome is much better.In our sample, it gave sufficient stability in stance, adequatestep length and energy conservation which are the basiccomponents of normal gait (Gage, 1991), which ourpatients attained post botox, post surgery.
Out of 17 patients, who were not standing pre-botox,today, post re-botox and post surgery, all of them arewalking independently or with support.
Some of the patients, n=4, needed re-botox, at anaverage interval of 1 year and 1 month, due to thepresence of primitive reflexes, reinforcement andpostural insecurity in these patients, which have beenextensively stated in the literature (Moore, 1984).
The remaining subgroup, n=8 have almost finished18 months post-botox and have achieved a status quoin their mean ashworth and % of function scales (Graph7 & 8). These patients will go for single level or multilevel or multi level surgeries. We don’t consider this tobe failure in management because the use of Botox Aenabled the more appropriate timing of Single EventMulti Level Surgery (SEMLS) after further gaitmaturation and musculo-skeletal growth has beenachieved (Boyd & Graham, 1999).
CHANGE OF ADDRESSIAP Members
Please send the change of address to the following members of executive council
To
Dr. S. Prabhu PTGeneral Secretary IAPB901, Casagrande AttovaraMangalore - 575 001.
Copy to
Dr. Subodh G. DesaiTreasurer IAPA-101, ParshavdeepNear Arjun Compl., Bhatar Road,Surat - 395 001.
Name: .........................................................................
IAP No: ......................................................................
Old Address: ..............................................................
.......................................................................................
.......................................................................................
New Address................................................................
.......................................................................................
5
6

7
CONCLUSION
Botulinum toxin helps in reduction of spasticity andimprovement of function. It also helps in gaining trunkcontrol and developing antigravity muscles, whichultimately helps in surgical outcome.
BIBLIOGRAPHY
1. Alderson K., Holds J.B., Anderson R.L., (1991)Botulinum induced alteration of nerve muscle interactionsin the human orbicularis oculi following treatment forblepharospasm. Neurology 41 (11): 1800-1805.
2. Boyd and Graham (1997) Botulinum toxin A in themanagement of children with cerebral palsy: indicationsand outcome. European Journal of Neurology 4 (Supply2): 515-522.
3. Cosgrove and Graham (1994) Botulinum toxin A preventsthe development of contracture in the hereditary spasticmouse. Developments Medicine Child Neurology36:376-385.
4. Sutherland (1999): Double-blind study of Botox type Ainjection in Gastrocnemius Muscle in children withCerebral Palsy. Gait Posture 10:1-9.
5. Corry: Botox A compared with stretching cast intreatment of spastic equinus : A randomized double-blindtrial: Journal of Paediatric Orthopaedics 14: 229-303.
6. Koman: Management of Cerebral Palsy with Botox A:A report of preliminary randomized double-blind trial:Journal of Paediatric Orthopaedics 14: 229-303.
7. J. R. Gage (1991) Gait analysis in Cerebral PalsyLondon:Mac. Kieth Press.
8. Pellico L. G. (1995) Changes in walking pattern within5-6 years of age. Development Medicine Child Neurology37:800-806.
9. Blanche E., Burke J-Combining N.D.T. & S.I. intreatment of neurologically impaired child, parts 1 & 2,sensory international quarterly xix (1/2).
10. Bly L. Components of normal movements in the 1st yearof life and abnormal motor development. MonographNDTA incorporated (1983).
11. Bobath K. (1966)-The motor deficits in patients withcerebral palsy. Clinics in development medicine No.23London. Spastics international medical publication withWilliam Heinenan.
12. Moore J. (1984)-The neuroanatomy & pathology ofcerebral palsy. Selected proceeding from Barbo Salekmemorial symposium NDTA. Newsletter, May 1984.
13. Shunway, Cook, Horark (1985)-Assessing the influenceof sensory interaction on balance, suggestion from thefields. Journal APTA 66 (10): 1548.50.
8

EXTRACRANIAL CAUSES FOR HEAD PAIN: CLINICALIMPLICATIONS FOR THE PHYSICAL THERAPIST
Dr. DeepakSebastian B.P.T., PGDR, MHS. PT., MTC, DrPT.
Physical Therapist, Alternative Rehab Inc, Clinical Lab InstructorWayne State University, Detroit, Michigan.
Abstract
The clinical presentation of a myogenic headache is thought to be predominantly musculoskeletal,however, the portrayal may be variable. The exact reason is many times unknown. The fact that thepredominant cause for the dysfunction is often missed is probably due to the inadequacy of evaluationprocedures. This often renders the condition chronic. This literature review brings to light the intricacyof the musculoskeletal causes for this category of headaches. The focus is to create an awareness inthe clinician that the musculoskeletal cause may many times be missed due to the specificity of thedysfunction. An informed clinician may be in a situation to identify the dysfunction from amusculoskeletal perspective and break the continuity of persistence by appropriate management. Thepsychological and autonomic components warrant attention.
Key Words: Headache, Myogenic, Sub Occipital, Sub Cranial, Manual Therapy.
INTRODUCTION
Physical Therapists treat neuromusculoskeletaldysfunction as it determines their scope of practice. Theyare confronted with neuromusculoskeletal dysfunction ofthe limbs and the trunk and the intricacy of treatmentprocedures have considerably increased. This can beattributed to new knowledge on specific joint mechanicsof the extremities and the spine. The cranium or theskull, however, is often viewed as a neural structurewhich it is in actuality, as it lodges the most complexneural structure of the body. However, it’smusculoskeletal implications should not be ignored.
Headaches are a common affliction but have alwaysbeen within the realm of the medical practitioner. Therole of the physical therapist in the management ofheadaches have only recently been identified and has ledsubsequently to the recognition of headaches of amusculoskeletal origin. It has been described that thedifferential diagnosis of a headache is one of the longestin medicine, and the classification so elaborate that asmany as 300 different types of headache have beenidentified. For purpose of simplification, Makofsky1hasdescribed the more common types of headaches fromthe International Headache Society (which describesabout 13 categories and 64 subcategories) classificationsystem as:
1. Migraine without aura (common migraine)
2. Migraine with aura (classic migraine)
3. Tension type headaches (myogenic or musculoskeletal)
4. Tension-Migraine (mixed headache disorder)
5. Recurring headaches of a non-musculoskeletalnature
6. Headaches as symptoms of ominous disease
From the above classification the one most relevantto the physical therapist from a management perspectiveare the tension type headaches or myogenic headaches.The pathological origin of these headaches are frommusculoskeletal structures outside of the cranium andhence considered as an extracranial cause. Appropriatediagnosis and intervention can significantly minimizesymptoms and the chronicity of recurrences. Theidentification of it’s nature of occurrence is indeed ofimportance to the physical therapist and hence thepurpose of this literature review.
Relevant Anatomy
The cervical spine consists of seven vertebralsegments, numbered C1 to C7. Superiorly they attachto the occiput of the cranium and inferiorly to the firstthoracic segment. C1 is termed the ’atlas’ and C2 the’axis’. The mechanics of the atlas and axis differ fromthe rest of the cervical segments and hence classifiable.Since the axis and atlas are closer to the occiput of thecranium, and function together, they are termed as thesub occipital or sub cranial spine2. The rest are termedthe mid and lower cervical spine. The purpose of thisclassification is for the fact that the difference inanatomy and mechanics in the two regions has rendereda difference in their clinical relevance as well. As muchas the mid cervical area is known to refer symptomsinto the upper extremities, the sub cranial area has beenidentified as a source for referred pain into the head7.Hence, they along with their muscle attachments are
9

described as the source for musculoskeletal or‘myogenic’ headaches.
The Sub Occipital Triangle
The sub occipital triangle2 is formed by thearrangement of the small muscles related to the occiput,atlas and the axis. In the midline are the rectus muscles:
1 The rectus capitis posterior minor, and2. The rectus capitis posterior major
The rectus capitis minor arises from the posteriorarch of the atlas and inserts into the occiput. The rectuscapitis posterior major arises from the spine of the axisand ascends to the occiput. Lateral to the recti are theobliquus muscles:
3. The obliquus capitis superior, and4. The obliquus capitis inferior.
The large inferior oblique muscle arises form thespinous process of the axis and adjacent lamina andattaches to the transverse process of the atlas. Thesuperior oblique muscle arises from the transverseprocess of the atlas and runs superiorly to attach to theocciput.
The two recti draw the head backwards and theobliquus superior also draws the head backwards. Thesub-occipital muscles also rotate the head, the rectuscapitis posterior major and the obliquus capitis inferiorto the same side and the obliquus capitis superior to theopposite side.
The posterior division of the second cervical nerveemerges from the spinal canal between the posterior archof the atlas and the lamina of the axis, below the inferiorobliquus. It supplies a twig to this muscle and receives
a communicating filament from the first cervical nerve.It then divides into an internal and external branch.
The internal branch, called the Greater OccipitalNerve ascends obliquely inwards between the obliquusinferior and the complexus. It pierces the latter muscleand the trapezius near their attachment to the cranium.It is now joined by a filament from the posterior divisionof the third cervical nerve, and ascending on theposterior part of the head with the occipital artery,divides into two branches, which supply the integumentof the scalp as far forwards as the vertex communicationwith the Lesser Occipital Nerve. It gives off an Auricularbranch to the posterior part of the ear and a muscularbranch to the complexus.
Etiopathology
The occipital nerve is of clinical significance as itis the irritation of the occipital nerves that result inheadache, by virtue of their supply to the integument ofthe scalp. The pain typically occurs behind the head(occiput), vertex and the temporal areas. The irritationoccurs secondary to a dysfunction of the suboccipitalmuscles, the occipitoatlanto-axial joint or both.3,15 Thereasons for dysfunctional states of the sub-occipitalmuscles and the occipto-atlanto-axial joint arepredominantly secondary to
1. Faulty posture2. Overuse/Fatigue3. Trauma
Faulty Posture and Overuse
Faulty posture may be the result of a naturaltendency or occupational stress. Commonly seen inindividuals that have a ’desk job’, performing prolongedperiods of typing, reading, computer programming etc.The forward head posture 4,15 is often times the root ofthe problem and is seen in individuals either as a habit,slouching, or wearing bifocals where they extend theirsub-cranial spine to view through their glasses.
10
The nature of the dysfunction is that, to maintainthe head in neutral, there occurs a backward bending inthe sub cranial spine. This causes the sub-occipitalmuscles to contract and the occipito-axial joints (OAA)to become restricted in that position. The end results isan irritation of the occipital nerve giving rise toheadaches.
The function of the sub-occipital musculature todraw the head backwards also increases theirvulnerability to dysfunction. Prolonged flexion of thehead for extended periods of time, as a surgeon or awriter would do for example (looking down on theoperating table or the desk), can fatigue the sub-occipitalmuscles. The immediate response to excessive fatigue isa contraction, which can be continual in occupationalsituations. This results in dysfunctional states of thesub-occipital musculature and the sub cranial joints byvirtue of their attachment to them. This can subsequentlyirritate the occipital nerves and result in a myogenicheadache.
Trauma
The commonest cause for trauma and subsequentirritation of the sub cranial area are whiplash injuries.Often occurs secondary to being hit from behind by amoving vehicle or being violently pushed from behind.The resultant momentum causes the head to violentlysnap back into extension and subsequently flexion. Thisresults in trauma of the suboccipital and cervical musclesand the facet joints of the occipito-atlanto-axial complex.
The previous causes described were secondary tofatigue and overuse, however, whiplash injuries causeactual trauma to the sub-occipital musculature and thefacet joints of the subcranial spine. They hence resultin a wider array of symptoms, making their managementrelatively difficult.
Owing to the strain of the facet capsule andsubsequent muscle guarding, the joints of the subcranialcomplex can exhibit a greater deal of restriction and painwith more intense headaches. The sub-occipital musclesare intimately related physiologically to the extrinsic andintrinsic ocular muscles and other neck and trunkmusculature. Hence, pain in the region of the eye is acommon feature. Proprioceptive impulses from them areconveyed (over the first and second spinal nerves) tothe upper cord and thence redistributed to appropriatestations at the segmental and suprasegmental levels. Thedirection of gaze, the visual axes and accompanyinghead, neck and trunk posturing are produced andmaintained by movement and fixations, among whichthese small suboccipital muscles play a major role. Theprincipal interconnecting pathways between ocular andneck musculature include the medial longitudinalfasciculi and the reticular substance of the brain stem,both of which receive proprioceptive, exteroceptive andinteroceptive modalities essential for the integration and
regulation of external orientation and internalhomeostasis. These brainstem and cord functions guideand are governed by higher stations of neural integration,including the neuropsychic levels. It is not surprising,therefore, that disturbances of equilibrium and autonomicfunctions, both subjective and objective occur in atraumatic situation since deep pain in the neck and head,together with evidence of cervical muscle spasm andhead and neck alignment changes are prominent featuresin whiplash injuries5.
It may be of value to add that these symptoms arenot only seen in whiplash situations, but also inprolonged and chronic overuse/fatigue syndromes of thesubcranial spine.
Their occurrence in whiplash injuries however, arerelatively more common.
Evaluation
The symptoms of a myogenic headache arerecognizable and the condition is diagnosed with aproper history and physical examination. When thepossibility of a vascular or a traction cause is ruled out,the specificity of the physical exam, especially of thesub cranial spine, is essential.
The headache usually starts at the neck and theoccipital area and radiates to the vertex, the temporalareas and sometimes into the eye. There usually is ahistory of postural stress secondary faultymechanics,fatigue and overuse and in some instances ahistory of trauma of a whiplash type. Anxiety andemotional stress are also some common features. Theyoften mention a feeling of a tight band around the headand neck and sometimes a throbbing sensation as well.The pain may be brought about by activity involvingfaulty mechanics, as in front of their computer or desk,and depending on the severity may start sooner after theactivity is initiated or later during the day as fatiguesets in. They may present with a forward head, roundedshoulders type of a posture and may also wear bifocals.In many instances a decrease in the severity of thesymptoms is experienced by pausing the stressful activityand resting by laying down. The neck often feels stiffwith a certain tightness felt around the neck muscles.Tenderness can be noted in the suboccipital area, theTrapezius and the Sternomastoid5. Weakness is oftennoted in the short cervical muscles and the postural andphasic muscles of the cervico thoracic area. There maybe a previous history of cervico thoracic or atemporomandibular dysfunction.
A clearer understanding of the sub cranial mechanicsis a mandatory precursor for evaluation. Failure tounderstand the mechanics may often result in thedysfunction being missed, resulting in persistence ofsymptoms. It is of a basic understanding that thesubcranial spine comprises the occipito atlanto joints
11
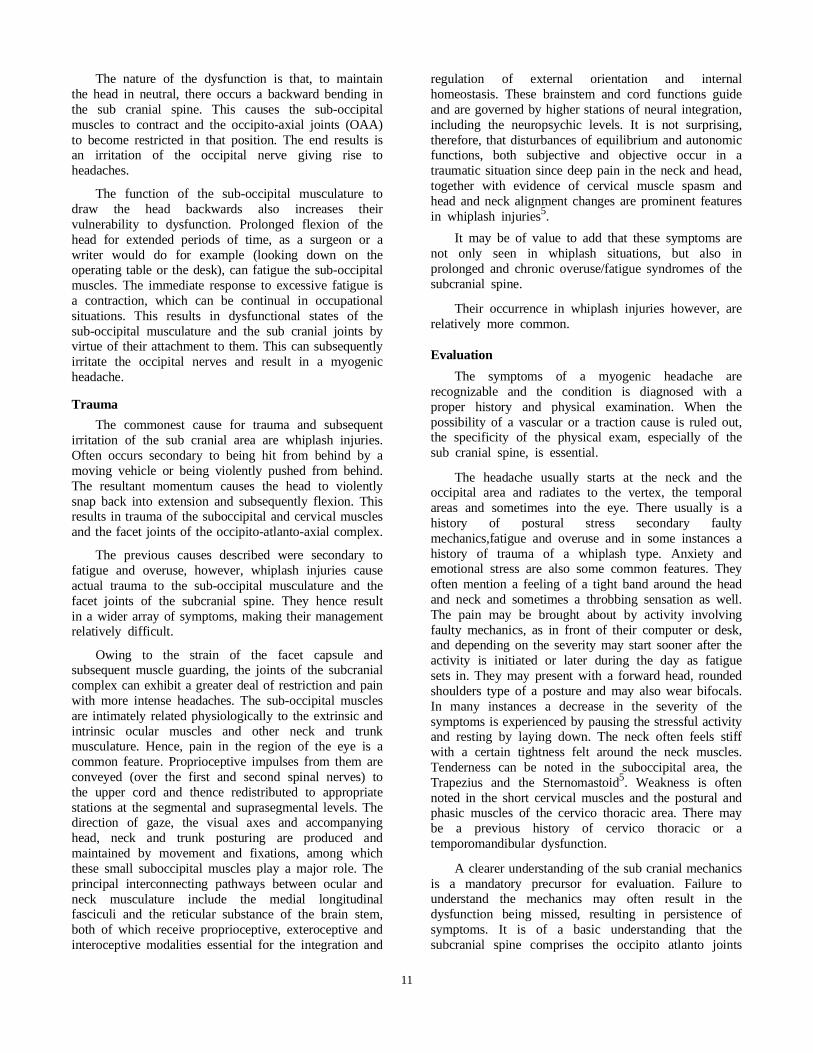
(OA) and the atlanto axial joints (AA). The movementsthat occur in the OA joints are forward and backwardnodding, (not bending) and that of the AA joints,rotation.
1. 45 degree orientation of cervical facet joints
The orientation of the mid cervical facet joints areabout 45 degrees. Rotation occurs when one facet slidesup and conversely the opposite slides down. As anexample, for left rotation to occur the right facet slidesup and the left facet slides down. By virtue of their 45degree orientation, sidebending also occurs in the samemanner. Then left sidebending is caused by the rightfacet sliding up and the left facet sliding down.
To analyze sidebending more intricately, (with thefacet joints are aligned at a 45 degree angle) if leftsidebending causes the right facet to slide up and theleft facet to slide down then technically the face shouldbe looking down to the left shoulder.
However, the face is always looking straight ahead.
This is a confounding situation, but this is wherethe sub cranial mechanics comes in to play. The reasonfor the head to look straight and forward duringsidebending is because, for every degree of sidebendingthat occurs in the mid cervical spine, a relativerotation in the opposite direction occurs in the subcranial spine6.
Thus, on examination of cervical spine range ofmotion, the gross motion of rotation is technically whatwe see as also occurring in the mid cervical spine. Tolocalize movement to the sub cranial spine, the midcervical spine, the mid cervical spine is first side bentto one side and (hence locked) then rotated to theopposite side. This tests movement at the sub cranialspine or the atlanto-axial joint. A restriction in AAmovement is indicative of sub cranial restriction.
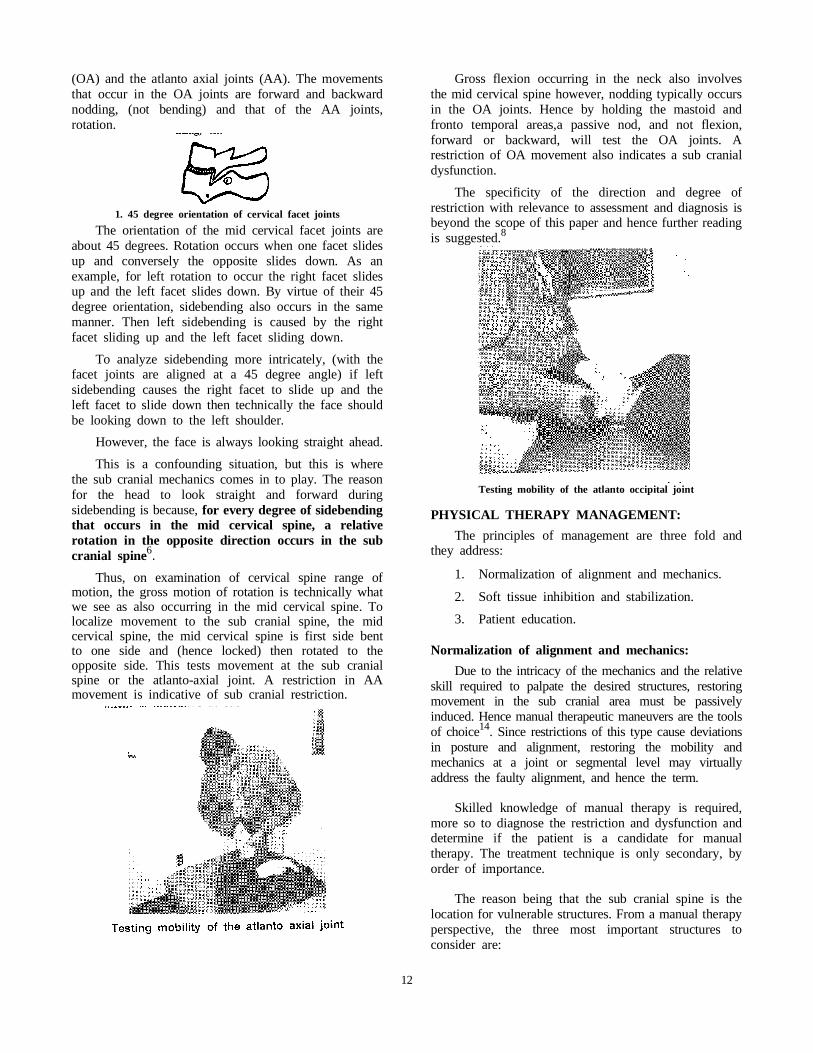
Gross flexion occurring in the neck also involvesthe mid cervical spine however, nodding typically occursin the OA joints. Hence by holding the mastoid andfronto temporal areas,a passive nod, and not flexion,forward or backward, will test the OA joints. Arestriction of OA movement also indicates a sub cranialdysfunction.
The specificity of the direction and degree ofrestriction with relevance to assessment and diagnosis isbeyond the scope of this paper and hence further readingis suggested.8
Testing mobility of the atlanto occipital joint
PHYSICAL THERAPY MANAGEMENT:
The principles of management are three fold andthey address:
1. Normalization of alignment and mechanics.
2. Soft tissue inhibition and stabilization.
3. Patient education.
Normalization of alignment and mechanics:
Due to the intricacy of the mechanics and the relativeskill required to palpate the desired structures, restoringmovement in the sub cranial area must be passivelyinduced. Hence manual therapeutic maneuvers are the toolsof choice14. Since restrictions of this type cause deviationsin posture and alignment, restoring the mobility andmechanics at a joint or segmental level may virtuallyaddress the faulty alignment, and hence the term.
Skilled knowledge of manual therapy is required,more so to diagnose the restriction and dysfunction anddetermine if the patient is a candidate for manualtherapy. The treatment technique is only secondary, byorder of importance.
The reason being that the sub cranial spine is thelocation for vulnerable structures. From a manual therapyperspective, the three most important structures toconsider are:
12
1. The vertebral artery.
2. The alar ligament.
3. The transverse ligament.
The vertebral artery is a source of vascular supplyto the brain and it is reported that forceful or faultymaneuvers of the sub cranial spine in a patient withvertebral artery compromise can result in a stroke andsometimes death9.
The alar and transverse ligaments reinforce andstabilize the odontoid process2 (Dens) of the axis. Laxityof these ligaments, are seen in traumatic (whiplash) ordisease states (rheumatoid). Failure to identify theintegrity of these ligaments may result in compressionof neural structures like the foramen magnum or thespinal cord, secondary to an improper manual therapydiagnosis or technique.
Given the fact that all contraindications are ruledout, the appropriate manual therapy diagnosis willdetermine the direction of restriction of any or all ofthe movements of the sub cranial spine. The appropriatemanual therapy technique will restore mobility andmechanics in the sub cranial spine, decreasing stress onthe sub occipital musculature and the occipital nerves.The result may be a decrease in the intensity of therelevant headache. Details of the techniques are beyondthe scope of this paper and hence further reading issuggested8.
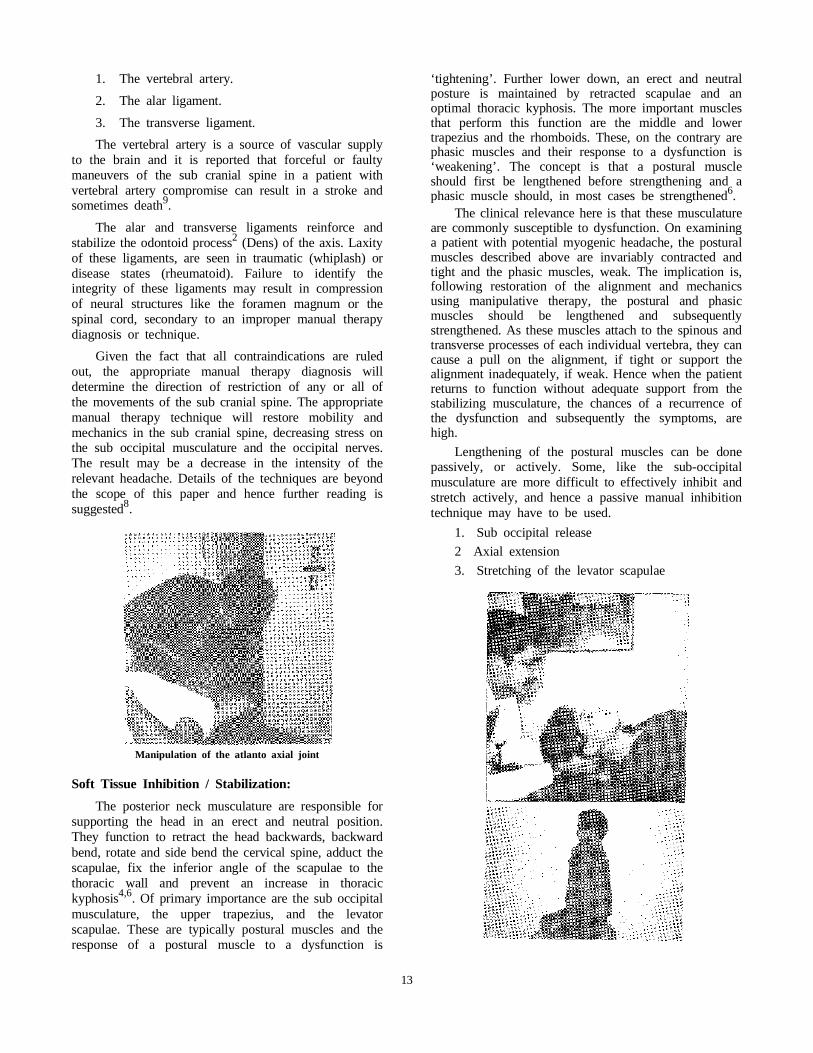
Manipulation of the atlanto axial joint
Soft Tissue Inhibition / Stabilization:
The posterior neck musculature are responsible forsupporting the head in an erect and neutral position.They function to retract the head backwards, backwardbend, rotate and side bend the cervical spine, adduct thescapulae, fix the inferior angle of the scapulae to thethoracic wall and prevent an increase in thoracickyphosis4,6. Of primary importance are the sub occipitalmusculature, the upper trapezius, and the levatorscapulae. These are typically postural muscles and theresponse of a postural muscle to a dysfunction is
‘tightening’. Further lower down, an erect and neutralposture is maintained by retracted scapulae and anoptimal thoracic kyphosis. The more important musclesthat perform this function are the middle and lowertrapezius and the rhomboids. These, on the contrary arephasic muscles and their response to a dysfunction is‘weakening’. The concept is that a postural muscleshould first be lengthened before strengthening and aphasic muscle should, in most cases be strengthened6.
The clinical relevance here is that these musculatureare commonly susceptible to dysfunction. On examininga patient with potential myogenic headache, the posturalmuscles described above are invariably contracted andtight and the phasic muscles, weak. The implication is,following restoration of the alignment and mechanicsusing manipulative therapy, the postural and phasicmuscles should be lengthened and subsequentlystrengthened. As these muscles attach to the spinous andtransverse processes of each individual vertebra, they cancause a pull on the alignment, if tight or support thealignment inadequately, if weak. Hence when the patientreturns to function without adequate support from thestabilizing musculature, the chances of a recurrence ofthe dysfunction and subsequently the symptoms, arehigh.
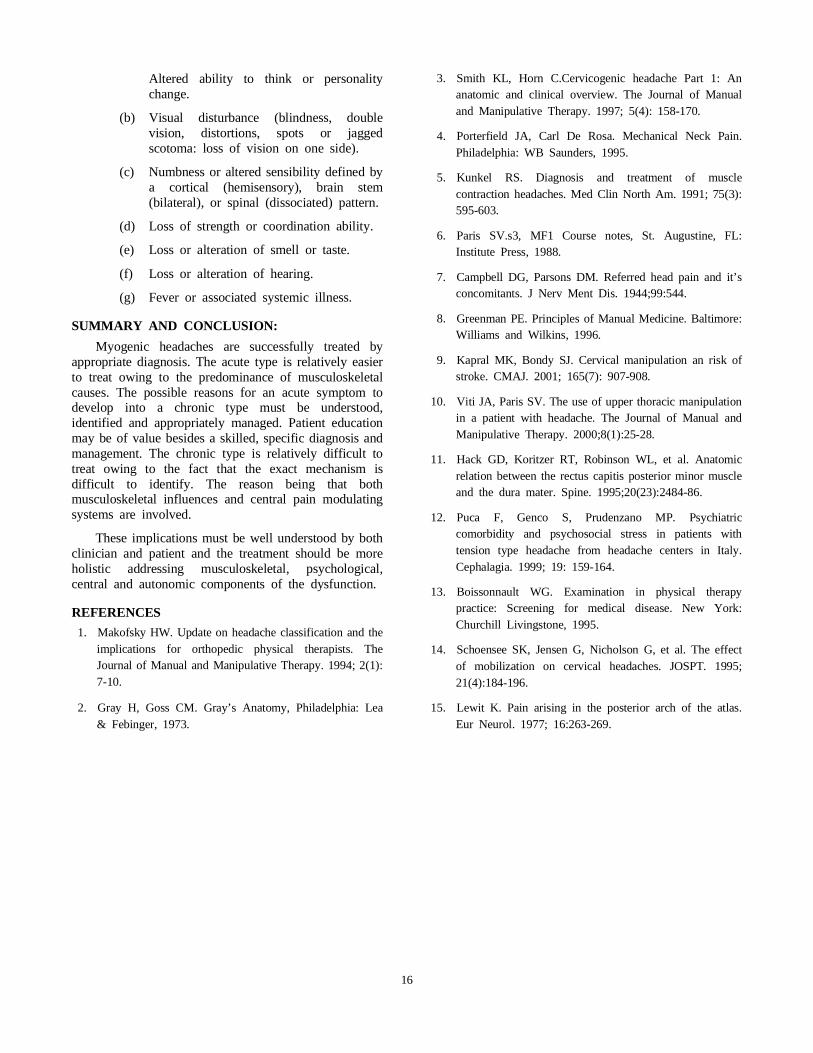
Lengthening of the postural muscles can be donepassively, or actively. Some, like the sub-occipitalmusculature are more difficult to effectively inhibit andstretch actively, and hence a passive manual inhibitiontechnique may have to be used.
1. Sub occipital release
2 Axial extension
3. Stretching of the levator scapulae
13

The phasic muscles should be routinely strengthenedand these should be incorporated into the patient’s homeprogram and practiced indefinitely if the patient wishesto continue the type of work he or she does. It may beof benefit to address the endurance component whiletraining the relevant musculature, which may correlateto their nature of function.
Strengthening upper and mid back retractors
Patient Education
This is the most important component of themanagement triad. Often it is the lack of awareness ofthe mechanical hazards that lead to the problem. Thepatient needs to be clearly explained as to how the neckand the neck musculature function and how faultyposture can stress the joints of the spine, tighten andweaken the supporting musculature and subsequentlycause a dysfunction. He or she should be aware of theimportance of continuation of their respective homeprograms incorporating active stretching of the posturalmuscles and subsequently strengthening of the phasicand postural muscles, to maintain neutral alignment.
The headaches of a myogenic origin are intense.Any head pain of a high and persistent intensity cancreate a certain anxiety in the patient for fear of a majorpathology as in a space occupying lesion or tumor. Theanxiety component can further aggravate the symptomsas the musculature contracts even further. Henceeducating the patient can minimize this anxietycomponent and help decrease the intensity of symptoms.Other personal reasons for anxiety may warrant referralto a psychologist or psychiatrist.
Due to it’s subjective nature, each patient should beindividually questioned regarding their possible stressors.If their computer monitor is below head level, then itshould be set at eye level to minimize constant flexionof the neck. Frequent interruptions with two or threestretches of the cervical musculature and subsequentresumption of activity should be advised to maintain thelength of the muscle, especially in people that spendexcessive periods of time looking down at work.
If the patient wears bi-focals, where there is atendency to have a forward head posture, the patientshould be advised to use separate glasses for readingand normal viewing, if feasible. If there are otherpersonal stressors in their lives, appropriate help mustbe sought. Overall proper rest, nutrition, diet andexercise may help maintain the elasticity and resilienceof connective tissue and minimize the vulnerability toinjury.
Variations
The Thoracic Spine:
The upper thoracic region has also been identifiedas a source for headaches and significant reduction insymptoms have been identified by addressing this areain potential patients10. The theories propounded to justifythe relationship are as follows:
1. Forward bending of the thoracic spine,especially T1 and T2 can significantly increasebackward bending in the sub cranial spinecausing a forward head posture andsubsequently the symptoms that go with it.
14

2. The semispinalis capitis arises from thetransverse processes of C7 and T1-6 or 7 andinserts into the inferior and superior nuchal lineof the occiput. The Greater Occipital nervepierces it near it’s attachment to the occipitalbone. Reflex relaxation of this muscle byincorporating a high velocity manipulationcould potentially decrease nerve compression.
Manipulation of the upper thoracic spine
The Rectus Capitis Posterior Minor and the DuraMater:
In the sub occipital triangle, the rectus capitisposterior minor (RCPM) and the posterior atlantooccipital membrane (PAO) are connective tissue bridge.The PAO has been described as being intimatelyattached to the underlying spinal dura. When the headand neck are extended, the spinal dura has a tendencyto fold inward toward the spinal cord. The in foldingof the dorsal spinal dura is prevented by the increasedelasticity of the dorsal dura. It is suggested that theconnective tissue bridge may assist in resisting dural infolding. Dysfunctional states of the RCPM couldpotentially compromise this mechanism11. This indicatesthat the sub occipital muscles may have a directinfluence on the dura mater, a pain sensitive structure,suggesting an alternative mechanism of pain generationfor cervical headaches.
Psychological and Autonomic influences:
Chronicity and persistence of symptoms inmyogenic headaches may be due to
1. Failure to identify the intricate musculoskeletalcomponent of the dysfunction at a sub cranialand upper thoracic level.
2. Unidentified psychological stressors that canhave a direct and prolonged influence on themusculoskeletal component.
3. The central and autonomic influences on thepersistent and repetitive chronic nature of thepain due to unidentified etiology.
Although the musculoskeletal component hasreceived considerable attention in this category ofheadaches the psychological and autonomic influenceswarrant attention. Psychological comorbidity and changesin autonomic function have been identified in patientswith myogenic headaches. Reasons are attributed toinfluences at a brainstem or central level and also at athoracic level due to the origin of sympatheticinnervations to the head and neck5,10. Appropriatediagnosis and identification of stressors and theirmanagement which may include but not limited tocounselling, bio feedback, relaxation and breathing, etc,have been suggested.
WARNING SIGNS:
Physical therapists are increasingly confronted bypatients with headache or facial pain as a consequenceof musculoskeletal system dysfunction. When a patientapproaches a physical therapy clinic with symptoms ofhead pain the clinician should be aware of situationswhere the pain may not be of a musculoskeletal origin.Astute observation for signs that may not be of amusculoskeletal origin may aid the physical therapyclinician to make a meaningful referral to a medicalpractitioner to optimize outcomes. The following aresome of the more important warning signs that maywarrant a medical referral13.
1. Headaches that worsen with activity or exertion.
2. Headaches that begin suddenly and that areimmediately severe and generalized in location.
3. Headaches that begin after lying down,especially if they awaken the patient from sleep.
4. Headaches associated with projectile vomiting,but no nausea.
5. Headaches that begin with, or remain as,unilateral pulsating pain in synchrony with heartbeat.
6. Focal tenderness over the temporal artery in anypatient past the age of 60.
7. Sudden, intense, lancinating, brief pain that iseither spontaneous or triggered by a mildstimulus.
8. Intense pain localized over a sinus or aroundthe teeth.
9. Headaches associated with other symptoms
(a)
15
Altered ability to think or personalitychange.
(b) Visual disturbance (blindness, doublevision, distortions, spots or jaggedscotoma: loss of vision on one side).
(c) Numbness or altered sensibility defined bya cortical (hemisensory), brain stem(bilateral), or spinal (dissociated) pattern.
(d) Loss of strength or coordination ability.
(e) Loss or alteration of smell or taste.
(f) Loss or alteration of hearing.
(g) Fever or associated systemic illness.
SUMMARY AND CONCLUSION:
Myogenic headaches are successfully treated byappropriate diagnosis. The acute type is relatively easierto treat owing to the predominance of musculoskeletalcauses. The possible reasons for an acute symptom todevelop into a chronic type must be understood,identified and appropriately managed. Patient educationmay be of value besides a skilled, specific diagnosis andmanagement. The chronic type is relatively difficult totreat owing to the fact that the exact mechanism isdifficult to identify. The reason being that bothmusculoskeletal influences and central pain modulatingsystems are involved.
These implications must be well understood by bothclinician and patient and the treatment should be moreholistic addressing musculoskeletal, psychological,central and autonomic components of the dysfunction.
REFERENCES
1. Makofsky HW. Update on headache classification and theimplications for orthopedic physical therapists. TheJournal of Manual and Manipulative Therapy. 1994; 2(1):7-10.
2. Gray H, Goss CM. Gray’s Anatomy, Philadelphia: Lea& Febinger, 1973.
3. Smith KL, Horn C.Cervicogenic headache Part 1: Ananatomic and clinical overview. The Journal of Manualand Manipulative Therapy. 1997; 5(4): 158-170.
4. Porterfield JA, Carl De Rosa. Mechanical Neck Pain.Philadelphia: WB Saunders, 1995.
5. Kunkel RS. Diagnosis and treatment of musclecontraction headaches. Med Clin North Am. 1991; 75(3):595-603.
6. Paris SV.s3, MF1 Course notes, St. Augustine, FL:Institute Press, 1988.
7. Campbell DG, Parsons DM. Referred head pain and it’sconcomitants. J Nerv Ment Dis. 1944;99:544.
8. Greenman PE. Principles of Manual Medicine. Baltimore:Williams and Wilkins, 1996.
9. Kapral MK, Bondy SJ. Cervical manipulation an risk ofstroke. CMAJ. 2001; 165(7): 907-908.
10. Viti JA, Paris SV. The use of upper thoracic manipulationin a patient with headache. The Journal of Manual andManipulative Therapy. 2000;8(1):25-28.
11. Hack GD, Koritzer RT, Robinson WL, et al. Anatomicrelation between the rectus capitis posterior minor muscleand the dura mater. Spine. 1995;20(23):2484-86.
12. Puca F, Genco S, Prudenzano MP. Psychiatriccomorbidity and psychosocial stress in patients withtension type headache from headache centers in Italy.Cephalagia. 1999; 19: 159-164.
13. Boissonnault WG. Examination in physical therapypractice: Screening for medical disease. New York:Churchill Livingstone, 1995.
14. Schoensee SK, Jensen G, Nicholson G, et al. The effectof mobilization on cervical headaches. JOSPT. 1995;21(4):184-196.
15. Lewit K. Pain arising in the posterior arch of the atlas.Eur Neurol. 1977; 16:263-269.
16

A COMPARATIVE STUDY OF THE EFFICACY OFIONTOPHORESIS AND PHONOPHORESIS IN THE
TREATMENT OF SHIN SPLINT
Amarjeet Singh*, G.B. Sethy**, J.S. Sandhu*, A.G.K. Sinha**Department of Sports Medicine and Physiotheraphy, Guru Nanak Dev University, Amritsar (Punjab), India.
**Sports Authority of India, Western Centre, Gandhinagar, Gujrat.
Abstract
Clinical use of iontophoresis and phonophoresis with different medications in the treatment of shinsplints is limited. Comparison of the efficacy of iontophoresis and phonophoresis with diclofenac sodium(1%) in the treatment of shin splints were examined in this study. Twenty five athletes with shin splintsof the age group 18-29 years were randomly divided into two groups: Ionto group (N=13) and Phonegroup (N=12). Diclofenac sodium (1%) was used for Iontophoresis (5 mA, 15 min) and
Phonophoresis (1W/cm2 , 10 min). Treatment was given 5 times in a week for a period of 2 weeks.The recovery from pain and function was judged by recording VAS and functional score on 7th and14th day of treatment. No significant differences were noted when ionto group compared with phonogroup.
Keywords: Shin splints, Iontophoresis, Phonophoresis, Diclofenac-sodium, Non-steroidal anti-inflammatorydrug (NSAID).
INTRODUCTION
Multiple pharmaceutic methods exist for deliveringmedications transcutaneously. Apart from injection, useof alternative methods like iontophoresis (withelectromotive force) and phonophoresis (with mechanicalforce) is very common. These methods avoid adverseeffects of oral administration of the same agents and alsoprovide the potential for localized delivery to the tissuesunderlying the site of application. The pharmacologicagents that have been transcutaneously administered forlocal tissue anti-inflammatory effects include steroidaland non-steroidal drugs1. Diclofenac sodium is a NSAID(Non-steroidal anti-inflammatory drug) and has goodanti-inflammatory analgestic potency.
Shin splints is a poorly understood condition, whichcommonly afflicts long distance runners, joggers,jumpers and aerobic dancers. Otherwise called exerciseinduced leg soreness, this refers to inflammation ofmuscles, tendons and periosteum of the lower leg. Asper the American Medical Association (1966)2 thediagnosis of shin splints should be limited tomusculo-skeletal inflammation excluding stress fracturesand ischaemic disorders. There is typical clinicalpresentation of pain and tenderness along the anterioror posteromedial border of tibia and all weight bearingactivities become painful2. The usual management ofshin splints with rest, icing and oral administration ofNSAID was found ineffective in bringing back theathlete to previous level of activity in short period.Several clinical methods have been tried to give speedy
and permanent recovery to the patient. Delacerda (1982)4
found iontophoresis with 0.5% hydrocortisone effectivein the treatment of shin splints. Smith, Winn and Parette(1986)5 in their study showed that ice, ultrasound andphonophresis are very much effective in the treatmentof shin splints. Several clinical investigations havedemonstrated positive clinical outcomes when differentanti-inflammatory drugs were delivered transcutaneouslythrough these methods. But there is scanty of supportivestudies on iontophoresis and phonophoresis. withdifferent ions for the treatment of shin splints. Thepurpose of the present study was to (1) evaluate theefficacy of iontophoresis and phonophoresis on the painand functional recovery of the patient with shin splints(2) finding out the effectivity of diclofenac sodium (1%)as NSAID in the reduction of pain and inflammation.
MATERIALS AND METHODOLOGY
Materials - Electrical stimulation machine withcontinuous direct current, ultrasound machine,Diclofenac sodium (1%) emulgel.
The present study is a randomized controlled clinicaltrial. The sample comprised of 25 patients with shinsplints in the age group of 18-29 years (Male = 16,Female = 9). They were randomly divided into twogroups - lonto group N=13 (M=9, F=4) and Phono groupN=12 (M=7, F=5). The study was conducted in sportsmedicine centre, GNDU, Amritsar (Punjab) and SportsAuthority of India, west zone centre, Gandhinagar(Gujarat). The study was approved by the Research wingof these centres and all patients approached agreed to
17

participate. Acceptable subjects were diagnosed on thebasis of consistent medical history. Physical examinationfindings and response to some provocative andfunctional tests6. Radiographs were taken only in fewsuspected cases to exclude stress fracture. Patients wereadvised rest from weight bearing activities, icing for10-12 minutes, 3-4 times in a day and no additionaltherapies were provided.
Treatment with iontophoresis and phonophoresis wasgiven 5 days per week for the period of two weeks.Iontophoresis was applied with continuous direct currentat the intensity of 5 mAmp for the period of 15 minutes.Phonophoresis was applied with continuous ultrasoundat a frequency of 1 MHz and at the intensity of 1 w/cm2
for the time period of 10 minutes. For both the treatmentmethods, diclofenac sodium (1%) gel was used.Recovery from pain was assessed by response of thepatient to a Visual Analog Scale (VAS). Functionalrecovery was judged by 6 mt. distance hop test, wherethe patient was asked to hop of the affected leg as muchdistance as possible without any pain and discomfort.VAS and functional score was recorded on 1st,7st,and14th day of treatment. The data was analyzed using ’t’test.
RESULTS
In table 1 the comparison of pain score improvementand functional score improvement between the group I(Ionto group) and group II (Phono group) from 1st - 7th
day of treatment is shown. The mean scores for groupI & group II was 1.35 & 1.17 respectively, ’t’ value of1.10 at non-significant level for pain score improvement.Whereas, the mean score for functional scoreimprovement was noted 0.81 for group I and 0.83 forgroup II respectively, with the ’t’ value of 0.26 atnon-significant level. This suggests that no significantdifference in level of improvement of pain score andfunctional score from 1st - 7th day of treatment wasnoted between Iontophoresis and Phonophoresis groupthough more improvement was noted in Ionto group forpain score.
Table 3 shows comparison in between group I(Ionto) and Group II (Phono) from 1st - 14th day forpain score and functional score improvement. The meanscore of improvement for pain score were 4.35 for groupI and 4.17 for group II, with the ’t’ value of 0.77 atnon-significant level. Whereas, the mean scores forfunctional score improvement were 2.50 and 2.54 forgroup I and group II respectively, with the ’t’ value of0.26 at non-significant level. This again suggests thattreatment with Iontophoresis and Phonophoresis does notexhibit any significant difference in pain score andfunctional score improvement from 1st - 14th day oftreatment. Iontophoresis group showed slightly better rateof improvement.
DISCUSSION
Evaluation of results showed that both iontophoresisand phonophoresis is effective in introducing themedication (Diclofenac sodium- 1%) deep into theperiosteum and adjacent musculo-tendinous structures.This supports the study of Glass et al. 19807 and Griffinand Touchstone 19688. Glass et al found that significantamount of dexamethasone penetrated into the muscles,cartilage, periosteum and joints by iontophoresis (4mAfor 20 min) on rhesus monkeys. Griffin and Touchstonereported in vitro research on swine tissue that cortisolcould be driven into skeletal muscles and paravertebralnerve by ultrasound.
Iontophoresis seems to be much effective in theinitial days than phonophoresis. This may be due to theanalgesic effect of low intensity direct current(Wadsworth & Chanmugam, 19809 andanti-inflammatory analgesic properties of the drug. Thethermal effect of continuous ultrasound may be the causefor its decreased efficacy in the initial days. In thesecond week, the healing effect of ultrasound (Dyson &Brookes. 198310 would have been the factor in therecovery of the patient.
The pathological process of shin splints involveinflammation of teno-periosteal junction and adjacentstructures; rest and icing helps to resolve theinflammatory process, continuous direct current andultrasound also assists the healing process as studied byFriedenberg et al. 197111 and Mark D. Klaiman et al.199812. The recovery of the patient by iontophoresis asobserved on 7th and 14th day support the study of Harris198213 who found 38 out of 50 patients withmusculo-skeletal conditions improved in the functionaluse of body part with iontophoresis. The efficacy ofphonophoresis support the study by Stratford PW. et al.198914 on the efficacy of phonophoresis on lateralepicondylitis of elbow.
The study shows the potential advantages ofiontophoresis and phonophoresis with diclofenac sodiummedication in the treatment of shin splints of lower leg.This is a noninvasive method and without having anyadverse effects.
CONCLUSION
Iontophoresis and phonophoresis can be usedclinically to decrease pain and inflammation and toincrease the healing of bone in the treatment of shinsplints. Both iontophoresis and phonophoresis is effectiveon the functional recovery of the patient as determinedby 6 metre. distance hop test. Transcutaneous permeationof diclofenac sodium in clinical relevant concentrationfollowing iontophoretic and phonophoretic applicationdown the periosteum and superficial musculo-tendinousstructures is possible as the result of this study shows.
18
Both VAS and 6 mt. distance hop test can be usedto monitor changes in pain level and functional recoveryof the patient. Further studies are required to find outthe efficacy of iontophoresis and phonophoresis withdifferent type of medications in the treatment of shinsplints. Pharmacokinetic and pharmacodynamicinvestigations is also required to document the clinicalvalue of anti-inflammatory drugs at these applicationsites in different clinical stages of shin splints.
ACKNOWLEDGEMENT
The Authors wish to acknowledge helping of Mr.Amit Arora for preparation of this manuscript. Also,many special thanks to Dr. P.K. Mitra, NIOH, Calcuttafor reviewing this manuscript and providing his valuableideas.
REFERENCES
1. Banga AK, Panus Pe; Clinical applications ofiontophoresis devices in rehabiliation medicine. CriticalReviews in Rehab.Med. 10: 147-179, 1998.
2. AMA subcommitte on the classification of sports injuries,standard nomenclature of athletic injuries, Chicago, 1966.
3. Oakes BW: Tibial pain or shin soreness (shin splints) -itscauses, differential diagnosis and management. In :Draper J (ed) second report on the national sportsresearch program, Austr. Sports Commission, Canberra,PP. 47-51, 1986.
4. Delacerda FG: Iontphoresis for the treatment of shinsplints.J. Orthop Sports Phys Ther 3(4) : 183-185, 1982.
5. Smith, Winn and Parette R : Comparative study usingfour modalities in shin splint treatments. J Orthop. Sports.Phys. Ther. 8: 77-80, 1986.
6. Genuario SE : Differential diagnosis : Exertionalcompartment syndrome, stress fractures and shinsplints.Ath. Training 24(1): 31-34, 1989.
7. Glass JM, Stephen RL, Jacobsen SC: The quantity anddistribution of radiolabelled dexamethasone delivered totissues by iontophoresis. Interest. J. Dermatol. 19 (9)519-525, 1980.
8. Griffin JE, Touchstone JE: Low intensity phonophoreisof cortisol in swine. Phys Ther. 48: 1336-1344, 1968.
9. Wadsworth and Chanmugam: Electrophysical agents inphysiotherapy. Marrick ville, Austr: Science press, 1980.
10. Dyson & Brookes M : Stimulation of bone repair byultrasound. In Lerski RA, Morley, P(eds) US 82,proceedings 3rd meeting world Federation of US inMedicine & Biology. Pergamon Press, Oxford, 1983.
11. Fridenberg et al: Healing of non union of the medialmalleolus by means of direct current. A case report J.Trauma, 11: 883-885, 1971.
12. Mark D. Klaiman, Joseph A. Shrader, Jerome V. Danoff,Jeanne E. Hicks, Williams J. Pesce and James Ferland:Phonophoresis versus Ultrasound in the treatment ofcommon musculo-skeletal conditions. Med. & Sc. Sportsand Exer., Vol., 30 (9) 1349-1355, 1998.
13. Harris HR : Iontophoresis - Clinical Research inmusculo-skeletal inflammatory conditions,JOSPT4:109,1982.
14. Stratford PW, Levy DR., Gauldies, et al. : The evaluationof phonophoresis and friction massage as treatment forextensor carpi radialis tendonitis : A randomized clinicaltrial, Physiotherapy Canada, 41: 93-99, 1989.
Tables
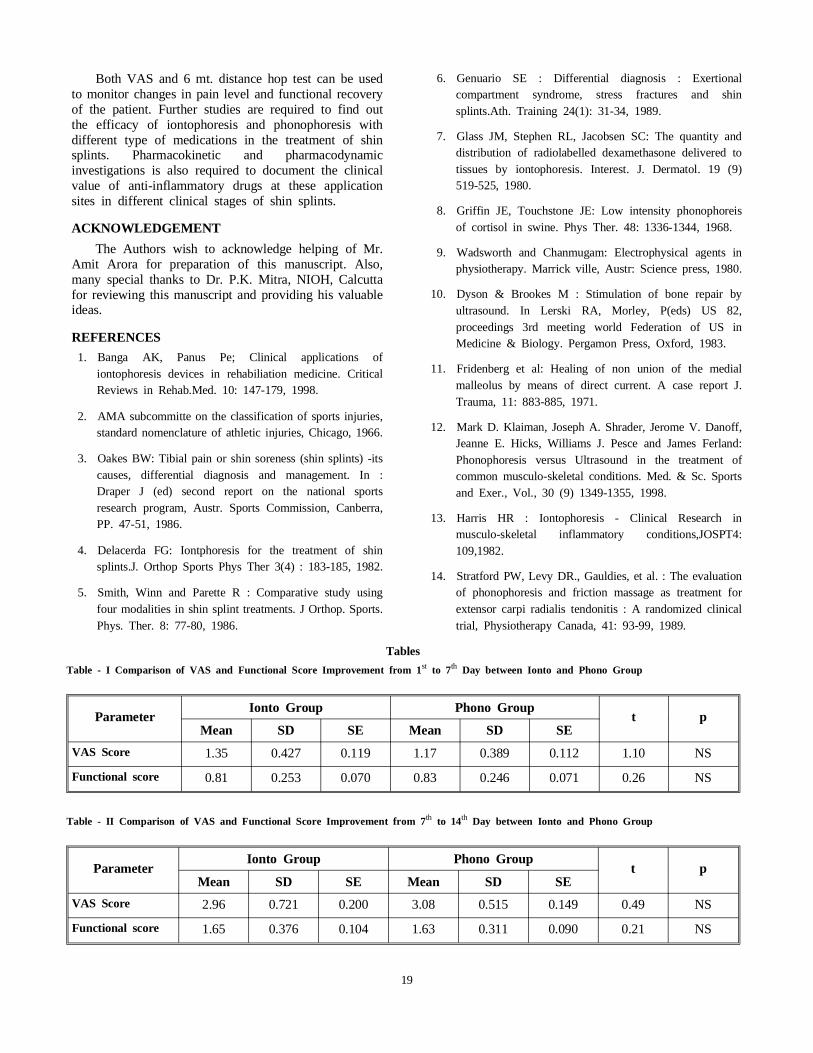
Table - I Comparison of VAS and Functional Score Improvement from 1st to 7th Day between Ionto and Phono Group
ParameterIonto Group Phono Group
t pMean SD SE Mean SD SE
VAS Score 1.35 0.427 0.119 1.17 0.389 0.112 1.10 NS
Functional score 0.81 0.253 0.070 0.83 0.246 0.071 0.26 NS
Table - II Comparison of VAS and Functional Score Improvement from 7th to 14th Day between Ionto and Phono Group
ParameterIonto Group Phono Group
t pMean SD SE Mean SD SE
VAS Score 2.96 0.721 0.200 3.08 0.515 0.149 0.49 NS
Functional score 1.65 0.376 0.104 1.63 0.311 0.090 0.21 NS
19

Table - III Comparison of VAS and Functional Score Improvement from 1st to 14th Day between Ionto and Phono Group
ParameterIonto Group Phono Group
t pMean SD SE Mean SD SE
VAS Score 4.35 0.591 0.164 4.17 0.577 0.167 0.77 NS
Functional score 2.54 0.380 0.105 2.50 0.369 0.107 0.26 NS
20
BT]X^a _P_Ta PfPaS Pc cWT #�cW =PcX^]P[ 2^]UTaT]RT ^U 8]SXP] 0bb^RXPcX^] ^U ?WhbX^cWTaP_Xbcb Pc
8]S^aT� 5TQadPah !��!
Wound area measurement in experimental Animals: Conventionalgraph paper method versus Autocad RL 14 Computer Analyses
Maiya Arun G. Kumar Praod, Nayak Shivanand.
Keywords: Wound area measurement, conventional graph method, Autocad RL 14 computer analyses.
INTRODUCTION
In Recent years increasing interest has been focusedon the technique available for assessing and measuringwound in the clinical setting. Katelaris and coworkershighlighted the lack of universally accepted method andnoted that current methods to assess healing areunsatisfactory1.
The evaluation of wounds has become a priorityfrom both research and clinical perspectives.Physiotherapists treating wounds need accurate, practicalmethods to describe and quantify the wound size if theyare to accurately characterize wound healing2. Reliablemeasurements assume particular importance for theclinician comparing the same wound on severaloccasions, and for the researcher evaluating a wound’sresponse to therapeutic interventions3. These methods areof particular interest to , and have been popularly usedby researchers to assess response to treatment during invitro animal studies4-8.
Researchers have monitored wound healing bymeans of histochemical studies, and microscopichistologic evaluation using bioassays of excised woundtissue. The macroscopic quantifications of wounds hasproven more popular for clinical studies in humans9-11.Such techniques have ranged from conventional methods(graph paper, ruler, and tracing taken from the woundsize) and photographic tracing of wound12-15.
Despite the wide range of available techniques,clinical methods that are both accurate for the researcherand minimally invasive and comfortable for the patientare lacking. Therefore we undertook this study tocompare directly two separate methods of measurement.The present study is taken to find a better method forwound area measurement in experimental animals.
MATERIAL AND METHOD
Experimental Animals 12 Wistar rats
Transperency Sheets
Graph Paper
Autocad RL 14 computer
METHODOLOGY
After research approval by the university of MAHEresearch ethical committee, the study was conducted inthe department of experimental medicine and surgery,the wistar rats with age group of 4 to 6 month withweight of 180 to 250 grams are selected for the study.The animals are divided in to two groups as study groupwith wound area measurement with conventional graphpaper method and study group with wound areameasurement with AUTO CAD RL 14 computeranalyses with six animals in each group. The animalswere fed with standard laboratory food and animals hadfree access to water. Both the group of animals wereacclimated to climate and light controlled environment.The animals were housed in cage separately andcontinuously monitored throughout the study period forany change in health.
SURGICAL PROCEDURE: The dorsal fur of theanimals were shaved. Then with aseptic precaution theanimals were anesthetised with ketamine of 2ml/kg bodyweight given intravenously. The area of wound to be
created is marked on back of animals and 2 × 2 cm2 fullthickness excisional wound is created. Then the area ofthe wound was recorded on transparency paper. All thewounds are undressed and kept open.
The measurement of the wound was taken everyalternate day on transperency paper with permanentmarker pen until the wound healed completely. Thewound was healed completely on 24th day.
Then the transparency sheet is kept over the graphpaper and the area was calculated in millimeters bycounting squared of graph paper within the markedwound area. The time taken to calculate the each woundarea measurement and area of the wound is noted.
21
In other group the wound area recorded on thetransparency paper is transferred to Autocad RL 14computer by digitizer and the time taken to calculateand area of the wound is noted.
Result: The result is statically analysed with paired ‘t’test wound area measurement with conventional graphpaper method and autocad RL 14 computer analyses
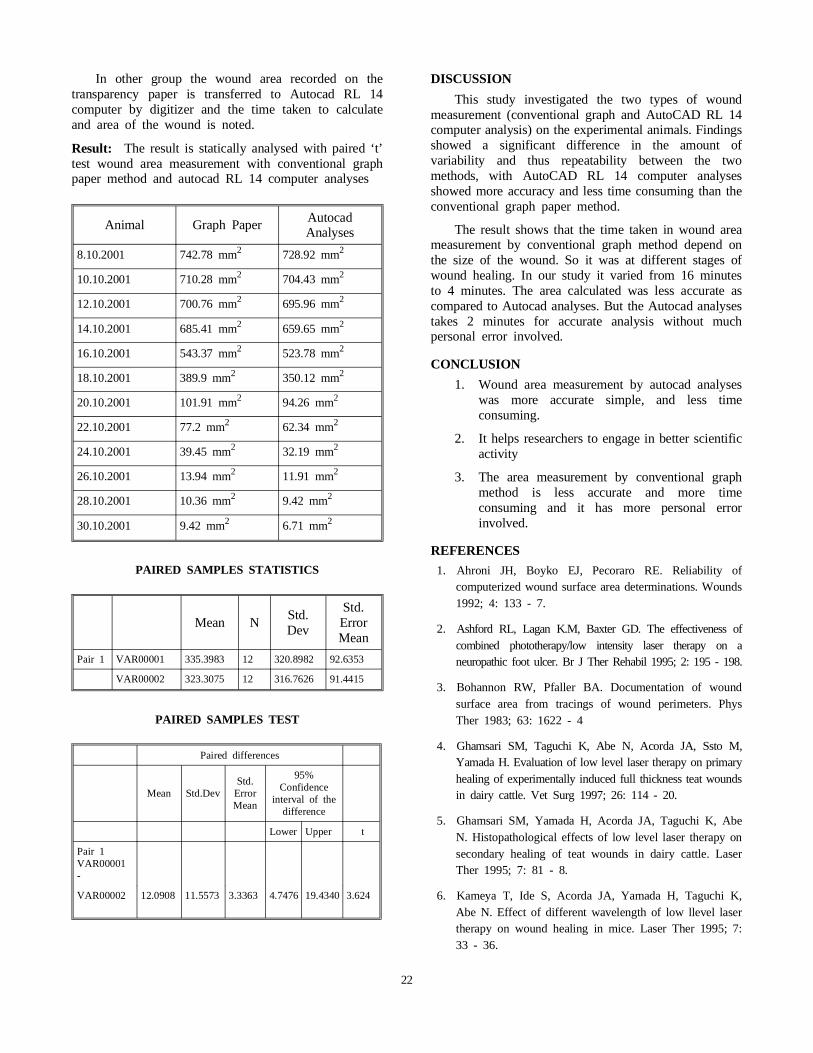
Animal Graph Paper AutocadAnalyses
8.10.2001 742.78 mm2 728.92 mm2
10.10.2001 710.28 mm2 704.43 mm2
12.10.2001 700.76 mm2 695.96 mm2
14.10.2001 685.41 mm2 659.65 mm2
16.10.2001 543.37 mm2 523.78 mm2
18.10.2001 389.9 mm2 350.12 mm2
20.10.2001 101.91 mm2 94.26 mm2
22.10.2001 77.2 mm2 62.34 mm2
24.10.2001 39.45 mm2 32.19 mm2
26.10.2001 13.94 mm2 11.91 mm2
28.10.2001 10.36 mm2 9.42 mm2
30.10.2001 9.42 mm2 6.71 mm2
PAIRED SAMPLES STATISTICS
Mean NStd.Dev
Std.ErrorMean
Pair 1 VAR00001 335.3983 12 320.8982 92.6353
VAR00002 323.3075 12 316.7626 91.4415
PAIRED SAMPLES TEST
Paired differences
Mean Std.DevStd.ErrorMean
95%Confidence
interval of thedifference
Lower Upper t
Pair 1VAR00001-
VAR00002 12.0908 11.5573 3.3363 4.7476 19.4340 3.624
DISCUSSION
This study investigated the two types of woundmeasurement (conventional graph and AutoCAD RL 14computer analysis) on the experimental animals. Findingsshowed a significant difference in the amount ofvariability and thus repeatability between the twomethods, with AutoCAD RL 14 computer analysesshowed more accuracy and less time consuming than theconventional graph paper method.
The result shows that the time taken in wound areameasurement by conventional graph method depend onthe size of the wound. So it was at different stages ofwound healing. In our study it varied from 16 minutesto 4 minutes. The area calculated was less accurate ascompared to Autocad analyses. But the Autocad analysestakes 2 minutes for accurate analysis without muchpersonal error involved.
CONCLUSION
1. Wound area measurement by autocad analyseswas more accurate simple, and less timeconsuming.
2. It helps researchers to engage in better scientificactivity
3. The area measurement by conventional graphmethod is less accurate and more timeconsuming and it has more personal errorinvolved.
REFERENCES
1. Ahroni JH, Boyko EJ, Pecoraro RE. Reliability ofcomputerized wound surface area determinations. Wounds1992; 4: 133 - 7.
2. Ashford RL, Lagan K.M, Baxter GD. The effectiveness ofcombined phototherapy/low intensity laser therapy on aneuropathic foot ulcer. Br J Ther Rehabil 1995; 2: 195 - 198.
3. Bohannon RW, Pfaller BA. Documentation of woundsurface area from tracings of wound perimeters. PhysTher 1983; 63: 1622 - 4
4. Ghamsari SM, Taguchi K, Abe N, Acorda JA, Ssto M,Yamada H. Evaluation of low level laser therapy on primaryhealing of experimentally induced full thickness teat woundsin dairy cattle. Vet Surg 1997; 26: 114 - 20.
5. Ghamsari SM, Yamada H, Acorda JA, Taguchi K, AbeN. Histopathological effects of low level laser therapy onsecondary healing of teat wounds in dairy cattle. LaserTher 1995; 7: 81 - 8.
6. Kameya T, Ide S, Acorda JA, Yamada H, Taguchi K,Abe N. Effect of different wavelength of low llevel lasertherapy on wound healing in mice. Laser Ther 1995; 7:33 - 36.
22

23

7. Kana JS, Hutschenreiter G, Haina D, Waidelich W. Effectof low power density radiation on healing of open skinwounds in rats. Arch Surg 1981; 16: 293 - 296.
8. Katelaris P, Flether JP, Little JM. A new means ofassessing healing in chronic venous ulceration. Aust N ZJ Surg 1986; 56: 99 - 102.
9. Palmar RM, Ring EFJ, Ledgard L. A digital videotechnique for radiographs and monitoring ulcers. JPhotogr Sci 1989; 37: 65 -67.
10. Plassman P, Jones BF, Measuring leg ulcers by colorcoded structured light. J Wound Care 1992; 3 : 35 - 38.
11. Santoianni P, Monfrecola G, Martelota D, Ayala F.Inadequate effect of He - Ne Laser on venous leg ulcer.Photodermatol 1984; 1: 245 - 249.
12. Smith DJ. Bhat S, Bulgrin JP. Video image analysis ofwound repair. Wounds 1992; 4: 6 - 15.
13. Smith RB, Rogers B, Tolstykh Gp, Walsh Ne, Davis MG,Bunegin L, etal. Three dimensional Laser imaging systemfor measuring wound geometry. Laser Surg Med 1998;23: 87 - 93.
14. Sugrue ME, Carolan J, Leen EJ, Feeley TM, Moore DJ,Shanik GD. The use of infra red laser therapy in thetreatment of venous ulceration. Ann Vasc Surg 1990; 4:179 - 181.
15. Whiston RG, Melhuish JM, Harding KG. High resolutionultrasound imaging in wound healing . Wounds 1993; 5:116 - 121.
24

ROLE OF THE CEREBELLUM IN MOTORLEARNING-RELEVANCE TO PHYSIOTHERAPY
(Literature Review)
Uday Kiran Reddy Emani Sustruta Institute of Physical Medicine and Rehabilitation.
Abstract
Traditionally, clinicians have sought to explain the role of Physiotherapy as one of promoting recoveryor compensation through the use of alternative pathways, when the original pathways that subserve aparticular function are destroyed (Gardiner M, 1963). This explanation is inadequate when seen in thelight of current neuroscience. This paper seeks to explain the role of Physiotherapy in cerebellar lesionsin the context of its role in motor learning. During the learning of a new motor task, the motor controlsystem makes use of extensive feedback to perform the task. This form of control is called as closedloop control (Iyer M et al.,1999). In closed loop control, the cerebellum performs the role of an errorcorrecting mechanism(Fredericks c,1996). Through constant practice of the task, the motor controlsystem can perform the task without the assistance of feed back. This form of control is called openloop control (Iyer Met al., 1999). In open loop control, the cerebellum performs the role of a modulator(Tach WT,1996). Since patients with cerebellar lesions perform all movements through closed loopcontrol, the aim of Physiotherapy would be to convert motor tasks from closed loop to open loopthrough constant practice of motor tasks.
Keywords: Cerebellum, Motor-learning, Motor program, Open-loop, Closed-loop, Recovery,Physiotherapy.
INTRODUCTION
Perhaps the most weather beaten phrase in neurologicalPhysiotherapy is “use of alternative pathways”. Traditionally,clinicians have sought to explain the role of Physiotherapyas one of promoting recovery or compensation through theuse of alternative pathways, when the original pathways thatsubserve a particular function are destroyed (Gardiner M,1963). However, this explanation begs the question- whatare those alternative pathways? Although, it is possible thatthe exact pathways have not been identified yet, there is stilla need to evolve a theory to explain how Physiotherapypromotes recovery/compensation following a lesion in thecontext of function of the affected part. This paper seeks toexplain how therapeutic techniques re establish the functionof a lesioned cerebellum in the context of its role in motorlearning.
Therapeutic techniques adopted in cerebellardysfunction
The therapeutic techniques adopted in cerebellardysfunction may be classified as:-
1. Nonspecific Exercises: Frenkels exercises are a typicalexample. Although they were originally developed byH.S.Frenkel for the treatment of sensory ataxia (GardinerM, 1963), their use has been advocated for cerebellarataxia (Urbscheit, 1990). These exercises make use of
visual and verbal feed back to re-establish smoothcoordinated movement with repeated practice andattention to the task during performance (Gardiner M,1963).
2. TASK SPECIFIC EXERCISES: These exercises focuson developing control during specific actions such asstanding up, sitting down, walking, reaching for andmanipulating an object (Carr J & Shepherd R, 1998).
Since this paper is concerned with how exercises workrather than what exercises work in cerebellar lesions, adetailed review of specific techniques is beyond thescope of this paper.
Role of the cerebellum in Motor Learning
When first learning a new task, movement is slow,incoordinate and requires extensive sensory feedback andattention to the task. Several areas in the brain areactivated during learning- (a) the prefrontal cortex(b) the lateral premotor cortex (c) the parietal associationcortex d) the cerebellum (Jenkins IH et al 1994) (seefig 1). The prefrontal cortex is responsible for motorplanning and attention to the task (Jueptner M et al 1997).The parietal association cortex is needed for sensoryintegration (Woollacott M & Shumway-cook A, 2001).The lateral premotor cortex controls movements guidedby external sensory cues and hence its activation duringinitial learning (Mier H et al 1998). Several studies haveconfirmed increased activation of the cerebellum during the
25

learning of new tasks (Jueptner M et al 1997, JenkinsIH et al 1994, Mier H et al 1998). What possible partdoes the cerebellum play in motor learning? It has beenhypothesised that the cerebellum is involved in theprocess by which a motor task is converted from anattentionally demanding to a more automatic state (LangCE & Bastian AJ, 2002; Jenkins IH et al 1994). Onecan understand how this is accomplished when oneconsiders the role of the cerebellum in the motor controlsystem.
The motor control system is analogous to the cruisecontrol system in a car (see fig 2a). The cruise controlof a car consist of a central computer(cc) which can beprogrammed to achieve a desired speed. The centralcomputer then tries to achieve the desired speed bycontrolling the accelerator. However, the actual speedmay differ from the desired speed due to extraneousfactors like the effect of wind resistance and frictionfrom the road. The actual speed is picked up by a sensorwhich then relays this information to an error correcting
computer (ECC) The ECC then compares the actualspeed with the desired speed and sends corrective signalsto the accelerator to compensate for the effect ofextraneous factors (Iyer M et al 1999). Similarly, themotor command centers in the brain (promoter area,anterior cingulate, primary motor area) try to produce adesired movement by activating the motor neurons inthe spinal cord and cranial nerve nuclei (see fig 2b).However, the actual movement produced by the musclesmay differ from the desired movement due to externalfactors (ex:-object being moved may be heavier thananticipate if) and internal factors (ex:-reduced range ofmovement in joints). The cerebellum receivesinformation regarding the actual movement from(a) musculoskeletal system through the spinocerebellarand cuneocerebellar tracts (b) visual system through thetectocerebellar tract (c) vestibular system through thevestibulocerebellar tract. The cerebellum also receivesinformation from the motor command centres regardingdesired movement directly through the
26
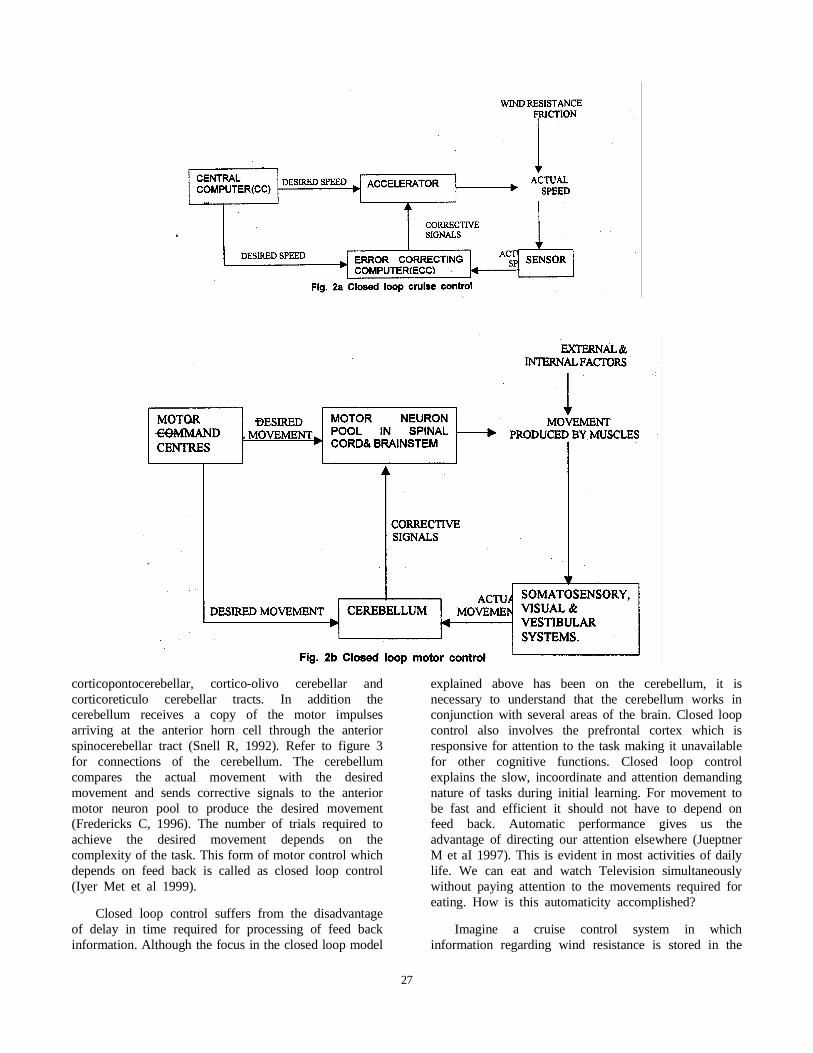
corticopontocerebellar, cortico-olivo cerebellar andcorticoreticulo cerebellar tracts. In addition thecerebellum receives a copy of the motor impulsesarriving at the anterior horn cell through the anteriorspinocerebellar tract (Snell R, 1992). Refer to figure 3for connections of the cerebellum. The cerebellumcompares the actual movement with the desiredmovement and sends corrective signals to the anteriormotor neuron pool to produce the desired movement(Fredericks C, 1996). The number of trials required toachieve the desired movement depends on thecomplexity of the task. This form of motor control whichdepends on feed back is called as closed loop control(Iyer Met et al 1999).
Closed loop control suffers from the disadvantageof delay in time required for processing of feed backinformation. Although the focus in the closed loop model
explained above has been on the cerebellum, it isnecessary to understand that the cerebellum works inconjunction with several areas of the brain. Closed loopcontrol also involves the prefrontal cortex which isresponsive for attention to the task making it unavailablefor other cognitive functions. Closed loop controlexplains the slow, incoordinate and attention demandingnature of tasks during initial learning. For movement tobe fast and efficient it should not have to depend onfeed back. Automatic performance gives us theadvantage of directing our attention elsewhere (JueptnerM et aI 1997). This is evident in most activities of dailylife. We can eat and watch Television simultaneouslywithout paying attention to the movements required foreating. How is this automaticity accomplished?
Imagine a cruise control system in whichinformation regarding wind resistance is stored in the
27

system so that the error computer can automaticallyinitiate corrective signals without the necessity for feedback (see fig 4a). Such form of control which does notmake use of feed back is called as open loop control(Iyer M et al 1999). The motor control system operatesin a similar manner to convert the motor task fromclosed loop to open loop. During every repetition, thefollowing information is stored in the brain:- (a) theinitial movement conditions such as the position of thebody and weight of an object moved (b) spatial and
temporal parameters of the task (c) the result of themovement and (d) sensory feel of the movement i.e whatit looked like, felt like and sounded like. The informationis abstracted and stored in the form of a motor program(Schmidt, 1975 cited in Woollacott M andShumway-cook A, 2001). Iyer and colleagues describethe motor program as “an algorithm of neuronalactivities that encodes the movement strategy forexecution of a desired movement behaviour”. Theadvantages of compiling a motor program are:- (a) with every
28

repetition, the necessity for feed back decreases(b) movement will eventually be performedautomatically so that conscious attention can be used forother tasks (c) the motor program can not only bere-activated to produce a particular movement, but canalso be adapted to a different task which is similar tothe original learned one. Thus, the cerebellum canmodulate motor behaviour without the assistance offeedback by drawing on the stored motor programs.
It is now evident why attention to the task andrepetition form the hallmarks of Frenkel’s exercise(Gardiner M, 1963). It is also obvious how some ofthese exercises can be adapted for activities of daily life.
For example, the common Frenkel’s exercise of touchingthe therapists finger with the index finger of the patientcan compile a motor program which can be adapted toturning on a switch or pointing to a target. Thetransference of skill from training to ADL depends onseveral variables and will not be discussed here.
The next question that needs to be addressed is ifthe cerebellum is the exact site of plastic changesassociated with motor learning. In other words, are themotor programs stored in the cerebellum? Unfortunately,the answer to this question remains elusive. To beginwith, synaptic plasticity has been observed in thecerebellum during motor learning (Thach WT, 1996).While some consider this to be evidence of motor
Fig. 4b Open loop motor control
29

learning (Thach WT. 1996) others conclude that thissynaptic plasticity cannot be conclusively proven to bethe basis of motor learning (Llinas R & t Welsh JP.1993). Medina and Mauk argue that those synapsesassociated with learning “can also be active duringnon-learning periods providing opportunities to modifytheir strength” (Medina J & Mauk M, 1999). Hence thedebate on the site of motor learning continues.
What happens when the Cerebellum Develops aLesion?
Mier and colleagues have found that “practiceproduces a shift in activity from one set of areas to adifferent area”. During learning, the promoter cortex,cerebellum and prefrontal cortex are preferentiallyactivated. When repeating a previously learned task,activity was found in the basal ganglia and thesupplementary motor area (Mier H et aI 1998). Theactivity of the cerebellum was found to decrease withpractice (Jenkins IH et al 1994; Mier H et al 1998) butdoes not disappear completely (Thach WT, 1996). Thecerebellum is still required to modulate the performanceof a prelearned activity. This is evident when thecerebellum develops a lesion. Although we learn walkingas infants and the neuronal circuitry for walking existsin the spinal cord (Fredericks C, 1996), lesions of thevermis causes walking to go haywire.
Following lesions in the cerebellum, either its accessto the motor programs is curtailed (if they reside outsidethe cerebellum) or the motor programs themselves aredestroyed (if they are housed in the cerebellum). It canno longer modulate the spatial and temporal parametersof previously learned movement. Motor impairmentssuch as dysmetria and dysdiadochokinesia are indicativeof the inability of the lesioned cerebellum to modulatethe parameters of movement. Due to this the motorcontrol system relies extensively on sensory feed back andattention to action to perform even the simplest ofmovements a characteristic of closed loop motor control.The reader is reminded that all new actions are performedin this manner.
The cerebellum does show a certain capacity forrecovery. Studies done on primates have demonstratedthe ability of the cerebellum to recover followingexperimentally induced lesions. The magnitude ofrecovery seems to depend on the area and site of thelesion. A bilateral lesion showed greater residual deficitthan a unilateral lesion and lesions of the cerebellarnuclei were more serious than lesions of the cortex. Itis assumed that if a part of the cerebellum becomesnon-functional, the remainder can take over its function.The cerebrum is also known to compensate to some extentfor the loss of cerebellar function (Urbscheit N, 1990).
Role of Physiotherapy in Cerebellar Lesions
Since patients with cerebellar lesions perform allmovements through closed loop control, the aim ofPhysiotherapy would be to convert motor tasks fromclosed loop to open loop motor control using the intact
part of the cerebellum. Based on the evidence presentedabove, it may be hypothesised that constant practice ofmovements would train the intact parts of the cerebellumto gain access to previously stored motor programs orbuild a new set of programs through trial and errorlearning. Motor learning following CNS lesions happensthrough the same biological processes as in the normalCNS and follows the same rules (Woollacott M andShumway-cook A, 2001). However, this does notnecessarily imply that every patient with a cerebellarlesion would learn to perform activities in the same waythat they were done prior to the injury.
In this context, it is necessary to appreciate thedistinction between normal and compensatory strategies.A patient is said to have recovery of normal strategy ifhe is able to achieve a functional goal in the same wayit was performed before injury to the nervous system.When normal strategies cannot be used by the patient,he may adopt compensatory strategies which involveaccomplishing a functional goal using alternative means(Woollacott & Shumway-cook, 2001). For example apatient with hypermetria, when reaching for a glass ofwater on a table, may use the table for braking. Anotherexample of compensation is the decomposition ofmovement in patients-who do not have multiple jointco-ordination. Compensatory strategies represent apatients attempt to accomplish a functional task giventhe limitations imposed by his neurological impairments.They are formed during the acute stage of neurologicalinjury and may persist, often to the detriment of normalrecovery processes (Carr & Shepherd, 1998).Compensatory strategies are seldom adaptable to varyingtask and environmental demands but they may be theonly option in patients in whom recovery of normalstrategies is not possible due to the constraints imposedby the lesion. This poses a serious question to theclinician- how should he decide weather to facilitatenormal or compensatory strategies?
The answer to this question would depend on thesize and site of the lesion. Lesions confined to smallareas of the cerebellar cortex seem to have a goodpotential for recovery. Barashl et al (1999) studied theeffects of lesions in the oculomotor vermis of monkeys.The monkeys developed saccadic hypometria post lesion.However they recovered from hypometria over time. Theauthors hypothesised that recovery from dysmetriaoccurred through a process of visuomotor adaptation i.e theprecision of saccades was modified according to their visualoutcome. The reader is reminded that motor learning innormal individuals as described in an earlier part of this paperhappens in much the same manner. Another interestingobservation in this study was that if the fastigial nucleus isablated along with the cortex of the vermis, the capacity forrecovery is lost and the saccades become permanentlydysmetric. The results of this study suggest that return to anormal or near normal status is possible if the lesion isconfined to a small portion of the cerebellar cortex but notif it includes the nuclei.
30

How do lesions in the cerebellar nuclei affect motorperformance? Wang et al (1998) studied the effects ofcerebellar nuclear inactivation on the learning of acomplex forelimb activity in cats. They found that themovement strategies employed by the cats were differentfrom normal and they were highly inco-ordinate.However, the cats were capable of modifying thesecompensatory strategies significantly with practice tomake them more efficient. The author hypothesised thatduring nuclear inactivation, the cats would have to learnthe task “through integrative processes that could notemploy the information processing normally done by thecerebellum”.
The following conclusions can be drawn from thestudies presented above:-
1. Normal strategies may be encouraged if thelesion is confined to a small part of thecerebellar cortex but not if the lesion extendsto the nuclei.
2. Compensatory strategies will have to beencouraged in patients with cerebellar nuclearlesions
3. Patients with even nuclear lesions are capableof modifying their movement strategies to makethem more efficient. However, these movementsmay not be comparable to normal strategies.
These guidelines for decision making have to betaken with a pinch of salt since neurological lesions havescant respect for anatomical boundaries. When in doubtthe clinician may initially ecourage normal strategies; ifnormal strategies are not learned despite practice, theclinician may encourage compensatory strategies(Woollacott & Shumway-cook A, 2001).
CONCLUSION
The theoretical model presented above is a viableexplanation of how physiotherapy works in cerebellarlesions based on pertinent findings in neuroscience.According to this model, it is theoretically possible forvictims of cerebellar lesions to regain their ability to controlpreviously learned tasks and even learn new tasks.However, we still await studies which unequivocallydemonstrate the ability of patients with cerebellar lesionsto regain control of old skills or learn new ones.
Melzack and Wall (1996) describe a theory as “anattempted solution to a puzzle or problem- like a guessmade by a detective presented with an array of clues ina system”. The theoretical model presented above ismerely that- a guess made on the basis of currentfindings in neuroscience. As new discoveries are madein the field of motor control this theory may have tobe modified to incorporate contemporary findings.
REFERENCES 1. Barash S, Melikyan A, Sivakov A, Zhang M,Glickstein
M, and Thier P (1999) Saccadi Dysmetria and Adaptationafter Lesions of the Cerebellar Cortex. The Journal ofNeuroscience, December 15,1999,19(24):10931-10939
2. Carr J and Shepherd R(1998) Cerebell arataxia.Neurological rehabilitation: Optimizing motorperformance. Oxford: Butterworth Heinemann.
3. Fredericks C (1996) Cerebellar mechanisms. In FredericksC and Saladin L, eds. Pathophysiology of the motorsystems. Philadelphia: FA Davis company.
4. Fredericks C (1996) Motor control at the spinal cordlevel. In Fredericks C and Saladin L,eds. Pathophysiologyof the motor systems. Philadelphia: FA Davis company.
5. Gardiner M (1963) Neuromuscular coordination. Theprinciples of exercise therapy.
6. Iyer M, Mitz A and Winstein (1999) Motor 1 :Lowercentres. In Cohen H, ed. Neuroscience for rehabilitation,2ed. Philadelphia: Lippincott Williams and Wilkins.
7. Jenkins IH, Brooks OJ, Nixon PO, Frackowiak RS andPassing ham RE (1994) Motor sequence learning: a studywith positron emission tomography. The Journal ofNeuroscience, vol 14, pg 3775-3790.
8. Lang CE and Bastian AJ (2002) Cerebellar damageimpairs automaticity of a recently practiced movement.The Journal of Neurophysiology, 87: pg1336-1347.
9. Llinas R and Welsh JP (1993) On the cerebellum andmotor learning. Curr opin neurobiol, Dec:3(6), 958-65.
10. Medina J and Mauk M (1999) Simulations of cerebellarmotor learning: computational analysis of plasticity at themossy fiber to deep nucleus synapse. The Journal ofNeuroscience, Aug 15, pg 7140-7151.
11. Melzack R and Wall PO (1996) The evolution of paintheories. The challenge of pain, 2nded. Penguin books.
12. Mier H, Tempel LW, Perlmutter JS, Raichle ME,Peterson SE (1998) Changes in brain activity duringmotor learning measured with PET: Effects of hand ofperformance and Practice. The Journal ofNeurophysiology, vol 80, pg 2177-2199.
13. Snell R (1992) Connections of the cerebellum. Clinicalneuroanatomy for medical students, 3rd ed. Boston: LittleBrown and Company.
14. Thach WT (1996) On the specific role of the cerebellumin motor learning and cognition: Clues from PETactivation and lesion studies in man. Behavioral and Brainsciences.19(3):411-431.
15. Urbscheit N (1990) Cerebellar dysfunction. In UmphredD, ed, Neurological Rehabilitation, 2nded. Philadelphia:The CV Mosby Company.
16. Wang J, Shimansky Y, Bracha V, Bloedel J (1998)Effects of cerebellar nuclear inactivation on the learningof a complex forelimb movement in cats; The Journal ofNeurophysiology, Vol.79, No.5, May1998, Pg 2447-2459.
17. Woollacott M and Shumway-cook A (2001) Physiology ofmotor control. Motor control theory and practical applications,2nded. Philadelphia:Llppmcott Williams and Willkins.
18. Woollacott M and Shumway-cook A (2001) Motorlearning and recovery of function. Motor control theoryand practical applications, 2nded. Philadelphia: LippincottWilliams and Wilkins.
19. Woolacott M and Shumway-cook A (2001) A conceptualframework for clinical practice. Motor Control theory andpractical applications, 2nded. Philadelphia: LippincottWilliams and Wilkins.
31

32

INSTRUCTIONS TO AUTHORS
Submission of Manuscripts. Manuscripts should besubmitted to the Editor, IAP Journal, Plot No 112,Shruthi Laya, Ashok Brindavan, Iyyapanthangal, Chennai- 600 056. The original and three copies of text andillustrations are required. The journal’s readership is forIAP members. All articles are sent anonymously to atleast two referees and are subject to editorial revision.Authors may give the names and addresses of up to fourpersons whom they judge would have appropriateknowledge and experience to review their manuscript.Submission of an article is taken as acceptance by theauthor that it contains nothing that is libellous orinfringes copyright. When an article is accepted forpublication the copyright will belong to the publisher(IAP).
Presentation of Manuscript. The manuscript, in English,should be typed with double spacing on one side onlywith a margin of at least 3 cm all around. It shouldcommence with a separate title page, showing title andauthor(s) name(s). Each author should indicate his/herprofessional discipline and current appointments.Author’s degrees and qualifications are required forarticles, book reviews and letters for publication. The fulladdress (including postal code) is required for eachauthor. The person to whom reprint requests are to besent should be indicated.
An abstract of not more than 200 words must followthe title page. Each page of the manuscript should benumbered consecutively. Typescripts should be carefullychecked before submission as no changes to the contentof the accepted manuscript can be allowed at any stageof production.
The format of the article should be in the followingsequence - Key words, Summary/Abstract, Introduction,Methodology, Results, Discussion, Conclusion, Details ofAuthor’s Address for Correspondence, Acknowledgementsand References.
Headings Normally only two categories of headingshould be used. Major ones should be typed in capitalletters in the middle of the page and underlined;sub-headings should be typed in lowercase and alsounderlined. Headings should not be numbered.
Data and Terminology All quantitative measurementsshould be given in System International (SI) units.Authors should indicate the statistical techniques todetermine significance, etc. Where percentage are given,the actual numbers on which these are based should alsobe provided.
Tables These should be typed double-spaced onseparate sheets (i.e. not incorporated within the writtentext). A short descriptive title should appear above eachtable with a clear legend, and any footnotes suitablyidentified below. All units must be included.
Illustrations Line drawings should be on separate sheetsof good quality white paper and drawn in black ink. Theyshould be about twice the size of final reproduction.Bromide prints made from original line drawings areacceptable. Half-tone figures should be clear,highly-contrasted black and white glossy prints (colourphotographs should be avoided). Photomicro- graphs shouldhave internal scale-markers where appropriate. X-ray filmsshould be submitted as photographic prints carefully madeto bring out the details to be illustrated, with an overlayindicating the area of importance.
Figures should be completely lettered, taking intoaccount necessary size reduction. Captions should betyped, double spaced, on a separate sheet. All figuresshould be clearly marked in pencil on the reverse sidewith the number, author’s name and top edge indicated.
References The accuracy and completeness ofreferences are of the utmost importance. The need toquery inaccurate or incomplete references causesunnecessary delay.
1. References in the Text: These should be quotedby the name(s) of the author(s) and the date ofpublication. In the case of two authors, both namesshould be stated. In the case of more than two authors,only the first should be stated, followed by “et al”.References must be indicated by numbers. Authors mustspecifically ensure that all references in the text alsoappear in the references list, and vice versa.
2. Reference List: This should appear at the end ofthe paper in alphabetical order. The author’s name shouldbe followed by his/her initials (unpunctuated), andseparated from that of the next author by a comma. Thenames of all authors should be given (do not use “etal” in the reference list). Next should appear the dateof publication, followed by details of the work inquestion:
Resubmission of Manuscripts. When manuscripts arereturned to authors for revision with referee’s comments,two copies of the revised paper should be resubmittedto the Editor. A letter must be enclosed detailing theaction taken with regard to each point raised by thereferees. If it is felt that no changes is appropriate withregard to a specific point, this should be clearlyexplained.
33