coping styles among families of children with hiv infection
TRANSCRIPT

This article was downloaded by: [University of Alberta]On: 15 October 2014, At: 13:43Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
AIDS Care: Psychological and Socio-medical Aspects of AIDS/HIVPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/caic20
Coping styles among families ofchildren with HIV infectionS. C. Martin PhD a b , P. L. Wolters a b , P. A. Klaas a b , L. Perez c &L. V. Wood aa HIV and AIDS Malignancy Branch , National Cancer Institute ,Maryland, Bethesda, USAb Medical Illness Counseling Center, Chevy Chase , Maryland,Bethesda, USAc Westat, Inc. , Maryland, Bethesda, USAPublished online: 27 Sep 2010.
To cite this article: S. C. Martin PhD , P. L. Wolters , P. A. Klaas , L. Perez & L. V. Wood (2004)Coping styles among families of children with HIV infection, AIDS Care: Psychological and Socio-medical Aspects of AIDS/HIV, 16:3, 283-292
To link to this article: http://dx.doi.org/10.1080/09540120410001665295
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, in relation to orarising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &

Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
Uni
vers
ity o
f A
lber
ta]
at 1
3:43
15
Oct
ober
201
4
Coping styles among families of childrenwith HIV infection
S. C. MARTIN,1,2 P. L. WOLTERS,1,2 P. A. KLAAS,1,2 L. PEREZ3 &
L. V. WOOD1
1HIV and AIDS Malignancy Branch, National Cancer Institute, Bethesda, 2Medical Illness
Counseling Center, Chevy Chase & 3Westat, Inc. Bethesda, Maryland, USA
Abstract The primary aim of this study was to examine coping strategies among families of HIV-
infected children and how they relate to medical, central nervous system (CNS) and family
environment factors. Caregivers of HIV-positive children (N�/52) completed a family coping
measure (F-COPES) and provided information regarding family environment. Data regarding
medical and CNS status were obtained from patient records. Results indicated that families’ passive
coping and spiritual support were among the coping techniques used most often, and social support was
used least often. Medical variables were unrelated to any coping styles. Families of children with CNS
impairment endorsed more passive coping techniques than families of children with no apparent
deficits. A trend was found for non-biological caregivers to seek out more community resources and
support than biological caregivers. Findings suggest the need to target families least likely to utilize
resources, and to teach them to effectively seek out and benefit from social and community supports.
Introduction
Children with HIV and their families are faced with various stressors stemming from medical
and psychosocial challenges. The way families cope with these challenges can impact their
psychological and physical well being. The majority of literature on coping in families of
children with medical illnesses comes from populations with diseases other than HIV, such as
cancer and diabetes. Results of such studies are varied with respect to specific types of coping
styles used and their effectiveness.
Common frameworks for conceptualizing coping
Researchers have examined coping styles in a variety of ways, most commonly in terms of
emotion- versus problem-focused coping and passive versus active coping. Emotion-focused
strategies occur when an individual believes that nothing can be done to change the situation
and include techniques such as avoidance (Lazarus & Folkman, 1984). Problem-focused
Address for correspondence: Staci Martin, PhD, 9030 Old Georgetown Road, #107, Bethesda, MD 20892-8200,
USA. Tel: �/1 (301) 496 0561; Fax: �/1 (301) 402 1734; E-mail: [email protected]
AIDS CARE (April 2004), VOL. 16, NO. 3, pp. 283�/292
ISSN 0954-0121 print/ISSN 1360-0451 online/04/030283-10 # Taylor & Francis Ltd
DOI: 10.1080/09540120410001665295
Dow
nloa
ded
by [
Uni
vers
ity o
f A
lber
ta]
at 1
3:43
15
Oct
ober
201
4

strategies are used when an individual views a stressful situation as amenable to change and
include techniques such as generating solutions and learning new skills. Another method of
conceptualizing coping strategies refers to passive and active techniques. Passive coping
techniques occur when a person relinquishes control of a problem to others, while active
coping involves an attempt to take a more active role in dealing with a problem (Brown &
Nicassio, 1987). These descriptions suggest that most passive techniques are analogous to
emotion-focused coping, while active coping techniques are more similar to problem-focused
coping.
Relationship of passive coping to psychological and medical factors
To understand the effects that specific strategies can have on one’s ability to cope with illness-
related stressors, several studies have compared the effectiveness of passive versus active styles
of coping. Most found little support for passive techniques with respect to physical and
psychological outcomes. Among HIV-positive adults, passive or avoidant techniques are
associated with higher levels of distress while active coping techniques are associated with
decreased emotional distress (Nannis et al ., 1997; Siegel et al ., 1997). This finding has been
reported among men (Wolf et al ., 1991) and women (Moneyham et al ., 1998), as well as
cross-culturally (Fukunishi et al ., 1997). One of the few paediatric studies examining this
topic found that children with cancer who employed passive coping strategies during a painful
medical procedure reported more pain than those who employed active strategies (Broome et
al ., 1990). To our knowledge, only one study has specifically examined various coping styles
among HIV-infected children, and findings indicated that school-age children with HIV who
use emotion-focused coping experienced more psychological distress than those using
problem-focused coping (Bachanas et al ., 2001).
Coping in the family
To understand the coping styles of paediatric patients, it is necessary to examine the nature of
coping within the family as a system. Certain family environment factors have been found to
influence child coping styles, such as parental supportiveness and the level of structure and
organization within the home (Hardy et al ., 1993). Significant relationships between parental
and child coping have been found for both girls and boys (Kliewer & Lewis, 1995), and
among various illness groups (Brown et al ., 1993; Kupst et al ., 1995). Some evidence suggests
that patterns of coping differ according to the family composition (one- versus two-parent
homes [Brazil & Krueger, 2002]) and the relationship of the caregiver to the child (biological
versus alternative caregivers [Rose & Clark-Alexander, 1998]).
Relationship of family coping to psychological and medical factors
Among families of children with traumatic brain injury (TBI), research has demonstrated that
use of denial is associated with more negative emotional impact at 12-months post-TBI
(Wade et al ., 2001), suggesting that families’ use of various coping strategies may influence
the emotional burden of paediatric injuries. To our knowledge, there are no studies that
examine family coping styles in the paediatric HIV population. Primary goals of this study
were (1) to identify coping strategies most frequently utilized by families of HIV-infected
children; and (2) to explore relationships among coping strategies, the child’s medical and
central nervous system (CNS) status and family environment factors. Based on previous
findings of an inverse relationship between passive or avoidant coping and medical markers
284 S. C. MARTIN ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f A
lber
ta]
at 1
3:43
15
Oct
ober
201
4

(Brown & Nicassio, 1987; Mulder et al ., 1999), it is hypothesized that families of children
with poorer medical functioning and CNS status will be more likely to use passive coping
strategies. Since a limited amount of research has suggested associations between coping and
family environment factors (e.g. family composition, caregiver�/child relationship), explora-
tory analyses will be conducted to assess relationships among these variables.
Methods
Participants
Families of HIV-positive children consecutively enrolled on antiretroviral treatment protocols
at the National Cancer Institute (NCI) between 1998 and 2001 were eligible for participation.
Children with HIV infection were referred to the NCI from around the USA to participate in
clinical trials of antiretroviral therapy. Protocols were approved by the NCI Institutional
Review Board, and informed consent was given by the parent or legal guardian prior to the
child’s enrollment. Family measures were administered as part of the baseline neuropsychol-
ogy evaluation included in antiretroviral studies. All data were collected during routine
outpatient clinic appointments. Questionnaires were completed by the caregiver who
generally spent the most time with the child.
Measures
Family coping . Caregivers completed the Family Crisis Oriented Personal Evaluation Scale (F-
COPES; McCubbin et al ., 1981), a 30-item measure designed to assess problem-solving and
coping strategies that families utilize when faced with difficult situations. The caregiver rates a
series of coping techniques on a five-point Likert scale according to whether their family
engages in that technique (1�/strongly disagree, 5�/strongly agree). Responses yield scores
on five sub-scales: Acquiring Social Support, Seeking Spiritual Support, Reframing,
Mobilizing Family Support and Passive Appraisal. Good reliability and validity of the F-
COPES have been documented in studies of various medical populations (Kong et al ., 1993;
Leavitt, 1990; Leiter, 1990; Samuelson et al ., 1992).
Family environment. Background data were obtained through interviews with the caregiver at
the on-study evaluation. Caregivers provided information on family environment factors
including composition of the family (one- versus two-parent home), relationship of the child
to the primary caregiver (biological, adoptive, foster, extended family) and HIV status of the
primary caregiver(s). Since only a small number of families fell into the categories of foster
parent or extended family, we combined data from these two groups and the adoptive
caregivers to form two more equivalent groups: biological versus not biological.
Child’s medical status. Medical markers including CD4 percentages and viral load (HIV-1
RNA PCR) were obtained at the same clinic visit during which the family measures were
administered. CD4 percentages were transformed to age-adjusted z-scores in order to account
for rapid age-related changes in normal CD4 levels that occur in the first four years of life
(Brouwers et al ., 1995; European Collaborative Study, 1992). A log transformation was
performed on viral load data since the distribution of values for this variable was not normal.
Child’s CNS status. All paediatric patients enrolled on antiretroviral protocols at the NCI are
categorized according to severity of HIV CNS disease. Specifically, patients are classified as
COPING STYLES AMONG FAMILIES WITH HIV-INFECTED CHILDREN 285
Dow
nloa
ded
by [
Uni
vers
ity o
f A
lber
ta]
at 1
3:43
15
Oct
ober
201
4
‘apparently not affected’, ‘CNS compromised’ or ‘encephalopathic’, as determined by specific
criteria consisting of cognitive test scores, results of brain imaging scans and neurologic exam
findings (Wolters & Brouwers, 1998).
Data analyses
Student’s t-tests were conducted to compare mean scores between F-COPES sub-scales.
Correlations and analyses of variance were used to assess relationships among family coping
scales and medical, CNS, and family environment variables. Typically, F-COPES interpreta-
tions are based on raw sub-scale scores. However, because the sub-scales differ in terms of
number of items and possible range of total raw scores, we divided sub-scale scores by the
number of items in that particular sub-scale, thus allowing for comparisons across sub-scales.
Results
Patient characteristics
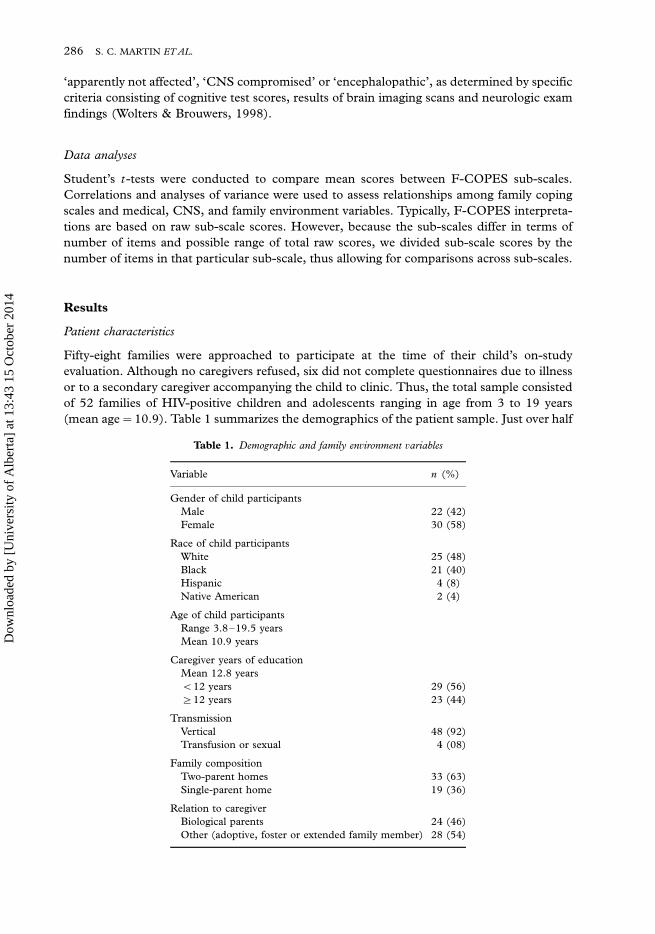
Fifty-eight families were approached to participate at the time of their child’s on-study
evaluation. Although no caregivers refused, six did not complete questionnaires due to illness
or to a secondary caregiver accompanying the child to clinic. Thus, the total sample consisted
of 52 families of HIV-positive children and adolescents ranging in age from 3 to 19 years
(mean age�/10.9). Table 1 summarizes the demographics of the patient sample. Just over half
Table 1. Demographic and family environment variables
Variable n (%)
Gender of child participants
Male 22 (42)
Female 30 (58)
Race of child participants
White 25 (48)
Black 21 (40)
Hispanic 4 (8)
Native American 2 (4)
Age of child participants
Range 3.8�/19.5 years
Mean 10.9 years
Caregiver years of education
Mean 12.8 years
B/12 years 29 (56)
]/12 years 23 (44)
Transmission
Vertical 48 (92)
Transfusion or sexual 4 (08)
Family composition
Two-parent homes 33 (63)
Single-parent home 19 (36)
Relation to caregiver
Biological parents 24 (46)
Other (adoptive, foster or extended family member) 28 (54)
286 S. C. MARTIN ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f A
lber
ta]
at 1
3:43
15
Oct
ober
201
4

of the children were female (58%) and about half were Caucasian (48%). A majority were
living in two-parent homes (63%), and almost half were the biological offspring of their
caregivers (46%). Most patients acquired HIV through vertical transmission (92%). The
mean years of education among primary caregivers was 12.8, and most caregivers who
completed the questionnaires were female (86%).
Medical and CNS status of patients
Table 2 summarizes the medical and CNS variables for our patient sample. Nineteen per cent
of child participants had undetectable viral loads (HIV-1 RNA PCR levels less than 50 copies/
ml). The mean value of HIV-1 RNA PCRs was 76146 (median 5345, range�/0�/773906),
and the mean log(10) copy number was 3.2519/1.9 (maximum of 5.889). Examination of
immune functioning indicated a mean CD4 percentage of 26% (median�/25.5, range�/0�/
51%), suggesting mild to moderate suppression in a majority of our sample. In terms of CNS
status, 14 (27%) of our patients were classified as ‘encephalopathic’ or ‘CNS compromised’,
while 38 (73%) were ‘apparently not affected’.
Family coping results
Prior to examining data from the F-COPES, reliability coefficients were computed for each
sub-scale. Alpha coefficients for our sample ranged from 0.61 (Passive Appraisal) to 0.86
(Acquiring Social Support). Reliability coefficients from the F-COPES validation sample
range from 0.63 (Passive Appraisal) to 0.83 (Acquiring Social Support). Results from our
sample were generally consistent with the validation sample with the exception of the
Reframing sub-scale. Our study found this scale’s alpha coefficient to be notably lower than
the validation study (0.66 and 0.82, respectively).
Comparison of F-COPES sub-scales. On the F-COPES, the highest mean scores were obtained
on the Reframing, Passive Appraisal and Seeking Spiritual Support sub-scales (4.079/0.52,
4.069/0.78 and 3.829/0.97, respectively) as shown in Figure 1. Means of these three scales
Table 2. Medical and CNS variables
Variable n (%)
HIV-1 RNA PCR
Mean�/76146.1
Median�/5345
Range�/0�/773906
CD4%
Mean�/26.2
Median�/25.5
Range�/0�/51
CDC classification
N, A (1�/3) 10 (19)
B (1�/3) 29 (56)
C (1�/3) 13 (25)
CNS classification
Encephalopathic or CNS compromised 14 (27)
Apparently not affected 38 (73)
COPING STYLES AMONG FAMILIES WITH HIV-INFECTED CHILDREN 287
Dow
nloa
ded
by [
Uni
vers
ity o
f A
lber
ta]
at 1
3:43
15
Oct
ober
201
4

were not significantly different from each other (ps�/0.05), while the mean score on the
Acquiring Social Support sub-scale was significantly lower than each of the other four sub-
scales (all psB/0.05). The mean score on the Mobilizing Family Support subscale was
significantly lower than mean scores on the Reframing and Passive Appraisal subscales and
was significantly higher than the mean score on the Social Support subscale (psB/0.05).
F-COPES and medical, CNS and family environment variables. None of the F-COPES sub-
scales were significantly related to any of the medical variables (all ps�/0.05). However,
families of children categorized as ‘encephalopathic’ or ‘CNS compromised’ scored higher on
the Passive Appraisal sub-scale compared with those categorized as ‘apparently not affected’
(F(1,50)�/4.02; p B/0.05).
None of the F-COPES sub-scales were significantly related to caregiver education level,
race of the family or the child’s gender or age. F-COPES sub-scale scores also were compared
between sub-groups based on family composition (two- or single-parent homes) and relation
between child and caregiver (biological or not biological). None of the F-COPES sub-scales
were significantly related to family composition. After partialling out variance from the
caregiver’s HIV status, a non-significant trend emerged for non-biological caregivers to score
higher on the Mobilizing Family Support sub-scale (r�/0.26, p�/0.06). Due to the absence of
a male caregiver in many of the families in our study (N�/17, 33%), the relationship between
HIV status of the male caregiver and F-COPES sub-scale scores could not be reliably
assessed.
Discussion
The coping techniques most frequently endorsed by families in our study included passive
appraisal, reframing and spiritual support. Items on the F-COPES Passive Appraisal sub-scale
reflect an avoidance of problem situations or the tendency to relinquish control of one’s
problems to others. Families who use passive coping may feel helpless regarding their ability to
FIG. 1. Means of F-COPES sub-scale scores.
288 S. C. MARTIN ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f A
lber
ta]
at 1
3:43
15
Oct
ober
201
4

positively impact their child’s medical status. These families may relinquish control of
decisions about the child’s disease to others, such as the medical team, rather than worry
about these problems themselves. This may be helpful in some situations, but could
potentially lead to problems if parents do not take an active role in overseeing their child’s
medication regimen.
Some items from the F-COPES Reframing scale portray an attitude of passive
acceptance, while others reflect a tendency to address problems within the family as opposed
to reaching out to others for support. Thus, families who score high on this scale are probably
not actively seeking out support from friends, extended family or community resources. This
hesitancy to seek support may stem from concern about the social stigma of HIV. Many
families of HIV-positive children have suffered ostracism or rejection in the past and have
developed an attitude of passivity or resistance to outside assistance.
Items on the Seeking Spiritual Support sub-scale relate to religious beliefs and activities.
Not surprisingly, some individuals with a life-threatening illness attempt to cope with such
events in the context of religion. There is a growing body of literature that examines spiritual
coping in chronic illness populations, as well as an emerging awareness that clinicians need to
incorporate an understanding of patients’ spiritual or religious beliefs in order to fully
comprehend their illness experience (Pendleton et al ., 2002; Ross, 1995).
Families in our study endorsed the use of social support as a means of coping significantly
less often than the four other coping mechanisms. Lack of social support among illness
populations is not a new finding, nor is it unique to individuals with HIV. Research has
demonstrated that children with chronic conditions report lower perceptions of support and
smaller support networks than healthy children, and perceptions of (or actual) social support
may vary between illness groups (Ellerton et al ., 1996). Other studies have suggested that a
considerable portion of women with HIV report spending little or no time socializing with
family and friends (Hudson et al ., 2001), and that lower perceptions of social support are
associated with feeling more emotionally burdened among caregivers of children with HIV
(Hughes & Caliandro, 1996).
Given that social support can be a valuable resource in maintaining the emotional health
of families dealing with chronic illness (Neville, 1998; Varni et al ., 1993), it is concerning that
families of children with HIV are not relying on social resources more often. This may stem
from a hesitancy to share information about the child’s diagnosis with others for fear of being
stigmatized. While this is certainly a valid concern, the absence of external support could
negatively affect psychological and physical well being. Thus, there is a need for interventions
aimed at helping caregivers effectively seek out and utilize supportive, non-judgmental social
relationships.
We failed to find significant relationships between medical variables and any of the family
coping sub-scales. Thus, while past studies have put forth evidence that immunological
functioning is related to coping styles in HIV-positive adults (Goodkin et al., 1992; Mulder et
al., 1999), this is not the case in our sample of HIV-infected children. This may be partly due
to the fact that previous studies have examined medical variables as they relate to coping in the
individual with the illness, whereas this study assesses coping in the family. Moreover, any
relationship that exists between these factors is likely mediated by several other variables such
as adherence.
As hypothesized, families of children with HIV-related CNS impairment endorsed more
passive coping techniques compared with families of children with no significant impairment.
Families whose children are more impaired may adopt an attitude of ‘learned helplessness’.
They may feel overwhelmed by their child’s developmental disabilities and be unsure about
how to address their child’s needs. These feelings of uncertainty may prevent parents from
COPING STYLES AMONG FAMILIES WITH HIV-INFECTED CHILDREN 289
Dow
nloa
ded
by [
Uni
vers
ity o
f A
lber
ta]
at 1
3:43
15
Oct
ober
201
4

actively encouraging their child’s progress, and advocating for appropriate educational
services and being involved in their child’s medical care. Caregivers could benefit from being
taught about the nature of HIV CNS disease, therapeutic and educational treatment of HIV-
related disabilities, and how to obtain special education services to help their child develop to
the best of their individual ability level.
Exploratory analyses revealed a borderline relationship between the Mobilizing Family
Support scale and characteristics of the maternal caregiver. Biological mothers tended to seek
out support from community resources less than adoptive, foster and extended family
caregivers. These women may worry about disclosing their child’s diagnosis since their own
diagnosis would likely be revealed as well. Another possibility is that the physical and
emotional impact of their own disease makes it difficult for caregivers to obtain appropriate
services for their child. Since this finding did not reach statistical significance, any
interpretations should be viewed as hypotheses to be examined in future studies.
Our study found no differences in coping between two-parent families and single-parent
families. This replicates a recent finding from a study that used the F-COPES to compare
one- and two-parent families of children with asthma (Brazil & Krueger, 2002). However,
past research with healthy families has found that single mothers use more strategies related to
accepting responsibility compared with mothers in two-parent families (Compas & Williams,
1990). Follow-up research is needed to compare coping styles in one- and two-parent families
of HIV-infected children and healthy children.
Future lines of coping research in paediatric HIV disease should consider the
family system and its potential influence on the child. A reciprocal relationship likely exists
such that the family’s use of coping strategies influences the child with respect to
psychological, CNS and medical functioning as mediated by factors such as adherence. In
turn, the child’s functioning in these areas may influence the family’s selection of coping
techniques. Research and intervention programmes should be implemented within the
context of the family unit, not just the individual with the illness. Interventions are needed
that teach coping strategies to families dealing with a child’s HIV status, and studies
examining their effectiveness should consider possible impacts on adherence that may
ultimately improve medical outcomes.
The finding that families of children with HIV are using social support less often than
other coping strategies demonstrates the necessity for clinical interventions aimed at fostering
communication with friends, extended family, members of the medical team or mental health
counsellors. In addition, future studies should examine differences between HIV-positive
caregivers compared with HIV-negative caregivers in terms of their perceptions of and
willingness to obtain social support.
Further research is needed to compare the use of various coping techniques across illness
populations and over longer time periods. Specific questions include: (1) are families who
utilize more effective coping strategies better able to manage their child’s medical needs over
time, thereby achieving better medical outcomes? and (2) do families change their coping
strategies in response to changes in their child’s clinical condition?
Many research studies assessing family functioning obtain information from only one
member of the family, which assumes that perceptions are similar across individual family
members. This is not always the case, and represents another limitation of this study. Finally,
there are many ways in which researchers conceptualize and assess coping. A multitude of
coping questionnaires are used in research which may not be measuring identical constructs.
Our knowledge about coping with chronic illness will be advanced when researchers reach a
consensus for methods of conceptualizing and measuring coping styles.
290 S. C. MARTIN ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f A
lber
ta]
at 1
3:43
15
Oct
ober
201
4

References
BACHANAS, P., KULLGREN, K., SCHWARTZ, K., LANIER, B., MCDANIEL, S., SMITH, J. & NESHEIM, S. (2001).
Predictors of psychological adjustment in school-age children infected with HIV. Journal of Paediatric Psychology , 26
(6), 343�/352.
BRAZIL, K. & KRUEGER, P. (2002). Patterns of family adaptation to childhood asthma. Journal of Paediatric Nursing , 17
(3), 167�/173.
BROOME, M., BATES, T., LILLIS, P. & MCGAHEE, T. (1990). Children’s medical fears, coping behaviors, and pain
perceptions during a lumbar puncture. Oncology Nursing Society , 17 (3), 361�/367.
BROUWERS, P., DECARLI, C., CIVITELLO, L., MOSS, H.A., WOLTERS, P. L. & PIZZO, P.A. (1995). Correlation between
computed tomographic brain scan abnormalities and neuropsychological function in children with symptomatic
human immunodeficiency virus disease. Archives of Neurology , 52 , 39�/44.
BROWN, G.K. & NICASSIO, P.M. (1987). Development of a questionnaire for the assessment of active and passive
coping strategies in chronic pain patients. Pain , 31 , 53�/64.
BROWN, R.T., KASLOW, N.J., DOEPKE, K., BUCHANAN, I., ECKMAN, J., BALDWIN, K. & GOONAN, B. (1993).
Psychosocial and family functioning in children with sickle cell syndrome and their mothers. Journal of the American
Academy of Child and Adolescent Psychiatry , 32 (3), 545�/553.
COMPAS, B.E. & WILLIAMS, R.A. (1990). Stress, coping, and adjustment in mothers and young adolescents in single-
and two-parent families. American Journal of Community Psychology , 18 (4), 525�/545.
ELLERTON, M.L., STEWART, M.J., RITCHIE, J.A. & HIRTH, A.M. (1996). Social support in children with a chronic
condition. Canadian Journal of Nursing Research , 28 (4), 15�/36.
EUROPEAN COLLABORATIVE STUDY (1992). Age-related standards for T lymphocyte subsets based on uninfected
children born to human immunodeficiency virus infected women. Paediatric Infectious Disease Journal , 11 , 1018�/
1026.
FUKUNISHI, I., HOSAKA, T., NEGISHI, M., MORIYA, H., HAYASHI, M. & MATSUMOTO, T. (1997). Avoidance coping
behaviors and low social support are related to depressive symptoms in HIV-positive patients in Japan.
Psychosomatics , 38 , 113�/118.
GOODKIN, K., BLANEY, N.T., FEASTER, D., FLETCHER, M.A., BAUM, M. K., MANTERO-ATIENZA, E., KLIMAS, N.G.,
MILLON, C., SZAPOCZNIK, J. & EISDORFER, C. (1992). Active coping style is associated with natural killer cell
cytotoxicity in asymptomatic HIV-1 seropositive homosexual men. Journal of Psychosomatic Research , 36 (7), 635�/
650.
HARDY, D.F., POWER, T.G. & JAEDICKE, S. (1993). Examining the relation of parenting to children’s coping with
everyday stress. Child Development , 64 , 1829�/1841.
HUDSON, A.L., LEE, K.A., MIRAMONTES, H. & PORTILLO, C.J. (2001). Social interactions, perceived support, and
level of distress in HIV-positive women. Journal of the Association of Nurses in AIDS Care , 12 (4), 68�/76.
HUGHES, C.B. & CALIANDRO, G. (1996). Effects of social support, stress, and level of illness on caregiving of children
with AIDS. Journal of Paediatric Nursing , 11 (6), 347�/358.
KLIEWER, W. & LEWIS, H. (1995). Family influences on coping processes in children and adolescents with Sickle Cell
Disease. Journal of Paediatric Psychology , 20 (4), 511�/525.
KONG, F., PERRUCCI, C.C. & PERRUCCI, R. (1993). The impact of unemployment and economic stress on social
support. Community Mental Health Journal , 29 (3), 205�/221.
KUPST, M.J., NATTA, M.B., RICHARDSON, C.C., SCHULMAN, J.I., LAVIGNE, J.V. & DAS, L. (1995). Family coping with
paediatric leukemia: ten years after treatment. Journal of Paediatric Psychology , 20 (5), 601�/617.
LAZARUS, R.S. & FOLKMAN, S. (1984). Stress, appraisal and coping . New York: Springer.
LEAVITT, M.B. (1990). Family recovery after vascular surgery. Heart and Lung: Journal of Critical Care , 19 (5, part 1),
486�/490.
LEITER, M. (1990). The impact of family resources, control coping, and skill utilization on the development of
burnout: a longitudinal study. Human Relations , 43 (11), 1067�/1083.
MCCUBBIN, H.I., OLSON, D. & LARSEN, A. (1981). Family Crisis Oriented Personal Scales (F-COPES) . Madison:
University of Wisconsin System.
MONEYHAM, L., HENNESSY, M., SOWELL, R., DEMI, A., SEALS, B. & MIZUNO, Y. (1998). The effectiveness of coping
strategies used by HIV-seropositive women. Research in Nursing & Health , 21 , 351�/362.
MULDER, C., DE VROOME, E., VAN GRIENSVEN, G., ANTONI, M. & SANDFORT, T. (1999). Avoidance as a predictor of
the biological course of HIV infection over a 7-year period in gay men. Health Psychology , 18 (2), 107�/113.
NANNIS, E.D., PATTERSON, T.L. & SEMPLE, S.J. (1997). Coping with HIV disease among seropositive women:
psychosocial correlates. Women & Health , 25 , 1�/22.
NEVILLE, K. (1998). The relationships among uncertainty, social support, and psychological distress in adolescents
recently diagnosed with cancer. Journal of Paediatric Oncology Nursing , 15 (1), 37�/46.
COPING STYLES AMONG FAMILIES WITH HIV-INFECTED CHILDREN 291
Dow
nloa
ded
by [
Uni
vers
ity o
f A
lber
ta]
at 1
3:43
15
Oct
ober
201
4

PENDLETON, S.M., CAVALLI, K., PARGAMENT, K. & NASR, S. (2002). Religious/spiritual coping in childhood cystic
fibrosis: a qualitative study. Paediatrics , 109 (1), E8.
ROSE, M.A. & CLARK-ALEXANDER, B. (1998). Caregivers of children with HIV/AIDS: Quality of life and coping styles.
Journal of the Association of Nurses in AIDS Care , 9 (1), 58�/65.
ROSS, L. (1995). The spiritual dimension: its importance to patients’ health, well-being, and quality of life and its
implications for nursing practice. International Journal of Nursing Studies , 33 , 457�/468.
SAMUELSON, J.J., FOLTZ, J. & FOXALL, M.J. (1992). Stress and coping in families of children with myelomeningocele.
Archives of Psychiatric Nursing , 6 (5), 287�/295.
SIEGEL, K., GLUHOSKI, V. & KARUS, D. (1997). Coping and mood in HIV-positive women. Psychological Reports , 81 ,
435�/442.
VARNI, J.W., KATZ, E.R., COLEGROVE, R. & DOLGIN, M. (1993). The impact of social skills training on the adjustment
of children with newly diagnosed cancer. Journal of Paediatric Psychology , 18 (6), 751�/767.
WADE, S.L., YEATES, K.O., BORAWSKI, E.A., TAYLOR, H.G., DROTAR, D. & STANCIN, T. (2001). The relationship of
caregiver coping to family outcomes during the initial year following paediatric traumatic injury. Journal of
Consulting and Clinical Psychology , 69 (3), 406�/415.
WOLF, T., BALSON, P., DRALLE, P., GAUMER, R., MORSE, E., WILLIAMS, M. & SIMON, P. (1991). A biopsychosocial
examination of symptomatic and asymptomatic HIV-infected patients. International Journal of Psychiatry in
Medicine , 21 (3), 263�/279.
WOLTERS, P.L. & BROUWERS, P. (1998). Evaluation of neurodevelopmental deficits in children with HIV infection. In:
GENDELMAN, H. E., LIPTON, S. A., EPSTEIN, L. & SWINDELLS, S. (Eds), The Neurology of AIDS (pp. 425�/442).
New York: Chapman & Hall.
292 S. C. MARTIN ET AL.
Dow
nloa
ded
by [
Uni
vers
ity o
f A
lber
ta]
at 1
3:43
15
Oct
ober
201
4