the difficult patient psychodynamics: coping styles, defense mechanisms and countertransference...
TRANSCRIPT

The difficult patient
Psychodynamics:Coping styles, defense mechanisms and
countertransference
Suicide: Assessment of suicide risk and management

Consult question
• „Sixty-five year old male with end-stage renal disease on hemodialysis. He has been kicked out of all other dialysis centers due to his obnoxious behaviour. He hollers and berates the staff. How to manage his behaviour?“

Difficult patient presents with
Vague and generalized somatic symptomsDepressionAnxietyMedication non-adherenceA personality disorderExcessive demands and repeated visits
15% of patients labeled as
difficult

Difficult patients evoke strong emotional reactions
• Aversion• Fear• Despair• Malice

Remember!Medical illness and hospitalization is stressful
• Experiencing a medical illness requiring admission is a narcissistic injury: a threat to self-worth or self-esteem
• Patient re-examines his self-view while confronting the impermanence of life
• Patient feels defective, weak and less desirable• Being in a hospital is very uncomfortable, body exposure,
personal and bodily intrusions• Patients are separated from their comfortable environment
and have to accept dependency on their caregivers

Understand psychodynamic factors
Personality structure of the patient: • coping styles: consciously applied behavioral
actions• defense mechanisms: unconscious,
psychological processes used by patients to deal with reality and to maintaint self-image
Emotions experienced by the team: countertransference

Personality
• Personality types• Personality disorders
Continuum
Personality types
• Personality: a combination of characteristics that predisposes them to think, feel and behave
• Inborn: temperament• Environmentally influenced: character

Identify personality types
Quizz:Have you seen this
picture before?a) Yesb) No
c) Do not know
SanguineMelancholicPhlegmatic
Choleric

Personality disorder
Individual uses a personality style:• Rigid• Extreme• Maladaptive• Damaging to self or others• Result: impairment in interpersonal, social or
occupational domains

Coping styles and illness behavior
• How an individual manages and attempts to alter stressful situation: consciously applied behavioral actions
• Problem-focused: Seeking information, planning, taking action
• Emotion-focused: Focusing on positive aspects of the situation, mental or behavioral disengagement and seeking emotional support from others
Name positive aspect ofthe illness and treatment

Healthy and adaptive copers
• Use combination of problem and emotion-focused copingto deal with a stressor and use different strategies for varied situations
• Are optimistic, practical, flexible and composed
• View illness as a challenge, strategy, value

Poor copers
• Are passive,• Deny excessively• Hold rigid and narrow views• Unable to make decisions• Paradoxically they have moments of
impulsivity and unexpected compliance• View illness as an enemy, punishment,
weakness, relief or irreparable loss

Coping style Description
Confrontative Hostile or aggressive efforts to alter a situation
Distancing Efforts to mentaly detach self from a situation
Self-controlling Attempting to regulate one´s feelings or actions
Seeking social support Atempting to seek emotional support or information from others
Accepting responsibility Accepting a personal role in the problem
Escape-avoidance Efforts to escape/avoid a problem or situation, both cognitively and behavioraly
Planful problem solving Attempting to come up with solutions to alter a situation
Positive re-appraisal Re-framing a situation in more positive light

Defense mechanisms
• Defenses: used by all individuals to protect the self from anxiety
• To provide refuge from a situation with which one cannot currently cope
• Psychotic, immature, neurotic and mature
What defenses are used by „difficult patients?“

Defense mechanism
Description
MatureHumor Emphasizing the amusing or ironic aspect of the conflict or stressors
Sublimation Channeling unacceptable impulses into more constructive activities
Suppression Intentional exclusion of material from conscioussness
NeuroticDisplacement Transfer of unacceptable thoughts, feelings or desires from one object to a less threatening substitute
Isolation of affect
Separation of painful idea /event from feelings associated with it
Rationalization Inventing a socially acceptable and logical reason why one is not bothered
Reaction formation
Going to the opposit extreme to overcompensate for unacceptable impulses
Repression Involuntary forgetting of a painful eventImmatureActing out Performing an action to express unconscious emotional conflicts usually antisocial in nature
Devaluation Exagerating negative qualities of othersIdealization Overestimating the desirable qualities of self or others
Passive aggression
Indirect and passive expression of anger towards others
Projection Attribution of own unaccpetable desires /imulses to another person
Regression Reversion of personality to a lower level of expression
Splitting Separating people and actions into categories of all good and all bad
PsychoticProjective identification
Projecting a negative aspect of the self onto another and then coercing the other into identifying with the projected emotion
Psychotic denial Failing to recognize obvious implications or consequences of a thought, act or situation
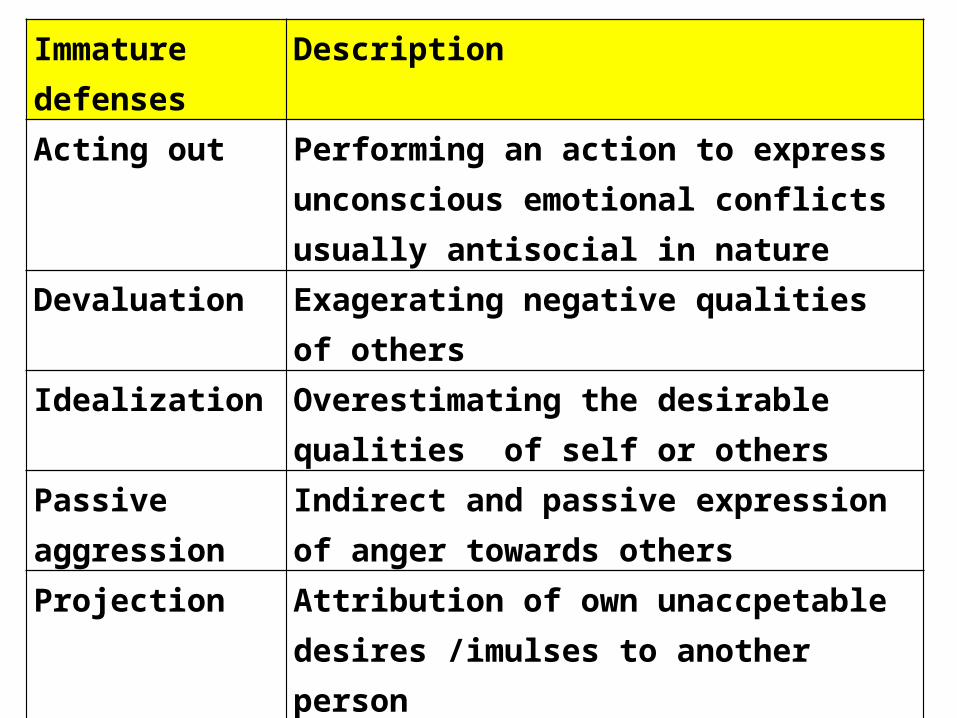
Immature defenses
Description
Acting out Performing an action to express unconscious emotional conflicts usually antisocial in nature
Devaluation Exagerating negative qualities of othersIdealization Overestimating the desirable qualities of self
or others
Passive aggression Indirect and passive expression of anger towards others
Projection Attribution of own unaccpetable desires /imulses to another person
Regression Reversion of personality to a lower level of expression
Splitting Separating people and actions into categories of all good and all bad
Immature defenses
• Characteristic of the cluster B personality disorders: antisocial, borderline, histrionic, narcissistic
• Irritating to others as this defense style transmits patients „shame, impulses and anxiety to those around them“
• Make others suffer (x neurotic defenses cause the self to suffer)
Do not confront the patient directly, as defenses are unconscious!
Risk of further escalation of oppositional behavior!

Identify defenses and understand behaviors
• Awareness of the potential for eidealizing/devaluing: Glowing praises follow by harsh criticizing
• Awareness of splitting: The patient tend to divide the medical staff as „all good“ or „all bad“ caregivers

Physician´s factors and countertransference
• Doctor – vs. Patient centered approach?• Strict bio-medical model – vs. Psychosocial
approach?• Countertransference: reactions to a patient
that represents the past life experiences of the clinician
Examples?

Management
• Ensure that the basic needs of the patient (privacy, food, etc.) including maintaining consistent staff are met.
• Attempt to understand and empathize with the patient and acknowledge the real stresses in the current situation (OARS!!!)
• Accept the patient´s limitations by not directly confronting immature defenses or poor coping styles
• Set firm limits on unreasonable expectations by consistently declaring „in order to provide the best medical care possible….“Reasonable requests should not be refused.
Understand them, recognize the defense
mechanisms and coping styles

Management
• Do not directly confront the patient´s entitlement or rage
• Gently discuss any irrational fears about the illness or treatment and assess ability for reality testing (transient psychosis?)
• Acknowledge and empathize with the primary team´s countertransference. Discuss with them the universality of these emotions.
• Use psychopharmacology when appropritate

Psychopharmacology
• depression and anxiety: SSRI, bupropion, avoid benzodiazepines
• insomnia: mirtazapine, trazodone, melatonin• irritability/impulsivity: divalproex,
quetiapine, olazapine, risperidone
Suicide
„There are only two kinds of psychiatrists: those who have had patients commit
suicide, and those who will.“
JZ

Suicide
• No treatment outcome is more devastating than suicide.
• Coping with the devastating aftermath – both in MDs and psychotherapists and families: shock, guilt and shame, isolation, grief, dissociation, crises of faith about psychotherapy and other treatments

Suicide
• 11th leading cause of death in te USA• 30 000 suicide attempts are reported annually in the USA• 5-6% of attempts occur in hospitals• Study of 76 patients who commited suicide on an inpatient
psychiatric unit, 78% denied suicide ideation or intent as their last communication
• Severe agitation or anxiety was found in 79% of the patients during the week before their suicide
Do not rely only on oral reports of patients denying suicidal ideas, but pay closer attention
to psychic and motor anxiety as a risk factor.

Medical conditions as predictors of suicide
• Severe pain • Congestive heart failure• Seizure disorder• Chronic lung disease

Suicide: Questions
• Have you ever felt that life was not worth living?• Did you ever wish you could go to sleep and just not
wake up?• Have things ever reached the point where you ´ve
thought about harming yourself?• When did you first notice such thoughts?• Have you made a specific plan to harm or kill
yourself? • If so, what does the plan include?
Source: APA Practice Guidelines for Assessment of Patients with Suicidal behaviors
AS
Suicide risk assessment
• The presenting suicide ideation and behaviors
• Recent suicide ideation and behavior over the preceding 8 weeks
• Past suicide ideation and behaviors• Immediate suicide ideation and future
suicide plans
Suicide risk assessmentS sex: maleA age: >45, <19D depression
P previous attemptsE ethanol abuseR rational thinking loss (psychosis?)S social suppot lackingO organized planN no spouseS sickness (somatic illness with pain)

Management
Each positive answer = 1 point
• 0-2: low risk• 3-4: medium risk; outpatient treatment,
observation• 5-6: high risk; hospitalization, especially in cases
without social support• 7-10: very high risk; hospitalization
Write it to the medical record!

Literature
• Amos JJ. And Robinson RG. Psychosomatic Medicine. An introduction to consultation-liaison psychiatry. Cambridge, 2010