copd alison boland str respiratory medicine. aims & objectives overview of copd recap basic...
TRANSCRIPT

COPD
Alison Boland
StR Respiratory medicine

Aims & Objectives
Overview of COPD
Recap basic knowledge
Update on COPD
Know when to use nebulisers and home oxygen therapy
The role of NIV in palliative setting / end stage COPD
Gain patient, carer and personal view about COPD

GOLD Definition
Airflow limitation
Not fully reversible
Progressive
Abnormal inflammatory response to noxious particles or gases

CHRONIC
Develops slowly
Early symptoms often go un-noticed
Symptoms present for much of the time
Progressive dyspnoea over time.
Worse on exercise

OBSTRUCTIVE
Narrowing of the bronchi
3 mechanisms:
•Bronchial walls become weakened•Mucus secretion into the bronchi.•Muscle spasm

Natural History

Activity
BREATHE THROUGH THE STRAW FOR A MINUTE
THNIK ABOUT HOW THIS FEELS.


Diagnosis
FEV1/FVC <70%
Post bronchodialator FEV1 <80% predicted.
FEV1/FVC more sensitive.

Diagnose COPD: assessment of severity
• Assess severity of airflow obstruction using reduction in FEV1
NICE clinical guideline 12
(2004)
ATS/ERS 2004 GOLD 2008 NICE clinical guideline 101
(2010)
Post-bronchodilato
r FEV1/FVC
FEV1 % predicted
Post-bronchodilato
r
Post-bronchodilator
Post-bronchodilator
< 0.7 80% Mild Stage 1 (mild) Stage 1 (mild)*
< 0.7 50–79% Mild Moderate Stage 2 (moderate)
Stage 2 (moderate)
< 0.7 30–49% Moderate Severe Stage 3 (severe) Stage 3 (severe)
< 0.7 < 30% Severe Very severe Stage 4 (very severe)**
Stage 4 (very severe)**
* Symptoms should be present to diagnose COPD in people with mild airflow obstruction** Or FEV1 < 50% with respiratory failure
[new 2010]

Patient with COPD
Palliative care
Smoking Breathlessness & exercise limitation
Frequent exacerbations
Respiratory failure
Cor pulmonale
Abnormal BMI
Chronic productive
cough
Anxiety & depression
Managing stable COPD
Assess symptoms/problemsManage those that are present as below
Patients with COPD should have access to the wide range of skills available from a multidisciplinary team

Treatment options
Pharmacological
Bronchodilators
Steroids
Antibiotics
Mucolytics
Antitussives
Narcotics

Treatment options
Non – pharmacological
•Pulmonary rehabilitation•Oxygen •NIV•Surgery
Bullectomy
Lung volume reduction surgery
Lung transplantation


Managing stable COPD: inhaled therapies
SABA or SAMA as required*Breathlessness and exercise limitation
Exacerbations or persistent breathlessness
Persistent exacerbations or breathlessness
LABA LAMADiscontinue
SAMA________
Offer LAMA in preference to regular SAMA four times a
day
LABA + ICS in a combination
inhaler________
Consider LABA + LAMA if ICS
declined or not tolerated
LAMADiscontinue
SAMA________
Offer LAMA in preference to
regular SAMA four times a day
FEV1 ≥ 50% FEV1 < 50%
LABA + ICS in a combination
inhaler________
Consider LABA + LAMA if ICS
declined or not tolerated
LAMA + LABA + ICS in a combination
inhaler
Offer Consider* SABAs (as required) may continue at all stages

BronchodilatorsIndividual effects unpredictable
Inhaled:
•Salbutamol (‘Ventolin’)•Ipatropium (‘Atrovent’)•Salmeterol (Serevent)•Terbutaline (‘Bricanyl’)•Tiotropium (‘Spiriva’)•Indacterol (‘onbrez)
Oral: Theophyllines (‘Uniphyllin’, ‘Phyllocontin’)

Inhaler technique!!

Steroids
Inhaled – Seretide, Symbicort
Oral prednisolone
Do not modify long term decline in FEV1

Oral therapy
Theophylline
Carbocisteine
Opioids
Anti anxiolytics

Nebulisers
On maximum medical therapy
Use salbutamol only
1 month trial
No improvement in symptoms then stop

New(ish) therapies
Indacterol
Roflumilast
(Azithromycin)

Indacaterol
Long acting Beta agonist
Rapid onset of action
24 hr duration of action
150micrograms od
Future use as add on to tiotropium

Phosphodiesterase inhibitors
Roflumilast
Severe COPD (FEV1 <50%)
Hx Chronic bronchitis, frequent exacerbations
500micrograms od
Reduces rate of moderate to severe exacerbations

Azithromycin
Macrolide antibiotic
Recurrent exacerbations
On maximum therapy
Long term 250mg x3 week
Caution re side effects

Oxygen provision
Long term oxygen therapy
Ambulatory oxygen
Short burst oxygen

LTOT
FEV1 <50% predicted OR < 1.5l
Signs of cor pulmonalae
Sats <92%
PO2 <7.3 (8kPa)
Drying of nasal passages, oxygen toxicity,
Palliative care – target saturations not indicated

Ambulatory Oxygen
O2 use during exercise /ADL
LTOT patients
Objective evidence of desaturation on exercise

Short burst oxygen
Or Palliative O2
To relieve SOB
Excludes LTOT & ambulatory oxygen users


HOOF
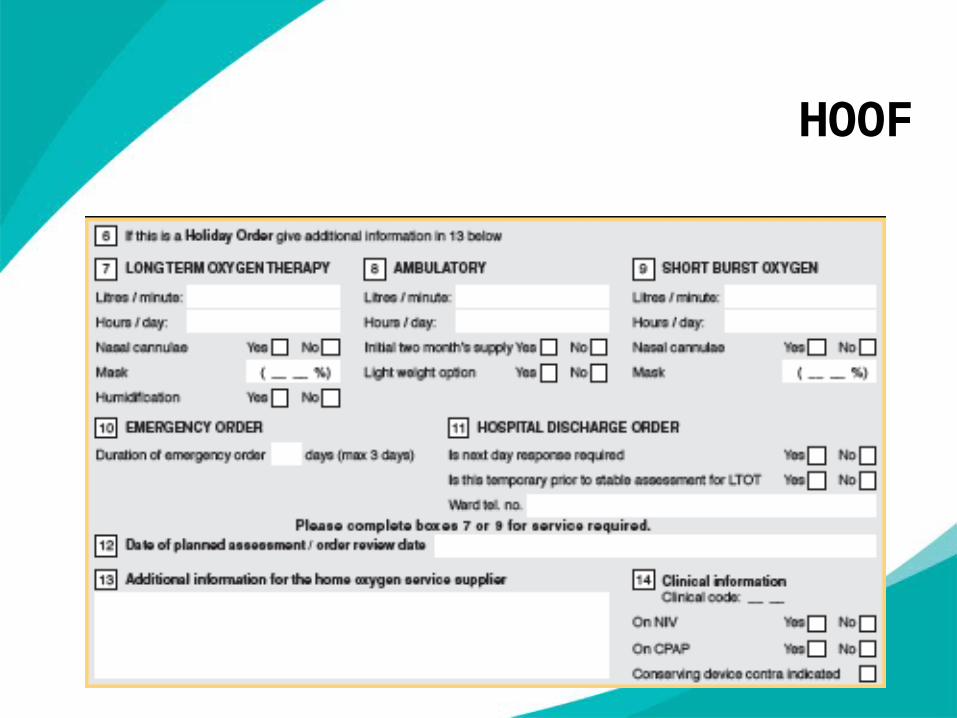
HOOF

Non invasive ventilation
Home NIV
•Recurrent acute type 2 respiratory failures •Intolerance LTOT•Increased co2 with symptoms •Overlap OSA / Obesity hypoventialtion
End of life care

Chronic disease management
Stop smoking
Prn Bronchodilator
Annual flu jab
Pneumococcal vaccine (5yrs)
Regular exercise
Maintain weight normal range

NutritionUnderweight usually
BMI <20
Assess co morbidities
Social factors
Encourage snacking, Higher fat foods
Supplements after 1 month of above
Dietician advise

Pulmonary rehab

Pulmonary rehab
SOB waking on level ground at normal pace
2hr sessions, 6 weeks
Motivated patients

Patient views about COPD
Key Messages
Consider Azithromycin in recurrent exacerbations
Prescribe short burst O2 with caution – expensive and little evidence
Pulmonary rehabilitation important multidisciplinary management
Finally remember how breathing through a straw felt!

Any Questions?