construction and renovation: infection control considerations ling...an impact on hais. and...
TRANSCRIPT

Construction and Renovation: Infection Control Considerations
Dr Ling Moi LinDirector
Infection Prevention & EpidemiologySingapore General Hospital

Construction and renovation projects have an impact on HAIs

and renovation among the published reports was 48%, rangingfrom 12.5% after surgery to 67% in rheumatology patients, pre-mature infants, or nephrology and dialysis patients (Table 2).Thus, the mortality of fungal outbreaks and infections was sub-stantially high but varied greatly according to underlying con-ditions and infection types.
RESERVOIRS AND SOURCES OF FUNGIOUTBREAKS AND INFECTIONS ASSOCIATEDWITH CONSTRUCTION AND RENOVATION
Construction was the most common type of source in this re-view (38 articles [78%]), followed by renovation (19), demoli-tion (4), and excavation (3). The data on reservoirs andsources are summarized in Table 1. Environmental sources inconstruction-related settings were described as follows: inflowof unfiltered outside air, backflow of contaminated air, air
filters, fireproofing materials, air conditioners, duct systems,and dust above false ceilings [55], thereby enabling fungalspores to be aerosolized and disseminated throughout hospitalareas. Aspergillus species can also be isolated from hospitalwater samples and be involved in invasive aspergillosis [52,63, 64]. However, it remains unclear how Aspergillus species iso-lated from hospital water contribute to nosocomial waterborneAspergillus infections, and there are no criteria for determiningwater contamination levels that have been correlated with a riskof fungal infections.
LABORATORY TESTING, AIR SAMPLING, ANDMOLECULAR TYPING IN INVESTIGATION OFFUNGAL OUTBREAKS AND INFECTIONS
In the special settings of construction and renovation, severalstudies described the monitoring of Aspergillus species usingquantitative polymerase chain reaction (PCR) of air samples[65, 66] or serum Aspergillus galactomannan in pediatric pa-tients with allogeneic stem cell transplant [67]. Although Asper-gillus infections were finally diagnosed at autopsy in manyarticles reviewed, the diagnosis of invasive aspergillosis duringa patient’s lifetime remains difficult. Clinical signs and radiolog-ical findings for Aspergillus infections can be nonspecific, and inless invasive testing methods, there are diagnostic limitationsfor conventional culture methods and serum biomarkers (eg,galactomannan and [1→3]-β-D-glucan assays) due to the lowsensitivities and for clinical implementation of PCR assays be-cause of the potential environmental contamination of Aspergil-lus DNA [68–72]. Recently, detection of Aspergillus antigen bythe lateral-flow device as a point-of-care test [73] or Aspergillussecondary metabolite signature in breath by thermal desorp-tion–gas chromatography/mass spectrometry [72] may bepromising, but further investigation is needed.
Air sampling may be used to measure airborne fungal levelsinside and outside of hospitals before, during, and after
Figure 1. Trend of fungal outbreaks and infections associated with con-struction, renovation, and demolition.
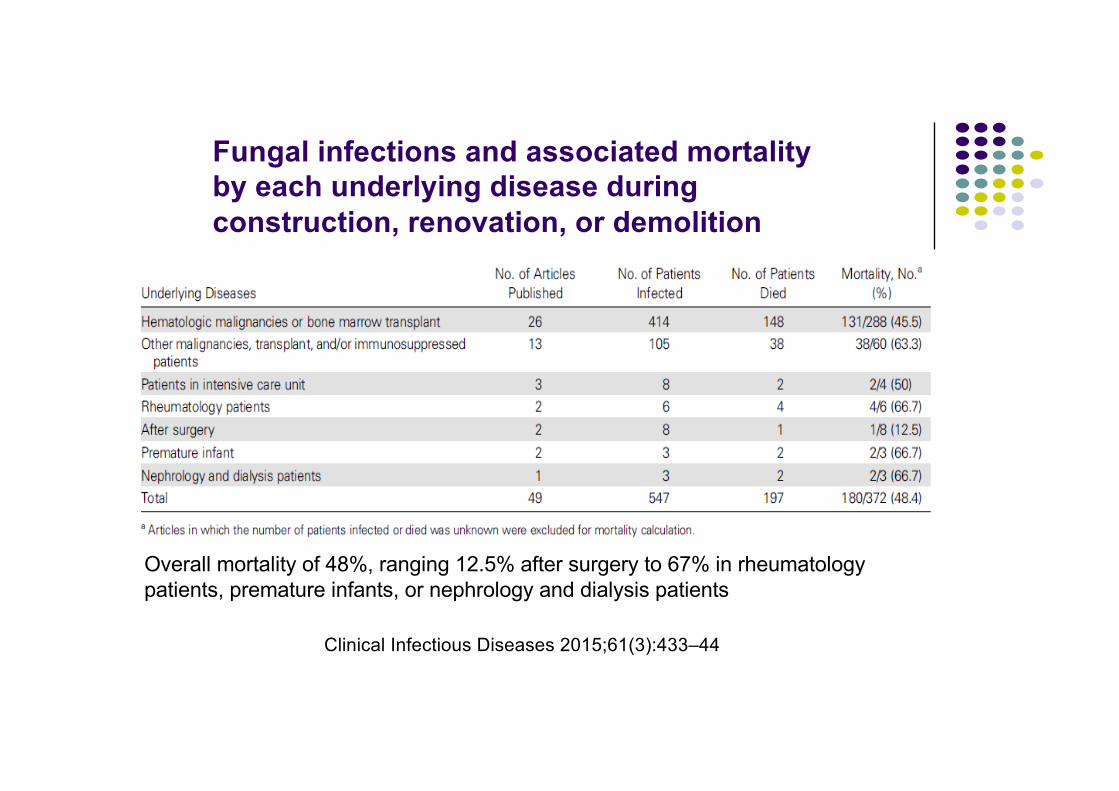
Table 2. Fungal Infections and Associated Mortality by Each Underlying Disease During Construction, Renovation, or Demolition
Underlying DiseasesNo. of Articles
PublishedNo. of Patients
InfectedNo. of Patients
DiedMortality, No.a
(%)
Hematologic malignancies or bone marrow transplant 26 414 148 131/288 (45.5)Other malignancies, transplant, and/or immunosuppressedpatients
13 105 38 38/60 (63.3)
Patients in intensive care unit 3 8 2 2/4 (50)Rheumatology patients 2 6 4 4/6 (66.7)After surgery 2 8 1 1/8 (12.5)Premature infant 2 3 2 2/3 (66.7)Nephrology and dialysis patients 1 3 2 2/3 (66.7)Total 49 547 197 180/372 (48.4)
a Articles in which the number of patients infected or died was unknown were excluded for mortality calculation.
440 • CID 2015:61 (1 August) • HEALTHCARE EPIDEMIOLOGY
Downloaded from https://academic.oup.com/cid/article-abstract/61/3/433/490927by gueston 29 August 2018
Fungal outbreaks associated with construction, renovation and demolition
I N V I T E D A R T I C L E H E A L T H C A R E E P I D E M I O L O G YRobert A. Weinstein, Section Editor
Review of Fungal Outbreaks and InfectionPrevention in Healthcare Settings DuringConstruction and Renovation
Hajime Kanamori,1,2 William A. Rutala,1,2 Emily E. Sickbert-Bennett,1,2 and David J. Weber1,21Hospital Epidemiology, University of North Carolina Health Care, and 2Division of Infectious Diseases, University of North Carolina School of Medicine,Chapel Hill
Hospital construction and renovation activities are an ever-constant phenomenon in healthcare facilities, caus-ing dust contamination and possible dispersal of fungal spores. We reviewed fungal outbreaks that occurredduring construction and renovation over the last 4 decades as well as current infection prevention strategiesand control measures. Fungal outbreaks still occur in healthcare settings, especially among patients with hema-tological malignancies and those who are immunocompromised. The causative pathogens of these outbreakswere usually Aspergillus species, but Zygomycetes and other fungi were occasionally reported. Aspergillusmost commonly caused pulmonary infection. The overall mortality of construction/renovation-associated fun-gal infection was approximately 50%. The minimal concentration of fungal spores by air sampling for acquisi-tion of fungal infections remains to be determined. Performing infection control risk assessments andimplementing the recommended control measures is essential to prevent healthcare-associated fungal outbreaksduring construction and renovation.
Keywords. fungal outbreaks; Aspergillus; healthcare-associated infections; construction; renovation.
Numerous fungal outbreaks have occurred in health-care settings and have been a serious threat to immuno-compromised hosts [1]. Construction and renovationactivities can cause serious dust contamination and dis-perse large amounts of fungal spores, and constructionactivity has been reported to be an independent risk fac-tor for invasive fungal infections [1,2]. A previous reviewrevealed that construction or renovation activities withinthe hospital or in surrounding areas accounted for ap-proximately half of the sources of healthcare-associatedAspergillus outbreaks [2]. Hospital construction andrenovation activities are an ever-constant phenomenon[2], and the cost of hospital construction is expected tobe nearly $200 billion dollars by 2015 in the United
States [3]. It is estimated that 5000 deaths due to con-struction-related infections occur each year in health-care settings [4].
The goal of this review article was to (1) examine fun-gal outbreaks that were related to hospital construction,renovation, and/or demolition over the last 4 decades;and (2) offer infection prevention and control measuresin healthcare facilities based on previous experiences,evidence, and guidelines.
SEARCH AND SELECTION CRITERIA
To select relevant articles, we searched the published lit-erature in PubMed using the following keywords [AllFields]: (aspergillosis OR Aspergillus OR ZygomycetesOR Mucor OR mycoses OR mycosis OR fungi) AND(hospital OR healthcare OR nosocomial) AND (con-struction OR renovation) AND (outbreak OR contam-ination OR infection OR prevention OR control). From1974 through 2014, 158 references were carefully re-viewed. Additional reports were also identified throughthe references cited. Finally, 49 studies [5–53] were
Received 10 February 2015; accepted 4 April 2015; electronically published 13April 2015.
Correspondence: Hajime Kanamori, MD, PhD, MPH, Hospital Epidemiology, Uni-versity of North Carolina Health Care, 1001 West Wing CB 7600, 101 Manning Drive,Chapel Hill, NC 27514 ([email protected]).Clinical Infectious Diseases® 2015;61(3):433–44© The Author 2015. Published by Oxford University Press on behalf of the InfectiousDiseases Society of America. All rights reserved. For Permissions, please e-mail:[email protected]: 10.1093/cid/civ297
HEALTHCARE EPIDEMIOLOGY • CID 2015:61 (1 August) • 433
Downloaded from https://academic.oup.com/cid/article-abstract/61/3/433/490927by gueston 29 August 2018
Fungal infections and associated mortality by each underlying disease during construction, renovation, or demolition
Overall mortality of 48%, ranging 12.5% after surgery to 67% in rheumatology patients, premature infants, or nephrology and dialysis patients
Clinical Infectious Diseases 2015;61(3):433–44

Invasive Aspergillosisl Caused by extremely common mold
l Spread through air easily
l Can be difficult to diagnose in severely immunosuppressed patients
l Mortality over 50%
l Prevention of exposure is Key

Patients at riskl Bone marrow transplant patients
l Hematology and oncology patients who develop severe and prolonged neutropenia
l Solid organ transplant patients (intestinal > lung > liver > heart > kidney)
l Patients who receive prolonged high-dose corticosteroids (~1 mg/kg)

Sources of Aspergillus spl Soil
l Dust in ventilation systems
l Contaminated dust dislodged during hospital renovation l Carpets, wall papers

How do fungi get in?l Fresh air intakes of HVAC
systemsl Open doors and windowsl Attached to people’s clothes,
shoes, and skinl Attached to new building
materials

Dust moves!

Ideal conditions for AspergillusNutrientsl Gypsum boardl Cellulose ceiling tilesl Carpetsl Upholsteryl Fibreglass lined ductsl Dirt on surfaces

Other bugs to look out for171 patients during a six-month period coinciding with large-scale construction work beside the hospital
Most patients presented with B cereus bacteraemia (146/171; 85.4%) with 46/171 (26.9%) requiring extended treatment courses with vancomycin or other interventions

Sampling confirmed extensive airborne dispersal inside the hospital, including isolation rooms and air-conditioned wards. Hospital linen was heavily contaminated [7403 cfu/cm2; 95% confidence interval (CI): 6349 - 8457; for 30 towels sampled], encouraged by inappropriate storage in airtight plastic bags (4437 cfu/cm2; CI: 3125 - 5750) compared with storage in porous canvas bags (166 cfu/cm2; CI: 76 - 256; P < 0.001)

l 4 episodes of peritonitis involved infection by more than one organism
l Air sampling of the environment detected a median of 110 colony forming units of bacteria per cubic meter of air, 10% of which were found to be Acinetobacter baumaniil The source of this polymicrobial outbreak was attributed to
the bamboo scaffolding structure covering the external wall of the hospital during renovation

Design matters!E. meningoseptica was more likely to be recovered from an aerator in a hand hygiene sink frequently used for rinsing re-usable patient care items or disposal of patient secretions (odds ratio 6.65, 95% confidence interval 2.22 -19.92; P < 0.001) compared with sinks that were not misused
Balm MND et al

Water-borne infectionsl Plumbing system
l Leaking water pipes causing damage to false ceiling
l Dust and mold particles were dispersed
l Soil contaminated with Legionella sp. entered water supply at time of installation of new pipes

Water-borne infection preventionl Regular maintenance and inspection of water supply system to
minimize stagnation and back flow and for temperature control
l Regular clean and maintain water faucet aerators to prevent and control for Legionella
l Avoid decorative water fountains in high risk patient care areas
l Where fountains are used - regular clean and maintenance

To minimize risk of HAIsl Build according to specifications (international standards)
l Proactive risk assessment before constructionl Infection control risk assessment (ICRA) matrix
l Control measures implemented
l Monitoring to assess efficacy of control measures

Is facility designed to support prevention and control of infection practice?
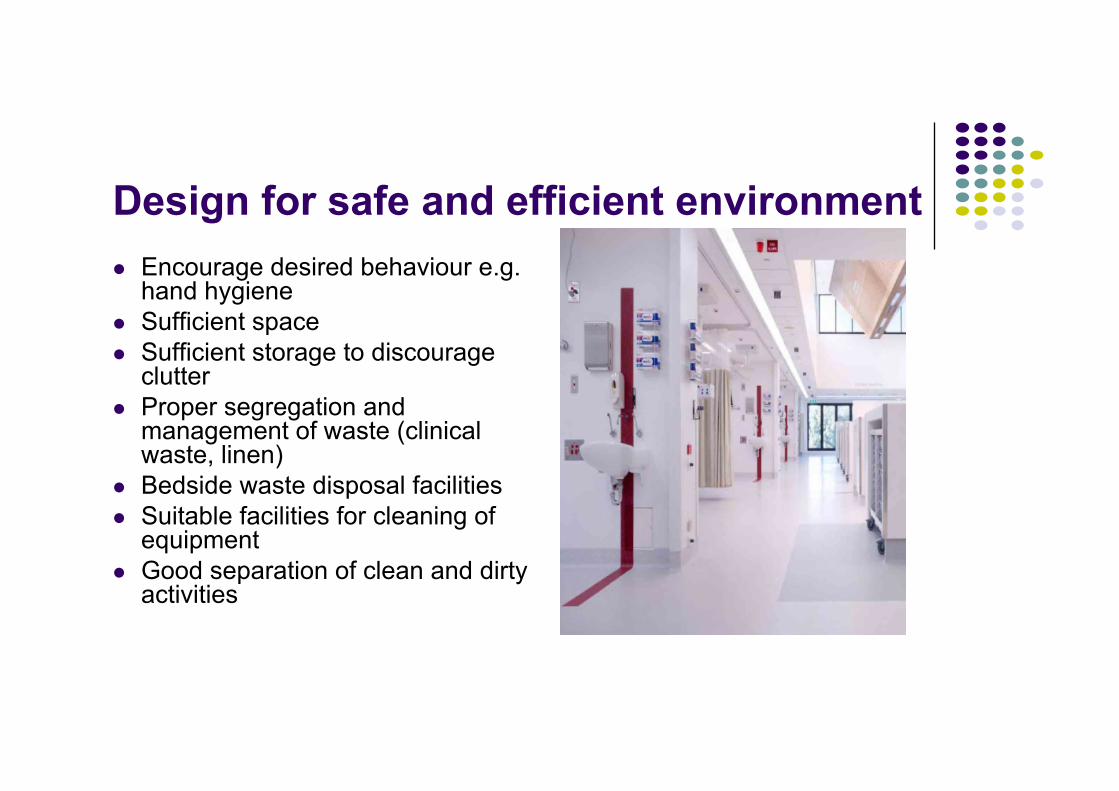
Design for safe and efficient environmentl Encourage desired behaviour e.g.
hand hygienel Sufficient spacel Sufficient storage to discourage
clutterl Proper segregation and
management of waste (clinical waste, linen)
l Bedside waste disposal facilitiesl Suitable facilities for cleaning of
equipmentl Good separation of clean and dirty
activities

Balancing use of materials – efficient and easy to cleanl Facilitate cleanliness and cleaning
l Impervious, smooth, seamless finishesl Run hard flooring up to walls (easy-to-clean cove)l Eliminated dead-legs and blind ends in water systeml Hands-free operation of utilitiesl Integral blinds as alternative to curtains at windows

Design principlesl Design for easy cleaning
l Finishes that are easy to cleanl Flooring in clinical areas are seamless, smooth, slip-resistant, easily
cleaned and water-resistantl Concealed supply pipework

Design for optimal and safe flowl Logical progression between clean and dirty areas
l In pandemic, modular shut down to isolate areas
l Plan for separate clean and dirty flows for waste including linen.

Design and structure issuesl Design, number and type of isolation rooms
l HVAC
l Mechanical systems involving water supply and plumbing
l Number, type and placement of hand hygiene fixtures, clinical sinks, dispensers for soap, alcohol hand-rub, paper towels and lotion

Design and structure issuesl Sharps disposal unit placementl Accommodation for PPEl Surfaces – ceilings, tiles, walls, counters, floor covering and
furnishingsl Utility rooms – soiled, clean, holding, workroomsl Clinical wastel Linen / laundryl Storage of used and sterile medical devices

Patient roomsl US, Europe, UK, Canada – single rooms for new acute care
facilityl UK – 50% single rooms for non-acute care facility
l Ireland – not more than 3 beds per cubicle!
l En-suite toilet

Isolation roomsl UK
l 1:150 for new general acute care facilityl 1:75 for regional and tertiary care facility
l Local recommendationl Acute care – 20% of beds
l 1 AII room per 100 bedsl Community hospital – 15% of beds
l 1 AII room per 200 bedsl Nursing home – 10% of beds

Item
Mode of Transmission
Targeted Pathogens or Infections CDC FGI 2010 Comments
Positive pressure rooms Air Multiple
Recommended for use in all protective environments and operating rooms (IB, IC)
Recommended for PE rooms.
Intent of positive pressure is to protect patient from pathogens external to room. Recommended air exchange rate to accompany positive pressure depends on room use.
Negative pressure rooms Air
Multiple (e.g., Mycobacterium tuberculosis, rubeola (measles), varicella-zoster (chickenpox)
Recommended for use in airborne infection isolation rooms (IB, IC)
Recommended for Airborne Infection Isolation (AII) rooms
Intent of negative pressure is to protect others from airborne pathogens harbored by infected patient in room. Recommended air exchange rate to accompany negative pressure depends on whether or not construction is new.
!
Isolation rooms

Pseudomonas aeruginosa outbreakl Outbreak at haematology wards from 15 November 2010 to 24 April 2011,
involving 11 patients l Contaminated sink drainage
Ling, Moi Lin and How, Kue Bien. Pseudomonas aeruginosa outbreak linked to sink drainage design [online].Healthcare Infection 18(4) 143-6

Research
MJA 198 (5) · 18 March 2013268
patient died due to clinical CRE infec-tion. Patient 1 had a prolonged CREbacteraemia that responded toremoval of a central venous catheter,the presumed source of infection.
A total of 111 rectal swabs werecollected from 71 patients. Only onepatient (Patient 11) was CRE-positivewith an E. coli isolate detected.
Antibiotic resistance profiles of clini-cal isolates indicated resistance to �-lactams and meropenem with MICs! 1 mg/L. All S. marcescens clinicalisolates were sensitive to piperacillin/tazobactam, ciprofloxacin and ami-kacin, while K. pneumoniae and E. coliwere only sensitive to amikacin. S.marcescens environmental isolatesshowed a higher meropenem MIC of! 16 mg/L.
S. marcescens was the only speciesrecovered from environmental samplesand was isolated persistently, evenafter six attempts to decontaminate thegrates and drains of eight of the 11central sinks in the ICU. Tap spout andwater cultures were negative for CRE.
Three of the four S. marcescens clin-ical isolates from 2010 and 2011 wereindistinguishable or closely related byPFGE to four isolates from sinks. S.marcescens was isolated from an inter-costal catheter swab of Patient 4,matching two sink isolates; Patient 5had an endotracheal aspirate identicalto two different sink locations; andthe urine isolate from Patient 6 was
closely related to a different sink. Theisolate from Patient 7 was unable to betyped by PFGE.
Sink inspection revealed aged anddeteriorating porcelain, even thoughsinks were only installed in 2005. Sinkdesign did not comply with Australa-sian clinical design standards,8 with asmall, shallow sink and a tap thatdirected water over the drain (Box 2).The design of the ICU sinks led to pooruse for hand hygiene (although meas-ured hand hygiene compliance usingalcoholic hand rub was around 70%
within the unit) and the potential fororganisms residing down the drain tobe splashed back onto staff hands orcontaminate patient areas. It was alsorevealed that the handwashing sinkshad been used incorrectly, with staffdisposing clinical waste and residualantibiotics directly into drains. Furtherenquiry also revealed that a singlebrush had been used to clean downthe drains of all sinks in the ICU with-out disinfection between sinks.
Cleaning was attempted in an effortto rid the organisms from the sinks.
1 Demographics and intensive care unit (ICU) admissions for patients with carbapenem-resistant Enterobacteriaceae isolates
PatientUnderlying condition
Year of first
positive culture
Culture type Organism
Total hospital
stay (days)
ICU stay
(days)
ICU admissions
in past 12 months
Total carbapenem
therapy (days) Outcome
1 Small bowel perforation,
post-hernia repair
2009 Blood Klebsiella pneumoniae
229 134 0 14 Discharged
2 Urosepsis, multiorgan failure
2010 Urine K. pneumoniae 44 16 0 0 Discharged
3 Bilateral pneumonia
2010 Bronchial washings
K. pneumoniae 61 33 0 0 Discharged
4 Pneumonia 2010 Intercostal catheter swab
Serratia marcescens
44 32 0 2 Discharged
5 Pneumonia 2010 Endotracheal aspirate
S. marcescens 46 6 0 0 Discharged
6 Buttock abscess 2011 Urine S. marcescens 49 10 0 0 Discharged
7 Pneumonia 2011 Penile swab S. marcescens 46 22 0 3 Discharged
8 Congestive cardiac failure
2011 Sputum Enterobacter cloacae
57 4 0 0 Died
9 Ischaemic stroke 2012 Sputum K. pneumoniae 31 3 0 3 Died
10 Periprosthetic hip fracture
2012 Urine K. pneumoniae 46 8 0 0 Discharged
11 Ketoacidosis 2012 Rectal screen swab
Escherichia coli 11 4 2 0 Discharged
2 Existing design of intensive care unit sink compared with a design that complies with Australasian standards8
A: Existing sink, showing water spray directly over drain. B: Compliant sink design, showing larger basin and less forceful water flow directed away from drain, to prevent splash back and contamination with drain contents. ◆
Kotsanas D et al. MJA 2013; 198:267–269
Ten clinical isolates (Klebsiella pneumoniae [n = 5], Serratia marcescens [n = 4] and Enterobacter cloacae [n = 1]) and one screening isolate (Escherichia coli) containing the blaIMP-4 gene detected over the 30-month period.

ICU toilet roomsl FGI guidelines 2012 l Each ICU room must now have direct access to an enclosed toilet
room or a soiled utility room with a clinical (flushing rim) sink for disposal of bodily waste
at minimum, a toilet room and toilet equipped with a bedpan washer or a soiled utility room with a flushing clinical sink between every 2 ICU rooms
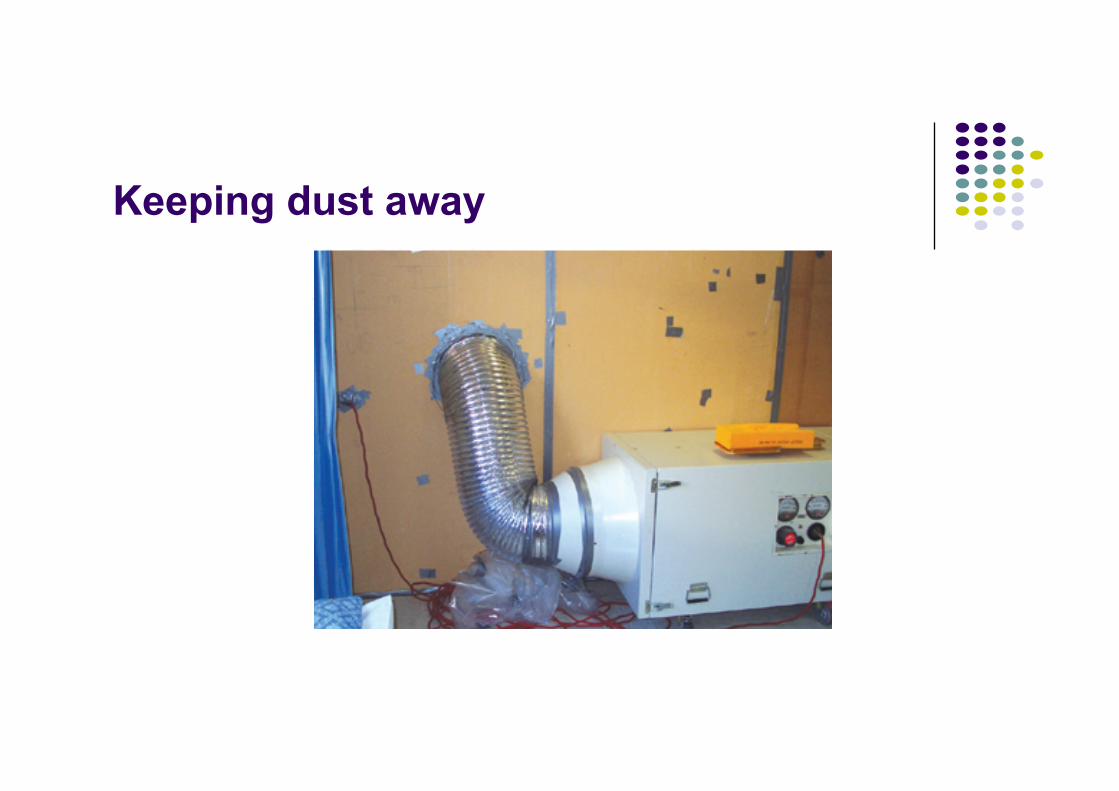
Keeping dust away
1312
After water damage or flooding, test plasterboard with a moisture meter. The plasterboard should be at the manufacturer’s moisture content within 72 hours or be replaced. This is critical for horizontal surfaces. These occurrences should be documented and reported on.
Negative pressurisation of the construction zone is essential to maintain correct airflow direction. The exhaust / extraction systems specified in the contract documentation must be constantly monitored and maintained to ensure no failures occur. These inspections should be documented and reported on.
If HEPA filtration is required, a person must be nominated as the responsible person for that duty. The filters should have differential pressure monitoring with alarms. Spare filter elements must be kept on hand. These inspections should be documented and reported on.Viable particle air sampling should be considered by the hospital to monitor the effectiveness of the barriers, pressurisation and housekeeping procedures. All air sampling should be documented and reported on.
vacuum cleaners disseminate huge quantities of dust and fungal spores and should not be used.
Control movement in and out of the site by restricting access to only those who have undergone site induction. This will assist in reducing the spread of contaminants. Document all inspections. Include a non-conformance system for defaults complete with a corrective and preventative action loop. All Inspections must be documented and reported on.
Hand-over and Pre-Occupation StageAfter hand-over it is the hospitals responsibility to ensure the area complies with hospital cleanliness standards for occupation. As a minimum the hospital should thoroughly clean and decontaminate all surfaces including walls, ceilings, and windows as well as in high-risk area ventilation systems, service cavities and ceiling spaces.
If air sampling and particle counts are being conducted, allow enough time for culturing and results prior to occupation. It is advisable to implement a program of air sampling in high-risk areas for a period of time after hand-over and occupation. Allow 48 hours for all culture results prior to occupation. Once all these tasks have been completed, re-certify HEPA filters and laminar / clean flow systems where installed.
A high level of site cleanliness is essential. Use tools with efficient dust extraction systems connected to HEPA filters. Tasks such as sanding plasterboard present a high level of potential risk; therefore only mechanical sanding should be used.
Demolition and jack hammering of concrete should be undertaken with a filter unit in close proximity. HEPA vacuuming, not sweeping, should be used to clean up. Conventional

Construction Activityl Type A: inspections and general upkeep activities, which do not generate
dust
l Type B: small scale, short duration activities, which create minimal dust
l Type C: any work that generates a moderate to high level of dust or requires demolition
l Type D: major demolition and construction projects requiring consecutive work shifts to complete

Patient risk groupsLow Risk Medium Risk High Risk Highest Risk
• Office areas
• Non-patient areas
• Cardiology• Echocardiography • Nuclear Medicine • Physiotherapy /
Occupational Therapy / Speech Therapy Department
• Radiology/MRI • Patient care areas not
covered under high or highest risk groups
• Public corridors (through which patients, supplies and linen pass)
• Lab not specified as high or highest risk groups
• Cafeteria• Kitchen• Material management
department• Linen room
• CCU• Emergency Medicine• Labour & Delivery• Laboratories (specimen) • Newborn Nursery • Ambulatory Surgery• Urology OT• Dialysis Centre• Haematology Centre• Endoscopy Centre• Paediatrics• Pharmacy • Surgical wards• Rehabilitation ward• Vascular and
interventional radiology
• Any areas caring for immuno-compromised patients
• Oncology ward• Bone marrow transplant
unit• Haematology ward• Neonatal ward• Burn Unit • Cardiac Cath Lab /
angiograph procedure areas
• Central Sterile Supply • Intensive Care Units • Medical wards • Isolation wards and
rooms• Operating theatres
including C-section rooms / labor OT
• Pharmacy admixture
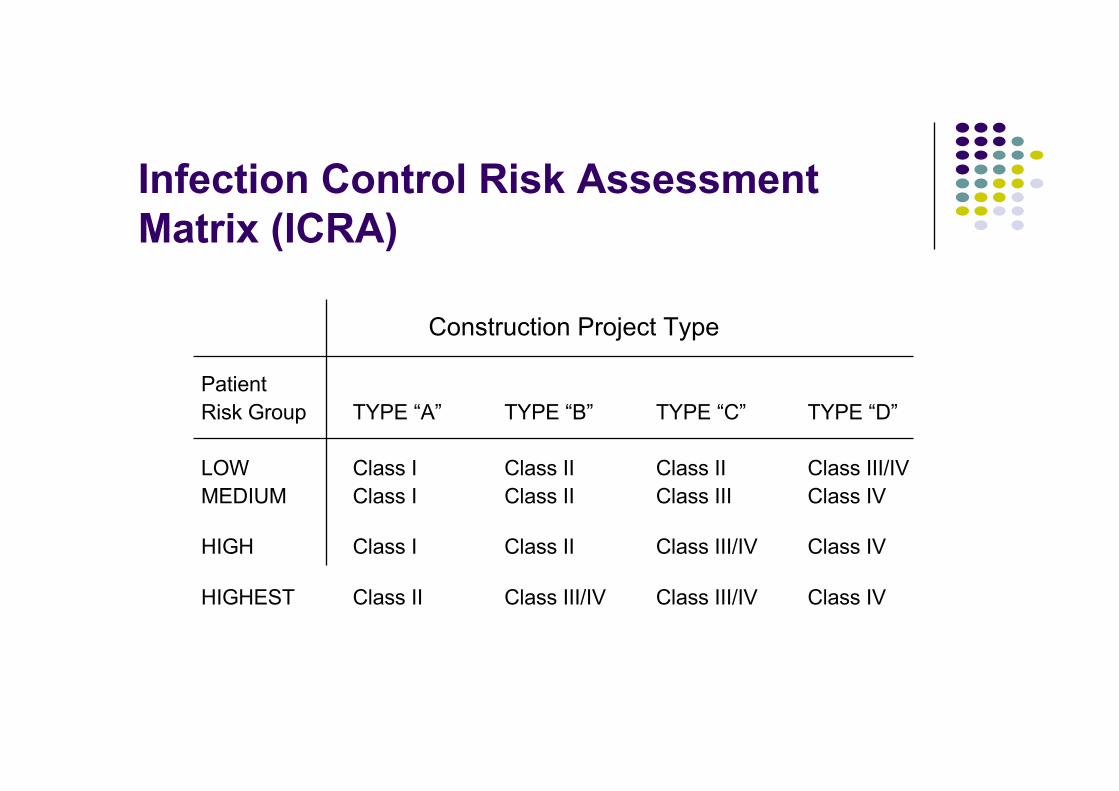
Infection Control Risk Assessment Matrix (ICRA)
Construction Project Type
Patient Risk Group TYPE “A” TYPE “B” TYPE “C” TYPE “D”
LOW Class I Class II Class II Class III/IVMEDIUM Class I Class II Class III Class IV
HIGH Class I Class II Class III/IV Class IV
HIGHEST Class II Class III/IV Class III/IV Class IV

Air sampling
1716
Passive SamplingPassive air sampling entails the placing of solid nutrient media in the open air to allow airborne particles to settle upon the plate due to gravity. The plates are left open in the area to be tested for a predetermined period of time then incubated and the results read as total CFU. The results from settle plates are considered neither quantitative nor qualitative. The following table lists some of the advantages and disadvantages of settle plates:
Advantages
• Cheap • Widely available • Multiple simultaneous sampling • Meaningful surface sample results • Reproduces real conditions • Sterile • Room airflow is not disturbed • Comparable results
Disadvantages
• Not quantitative • Not qualitative • Selectively collects larger particles • Results are not widely accepted • Not suitable for commissioning theatres
General criticism of settle plate sampling centres on the lack of correlation with active sampling results.13 However settle plates may be useful as they allow the study of airborne contaminants settling onto horizontal surfaces.
It has been shown that bacterial counts obtained from wound washes closely correlate with those of settle plates.13 This concludes that a settle plate exhibits similar characteristics to that of an exposed wound. On this basis settle plates should be considered as an adjunct to infection control investigations, particularly in operating suites.
In an attempt to standardise passive air sampling, the 1/1/1 sampling scheme offers a methodology for sampling with settle plates.14 This method suggests settle plates are positioned one metre off the floor, one metre from the walls or any obstacle and left open for one hour.
Active Sampling Procedure The main principle of active sampling of air is to sample the air for the enumeration of bacteria and fungi. As part of a building program or as an aid to investigation into infection clusters, air sampling is conducted at an interval determined by the Infection Control Committee, to determine fungi including Aspergillus fumigatus spore loads.
Equipment
Microbial Air Monitoring System Merck MAS-100.
The following sampling procedure is based on using a Merck MAS-100. The Merck is an impactor type of instrument based upon the principles described by Andersen, which aspirates air through a perforated plate. The resulting air-stream, which contains particles, is directed onto the agar surface of a standard Petri dish. After a collection cycle the Petri dish is incubated and the colonies are counted and expressed as colony forming units (CFU/m3). Other sampler types and brands are available. All samplers have advantages and disadvantages that should be considered prior to purchase.16 It is important to fully consider what is required of a sampler prior to purchase.
18 19
13. The edges of the petri dish are then covered with parafilm to prevent contamination during transport and spread of fungal spores during incubation.
14. Incubate the SABG plates at 30ªC for 7 days for total fungal counts or at 36ªC for 7 days for selective Aspergillus spp counts.
15. The fungal culture is examined at 4 days and 7 days. Handle plates very carefully especially at the 4 day reading. Take care not to spread spores as the plates are reincubated for up to 7 days.
16. Record: Total fungal count (Colony Forming Units, CFU) Aspergillus spp CFU Aspergillus fumigatus CFU
Confirm any Aspergillus fumigatus cultures by microscopic examination and record results.
The CFU counts will require adjustment if the colony count is >21 according to the positive hole conversion table. The microbial count is corrected based on Fellar’s statistical correction table (see page 17 Manufacturer’s Manual or appendix). The principle of this correction table is; “as the number of organisms per sample rises, the chance that several organisms will enter the same hole in the perforated lid also increases”. Two micro-organisms in the same hole will only produce one colony.
Interpretation:
There are no guidelines for the interpretation of fungal counts in the general environment.
Fungal counts should not vary significantly from baseline values (refer to initial and previous test results). Report results to a supervisor if results exceed:
• >0.1 CFU/m3 of Aspergillus fumigatus in a protective environment
• >1 CFU/m3 of Aspergillus fumigatus in an area with at risk patients
• >4 CFU/m3 of Aspergillus fumigatus in a general area.
The number of colony forming units that are counted on the Petri dish after appropriate incubation needs a statistical correction. The number of colonies is then related to the number of organisms per cubic meter of air sampled. This kind of correction was first described by mathematician, FELLER in 1950.(Active air sampling methodology reproduced with the kind permission of Austin & Repatriation Medical Centre, Microbiology Department)

Interpretation of fungal monitoringl No standardized guidelines for interpretation
l Regular monitoring to see performance over time

Roles of stakeholdersl Project officers
l Identify essential services that may be disrupted
l Liaise with ICN and managers to identify patient population at risk and implement appropriate preventive measures
l Area managersl Risk assessmentl Compliance checks
l Infection control personnell Advisoryl Audits
Conclusionl Effective planning and strict implementation of Infection
Prevention & Control Guidelines related to Renovation and Construction will prevent construction-related HAIs
l Teamworkl Awarenessl Educationl Policy and audits

Thank you