considerations in design of removable prosthetic devices with no posterior abutments
TRANSCRIPT

Removable partial prosthodmties
Conshtiions in design of devices with no posterior abutments
ic
Edward Boero, D.D.S.,* and Wilfred G. Forbes, D.D.S.** University of the Pacific, San Francisco, Calif.
T I n restorative dentistry, emphasis has been placed on terminology, philosophies, and techniques. These are important. However, a thorough understanding of basic me- chanics and biology would be more helpful in solving the problem of restoring denti- tions and maintaining the good health of the remaining teeth and tissues.
The basis of good restorative dentistry consists of establishing an equilibrium of forces SO stresses are conducive to developing a physiologic continuum rather than pathosis. Thus, when the loads are applied on the restorations, the sums of the vec- tors of the forces against the tissues should be normal at all points. This would re- sult in the soft tissue supporting a load being in a state of uniform displacement ex- cept at the denture borders of the denture base (Fig. 1) .
This ideal situation is most closely approached when the restoration allows the concentrated force of the occlusal load to be collinear with the long axes of the teeth (Fig. 2). This allows the forces (Fig. 3) to be distributed perpendicular to a tangent of the interface at the periodontal ligament with the tooth and bone (Fig. 2). The occlusal forces are controlled by the shape of the tooth so that, in the functional masticator-y stroke, the cusps never contact any tooth surface other than those sur- faces in which the resultant force will coincide with the long axes of the teeth (Fig. 4, A and B) .
A removable partial denture has two basic considerations in function: These are (1) a rigid casting over the bone of the residual ridge which has a practically incompressible mucosa between the casting and bone (Fig. 5, A) and (2) a rigid tooth which is in a rigid socket with a practically incompressible periodontal liga- ment between the tooth and the bone (Fig. 5, B) .
Presented before the Thirty-Sixth Annual meeting of the Pacific Coast Society of Pros- thodontists, Palo Alto, Calif.
*Professor of Prosthetic Dentistry Emeritus, Former Chairman, Department of Fixed and Removable Partial Dentures.
**Associate Professor of Prosthetic Dentistry, Department of Oral Diagnosis.
253

254 Boero and Forbes
Fig. 1
J. Prosthet. Dent. September, 1972
200 Ibs./ Sq. inch
DISPLACEMENT NORMAL THICKNESS I/IO,• OO OF AN’ INCH TRIPLED IN THICKNESS 27/10,000 OF AN INCH
Fig. 1. A cross section of the residual ridge and denture base of a removable partial denture. The arrows at the interface of the mucosa and base show the directions of forces on the base and the mucosa to be uniformly distributed when the load on the base is ideally applied.
Fig. 2. Cross section of one side of a mandible through a molar tooth. Note the uniform distribution of forces when the applied load of a concentrated force is in its ideal position and direction.
In the first system, the internal surface of the casting can be likened to the tooth socket; in the second, the bone can be likened to the tooth. Both systems have tissue cells (composed largely of water) between two essentially rigid bodies.
EFFECT OF TISSUE THICKNESS
The difference between the two systems, from an analytical viewpoint, lies in the different thicknesses of tissue between the two rigid bodies. Gabel,l in assessing the displacement of a tooth in its socket, came to the conclusion that, if a force of 1,300 p.s.i. were applied to a tooth along its long axis, the .tooth would be displaced ~,eoe of an inch. Using Synge’s mathematical deduction+ 3. concerning the compressibility of the periodontal membrane, Gabel deduced that, ,when a load was applied to a tooth in its socket, the amount of displacement of the tooth varied as a cube of the thickness of the periodontal ligament. In other words, if the thickness of the perio- dontal ligament would be doubled and if 1,300 p.s.i. were the assigned load, the tooth would be displaced R/l,000 of an inch; if the thickness was tripled, the dis- placement would be 27/1,eoe of an inch. If an assigned load of 200 p.sj. would give a displacement of l/lo,eeo of an inch and. if the thickness of the tissue were then tripled, the displacement would be 27/10,000 of an inch.
Fig. 2

Volume 28 Number 3 Design of prosthetic devices 255
Fig. 3. (A) A diagram illustrating the placement of a concentrated force (F) passing through the centroid of a rigid body (located at the interface of the contacting surfaces) which results in the uniform distribution of the load. (B) A diagram illustrating the placement of a concentrated force (F) passing through some point other than the centroid which wc)uld permit a lifting force (L) to more easily displace the rigid body.
A
Fig. 4. (A) A cross section through an upper and lower molar in which the tip of the protocone occludes into the base of the talonid. In this situation, the resultant force of occluding teeth can be made to more easily coincide with the long axis of the teeth. (B) An impression of the maxillary and mandibular teeth at the intercuspation position of a subject having an ideal occlusion. Note the relatively large amount of space surrounding the cusps and fossae of tln:se occluding teeth.
Dyment and Synge,4 assuming the periodontal membrane to be compressible, arrived at somewhat different figures. However, both studies agree that the thicker mucosal tissue permits more displacement than the thinner periodontal membrane will allow (Figs. 2 and 5) .
MOTIONS OF PARTIAL DENTURES
To visualize the motions possible by a partial denture in function (Fig. 6)) it is necessary to consider the controls inherent in the positions of occlusal rests (which can define an axis of rotation), clasps (which can, in developing an axis of rotation,

256 Boero and Forbes J. Pros&et. Dent. September, 1972
Fig. 5. A cross section of the maxillae in the region of the first molar showing a difference in thickness of the mucosa over the residual ridge (A) and the periodontal ligament of the tooth (B).
Y
Fig. 6, A-D. An illustration of one of the techniques that may be used for visualizing and assessing the motions of a removable free-end partial denture. (A) The partial denture is visualized as having no restrictions against any motion. (B) A right-handed Cartesian co- ordinate system is developed as a basis of reference. In this instance, the origin is placed at the centroid of the area covered by the denture base of the partial denture, and the Y axis is placed collinear with an ideal concentrated force. (C) An illustration of translation (T) parallel to the Y axis. (D) An illustration of translation (T) parallel to the X axis.

Design of prosthetic deuices 257
Fig. 6, E-H. Continuation of Fig. 6, A-D. (E) An illustration of translation (T) parallel to the Z axis. (F) An illustration of rotation (R) around an axis parallel to the Y axis. (Cl An illustration of rotation (R) around an axis paraHe1 to the X axis. (H) An ilhtstration of rotation (R) around an axis parallel to the Z axis. Each motion is a degree of freedom. A body in space subject to no restrictions is capable of any of the motions or any combination of the motions illustrated at any instant in time. A body free to move in all six of the degrees of freedom at the same instant in time is said to have six degrees of freedom.
apply torque to a tooth), and the occlusion (which can cause translator-y motiuns) . This article will develop a reference system related to the centroid (origin of the system) of the area to be covered by the denture base and with one axis collinear with the direction of an ideal concentrated force (Fig. 7).
After assessing the ideal equilibrium of forces developed by the partial denture under load, the type of occlusion, the type and location of clasps, the locations of
the rests, and the type of stress directors, the partial denture can be made to most favorably distribute the occlusal load to the periodontal membranes and to the mu- cosa covered by the denture base.
Much consideration must be given to the vertical force in the sagittal plane in the design of free end partial dentures. This force often creates unwanted displace-
258 Boero and Forbes f. Prosthet. Dent. September, 1972
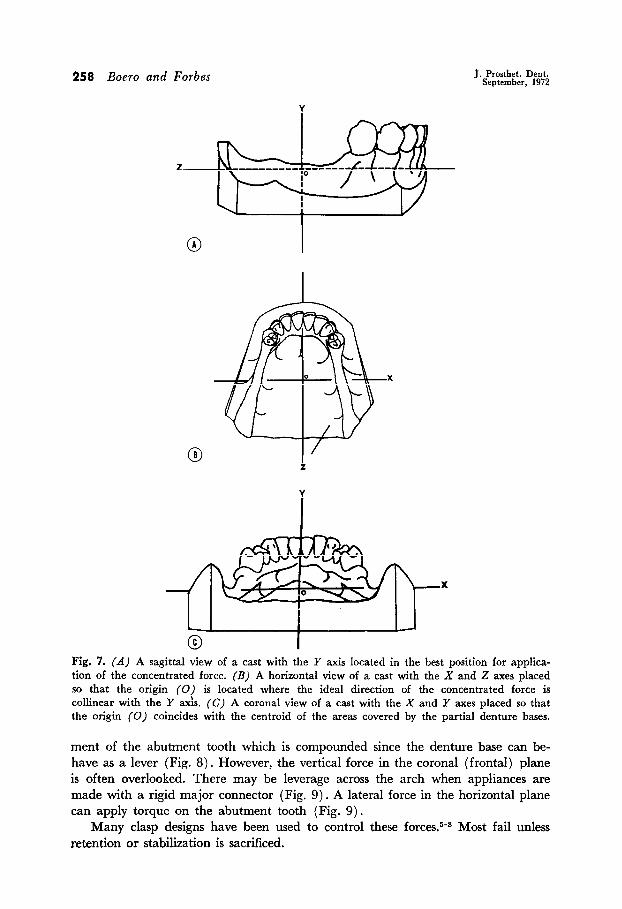
Fig. 7. (A) A sagittal view of a cast with the Y axis located in the best position for applica- tion of the concentrated force. (Bj A horizontal view of a cast with the X and Z axes placed so that the origin (0) is located where the ideal direction of the concentrated force is collinear with the Y axis. (C) A coronal view of a cast with the X and Y axes placed so that the origin (0) coincides with the centroid of the areas covered by the partial denture bases.
ment of the abutment tooth which is compounded since the denture base can be- have as a lever (Fig. 8). However, the vertical force in the coronal (frontal) plane is often overlooked. There may be leverage across the arch when appliances are made with a rigid major connector (Fig. 9) . A lateral force in the horizontal plane can apply torque on the abutment tooth (Fig. 9).
Many clasp designs have been used to control these forces.5*s Most fail unless retention or stabilization is sacrificed.
Volume 28 Number 3 Design of prosthetic devices 259
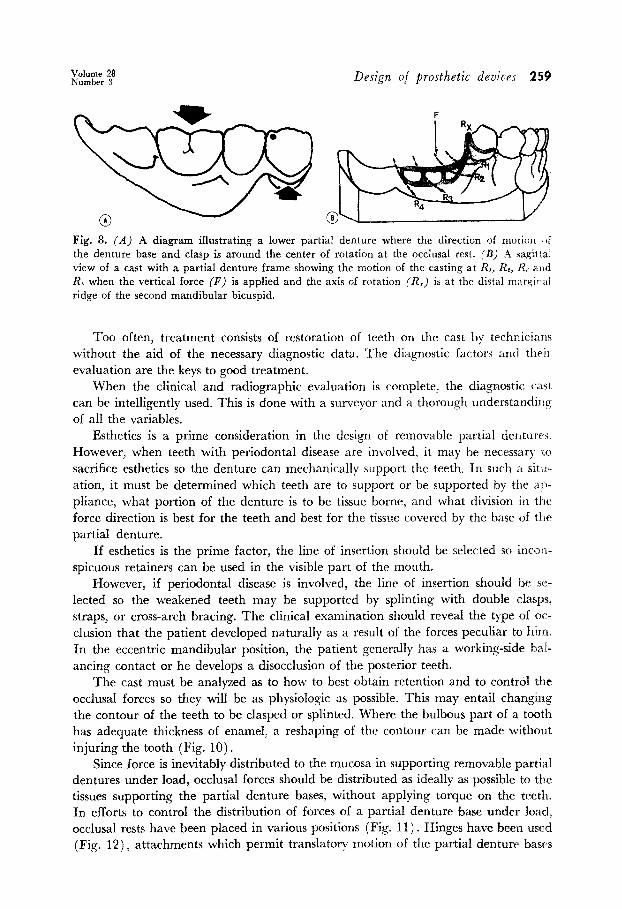
Fig. 8. (A) A diagram illustrating a lower partial denture where the direction of motion td
the denture base and clasp is around the center of rotation at the occlusal rest. (B) .4 sagrttal view of a cast with a partial denture frame showing the motion of the casting at RI, IL, 1-L and RL when the vertical force (F) is applied and the axis of rotation (R,) is at the distal marginJ1 ridge of the second mandibular bicuspid.
Too often, treatment consists of restoration of teeth on the cast by technicians without the aid of the necessary diagnostic data. The diagnostic factors and their evaluation are the keys to good treatment.
When the clinical and radiographic evaluation is complete, the diagnostic cast can be intelligently used. This is done with a surveyor and a thorough understanding of all the variables.
Esthetics is a prime consideration in the design of removable partial dentures. However, when teeth with periodontal disease are involved, it may be necessary LO sacrifice esthetics so the denture can mechanically support the teeth, In such a sitrt- ation, it must be determined which teeth are to support or be supported by the al+ pliance, what portion of the denture is to be tissue borne, and what division in the
force direction is best for the teeth and best for the tissue covered by the base of tlz partial denture.
If esthetics is the prime factor, the line of insertion should be selected so incon- spicuous retainers can be used in the visible part of the mouth.
However, if periodontal disease is involved, the line of insertion should be se- lected so the weakened teeth may be supported by splinting with double clasps, straps, or cross-arch bracing. The clinical examination should reveal the type of oc- elusion that the patient developed naturally as a result of the forces peculiar to him. In the eccentric mandibular position, the patient generally has a working-side bal- ancing contact or he develops a disocclusion of the posterior teeth.
The cast must be analyzed as to how to best obtain retention and to control the occlusal forces so they will be as physiologic as possible. This may entail changing the contour of the teeth to be clasped or splinted. Where the bulbous part of a tooth has adequate thickness of enamel, a reshaping of the contour can be made without injuring the tooth (Fig. 10).
Since force is inevitably distributed to the mucosa in supporting removable partial dentures under load, occlusal forces should be distributed as ideally as possible to the tissues supporting the partial denture bases, without applying torque on the teeth. In efforts to control the distribution of forces of a partial denture base under load, occlusal rests have been placed in various positions (Fig. 11) . Hinges have been used (Fig. 12)) attachments which permit translatory motion of the partial denture basrs

260 Boero and Forbes J. Prosthct. Dent. September, 1912
Fig. 9. (A) A coronal view of a cast with a partial denture frame which shows the motion of the casting at RI, RI, and R3 when the vertical force (F) is applied to the opposite side of the arch from the axis of rotation (R,). (B) A coronal view of a cast with a partial denture frame showing the motion of the casting at RI and RI when the vertical farce (F) ia applied on the same side of the arch as the axis of rotation (R.). (C) A view in the horizontal plane of a cast with a partial denture frame showing the possible motion around the axis (RJ when disharmony of occlusion is due to the contact on an incline plane.
have been used (Fig. 13), and clasps have been designed to disengage themselves from the teeth.” The translatory motion should be parallel with the idealized con- centrated force along the Y axis (Figs. 6 and 7). The occlusion of the teeth should be developed so the concentrated force transmitted to the partial denture is as close to being coIlinear with the Y axis as is possible to make it (Fig. 7),

Volume 28 Number 3 Design of prosthetic devices 261
Fig. 10. (A) A mesiodistal section of a maxillary canine illustrating the bulk of enamel in the region of the middle one third of the crown of the tooth. (B) A mesiodistal section of a maxillary canine after a small amount of enamel has been removed. This often helps to im- prove clasp design without materially harming the tooth. (C) A bucco lingual section of a mandibular bicuspid after being contoured on the lingual surface. This would permit a clasp or lingual casting to be placed in a more apical position. (D) A bucco lingual section of a mandibular bicuspid showing the lingual contour of the tooth without any alterations. Com- pare the contour and bulk of enamel with C.
Fig. 11. A sagittal view of a cast which illustrates the arcs of rotation controlled by the position of the rest at points I, 2, or 3. The rest at position 1 shows the arc of rotation with a line of dots. The rest at position 2 shows the arc of rotation with a broken line. The rest at position 3 shows the arc of rotation as a solid line. Fig. 12. A sagittal view of a cast illustrating the arcs of rotation at points B, C, D, and E which are defined by the hinge located at A.
262 Boero and Forbes J. Prosthet. Dent. September, 1972
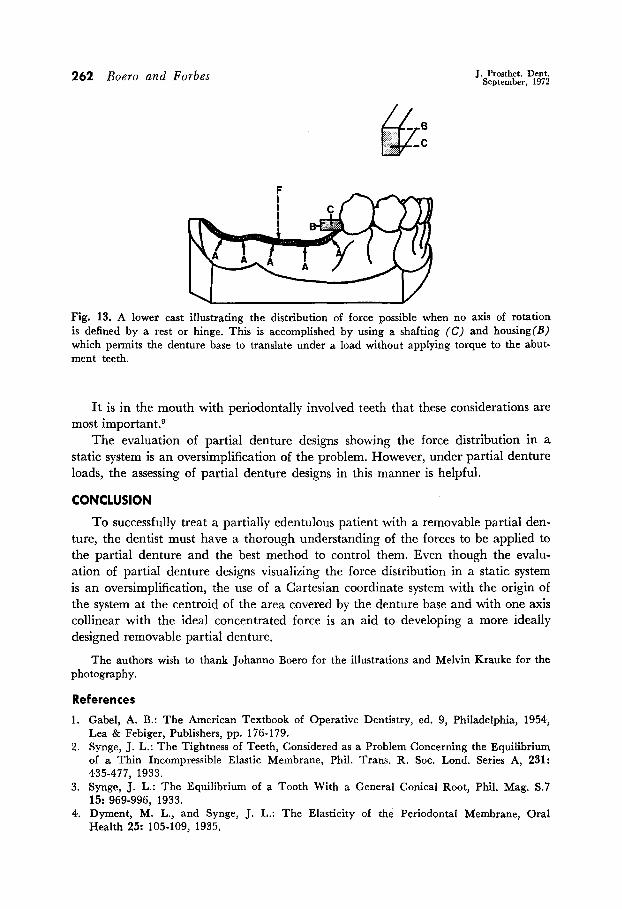
Fig. 13. A lower cast illustrating the distribution of force possible when no axis of rotation is defined by a rest or hinge. This is accomplished by using a shafting (C) and housing(B) which permits the denture base to translate under a load without applying torque to the abut- ment teeth.
It is in the mouth with periodontally involved teeth that these considerations are most important.g
The evaluation of partial denture designs showing the force distribution in a static system is an oversimplification of the problem. However, under partial denture loads, the assessing of partial denture designs in this manner is helpful.
CONCLUSION
To successfully treat a partially edentulous patient with a removable partial den- ture, the dentist must have a thorough understanding of the forces to be applied to the partial denture and the best method to control them. Even though the evalu- ation of partial denture designs visualizing the force distribution in a static system is an oversimplification, the use of a Cartesian coordinate system with the origin of the system at the centroid of the area covered by the denture base and with one axis collinear with the ideal concentrated force is an aid to developing a more ideally designed removable partial denture.
The authors wish to thank Johann0 Boero for the illustrations and Melvin Krauke for the photography.
References
1. Gabel, A. B.: The American Textbook of Operative Dentistry, ed. 9, Philadelphia, 1954, Lea & Febiger, Publishers, pp. 176-179.
2. Synge, J. L.: The Tightness of Teeth, Considered as a Problem Concerning the Equilibrium of a Thin Incompressible Elastic Membrane, Phil. Trans. R. Sot. Lond. Series A, 231: 435-477, 1933.
3. Synge, J. L.: The Equilibrium of a Tooth With a General Conical Root, Phil. Mag. S.7 15: 969-996, 1933.
4. Dyment, M. L., and Synge, J. L.: The Elasticity of the Periodontal Membrane, Oral Health 25: 105-109, 1935.

Design O/ prosthetic devices 263
5. Roach, F. E.: Principles and Essentials of Bar Clasp Partial Dentures, J. Am. Dent. .4ss~. 17: 124-138, 1930.
6. Clayton, J. A., and Jaslow, C.: A Measurement of Clasp Forces on Teeth, J. PROSTH~ 1, DENT. 25: 21-43, 1971.
7. Cecconi, B. T., Asgar, K., and Dootz, E.: The Effect of Partial Denture Clasp Design <*II Abutment Tooth Movement, J. PROSTHET. DENT. 25: 44-56, 1971.
8. Roach, F. E.: Principles and Essentials of Bar Clasp Partial Dentures, J. Am. Dent. :~SSW. 17: 124-138, 1930.
9. Geissler, P. R.: Disjunct Dentures for Patients with Teeth of Poor Prognosis, Dent. Pratt. Dent. Rec. 15: 421-423, 1965.
DR. BOERO 908 E ST.
SAN RAFAEL, CALIF. 94901
DR. FORBES UNIVERSITY OF THE PACIFIC SCHOOL OF DENTISTRY 2155 WEBSTER ST. SAN FRANCISCO, CALIF. 9411.5