connected health data meets the people: diversity, standards, and trust
TRANSCRIPT

@HL7 @efmi @chronaki @fridsma @eva_turk @annemoen_oslo
Connected health data meet the people: diversity, standards, and trust
The EFMI – HL7 partner event,
Thursday May 11th, 2017

www.efmi.org www.HL7.eu
This event is a continuation from previous partner events
2015 2016

• Federation of • 31 National societies for Medical Informatics in Europe• Institutional members from Academia and Industry
• Founded in 1978
• Activities • Medical Informatics Europe conferences, annually• Special topic conferences • Collaboration in research and policy at European level• 14 standing working groups,
• From standards, human factors, evaluation to education
www.efmi.org

4
HL7 Foundation: who we are..
HL7 Vision: A world in which everyone can securely access and use the right health data when and where they need it.
May 11, 2017
eHealthWeek2017
Malta
HL7 the best and most widely-used
eHealth standards since 1986
HL7 v2
Clinical Document Architecture
CIMI
HL7 FHIR
19 National Affiliates in Europe (~38 wordwide)
European HL7 foundation established in 2010
European Funded Research Projects
Annual HL7 in Europe Newsletter
Website: www.HL7.eu
eHealth policy & Research
SDO Joint Initiative Council

www.estandards-project.eu
Vision of eStandardseHealth Standards and Profiles in Action for Europe and Beyond
• Vision of the global eHealth ecosystem
– people need navigation tools for safe and informed health care
– interoperability assets fuel creativity, entrepreneurship, and innovation
• eStandards will:
– nurture digital health innovation
– strengthen Europe’s voice & impact
– enable co-creation and trusted provider-user relationships
Base Standards
Use Case basedStandards Sets
Assurance and Testing
LiveDeployment
Feedback and Maintenance
Tooling and Education
Forums and Monitoring
eStandards

www.estandards-project.eu
What do we need to make digital health work with standards and interoperability?
• Co-create
–to make it real using standards
• Governance
–to make it scale to large-scale deployment
• Alignment
–to make it stay in a sustainable way

© HIMSS Europe GmbH 8
CONNECTED HEALTH DATA MEET THE PEOPLE:
DIVERSITY, STANDARDS, AND TRUST
Using health data in a connected world requires new competencies, a
personal digital health compass calibrated to individual personalities
and needs.
– Patients and clinicians able to collect & manage data,
– Data-operational informatics professionals to analyze data,
– Cutting-edge researchers, innovators, and educators to apply knowledge
…will take learning health systems to the next level.
Topics for discussion:
– strategies for empowering and activating people to engage, share and use their
health data.
– diversity, trust, and HL7 FHIR to open up access and capacities and manage
data safely for patients, care-givers, and the health system.

© HIMSS Europe GmbH 9
PANELISTS
• Maturing a Telemedicine Infrastructure (MaTIS)- building the
human capital
• Health Professional Education in Biomedical & Health
Informatics: Accreditation and Certification – EFMI AC2
Initiative
• Digital health literacy: a necessity for Activating Citizens
• “Internet of People”: the elements of quality, safety and trust
• Putting it all together: The need for a learning health system
• Discussion

Maturing a Telemedicine Infrastructure (MaTIS)- building the human capital
Morten BRUUN-RASMUSSEN
MEDIQEFMI-HL7 Partner event. Malta. May 11th 2017
Denmark
5,5 mill. inhabitants
90,1% Danish
9,9 % other
5 Regions
98 Municipalities
Equal and free access to healthcare
MEDIQ

Disseminate telemedicine home monitoring to citizens with COPDin the entire country before the end of 2019
The dissemination is anchored in five programs with participation of regions and municipalities, which are responsible to ensure progress and realization of benefits
In addition an collective public portfolio steering group is established, to coordinate the national prerequisite projects and monitor the progress
Launch of preparing a national telemedicine infrastructure
Economic agreement for 2016
12 MEDIQ

NorthDK
(Region,Municipalities,
GP’s)
CentreDK
(Region,Municipalities,
GP’s)
SouthDK
(Region,Municipalities,
GP’s)
SealandDK
(Region,Municipalities,
GP’s)
CapitalDK
(Region,Municipalities,
GP’s)
Projects
Possiblecross sector
projects
Services&
logistics
Cross sectorprojects
Collective public portfolio steering group
Dissemination to patients with COPDis anchored in five programs
Collective public portfolio secretariat
ClinicalGuidelines
Nationalinfra-
structure
NewBusiness
Case
Blue: Municipal/regional ownershipRed: Collective public ownership
Nationalprerequisite projects
National boardof eHealth
Comprehensive governance
MEDIQ13
MaTIS
Scope?
MEDIQ14
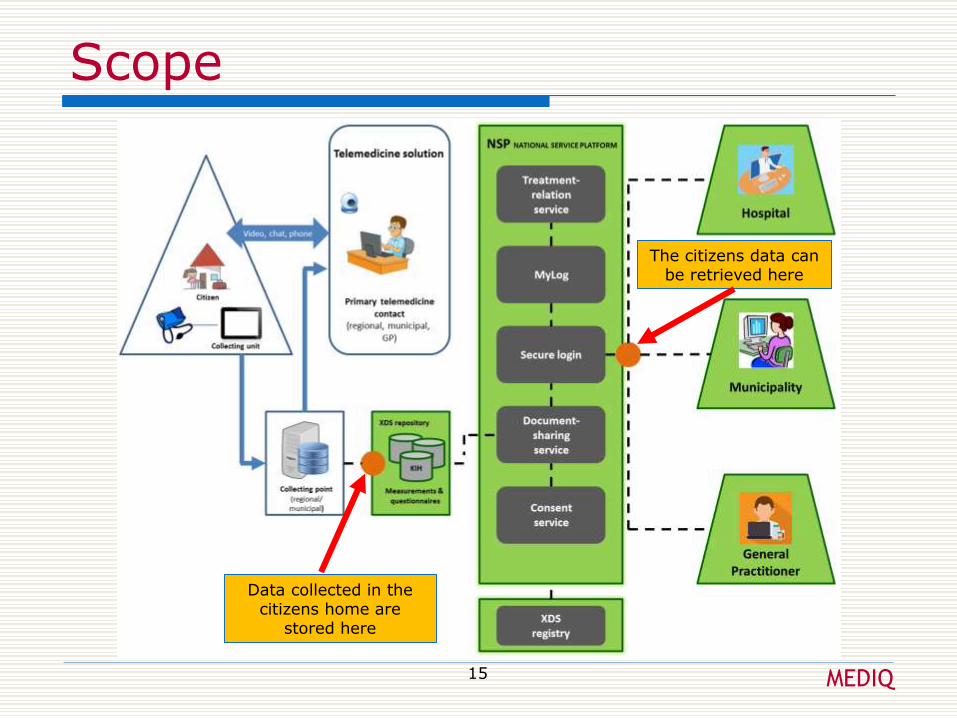
Scope
MEDIQ15
Data collected in the citizens home are
stored here
The citizens data can be retrieved here

Maturity of the infrastructure
MEDIQ16
MaTIS. TRL 7+. March 2017
Project management
Work Plan (WPs, Activities …) - as usual
Risk management
Develop a plan B for all critical activities ahead
If a potential risk, which will delay the project is detected, start plan B in parallel
Project and risk management
17 MEDIQ

Complexity management
Keep It Simple St…. (KISS)
The complexity shall be ..
Do not try to solve all problems
Engage the community
Inform also about what the solution not can do
Listen to other views/critic
Complexity management
18 MEDIQ

Handing over the infrastructure
MEDIQ19

Acknowledgement
MEDIQ
The National Board of eHealth Datawww.sundhedsdatastyrelsen.dk
MedComwww.medcom.dk
Health Professional Education in Biomedical & Health Informatics:
Accreditation and Certification – EFMI AC2 Initiative
John Mantas
Chair of the EFMI AC2 Task,
Hon Fellow EFMI

Accreditation
What• Accreditation is a diligent evaluation and monitoring
peer review process assuring that educational programs
and institutions meet academic standards, operational
integrity and quality.
Why• Accreditation is proof that a collegiate program has met
standards essential to produce graduates ready to enterthe critical fields of biomedical and health informatics.

Certification
What
• Certification is a credentialing process that
demonstrates and honor qualifications that an individual
can perform a specific professional role, or set of tasks.
Why
• Certification in Health Informatics is a requirement for
many professionals in many clinical institutions. Even
those professionals having acquired earlier degrees in
related fields to Health Informatics is required to update
and certify their current knowledge and skills.

What, Why, How (cont.)
There is a great number of European Universities and
Institutions implementing and having established
programs (undergraduate and postgraduate) in the
field of Biomedical and Health Informatics.
Visit the WG EDU page on www.efmi.org


• In Europe accreditation of academic programs is
provided as a requirement by governmental
agencies looking for program infrastructure,
integrity and quality.
• However, added value will be visible for a programs
when a Scientific Organization, such as EFMI,
provides accreditation in terms of peer reviewing
the contents of the curriculum whether meeting the
educational standards in our field of BMHI.
What, Why, How (cont.)
Procedure for Accreditation
Stepwise Approach procedure suggested for the
Implementation of the Accreditation, as follows:
Step 1: The program to be accredited applies via its authorities
(Dean, Program Director) to EFMI.
Step 2: The program is asked to prepare a self assessment report
(where also scope of program is defined). Template is provided.

Step 3: Accreditation Committee appoints a 3 members site visit
committee in the field of BMHI and experience in educational
programs; objectivity, independency, and transparency should be
fully observed.
Step 4: The site visit committee reviews the self-assessment
report and makes observations for possible additional
information to be provided.
Step 5: A site visit is agreed and planned with the program
authorities and the site visit committee.
Procedure for Accreditation
Step 6: The site visit committee provides an evaluation report
and judgement made based on predefined criteria and the result
and recommendations are announced at the spot
Step 7: The report is submitted to the Accreditation Committee.
The program director may provide additional information or
mention factual errors on the report. Final decision is taken by
the Accreditation Committee on advice from the site visit
committee.
Step 8: Accreditation is provided to the Program for a period of
3 years and program director is informed about the expiration
date.
Procedure for Accreditation

SWOT Analysis
Strengths
• EFMI is a European federation of national associations situated
in most European countries. The scientific and professional
community of Biomedical and Health Informatics is reflected
in EFMI as it is yearly depicted in the MIE Conferences.
Weaknesses
• EFMI is a volunteer organization without solid professional
secretariat support. Also decisions are delayed due to the
internal procedures. Clear mandates should be given to the
Accreditation and Certification Committee to ensure
minimization of bureaucracy leading to delays in
implementation and decisions taken.
SWOT Analysis
Opportunities
• Very few Universities/Institutions with programmes in
Health Informatics have been accredited by an
International organization. Similar initiatives had little
effect in Europe. In addition no Certification
programmes are established yet in Europe in our field.
Threats
• Other international organizations, some of them, more
professional ones than EFMI, have initiated similar
actions and they may apply them in Europe very soon.

Conclusions
• EFMI is determined to play an important role in both Accreditation and
Certification in the field of Biomedical and Health Informatics.
• The Scope of EFMI as a not-for-profit organization is to offer services to
the academic institutions and to professionals in health Informatics in
Europe. All cost related calculations will be based strictly on this
principle.
• To achieve this end we will require the active involvement and support of
our community and partners.

Digital Health Literacy:
a necessity for Activating People
Anne Moen, RN, PhD, FACMIProfessor, Director UiO:eColab
IMIA Vice President and Past President EFMI
Oslo, Norway [email protected]
@ annemoen_oslo

Citizens – what do they do ? Examples of storing and organizing health information artifacts in spaces
Moen A, Brennan PF. Health@Home: the work of Health Information Management in the Household (HIMH) - implications for Consumer Health Informatics (CHI) innovations. Journal of the American Medical Informatics Association, 2005;12:648-56.

Digital Health Literacy
@ annemoen_oslo
…. the ability to seek, find, understand,
and appraise health information from
electronic sources ….
… apply the knowledge gained to
addressing or solving a health problem …
Norman & Skinner (2006)

Personalized – universally designed tools
• Requirement – patient & family participates actively– “the patient will see you now”
– “let patients’ help”
• Access
– Right to personal information in digital formData Portability (Directive 2016/679/EU), Re-use of public sector
information (Directive 2013/37/EU), Cross border healthcare (Directive
2011/14/EU)
• Presentation – Collaboration – Contribution – Confusion
– Accountability – Autonomy -
@ annemoen_oslo

Organization - Meal plan
- Suggested food
- Hot – cold drink
Orientation - Time, day
- Meals reported
- Friends and family
Visualization - Feedback when
reporting meal/drink
- Overview; day, week
Opportunity: support diet – healthy aging (1)
@ annemoen_oslo

Illustrate - # – type of meals
- Nutritional value
- Day – Week
Daily goals- Protein
- Energy
- Fluid
Overview- List of selection
- Grocery shopping
- Companion
Opportunity: Visualizing nutritional value (2)
@ annemoen_oslo

Activate citizens
@ annemoen_oslo
• Require focus at
– Tools that are usable for the purpose
– Easier access to data actionable knowledge
– Presentation that is easy to grasp
– Skills and capacities
– Personal integrity
– Trust in data and people

DNV GL © 2017
Ungraded
06 October 2016 SAFER, SMARTER, GREENERDNV GL © 2017
Ungraded
06 October 2016
Internet of People
40
Eva Turk, Stephen McAdam
DNV GL
DNV GL © 2017
Ungraded
06 October 2016
DNV GL Vision for Healthcare
41
Free from
preventable
harm
Effective and efficient
Personalized
to individual
needs
Seamless in delivery
With
equitable
access

DNV GL © 2017
Ungraded
06 October 2016
16 May 2017
42
Internet of People
Personalized,
Predictive,
Participatory and
Preventive
healthcare.
Network of collective
intelligence and
interactive
communication among
our digital selves

DNV GL © 2017
Ungraded
06 October 2016
Risks and barriers in adopting Internet of People
16 May 2017
43

DNV GL © 2017
Ungraded
06 October 2016
The biggest risks to the adoption of Internet of People
44
1. Ownership and access of which data2. Inequality in access3. Different rules and regulations in different geographical 4. Different IT laws and regulations in different countries 5. Risk of intellectual property rights infringement
1. Low acceptance of the Internet of People due to resistance to change 2. Professional resistance 3. Perceived as conflicting with some cultural values and beliefs 4. Time consuming5. Confusion in how digital data can and should be analysed

DNV GL © 2017
Ungraded
06 October 2016
How to build trust
45
Data governance

DNV GL © 2017
Ungraded
06 October 2016
3rd party digital platform
46

DNV GL © 2017
Ungraded
06 October 2016
How can DNV GL start building trust?
47
SharingExploring how our 3rd party role could facilitate the responsible sharing of quality assured sensitive genomic data
AssuranceHarmonizing, standardizing and developing mechanisms for quality assurance
GovernanceDeveloping models to assess the maturity of big data management and data quality

DNV GL © 2017
Ungraded
06 October 2016
SAFER, SMARTER, GREENER
www.dnvgl.com
www.dnvgl.com/internet-of-people
48
www.dnvgl.com/internet-of-people

CLICK TO EDIT MASTER TITLE STYLE
• Click to edit Master text styles– Second level
• Third level
© HIMSS Europe GmbH 49
Putting it all together: The need for a learning health system
Doug Fridsma, MD, PhD, FACP, FACMI
President and CEO, AMIA
49

CLICK TO EDIT MASTER TITLE STYLE
• Click to edit Master text styles– Second level
• Third level
© HIMSS Europe GmbH 50© HIMSS Europe GmbH 50
Patient
PATIENTS WILL BE FIRST ORDER PARTICIPANTS IN
HEALTH, HEALTHCARE AND RESEARCH
50

CLICK TO EDIT MASTER TITLE STYLE
• Click to edit Master text styles– Second level
• Third level
© HIMSS Europe GmbH 51© HIMSS Europe GmbH 51
Patient Practice
EHR WILL NOT BE THE MOST IMPORTANT
HEALTH IT
51

CLICK TO EDIT MASTER TITLE STYLE
• Click to edit Master text styles– Second level
• Third level
© HIMSS Europe GmbH 52
EHRs will not be the most important Health IT
CLICK TO EDIT MASTER TITLE STYLE
• Click to edit Master text styles– Second level
• Third level
© HIMSS Europe GmbH 53© HIMSS Europe GmbH 53
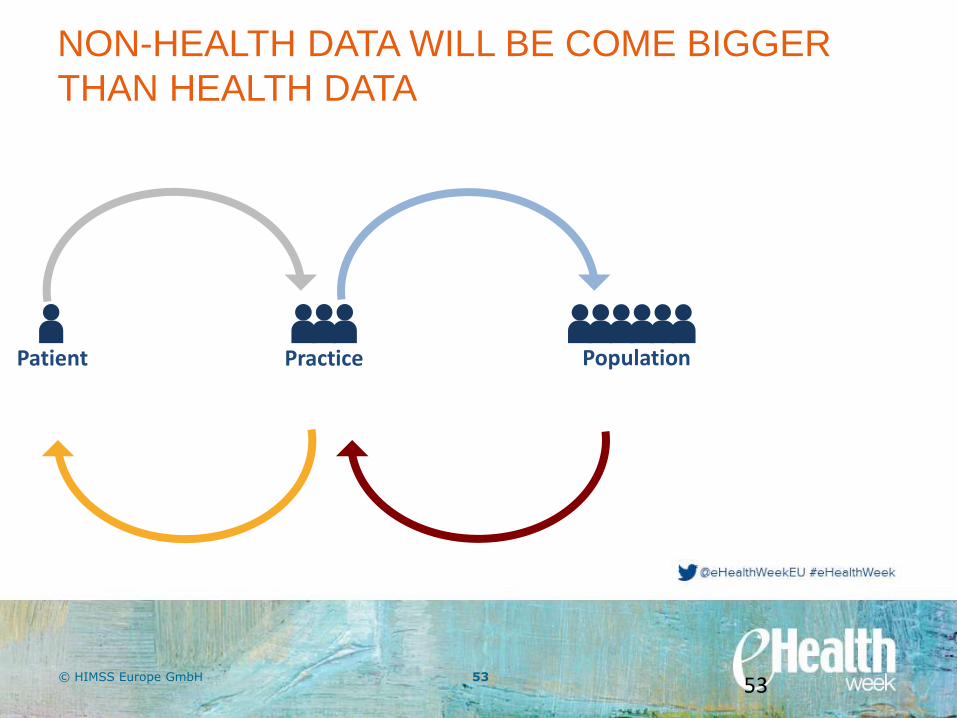
Patient Practice Population
NON-HEALTH DATA WILL BE COME BIGGER
THAN HEALTH DATA
53

CLICK TO EDIT MASTER TITLE STYLE
• Click to edit Master text styles– Second level
• Third level
© HIMSS Europe GmbH 54© HIMSS Europe GmbH 54
CLICK TO EDIT MASTER TITLE STYLE
• Click to edit Master text styles– Second level
• Third level
© HIMSS Europe GmbH 55© HIMSS Europe GmbH 55
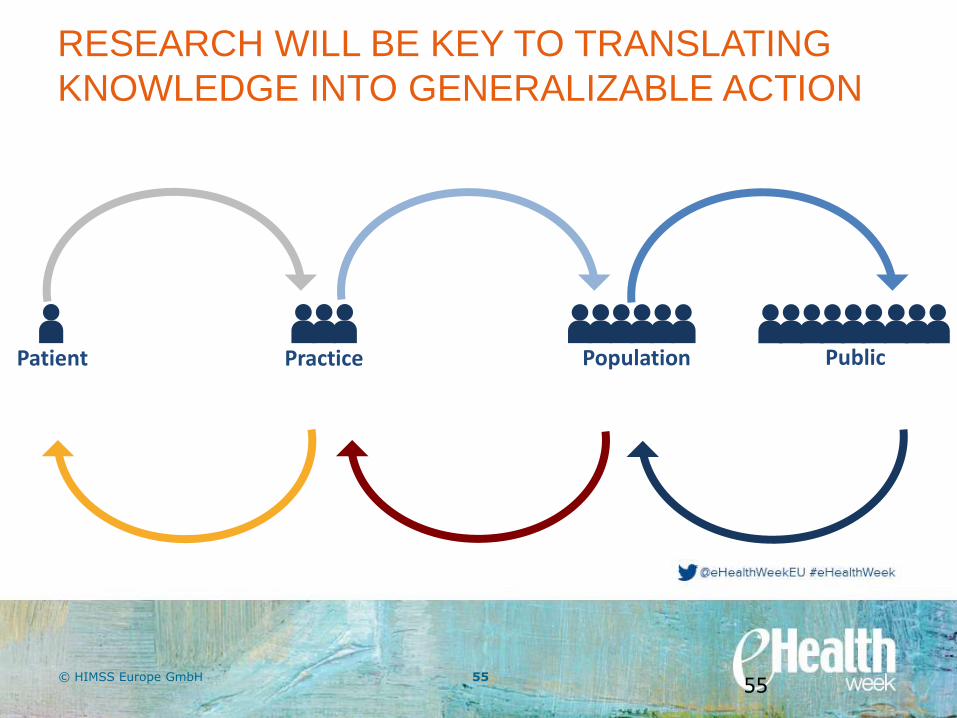
Patient Practice Population Public
RESEARCH WILL BE KEY TO TRANSLATING
KNOWLEDGE INTO GENERALIZABLE ACTION
55
CLICK TO EDIT MASTER TITLE STYLE
• Click to edit Master text styles– Second level
• Third level
© HIMSS Europe GmbH 56© HIMSS Europe GmbH 56
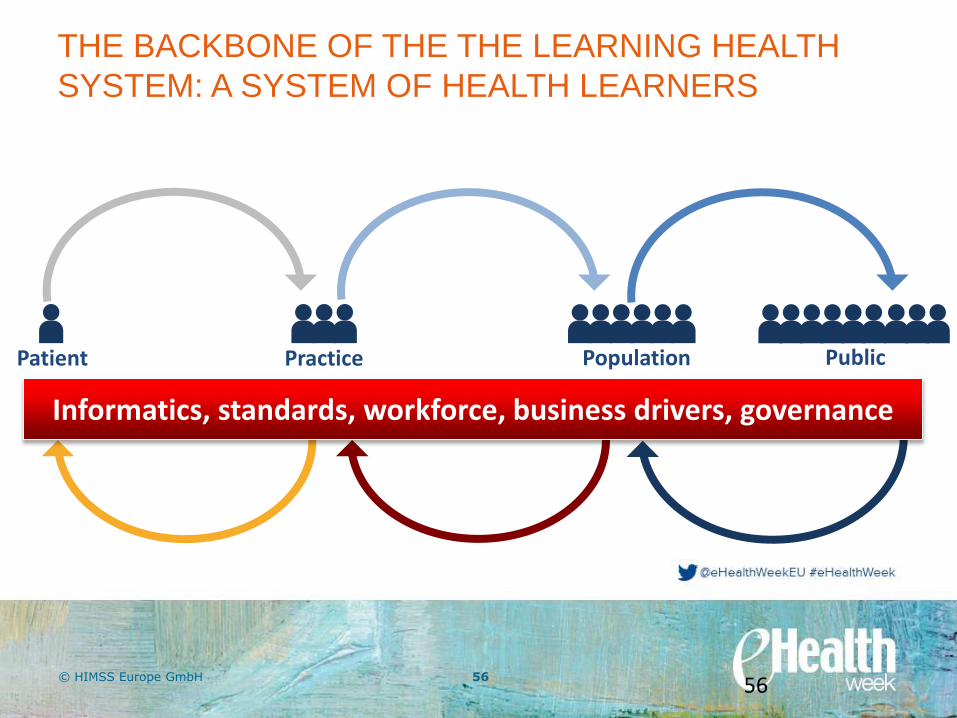
Patient Practice Population Public
THE BACKBONE OF THE THE LEARNING HEALTH
SYSTEM: A SYSTEM OF HEALTH LEARNERS
56
Informatics, standards, workforce, business drivers, governance

https://play.kahoot.it/#/k/f5de529b-4d8d-4b6d-a84c-e08d43f282b5

© HIMSS Europe GmbH 58
Join us at UPCOMING MEETINGS !
e-Health: equal access to health & sustainable growth